in service counselling referrals
TRANSCRIPT

PSYCHOLOGY IN CONFIDENCEPSYMANpart 2
Defence FOI 553/20/21 Item 1 Document 1
CHAPTER 33
IN–SERVICE COUNSELLING REFERRALS
INTRODUCTION
33.1 Defence Force Psychology Organisation (DFPO) psychologists may be required to conductpsychological assessments of serving members. Referral may be from a Service authority or self-referralby an individual member.
33.2 Assessment may involve:
a. interview;
b. administration of psychological tests, questionnaires or inventories; and/or
c. other interventions.
33.3 Instances where assessment may be required include:
a. Administrative Referrals (eg, suitability for retention, suitability for posting, formalwarning);
b. Training Referrals (eg, assessment of suitability for training, study assistance);
c. Medical Referrals or referrals from other specialist officers; and
d. Self Referrals.
33.4 Psychologists are required to familiarise themselves with the primary documents and policiesrelevant to the type of referral they are asked to conduct and for the particular Service for which they areproviding assessment advice. Primary documents include Defence Instructions, Australian Books ofReference, local Training Orders, and so on.
33.5 It is the professional responsibility of the psychologist conducting an assessment to carry outassessments consistent with the provisions of the Australian Psychological Society’s Code of Ethics.This includes the psychologist being professionally competent and appropriately trained to carry out theassessment. Where a breach of professional and/or ethical standards would be entailed, it is theresponsibility of the psychologist to decline to carry out the assessment. In making such a decision, thepsychologist is to consider the option of referring the matter further, particularly in those cases wherecompetence to carry out the assessment is at issue.
33.6 Directorate of Psychology (DPSYCH) is responsible for overall provision of services toAustralian Defence Force (ADF) units. This responsibility is delegated to Principal Psychologists and theCommanding Officer (CO) 1 Psych Unit who exercise the delegation in the part of DFPO for which theyhave professional control.
33.7 The Officer-in-Charge of a Psychology Support Section is responsible for ensuring that highprofessional standards are maintained. They should sight reports prior to their distribution to ensurethose standards are being met. DPSYCH reserves the right to require reports to be checked at theDirectorate prior to their being sent to ADF units. Relevant parties would be notified in advance if thiswere to occur.
33.8 Generally, referrals can be classified as Administrative Referrals, Medical Referrals, TrainingReferrals or Self Referrals. Administrative Referrals and Medical Referrals must be made throughappropriate official channels. On training establishments, Training Referrals should be arranged throughthe training or Divisional system. Self Referrals can be made through any process deemed appropriateby the local Senior Psychologist. It is important that the local Self Referral process is not seen by ADFmembers as a barrier to receiving psychological assistance.
PSYCHOLOGY–IN–CONFIDENCE

PSYCHOLOGY–IN–CONFIDENCEPSYMANpart 2
33–2
Defence FOI 553/20/21 Item 1 Document 1
DOCUMENTATION
33.9 To meet the ethical requirement to make and keep adequate records, an annotation in themember’s Psychology Record is required for every formal psychological intervention. This includes allinstances where the member is referred by a Service authority or self-refers. The document for recordingthese interventions is the Psychology Assessment Record—Trailer (PAR–T).
33.10 Additionally, in most instances where a person is seen by a psychologist following referral froma Service authority, a report is to be raised to provide an assessment and recommend action. Thedocument for this advice is the Form PS 6—Psychological Report. Form PS 6 is available on E–Forms.
33.11 Where psychological testing is conducted, testing details and scores are to be recorded on aPsychology Test Record (PTR). PTR compilation details are contained in part 3, chapter 3—‘Recordingand reporting Psychological Assessments—responsibilities of the Examiners’.
33.12 Wherever possible, a written referral should be obtained from the referring authority, identifyingthe problem to be addressed, relevant background information, and the nature of assistance sought fromthe psychologist. This represents the referring authority’s understanding of the reason for referral. Acopy of the referral is to be placed in the member’s Psychology Record.
33.13 It is the responsibility of the interviewing psychologist to make it clear to the member beinginterviewed, that interview and test information will be permanently recorded on the member’sPsychology Record and that this Record may be sighted by DFPO psychologists or other authorisedagencies in the future.
General guidelines
33.14 All psychology reports should be presented in a professional and coherent style. A Form PS 6should always be typed. The PAR–T must be legible, where possible it should be typed.
33.15 There will always be an element of personal preference and professional discretion in reportwriting, involving both content and style, and of recording interventions. An individual psychologist maychoose their own style, but all relevant information is to be covered while irrelevant information is not tobe included on either a Form PS 6 or a PAR–T.
33.16 Use of headings within a PAR–T or Form PS 6 is at the discretion of the psychologist.
PSYCHOLOGY ASSESSMENT RECORD—TRAILER
33.17 The PAR–T is written as a record of interview and/or therapy for individuals who haveconsulted or been assessed by a DFPO psychologist. The PAR–T is not for the sole use of theinterviewing psychologist and forms part of the Psychology Record. As such, it is accessible to other thanDFPO personnel. Access to Psychology Record documents, with the relevant authorisation, is open to:
a. the client, and anyone duly authorised by the client;
b. DPSYCH;
c. Courts and lawyers;
d. Relevant Government departments/agencies; and
e. any other person/agency who has a bona fide interest as defined by law.
33.18 The PAR–T is to be a structured summary of salient points of the psychologist’s assessment.It is not to contain a series of working notes. Neither is it to be an edited version of, or repeat informationcontained on the Form PS 6. There are to be no unsupported assertions, value judgments ordiscriminatory statements. A professional tone should be adopted at all times.
33.19 Completion of a PAR–T to a professional standard requires that there is no inclusion ofirrelevant information or value-laden judgments. The needs of the original referring authority must beconsidered, including who referred the individual, why they need to know the information, and what usethey will make of the information.
PSYCHOLOGY–IN–CONFIDENCE

PSYCHOLOGY–IN–CONFIDENCEPSYMANpart 2
33–3
Defence FOI 553/20/21 Item 1 Document 1
Structure of a Counselling Referral Psychology Assessment Record—Trailer
33.20 The primary information to be included in a PAR–T falls under some or all of the followingsubject areas which should be addressed as appropriate and relevant:
a. reason for referral;
b. background information;
c. Presentation;
d. relevant history;
e. assessment;
f. evaluation;
g. Treatment Plan, if applicable;
h. summary;
i. conclusion;
j. recommendation, if applicable; and
k. the primary addressee(s) of the Form PS 6, if applicable.
33.21 These information areas are considered in more detail below.
Reason for referral
33.22 This is a simple statement of why the client was referred and who referred them. It is possiblethat the underlying source of referral may not be immediately evident. For example, Self Referrals maybe coerced, while Medical Referrals may effectively be Self Referrals from individuals who did not knowhow to contact a DFPO psychology section directly. When this is the case, the PAR–T should documentthe fact accurately, (eg, ‘X is a Medical Referral but actually approached the MO for …’).
Background information
33.23 The PAR–T is to contain only factual information that provides a summary of the supportingdocumentation that comes with the client. This may include information gleaned from the written referral,personnel file, medical record, medical referral, and so forth. In completing this section, psychologistsshould ask themselves what they looked at and who they talked to before the client was seen.
Presentation
33.24 An individual’s presentation can give many hints as to potential underlying problems. If anyaspect of presentation is unusual or out of context, it should be reported. Areas which should beconsidered include:
a. physical appearance, (including dress, bearing, personal hygiene, etc);
b. speech (eg, voice tone, rate of speech, use of vocabulary and grammar,appropriateness of vocabulary for intelligence and education, word usage, swearing,poverty of content, etc);
c. body language, including eye contact;
d. orientation to place, time and person;
e. attitude toward situation, interviewer, and appropriateness of displayed attitude;
f. dyadic interaction;
g. behaviour and psychomotor activity (eg, tic, twitches, gestures, agitation, rigidity,noises);
PSYCHOLOGY–IN–CONFIDENCE

PSYCHOLOGY–IN–CONFIDENCEPSYMANpart 2
33–4
Defence FOI 553/20/21 Item 1 Document 1
h. waiting room behaviour and dealings with other DFPO staff; and
i. consistency of story.
Relevant history
33.25 Where applicable to the client and their case, the following should be considered and, whereappropriate, reported:
a. the client’s mood, including subjective report of any changes from past to present;
b. any stress-related symptoms;
c. sleep patterns;
d. substance abuse, (including alcohol, caffeine, nicotine, illegal drugs, abuse ofover-the-counter medication, etc);
e. diet;
f. referral antecedents;
g. unresolved traumas/major life events;
h. job history and work stress;
i. offence history;
j. course performance;
k. job performance;
l. how the referring problem is a problem to the individual;
m. duration of the current episode;
n. leisure interests;
o. family history;
p. previous occurrences of present and/or similar behaviour;
q. coping strategies used in similar circumstances (have they worked and why are they notworking now?);
r. interpersonal relations;
s. patterns and nature of medical attendances;
t. previous contact with professionals (chaplains, DCO, medical, psychiatrists and otherpsychologists);
u. previous interventions (eg, counselling, hospitalisation—did they work? If not, whynot?);
v. existing support networks (family, friends, religious affiliations, other professionals orpara-professionals, and within the workplace, including chain of command); and
w. medication history, including why it was taken, how much was taken, who prescribed itand for how long it was used.
Assessment
33.26 Results and interpretation of any psychometric tests should be reported on the PAR–T. Wherethere have been external referrals, their results should also be included.
PSYCHOLOGY IN CONFIDENCE

PSYCHOLOGY–IN–CONFIDENCEPSYMANpart 2
33–5
Defence FOI 553/20/21 Item 1 Document 1
Recording test results
33.27 To ensure that the DFPO is conforming to the various Acts relating to releasing information, alltest scores (raw scores, standard scores, stens, etc) are to be transcribed onto the PTR. This includespersonality and intelligence tests. All psychology tests, answer sheets and profiles are exempt fromrelease under the Freedom of Information Act 1982 because of possible copyright infringements.Therefore, simply adding the answer sheets and profiles to the member’s Psychology Record does notcomply with the requirements for the release of information. In accordance with the relevant AustralianArchives Disposal Schedule, once counselling has finished and test results have been transcribed,completed answer sheets and profiles are to be destroyed. They do not become part of the PsychologyRecord.
33.28 Recorded test results should include sufficient detail to permit accurate interpretation byanother psychologist. For example, if a WAIS is administered, recorded results would include subtestscaled scores as well as Verbal, Performance and Full Scale IQ scores.
Evaluation
33.29 In this section, tie together and interpret professionally all the preceding information. Whereapplicable, include diagnostic hypotheses, an outline of possible secondary gains for the client from thesymptomatology, and their motivation for change.
Treatment plan
33.30 This area should be covered only if applicable. Agreed treatment goals and a provisionaltreatment program should be noted. Existing support networks should be reviewed and otherprofessional networks canvassed. Procedures for follow-up, homework assigned, prognosis and anyonward referrals should be covered.
Summary
33.31 A brief outline of the major points of the case should be covered. No new information is to beincluded here.
Conclusion
33.32 This follows logically from the summary and identifies conclusions drawn.
Recommendations
33.33 Provide a statement of recommendations made, relating them to the reason for referral.
Whether Form PS 6 raised
33.34 Note whether a Form PS 6 has been raised and the referring authority to whom it has beensent.
FORM PS 6—PSYCHOLOGICAL REPORT
33.35 The Form PS 6 is the only psychological report that is to be used. Where a medical referralaccompanied the client, the words ‘see attached Form PS 6’ are to appear on the medical referral form.A report is not to be written on the referral form.
33.36 The primary consideration in structuring and presenting a Form PS 6 is that it must be of aprofessional standard that is appropriate for its intended purpose. Any report should be written inlanguage that can be understood by the intended recipient(s). A Form PS 6 that is going to a MedicalOfficer will tend to be different to one that is going to a Commanding Officer or Divisional Officer.Professional jargon should be used only in rare cases, for example, when reporting to another healthprofessional. Information on psychological matters that is not directly relevant to the referring authority’sinterest in the matter is not to be included in the Form PS 6. For example, if sexual abuse as a child isinvolved in the problem, reference along the lines of ‘incidents in LAC Bloggs’ background’ as underlyingthe problem means that client confidences are not betrayed.
PSYCHOLOGY–IN–CONFIDENCE

PSYCHOLOGY IN CONFIDENCEPSYMANpart 2
33–6
Defence FOI 553/20/21 Item 1 Document 1
33.37 A referring authority’s requirements of psychological assessment and advice are that it bepresented accurately, that it does not contain irrelevant material, and that advice and recommendationsare specific and unambiguous. This is encapsulated by the acronym ABC:
a. Accuracy.
b. Brevity.
c. Clarity.
Content of Form PS 6
33.38 A Form PS 6 should:
a. address issues requested by the referring authority,
b. contain a professional assessment,
c. identify actions taken by the psychologist, and
d. recommend further action or outcomes.
Structure of a Form PS 6
33.39 For different reports, headings may or may not be required. As a general rule, a Form PS 6should contain the following features:
a. a statement of the reason for referral;
b. relevant and appropriate background information;
c. observations from interview pertinent to the referral;
d. assessment and interpretation of the above information;
e. conclusions; and
f. a clear, concise and unambiguous recommendation.
33.40 These areas are considered in more detail below.
Reason for referral
33.41 A statement should be made of the reason for referral so that the context of assessment isclear. This will usually be a restatement of the written referral.
Background information
33.42 Background information that is directly relevant to the current case or issue should be reported.This should not be a comprehensive life and Service history but an identification of material that pertainsto or may help explain the member’s current situation. This section may also contain backgroundinformation that will assist the referring authority to make an appropriate and reasoned decision.
Interview Observations
33.43 Observations from interview that are pertinent to the referral should be reported. Suchobservations may include aspects of the member’s presentation and their perception of what hasoccurred, especially where this provides an alternative interpretation of relevant events.
Assessment and interpretation
33.44 Assess information gained from the various available sources, including psychometricassessment, if applicable. Provide an interpretation of this material as it relates to the reason for referral.Keep in mind the requirements of the referring authority to ensure that these assessments andinterpretations are accurate and fair representations of available information, and present them in a waythat will assist the authority to make their decision.
PSYCHOLOGY IN CONFIDENCE

PSYCHOLOGY IN CONFIDENCEPSYMANpart 2
33–7
Defence FOI 553/20/21 Item 1 Document 1
Conclusions
33.45 Conclusions should follow logically from the preceding sections of the report and relate clearlyto the assessments and interpretations that have been made in the previous section.
Recommendation
33.46 Provide a clear, concise and unambiguous recommendation to the referring authority, relatingthe recommendation to the reason for referral.
REPORT DISTRIBUTION
33.47 A Form PS 6 is to contain a Distribution List to indicate where copies of the document havebeen sent or placed. The referring authority to whom the report is sent is to be the first designation onthe Distribution List. This list is to be located at the end of the report.
33.48 Standard distribution of Form PS 6 reports is:
a. The original report is to be forwarded to the member’s Unit Commander, for attention ofthe referring authority (where the commander is not the referring authority). Forexample: CO SAN (Attention: ADMINO). The report should be delivered in a timelyfashion. In cases where delays in providing the report are considered unavoidable, theunit should be informed of the delay and be given advice on when the report will beprovided.
b. A copy of the Form PS 6 is to be forwarded to the Principal Psychologist withprofessional oversight of the member’s unit. This requirement does not apply in caseswhere the report has already been sighted by one of the above psychologists as part ofnormal supervisory activities. For example, if a 1 Psych Unit psychologist conducts anassessment of a member serving in a Maritime Command unit, the copy of theForm PS 6 should go to Senior Psychologist—Maritime East.
c. A copy is placed on the member’s Psychology Record.
33.49 If copies are to be forwarded to other Service authorities or agencies for information or action,these should also be annotated on the Distribution List.
33.50 Exceptions to this distribution are:
a. Interim training reports. Interim training reports are not sent to the relevant PrincipalPsychologist. As a general rule, it is only reports making definitive recommendations forthe disposal of the member (eg, suspension from training, etc) that need to beforwarded.
b. Medical Referrals. The Form PS 6 is to be sent to the referring authority, NOT themember’s unit. Interim reports on counselling are to be sighted by the local professionalsupervisor, as appropriate, but are not forwarded beyond that level. Final reports withrecommendations are to be forwarded to the Principal Psychologist as above. Forsubsequent referrals (eg, to a psychiatrist), every reasonable effort should be made toensure a copy of the resultant report is placed on the member’s Psychology Record.
c. Self Referrals. Self Referrals do not require the raising of a Form PS 6. Details ofcounselling are to be recorded on a PAR–T. It should be made clear to self-referredclients that the information recorded on their psychology file will form part of theirpermanent record and may be sighted by other DFPO psychologists in the event offuture dealings with the DFPO, or by other persons or agencies under normal accessprovisions.
PSYCHOLOGY IN CONFIDENCE

PSYCHOLOGY–IN–CONFIDENCEPSYMANpart 2
33–8
Defence FOI 553/20/21 Item 1 Document 1
ACCESS TO REPORTS
33.51 A member may request a complete copy of their Psychology Record, or part thereof, througha formal request to DPSYCH. Copies are not to be provided by local psychologists.
33.52 Members may be permitted to sight a copy of the current Form PS 6, in the presence of theauthor or another DFPO psychologist, once a copy has been sent to the referring authority. Anyfeedback to members about the content of a report to which they are subject must be accurate. Ifaccurate feedback cannot be provided, then no feedback at all should be provided.
PSYCHOLOGY IN CONFIDENCE





2
Defence FOI 553/20/21 Item 1 Document 3
Comparison between Kessler Psychological Distress Scale—10 and other measures
7. Research has revealed a strong association between high scores on the K10 and a currentComposite International Diagnostics Interview (CIDI) diagnosis of anxiety or affective disorders.Sensitivity and specificity data analysis has indicated that the K10 is an appropriate screening tool toidentify likely cases of anxiety and depression in the community. There is a lesser but significantassociation between the K10 and other mental disorder categories, or with the presence of any currentmental disorder. The K10 has been found to have better overall discriminatory power than the GHQ–12in detecting DSM–IV depressive and anxiety disorders.
Scoring
8. The K10 is a 10-item scale that has five response categories. A copy of the K10 is in annex A.Responses to the questions are scored from left to right in the following manner:
5 for All of the time4 for Most of the time3 for Some of the time2 for A little of the time1 for None of the time
The scores for each item are added to yield an overall score.
Interpretation
9. A set of cut-off scores for the K10 was developed by the Clinical Research Unit for Anxiety andDepression (CRUfAD), School of Psychiatry, University of New South Wales to determine theprevalence of anxiety or depressive disorders.
10. Scores range from 10 to 50, with the ranges shown below indicating the following:
a. People who score 10–15 report a low-level of psychological distress. They have one quarterthe population risk of meeting criteria for an anxiety or depressive disorder as identified by theCIDI. There is a remote chance of these individuals reporting a suicide attempt in their lifetime;
b. People who score 16–29 report a medium level of psychological distress. They have a one infour chance (three times the population risk) of having a current anxiety or depressivedisorder. They have a one per cent chance (three times the population risk) of ever havingmade a suicide attempt; and
c. People who score 30–50 report a high-level of psychological distress. They have a three outof four chance (ten times the population risk) of meeting criteria for an anxiety or depressivedisorder and six per cent chance (20 times the population risk) of ever having made a suicideattempt.
11. The first group in subparagraph 10.a. comprise 78 per cent of the population, and are unlikelyto require any significant interventions. Groups in subparagraph 10.b. and c. are to be appropriatelyreferred for more thorough assessment, and possibly treatment, if their distress is adversely impactingtheir quality of life. Psychologists are to refer to the appropriate technical instruction for further guidanceon how to manage groups in subparagraph 10.b. and c. Finally, these groups should also be giveninformation on self-help techniques and any support resources that are available to them.
POST–TRAUMATIC STRESS DISORDER CHECK LIST
General
12. The Post-traumatic Stress Disorder Check List (PCL) (Weathers, Litz, Herman, Huska andKeane, 1993) is self-report rating scale for assessing the 17 DSM–IV symptoms of PTSD. Threeversions of the PCL are available, although the differences between them are small. The PCL–Militaryis a specific military version, with questions referring to ‘a stressful military experience’. The PCL–S is anon-military version that can be referenced to any specific traumatic event, with questions referring to‘the stressful experience’. The PCL–C is a general civilian version that is not linked to a specific event,with questions referring to ‘a stressful experience from the past’. The PCL–C is the version currentlyused by the ADF as, at this stage, few ADF members are involved in prolonged combat operations, andare more likely to be exposed to traumatic events other than combat.

