in vitro cytotoxicity of igg antibodies on vascular endothelial cells from patients with endemic...
TRANSCRIPT
Atherosclerosis 137 (1998) 141–147
In vitro cytotoxicity of IgG antibodies on vascular endothelial cellsfrom patients with endemic peripheral vascular disease in Taiwan
Hsin-Su Yu a,*, Kee-Lung Chang b, Ying-Hsien Kao a, Chia-Li Yu c, Gwo-Shing Chen a,Chung-Hsing Chang a, Kan-Tang Fang d
a Department of Dermatology, Kaohsiung Medical College, 100 Shih Chuan 1st Road, Kaohsiung 80708, Taiwanb Department of Biochemistry, Kaohsiung Medical College, 100 Shih Chuan 1st Road, Kaohsiung 80708, Taiwan
c Department of Medicine, Veterans General Hospital Taipei, National Yang-Ming Uni6ersity School of Medicine, 201, Sec 2, Shih-Pai Road,Peitou, Taipei 11217, Taiwan
d Department of Dermatology, Kaohsiung Municipal Hospital, 138 Kai-Hsuan 2nd Road, Kaohsiung 80242, Taiwan
Received 7 May 1997; received in revised form 23 September 1997; accepted 5 November 1997
Abstract
A unique peripheral vascular disorder called ‘blackfoot disease’ is endemic in a limited area on the south-west coast of Taiwan.Clinically, the signs and symptoms of blackfoot disease (BFD) are similar to those of arteriosclerosis and Buerger’s disease. Adestruction of vascular endothelial cells (ECs) takes place at an early stage in the affected limbs. Currently, the cause of BFD isbelieved to be artesian drinking water containing a high concentration of arsenic and/or humic substances, although themechanism of EC destruction is not entirely understood. The purpose of the present study was to examine the factors related toEC damage in BFD. Thus, we investigated the effects of purified IgG collected from patients with BFD (BFD-IgG) and fromnormal controls (N-IgG) on cultured EC. We found that: (1) EC binding activity of BFD-IgG was significantly higher than thatof N-IgG; (2) BFD-IgG, at a concentration higher than 100 mg/ml but not N-IgG, induced concentration-dependent ECcytotoxicity; (3) BFD-IgG at a concentration of 100 mg/ml stimulated neither the release of von Willebrand factor nor theexpression of intercellular adhesion molecule-1 by EC. Fluorescent video microscopic examination revealed an increase intranscapillary and interstitial diffusion of nailfold capillary loops in clinically normal fingers of BFD patients. These findingsstrongly suggested that immunological mechanisms played a significant role in the pathogenesis of BFD. We propose that onlypersons who produce the IgG anti-endothelial cell antibody are potential victims of BFD. © 1998 Elsevier Science Ireland Ltd.All rights reserved.
Keywords: IgG antibody; Endothelium; Cytotoxicity; Blackfoot disease
1. Introduction
A peripheral vascular disorder named ‘blackfoot dis-ease’, endemic in certain limited regions on the south-west coast of Taiwan, results in gangrene of theextremities, especially of the feet [3]. Clinically, thesigns and symptoms of blackfoot disease (BFD) aresimilar to, though much more severe than those of
arteriosclerosis and Buerger’s disease [17]. Pathologicalstudy has revealed that 30% of BFD patients hadfeatures compatible with thromboangiitis obliteransand 70% showed clinical characteristics of arteriosclero-sis obliterans [2]. In both groups, a destruction ofvascular endothelial cells occurs in affected limbs at anearly stage of the disease [13,14]. Recent reports re-vealed that a development of impairment of cutaneousmicrocirculation was found in clinically normal skin ofboth BFD patients and inhabitants in the endemic area[28,29]. All these evidences suggest that vascular en-
* Corresponding author. Tel.: +886 7 3208214; fax: +886 73216580; e-mail: [email protected]
0021-9150/98/$19.00 © 1998 Elsevier Science Ireland Ltd. All rights reserved.PII S 0 021 -9150 (97 )00272 -4
H.-S. Yu et al. / Atherosclerosis 137 (1998) 141–147142
dothelial cells are target cells in the pathogenesis ofBFD.
BFD has been linked to the high concentrations ofarsenic [1,3] and humic substances [12] in drinkingwater of endemic areas. The overall prevalence rate ofBFD in 1968 was 8.9 per thousand people [3]. However,toxic substances in well water cannot be the sole causeof BFD because the incidence of BFD is relatively loweven in an endemic area. The purpose of this study wasto examine the factors related to endothelial cell dam-age in BFD, as compared with normal controls. Wecollected IgG from both BFD patients and controls andfound that only patients IgG caused damage to humanvascular endothelial cells in vitro. Furthermore, resultsof fluorescence video microscopy revealed the impair-ment of transcapillary diffusion and interstitial diffu-sion of nailfold capillaries in clinically normal fingers ofBFD patients.
