incident preclinical mobility disability (pcmd) increases future risk of new difficulty walking and...
TRANSCRIPT
Archives of Gerontology and Geriatrics 54 (2012) e329–e333
Contents lists available at SciVerse ScienceDirect
Archives of Gerontology and Geriatrics
journa l homepage: www.e lsev ier .com/ locate /archger
Incident preclinical mobility disability (PCMD) increases future risk of newdifficulty walking and reduction in walking activity
Carlos O. Weiss a,1,*, Jennifer L. Wolff a,b, Brian Egleston c, Christopher L. Seplaki d, Linda P. Fried e
a Johns Hopkins School of Medicine, 5200 Eastern Avenue, Baltimore, MD 21224-2734, USAb Johns Hopkins Bloomberg School of Public Health, 624 N. Broadway, Baltimore, MD 21205-1996, USAc Fox Chase Cancer Center, 333 Cottman Avenue, Philadelphia, PA 19111-2497, USAd University of Rochester Medical Center, 601 Elmwood Avenue, Box 644, Rochester, NY 14642, USAe Mailman School of Public Health, Columbia University, 722 W. 168th St., New York, NY 10032, USA
A R T I C L E I N F O
Article history:
Received 15 June 2011
Received in revised form 1 August 2011
Accepted 29 August 2011
Available online 23 September 2011
Keywords:
Disability
Geriatrics
Epidemiology
Prevention
Physical activity
A B S T R A C T
Purpose: This study examines whether and how report of a change in walking behavior, incident PCMD,
predicts subsequent reduction in walking activity. Materials and methods: Data are from a prospective
study of 436 community-dwelling women age 70–79 years. Outcome measures include subjective and
objective measures of walking ability at 3 years. Principal results: Incident PCMD is associated with the
loss of walking abilities at 3-years, regardless of baseline physical impairment. Compared to women
without, women with incident PCMD at 1.5 years after baseline were 2.7 (95%CI 1.4–7.2) times more
likely to report that they no longer walk outdoors at least 8 blocks and 4.9 (1.9–13.1) times more likely to
report new difficulty walking. Incident PCMD was also associated with declines in objective outcomes.
Incident PCMD is an independent marker of subsequent decreased walking activity. Major conclusions:
Incident PCMD appears to be a target for programs to prevent declines in walking activity in older adults.
� 2011 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
In the U.S. roughly one-half of older adults (age 65 years andolder) report at least some difficulty walking, which includesdifficulty walking, needing help from another person to walk, oravoiding walking (Shumway-Cook et al., 2005). Difficulty with thisessential task is associated with an increased risk of more severephysical disability, institutionalization and death (Fried andGuralnik, 1997; Clark et al., 1998; Harris et al., 1989). The keysto improving the primary prevention of loss of walking activity inan aging society include understanding who is at risk of loss ofwalking ability and how that risk can be modified (Whiteneck,2006; Weiss et al., 2007).
Early changes in physical task performance are sometimes acompensatory strategy: a way of doing a task in a way that is not‘‘usual’’ and can take the forms of behavioral adaptations, the use ofassistive devices, or the receipt of human assistance (Agree, 1999;Hoenig et al., 2003). Compensatory strategies are responses to taskdemand and can have opposing significance: on the one hand they
* Corresponding author at: Mason F. Lord Center Tower, 5200 Eastern Avenue,
Baltimore, MD 21224-2734, USA. Tel.: +1 410 550 8669; fax: +1 410 550 8701.
E-mail address: [email protected] (C.O. Weiss).1 Present address: Department of Family Medicine, Michigan State University,
300 Lafayette Avenue SE Suite 3400, Grand Rapids, MI 49503, USA.
0167-4943/$ – see front matter � 2011 Elsevier Ireland Ltd. All rights reserved.
doi:10.1016/j.archger.2011.08.018
may signify taking wise precautions or striving for independence(Ward-Griffin et al., 2004); on the other they may indicateunderlying risk of poor outcomes (Weiss et al., 2007). PCMD is acompensatory strategy in the form of behavioral adaptation.