3
Defence FOI 553/20/21 Item 1 Document 3
Validity and reliability
13. The PCL has excellent test-retest reliability over a 2–3 day period. Internal consistency is veryhigh and the PCL correlates strongly with other measures of PTSD, such as the Mississippi Scale.
Scoring
14. The PCL is a 17 item scale that has five response categories (a copy is in annex B). Theresponses are scored left to right as follows:
1 for Not at all2 for A little bit3 for Moderately4 for Quite a bit5 for Extremely
A total score is computed by adding the scores on the 17 items, so that possible scores range from 17to 85.
Interpretation
15. In Vietnam combat veterans a cut-off of 50 on the PCL was found to be a good predictor of aPTSD diagnosis. It is therefore recommended that respondents who score above or close to 50 on thePCL be appropriately referred for a more thorough assessment.
ALCOHOL USE DISORDERS IDENTIFICATION TEST
General
16. Hazardous or harmful levels of drinking are often undetected and many people may presentto health care facilities with signs and symptoms that would not necessarily be linked to their drinking.Screening therefore is a simple way to identify people whose drinking may pose a risk to their health,as well as those who are already experiencing alcohol-related problems, including dependence.
17. Screening is extremely valuable as, given appropriate support and assistance, people who arenot alcohol dependent may reduce or stop their consumption. However, once alcohol dependence hasdeveloped, cessation or changes to consumption are much more difficult to achieve and usually requirespecialised treatment. Not all individuals who are drinking at risky or high risk levels will becomedependent, but no one becomes dependent without having first engaged for some time in consumptionat those levels.
18. The AUDIT screening test was developed by the WHO as a simple method of both screeningfor hazardous and harmful use of alcohol and assisting in the formulation of brief interventions. Itprovides a framework for an intervention with hazardous and harmful drinkers that aims to reduce orcease their alcohol consumption. It also helps to identify alcohol dependence and some of the specificconsequences of hazardous and harmful drinking.
19. The AUDIT provides an accurate measure of risk across gender, age, and cultures. Its validity,brevity and flexibility make it the most widely used alcohol-screening instrument around the world. TheAUDIT is particularly designed for health care practitioners in a range of health settings. Furthermore,with suitable instruction it can be self-administered or used in other settings by non-health professionals.
Administration
20. The Interview Version AUDIT screen is to be administered by health and allied healthprofessionals who have received appropriate training in the use of the tool. Training in the use of AUDITwill be coordinated and provided by the ADF Drug and Alcohol Program, Directorate of Mental Health.The version of the AUDIT to be utilised by Defence Health Service uniformed and contracted personnelwhen performing screening for hazardous and harmful alcohol use appears in annex C.

4
Defence FOI 553/20/21 Item 1 Document 3
Scoring
21. The AUDIT consists of ten scored questions (questions 1–10). Two additional non-scoredquestions (questions 11–12) provide an indication of readiness or motivation to change and have beendesigned to assist in determining appropriate levels of intervention.
22. AUDIT questions are related to the following conceptual domains:
a. questions 1–3 ask about frequency and quantity of drinking and lie within the hazardousalcohol use domain;
b. questions 4–6 ask about impairment of control over drinking, salience of drinking and morningdrinking. These questions lie within the dependence symptoms domain;
c. questions 7–10 ask about feelings of guilt, blackouts, injury and concern by others. Thesequestions lie within the harmful alcohol use domain.
23. Scoring of AUDIT is a simple activity. Each of the questions 1–10 has a set of responses tochoose from and each response has a value ranging from 0–4 (the number within parentheses). In theAUDIT—Interview Version, the interviewer enters the score corresponding to the response into the boxbeside each question. Then adds the scores from all the questions and records the answer in the boxbelow question 10.
Interpretation
24. Total scores of 8 or more are regarded as indicators of hazardous or harmful alcohol use, orpossible alcohol dependence. Higher scores indicate greater likelihood of hazardous and harmfuldrinking and may also reflect greater severity of alcohol problems and dependence.
25. More detailed interpretation of an individual’s total score may be obtained by determining onwhich questions points were scored. In general, a score of 1 or more on questions 2 or 3 indicatesconsumption at a hazardous level. Points scored above 0 on questions 4–6 imply the presence orincipience of alcohol dependence. Points scored on questions 7–10 indicate that alcohol-related harmis already being experienced. The total score, consumption level, signs of dependence, and presentharm all should play a role in determining how to manage an individual. Questions 9 and 10 should alsobe reviewed to determine whether there is evidence of a past problem.
26. Questions 11 and 12 are not scored. Responses to these questions indicate readiness ormotivation to change, and assist the person administering the AUDIT to determine the most appropriateintervention.
Intervention
27. Individuals scoring 0–7 on AUDIT are regarded as low risk drinkers (or may be abstinent).Feedback affirming the low risk nature of alcohol consumption, and alcohol education, is appropriate.Provision of standard drinks health promotion material such as the ‘Alcohol and Your Health’ bookletproduced by the National Health and Medical Research Council is also appropriate. Copies of thisbooklet can be obtained through the ADF Drug and Alcohol Program.
28. Individuals scoring 8–15 on AUDIT are consuming alcohol in excess of low risk guidelines. Abrief intervention using simple advice and health education materials is the most appropriate course ofaction. Focussing on immediate goals may allow for more immediate success in the treatment process,whatever the long-term goals may be. Immediate goals might include decreasing the frequency ofdrinking, maintaining an alcohol-free day or keeping a drinking diary. Where there is no opportunity toconduct an opportunistic brief intervention, the member should be provided with a ‘TakeawayIntervention Pack—TIP’ for modifying alcohol consumption. TIPs for modifying alcohol consumption arepackages containing a range of materials providing basic health information and practical approachesto cutting down drinking. TIPs are distributed to all ADF health and psychology facilities by the ADF Drugand Alcohol Program.
29. AUDIT scores of between 16–19 indicate hazardous and harmful levels of alcoholconsumption. Hazardous and harmful use of alcohol can be managed by a combination of simpleadvice, brief counselling and continued monitoring by a health or allied health professional. Furtherdiagnostic evaluation is indicated if the individual fails to respond to the intervention or if possible alcoholdependence is suspected.





DIRECTOR–GENERAL DEFENCE HEALTH SERVICE
C
Defence FOI 553/20/21 Item 1 Document 4
HEALTH BULLETIN NO 10/2003Note: Director-General Defence Health Service Health Bulletins are produced to disseminate HealthInformation. They are to be filed in a separate binder, readily accessible to all staff. They remain in effectuntil cancelled in accordance with instructions in the Bulletin. Publications can be accessed on theDefence Intranet at http://defweb.cbr.defence.gov.au/home/documents/adfdocs/healthindex.htm
13 AUGUST 2003
AUSTRALIAN DEFENCE FORCE REGIONAL MENTAL HEALTH TEAMSINTRODUCTION
1. The integration of mental health services in Defence is a fundamental initiative of the Aust lianDefence Force (ADF) Mental Health Strategy (MHS), with delivery of mental health services eingfocussed on regions, and the various command structures in those regions. An esse ial part o heADFMHS is the formation of Regional Mental Health Teams (RMHT). These t ams are a crit alcomponent in both implementing the ADFMHS and the delivery of mental health servic s in th regionThe development and maintenance of these multidisciplinary teams is ased on a co ltation-liaisomodel and:
a. facilitates access to the most appropriate servi es f ADF person el;
b. is cost-effective and avoids duplicatio
c. promotes mental wellbein ;
d. facilitates early id ntific on and intervent n;
e. is gover by com on d ctrine;
f. as centra sed su po and direction;
provi s a p er review capability; and
h. conforms to privacy and confidentiality requirements.
AIM
2. The aim of this Health Bulletin is to promulgate ADF policy on the structure and function ofRMHT.
POLICY
General
3. The location of teams has been determined by the demand for services, the locations ofmilitary personnel and the availability of mental health professionals employed by Defence in thoseregions (see annex A). RMHT members should be, where possible, experienced senior practitioners intheir discipline. These practitioners are to be members from the following professions: Psychiatry,Psychology, Social Work, Nursing, Chaplaincy, General Medicine and the alcohol and other drug area(see annex B).
Membership
4. To fill RMHT positions, the following key stakeholders are to nominate senior representativesin each appropriate region:
a. Joint Health Support Agency;
b. Environmental Commands (Senior Medical Officers when available);
ANCELLED

2
C
Defence FOI 553/20/21 Item 1 Document 4
c. Defence Force Psychology Organisation;
d. Single Service Psychology Agencies (where available);
e. Defence Community Organisation (DCO); and
f. Principal Chaplains Department.
Director Mental Health (DMH) will appoint the Convenor of each RMHT. Within the guidance providedin annex B, RMHT can augment their membership to meet regional command structures and demands.It is also recognised that RMHT may not be able to meet the guidance in annex B due to the varyingavailability of Defence mental health professionals in their region.
Roles and responsibilities
5. The role of the RMHT is to facilitate delivery and integration of mental health services for ADFpersonnel. Whilst delivery of mental health services is primarily provided through the chain of command,RMHT provide commanders with additional tools to assist in the effective management of personnel.RMHT should integrate and augment the relationships commanders may already have with local serviceproviders such as Area Health Service, local Australian Defence Organisation psychologists, DCO andDefence Chaplains. The role of the RMHT is in no way intended to replace existing relationshipbetween command and local service providers. The roles and responsibilities of the RMHT are lis ed inannex C.
Peer review
6. RMHT meetings can provide a forum in which members will e able to of problems of aprofessional nature to the team for constructive peer review. The overall g al of peer rev w in this fo umis to advance the professional development of Defence ment l health profe sionals. To that en RMHTprovide a facility for members to explore professional is es, f ce new chall ges, develop professionalstrength and work on minimising the impact of an weaknesse 1.
7. The environment for peer r i w ne ds to b safe, upporti and non-threatening. Theprocess is voluntary and is to be col egiate in natu Peer review m utilise methods such as coaching,teaching, guest lecturing, formall led discussions or the use of formal one-on-one meetings. RMHTmeetings also provide e o portunity for c ss iscipline professional development andcommunication. DMH is also enga ed in the p cess both within its own team and with all RMHT.
Admini ration
8. RMHT are ncourage to identify local Reserve mental health or administrative personnelwho ar willin o pro de administrative support to teams. DMH will bid for reserve training days onbehalf o ach RMHT.
Funding
9 RMHT are to be fundamentally self-sustaining by stakeholder contributions for regionalactivities. Commanders may organise special events that include mental health activities, and RMHTare encouraged to contribute their ideas early to commanders for budget consideration. In addition,DMH will consider all formally submitted requests for funding for specific activities, projects or resourcessuch as extra Reserve days. RMHT should submit business cases to DMH as outlined in annex D.
Regular meetings
10. RMHT are to meet a least quarterly. Agenda items may be accepted from sources such asDMH, RMHT, Defence service providers and commanders. The convenor should determine the mostappropriate way to provide feedback. The convenor may invite commanders to address specific agendaitems at meetings as well as ensuring that commanders and service providers are briefed on theactivities of the RMHT as appropriate. Annex E provides a list of agenda items that may be considered.Teams are to forward copies of their minutes to DMH.
1 Some professional bodies/organisations may deem that these activities meet their professional membershiprequirements. RHMT members should contact their professional organisation for further clarification.
ANCELLED


ANNEX A
C
Defence FOI 553/20/21 Item 1 Document 4
REGIONAL MENTAL HEALTH TEAMS LOCATIONS
1. Regional Mental Health Team locations are:
Australian Capital TerritoryCanberra
QueenslandAmberleyBrisbane metropolitan areasCairnsTownsvilleDarling Downs
Northern TerritoryDarwinTindal
New South WalesSydney
• Central• Richmond/Glenbrook/Orchard Hills• Holsworthy
Nowra/Jervis Bay—HMAS ALBATROSS, HMAS CRESWELLWagga WaggaWilliamtown/Singleton
VictoriaAlbury/WodongaWestern Port—HMAS CERBERUSMelbourne metroPuckapunyalSale
South AustraliaAdelaide/RAAF Edinbu h
Wes rn Aus aliaP rth C ntral/R AF Base PearceHMAS T RLING
Ta maniaH bartANCELLED

ANNEX B
C
Defence FOI 553/20/21 Item 1 Document 4
MEMBERSHIP OF A REGIONAL MENTAL HEALTH TEAM1. The Regional Mental Health Teams (RMHT) will be multidisciplinary, and personnel should be,where possible, experienced senior practitioners in their profession. RMHT membership will be byinvitation from their parent organisations. It is recognised that not all regions will have all the professionsidentified below. Ideally, the team is to include the following key roles:
a. A medical officer from Area Health Service (AHS) to provide specialist medical advice and a directlink to AHS;
b. A medical officer(s) from environmental command health unit(s) to provide specialist medicaladvice and a direct link back to local commands;
c. A Defence Social Worker to provide specialist social work advice and a direct link to the DefenceCommunity Organisation;
d. A Defence Psychologist to provide specialist psychological advice and a direct link to the DefenceForce Psychology Organisation;
e. Single Service psychology elements specific to the environmental command;
f. A psychiatrist to provide specialist psychiatric advice (this person will usually be Rese vist,exceptions are to be discussed with Director Mental Health (DMH) on a case-b case basis);
g. A Defence Chaplain to provide specialist chaplaincy advice;
h. An alcohol and other drug (AOD) staff member to provide specialist dvice and to rovide a di ectlink to Australian Defence Force National Coordinator rug and Alc ol program;
i. The Regional Critical Incident Mental Healt Support coo dinator if not lrea y represented; and
j. Reserve administrative assista re av ilabl
2. The RMHT is directly respo sible to DMH, v the DMH appointed convenor.
ANCELLED

ANNEX C
C
Defence FOI 553/20/21 Item 1 Document 4
REGIONAL MENTAL HEALTH TEAM ROLES AND RESPONSIBILITIES
Team functions
1. The Director Mental Health (DMH) and Regional Mental Health Teams (RMHT) are the essentialcomponents of the Australian Defence Force (ADF) multidisciplinary mental health model. Throughpolicy and centrally based supervision, DMH provides strategic guidance for RMHT. The RMHTrepresents a consultative liaison model of service delivery and aims to:
a. provide a coordinated and integrated information resource for commanders;
b. implement ADF Mental Health Strategy (MHS) initiatives at a regional level;
c. coordinate mental health services at a regional level;
d. conduct and coordinate regional primary prevention projects;
e. encourage information sharing between mental health service providers;
f. coordinate regional mental health monitoring;
g. provide opportunities for professional development, supervision, support and p er review;
h. facilitate regional mental health training;
i. facilitate the networking for case-conferencing as required;
j. maximise the services and specialist skills of De ence Reserve menta health professionals;
k. maintain a register of local community me tal health prov ers and any peciality skills or interestareas;
l. maintain a register of lo al Australian D fence Or anisation mental health professionals(including local Rese ists) nd any specialis skill or their areas of interest;
m. support the ominated conve or in his/her leadership role in implementing this policy, and
n. c m unicate with ne gh ouring RMHT and organise convenor meetings when there ares nific t bene its to the ADFMHS.
2. C ck list fo administrative responsibilities of the RMHT:
a. th RMHT must meet at least quarterly;
b there must be a Chairperson (convenor) appointed by, and responsible for liaison with, DMH;
c. there is to be a secretary appointed by the convenor;
d. at least shortened minutes of the meetings are to be kept in accordance with Australia DefenceForce Publication 102—Defence Writing Standards, part 2, chapter 5—‘Agenda and minutes ofmeetings’;
e. RMHT convenors to provide reports to DMH by the end of May and November (see annex F); and
f. maintain registers.
ANCELLED

ANNEX D
C
Defence FOI 553/20/21 Item 1 Document 4
BUSINESS CASE PREPARATION AND SUBMISSION FORMAT
Purpose
1. The purpose should clearly state the result or course of action being sort, and indicate any timingpressures.
Issues
2. For issues:
a. Summarise the important issues and matters for decision.
b. Identify risk issues potentially resolved by the business case as well as risks if the case isunsuccessful.
c. Use dot point format.
Consultation
3. List personnel who have been consulted, and indicate whether there is agreement.
Resource implications
4. Identify the financial and cost details of any proposal including personnel costs eg Reser e dayservice providers and consultants. Include an overall cost estimate and time frame.
Recommendations
5. It is recommended the business case:
a. be concise; and
b. clearly express the proposed course of ction, who is accountable, and time frames forimplementation.
Contact Officer: ( me and te epho e)Authorised by: (name d tele honeDate:
ANCELLED

ANNEX E
C
Defence FOI 553/20/21 Item 1 Document 4
AGENDA ITEMS FOR THE REGIONAL MENTAL HEALTH TEAM MEETING
1. The approved standard for meetings at all levels throughout Defence is Australian Defence ForcePublication 102—Defence Writing Standards. Issues that may be included in a Regioinal Mental HealthTeam agenda but are not be limited to:
• Business arising from previous meetings.
• Commanders’ communications, and concerns identified by command.
• Implementation of the Australian Defence Force Mental Health Strategy.
• Feedback on the multidiscipinary approach to delivery of mental health services.
• Feedback from customers and interested parties (including complaints).
• New opportunities and business improvement suggestions.
• Progress report on current works or projects.
• Service provider evaluation and performance.
• The competency and training requirements of staff.
ANCELLED

ANNEX F
PRO FORMA FOR REGIONAL MENTAL HEALTH TEAMS ACTIVITY REPORT
STAFF–IN–CONFIDENCE
1. The activities and observations of the Regional Mental Health Teams (RMHT) are to be reportedto the Defence Health Service Steering Committee twice yearly. These reports will be compiled byDirector Mental Health from the RMHT submitted reports based on the following criterion:
a. Establishment or Region.
b. Period From ………….. To ………….
c. Name, title and period of convenor(s).
d. Name and title of all persons on RMHT over this period.
e. Dates of RMHT meetings.
f. Quality issues such as opportunities for improvement and corrective actions taken.
g. Business case submissions and date.
h. Business activities and progress.
i. Mental Health Activity Report (eg morale, critical incidents, training etc).
STAFF–IN–CONFIDENCE
CANCELLED
Defence FOI 553/20/21 Item 1 Document 4

DIRECTOR–GENERAL DEFENCE HEALTH SERVICE
Defence FOI 553/20/21 Item 1 Document 5
HEALTH BULLETIN NO 11/2003Note: Director-General Defence Health Service Health Bulletins are produced to disseminate HealthInformation. They are to be filed in a separate binder, readily accessible to all staff. They remain in effectuntil cancelled in accordance with instructions in the Bulletin. Publications can be accessed on theDefence Intranet at http://defweb.cbr.defence.gov.au/home/documents/adfdocs/healthindex.htm
13 AUGUST 2003
MENTAL HEALTH SUPPORT TO OPERATIONALLY DEPLOYED FORCESINTRODUCTION
1. The Australian Defence Force (ADF) recognises that war, warlike, peacekeeping andpeacemaking operations expose personnel to significant risk factors for the development of long-termmental health problems and mental disorders. The ADF is therefore required to provide operationallyfocused mental health promotion, prevention and early treatment services for all such deployed forces.The aim of operational support is to assist personnel to deploy, perform their operational dutieseffectively, and then return to work and private lives with minimum disruption.
2. The focus of this Health Bulletin (HB) is to provide guidance on mental health services foroperationally deployed forces. It is expected that this guidance will be incorporated into the health plansfor designated operations. There is to be no alteration to the procedures outlined in this HB without theapproval of the Director Defence Force Psychology Organisation (DFPO).
AIM
3. The aim of this HB is to outline the mental health support to be provided to forces deployed onwar, warlike, peacekeeping and peacemaking operations.
SCOPE
4. This HB includes key service providers, principles of service delivery, and instructions formandatory psychological preparation and screening for designated operations.
GENERAL
5. Mental health support to operationally deployed forces is comprised of the following three keyelements:
a. Pre-deployment psychological preparation;
b. In-country support; and
c. Post-deployment psycho-education, screening and follow-up.
These elements are aimed at assisting ADF personnel to manage the psychological demands of theoperational environment. They are also aimed at enhancing the operational effectiveness of deployedADF personnel, and identifying/assisting those individuals who experience adjustment difficulties andpsychological or psychiatric disorders as a result of their operational experience. The model for mentalhealth support is detailed in annex A.