2. Materials and methods
2.1. Selection of patients
A total of 12 patients with BFD were selected fromthe endemic area. At the time of assessment, all patientswere in the erythematous stage, i.e. an early stage, andfour patients had previously suffered from ulcerationand gangrene. For comparison, an equal number ofage- and sex-matched healthy volunteers served as con-trols for the present study. None of the studied subjectshad hypertension or diabetes mellitus, nor received anytreatment before participating in the study. Laboratorystudies in patients with BFD showed a complete bloodcell count, serum electrolyte concentrations, serumblood chemistry findings and urinalysis results to bewithin normal limits, except for an elevated serum GOTand GPT level in one patient. Quantitative immunolog-ical examinations revealed normal ranges of IgG(1440.2952.7 mg/dl), IgM (112.4937.2 mg/dl), IgA(226.1932.3 mg/dl), IgE (72.7932.3 IU/ml), C3(98.3924.2 mg/dl) and C4 (31.1911.2 mg/dl).
2.2. Purification of IgG from serum of BFD patientsand normal controls
Each serum sample collected from patients and con-trols was individually gel-filtrated at a flow rate of 30ml/h through a 1.5×90 cm column of Sephacryl S-300(Sigma, St. Louis, MO) by phosphate-buffered saline(PBS), pH 7.2. Fraction II (IgG) from the filtrationcolumn was absorbed into protein A–Sepharose 4B(Pharmacia LKB, Uppsala, Sweden). Sepharose-conju-gated IgG was eluted with sodium acetate buffer at pH2.5 and immediately neutralized to pH 7.2 with 1NNaOH. After adequate dialysis against distilled water,
the IgG was lyophilized [18] and the concentration ofpurified IgG was determined with the Bio-Rad proteinassay kit (Bio-Rad, Richmond, CA).
2.3. Vascular endothelial cell culture and itsidentification
Vascular endothelial cells (ECs) isolated from humanumbilical cords were cultured as described by Jaffe etal. [7]. Endothelial cells in culture were identified fromtheir morphologic characteristics and presence of factorVIII-related protein [11]. Staining for factor VIII-re-lated antigen was performed by indirect immu-nofluorescence as previously reported [15]. ECs wereused between the second and fifth passage.
2.4. IgG anti-endothelial cell antibody detection
Endothelial cells were incubated with IgG from pa-tients or controls in various concentrations at 37°C for48 h. Anti-endothelial cell activity of individuallypurified IgG samples was determined by cellular en-zyme-linked immunoabsorbent assay (cELISA) as re-ported [26]. The relative titer of anti-endothelial cellantibody was detected at an optical density of 490 nm.
2.5. Stimulation of EC with IgG from BFD or controls
Endothelial cells were plated on 96-well plates (Nunc,Roskilde, Denmark) at a subconfluent density of 1×104 cells/per well. Into each well, 100 m1 of IgG frompatients (BFD-IgG) or controls (N-IgG) was added invarious concentrations and the mixture was incubatedat 37°C in 5% CO2/95% air for 48 h. Some ECs were setaside for further studies. Cell free supernatants werecollected and stored at −20°C.
2.6. XTT cell proliferation assay
The commercially available ELISA test kit for cellproliferation (Kit II; XTT; Boehringer MannheimGmbH, Mannheim, Germany) was used according tothe manufacturers instruction, for measuring the influ-ence of IgG on endothelial cell proliferation. Ab-sorbance of formazan product was measured at awavelength of 490 nm, with reference wavelength at 690nm.
2.7. Measurement of 6on Willebrand factor releasefrom endothelial cells by ELISA
We used another commercially available ELISA testkit (Diagnostica Stago, Asnieres, France), as recom-mended by the manufacturer, for determining the con-centration of von Willebrand factor (vWF) in a culturesupernatant derived from 1×106 endothelial cells aftera 48 h incubation with BFD-IgG or N-IgG.
H.-S. Yu et al. / Atherosclerosis 137 (1998) 141–147 143
2.8. Immunofluorescence staining of ICAM-1 on ECs
ICAM-1 of ECs was detected by an indirect immu-nofluorescence staining technique. We used mouse anti-human ICAM-1 (Boehringer Mannheim GmbH) andgoat anti-mouse IgG-FITC (KPL, Gaithersburg, MD)as the first and second antibody, respectively. The cellswere analysed by flow cytometry (FACScan, Becktonand Dickinson, San Jose, CA). Mean fluorescence in-tensity was used as a parameter for ICAM-1 expressionon the cell surface.
2.9. Dynamic capillaroscopy with Na-fluorescein
Cutaneous microcirculatory evaluations were per-formed after 30 min of equilibration in a constant roomtemperature of 23–25°C. A fully computerized systemfor dynamic capillaroscopy [8] was used in this study.This included a microscope, television camera, monitorand software to calculate automatically the whole pro-cess of capillary blood cell velocity (CBV) and tran-scapillary diffusion of Na-fluorescein (NaF) throughthe wall of single capillaries [24,30]. Clinically normalleft ring finger nailfold capillary loops were studied witha Leitz Laborlux 12 MES capillary microscopeequipped with a TV camera (Ikegami CTC-2110,Tokyo, Japan). The image was displayed on a TVmonitor. All recordings were stored on video tape andanalyzed by the CapiFlow computerized analysis sys-tem (CapiFlow, Kista, Sweden). For dynamic capil-laroscopy with NaF, 5 ml of 10% NaF (Alcon,Fortworth, TX) was injected into the right antecubitalvein as a bolus, followed immediately by 10 ml normalsaline. The NaF fluorescein was rendered visible by theuse of capillaroscopy with fluorescence filter set toexcitation at 450–500 nm and barrier at 515 nm. Tran-scapillary and interstitial diffusion patterns and mi-crovascular flow distribution were observed. A linerunning perpendicular to the capillary loop at 33 mmfrom the apex of the capillary loop has been used inthis study. A distance of 6 mm from the external borderof the red blood cell column (arterial limb of thecapillary) is for transcapillary diffusion measurement(site 1), a distance of 40 mm for interstitial diffusiondetermination (site 2) [24]. The determinations wererepeated three times at 30 and 60 s after the firstappearance of NaF in the capillary selected for study.Fluorescent light intensities were expressed in percentof the individual maximal light intensity reached duringthe investigation [9].