Existing work shows that prevalent PCMD is a marker ofvulnerability to the challenges of task performance. Specifically,prevalent PCMD can identify older adults who have worse taskperformance (Fried et al., 2001) and those who report walkingfewer steps per day (Petrella and Cress, 2004), compared to thosewith no reported PCMD. In addition, longitudinal studies demon-strate that prevalent PCMD predicts self-reported incidentmobility difficulty (Fried et al., 2000; Wolinsky et al., 2005).However, the use of prevalent PCMD as a risk factor is susceptibleto reverse causation bias. It remains to be determined whetherPCMD is in the causal pathway of loss of walking activity.
Our first study aim is to describe the types of incident PCMDstrategies used by relatively high-functioning older women. Thesecond aim is to estimate whether incident PCMD implementedafter the onset of physical impairment is associated with increasedor decreased self-reported mobility difficulty or objective changesin walking ability. We also posited that the effect associated withincident PCMD may vary according to the presence of physicalimpairment. We achieve our aims by employing methodsspecifically designed to address the effects of a risk factor inobservational data. Our study extends prior work by (a) focusingon incident PCMD among people with and without physical

C.O. Weiss et al. / Archives of Gerontology and Geriatrics 54 (2012) e329–e333e330
impairments; (b) examining both subject self-reports of difficultyand objective, performance-based outcome measures; and (c)extending the length of follow-up to 3 years.
2. Materials and methods
2.1. Data source
The Women’s Health and Aging Study II (WHAS II) is alongitudinal cohort study designed to ascertain the causes andcourse of disability in old age. The recruitment of 436 women hasbeen described previously (Fried et al., 2000). Eligibility wasdefined on the basis of self-reported difficulty (in �1 out of 4physical domains), Mini-Mental State Examination (MMSE)(Folstein et al., 1975) score �24 and ability to participate in abaseline clinic examination. Participants were recruited from asample representing the higher functioning two-thirds of womenage 70–79 in eastern Baltimore City and Baltimore County,Maryland and were enrolled in 1994 and 1995. Data from baseline,1.5- and 3-year follow-ups were used for this study. The JohnsHopkins Medicine Institutional Review Board approved the studyand informed consent was obtained from all participants.
2.2. Main predictors
The main variable of interest, reported PCMD, was obtained aspart of a series of task-specific questions about changing thefrequency or method of performing daily activities: ‘‘Have youchanged the way you walk 1/2 mile (about 5–6 city blocks), or howoften you do this, due to a health or physical condition?’’ Responseoptions were no, yes, no longer do the task due to difficulty, or, coulddo the task but do not for non-health reasons. In addition responsesof do not know and refusals were recorded. People who respondedaffirmatively were then asked a series of more specific questions. Inorder to avoid reverse bias by PCMD that preceded impairment,people who reported PCMD at baseline (n = 131) were excludedfrom longitudinal analyses. WHAS II collected both self-report dataand measured performance on standardized objective tests ofcorresponding physical function, previously described in detail(Fried et al., 2001). Physical impairment was captured usingmeasured knee extensor strength (using a handheld dynamometer)and a timed test of balance on one leg, taking the best attempt fromeither leg. We define participants as having a physical impairmentwho are in the lower half of performance in at least one of thesemeasures, i.e. <0.31 kg knee strength or <8.0 s standing balance.
2.3. Outcomes
The main outcomes were two self-reported measures of mobilityfunctioning. Distance walked was asked at each round using thequestion ‘‘Think about the walking you do outside your home.During the last week, about how many city blocks or their equivalentdid you walk?’’ The number was recorded, with 0 in place of <1block. The cutoff of 8 blocks per week was chosen because it has beenshown previously to discriminate between those who do and do notmaintain walking speed or walking activity (Simonsick et al., 2005).Difficulty walking was based on self-reported difficulty walking 1/2mile ‘‘due to health or a physical condition,’’ a question which hasbeen shown to precede and predict mobility dependence (Gill et al.,1998). Response options were no, yes, no longer do the task due todifficulty, or, could do the task but do not for non-health reasons. Inaddition responses of do not know and refusals were recorded. Twosecondary (confirmatory) outcomes were objective performancemeasures that predict concurrent and future mobility difficulty,institutionalization and death in older adults (Guralnik et al., 2000):self-selected walking speed (SSWS) was measured over a 4-m course
from a standing start, corrected for height by dividing by kneeheight; and a Summary Performance Score (SPS) (Onder et al., 2002)of combined timed performance on three standardized tests of lowerextremity function (balance, chair stands and SSWS), which rangesbetween 0 and 12. Both were studied as continuous outcomes. SSWShas been found to have a test-repeat reliability ICC (within-subject)of 0.96 (Weiss et al., 2008) and SPS an ICC of 0.81 (Mangione et al.,2010) or Cronbach’s alpha of 0.76 (Guralnik et al., 1994). Because weare interested in the risks associated with onset of PCMD, peoplewith PCMD or outcome at baseline were excluded. For this reasonand missing data, the numbers of people analyzed in each outcomemodel were 236 for blocks walked, 255 for walking difficulty, and262 for SSWS and SPS.