2
Defence FOI 553/20/21 Item 1 Document 5
SERVICE PROVIDERS
6. The main providers of mental health support to deployed forces are:
a. Defence force psychology provides pre-deployment psychological preparation and/ormental health screening, in-country support (when deployed to the Area of Operations (AO)),post-deployment mental health screening and individual follow-up (including psychologicaltreatments and general counselling).
b. Defence health services provides general health preparation for operations, in-countrymedical treatment facilities, medical evacuation, post-deployment general health screening,and post-deployment treatment facilities.
c. Defence Community Organisation provides welfare support for the families of deployedpersonnel.
d. ADF Chaplains provide specialised services (such as incident management and griefcounselling) as well as ongoing pastoral care and supportive counselling.
e. Unit Personnel (leaders and peer supporters) provide ongoing mental health promotion andsurveillance.
f. Operational Commanders maintain leadership, training, unit cohesion and morale, andcombat readiness to protect personnel from operational mental health risk factors.
AIMS OF SERVICE DELIVERY
7. The major aims of mental health support to operationally deployed forces are:
a. promotion of mental wellbeing and positive living skills before, during and after thedeployment;
b. continued engagement of, and liaison with, command and its elements;
c. proactive screening and intervention for personnel exposed to significant risk factors(see Health Bulletin—Critical Incident Mental Health Support Program for guidance withrespect to the management of critical incidents and potentially traumatising events);
d. appropriate mental health treatment for those displaying acute and chronic psychologicalinjuries before, during and after operational deployments;
e. maintenance of unit support and cohesion during all aspects of service delivery, with therebeing an expectation of returning personnel to duty after successful treatment;
f. mandatory pre-deployment psychological preparation; and
g. mandatory post-deployment mental health screening for designated operations.
8. Services are mandated to ensure that all members deployed receive standard information andcare before, during and after an operational deployment. Mandated education and screening allows theADF to exercise its duty of care to all members in a consistent and standardised fashion that isindependent of the Service the member belongs to. It allows for ongoing surveillance that may assist infuture planning and management of operationally deployed forces. It must be noted that mandatededucation and screening does not equate with mandated treatment. Screening ensures that allmembers receive reliable guidance regarding their current mental health needs, guidance that mayassist them to make an informed decision regarding whether or not to seek treatment.

3
Defence FOI 553/20/21 Item 1 Document 5
PRE–DEPLOYMENT PSYCHOLOGICAL PREPARATION
9. Psychological preparation for an operational deployment is designed to equip members withknowledge to assist them to adapt more effectively to the deployment environment. All operationallydeployed personnel should receive this preparation as one of the modules during the broaderpre-deployment training period, either at their individual ship or unit, or during processing by DeployedForces Support Unit or Force Preparation Unit.
10. Common to all operational deployments is the requirement for ADF personnel to receive thePsychological Preparation for Deployment psycho-educational briefing. This is a standardised briefingpackage that is available from 1 Psych Unit, Directorate of Mental Health (DMH), or respective singleService principal psychologists. It is to be delivered by Service psychologists as part of the broaderpre-deployment training.
11. In addition to general psychological preparation for operational deployment, membersdeploying on specific missions may also benefit from receiving other, supplementary, briefing packagesthat can be delivered by ADO psychology personnel. Such briefing packages may include:
a. hostage survival skills;
b. dealing with refugees/internally displaced people;
c. conflict resolution skills;
d. fatigue management;
e. dealing with human remains; and
f. negotiation skills in hostile environments.
12. A complete list of available packages is available from DMH, and also from 1 Psych Unit.Psychology personnel are encouraged to liaise directly with unit commanders about the range of topicsthey would like to have included in their pre-deployment training.
13. All personnel preparing to deploy should receive the latest version of the Deployment Guidebooklet. The Deployment Guide contains detailed information on separation, stress,stress-management strategies, critical incident mental health support, and homecoming issues.Supplies of the Deployment Guide can be obtained either from DMH or 1 Psych Unit.
14. Commanders may also exercise their option of referring personnel identified for operationaldeployment for psychological assessment should they have concerns about the member’s suitability fordeployment. Such referrals need to be made under coverage of a Form PM 008—Report on a CaseReferred for Psychiatric or a Psychological Examination.
15. Administrative details regarding the gathering of personal details for deployed personnel areoutlined in DFPO technical instructions.
MENTAL HEALTH SUPPORT IN THE AREA OF OPERATIONS
16. Mental health in an AO is typically managed, in accordance with health management plans,by medical officers, nursing officers and medical assistants in the AO. However, with large deployedcontingents, or with missions that have been identified as having the potential for exposure to largescale psychological trauma, Psychology Support Teams (PsST) may form part of the deployed healthelements. In-country PsST provide the full range of psychological services available in Australia,including Critical Incident Mental Health Support (CMS). The role of the PsST is to promote and maintainthe mental health of ADF personnel, and to provide operational support to commanders. Similarly, apsychiatrist and mental health nurse may deploy as part of the health element, with their tasking beingin accordance with the detailed health plan.

4
Defence FOI 553/20/21 Item 1 Document 5
17. In support of an operation, it may be necessary to provide regular mental health monitoring forspecific populations. Specified populations may include personnel involved in the recovery of humanremains, interrogations, hostage situations, and other duties that involve higher levels of intensity,longer duration or frequent exposure to trauma. Previous operational experience has also indicated thatchaplains, service police, ADF journalists and photographers, and medical personnel may requireadditional attention due to the nature of their duties. This list is not exhaustive, and commanders andmental health support staff should be constantly vigilant for groups or individuals who warrantspecialised support.
18. Where there is no PsST or psychiatrist deployed, care of the psychiatric casualty is inaccordance with the heath management plan for that operation. That plan may include reliance uponmental health support resources from allied forces, or the use of ‘fly-in’ teams for specific events/incidents.
RETURN TO AUSTRALIA PSYCHOLOGICAL SUPPORT
19. Return to Australia Psychological Screening (RTAPS) is administered by Defence Psychologypersonnel and aims at both assessing the deployment’s impact upon the member’s current level ofpsychological functioning, and indicating which members may be experiencing adjustment difficulties.
20. RTAPS processing comprises the following:
a. Psycho-educational brief;
b. RTAPS questionnaire; and
c. Individual psychological screening interview.
Administrative procedures for conducting RTAPS are detailed in reference B.
21. Where possible, RTAPS should be conducted during the Force Extraction process in the AO.For RAN personnel, it is most likely that RTAPS will be conducted onboard ship, on route to Australia.It is recognised that Service or operational reasons may preclude the provision of RTAPS prior to themember’s return to Australia. These circumstances may include the number of personnel involved, theremoteness of the location, lack of qualified personnel, or emergency conditions that precludescreening. In such circumstances, RTAPS will be conducted as soon as practicable after their return toAustralia (preferably within 72 hours).
22. Where a member attends, but refuses to participate in any or all of the RTAPS procedure, thisshould be noted by the psychologist on the Psychological Screening Record (PSR). However, a pointof contact for follow-up is to be provided to that member.
23. During the RTAPS process members are to be offered a copy of the Homecoming Guidebooklet. This booklet includes information on separation, homecoming and tips for reunion. Stocks ofthis booklet can be provided either through DMH or 1 Psych Unit.
24. When large numbers of personnel are being processed, the senior psychologist is to ensurethat daily staff consultations occur. The aim of this is to identify trends within the deployed population,provide supervision to less experienced members of the psychology team, and to monitor each other’swellbeing. Where RTAPS is being conducted in the National Support Area, additional psychologicalresources can be provided upon request to the DFPO.

5
Defence FOI 553/20/21 Item 1 Document 5
POST–OPERATIONAL PSYCHOLOGICAL SUPPORT
25. Personnel generally manage the strain of deployed operations quite well. However, for somemembers problems may arise in the months following their return to Australia. For example, there maybe problems with reintegration into the family, the civilian community and routine military duties followingthe higher tempo and differing priorities and experiences of deployed operations. Mandatorypost-operational screening may assist in identifying personnel who are having difficulties readjustingand then helping them to access appropriate support.
26. The aims of post-operational screening are:
a. to provide an effective mechanism to preserve personnel capability, by identifying whethermembers require any assistance to return to pre-deployment psychological functioning;
b. to fulfil the ADF’s duty of care to members exposed to operational environments by assistingin the identification of members experiencing negative consequences and then facilitatingappropriate follow-up care for such members;
c. to provide a mental health surveillance and feedback mechanism to commanders and thegeneral health planning community; and
d. to assist in research regarding operational impact, with a further aim of tailoring appropriateintervention techniques for members.
27. Six months after the deployment, Post Operational Psychological Screens (POPS) areconducted by Defence psychology personnel to ensure that deployed personnel have adequatelyreadjusted to life in Australia. POPS is not simply surveillance, it is about exercising a responsible‘duty of care’ by careful identification and appropriate follow-up care. The POPS process consists of:
a. the administration of standardised and widely used mental health screening inventories, and
b. an individual screening interview with a psychologist.
28. The administration and interpretation of POPS is detailed in DFPO technical instructions. A listdetailing personnel requiring POPS will be sent out to a member’s servicing psychology element on aregular basis. Upon receipt of this advice, psychology elements are to arrange for the personnel to bescreened as close as practicable to the six months post-operation time frame.
29. Where a member attends, but refuses to participate in any element of the POPS, thepsychologist should be noted on the PSR. A point of contact for follow-up should, however, be providedto the member.
30. Personnel who are identified through the POPS as requiring follow-up are to be referred bythe psychologist to appropriate agencies for further assessment and treatment. In some circumstancesit may also be appropriate for the psychologist administering the POPS to also undertake follow-up carewith the member. This is dependent upon the professional skills of the psychologist and the willingnessof the member to enter into follow-up with that psychologist. With respect to follow-up, it is expected thatthe psychologist will engage the member in this process, securing their ‘cooperation’ and acceptancethat referral is in their best interests. The member has the right to refuse such referral, but the refusalmust be noted in the member’s psychology file on the PSR.
COMMAND RESPONSIBILITY
31. It is mandatory that all commanders ensure that personnel who have been on deploymentscomplete both RTAPS and POPS. This includes both permanent and reserve personnel, and those ondetachment or temporary duty.



DIRECTOR–GENERAL DEFENCE HEALTH SERVICE
Defence FOI 553/20/21 Item 1 Document 6
HEALTH DIRECTIVE NO 260Note: Director-General Defence Health Service Health Directives are of a permanent nature and remainin force until cancelled. They are reviewed every three years and repromulgated only where asignificant change of content is necessary. Publications can be accessed on the Defence Intranet at http://defweb.cbr.defence.gov.au/home/documents/adfdocs/healthindex.htm
18 AUGUST 2003
AN INTRODUCTION TO THE MANAGEMENT OF MENTAL HEALTH PROBLEMS IN THE AUSTRALIAN DEFENCE FORCE
References: A. Australian Defence Force Mental Health Strategy ReportB. Diagnostic and Statistical Manual of the American Psychiatric Association, Volume IV, text
revision (DSM–IV–TR:APA, 2000)C. National Mental Health Strategy 2000D. Australian Defence Force Health Status Report 2000E. Defence Instruction (General) (DI(G)) PERS 16–1—Health care of Australian Defence Force
personnelF. Health Directive (HD) 236—Medical Employment Classification Procedures
INTRODUCTION
1. Mental health is a state of successful performance of mental function, resulting in productiveactivities, fulfilling relationships with other people, and the ability to both adapt to change and cope withadversity. The Australian Defence Force Mental Health Strategy Report (reference A) identified mentalhealth as a key component in the overall health of the ADF and, therefore, an important factor indetermining Australian Defence Force (ADF) capability. An ADF member may be completely healthy ina physical capacity, but if not mentally fit, the member’s ability to perform military duties, particularly ondeployment, may be partially or totally impaired.
2. Reference A further recognised that the ADF may experience a decrease in its personnelcapability, and therefore, operational capability through the impact of:
a. the inherent stressors of military service,
b. normal life cycle issues, and/or
c. genetic predispositions.
Essentially, the effects of such stressors may cause or exacerbate a diagnosable mental disorder, orother subclinical mental health problem.
3. Often, a definitive mental health intervention is initiated only when the individual presents formanagement of an acute problem, or when administrative processes suggest a possible underlyingmental health concern. However, mental health concerns are not limited to the diagnosis of psychiatricproblems. Mental health concerns also include conditions such as anxiety, stress reactions, reactivetransient depressive episodes or other mental health problems that may, in turn, arise out of:
a. operational service (war, warlike, peacekeeping or peacemaking);
b. service within the National Support Area (eg occupational stressors, training incidents,etc);
c. family problems (eg relationships, children, etc);
d. life cycle problems (eg bereavement);
e. personal variables (eg personality problems); or
f. general medical or health issues.

2
Defence FOI 553/20/21 Item 1 Document 6
4. Health providers should also understand that symptoms might be present in a person withoutbeing clinically significant. Such symptoms may be subclinical and only marginally impact an individual’spersonal or working life. In fact, the degree to which problems or symptoms pervade a person’s life is amajor determining factor of clinical significance. Mental health problems may not, therefore, necessarilyrequire specific psychiatric intervention but can, instead, be dealt with by a range of mental healthproviders. Depending on the severity of the individual’s condition, treatment modalities may include, butnot be restricted to, the following:
a. in-patient care;
b. psychiatric intervention, either inpatient or outpatient;
c. counselling;
d. psychopharmacological treatment;
e. family therapy; and
f. outpatient group programs, including anger management groups.
5. The treatment and management of mental health problems in the ADF has traditionally beenthe domain of several key organisations, including the:
a. Defence Health Service Branch (DHSB);
b. Defence Force Psychology Organisation;
c. Single Service psychology agencies;
d. Defence Community Organisation (DCO); and
e. Defence Chaplaincy.
6. Historically, coordination between these agencies has not been ideal. Noting this, reference Asubsequently recognised that the creation of a cohesive and holistic ADF Mental Health Service (MHS)would assist in providing improved outcomes for ADF personnel who present with mental healthproblems. In view of this, DHSB has developed appropriate guidelines to address the identifieddeficiencies.
AIM
7. The aim of this HD is to provide guidance to health professionals for the clinical andadministrative management of ADF members presenting with a mental health problem.
SCOPE
8. This Directive’s aim will be addressed by discussing the following elements of patientmanagement:
a. Clinical management. The evaluation and treatment of clinical and subclinical mentalhealth problems in a military setting is addressed in paragraphs 21. to 27. Theevaluation and treatment of specific mental disorders that are of particular concernwithin the ADF population is contained in the remainder of the 260 series of HDs, witheach addressing a particular disorder.
b. Administrative management. Administrative management may include assignment ofan appropriate Medical Employment Classification (MEC) to a member with relevantemployment and deployability restrictions being noted. The process is introduced in thisHD, but each disorder is addressed separately in ensuing health directives.
c. Personnel management. The issue of liaison with Commanding Officers (CO), who willfrequently be required to take some form of responsibility for the immediate and ongoingmanagement of a member with a mental health problem or disorder, is discussed inparagraphs 30. to 32.

3
Defence FOI 553/20/21 Item 1 Document 6
DEFINITIONS
9. The following definitions are offered:
a. Mental Health Problem(s). A term that refers to a range of more common mentalcomplaints. It includes reactions to life stressors that are not necessarily diagnosable(within the normally accepted diagnostic framework), but still impact peoples’ lives andfunctioning.
b. Mental Disorders. These are diagnosable mental health conditions that arecharacterised by alterations in thinking, mood, or behaviour (or some combinationthereof), and are associated with distress and/or impaired functioning.
c. Subclinical. Essentially this means without clinical manifestations, and may be theearly stage of an abnormality before the signs and symptoms become apparent ordetectable by clinical examination. A very mild form of an abnormality can also beclassified as subclinical.
d. Comorbidity. Comorbidity is the presence of coexisting or additional disorders withreference to an initial diagnosis. Comorbidity may affect the ability of affectedindividuals to function, and may be used as a prognostic indicator for such issues aslength of inpatient care, cost factors (associated with treatment, retention or discharge),and clinical outcome.
e. Mental Health Practitioner. The terms Mental Health Practitioner or Mental HealthProvider are applied to the following Defence employed or contracted personnel whoprovide mental health services to ADF personnel on behalf of the ADF:
(1) medical officers, including specialist psychiatrists;
(2) nursing officers;
(3) psychologists;
(4) social workers; and
(5) chaplains.
MENTAL HEALTH MANAGEMENT
General
10. The DSM–IV–TR: APA, 2000, Volume IV, text revision (reference B) is the standard means ofclassifying mental disorders within the ADF. The function of DSM–IV–TR: APA, 2000 is to:
a. provide a consistent and standardised method for classifying signs and symptoms;
b. facilitate communication among mental health professionals, with diagnostic terms inthe manual providing a consistent and standardised means of doing so; and
c. act as a tool for collecting and communicating accurate public health information andstatistics.

4
Defence FOI 553/20/21 Item 1 Document 6
Referral sources
11. An ADF member may present to a mental health provider via, or be presented by, any of thefollowing referral sources:
a. self-referral, where a member may be concerned about the members own symptoms;
b. a Defence medical or dental centre, either as part of a regular health assessment,routine medical appointment or presentation to ‘sick parade’1;
c. the Royal Australian Navy Divisional System;
d. the military chain of command;
e. the ‘All Hours Support Line (ASL)’; or
f. other professions in the Australian Defence Organisation (ADO), such as chaplains,social workers, and psychologists.
Management principles
12. The following principles are to be applied to the management of ADF members who presentwith potential mental health problems.
13. All ADF members are entitled to mental health evaluation. As outlined in paragraph 9., amember may present with a range of physical or psychological mental health symptoms from a varietyof referral sources. Regardless of referral source, all members who present, or are presented, forassistance are to be assessed by an appropriately qualified mental health practitioner. The assessmentprocess is discussed in paragraphs 22. to 27. of this HD.
14. No ADF member should be denied access to mental health treatment. Once a mentalhealth problem has been identified, all serving members are entitled to mental health treatment servicesthat are responsive, accessible, orientated to the needs of ADF personnel and integrated with generalhealth care (reference C). No member should be denied treatment due to:
a. the member’s own fear of being pejoratively labelled, or in any way stigmatised ordiscriminated against;
b. pressure from work to continue to perform at full capacity regardless of the member’smental health problem(s); or
c. employment and deployment consequences.
To assist members who may be reluctant to either seek advice or proceed with treatment, the ADFMHSweb site (see www.defence.gov.au/dpe/dhs) has been designed to demystify mental health and toencourage members to ask for assistance.
15. The establishment of the ASL may also assist in easing access to services and destigmatisingand demystifying mental health support.
1 A medical officer, dental officer, nursing officer, physiotherapist or medical assistant can identify mentalhealth symptoms that require assessment and opinion.

5
Defence FOI 553/20/21 Item 1 Document 6
16. Early intervention and appropriate management of mental health problems will providethe best health outcome for the individual, the family, coworkers and the ADF. The level of serviceprovided should incorporate the principles of best practice. Table 1 outlines the level of serviceappropriate when symptoms of a mental health problem arise in an individual member. The treatmentlevels of Psychological First Aid and Level One will be discussed in HD 261—Prevention of MentalHealth Problems in the Australian Defence Force (to be issued). The remainder of this HD willconcentrate on Levels Two, Three and Four.
Notes
(a) This involves better education of existing ADF members with stress management, suicide prevention andalcohol awareness. In addition, education at a number of training levels is to be introduced so that ADFpersonnel will be exposed to ongoing training throughout the life of their ADF career.
Table 1: Mental Health Treatment Levels for ADF personnel
17. An individual military member cannot be treated or supported independently from theirsocial and personal circumstances. Military life creates unique pressures that affect the individualand family. Therefore, it is essential that families be considered as part of the mental healthmanagement of the member. This can be achieved by families having access to:
a. DCO,
b. chaplains, and
c. any other individual or group provider who has the potential to be of benefit to the family.
Level What When Who
Psychological First Aid(a)
Indicated prevention and early intervention
immediate ALL ADF personnel
Level One Case identification and first aid
hours ChaplainsSocial WorkersDCO Military Support OfficersPsychological ExaminersEEO Contact OfficerMedical AssistantsNursing OfficersMedical OfficersDental OfficersPsychologistsJunior CommandersOthers
Level Two Early treatment days Medical OfficersPsychologistsSocial WorkersPsychiatric NurseChaplains
Level Three Standard treatment months Psychologist with appropriate clinical training and experience.Medical Officer with appropriate clinical training and experience.Psychiatric Nurse with appropriate clinical training and experience.Social Worker with appropriate clinical training and experience.Psychiatrist with appropriate military experience.
Level 4 Expert advice and supervision
ongoing Panel of Senior Specialists with relevant professional and military experience.