2.10. Statistical analysis
Results of measurements made in triplicate werepresented as mean9S.D. The unpaired Student’s t-testwas used to analyze statistical differences between pa-
tients and controls. A difference of PB0.05 was con-sidered statistically significant.
3. Results
3.1. Identification of 6ascular endothelial cells
The typical appearance of endothelial cells in conflu-ent monolayer revealed a hexagonal or cuboid shapeand closely apposed large round nuclei. Following indi-rect immunofluorescence staining of endothelial cellsfor factor VIII associated proteins, fluorescence of agranular pattern localized in cytoplasm, especially inthe perinuclear region.
3.2. Binding acti6ity of purified IgG to endothelial cells
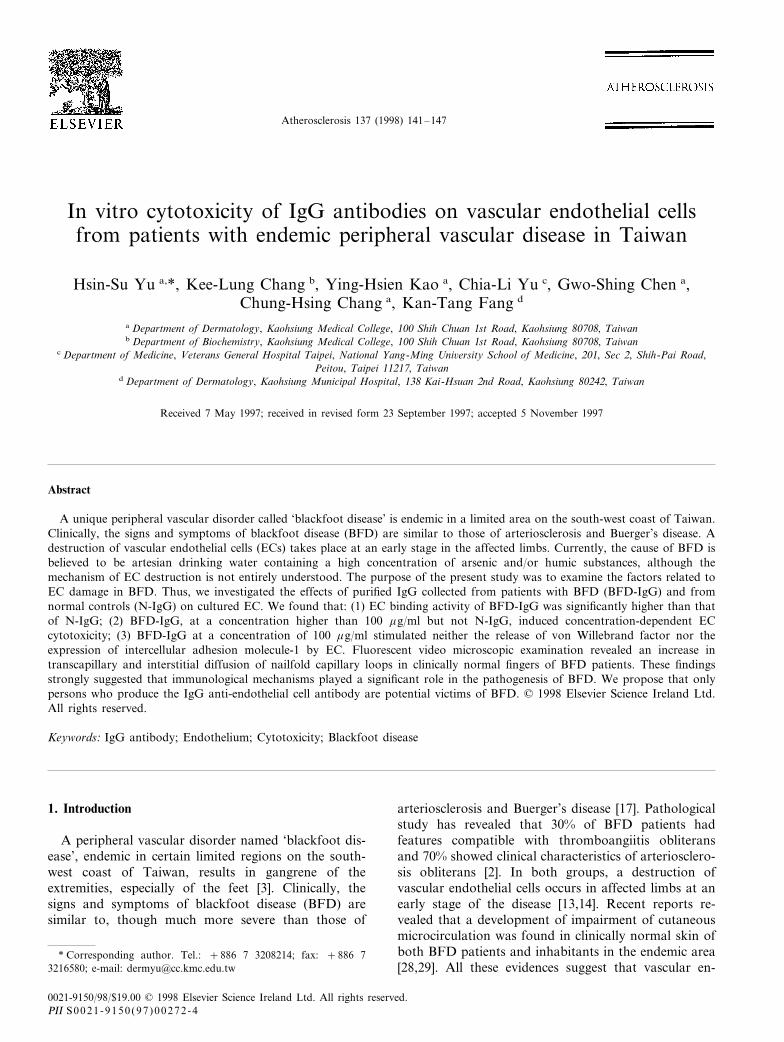
Optical density at 490 nm of cultured EC substrate,as monitored by cELISA, was found to be concentra-tion dependent for IgG in both patients and controls(Fig. 1). The binding activity of BFD patients IgG wasstatistically significantly higher than that of controls(PB0.05).