2.4. Covariates
Covariates considered due to a priori knowledge of theirassociation with physical difficulty included personal factors: race(African American, White), age (75+ versus 70–74 years), educa-tion (years), living alone, financial strain (having not enough or justenough to make ends meet at the end of each month); healthconditions: Geriatric Depression Scale (Yesavage et al., 1982) score(GDS, 0–30), body mass index (BMI, kg/m2), comorbidity (countamong 14 chronic diseases), and MMSE score; and environment:having 2 or more steps to get into the home.
2.5. Statistical analysis
To describe the population, baseline proportions and meanvalues were calculated for personal, health and environmentalcharacteristics. PCMD strategies were examined across study wavesand, because they did not differ substantially, frequencies at baselineare reported. T-tests assuming unequal variances and x2 tests wereused to test differences for continuous and categorical variables. Weexamined binary and continuous outcomes using a marginalstructural model approach (Robins et al., 2000), where adjustedprobability risk ratios (RRs) for binary outcomes and adjustedchanges in mean for continuous outcomes are estimated usinglogistic regression and generalized linear models, respectively.Robust variance estimates were used throughout. Marginalstructural models were designed to estimate associations fromobservational data in cases where the exposure may be simulta-neously a confounder and intermediate variable. The RR or adjustedchange in mean was estimated with those without PCMD, not theoverall population, as the reference group. A standardized mortalityratio weight (Sato and Matsuyama, 2003; Kurth et al., 2006) based onpropensity score methods (Rosenbaum and Rubin, 1984; Brookhartet al., 2006) was employed. An advantage of these weights was animproved ability to identify and minimize residual selection bias inmeasured variables. Appropriateness of propensity scores wasconfirmed by examining the density function of propensity scoresacross PCMD strata for sufficient overlap and by confirminggraphically that there was a balance of confounders between PCMDstrata within propensity score quartiles. To examine the RR for thesubgroup with no impairment, an adaptation of Rubin’s model(Egleston et al., 2007) was employed and bootstrapping with 1000replications was used to create robust standard errors.
The association between PCMD, baseline gait speed andoutcomes was examined by graphing the adjusted probability ofreporting PCMD for impairment strata across a continuous range ofSSWS. Potential non-linearity was tested with quadratic and splineterms, and collinearity was assessed by examining varianceinflation factors. Hosmer–Lemeshow x2 goodness-of-fit statisticstested the fit of final models with data.