6
Defence FOI 553/20/21 Item 1 Document 6
18. A holistic approach to treatment should be facilitated through the professional networkembodied in ADF multi-disciplinary Regional Mental Health Teams. An initiative of the ADFMHShas been the establishment of a multidisciplinary collaboration between the ADO, individual membersand all levels of mental health service provision. ADF Regional Mental Health Teams (RMHT) havesubsequently been established in each ADF area. These teams:
a. facilitate access to the most appropriate services for ADF personnel;
b. are cost-effective and avoid duplication of services;
c. promote mental wellbeing;
d. facilitate early identification and intervention;
e. are governed by common doctrine;
f. have centralised support and direction;
g. provide a peer review capability; and
h. conform to privacy and confidentiality requirements.
19. The composition, roles and tasks of RMHT are the subject of a draft DI(G) Australian DefenceForce Regional Mental Health Teams. RMHT are to collaborate with Directorate of Mental Health (DMH)to ensure that policy and best practice guidelines are being applied in each area.
20. Treatment should be based on both best practice and evidence-based clinical practice.Evidence-based practice is an approach to health care wherein health professionals use the bestevidence possible; that is, the most appropriate information available, in order to make clinical decisionsfor individual patients. This approach values, enhances and then builds upon clinical expertise, and alsoenhances a provider’s knowledge of illness mechanisms and pathophysiology. It involves complex andconscientious decision making based not only on the available evidence but also on patientcharacteristics, situation and preferences. Finally, such treatment recognises that health care needs tobe individualised, fluid, and involves uncertainties and probabilities.
21. Whenever possible, evaluation and treatment at or near the member’s unit is thepreferred first line of management. Whether the situation is a crisis or a clinical/subclinicalpresentation, the initial contact person must respond swiftly and sympathetically. By remaining close toknown health practitioners and personal support systems, the member may feel safer and be more likelyto accept help. However, it is also important to recognise that, in some cases, immediate referral to aspecialist area or person away from the member’s normal geographical location may be required,eg hospital (civilian or Service), Alcohol Rehabilitation and Education Program, psychiatrist or clinicalpsychologist. If this is the case, the member should be reassured that both personal safety and mentalwellbeing are of the utmost importance and remain a primary health priority. At this stage, it is alsoessential that family support mechanisms be put into place to assist the member and family to adjust to,and cope with, the member’s absence and treatment plan.
22. In areas of deployment, at sea or remote localities, unless psychological assets aredeployed, the principles of ‘Psychological First Aid’ as outlined in HD 261 (to be issued) will needto be applied. Thereafter, when the member can be repatriated, appropriate mental health managementwill be conducted in a facility most suited to the member’s requirements eg own medical unit, externalfacility or organisation.

7
Defence FOI 553/20/21 Item 1 Document 6
CLINICAL MANAGEMENT
23. Preliminary assessment and evaluation. In order to identify those members who requirefurther mental health evaluation and some form of treatment, the following personnel should be trainedto administer and evaluate a preliminary screening mental health questionnaire (the Mental HealthScreen) during a structured interview setting:
a. mental health practitioners,
b. senior medical assistants, and
c. psychological examiners.
The content of the Mental Health Screen, along with instructions for its administration and interpretationis found in HD 262—Administration of the Mental Health Screen (to be issued). Mental Health Screenresults may indicate that a patient needs to move along to the next step in the assessment process; thatis, referral to a suitably trained mental health practitioner for further evaluation, assessment and/ortreatment.
24. Even at the earliest stages of assessment and evaluation, if a mental health problem can beidentified, be it clinical or subclinical, the member should be reassured that mental health problems are:
a. common, thereby reducing any concerns about stigmatisation;
b. generally responsive to effective treatment;
c. addressed in a step-wise manner using best practice methods; and
d. treated in a confidential setting.
Often these facts are enough for a member to both accept ownership of their symptoms and embark onformal mental health treatment. This reassurance is particularly powerful when delivered by personnelwho are already known to the patient, eg a trusted medical officer, nursing officer or chaplain.
25. Advanced assessment, evaluation and treatment. As indicated above, when the MentalHealth Screen indicates that further assessment or treatment is warranted, the patient is to be referredto a suitably trained mental health practitioner. At the conclusion of this more advanced assessment,the practitioner should be able to offer an appropriate treatment plan, or may decide that referral formore specialised assessment and opinion or treatment is necessary (for example, forneuropsychological assessment and rehabilitation recommendations). At this stage, additionalconsultation, advice and treatment may also be sought from, or provided by, any of the following:
a. liaison with a member’s work supervisor and/or CO;
b. the Military Compensation and Rehabilitation Service (MCRS);
c. Transition Management Services;
d. the Department of Veterans’ Affairs (DVA);
e. the Vietnam Veterans’ Counselling Service; and
f. any other service provider whose expertise has been demonstrated to be effective andefficient.
26. Any treatment offered to a patient should be planned on an individual basis, but may include:
a. counselling (individual and family);
b. behaviour therapy;
c. cognitive behaviour therapy;
d. psychotherapy;
e. pharmacotherapy;

8
Defence FOI 553/20/21 Item 1 Document 6
f. inpatient programs;
g. outpatient programs; and
h. support groups.
27. The procedures outlined in paragraphs 23. to 26. should apply regardless of whether themember is presenting for the first time with a mental health problem or with a recurrence of a pre-existingproblem.
28. Medications. The prescribing of, and maintenance of prescription documentation for, anypsychotropic medication is to be in accordance with extant health policy. Specific medications will be thesubject of health directives related to each specific disorder. Procedures for the issue of emergencyprescriptions are also to be in accordance with extant health policy.
29. Reserve members. Reserve member entitlements for assessment and treatment of mentalhealth conditions related to their military service are articulated in DI(G) PERS 16–1.
30. Specialist employments. Where necessary, the following categories of specialistemployment will be dealt with separately in each HD:
a. aircrew,
b. divers,
c. submariners,
d. air traffic controllers,
e. ground defence, and
f. special forces.
ADMINISTRATIVE MANAGEMENT
31. General. The member’s Medical Officer should not only be the primary caregiver but shouldalso manage any medical administrative matters that arise. Essentially, this will mean that the MedicalOfficer takes on a case manager function, with input provided from other relevant mental health carepractitioners. Liaison with the Senior Medical Officer may also be required for general advice, incomplicated cases, or when a second opinion is required.
32. MEC and deployability. When a member presents with a mental health problem, the MedicalOfficer should, in consultation with other mental health practitioners involved in the case, make anassessment as to the member’s current deployability, prognosis and consequent appropriate MEC.General guidelines as to appropriate MEC are provided in the specific HD for each disorder. However,attention is drawn to extant policy, HD 236—Medical Employment Classification Procedures for generalguidance regarding assignment of a MEC to an ADF member.
PERSONNEL MANAGEMENT
33. Mental health is a command responsibility, and mental health intervention in the militaryenvironment aims to contribute to the operational effectiveness of personnel. Commanders are notexpected to treat a member in any health professional capacity, however, ‘treatment of the situation’ isessential. Essentially, this means that commanders need to be cognisant of any special workplaceconsiderations that may apply to their member, and the expected duration of those changes/considerations. For example, commanders will need to understand what work restrictions may be placedon the member. Mental health providers should, similarly, have a full understanding of the member’sworkplace, how that workplace can help or hinder treatment, and also how any employment restrictionscan impact the workplace and therefore the member.

9
Defence FOI 553/20/21 Item 1 Document 6
34. Commanders should feel confident in referring a member for mental health evaluation. Unlikea medical referral between health professionals, a CO is not expected to make any subjective commentson a member’s mental health status. However, the CO should complete a Form PM 008—Report on aCase Referred for a Psychiatric or Psychological Examination and forward it to the medical officer orpsychologist. It is vital that the member is aware of the reason(s) for referral, and therefore the membershould be advised as to the nature of the referral, and why the referral has been made.
35. It is important to develop a solid relationship between mental health professionals,commanders and ADF members. Part of the role of the RMHT will be to liaise with command, and thusdemystify the process of mental health evaluation and treatment. Command will benefit from educationregarding the nature of mental health problems, and one of the functions implicit in the ADFMHS iseducation of command at all levels.
REHABILITATION AND SEPARATION FROM THE AUSTRALIAN DEFENCE FORCE
36. Most members will make a full recovery from their mental health problem. However, somemembers will not recover within the time frame dictated by extant health policy and will therefore needto be discharged from the Services. Other members may elect to take discharge regardless of theirMEC.
37. Members being discharged from the military on the grounds of invalidity, for a mental healthdisorder, require more intensive management than those separating routinely at their own request. Infact, the military may be discharging people into civilian society who may lack the requisite abilities tofunction effectively within that society. Furthermore, separation following diagnosis of a chronic orintractable mental health condition often leaves the member with a number of additional problems:
a. inability to find or maintain remunerated employment;
b. likelihood of poor social and economic circumstances;
c. social isolation;
d. stigmatisation;
e. perception of being discharged unfairly by the organisation, and the oftenaccompanying perception of disloyalty being shown by the organisation towards themember; and
f. impairments in areas of functioning such as:
(1) self-care;
(2) self-direction;
(3) interpersonal relationships;
(4) learning and recreation; and
(5) independent living.
38. These sequelae will significantly hamper the resolution or management of the primarycondition unless strategies are in place to mitigate such additional problems. Strategies for such casesshould aim at:
a. focussing on improving patient capabilities, competencies, and maximising health;
b. improving the patient’s ability to adjust and adapt to their environment;
c. improving vocational outcomes, such that the patient can enter the paid workforce andgain the positive outcomes of such involvement;
d. actively involving the patient in their own transition management, such that the patientviews him/herself as a stakeholder, not someone who is having something done tothem; and
e. ensuring that appropriate evaluation and follow-up is built into the specific strategy.


DIRECTOR–GENERAL DEFENCE HEALTH SERVICE
Defence FOI 553/20/21 Item 1 Document 7
HEALTH BULLETIN NO 12/2003Note: Director-General Defence Health Service Health Bulletins are produced to disseminate HealthInformation. They are to be filed in a separate binder, readily accessible to all staff. They remain in effectuntil cancelled in accordance with instructions in the Bulletin. Publications can be accessed on theDefence Intranet at http://defweb.cbr.defence.gov.au/home/documents/adfdocs/healthindex.htm
19 AUGUST 2003
CRITICAL INCIDENT MENTAL HEALTH SUPPORT PROGRAM
INTRODUCTION
1. A crisis or traumatic event that has a stressful impact sufficient to overwhelm the usuallyeffective coping skills of either an individual or a group is known as a ‘critical incident’ (CI) or ‘potentiallytraumatising event’ (PTE). These incidents are typically sudden and powerful events outside the rangeof ordinary human experiences, and can overwhelm even well trained and experienced people, either atthe time or later on.
2. Due to the nature of Australian Defence Force (ADF) work and training, the likelihood ofpersonnel being involved in a CI or PTE, both in peacetime and during operations, is greater than in mostcivilian occupations. The provision of Critical Incident Mental Health Support (CMS) is therefore afundamental part of the ADF’s recognition of, and response to, such incidents. CMS is also part of abroad suite of responses that can be provided in an operational area; Australian Defence ForcePublication 714—Operational Stress Management provides a more complete description of the types ofresponses that can be provided in the operational environment.
3. CMS refers to a process of intervention with individuals who have been involved, either directlyor indirectly, in a CI or PTE. CMS is a mental health initiative that sits within a broad framework that aimsto promote strategies for individuals and groups to mitigate and alleviate possible psychological injuriesfollowing a CI or PTE. CMS is designed to bolster personal resources in order for personnel to maintainperformance throughout incidents, or to return to duty and perform to their full capacity as quickly aspossible.
4. Stress management is a command responsibility, but specialist assets are available tocommanders to assist them in the maintenance of the mental health of their personnel. CMS is designedto augment existing personnel support services.
AIM
5. The aim of this Health Bulletin (HB) is to detail the ADF policy for the management of personnelinvolved in CI or PTE. In an operational context, this Bulletin should be read in conjunction with the HB—Mental Health Support to Operationally Deployed Forces. This HB will become a Defence Instruction(General).
DEFINITIONS
6. For the purpose of this HB, the following definitions apply:
a. Critical Incident (CI). A CI is an incident that can both evoke unusually strong emotionalreactions and have the potential to interfere with the ability of personnel to functionappropriately. These incidents are outside the range of usual experience and mayinclude, but are not restricted to, traumatic events. It is the unique context in whichincidents occur, and the potential for strong negatively perceived emotional reactions bypersonnel involved, that determine whether incidents are critical. An example of a CIcould be where a suicide has occurred and the workplace or deceased person’s friendsare strongly and negatively impacted by the death.

2
Defence FOI 553/20/21 Item 1 Document 7
b. Potentially Traumatic Event (PTE). A PTE usually involves personnel havingexperienced, witnessed, or being confronted with an event or events that involvedactual or threatened death or serious injury, or a threat to the physical integrity of selfor others. An incident is only considered traumatic if the reactions of the personnelincluded intense fear, helplessness and horror. An example of a PTE could be where aperson finds the body of someone who has suicided.
c. Mental Health Professional. The term Mental Health Professional is applied to thefollowing Defence employed or contracted personnel who provide mental healthservices to ADF personnel on behalf of the ADF:
(1) medical officers, including specialist psychiatrists;
(2) nursing officers;
(3) psychologists;
(4) social workers; and
(5) chaplains.
d. CMS Team. A specifically trained and formed team that is capable of complementinglocal resources in the provision of specialist services following a CI or PTE. The CMSTeam Leader will, in most cases, be a psychologist; however, in locations where apsychologist is unavailable, the Team Leader will be the most senior CMS provideravailable. Director Defence Force Psychology Organisation (DFPO), will nominate allTeam Leaders.
e. Levels of service providers. The CMS framework is multidisciplinary, and involveslayers of CMS providers based on their professional background and level of CMStraining. Descriptions of levels of service provision can be found in annex A to this HB.
MANAGEMENT OF CRITICAL INCIDENT MENTAL HEALTH SUPPORT IN THE AUSTRALIAN DEFENCE FORCE
7. Director DFPO is responsible for coordinating tri-Service CMS management, which includes:
a. policy;
b. training development, delivery and accreditation;
c. availability of trained personnel;
d. operations;
e. funding and resources allocation; and
f. quality assurance.
OVERVIEW OF CRITICAL INCIDENT MENTAL HEALTH SUPPORT FRAMEWORK
8. The major elements of the ADF CMS framework are:
a. preincident education and preparation for personnel management aspects of CI or PTE;
b. assessment of the potential impact of a CI or PTE upon the effectiveness and efficiencyof individuals and military units;
c. psychological first aid for those with acute psychological injuries;
d. mental health surveillance and case identification of those considered at risk ofdeveloping chronic psychological injuries;
e. appropriate treatment or referral for those displaying early signs of potential chronicpsychological injuries, with the aim of preventing development into chronic conditions;

3
Defence FOI 553/20/21 Item 1 Document 7
f. education aimed at:
(1) improving self-management, both at unit and individual levels, following a CI orPTE;
(2) assisting self-identification and self-referral for personnel at risk of developingpsychological injuries; and
(3) maximising treatment/management acceptance, compliance and effectiveness.
g. awareness programs on stress and psychological injuries following CI or PTE;
h. provision of formally trained CMS Teams to supplement local resources; and
i. support for spouses and families.
9. The major principles of ADF CMS are:
a. strong engagement and consultancy with command at all levels during all stages ofCMS delivery;
b. recognition that unit members have a significant part to play in the successfulmanagement of a CI or PTE, and that individual service members are responsible formaking a positive contribution to their own mental health;
c. provision of a flexible, multidisciplinary approach to mental health promotion andmaintenance, and to deliver effective early mental health interventions following a CI orPTE;
d. effective management of chronic post-traumatic pathology (this involves early caseidentification and treatment of acute conditions); and
e. maximising resilience through effective social support and appropriately indicated andtargeted prevention strategies.
10. Whilst CMS is based upon an assumption of normal recovery for the majority of individualsfollowing the majority of events, CMS provides for immediate interventions based around containmentof symptoms and support of the individual, as well as referral for psychological or psychiatric treatmentwhen indicated.
11. CMS provides a flexible phased structure designed to allow the CMS provider (in conjunctionwith command) to select and implement CMS interventions according to the circumstances of thepersonnel, the unit and the event. A full description of each CMS phase is contained in annex B.
12. Although CMS is an ADF framework, there will be potentially traumatising or critical incidentsthat include ADO civilians, families and the general community. The guidelines for such groups arecontained in annex B. Reservists should be included in all stages of CMS for any event that hasoccurred in relation to their military service.
CRITICAL INCIDENT MENTAL HEALTH SUPPORT TEAM MEMBERS
13. Although technical management of CMS is vested in the Director DFPO, any Defenceemployed personnel who has undertaken appropriate ADF CMS training can be employed in CMSactivities according to subparagraph 5.e.
14. The aim is for each Defence area or unit to have access to an appropriately trained CMSTeam. CMS support to establishments and bases will be coordinated by Regional Mental HealthTeams (RMHT), and CMS support to deployed units will be coordinated from command specific CMSTeams. Each region has a RMHT, and a member of that RMHT is a regional CMS coordinator(appointed by Director DFPO). The CMS coordinator, with the remainder of the RMHT, facilitatesdelivery and integration of CMS services within their area of responsibility. It is recognised some areaswill have limited personnel, and that some of those CMS trained personnel may be personally involvedin an incident. When this is the case, DFPO staff can, through liaison with the local CMS provider andother areas of command, assist in allocating assets from other regions.

4
Defence FOI 553/20/21 Item 1 Document 7
CRITICAL INCIDENT MENTAL HEALTH SUPPORT TEAM LEADER RESPONSIBILITIES
15. The CMS Team leader for each region is appointed by the Director DFPO, in consultation withother CMS stakeholders. The CMS Team leader has the following responsibilities:
a. Development and coordination of a local CMS plan in conjunction with other regionalmental health assets and command.
b. Integrating and maintaining CMS planning in local area emergency planning.
c. CMS plans are to be revised annually and staffed through Director DFPO for inclusionin the national plan.
d. When approved by Director DFPO, plans are to be promulgated to all units within thelocal area.
e. Developing, training and exercising CMS teams to maintain preparedness. There is tobe an annual exercise of CMS procedures in each area.
f. Establishing and maintaining local access, callout and operational arrangements (forworking hours and out-of-hours).
g. Promoting CMS and wider mental health education and awareness.
CRITICAL INCIDENT MENTAL HEALTH SUPPORT TEAM FUNCTIONS AND ROLES
16. The roles and functions of CMS teams are:
a. to work in conjunction with RMHT to prepare Service personnel to manage their stressand understand the range of normal responses to a CI or PTE (this is part of mentalhealth literacy); and
b. to assist Service personnel who are experiencing the negative or debilitating effects ofexposure to a CI or PTE. This includes liaison and consultancy with Command, thedelivery of an appropriate CMS response and referral to other service providers asnecessary.
ACTIVATION OF CRITICAL INCIDENT MENTAL HEALTH SUPPORT TEAM
17. The single Services are responsible for establishing call-out procedures appropriate to theirsingle Service needs. However, in general, CMS teams will be activated following a request from aCommanding Officer (CO) or delegate, or on occasion by higher authority and on approval from theappropriate headquarters. Requests for CMS activation should be made directly to the regional CMScoordinator or their representative. Requests for CMS responses should be recognised as only oneaspect of appropriate management of personnel in times of high demand on personal and personnelresources. Activation should normally occur as soon as practicable after the incident, usually in the firstday following an incident. Where possible, notification of possible call-out should be considered to allowCMS personnel to be placed on standby, and to commence preliminary activity arrangements. Thefollowing incidents are offered as a guide to when activation should be considered:
a. line of duty and non-duty death;
b. rescue and casualty incidents involving exposure to gruesome sights, including bodyrecovery etc;
c. significant events where there is personal identification with victims and theircircumstances;
d. training accidents and 'near misses';
e. prolonged involvement in incidents or activities with potential danger;

5
Defence FOI 553/20/21 Item 1 Document 7
f. overseas deployments which involve critical incidents, eg accidents/incidents in ships/units/formations on deployment;
g. natural disasters; and
h. any combination of the above or any incidents deemed by a CO, or delegate, to becritical or potentially traumatic, or to have a potentially significant negative effect onpersonnel.
Where doubt exists as to the requirement of a CMS intervention, consultancy with CMS providers isstrongly recommended.
18. Documentation to be completed for call out is in annex C.
CRITICAL INCIDENT MENTAL HEALTH SUPPORT EDUCATION AND TRAINING
19. Training sponsor. The training sponsor for all CMS training is Director DFPO. All CMStraining is to be undertaken according to DFPO training guidelines, with only DFPO accredited trainersdelivering such training. Director DFPO is therefore responsible for both training and accreditation.
20. General. There are three types of training relevant to the CMS program:
a. enhanced general mental health literacy for the ADF population;
b. CMS awareness training; and
c. specialist CMS program training.
21. Enhanced mental health literacy. This is a primary aim of the ADF Mental Health Strategyand encompasses ongoing awareness training for all members. Education can include:
a. stress identification and management education;
b. the nature of a CI or PTE, and its potential impact on family and/or friends;
c. substance misuse education;
d. general health promotion education; and
e. suicide awareness and risk education.
22. CMS awareness training. CMS awareness training will be provided to all ADF membersthroughout their Service career. This training will be conducted by suitably CMS qualified and trainedADO mental health professionals. It is to cover a summary of CMS policy, principles and proceduresand will be provided to the following courses:
a. all initial entry officer training courses;
b. promotion courses for Leading Seaman (E) and above;
c. single Service command and precommand courses;
d. tri-Service Command and Staff training;
e. medical assistant and psychological examiner courses; and
f. other courses and ad hoc training as requested.