Fig. 1. Optical density at 490 nm as detected by cellular ELISA in asubstrate of cultured endothelial cells was concentration dependentfor IgG in both blackfoot disease (BFD) and healthy control. En-dothelial cell binding activity of IgG in BFD was significantly higherthan that in normal controls (n=12). * Denotes PB0.05 comparedto controls
H.-S. Yu et al. / Atherosclerosis 137 (1998) 141–147144
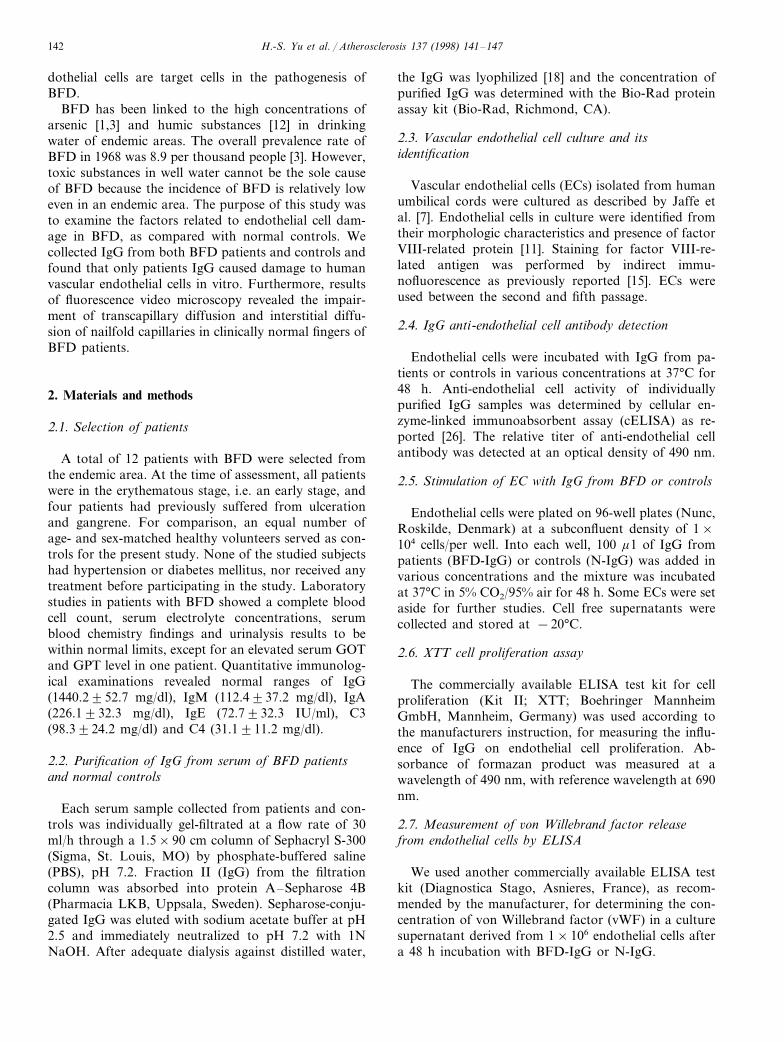
Fig. 2. IgG from patients with blackfoot disease (BFD-IgG) at concentrations higher than 100 mg/ml caused damage to cultured endothelial cells.In contrast, 400 mg/ml IgG from healthy controls (N-IgG) showed no cytotoxicity. (a) 100 mg/ml BFD-IgG, (b) 200 mg/ml BFD-IgG, (c) 400mg/ml BFD-IgG, (d) 400 mg/ml N-IgG.
3.3. IgG damage to endothelial cells
Following 48 h of incubation, morphologic differ-ences between EC exposed to BFD-IgG or N-IgGwere not significant under a concentration of 100 mg/ml (Fig. 2a). At concentrations of 200 or 400 mg/ml,however, BFD-IgG, but not N-IgG, caused destruc-tion of endothelial cells (Fig. 2b, c). The cytotoxicityof BFD-IgG treatment was wholly concentration de-pendent.
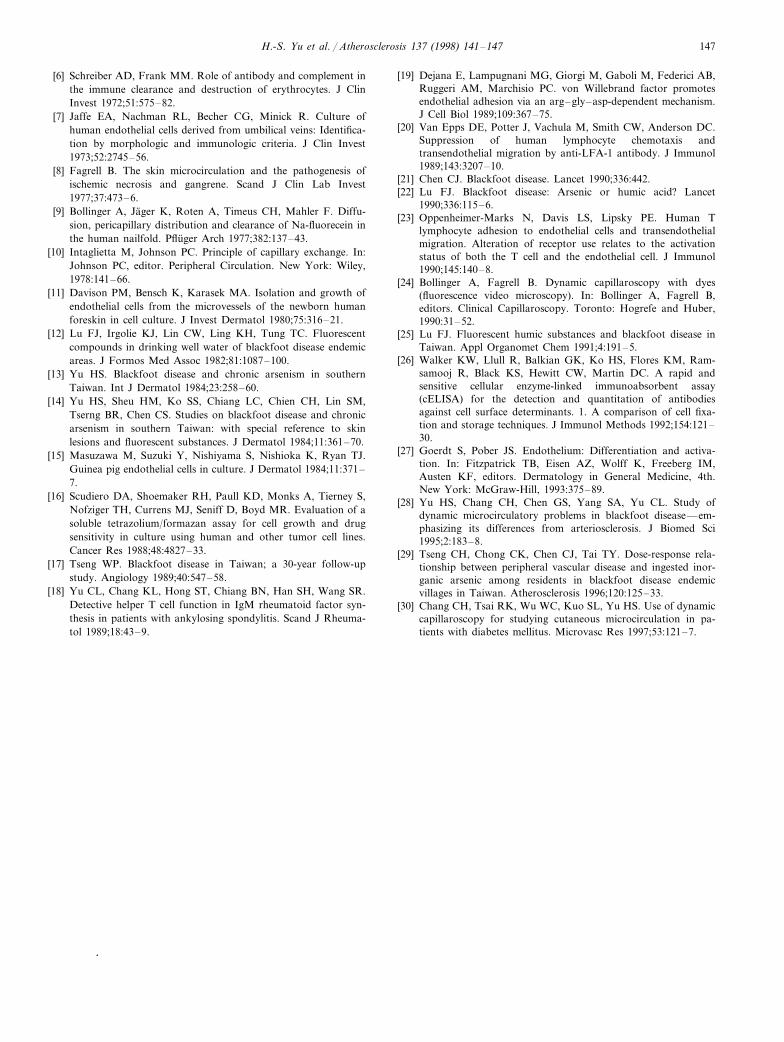
3.4. Cytotoxic BFD-IgG to endothelial cells by XTTcell proliferation assay
As demonstrated in Fig. 3, BFD-IgG treated en-dothelial cells, unlike N-IgG treated cells, displayedsignificant cytotoxic reactions (PB0.05), which wereconcentration dependent. There were no apparent cy-totoxic effects of BFD-IgG at a concentration up toand including 100 mg/ml. However, concentrationshigher than 100 mg/ml clearly caused cytotoxicity. Thesurvival rates of endothelial cells treated at 100, 200and 400 mg/ml concentrations were 86.9191.26,
52.4292.02 and 15.3291.52%, respectively, as com-pared with untreated cells.