Two analyses were carried out to explore the possibility ofbiases. First, to assess whether the competing outcome of death
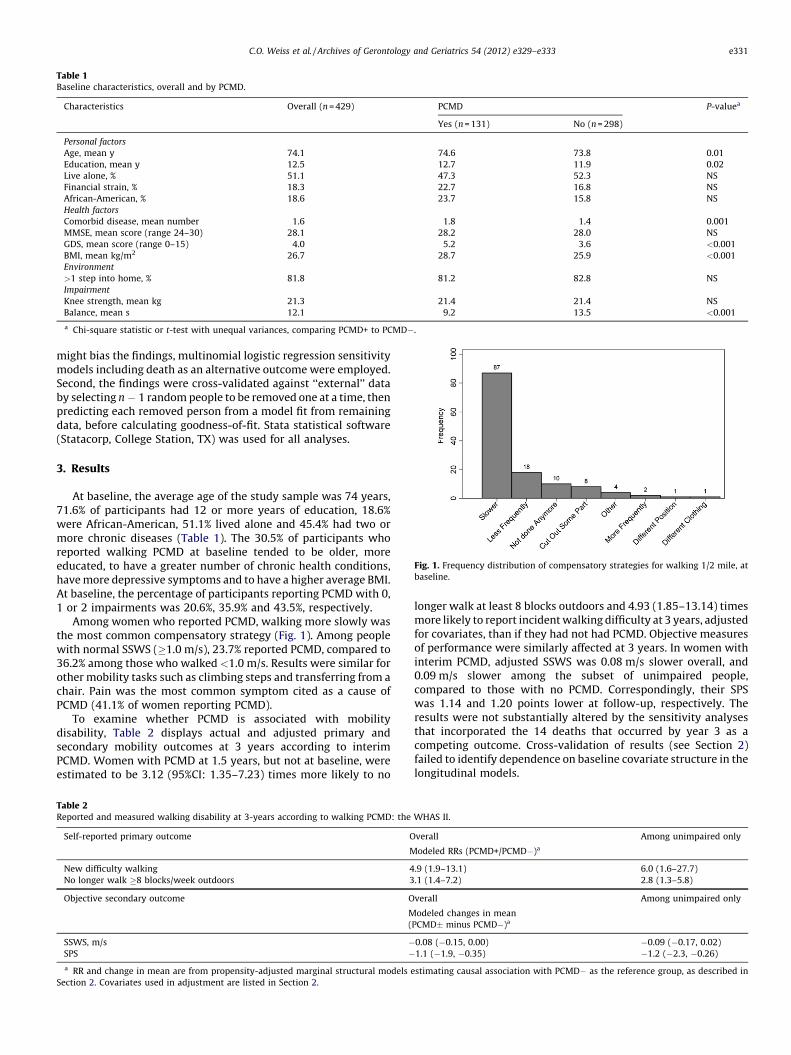
Table 1Baseline characteristics, overall and by PCMD.
Characteristics Overall (n = 429) PCMD P-valuea
Yes (n = 131) No (n = 298)
Personal factors
Age, mean y 74.1 74.6 73.8 0.01
Education, mean y 12.5 12.7 11.9 0.02
Live alone, % 51.1 47.3 52.3 NS
Financial strain, % 18.3 22.7 16.8 NS
African-American, % 18.6 23.7 15.8 NS
Health factors
Comorbid disease, mean number 1.6 1.8 1.4 0.001
MMSE, mean score (range 24–30) 28.1 28.2 28.0 NS
GDS, mean score (range 0–15) 4.0 5.2 3.6 <0.001
BMI, mean kg/m2 26.7 28.7 25.9 <0.001
Environment
>1 step into home, % 81.8 81.2 82.8 NS
Impairment
Knee strength, mean kg 21.3 21.4 21.4 NS
Balance, mean s 12.1 9.2 13.5 <0.001
a Chi-square statistic or t-test with unequal variances, comparing PCMD+ to PCMD�.[(Fig._1)TD$FIG]
Fig. 1. Frequency distribution of compensatory strategies for walking 1/2 mile, at
baseline.
C.O. Weiss et al. / Archives of Gerontology and Geriatrics 54 (2012) e329–e333 e331
might bias the findings, multinomial logistic regression sensitivitymodels including death as an alternative outcome were employed.Second, the findings were cross-validated against ‘‘external’’ databy selecting n � 1 random people to be removed one at a time, thenpredicting each removed person from a model fit from remainingdata, before calculating goodness-of-fit. Stata statistical software(Statacorp, College Station, TX) was used for all analyses.
3. Results
At baseline, the average age of the study sample was 74 years,71.6% of participants had 12 or more years of education, 18.6%were African-American, 51.1% lived alone and 45.4% had two ormore chronic diseases (Table 1). The 30.5% of participants whoreported walking PCMD at baseline tended to be older, moreeducated, to have a greater number of chronic health conditions,have more depressive symptoms and to have a higher average BMI.At baseline, the percentage of participants reporting PCMD with 0,1 or 2 impairments was 20.6%, 35.9% and 43.5%, respectively.
Among women who reported PCMD, walking more slowly wasthe most common compensatory strategy (Fig. 1). Among peoplewith normal SSWS (�1.0 m/s), 23.7% reported PCMD, compared to36.2% among those who walked <1.0 m/s. Results were similar forother mobility tasks such as climbing steps and transferring from achair. Pain was the most common symptom cited as a cause ofPCMD (41.1% of women reporting PCMD).