7
Defence FOI 553/20/21 Item 1 Document 7
Annexes: A. Levels of Critical Incident Mental Health Support Service ProvidersB. Critical Incident Mental Health Support PhasesC. Critical Incident Mental Health Support Call–Out Form
DISTRIBUTION: DHS
SPONSOR: DMH
EARLIER HEALTH BULLETIN CANCELLED: Nil

ANNEX ADefence FOI 553/20/21
Item 1 Document 7
LEVELS OF CRITICAL INCIDENT MENTAL HEALTH SUPPORT SERVICE PROVIDERS
1. For the purpose of this Health Bulletin the following Critical Incident Mental Health Support(CMS) levels apply:
a. Level One—Mental Health Literacy. Individual Australian Defence Force (ADF)personnel have primary responsibility for their own mental health. ADF members andtheir commanders will be provided with education to assist with mental health self-careand the care of others. Specialist CMS awareness training will be provided to all ranks.
b. Level Two—Primary Referral or Identification. At this level are personnel with basicCMS awareness training. This level recognises that some trained non-mental healthprofessionals at the scene of a CI or PTE are often in the best position to:
(1) identify personnel experiencing mental health problems,
(2) advocate for such personnel,
(3) facilitate access to appropriate referral sources,
(4) provide unit liaison with CMS Teams, and
(5) provide appropriate basic CMS advice to both command and personnel.
c. This level can include Senior Medical Assistants, Psychological Examiners, Chaplains,Nurses, Military Liaison Officers, and trained CMS advisers.
d. Level Three—Psycho-education and Basic Prevention. At this level are non-mentalhealth personnel with basic mental health management skills. In addition to the servicesof Level 2 providers, Level 3 providers undertake basic psycho-education, prevention,psychological first-aid, and assist higher level providers in facilitating more specialisedCMS interventions (including screening of personnel). This level includes appropriatelytrained Senior Medical Assistants and Psychological Examiners, Chaplains, andNursing Officers.
e. Level Four—Primary Mental Health Care by generalist mental healthprofessionals. Level 4 providers work in CMS Teams to deliver CMS specificinterventions (including psychological first aid, screening, assessment and referral asrequired), supervision of lower level providers and, when accredited, provide CMStraining. This level health and mental health personnel with professional (tertiary)qualifications, but not necessarily with specialist skills or great experience in traumamanagement (ie medical practitioners, psychologists, social workers and some nursingand chaplaincy staff).
f. Level Five—Secondary Mental Health Care. This level recognises that specialistskills, training and experience may be required to effectively diagnose, treat andmanage trauma responses. The aim is to prevent or minimise the possible long termdebilitating effect of trauma. Within the ADF, psychiatrists, and senior psychologists,nursing officers, medical practitioners and social workers who have clinical mentalhealth training, provide this level of service. These providers also assist and support theLevel 2, 3 and 4 providers.
g. Level Six—Tertiary Mental Health Care. This level recognises the need forprofessionals with specialist clinical skills and qualifications to deal with more complexand severe mental health issues following trauma, and to provide clinical supervision toother service providers. Service providers at this level include mental healthpractitioners with the advanced qualifications, skills and experience to provide clinicalsupervision (ie psychiatrists and clinical psychologists).

ANNEX BDefence FOI 553/20/21
Item 1 Document 7
CRITICAL INCIDENT MENTAL HEALTH SUPPORT PHASES
General
1. In general Critical Incident Mental Health Support (CMS) is designed to:
a. provide a high-level of flexibility to accommodate the vast array of incidents andcircumstances that may occur within the Australian Defence Force (ADF), from thedeath of a colleague on base through to personnel exposed to a situation which presentsextreme threat;
b. include extensive and ongoing liaison with Command;
c. include a process by which the provider assesses the needs, provides first lineintervention, reassesses and provides further intervention when necessary, orreassesses and refers to a qualified mental health practitioner (ie when specialisttreatment is needed);
d. include follow-up and ongoing care for individuals;
e. maximise existing support mechanisms;
f. not force individuals into unusual and potentially harmful modes of coping;
g. screen for protective and risk factors;
h. screen for chronic problems;
i. provide appropriate intervention for all ADF personnel, including Reservists;
j. allow for Australian Defence Organisation members to be involved in initial phasesbefore referral to appropriate civilian services; and
k. include the coordinated support to families through the inclusion of Defence CommunityOrganisation (DCO) and Chaplaincy.
2. CMS offers the following four phases:
a. Planning and Immediate Response;
b. Psycho-education and Screening;
c. First Follow-up; and
d. Second Follow-up.
Phase One—Planning and Immediate Response
3. The planning element of Phase One for the CMS provider includes:
a. liaison with command,
b. information gathering,
c. assessment of need for intervention by determining how potentially traumatising theevent was, and
d. planning initial intervention and determining required resources.
This element is conducted as soon as possible after a call out has been received.

B–2Defence FOI 553/20/21
Item 1 Document 7
e. The immediate response element can be conducted either individually or in smallinformal groups and includes:
(1) ensuring affected members receive adequate rest;
(2) removing affected members from the worst of the stress (if possible);
(3) reassuring members and command;
(4) psychological first aid; and
(5) psychological consultancy and liaison.
Phase Two—Psycho-education and Initial Screening
4. Phase Two has the following three options:
a. Option One. No response required at this time. This decision is made by the CMSprovider in consultation with local command, and is based on a thorough assessment ofthe event(s) and responses to the event(s).
b. Option Two. Psycho-education and Initial Screening. The function here is:
(1) provision of quality psycho-education;
(2) brief non-invasive screening and psychological triage;
(3) provision of specific psychological first aid techniques;
(4) referral of those individuals identified as requiring further assistance; and
(5) further planning.
This can be completed either on an individual basis or in a group format, dependent upon theoperational requirements of the time. This option is conducted when the events were assessedas potentially traumatising.
c. Option Three. This consists of psychological support and consultancy to unit activitiessuch as memorial services, ritual ceremonies, command briefings, informal groupdiscussions, planned support meetings for personnel and/or their families or any othergroup support scenario. Such interventions are voluntary and are both initiated andcontrolled by the unit or group themselves (with consultancy provided by CMSpersonnel). Their use is indicated when:
(1) significant loss was involved in the event,
(2) there is a lack of knowledge,
(3) there are different perceptions and rumours persisting, and
(4) command identifies problems with group cohesion.
Phase Three—First Follow-up
5. This phase is individually based and conducted approximately one week after the initial screenin Phase One. It is targeted at all personnel who completed initial screening. Its function is to:
a. screen for and triage acute psychological injuries (such as Acute Stress Disorder), asdistinct from expected and transient distress; and
b. provide appropriate psychological treatments and management advice for personneldisplaying acute psychological injuries.

B–3Defence FOI 553/20/21
Item 1 Document 7
Phase Four—Second Follow-up
6. This is completed approximately three months after the initial screen and is individually based.It is aimed at determining whether any ongoing adjustment difficulties are present. It also functions to:
a. screen for, and triage chronic psychological injuries; and
b. provide appropriate psychological treatments and management advice for personneldisplaying chronic psychological injuries.
Guidelines for Australian Defence Organisation Civilians, Families and the General Community
7. Guidelines for the above populations are:
a. Within the CMS framework any individual at the scene of the event/incident is includedin the initial phase of the CMS response.
b. Work groups may be included in the psycho-educational phases, but formal screening,and mental health care, of civilians (including Defence civilians) is not undertakenunless there is formal and approved Defence Assistance to the Civil Community tasking.
c. Work groups should be considered when planning rituals or memorials.
d. Families at all times can seek assistance from DCO or a chaplain.
e. Defence civilians can be encouraged to seek assistance from their local DefenceEmployee Assistance Program (EAP) provider, general practitioner or communitymental health service.
f. Members of the community can seek assistance from their general practitioner andcommunity mental health services. They may also be eligible for government-fundedvictim’s counselling or their employer may have an EAP.

ANNEX CDefence FOI 553/20/21
Item 1 Document 7
CRITICAL INCIDENT MENTAL HEALTH SUPPORT CALL–OUT FORM1
1 To be completed by both requesting unit and Critical Incident Mental Health Support Team Leader.
Ship/Unit/Base:Service:Requesting officer:Requesting officer contact details:Date of contact:Date of incident:
1. Location of the incident:
2. The Ship/Units/Base involved:
3. A brief description of the incident:
4. Did the incident involve any of the following (Yes/No)?
a. line of duty death?
b. non-duty death?
c. rescue and casualty incidents involving exposure to gruesomesights, including body recovery?
d. general accident, training accident or near miss ?
e. natural disaster?
f. exposure to a noxious agent?
g. severe physical harm or injury?
h. other (explain)?

C–2Defence FOI 553/20/21
Item 1 Document 7
5. Extent of any injuries involved:________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
6. Details of those involved in the incident:______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
7. Current location of these personnel:________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
8. Current status of incident:________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
9. When personnel will be available for CMS:________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
10. Whether any personnel involved are required to return to anotherlocation. If so, details of their movements are required:________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
11. The status of any investigation into the incident:________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
12. The extent of media interest in the incident:________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Action Required (to be completed by CMS provider with Commandinput)
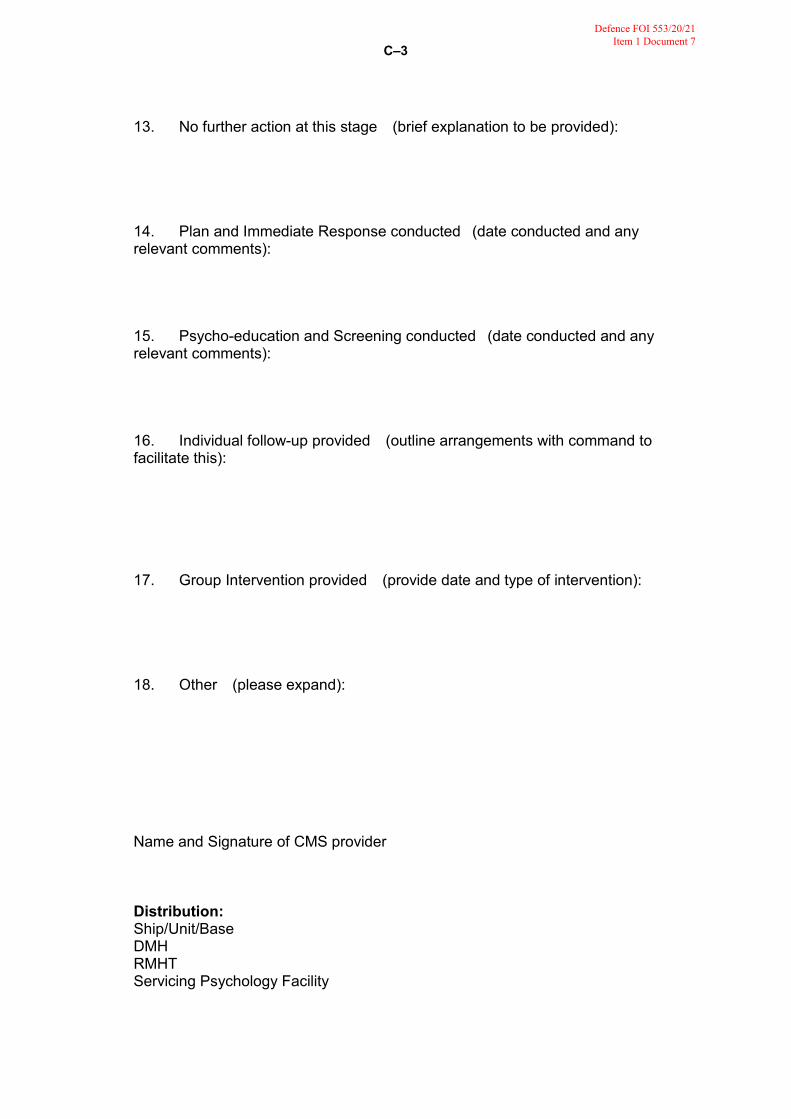
C–3Defence FOI 553/20/21
Item 1 Document 7
13. No further action at this stage (brief explanation to be provided):
14. Plan and Immediate Response conducted (date conducted and anyrelevant comments):
15. Psycho-education and Screening conducted (date conducted and anyrelevant comments):
16. Individual follow-up provided (outline arrangements with command tofacilitate this):
17. Group Intervention provided (provide date and type of intervention):
18. Other (please expand):
Name and Signature of CMS provider
Distribution:Ship/Unit/BaseDMHRMHTServicing Psychology Facility


Defence FOI 553/20/21 Item 2 Document 1
© Commonwealth of Australia 2002
This work is copyright. Apart from any use as permitted under the Copyright Act 1968, no part may bereproduced by any process without prior written permission from the Department of Defence.
Announcement statement—may be announced to the public.
Secondary release—may be released to the public.
All Defence information, whether classified or not, is protected from unauthorised disclosure under theCrimes Act 1914. Defence information may only be released in accordance with the Defence ProtectiveSecurity Manual (SECMAN 4) and/or Defence Instruction (General) OPS 13–4—Release of ClassifiedDefence Information to Other Countries, as appropriate.
Requests and inquiries should be addressed to the Director, Defence Publishing Service, CP3–1–102,Department of Defence, CANBERRA ACT 2600.
ABR 6303
First edition 1998Second edition 1999Third edition 2002
NCELLED
Sponsor
Director-General Navy Certification, Safety and Acceptance Agency
Developer
Director Navy Safety Systems
Publisher
Defence Publishing ServiceDepartment of DefenceCANBERRA ACT 2600
Defence Publishing ServiceDPS: January 2002



ABR 6303vii
Defence FOI 553/20/21 Item 2 Document 1
AMENDMENT CERTIFICATE
Proposal for amendment/notification of error of ABR 6303 are to be forwarded to:
Director Navy Safety SystemsCP4–6–099Department of DefenceCANBERRA ACT 2600
Amendment Effected
No Date Signature Date
NCELLED

ABR 6303ix
Defence FOI 553/20/21 Item 2 Document 1
CONTENTSPage
Authorisation iiiAmendment Certificate viiList of Figures xiiiList of Tables xv
Paragraph
CHAPTER 1 NAVSAFE—NAVY’S SAFETY MANAGEMENT SYSTEM
INTRODUCTIONObjective 1.1
LEGISLATIVE REQUIREMENTSOccupational Health and Safety (Commonwealth
Employment) Act 1991 1.4
AUSTRALIAN DEFENCE FORCE SAFETY POLICYDefence Safety Management Agency 1.8Group Executives 1.9
NAVY SAFETY POLICYIssuing Authority 1.10Navy safety requirements 1.11
NAVSAFE OVERVIEWApplicability 1.13Objectives and requirements of NAVSAFE 1.14Components of the NAVSAFE system 1.16Implementation 1.17
Annexes:A. Navy Safety Managemen System (NAVSAFE) principles and
elementsB. The NAVSAFE system
CHAPTER 2 NAVSAFE DUTIES AND RESPONSIBILITIES
ROYAL AUSTRALIAN NAVY CORPORATE SAFETY MANAGER
DIRECTOR–GENERAL NAVY CERTIFICATION, SAFETY AND ACCEPTANCE AGENCY
Role 2.2Tasks 2.5
MARITIME COMMANDER AUSTRALIARole 2.6Tasks 2.7
COMMANDER AUSTRALIAN NAVY SYSTEMS COMMANDRole 2.8Tasks 2.9
FORCE ELEMENT GROUP COMMANDERSRole 2.10Tasks 2.11
DEFENCE SERVICE PROVIDERS
ROYAL AUSTRALIAN NAVY SAFETY COUNCIL AND SAFETY BOARDS
RAN Safety Council 2.13Safety Boards 2.14Safety Management Group 2.16
Annexes:A. Royal Australian Navy Safety Council—Terms of ReferenceB. Royal Australian Navy Safety Boards—Terms of ReferenceC. Roles and Functions of Directorates within Navy Certification
and Safety Agency
NCELLED

ABR 6303x
Defence FOI 553/20/21 Item 2 Document 1
CHAPTER 3 UNIT RESPONSIBILITIES
RISK, OPERATIONS AND SAFETYDefinition 3.1Aim 3.2Safety culture 3.3
SHIP SAFETY MANAGEMENTThe Ship’s Safety Team 3.5Team composition and qualifications 3.7Roles and Functions of the Ship’s Safety Team 3.10Form OS 006—Ships Occupational Health and Safety Log 3.12
PERSONNEL INDUCTION PROCESSESRationale 3.14Requirement 3.15
SAFETY DURING MAINTENANCERationale 3.16Dangers posed during maintenance 3.17Relations with contractors 3.18
INTRODUCTION OF HAZARDOUS SUBSTANCESRationale 3.19Command responsibilities 3.20Material Safety Data Sheets 3.21
ORDNANCE SAFETY MANAGEMENTRationale 3.22Ordnance safety procedures 3.23References 3.24
RADIATION SAFETY MANAGEMENTTypes of hazard 3.25Electromagnetic Radiation safety 3.26Laser safety 3.27References 3.28
SUBMARINE SAFETY MANAGEMENTSUBSAFE purpose 3.29Overview 3.30References 3.32
AVIATION SAFETY MANAGEMENTAIRSAFE purpose 3.33Overview 3.34References 3.36
HYPERBARIC AND DIVING SAFETY MANAGEMENTHYPERSAFE purpose 3.37Overview 3.38References 3.41
ESTABLISHMENT SAFETY MANAGEMENTDuty of Care 3.42Implementation 3.43Service providers and enablers 3.45Designated Work Groups and Health and Safety Representatives 3.51Management of Plant 3.52Ship/Shore interface 3.56
SPORT AND ADVENTUROUS TRAINING
NCELLED

ABR 6303xi
Defence FOI 553/20/21 Item 2 Document 1
CHAPTER 4 PERSONNEL SAFETY AND TRAINING
RESPONSIBILITIESIndividual responsibilities 4.1Management responsibilities 4.2Command responsibilities 4.3
OCCUPATIONAL HEALTH AND SAFETY TRAINING PHILOSOPHYPhilosophy 4.4Guidelines for Occupational Health and Safety Training 4.5Sailor career progression training 4.6Officer career progression training 4.10
OCCUPATIONAL HEALTH AND SAFETY COURSESNavy safety training courses 4.11Royal Australian Navy Ship safety management courses 4.12Civilian ship safety management course 4.13Marine Incident Investigator’s course 4.14
REVIEWSafety Training Review 4.15
CHAPTER 5 NAVSAFE HAZARD AND RISK MANAGEMENT
OVERVIEWRisk management fundamentals 5.1
MAJOR REFERENCESAustralian Standard/New Zealand Standard 4360:1999—Risk
Management 5.2Australian Standard/New Zealand Standard 4804 1997—Occupational
Health and Safety Management System —General Guidelines on Principles, Systems and Suppo ting T chniques 5.3
RISK MANAGEMENT PROCESSESOverview 5.4Risk managem nt terminology 5.7
DESCRIPTION OF THE ELEMENTS OF RISK MANAGEMENTEstablishing the context 5.9Identifying risks 5.15Analysing risks 5.18Evaluating risks 5.20Implementing risk control measures 5.22Monitoring and reviewing 5.28Communication and consultation 5.29Emergency/contingency planning 5.30
OPERATIONAL RISK MANAGEMENTRisk in naval operations 5.31Definition 5.32Aim 5.33Operational Risk Management—six steps 5.35Fundamental principles of Operational Risk Management 5.36
Annexes:A. Hazard assessment—obtaining a Hazard Risk IndexB. Controlling risk—the Hierarchy of ControlsC. Risk management documentationD. Risk management terminologyE. NAVSAFE risk management elements
NCELLED

ABR 6303xii
Defence FOI 553/20/21 Item 2 Document 1
CHAPTER 6 THE SAFETY CASE
OVERVIEWWhat is a Safety Case? 6.1Requirements of Safety Cases 6.4
ELEMENTS OF THE NAVY SAFETY CASECore components 6.7Ship/facility description 6.8Formal Safety Assessment 6.11Hazard identification 6.13Hazard analysis 6.15Hazard evaluation 6.16Hazard controls 6.17Safety management system 6.21Monitoring and feedback measures 6.22Emergency procedures 6.23Safety Case report 6.24Communication plan 6.27
CHAPTER 7 ACCIDENTS AND INCIDENTS
Make safe 7.1Facilitate a thorough investigation 7.2
INCIDENT AND ACCIDENT REPORTING REQUIREMENTSStatutory requirements 7.3Comcare and Defence Safety Management Agency functions 7.5Australian Defence Force reporting requirements 7.7Command responsibility 7.8Defence Report—Form AC 563 7.9
NOTICAS/FATALCASRoyal Australian Navy requirements 7.13Occupational Health and Safety ncident Report. 7.15
INCIDENT INVESTIGATIONBasic Elements 7.21Technique 7.24Purpose of investigation 7.28Witnesses 7.29The facts 7.32The report 7.35Royal Australian Navy marine incident investigators 7.38COMCARE investigation 7.39
Annexes:A. Personnel safety event—checklistB. Occupational Health and Safety Incident Report format
Glossary
Acronyms and Abbreviations
NCELLED