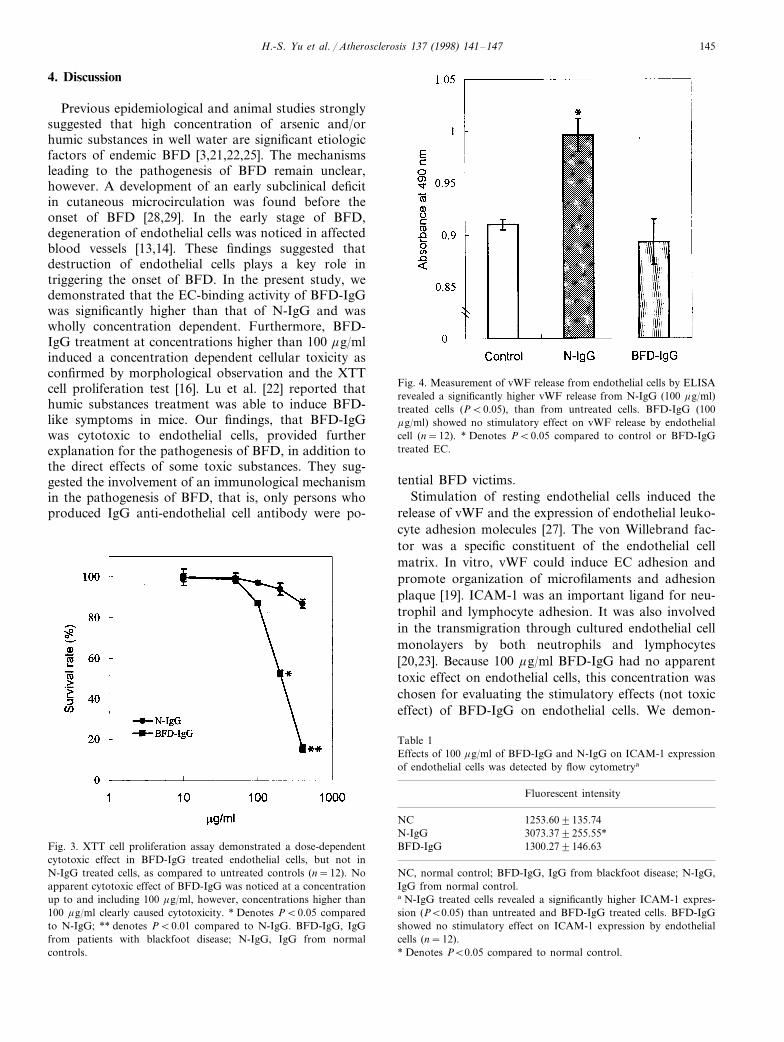
3.5. The stimulatory effect of BFD-IgG on 6WFrelease and ICAM-1 expression by EC
N-IgG treated endothelial cells revealed a signifi-cantly higher vWF release (PB0.05; Fig. 4) andICAM-1 expression (PB0.05; Table 1) than untreatedcells. BFD-IgG treatment showed no stimulatory effecton vWF release and ICAM-1 expression by ECs.