To examine whether PCMD is associated with mobilitydisability, Table 2 displays actual and adjusted primary andsecondary mobility outcomes at 3 years according to interimPCMD. Women with PCMD at 1.5 years, but not at baseline, wereestimated to be 3.12 (95%CI: 1.35–7.23) times more likely to no
Table 2Reported and measured walking disability at 3-years according to walking PCMD: the
Self-reported primary outcome O
M
New difficulty walking 4
No longer walk �8 blocks/week outdoors 3
Objective secondary outcome O
M
(
SSWS, m/s �SPS �a RR and change in mean are from propensity-adjusted marginal structural models e
Section 2. Covariates used in adjustment are listed in Section 2.
longer walk at least 8 blocks outdoors and 4.93 (1.85–13.14) timesmore likely to report incident walking difficulty at 3 years, adjustedfor covariates, than if they had not had PCMD. Objective measuresof performance were similarly affected at 3 years. In women withinterim PCMD, adjusted SSWS was 0.08 m/s slower overall, and0.09 m/s slower among the subset of unimpaired people,compared to those with no PCMD. Correspondingly, their SPSwas 1.14 and 1.20 points lower at follow-up, respectively. Theresults were not substantially altered by the sensitivity analysesthat incorporated the 14 deaths that occurred by year 3 as acompeting outcome. Cross-validation of results (see Section 2)failed to identify dependence on baseline covariate structure in thelongitudinal models.
WHAS II.
verall Among unimpaired only
odeled RRs (PCMD+/PCMD�)a
.9 (1.9–13.1) 6.0 (1.6–27.7)
.1 (1.4–7.2) 2.8 (1.3–5.8)
verall Among unimpaired only
odeled changes in mean
PCMD� minus PCMD�)a
0.08 (�0.15, 0.00) �0.09 (�0.17, 0.02)
1.1 (�1.9, �0.35) �1.2 (�2.3, �0.26)
stimating causal association with PCMD� as the reference group, as described in
[(Fig._2)TD$FIG]
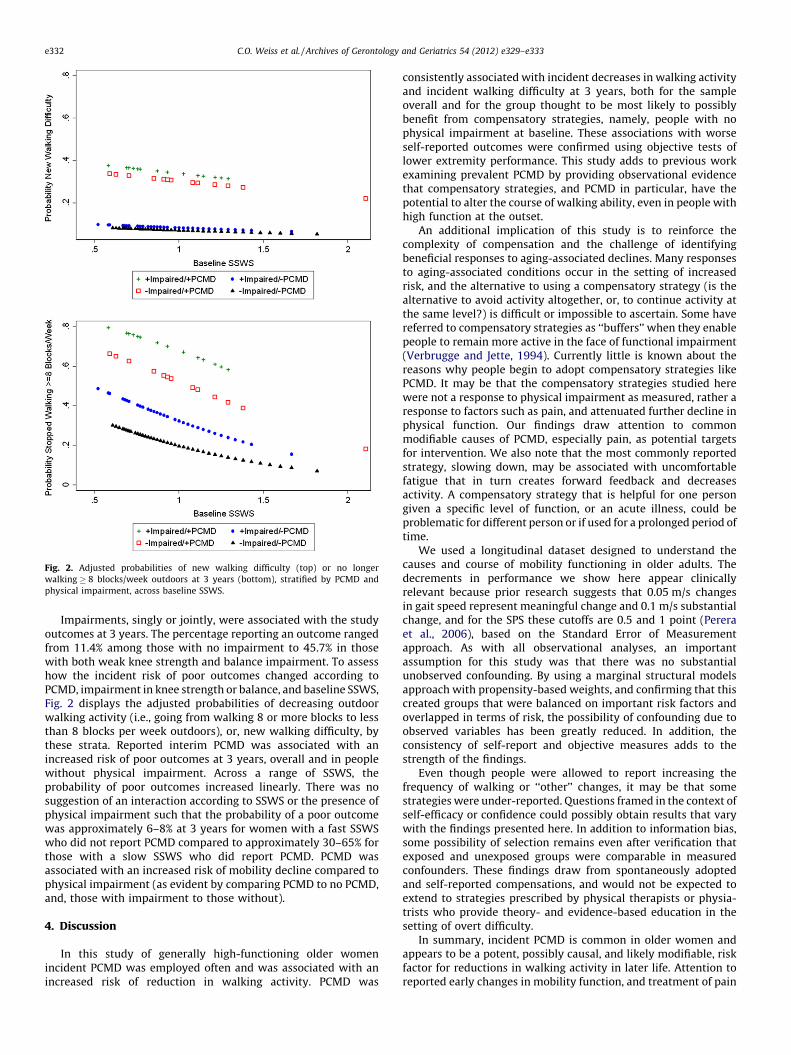
Fig. 2. Adjusted probabilities of new walking difficulty (top) or no longer
walking � 8 blocks/week outdoors at 3 years (bottom), stratified by PCMD and
physical impairment, across baseline SSWS.