ABR 6303xiii
Defence FOI 553/20/21 Item 2 Document 1
LIST OF FIGURES
Figure Title Page
5–1 Risk management steps 5–25–2 The As Low As Reasonably Practicable Triangle 5–65A–1 As Low As Reasonably Practicable vs Acceptability of Risk 5A–6
NCELLED

ABR 6303xv
Defence FOI 553/20/21 Item 2 Document 1
LIST OF TABLES
Table Title Page
5A–1 Hazard likelihood 5A–25A–2 Hazard Severity (Personnel) 5A–35A–3 Hazard Severity (Equipment) 5A–35A–4 Hazard Severity (Mission) 5A–45A–5 Hazard Risk Index 5A–45A–6 Acceptability of Risk 5A–55B–1 The Hierarchy of Controls 5B–1
7–1 Form AC 563—Incident and Fatality report 7–3
NCELLED

ABR 6303 Defence FOI 553/20/21 Item 2 Document 1
CHAPTER 1
NAVSAFE—NAVY’S SAFETY MANAGEMENT SYSTEM
INTRODUCTION
Objective
1.1 The objective of Australian Book of Reference 6303—NAVSAFE Manual—Navy SafetyManagement (ABR 6303) is to detail the Navy Safety Management system (NAVSAFE) which has beendeveloped to ensure that Navy complies with the following:
a. a moral duty of care to personnel;
b. Commonwealth legislation, especially the Occupational Health and Safety(Commonwealth Employment) Act 1991 (OHS(CE) Act 1991), and associatedregulations;
c. Common Law requirements for safety of personnel;
d. Australian Defence Force (ADF) wide requirements for the management of safety; and
e. key requirements of the International Safety Management Code for Ships1 and otherinternational maritime standards applicable to naval ships.
1.2 These requirements must be met whilst ensuring the Navy operates eff ciently and effectivelywithin a maritime environment.2
1.3 ABR 6303 provides instruction on the process s that will allow managers and supervisors tosecure the highest standard of health and safe y for al personnel, ships, establishments and theirsystems. In addition, this manual describes the sa ety framework, entitled ‘NAVSAFE’, through whichthis policy is implemented throughout the Navy.
LEGISLATIVE REQUIREMENTS
Occupational Health and Safety (Commonwealth Employment) Act 1991
1.4 Navy is bound by the provisions of the OHS(CE) Act 1991. Further, statutory rules have beenissued entitled Occupational Health and Safety (Commonwealth Employment) (National Standards)Regulations [Statutory Rules 1994 No. 414 as amended] which deal with competency standards forusers and operators of industrial equipment, occupational noise, operational plant, manual handling,hazardous substances, confined spaces, storage and handling of dangerous goods, and majorhazardous facilities.
1.5 The objectives of the OHS(CE) Act 1991 are:
a. to secure the health, safety and welfare at work of employees;
b. to protect people at or near workplaces from risk to their health and safety arising out ofthe activities of employees at work;
c. to ensure that expert advice is available on occupational health and safety mattersaffecting employers, employees and contractors;
1 The International Management Code for the safe operation of ships and for pollution prevention adopted by theInternational Maritime Organisation Assembly.
2 Royal Australian Navy (RAN) Doctrine 1 (2000): [Australian Maritime Doctrine] articulates this concept.
NCELLED

ABR 63031–2
Defence FOI 553/20/21 Item 2 Document 1
d. to promote an occupational environment for employees at work that is adapted to theirhealth and safety needs; and
e. to foster a cooperative consultative relationship between employers and employees onhealth, safety and welfare of employees at work.
1.6 The OHS(CE) Act 1991 details the requirements placed upon:
a. the employer in relation to employees;
b. the employer in relation to third parties;
c. manufacturers in relation to plant and substances;
d. suppliers in relation to plant and substances;
e. persons erecting or installing plant; and
f. employees in relation to Occupational Health and Safety (OHS).
1.7 The OHS(CE) Act 1991 also details the way in which safety is to be managed in the workplace,the requirements for accident and incident reporting, and the power conferred upon Comcare toinvestigate, make recommendations, and issue orders (including Improvement notices and Prohibitionnotices).
AUSTRALIAN DEFENCE FORCE SAFETY POLICY
Defence Safety Management Agency
1.8 The safety policy for the Australian Defence Organisation (ADO) is issued by Chief of theDefence Force and Secretary. The Defence Safety Management Agency is chartered with responsibilityfor the formulation and promulgation of safety poli y in the ADO, and provision of services and expertadvice on ADO OHS matters.
Group Executives
1.9 Within the ADF, each Group Executive (Chief of Navy (CN) for Navy) has the responsibility andaccountability to ensure that:
a. appropriate safety management systems and structures are established, for themanagement of hazards that have as core goals the identification, assessment andcontrol of workplace hazards; including consultative mechanisms and preventativeprograms implemented for continual improvement;
b. appropriate documentation is maintained on the safety management systemsestablished;
c. appropriate safety training programs are established;
d. appropriate resources are allocated for the proper management of the safetymanagement systems and programs within their Group;
e. key performance indicators are established that allow for the measurement of theGroup’s safety performance; and
f. the performance levels are reported and included in the Defence Annual Report.
NCELLED

ABR 63031–3
Defence FOI 553/20/21 Item 2 Document 1
NAVY SAFETY POLICY
Issuing Authority
1.10 The safety policy for the RAN is issued by CN. The Navy Safety Policy is reproduced as aforeword to this manual. The Navy Safety Policy will be reviewed for currency by the RAN SafetyCouncil, with recommendations for change made to CN.
Navy safety requirements
1.11 Navy safety policy tailors broader legislative and policy requirements to the unique operatingenvironment in which Navy operates. The Navy Safety Policy outlines the manner in which the Navydischarges its duty of care, whilst maximising capability, through:
a. an organised and accountable safety management system;
b. a culture of open reporting that allows for learning from mistakes, near misses andhazard identification processes;
c. a management system which does not attribute blame for errors, but does not tolerateviolation or deliberate non-compliance with orders;
d. full and integrated use of risk management through all elements of Navy; and
e. a safety target for commanders of a zero accident rate.
1.12 Notwithstanding this unique environment, the NAVSAFE system accords with theAustralian/New Zealand Standard (AS/NZS) 4804:1997—Occupational Hea th and Safety ManagementSystems—General guidelines on principles, systems and supporting techniques. A summary of therequirements of the Navy Safety Management system is in annex A to this chapter.
NAVSAFE OVERVIEW
Applicability
1.13 The NAVSAFE system is applicable to:
a. all Navy owned or operated ships, aircraft, establishments, teams or groups;
b. Service personnel, civilians or cadets serving in, or visiting, the units mentioned above,or undertaking Navy sponsored activities elsewhere;
c. those involved in the design, procurement, support, operation or disposal of Navyequipment or systems;
d. Navy activities which have potential impact upon the health and safety of any otherindividual; and
e. in certain circumstances platforms and equipment owned by other services for whichNavy has been assigned regulatory authority.
NCELLED

ABR 63031–4
Defence FOI 553/20/21 Item 2 Document 1
Objectives and requirements of NAVSAFE
1.14 NAVSAFE is designed to be a structured process that assists in lowering the risks of accidentsand dangerous occurrences. To achieve this objective, NAVSAFE avoids narrow definitions of the termOHS, and instead focuses upon mandating a system that achieves safety through materiel integrity; andpersonal preparedness and commitment.
1.15 In order to achieve the objectives of NAVSAFE, the following requirements must be met:
a. Initial ship/establishment/facility, systems and equipment designs and any subsequentdesign changes are, and remain, inherently safe given their role and purpose. They arealso to be capable of safe maintenance and safe operation in their intended role.
b. Ships/establishments/aircraft/facilities, and their systems, are to be constructed andmaintained in a safe material condition in accordance with the current design intent andeventually disposed of safely.
c. Ships/establishments/aircraft/facilities are to be crewed in accordance with an approvedScheme of Complement.
d. All ships, units, groups and naval establishments are to have in place operational safetyteams focused on the identification and elimination of hazards; and raising safetyawareness. Hazards are to be identified, reported and managed within a process thatensures appropriate levels of command are both empowered and accountable forresolution or reduction measures.
e. Collective and individual training is to meet operational requirements appropriate toeach type of ship/establishment/facility and system, and establish and maintain aminimum acceptable standard of competency for each level of responsibility.
f. Ships/establishments/aircraft and their systems are to e operated safely in accordancewith the intended role and within limitations speci ied by the design, material support andoperating authorities. Any depa ture fr m these limitations to meet operationalrequirements is to be managed with due regard to health and safety and with theappropriate level o command approval. Operations are to be conducted utilising riskmanagement as a core c mponent of the decision making process.
Components of the NAVSAFE system
1.16 The principal components of the NAVSAFE System, which are described in detail insubsequent chapters are:
a. ship, establishment and squadron safety management systems, including their safetyteams;
b. Force Element Groups (FEG);
c. Maritime Command;
d. Navy Systems Command;
e. Navy Certification Safety and Acceptance Agency;
f. Safety Boards;
g. the Safety Management Group;
h. the RAN Safety Council;
i. Navy Headquarters; and
j. Defence Enabling Executives, Defence Output Executives and civilian organisationswhich provide goods and services.
NCELLED

ABR 63031–5
Defence FOI 553/20/21 Item 2 Document 1
Implementation
1.17 Implementation of the RAN Safety Management System will be through Navy’s corporatesafety management and line management structure. Primary responsibility for implementation restswith:
a. Subgroup managers (Maritime Commander Australia, Systems Commander, FEGCommanders) who have responsibility for provision of resources and for ensuring thatNAVSAFE is established within their areas of responsibility.
b. Subgroup manager’s staff who must ensure the inclusion of safety and riskmanagement in staff, operational and material requirements.
c. Navy and Enabling Executive resources planning staff who are responsible forensuring that any required safety management funding is provided in good time.
d. Acquisition and Sustainment line managers who have responsibility forimplementing and maintaining NAVSAFE within the procurement and sustainmentphases of equipment service.
e. Training staff who are responsible for the provision of adequately trained competentpersons for the effective achievement of NAVSAFE objectives.
f. Operators who are responsible for maintaining the integrity of established safetymanagement systems onboard ships/establishments/aircraft, and for the operation ofthe platform or equipment within the boundaries of:
(1) manufacturer’s or supplier’s properly established op rating parameters;
(2) parameters set as a result of the RAN Test, Evaluation and Acceptance process;
(3) conditions set by safety cases, or safety case reports; and
(4) limitations imposed by operating authorities.
1.18 As well as building on success ul safety programs in use, NAVSAFE incorporates conceptsadopted by safety managers in industry, such as the Safety Case process and an organisational safetyculture.
Annexes:A. Navy Safety Management System (NAVSAFE) principles and elementsB. The NAVSAFE system
NCELLED

ABR 6303ANNEX A TOCHAPTER 1
Defence FOI 553/20/21 Item 2 Document 1
NAVY SAFETY MANAGEMENT SYSTEM (NAVSAFE) PRINCIPLES AND ELEMENTS
General requirements
1. Safety management systems must be established and maintained in a manner that best suitsthe environment in which an organisation operates. The unique environment in which Navy operatescalls for a system (NAVSAFE) specifically tailored to that environment. The following requirements havebeen considered:
a. Safety must not be seen in isolation, as an end unto itself. Safety must be integrated intoNavy Management Systems and culture.
b. NAVSAFE must aim to improve capability through preservation of resources andenhancement of operational capability.
c. NAVSAFE must be geared towards assisting with discharging the Duty of Care to Navyand other effected personnel, including compliance with legislative and common lawrequirements.
d. Efficiencies can be gained through applying Defence wide safety systems, but thesesystems must be checked against Navy requirements.
e. NAVSAFE must facilitate a process of continual improvement.
2. The unique environment in which Navy operates includes the following considerations:
a. the additional legal and regulatory requirements stemming f om the operation of ships,aircraft and their associated systems;
b. the requirement to manage the safety of ships of war, including the interface betweenlarge numbers of personnel, se sors emitting many types of radiation, weaponssystems (including explosive ordna ce) and operational requirements;
c. the requirement to oversee acquisition, support and service provision systems notdirectly owned or managed by Navy;
d. the challenges associated with being a ‘parent navy’ for many items of inventory; and
e. the requirement to also manage shore based personnel and equipment.
3. NAVSAFE will therefore consist of the following:
a. A Navy Safety Policy issued by Chief of Navy,
b. A plan to manage:
(1) the identification, assessment and control of risks;
(2) compliance with Occupational Health Safety legislation and regulations;
(3) the setting of safety objectives and targets; and
(4) the achievement of safety objectives and goals.
c. An implementation process that defines:
(1) resource requirements;
(2) lines of responsibility and accountability;
(3) training and competency needs;
(4) consultation, communication and reporting requirements;
NCELLED

ABR 63031A–2
Defence FOI 553/20/21 Item 2 Document 1
(5) documentation requirements;
(6) hazard and risk management processes; and
(7) emergency and contingency arrangements.
d. A performance measurement system which measures against both internal goals, andexternal legislative requirements, encompassing:
(1) documentation and promulgation of requirements,
(2) health surveillance requirements,
(3) incident investigation procedures and reports,
(4) records and record management procedures, and
(5) audit procedures and requirements.
e. A system for management review of NAVSAFE’s performance.
NCELLED


ABR 6303 Defence FOI 553/20/21 Item 2 Document 1
CHAPTER 2
NAVSAFE DUTIES AND RESPONSIBILITIES
ROYAL AUSTRALIAN NAVY CORPORATE SAFETY MANAGER
2.1 The Deputy Chief of Navy (DCN) is the Royal Australian Navy (RAN) Corporate SafetyManager responsible to the Chief of Navy (CN) for safety in the Navy Program. DCN is the chair of theRAN Safety Council.
DIRECTOR–GENERAL NAVY CERTIFICATION, SAFETY AND ACCEPTANCE AGENCY
Role
2.2 The Navy Certification, Safety and Acceptance (NCSA) Agency supports the effective deliveryof naval and combat capability by Force Element Groups (FEG), through oversight and delivery of aregulatory and certification system that ensures the safety, fitness for purpose, material and operationalintegrity of naval capability.
2.3 The NCSA Agency is an independent regulatory agency, with responsibilities and authorityencompassing all areas of the Navy, as well as organisations supporting the Navy. It comprises aDirector-General Navy Certification, Safety and Acceptance (DGNCSA) the Director Navy SafetySystems (DNAVSAFE), the Director Navy Certification and Safety—Su face Ships (DNCS–SS), DirectorNavy Certification and Safety—Submarines (DNCS–SM), and the Director RAN Test Evaluation andAcceptance Authority (DRANTEAA).
2.4 The signal address for DGNCSA, DNAVSAFE, DNCS–SS and DNCS–SM is Director-GeneralNavy Certification and Safety (DGNAVCERTSAFE). RANTEAA is a separate signal address. A moredetailed description of director’s roles and unctions is in annex C to this chapter.
Tasks
2.5 The NCSA Agency is to:
a. promulgate Navy regulatory policy;
b. promulgate Navy safety and risk management policy;
c. promulgate Navy acceptance into service policy;
d. manage RAN regulation, certification and audit;
e. develop recommendations to the CN, through Maritime CommanderAustralia (MCAUST), for provisional acceptance and acceptance into Naval Service ofmaritime capability (DRANTEAA task);
f. liaise with Director-General Technical Airworthiness (Support Command Australia (Air))and Director Flying Safety on AIRSAFE and Naval Aviation regulation issues;
g. review Navy compliance with statutory safety regulations;
h. liaise with other Defence agencies including Defence Safety Management Agency toensure compliance with Australian Defence Organisation safety policies;
i. liaise with external safety agencies to ensure Navy compliance with safety regulationsand best practice;
j. conduct reviews, audits and investigations as required in order to provide independentassurance of compliance with safety requirements; and
k. manage and promote the NAVSAFE program.
NCELLED

ABR 63032–2
Defence FOI 553/20/21 Item 2 Document 1
MARITIME COMMANDER AUSTRALIA
Role
2.6 MCAUST is responsible to CN for the maintenance of fleet standards, including safetystandards, within the RAN; and to the Commander Australian Theatre for the conduct of Combined, Jointand Maritime Operations.
Tasks
2.7 In order to discharge the safety requirements of this role, MCAUST is to:
a. facilitate, and audit compliance with, the requirements of NAVSAFE for ships andestablishments under MCAUST command;
b. set boundaries of operation for, and provide guidance on, the conduct of operationalprocedures and evolutions;
c. oversee the safety management systems of the FEG; and
d. manage the interface between Enabling Groups, equipment and service providers, andfleet units, in order to ensure the integrity of safety management systems.
COMMANDER AUSTRALIAN NAVY SYSTEMS COMMAND
Role
2.8 The Commander Australian Navy Systems Command has f ur prim ry areas of responsibility:
a. integrated Naval personnel policy implementation and delivery;
b. Naval systems requirements, standards development and support;
c. support for command of fleet bases and establishments, and associated nationalservices; and
d. safety, certification and audit.
Tasks
2.9 In order to discharge these areas of responsibility, with respect to safety, the SystemsCommander is to:
a. establish and manage agreements with Enabling Groups and other agencies withrespect to safety and safety management;
b. support and service the safety management systems of Navy FEG;
c. provide cross FEG safety, and safety management systems support;
d. develop, implement and deliver safety and safety management systems training; and
e. manage and audit the safety systems of fleet bases and associated services; and portservices and support craft.
FORCE ELEMENT GROUP COMMANDERS
Role
2.10 FEG Commanders are responsible for implementing, managing and monitoring the safetyperformance of units within their group. FEG commanders are responsible for providing expert advice toMCAUST on matters affecting the safety of units within the group.
NCELLED

ABR 63032–3
Defence FOI 553/20/21 Item 2 Document 1
Tasks
2.11 FEG Commanders are to:
a. develop and implement a safety management plan for the FEG,
b. promote a safety culture within the FEG,
c. provide FEG specific safety advice as required.
DEFENCE SERVICE PROVIDERS
2.12 Other Defence groups, especially Defence Materiel Organisation, Corporate Services andInfrastructure Group and Defence Science and Technology Organisation are responsible for theprovision of equipment and services to Navy. As such they will be required to support theNAVSAFE program, as well as the RAN regulatory system.
ROYAL AUSTRALIAN NAVY SAFETY COUNCIL AND SAFETY BOARDS
RAN Safety Council
2.13 The role of the RAN Safety Council is to provide advice to DCN on corporate safety policy andto oversee the implementation of Navy safety policies. Terms of reference for the RAN Safety Councilare in annex A.
Safety Boards
2.14 The Safety Boards are those groups constitut d to develop policy and oversee safety withinspecific areas. Terms of reference for the Boards are n ann x B. The Boards’ titles and areas ofresponsibility areas follows:
a. SHIPSAFE Board The SHIPSA E Board is responsible for safety policy developmentand oversight of all safety aspects relating to maritime operations including surface ship,mine clearance and diving activities and all maritime operations not otherwise coveredby the SUBSAFE, ARMSAFE and AIRSAFE Board responsibilities.
b. AIRSAFE Board. The AIRSAFE Board is responsible for safety policy development andoversight of all safety aspects of naval aviation. The Director of Flight Safety supportsAIRSAFE and Australian Defence Force flight safety.
c. SUBSAFE Board. The SUBSAFE Board is responsible for safety policy developmentand oversight of all aspects related to the safety of submarines.
d. ARMSAFE Board. The ARMSAFE Board is responsible for safety policy developmentand oversight of safety aspects which relate to the handling, transport, storage andmaintenance of explosive ordnance.
e. SHORESAFE Board. The SHORESAFE Board is responsible for safety policydevelopment and oversight of safety aspects related to shore and support operationsand other shore activities not otherwise covered by other Boards.
f. RADSAFE Board. The RADSAFE Board is responsible for safety policy developmentand oversight of all safety aspects of radiation safety.
2.15 Terms of reference for the Safety Boards are in annex B.
NCELLED

ABR 63032–4
Defence FOI 553/20/21 Item 2 Document 1
Safety Management Group
2.16 The Safety Management Group consists of the Executive Directors of the Safety Boards, theFleet Environmental and Occupational Health and Safety Coordinator, Director Establishments andInfrastructure, and DNAVSAFE who acts as chair. The Safety Management Group is a forum forcommunication between boards, the sharing of lessons learned, and the formulation of policyrecommendations.
Annexes:A. Royal Australian Navy Safety Council—Terms of ReferenceB. Royal Australian Navy Safety Boards—Terms of ReferenceC. Roles and Functions of Directorates within Navy Certification and Safety Agency
NCELLED