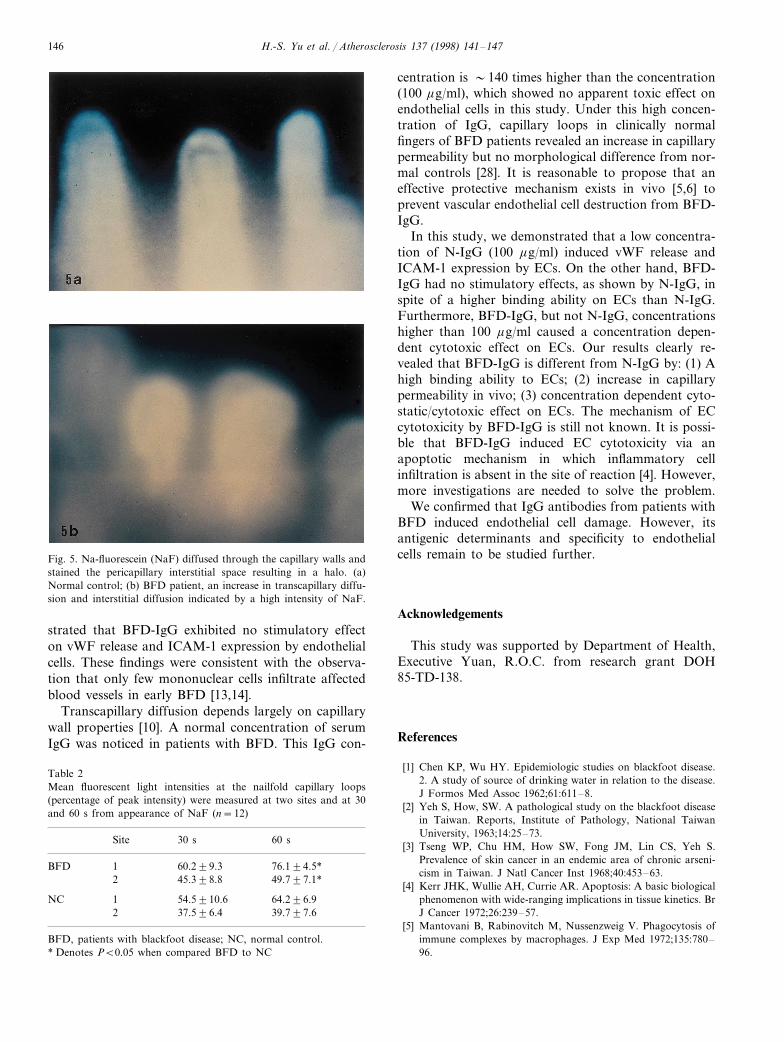
3.6. An increase in transcapillary diffusion andinterstitial diffusion in patients with BFD
Results of dynamic capillaroscopy with NaF revealedan increase in transcapillary diffusion and interstitialdiffusion in clinically normal nailfolds of patients withBFD (Fig. 5a, b; Table 2). A statistically significantincrease in NaF diffusion at site 1 (76.194.5%) andsite 2 (49.797.1%) was noticed in BFD, as comparedto those of the normal controls (64.296.9 and 39.797.6%, respectively) (PB0.05) at 60 s, but not 30 s, afterthe first appearance of NaF in the capillary.
H.-S. Yu et al. / Atherosclerosis 137 (1998) 141–147 145
4. Discussion
Previous epidemiological and animal studies stronglysuggested that high concentration of arsenic and/orhumic substances in well water are significant etiologicfactors of endemic BFD [3,21,22,25]. The mechanismsleading to the pathogenesis of BFD remain unclear,however. A development of an early subclinical deficitin cutaneous microcirculation was found before theonset of BFD [28,29]. In the early stage of BFD,degeneration of endothelial cells was noticed in affectedblood vessels [13,14]. These findings suggested thatdestruction of endothelial cells plays a key role intriggering the onset of BFD. In the present study, wedemonstrated that the EC-binding activity of BFD-IgGwas significantly higher than that of N-IgG and waswholly concentration dependent. Furthermore, BFD-IgG treatment at concentrations higher than 100 mg/mlinduced a concentration dependent cellular toxicity asconfirmed by morphological observation and the XTTcell proliferation test [16]. Lu et al. [22] reported thathumic substances treatment was able to induce BFD-like symptoms in mice. Our findings, that BFD-IgGwas cytotoxic to endothelial cells, provided furtherexplanation for the pathogenesis of BFD, in addition tothe direct effects of some toxic substances. They sug-gested the involvement of an immunological mechanismin the pathogenesis of BFD, that is, only persons whoproduced IgG anti-endothelial cell antibody were po-
Fig. 4. Measurement of vWF release from endothelial cells by ELISArevealed a significantly higher vWF release from N-IgG (100 mg/ml)treated cells (PB0.05), than from untreated cells. BFD-IgG (100mg/ml) showed no stimulatory effect on vWF release by endothelialcell (n=12). * Denotes PB0.05 compared to control or BFD-IgGtreated EC.
tential BFD victims.Stimulation of resting endothelial cells induced the
release of vWF and the expression of endothelial leuko-cyte adhesion molecules [27]. The von Willebrand fac-tor was a specific constituent of the endothelial cellmatrix. In vitro, vWF could induce EC adhesion andpromote organization of microfilaments and adhesionplaque [19]. ICAM-1 was an important ligand for neu-trophil and lymphocyte adhesion. It was also involvedin the transmigration through cultured endothelial cellmonolayers by both neutrophils and lymphocytes[20,23]. Because 100 mg/ml BFD-IgG had no apparenttoxic effect on endothelial cells, this concentration waschosen for evaluating the stimulatory effects (not toxiceffect) of BFD-IgG on endothelial cells. We demon-
Fig. 3. XTT cell proliferation assay demonstrated a dose-dependentcytotoxic effect in BFD-IgG treated endothelial cells, but not inN-IgG treated cells, as compared to untreated controls (n=12). Noapparent cytotoxic effect of BFD-IgG was noticed at a concentrationup to and including 100 mg/ml, however, concentrations higher than100 mg/ml clearly caused cytotoxicity. * Denotes PB0.05 comparedto N-IgG; ** denotes PB0.01 compared to N-IgG. BFD-IgG, IgGfrom patients with blackfoot disease; N-IgG, IgG from normalcontrols.