C.O. Weiss et al. / Archives of Gerontology and Geriatrics 54 (2012) e329–e333e332
Impairments, singly or jointly, were associated with the studyoutcomes at 3 years. The percentage reporting an outcome rangedfrom 11.4% among those with no impairment to 45.7% in thosewith both weak knee strength and balance impairment. To assesshow the incident risk of poor outcomes changed according toPCMD, impairment in knee strength or balance, and baseline SSWS,Fig. 2 displays the adjusted probabilities of decreasing outdoorwalking activity (i.e., going from walking 8 or more blocks to lessthan 8 blocks per week outdoors), or, new walking difficulty, bythese strata. Reported interim PCMD was associated with anincreased risk of poor outcomes at 3 years, overall and in peoplewithout physical impairment. Across a range of SSWS, theprobability of poor outcomes increased linearly. There was nosuggestion of an interaction according to SSWS or the presence ofphysical impairment such that the probability of a poor outcomewas approximately 6–8% at 3 years for women with a fast SSWSwho did not report PCMD compared to approximately 30–65% forthose with a slow SSWS who did report PCMD. PCMD wasassociated with an increased risk of mobility decline compared tophysical impairment (as evident by comparing PCMD to no PCMD,and, those with impairment to those without).
4. Discussion
In this study of generally high-functioning older womenincident PCMD was employed often and was associated with anincreased risk of reduction in walking activity. PCMD was
consistently associated with incident decreases in walking activityand incident walking difficulty at 3 years, both for the sampleoverall and for the group thought to be most likely to possiblybenefit from compensatory strategies, namely, people with nophysical impairment at baseline. These associations with worseself-reported outcomes were confirmed using objective tests oflower extremity performance. This study adds to previous workexamining prevalent PCMD by providing observational evidencethat compensatory strategies, and PCMD in particular, have thepotential to alter the course of walking ability, even in people withhigh function at the outset.
An additional implication of this study is to reinforce thecomplexity of compensation and the challenge of identifyingbeneficial responses to aging-associated declines. Many responsesto aging-associated conditions occur in the setting of increasedrisk, and the alternative to using a compensatory strategy (is thealternative to avoid activity altogether, or, to continue activity atthe same level?) is difficult or impossible to ascertain. Some havereferred to compensatory strategies as ‘‘buffers’’ when they enablepeople to remain more active in the face of functional impairment(Verbrugge and Jette, 1994). Currently little is known about thereasons why people begin to adopt compensatory strategies likePCMD. It may be that the compensatory strategies studied herewere not a response to physical impairment as measured, rather aresponse to factors such as pain, and attenuated further decline inphysical function. Our findings draw attention to commonmodifiable causes of PCMD, especially pain, as potential targetsfor intervention. We also note that the most commonly reportedstrategy, slowing down, may be associated with uncomfortablefatigue that in turn creates forward feedback and decreasesactivity. A compensatory strategy that is helpful for one persongiven a specific level of function, or an acute illness, could beproblematic for different person or if used for a prolonged period oftime.
We used a longitudinal dataset designed to understand thecauses and course of mobility functioning in older adults. Thedecrements in performance we show here appear clinicallyrelevant because prior research suggests that 0.05 m/s changesin gait speed represent meaningful change and 0.1 m/s substantialchange, and for the SPS these cutoffs are 0.5 and 1 point (Pereraet al., 2006), based on the Standard Error of Measurementapproach. As with all observational analyses, an importantassumption for this study was that there was no substantialunobserved confounding. By using a marginal structural modelsapproach with propensity-based weights, and confirming that thiscreated groups that were balanced on important risk factors andoverlapped in terms of risk, the possibility of confounding due toobserved variables has been greatly reduced. In addition, theconsistency of self-report and objective measures adds to thestrength of the findings.
Even though people were allowed to report increasing thefrequency of walking or ‘‘other’’ changes, it may be that somestrategies were under-reported. Questions framed in the context ofself-efficacy or confidence could possibly obtain results that varywith the findings presented here. In addition to information bias,some possibility of selection remains even after verification thatexposed and unexposed groups were comparable in measuredconfounders. These findings draw from spontaneously adoptedand self-reported compensations, and would not be expected toextend to strategies prescribed by physical therapists or physia-trists who provide theory- and evidence-based education in thesetting of overt difficulty.