ABR 6303ANNEX A TOCHAPTER 2
Defence FOI 553/20/21 Item 2 Document 1
ROYAL AUSTRALIAN NAVY SAFETY COUNCIL—TERMS OF REFERENCE
1. The Royal Australian Navy (RAN) Safety Council will meet at least annually after thecompletion of the financial year, and as required, to provide executive oversight of the RAN SafetyManagement System (NAVSAFE). The council will receive reports from the Chairperson of allSafety Boards, and a report on overall naval safety matters from Director-General Navy Certification,Safety and Acceptance (DGNCSA).
2. Membership of the RAN Safety Council will be determined by Deputy Chief of Navy, and willnormally include representation from each functional area of Navy. Director Navy Safety Systems is toact as secretary to the RAN Safety Council.
3. The content of the annual report submitted by DGNCSA to the Defence Annual Report,required under the Occupational Health and Safety (Commonwealth Employment) Act 1991 is to besubmitted to the board as part of the DGNCSA annual report.
4. The Safety Council is to review the Navy Safety Policy annually, and make anyrecommendations for change to Chief of Navy.
NCELLED

ABR 6303ANNEX B TOCHAPTER 2
Defence FOI 553/20/21 Item 2 Document 1
ROYAL AUSTRALIAN NAVY SAFETY BOARDS—TERMS OF REFERENCE
General responsibilities
1. Safety Boards are a means of providing the Chief of Navy with an independent confidence, orotherwise, that ships, submarines, aircraft, establishments and their related equipment are beingmaintained and operated in a manner which is considered safe. In discharging this responsibility, thefollowing principles apply:
a. Boards are to be independent of the safety management system they oversee. Thesafety management system must not rely on the board to assure safety, as the board isto sit outside the system, providing an independent confidence.
b. The responsibility for ensuring that systems are safe rests with the operators,maintainers and managers of the system. The burden of proof rests with thesepersonnel to be able to prove that a system is safe when required to do so by a board.There is no burden of proof to prove that a system is not safe.
2. The Safety Boards are responsible to Deputy Chief of Navy (DCN) for the management ofsafety in their relevant areas. They are responsible for the following tasks:
a. Monitoring the prompt implementation of safety recommendations arising from anyformal proceedings, following accidents or incidents.
b. Monitoring the closure of all safety issues for which they have been designatedresponsibility for oversight.
c. Directing audits of facilities or organisations within the r areas of responsibility, to ensurecompliance with the Occupational Health and Safety (CommonwealthEmployment) Act 1991 and regulations, and the NAVSAFE system.
d. Reporting to DCN detai s of safety ssues which have not been resolved in a timely oreffective manner.
e. Reporting to DCN d tails of any outstanding safety issues from the business of thesafety board for which there is dissent or disagreement amongst board members.
3. Each Safety Board is to meet at least twice annually.
4. Membership of the board should be agreed by the chair of the board andDirector-General Navy Certification, Safety and Acceptance (DGNCSA), and should includerepresentation from all stakeholders. Members must have sufficient authority to be able to take actionsas agreed by the board. Board members are to be appropriately trained in safety management. DirectorNavy Safety Systems (DNAVSAFE) and the Executive Directors of the boards are to liaise, providingtraining as required.
5. An annual report is to be provided to the Royal Australian Navy (RAN) Safety Council at theend of the financial year by each board. As a minimum, the report should contain:
a. Briefings on major safety events that affected the board’s area of responsibility.
b. Significant hazards or issues that have been resolved.
c. Significant hazards or issues that remain outstanding.
d. Safety performance indicators, with an analysis of trends.
e. Status of Board Member training.
f. Priorities for the next financial year.
NCELLED

ABR 63032B–2
Defence FOI 553/20/21 Item 2 Document 1
Executive Directors of Boards
6. The SHIPSAFE, SUBSAFE, SHORESAFE boards have full time Executive Directors. TheExecutive Director of each Board is responsible to the Chair of that Board for the day-to-daymanagement of activities. Executive Directors, together with Director, Establishments and Infrastructure,Fleet Environmental and Occupational Health and Safety Coordinator and DNAVSAFE (chairperson),will function as the Safety Management Group responsive to the direction of the DCN, the RAN SafetyCouncil and DGNCSA as appropriate.
Specific roles and functions of Safety Boards
7. Specific roles and functions may be given to individual Boards in order to manage safety withintheir areas of responsibility. They may communicate directly with RAN Commands, other Service andcivil organisations, domestic and foreign, and with other cognisant authorities on safety relatedoperational and support matters. Boards are encouraged to establish structures down to unit level forthe purpose of disseminating policy and information and obtaining statistical and performance feedback.
8. Specific guidance on the ARMSAFE Board’s Terms of Reference and composition can befound in DI(N) ADMIN 17–33—ARMSAFE Board—Terms of Reference and Composition. Specificguidance on the AIRSAFE Board can be found in Australian Book of Reference (ABR) 5150—NavalAviation Instructions and ABR 5147—RAN Aviation Safety Manual.
NCELLED

ABR 6303ANNEX C TOCHAPTER 2
Defence FOI 553/20/21 Item 2 Document 1
ROLES AND FUNCTIONS OF DIRECTORATES WITHIN NAVY CERTIFICATION AND SAFETY AGENCY
Director of Navy Safety Systems
1. Director of Navy Safety Systems (DNAVSAFE) is responsible for sponsoring and coordinatingthe Navy safety program, supporting the Royal Australian Navy (RAN) Safety Council and coordinatingSafety Boards. The directorate also reviews overall Navy compliance with Occupational Health andSafety legislation and regulations, deferring to specialist authorities as required.
2. DNAVSAFE is also to act as Navy’s liaison officer and point of contact with external regulatoryauthorities which have scrutiny of Navy safety management activities, especially Comcare, and with theDefence Safety Management Agency (DSMA). DNAVSAFE is to ensure close liaison is maintained withDSMA to ensure that Navy and Australian Defence Organisation safety policies remain consistent.
Director of Navy Certification and Safety—Surface Ships
3. Director of Navy Certification and Safety—Surface Ships (DNCS–SS) is responsible toDirector-General Navy Certification, Safety and Acceptance (DGNCSA) for the development andcoordination of surface ship material regulation processes to provide Chief of Navy (CN) with assurancethat RAN surface ships are safe and fit for Naval service.
4. DNCS–SS is responsible for coordinating and controlling the definition and status ofcertification, safety and support aspects for surface Navy vessels through life.
Director of Navy Certification and Safety —Submarines
5. Director of Navy Certification and Safety—Submarines (DNCS SM) is responsible toDGNCSA for the provision of confidence that SUBSAFE Certification, Safety and RAN TechnicalRegulation requirements are achieved and maintained for RAN Submarines, Hyperbaric and DivingSystems.
6. DNCS–SM coordinates the Mate ial Safety and Quality systems elements of the SUBSAFEProgram and Material aspects of Escape, Rescue and Hyperbaric systems.
Director of Royal Australian Navy Test, Evaluation and Acceptance Authority
7. Royal Australian Navy Test, Evaluation and Acceptance is a professional and independentauthority for Operational Test and Evaluation of new and enhanced maritime capabilities for theAustralian Defence Force. Director of Royal Australian Navy Test, Evaluation and Acceptance Authorityis responsible for the development of a recommendation to CN, through the Maritime CommanderAustralia, for Provisional Acceptance and Acceptance Into Naval Service of maritime capability.
NCELLED

ABR 6303 Defence FOI 553/20/21 Item 2 Document 1
CHAPTER 3
UNIT RESPONSIBILITIES
RISK, OPERATIONS AND SAFETY
Definition
3.1 The NAVSAFE program is the Navy Safety Management system designed to allowcommanders to exercise a balanced approach towards risk, operations and safety. Whilst significanteffort and expense can ensure that ships and equipment are delivered to the operator as safe and fit forpurpose, it is ultimately those who take the ship to sea, or operate the equipment that are charged withthe responsibility for equipment and personnel safety.
Aim
3.2 The aim of this chapter is to detail the requirements for managing safety that will be enactedby unit level commanders.1
Safety culture
3.3 The United Kingdom’s Health and Safety Commission in 1993 defined Organisational SafetyCulture as ‘The safety culture of an organisation is the product of individual and group values, attitudes,competencies, and patterns of behaviour that determine the commitment to, and the style andproficiency of, an organisation’s health and safety programs. Organisations with a positive safety cultureare characterised by communications founded on mutual trust, by shared pe cept ons of the importanceof safety, and by confidence in the efficacy of preventive measures.’
3.4 Chief of Navy addressed the issue of safety cul ure in he Navy Safety Policy:
I acknowledge that all personnel are prone to errors. We should learn from our errors and the errors ofothers. However this will not happen i personnel do not report their near misses for fear of being blamed.Therefore, blame will not be attribu ed for reported accidents or incidents where there is no violation oforders or instructions. The failure to report accidents or near misses is an abrogation of responsibility anda failure of management.
Violations, or deliberate non-compliance with orders, will not be tolerated. If orders are not appropriate,bring this to the attention of the originator. In the case of violations, disciplinary or dismissal action maybe taken, or the professional qualifications of violators reviewed.
Commanders are to recognise ‘Effectiveness and Safety’ of units and personnel under their command.This will equate to recognising our ‘Best and Fairest’.
SHIP SAFETY MANAGEMENT
The Ship’s Safety Team
3.5 Safety is the responsibility of every person in the workplace. However, in order to managesafety and risk it is necessary to formalise a structure for the management of hazards, and for theimplementation of control and reporting procedures.
3.6 In Navy this is known as the Ship’s Safety Team (SST). Establishments should generallycomply with these provisions, but may alter their structure as necessary to comply with the uniquerequirements of each shore establishment. Efficiencies should be gained by utilising common Defenceresources, promulgated by Defence Safety Management Agency (DSMA), provided the requirements ofthe NAVSAFE program are met.
1 Many areas of specialist safety management are comprehensively addressed in other books of reference, such as flightsafety and submarine safety. When this occurs, description in this manual of the safety management system has beenkept to an overview, designed for an uninitiated reader, and refers the reader to the relevant reference for more detail.
NCELLED

ABR 63033–2
Defence FOI 553/20/21 Item 2 Document 1
Team composition and qualifications
3.7 The SST is to be headed by the Executive Officer in recognition of the importance of this job.The team is to be representative of all personnel, and as such must include at least one junior sailor, andshould have representatives from technical and non-technical specialisations. As a guideline, ships andestablishments with a complement of 70 or less should have a minimum of three and a maximum of fiveteam members. Other ships and establishments should have a maximum number of no more than thechair considers workable depending on the size and cross section of the complement.
3.8 Team members are to undertake appropriate safety training as soon as is practicable. Acommitment to safety culture cannot be sustained whilst inexperienced personnel are charged withimplementation of safety. A well trained and motivated safety team will have a multiplying effect on thesafety culture within a ship. Whilst Junior Officers can gain valuable experience in safety managementfrom participation in this process, it is not appropriate to delegate significant responsibilities toinexperienced personnel.
3.9 The Commanding Officer (CO) is to approve the nomination of members of the SST. Detailsof the SST, by name, are to be promulgated in a prominent position(s) within the ship.
Roles and Functions of the Ship’s Safety Team
3.10 The SST is to perform the following functions:
a. Identification of hazards through regular workplace inspection. All areas are to beinspected for hazards at regular intervals. Use of personnel less familiar with theworkplace, as an independent set of eyes, is to be encouraged.
b. Recording of hazards identified by the SST or brought to the attention of SST by otherpersonnel.
c. Assessment of hazards. Once identified the severity of hazards is to be determined.Hazards assessed as unacceptable or undesirable.
d. Implementation of controls to mitigate hazards. This may include short term controls toprevent further safety incidents. This process may also involve recommendations to theCommand to elevate the responsibility for hazard control to the appropriate authority,should the control measure be beyond the capability of the ship.
e. Monitoring of the effectiveness of control measures put in place.
f. Recording of safety related information, including documentation of hazards and theprocesses of implementation, recording injuries, raising of Form AC 563—Incident andFatality Report and compliance with other reporting obligations as required by currentregulations as detailed in chapter 7—‘Accidents and incidents’.
g. Raising Occupational Health and Safety Incident Report (OHSIR) as detailed inchapter 7.
h. Recording minutes of the SST committee meetings;
i. Arranging for appropriately qualified persons to conduct workplace surveys shouldconcerns be raised about hazards which cannot be readily measured using onboardequipment (eg noise, dust or particulate levels).
NCELLED

ABR 63033–3
Defence FOI 553/20/21 Item 2 Document 1
3.11 The aim of workplace inspections is to detect hazards and unsafe acts as well as to recognisewhether safety awareness and safety initiatives are improving. The inspection should be conductedseparately from any other organised inspection or routine rounds. The result of these inspections are tobe recorded and reported to the CO with action recommended where necessary. The report to the COis to show:
a. whether safety awareness and pro-active safety is improving;
b. action which can be taken within the ship/establishment to eliminate hazards and unsafeacts;
c. organisational faults affecting safety and unsafe acts; and
d. that appropriate action has been initiated on all entries of Form OS 006—ShipsOccupational Health and Safety Log.
Form OS 006—Ships Occupational Health and Safety Log
3.12 Form OS 006 was introduced to assist the SST in recording and managing hazards. It isdivided into two sections:
a. Section 1. Section 1 is designed to record all reported accidents and near misses. Allaccident/incident forms raised are to be recorded in sequence in this section, beforethey are forwarded by Form AC 563 to Comcare and/or DSMA as appropriate. If anOHSIR is raised, this should also be noted. The assigned Hazard Risk Index (HRI)should also be recorded. (See chapter 7 of this manual for more details on reportingrequirements).
b. Section 2. Section 2 is designed to record the results of haza d surveys and is to containdetails of all hazards and the action taken to rectify or eliminate them. This sectionshould also be used to record near m sses, ncluding details of supporting OHSIRmessages, and the assigned HRI
3.13 The log is to be kept by the head of th SST, or a delegated member of the team. Theinformation in the log should be reviewed by the SST at each meeting, and on other occasions asrequired, in order to ensure that hazards o not remain untreated. Instructions for the use of the log arecontained inside the front cover. A suitable electronic substitute for the log may be used, provided allrequired information is recorded. The CO should review the log periodically. Duplicate copies should beforwarded to the NAVSAFE records section (CP4–6–096, Department of Defence, ACT 2600)
PERSONNEL INDUCTION PROCESSES
Rationale
3.14 Personnel are often at their most vulnerable when first taking up duties in a new workplace.Factors such as inexperience, a reluctance to ask questions for fear of looking ignorant, and the need totransition from the classroom environment to the real workplace are all factors which can contribute toan elevated level of risk exposure to inexperienced and junior personnel. The duty of care to thesepersons is to ensure they are adequately equipped to remain safe in both normal, and abnormal,conditions in the workplace.
Requirement
3.15 Commanders and managers are to ensure that personnel are inducted into work environmentssuch that they are:
a. adequately prepared for the safe conduct of their duties,
b. aware of the hazards associated with the workspace or compartment, and
c. competent to react to abnormal conditions such as emergency situations.
NCELLED

ABR 63033–4
Defence FOI 553/20/21 Item 2 Document 1
SAFETY DURING MAINTENANCE
Rationale
3.16 History has shown that the level of personal injury increases significantly during maintenance,especially in periods of dockyard availability. Combinations of low personnel numbers, unfamiliarsurroundings, unusual modifications to access and egress provisions, and hazards associated with theconduct of maintenance, can all contribute to an elevated risk of personal injury.
Dangers posed during maintenance
3.17 Hazards posed by the environment in which maintenance takes place are innumerable. Fallhazards from the nature of the dock, removal of rails, guards, steps and ladders, are common. Unwantedexposure to fumes, chemicals, dust and other toxic substances has been common in the past. Soundrisk management processes must be in place to ensure that, as far as possible, hazards are foreseenand managed.
Relations with contractors
3.18 An essential element of creating a safe working environment during maintenance, is theestablishment of a sound working arrangement with the contractors involved. Work plans must bedeveloped so that the ship’s company are aware of the intended work, and therefore the safetyimplications. Coordination of contractors, when more than one is on site, is essential to the maintenanceof safety; conflicting activities have often resulted in personal injury. Equally, it is essential that safetyroutines and procedures mandated by appropriate dockyard authorities are adhered to byNavy personnel. All personnel must be familiar with the established safety and emergency procedures.
INTRODUCTION OF HAZARDOUS SUBSTANCES
Rationale
3.19 Significant improvements hav been made in the management and awareness of hazardoussubstances, but it still remains a so rce of personal injury, and must be managed effectively. Hazardoussubstances can potentially be introduced hrough a number of sources, and it is only through diligenceand training that they can be managed.
Command responsibilities
3.20 It is a requirement of Command that hazardous substances be managed through themaintenance of appropriate registers, the meeting of specific labelling and packaging requirements, andthe provision of Material Safety Data Sheets (MSDS). Specific attention needs to be given to:
a. Hazardous materials already in the workplace, which may not be managed effectively.
b. The method of introduction of hazardous materials, via recognised stores systems, orby less rigorous systems such as local purchase.
c. The hazards associated with combining armament stores and hazardous substances.
d. The competency of personnel involved in the introduction of substances.
e. Protection measures against inadvertent introduction of hazardous substances; and
f. first aid and emergency procedures and plans.
Material Safety Data Sheets
3.21 MSDS contain the necessary precautions, handling and first aid instructions necessary tomanage hazardous substances in the workplace. They are effective only if they are readily available forconsultation, and if personnel potentially exposed to hazardous substances are aware of them, and theircontents. Chemwatch maintains an electronic database of current MSDS, which can be accessedthrough the DSMA intranet web site at http://dsma.dcb.defence.gov.au/. A toll free telephone number(1800 039 008) may be used for emergency situations.
NCELLED

ABR 63033–5
Defence FOI 553/20/21 Item 2 Document 1
ORDNANCE SAFETY MANAGEMENT
Rationale
3.22 It is axiomatic that the firing of weapons and handling of ammunition and other forms ofExplosive Ordnance (EO), including seemingly innocuous devices as pyrotechnics and fireworks, areinherently dangerous activities. It is with this in mind, that all users of weapons systems and EO shouldhave a strong safety focus and adhere to all prescribed safety procedures.
Ordnance safety procedures
3.23 There is no one reference or source of ordnance systems safety procedures so it is incumbenton operators and maintainers that they be well versed in the unique safety requirements of the systemsfor which they are responsible. With regard to EO, there are a number of references that detail the safetyrequirements for the handling, storage and use of EO. It is imperative that personnel involved be fullyconversant with these requirements.
References
3.24 The following references provide information on ordnance safety:
a. Australian Book of Reference (ABR) 862—Naval Magazine and Explosive Instructions;
b. NAVSEA OP4—Ammunition Afloat;
c. NAVSEA SW300–BC–SAF–010—Clearing of Live Ammunition from Guns;
d. ABR 1043—RAN Firing Manual;
e. Defence Instruction (Navy) DI(N) ADMIN 17–33—ARMSAFE Board—Terms ofReference and Composition
RADIATION SAFETY MANAGEMENT
Types of hazard
3.25 There are several forms of radiation to which personnel can potentially be exposed, includingionising radiation (radioactive materials), non-ionising radiation (radio-frequency RadiationHazard (RADHAZ)), lasers and ultra violet radiation.
Electromagnetic Radiation safety
3.26 Electromagnetic Radiation has the capability to harm and create permanent damage topersonal working in the vicinity of a RADHAZ area. All personnel are to be fully conversant with theRADHAZ procedures applicable to their ship or workplace.
Laser safety
3.27 Laser radiation is hazardous to the human eye and can cause serious damage or evenblindness. A detailed description of the hazards and laser equipment requirements is found inAustralian Standard AS/NZS 2211.1—Laser Safety.
References
3.28 The following references should be consulted for further information on radiation safety:
a. Defence Instruction (General) DI(G) PERS 19–3—Occupational Health and SafetyRadio-Frequency Radiation Hazards (RADHAZ);
b. ABR 2924—Electromagnetic Radiation Hazards in the RAN;
NCELLED

ABR 63033–6
Defence FOI 553/20/21 Item 2 Document 1
c. DI(N) LOG 88–4—Royal Australian Navy Safe-to-Fire Zones (Including LaserSafe-To-Fire Zone);
d. DI(N) LOG 72–6—Royal Australian Navy Laser Safety.
SUBMARINE SAFETY MANAGEMENT
SUBSAFE purpose
3.29 The Royal Australian Navy (RAN) SUBSAFE Program was established during the acquisitionof the Collins class submarines to manage the risks involved in introducing the new class to the RAN.The SUBSAFE program is the management system used by Navy and non-Navy activities involved withRAN Submarines to comply with the Occupational Health and Safety (Commonwealth Employment)Act 1991 (OHS(CE) Act 1991).
Overview
3.30 The SUBSAFE Program is a broad program with a strong emphasis on prevention, planningand the management of hazards. The program also includes comprehensive contingency and accidentrecovery plans, training and equipment.
3.31 The aim of SUBSAFE program is to provide a management system that safeguards the healthand safety of all personnel in friendly contact with RAN Submarines.
References
3.32 The SUBSAFE program is described in the SUBSAFEMAN series of ABRs.ABR 6103, SUBSAFEMAN 1, volume 1—SUBSAFE Program General Requirements, provides anoverview of the program and a guide to the SUBSAFE manuals
AVIATION SAFETY MANAGEMENT
AIRSAFE purpose
3.33 The purpose of AIRSAFE is to preserve human and material resources. The Program isintended to enhance operational readiness and combat effectiveness, by preserving the resources usedin accomplishing naval aviation missions.
Overview
3.34 AIRSAFE is based on the concept that events are determined by preceding causes. Byeliminating these causes, injury to personnel and damage to resources can be prevented. This isachieved through; Aviation safety awareness, Hazard identification, Reporting and Reduction andSafety Surveys.
3.35 The closed loop reporting system employed by AIRSAFE and the AIRSAFE System SafetyWorking Group (ASSWG) is used to track, to completion all actions arising from hazard reports, incidentand accident investigations. This guarantees a resolution to all identified hazards.
References
3.36 Information on AIRSAFE is found in ABR 5150—Naval Aviation Instructions andABR 5147—RAN Aviation Safety Manual. The AIRSAFE program is described in detail in ABR 5147.
NCELLED