Table 1Effects of 100 mg/ml of BFD-IgG and N-IgG on ICAM-1 expressionof endothelial cells was detected by flow cytometrya
Fluorescent intensity
NC 1253.609135.743073.379255.55*N-IgG
BFD-IgG 1300.279146.63
NC, normal control; BFD-IgG, IgG from blackfoot disease; N-IgG,IgG from normal control.a N-IgG treated cells revealed a significantly higher ICAM-1 expres-sion (PB0.05) than untreated and BFD-IgG treated cells. BFD-IgGshowed no stimulatory effect on ICAM-1 expression by endothelialcells (n=12).* Denotes PB0.05 compared to normal control.
H.-S. Yu et al. / Atherosclerosis 137 (1998) 141–147146
Fig. 5. Na-fluorescein (NaF) diffused through the capillary walls andstained the pericapillary interstitial space resulting in a halo. (a)Normal control; (b) BFD patient, an increase in transcapillary diffu-sion and interstitial diffusion indicated by a high intensity of NaF.
centration is �140 times higher than the concentration(100 mg/ml), which showed no apparent toxic effect onendothelial cells in this study. Under this high concen-tration of IgG, capillary loops in clinically normalfingers of BFD patients revealed an increase in capillarypermeability but no morphological difference from nor-mal controls [28]. It is reasonable to propose that aneffective protective mechanism exists in vivo [5,6] toprevent vascular endothelial cell destruction from BFD-IgG.
In this study, we demonstrated that a low concentra-tion of N-IgG (100 mg/ml) induced vWF release andICAM-1 expression by ECs. On the other hand, BFD-IgG had no stimulatory effects, as shown by N-IgG, inspite of a higher binding ability on ECs than N-IgG.Furthermore, BFD-IgG, but not N-IgG, concentrationshigher than 100 mg/ml caused a concentration depen-dent cytotoxic effect on ECs. Our results clearly re-vealed that BFD-IgG is different from N-IgG by: (1) Ahigh binding ability to ECs; (2) increase in capillarypermeability in vivo; (3) concentration dependent cyto-static/cytotoxic effect on ECs. The mechanism of ECcytotoxicity by BFD-IgG is still not known. It is possi-ble that BFD-IgG induced EC cytotoxicity via anapoptotic mechanism in which inflammatory cellinfiltration is absent in the site of reaction [4]. However,more investigations are needed to solve the problem.
We confirmed that IgG antibodies from patients withBFD induced endothelial cell damage. However, itsantigenic determinants and specificity to endothelialcells remain to be studied further.
Acknowledgements
This study was supported by Department of Health,Executive Yuan, R.O.C. from research grant DOH85-TD-138.
References
[1] Chen KP, Wu HY. Epidemiologic studies on blackfoot disease.2. A study of source of drinking water in relation to the disease.J Formos Med Assoc 1962;61:611–8.
[2] Yeh S, How, SW. A pathological study on the blackfoot diseasein Taiwan. Reports, Institute of Pathology, National TaiwanUniversity, 1963;14:25–73.
[3] Tseng WP, Chu HM, How SW, Fong JM, Lin CS, Yeh S.Prevalence of skin cancer in an endemic area of chronic arseni-cism in Taiwan. J Natl Cancer Inst 1968;40:453–63.
[4] Kerr JHK, Wullie AH, Currie AR. Apoptosis: A basic biologicalphenomenon with wide-ranging implications in tissue kinetics. BrJ Cancer 1972;26:239–57.
[5] Mantovani B, Rabinovitch M, Nussenzweig V. Phagocytosis ofimmune complexes by macrophages. J Exp Med 1972;135:780–96.
strated that BFD-IgG exhibited no stimulatory effecton vWF release and ICAM-1 expression by endothelialcells. These findings were consistent with the observa-tion that only few mononuclear cells infiltrate affectedblood vessels in early BFD [13,14].
Transcapillary diffusion depends largely on capillarywall properties [10]. A normal concentration of serumIgG was noticed in patients with BFD. This IgG con-
Table 2Mean fluorescent light intensities at the nailfold capillary loops(percentage of peak intensity) were measured at two sites and at 30and 60 s from appearance of NaF (n=12)
Site 30 s 60 s
60.299.3BFD 76.194.5*12 49.797.1*45.398.8
1NC 54.5910.6 64.296.92 37.596.4 39.797.6
BFD, patients with blackfoot disease; NC, normal control.* Denotes PB0.05 when compared BFD to NC
H.-S. Yu et al. / Atherosclerosis 137 (1998) 141–147 147
[6] Schreiber AD, Frank MM. Role of antibody and complement inthe immune clearance and destruction of erythrocytes. J ClinInvest 1972;51:575–82.
[7] Jaffe EA, Nachman RL, Becher CG, Minick R. Culture ofhuman endothelial cells derived from umbilical veins: Identifica-tion by morphologic and immunologic criteria. J Clin Invest1973;52:2745–56.