In summary, incident PCMD is common in older women andappears to be a potent, possibly causal, and likely modifiable, riskfactor for reductions in walking activity in later life. Attention toreported early changes in mobility function, and treatment of pain

C.O. Weiss et al. / Archives of Gerontology and Geriatrics 54 (2012) e329–e333 e333
and other causes of slowing down appear warranted as part ofprograms to maximize the likelihood of preventing physicalmobility disability, pending confirmation in randomized trials.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Acknowledgements
The original study for this research was funded by NIAN01AG12112 and supported by NIH NCRR M01-RR00052. Dr.Weiss was funded by the Robert Wood Johnson Harold AmosMedical Faculty Development Program. Dr. Seplaki was supportedby Mentored Research Scientist Development Award numberK01AG031332 from the National Institute on Aging. The content issolely the responsibility of the authors and does not necessarilyrepresent the official views of the National Institute on Aging or theNational Institutes of Health. Dr. Fried was supported by NIA R37-AG19905. An abstract of preliminary work related to some portionsof this study was presented at the American Geriatrics SocietyAnnual Scientific Meeting in 2005. The study sponsors had noinvolvement in the study design; the collection, analysis andinterpretation of data; the writing of the manuscript; or thedecision to submit the manuscript for publication.
References
Agree, E.M., 1999. The influence of personal care and assistive devices on themeasurement of disability. Soc. Sci. Med. 48, 427–443.
Brookhart, M.A., Schneeweiss, S., Rothman, K.J., Glynn, R.J., Avorn, J., Sturmer, T.,2006. Variable selection for propensity score models. Am. J. Epidemiol. 163,1149–1156.
Clark, D.O., Stump, T.E., Hui, S.L., Wolinsky, F.D., 1998. Predictors of mobility andbasic ADL difficulty among adults aged 70 years and older. J. Aging Health 10,422–440.
Egleston, B.L., Scharfstein, D.O., Freeman, E.E., West, S.K., 2007. Causal inference fornon-mortality outcomes in the presence of death. Biostatistics 8, 526–545.
Folstein, M.F., Folstein, S.E., McHugh, P.R., 1975. Mini-mental state. A practicalmethod for grading the cognitive state of patients for the clinician. J. Psychiatr.Res. 12, 189–198.
Fried, L.P., Guralnik, J.M., 1997. Disability in older adults: evidence regardingsignificance, etiology, and risk. J. Am. Geriatr. Soc. 45, 92–100.
Fried, L.P., Bandeen-Roche, K., Chaves, P.H., Johnson, B.A., 2000. Preclinical mobilitydisability predicts incident mobility disability in older women. J. Gerontol. A:Biol. Sci. Med. Sci. 55, M43–M52.
Fried, L.P., Young, Y., Rubin, G., Bandeen-Roche, K., 2001. Self-reported preclinicaldisability identifies older women with early declines in performance and earlydisease. J. Clin. Epidemiol. 54, 889–901.
Gill, T.M., Robison, J.T., Tinetti, M.E., 1998. Difficulty and dependence: two compo-nents of the disability continuum among community-living older persons. Ann.Intern. Med. 128, 96–101.
Guralnik, J.M., Simonsick, E.M., Ferrucci, L., Glynn, R.J., Berkman, L.F., Blazer, D.G.,Scherr, P.A., Wallace, R.B., 1994. A short physical performance battery assessing
lower extremity function: association with self-reported disability and predic-tion of mortality and nursing home admission. J. Gerontol. 49, M85–M94.
Guralnik, J.M., Ferrucci, L., Pieper, C.F., Leveille, S.G., Markides, K.S., Ostir, G.V.,Studenski, S., Berkman, L.F., Wallace, R.B., 2000. Lower extremity function andsubsequent disability: consistency across studies, predictive models, and valueof gait speed alone compared with the short physical performance battery. J.Gerontol. A: Biol. Sci. Med. Sci. 55, M221–M231.
Harris, T., Kovar, M.G., Suzman, R., Kleinman, J.C., Feldman, J.J., 1989. Longitu-dinal study of physical ability in the oldest-old. Am. J. Public Health 79, 698–702.