[8] Fagrell B. The skin microcirculation and the pathogenesis ofischemic necrosis and gangrene. Scand J Clin Lab Invest1977;37:473–6.
[9] Bollinger A, Jager K, Roten A, Timeus CH, Mahler F. Diffu-sion, pericapillary distribution and clearance of Na-fluorecein inthe human nailfold. Pfluger Arch 1977;382:137–43.
[10] Intaglietta M, Johnson PC. Principle of capillary exchange. In:Johnson PC, editor. Peripheral Circulation. New York: Wiley,1978:141–66.
[11] Davison PM, Bensch K, Karasek MA. Isolation and growth ofendothelial cells from the microvessels of the newborn humanforeskin in cell culture. J Invest Dermatol 1980;75:316–21.
[12] Lu FJ, Irgolie KJ, Lin CW, Ling KH, Tung TC. Fluorescentcompounds in drinking well water of blackfoot disease endemicareas. J Formos Med Assoc 1982;81:1087–100.
[13] Yu HS. Blackfoot disease and chronic arsenism in southernTaiwan. Int J Dermatol 1984;23:258–60.
[14] Yu HS, Sheu HM, Ko SS, Chiang LC, Chien CH, Lin SM,Tserng BR, Chen CS. Studies on blackfoot disease and chronicarsenism in southern Taiwan: with special reference to skinlesions and fluorescent substances. J Dermatol 1984;11:361–70.
[15] Masuzawa M, Suzuki Y, Nishiyama S, Nishioka K, Ryan TJ.Guinea pig endothelial cells in culture. J Dermatol 1984;11:371–7.
[16] Scudiero DA, Shoemaker RH, Paull KD, Monks A, Tierney S,Nofziger TH, Currens MJ, Seniff D, Boyd MR. Evaluation of asoluble tetrazolium/formazan assay for cell growth and drugsensitivity in culture using human and other tumor cell lines.Cancer Res 1988;48:4827–33.
[17] Tseng WP. Blackfoot disease in Taiwan; a 30-year follow-upstudy. Angiology 1989;40:547–58.
[18] Yu CL, Chang KL, Hong ST, Chiang BN, Han SH, Wang SR.Detective helper T cell function in IgM rheumatoid factor syn-thesis in patients with ankylosing spondylitis. Scand J Rheuma-tol 1989;18:43–9.
[19] Dejana E, Lampugnani MG, Giorgi M, Gaboli M, Federici AB,Ruggeri AM, Marchisio PC. von Willebrand factor promotesendothelial adhesion via an arg–gly–asp-dependent mechanism.J Cell Biol 1989;109:367–75.
[20] Van Epps DE, Potter J, Vachula M, Smith CW, Anderson DC.Suppression of human lymphocyte chemotaxis andtransendothelial migration by anti-LFA-1 antibody. J Immunol1989;143:3207–10.
[21] Chen CJ. Blackfoot disease. Lancet 1990;336:442.[22] Lu FJ. Blackfoot disease: Arsenic or humic acid? Lancet
1990;336:115–6.[23] Oppenheimer-Marks N, Davis LS, Lipsky PE. Human T
lymphocyte adhesion to endothelial cells and transendothelialmigration. Alteration of receptor use relates to the activationstatus of both the T cell and the endothelial cell. J Immunol1990;145:140–8.
[24] Bollinger A, Fagrell B. Dynamic capillaroscopy with dyes(fluorescence video microscopy). In: Bollinger A, Fagrell B,editors. Clinical Capillaroscopy. Toronto: Hogrefe and Huber,1990:31–52.
[25] Lu FJ. Fluorescent humic substances and blackfoot disease inTaiwan. Appl Organomet Chem 1991;4:191–5.
[26] Walker KW, Llull R, Balkian GK, Ko HS, Flores KM, Ram-samooj R, Black KS, Hewitt CW, Martin DC. A rapid andsensitive cellular enzyme-linked immunoabsorbent assay(cELISA) for the detection and quantitation of antibodiesagainst cell surface determinants. 1. A comparison of cell fixa-tion and storage techniques. J Immunol Methods 1992;154:121–30.
[27] Goerdt S, Pober JS. Endothelium: Differentiation and activa-tion. In: Fitzpatrick TB, Eisen AZ, Wolff K, Freeberg IM,Austen KF, editors. Dermatology in General Medicine, 4th.New York: McGraw-Hill, 1993:375–89.
[28] Yu HS, Chang CH, Chen GS, Yang SA, Yu CL. Study ofdynamic microcirculatory problems in blackfoot disease—em-phasizing its differences from arteriosclerosis. J Biomed Sci1995;2:183–8.
[29] Tseng CH, Chong CK, Chen CJ, Tai TY. Dose-response rela-tionship between peripheral vascular disease and ingested inor-ganic arsenic among residents in blackfoot disease endemicvillages in Taiwan. Atherosclerosis 1996;120:125–33.
[30] Chang CH, Tsai RK, Wu WC, Kuo SL, Yu HS. Use of dynamiccapillaroscopy for studying cutaneous microcirculation in pa-tients with diabetes mellitus. Microvasc Res 1997;53:121–7.
.