Hoenig, H., Taylor Jr., D.H., Sloan, F.A., 2003. Does assistive technology substitute forpersonal assistance among the disabled elderly? Am. J. Public Health 93, 330–337.
Kurth, T., Walker, A.M., Glynn, R.J., Chan, K.A., Gaziano, J.M., Berger, K., Robins, J.M.,2006. Results of multivariable logistic regression, propensity matching, pro-pensity adjustment, and propensity-based weighting under conditions of non-uniform effect. Am. J. Epidemiol. 163, 262–270.
Mangione, K.K., Craik, R.L., McCormick, A.A., Blevins, H.L., White, M.B., Sullivan-Marx, E.M., Tomlinson, J.D., 2010. Detectable changes in physical performancemeasures in elderly African Americans. Phys. Ther. 90, 921–927.
Onder, G., Penninx, B.W., Lapuerta, P., Fried, L.P., Ostir, G.V., Guralnik, J.M., Pahor, M.,2002. Change in physical performance over time in older women: the Women’sHealth and Aging Study. J. Gerontol. A: Biol. Sci. Med. Sci. 57, M289–M293.
Perera, S., Mody, S.H., Woodman, R.C., Studenski, S.A., 2006. Meaningful change andresponsiveness in common physical performance measures in older adults. J.Am. Geriatr. Soc. 54, 743–749.
Petrella, J.K., Cress, M.E., 2004. Daily ambulation activity and task performance incommunity-dwelling older adults aged 63–71 years with preclinical disability.J. Gerontol. A: Biol. Sci. Med. Sci. 59, 264–267.
Robins, J.M., Hernan, M.A., Brumback, B., 2000. Marginal structural models andcausal inference in epidemiology. Epidemiology 11, 550–560.
Rosenbaum, P.R., Rubin, D.B., 1984. Reducing bias in observational studies usingsubclassification on the propensity score. J. Am. Stat. Assoc. 79, 516–524.
Sato, T., Matsuyama, Y., 2003. Marginal structural models as a tool for standardiza-tion. Epidemiology 14, 680–686.
Shumway-Cook, A., Ciol, M.A., Yorkston, K.M., Hoffman, J.M., Chan, L., 2005. Mobilitylimitations in the Medicare population: prevalence and sociodemographic andclinical correlates. J. Am. Geriatr. Soc. 53, 1217–1221.
Simonsick, E.M., Guralnik, J.M., Volpato, S., Balfour, J., Fried, L.P., 2005. Just get outthe door! Importance of walking outside the home for maintaining mobility:findings from the women‘s health and aging study J. Am. Geriatr. Soc. 53, 198–203.
Verbrugge, L.M., Jette, A.M., 1994. The disablement process. Soc. Sci. Med. 38, 1–14.
Ward-Griffin, C., Hobson, S., Melles, P., Kloseck, M., Vandervoort, A., Crilly, R., 2004.Falls and fear of falling among community-dwelling seniors: the dynamictension between exercising precaution and striving for independence. Can. J.Aging. 23, 307–318.
Weiss, C.O., Hoenig, H.M., Fried, L.P., 2007. Compensatory strategies used by olderadults facing mobility disability. Arch. Phys. Med. Rehabil. 88, 1217–1220.
Weiss, C.O., Seplaki, C.L., Wolff, J.L., Kasper, J.D., Agree, E.M., 2008. Self-selectedwalking speed was consistent when recorded while using a cane. J. Clin.Epidemiol. 61, 622–627.
Whiteneck, G., 2006. Conceptual Models of Disability: Past, Present, and Future. In:Field, M.J., Jette, A.M., Martin, L. (Eds.), Workshop on Disability in America. ANew Look. National Academies Press, Washington, D.C, pp. 50–66.
Wolinsky, F.D., Miller, D.K., Andresen, E.M., Malmstrom, T.K., Miller, J.P., 2005.Further evidence for the importance of subclinical functional limitation andsubclinical disability assessment in gerontology and geriatrics. J. Gerontol. B:Psychol. Sci. Soc. Sci. 60, S146–S151.
Yesavage, J.A., Brink, T.L., Rose, T.L., Lum, O., Huang, V., Adey, M., Leirer, V.O., 1982.Development and validation of a geriatric depression screening scale: a pre-liminary report. J. Psychiatr. Res. 17, 37–49.