ABR 63033–7
Defence FOI 553/20/21 Item 2 Document 1
HYPERBARIC AND DIVING SAFETY MANAGEMENT
HYPERSAFE purpose
3.37 The purpose of HYPERSAFE is to develop and implement a system safety program ofsufficient comprehensiveness to identify the hazards of all RAN diving and diving related hyperbaricsystems, and to make recommendations for design requirements and management control, in order toeliminate hazards or reduce the associated risk to an acceptable level.
Overview
3.38 The Hyperbaric and Diving Safety Sub-Group of SHIPSAFE was established for Hyperbaricsystem safety management, pursuing best practice as compared to the Offshore Oil and Gas Industryand leading Navies.
3.39 HYPERSAFE employs an holistic approach to safety management embracing and integratingtraining, operational procedures, design, maintenance and equipment selection, to enable bettermanagement of the RAN’s hyperbaric assets by maximising operational availability whilst optimising lifecycle costs. Of particular note, HYPERSAFE provides a forum for the overview of safety cases for newequipment and procedures and the compilation of the HYPERSAFE Hazard Log and risk assessment.
3.40 The HYPERSAFE Program has a strong emphasis on prevention, planning and themanagement of hazards and given much is its charter covers direct life support, actively promotes theopen and timely reporting of incidents and accidents.
References
3.41 ABR 155—RAN Diving Manual, volume 2, chapter 18 details the sp cific procedures andreporting requirements for hyperbaric and diving incidents and accid nts.
ESTABLISHMENT SAFETY MANAGEMENT
Duty of Care
3.42 The diversity of organisations and activities within establishments dictates the necessity for theimplementation of detailed, formal agreements and processes to manage the diverse safety issues thatwill be encountered. The CO of Navy establishments is responsible for managing the safety of allpersonnel in that establishment.
Implementation
3.43 Regardless of whether personnel present in an establishment are Navy personnel, membersof other Defence groups, service providers, contractors, or visitors, the Occupational Health and Safety(OHS) system must cater for the requirement to manage their safety. The DSMA provides guidance onthe establishment of safety and emergency management systems, and their intranet web site containsa large amount of useful safety information. Much of the information supplied can be used by the CO ofNavy facilities, but the CO must tailor the safety management system for the establishment to suit thespecific needs of the facility. The interaction between ships and establishments, unique to Navy facilities,is an example of the tailored safety management that is required.
3.44 It may not always be practicable for the establishment’s OHS committee structure to deal withthe day-to-day management of safety in separate facilities within an establishment, especially in thecase of lodger units. In such cases the CO should direct the lodger unit to maintain a separateOHS system to manage the nominated workplace. Minutes of the lodger unit’s safety managementmeetings are to be provided to the CO in order to provide an assurance that OHS managementrequirements are being met. The lodger unit should remain represented on the central OHS committee.
NCELLED

ABR 63033–8
Defence FOI 553/20/21 Item 2 Document 1
Service providers and enablers
3.45 Service providers, contractors and other enablers, providing plant, facilities, equipment or anyother goods or services, have a duty of care, and shall adhere to the provisions of theOHS(CE) Act 1991, sections (18), (19) and (20). Summarised, this requires that:
a. Manufacturers of plant or equipment must ensure that the plant is designed andconstructed so as to be, when properly used, safe for use and without risk to health; theymust carry out, or cause to be carried out, the research, testing and examinationnecessary in order to discover, and to eliminate or minimise, any risk to health or safetythat may arise from the use of the plant or equipment; and they must make availableadequate information concerning the designed use, details of design and constructionand any conditions necessary to ensure that, when put to use, it will be safe.
b. Manufacturers of a substance must ensure that the substance is so manufactured as tobe, when properly used, safe for use and without risk to health; they must carry out, orcause to be carried out, the research, testing and examination necessary in order todiscover, and to eliminate or minimise, any risk to health or safety that may arise fromthe use of the substance; and they must make available adequate information inconnection with the use of the substance, adequate information concerning; the use forwhich it is manufactured and has been tested, details of its composition, any conditionsnecessary to ensure that, when put to the use for which it was manufactured and tested,it will be safe and without risk to health, and the first aid and medical procedures thatshould be followed if the substance causes injury.
c. Suppliers must ensure that at the time of supply, the plant or substance is in such acondition as to be, when properly used, safe for use and without r sk to health; they mustcarry out or cause to be carried out, the research, testing and examination necessary inorder to discover, and to eliminate or minimise any risk to the health and safety that mayarise from the condition of the plant or substance, and; they must make available, inconnection with the use of the plant or substance adequate information concerning thecondition of the plant or substance at the time of supply, any risk to the health and towhich the condition of the plant or substance may give rise unless it is properly used,the steps that need to be taken in order to eliminate such risk, and in the case of asubstance, the first aid and medical procedures that should be followed in the event ofthe condition of the substance causing injury.
d. Persons who erect or install any plant in a workplace must take all reasonablypracticable steps to ensure that the plant is not erected or installed in such a mannerthat it is unsafe for use or constitutes a risk to health.
3.46 Service providers, contractors and other enablers, providing plant, facilities, equipment or anyother goods or services, should be able to provide to the CO details of the manner in which the aboveprovisions of the OHS(CE) Act 1991 have been satisfied. Enabling Groups, who engage outsidecontractors to provide goods or services, should provide to the CO evidence of the sub-contractorscompliance with these provisions. As a minimum, Hazard Assessments, Site Safety Agreements, andContractor Safety Management Plans applicable to the establishment should be provided to the CO.
3.47 The CO may invoke any entry restrictions, briefings, training requirements or processes for civilcontractors operating within establishments, or mandate participation in safety management meetingsas a condition of their entry and work on the establishment. Service provision contracts shall recognisethis authority. Enabling Groups engaging sub-contractors to perform work or provide services are toensure that the sub-contractor is fully aware of any requirements invoked by the CO, and are to ensuretheir compliance.
3.48 In the event of contractor violation of establishment OHS requirements, accidents or incidents,COs have the authority (and often a duty) to report contractor shortcomings to Director-General NavyCertification, Safety and Acceptance, Comcare and/or State Workplace Safety Authorities. EnablingGroups managing contractors must ensure that contracts reflect this authority.
3.49 COs may refuse entry to the establishment or performance of work by any contractor or personwho refuses to accept the requirements of the establishment OHS system and the OHS(CE) Act 1991.
NCELLED

ABR 63033–9
Defence FOI 553/20/21 Item 2 Document 1
3.50 COs are to ensure that Enabling Groups provide details of the relevant OHS LiaisonOfficer (OHSLO) associated with the services being provided to the establishment. Details of the rolesand function of the OSHLO can be obtained from the contractor safety management guidelines issuedby DSMA.
Designated Work Groups and Health and Safety Representatives
3.51 The OHS(CE) Act 1991 (sections 24 to 38) contains provisions with regard to workplacearrangements, including requirements for Designated Work Groups and Health and SafetyRepresentatives (HSRs). COs of shore establishments should be conversant with the requirements ofthese sections, and should ensure that the requirements are met for all civilians in their establishment.Chief of the Defence Force (CDF) made a declaration, which appeared in the Commonwealth ofAustralia Gazette Number PS49 on 13 February 1992, to the effect that ‘References in sections 24 to 38inclusive, to employees will not include members of the Australian Defence Force (ADF)’. In essence,this exempts the requirement for compliance with those sections for uniformed personnel, but maintainsthe requirement for civilians to comply. ADF personnel cannot be members of Designated Work Groupsand cannot be elected as HSRs.
Management of Plant
3.52 The Department of Defence manages, under the provision of the Joint Special Licence (JSL),the special plant under its control. Special Plant Licence provisions apply to:
a. boilers categorised as hazard level A, B, C, or D in accordance with AS 3920.1–1993Amdt 2–1999—Assurance of Product Quality—Pressure equipment manufacture;
b. pressure vessels at hazard levels A, B or C in accordance with AS 3920.1–1993;
c. mobile cranes with a Safe Working Load greater than 10 tonnes; and
d. certain other plant which is not applicabl to the defence environment.
3.53 Other items of plant and equipment, not covered by JSL, require documentation to bemaintained on site, as to their maintenance stat s, safety and operation. Examples include asbestosregisters, fire fighting systems and eq ipment fork lifts, gas bottles, fuel installations, cooling towers andhazardous substances.
3.54 These items of plant, special plant and other equipment and substances are often owned byGroups other than Navy, but may be operated or used by Navy personnel, or other personnel over whomthe CO has a duty of care. The CO of an establishment cannot be reasonably expected to discharge thisduty of care without full and accurate documentation as to the hazards present, and the managementprocesses in place, to control hazards in workplaces under their authority. The owner, or Enabling Groupresponsible for the plant, shall provide the CO with all documentation required by relevant Federal, Stateand Territory authorities for the management of such plant, including hazard management. COs are topro-actively ensure that these requirements are met.
3.55 The operation of mobile cranes is a hazardous activity. Significant management effort must beexpended to ensure that these operations are conducted safely, by personnel who are competent. Inparticular, managers must ensure that operator competencies are appropriate and current, and that therequirements of the Occupational Health and Safety (Commonwealth Employment) (NationalStandards) Regulations 1994 are met.
Ship/Shore interface
3.56 Many Navy establishments contain berthing facilities for ships and other vessels. The interfacebetween ships and the parent establishment is an essential part of safety management. Hazards suchas shore supply cables, gangways and cranes need to be managed carefully, as history has shown thatthese hazards have been the source of many injuries and near misses.
3.57 The CO of the shore establishment is best placed to manage the safety of shore services, andis therefore charged with the responsibility for controlling and managing these facilities. Orders andinstructions relating to the provision of shore services should detail hazard information and emergencyprocedures.
NCELLED

ABR 63033–10
Defence FOI 553/20/21 Item 2 Document 1
SPORT AND ADVENTUROUS TRAINING
3.58 Historically, approximately one third of injuries to Navy personnel stem from sporting relatedinjuries. Fitness is an important element of preparedness for a defence force, and considerablereductions in the injury rate can be achieved by following simple processes such as:
a. Appropriate supervision of sporting activities by qualified personnel.
b. Preparedness (not attempting too much too soon).
c. Planning, including contingency and emergency planning. This is particularly relevantwhen planning adventurous training.
3.59 The requirement to report sports related injuries to Comcare has been exempted by CDF,however the reporting requirements to DSMA remain extant. Further details of these reportingrequirements can be found in chapter 7.
NCELLED

ABR 6303 Defence FOI 553/20/21 Item 2 Document 1
CHAPTER 4
PERSONNEL SAFETY AND TRAINING
RESPONSIBILITIES
Individual responsibilities
4.1 Under the Occupational Health and Safety (Commonwealth Employment) Act 1991(OHS(CE) Act 1991), individuals must:
a. take all reasonably practicable steps to ensure that they do not take any action, or makeany omission, that creates risk, or increases existing risk, to their own or any otherperson’s health or safety;
b. cooperate with the implementation of Defence and Navy safety programs; and
c. use equipment in accordance with any relevant orders and instructions to ensure itssafe and proper use.
Management responsibilities
4.2 The OHS(CE) Act 1991 requires the employer to take all reasonably practicable steps toprotect the health and safety at work of the employer’s employees. In particular the employer must:
a. provide and maintain a working environment that is safe for the employees and withoutrisk to their health, and that provides adequat facilit es for their welfare at work;
b. ensure the workplace is safe for employe s, without isk to their health, and provide andmaintain a means of access to and egress from, the workplace that is safe;
c. ensure the safety and bsence of isk at work in connection with the use, handling,storage or transpor of plant or substances;
d. develop an appropriate health and safety system that will promote and developmeasures to improve health and safety, and provide adequate mechanisms forreviewing the effectiveness of these measures; and
e. provide employees with the information, instruction, training and supervision necessaryto enable them to perform their work in a manner that is safe and without risk to theirhealth.
Command responsibilities
4.3 Commitment by all personnel in positions of responsibility, especially Command, is vital tosatisfying the moral and legal obligation to protect the health and safety of Navy personnel, and all otherpersonnel over whom Navy has influence. This can only be achieved through the following:
a. knowledge of, and commitment to, achieving the aims of the Navy Safety Policy;
b. knowledge of, and commitment to, the processes involved in safety risk management;
c. support of the safety culture which allows open reporting; and
d. ensuring decisions with respect to safety are made at the appropriate level.
NCELLED

ABR 63034–2
Defence FOI 553/20/21 Item 2 Document 1
OCCUPATIONAL HEALTH AND SAFETY TRAINING PHILOSOPHY
Philosophy
4.4 Maintaining operations that are safe, and which conform to Occupational Health andSafety (OHS) legislation, requires the careful selection, placement, ongoing assessment and propertraining of personnel. OHS training will be implemented via induction, promotion prerequisite,billet prerequisite and specialist OHS training courses.
Guidelines for Occupational Health and Safety Training
4.5 The OHS training philosophy will be met using the following guidance, which is the minimumstandard:
a. All uniformed inductees are to receive the OHS induction course within 30 days ofenlistment in accordance with the OHS(CE) Act 1991.
b. OHS induction training for Defence civilians is conducted during the Australian PublicService induction process. Supervisors are to ensure that Defence civilians areconversant with workplace safety arrangements applicable to their individual workplace.
c. Individual category courses are to contain OHS training relevant to the specific job ortask for which they are being trained.
d. Officers and sailors are to continue to receive all necessary OHS training throughouttheir career in order to equip them to be effective supervisors and managers. This willprimarily centre on OHS billet prerequisite training courses
e. Managers are to ensure that their local induction procedures are appropriate to preparepersonnel for their place of work. These procedures must include a safety brief coveringthe ship, Force Element Group or establ shmen In the case of ships, this brief is to bepromulgated by the class coordin tor
f. Senior personnel attending Comma ding Officer/Executive Officer/Head of DepartmentDesignate courses and members of safety boards are to be briefed on the principles ofship safety management n general and the NAVSAFE system in particular.
g. Personnel with specialist requirements for managing Naval Safety will be trained viaspecialist courses.
h. Members of the Australian Naval Cadet corp are to conform to the spirit of thesedirections.
Sailor career progression training
4.6 In keeping with the RAN’s legal and moral obligation to nurture working environments free fromrisk, sailors will be provided OHS training as modules of the Sailor non-core category training continuum.
4.7 The Leading Seaman Leadership Course (LSLC) is the first formal course in this continuum.The aim of the OHS training offered to this course is to educate Leading Seaman on workplace safety,and an appreciation of the hazard management process at the small group or team level. This objectiveis achieved by the presentation of the ‘OHS for Supervisors (Introduction)’ to the LSLC. On completionof the LSLC, graduates will be able to:
a. identify the rationale for OHS in Defence;
b. examine the intent of the OHS(CE) Act 1991, noting the responsibilities defined withinthe Act and its application in Defence;
c. identify, assess and control hazards within the Defence workplace; and
d. describe the process of reporting and investigating accidents and incidents in theDefence community.
NCELLED

ABR 63034–3
Defence FOI 553/20/21 Item 2 Document 1
4.8 Noting their increased level of responsibility, Petty Officers will require the ability to objectivelyexamine operations, identify potential risks and institute procedures to effectively manage those risks,thus mitigating the possible effects on personnel and assets. This requirement is met by providing thePetty Officer Management course (POMC) with the ‘OHS for Supervisors (Advanced)’ module. Themodule will focus on the application of Operational Risk Management techniques in theNaval environment.
4.9 Personnel who have completed OHS 1 Working Safely (EDP 400310) andOHS 2 Hazard Management (EDP 400870), or Unit Safety Coordinator (EDP 906080) shall be deemedto have met the requirements of OHS for Supervisors (Introduction) (EDP 420434).
Officer career progression training
4.10 The responsibilities placed upon Junior Officers, in many situations, match those expected ofSenior Sailors. Consequently, Junior Officers are to be educated to the same degree as memberscompleting the POMC. To achieve this objective the Junior Officer Leadership Course will incorporateboth the Introductory and Advanced modules of OHS for Supervisors.
OCCUPATIONAL HEALTH AND SAFETY COURSES
Navy safety training courses
4.11 The Navy OHS training courses were developed to align with a set of generic OHS courses,as follows:
Royal Australian Navy Ship safety management courses
4.12 The Director of Navy Certification and Safety—Surface Ships (DNCS–SS) conducts a courseentitled ‘Ship Safety Management and the Royal Australian Navy Regulatory Framework’ on a regularbasis. Course dates are notified by DEFGRAM, or can be obtained from DNCS–SS. The course isapplicable to personnel within and external to Defence including ship’s staff, acquisition, class logisticsoffices, Maritime Command Australia, Force Element Group staff, Safety Boards, OHS teams,classification societies, contractors and the broader maritime industry. On completion of the course,students will be able to:
a. Understand the rationale behind the importance placed upon safety management withinthe Navy from a legal, financial, community expectation, and operational perspective.
b. Understand the roles, responsibilities and expectations at all levels of all participantsinvolved in the management of safety for and within Navy;
c. Understand and experience the format and development of the Safety Case.
d. Understand the diversity of safety considerations and appreciate key areas in designand operational practice to avoid or mitigate safety hazards.
a. OHS Induction EDP No 100311 (old 400311) two hours
b. OHS 1 Working Safely EDP No 400310 (old 400310) two days
c. OHS 2 Hazard Management EDP No 100868 (old 400870) two days
d. OHS 3 Managing Safety EDP No 100309 (old 400309) one day)
e. OHS Supervisor (Int oduc ion) EDP No 105792 420434 (replacing OHS 1 and 2 IDC)
f. Unit Safety Coordinator EDP No 102835 (old 906080) four days
g. Advance OHS Management EDP No 103128 (old 910440) ten days
h. OHS Internal Auditing EDP No 105793 (old 420435) five days
NCELLED

ABR 63034–4
Defence FOI 553/20/21 Item 2 Document 1
Civilian ship safety management course
4.13 DNCS–SS sponsors the conduct of a civilian ship safety management course which isdesigned to familiarise students with the fundamental requirements of ship’s safety managementsystems. The course is of five days duration. Further details of this course can be obtained fromDNCS–SS.
Marine Incident Investigator’s course
4.14 Director Navy Safety Systems sponsors a ‘Marine Incident Investigator’s course’, which isconducted as required to ensure Navy retains a pool of suitably qualified marine incident investigators.
REVIEW
Safety Training Review
4.15 The Defence Safety Management Agency has commenced a training review, which willexamine the needs of the entire Australian Defence Organisation. Navy safety training will be revieweddeveloped in light of the results of this examination.
NCELLED

ABR 6303 Defence FOI 553/20/21 Item 2 Document 1
CHAPTER 5
NAVSAFE HAZARD AND RISK MANAGEMENT
OVERVIEW
Risk management fundamentals
5.1 The Royal Australian Navy, as an organisation structured to fight and win in the maritimeenvironment, must manage risk as an integral part of doing business. Risk management, whether as aformally researched, quantified and in-depth analysis process (such as would be applicable for anacquisition project); or as a simple process conducted prior to commencing an every day activity, alwaysfollows the same basic principles which are described in this chapter. The differences lie in the level ofanalysis required, the longevity of the assessment, and the scope of what is to be achieved.
MAJOR REFERENCES
Australian Standard/New Zealand Standard 4360:1999—Risk Management
5.2 The current Australian Standard applicable to risk management is AustralianStandard (AS)/New Zealand Standard (NZS) 4360:1999—Risk Management. This standard provides ageneric guide for establishing and implementing the risk management process; which involvesestablishing context, identification, analysis, evaluation, treatment, monito ing and review, andconsultation and communication. The focus of this standard is not only upon the establishment of riskmanagement systems, but of the implementation of sequent al steps leading to continuousimprovement in decision making.
Australian Standard/New Zealand Standard 4804:1997—Occupational Health and Safety Management Systems—General Guidelines on Principles, Systems and Supporting Techniques
5.3 AS/NZS 4804:1997—Occupational Health and Safety Management Systems—GeneralGuidelines on Principles, Systems and Supporting Techniques is the standard which provides guidelinesto assist in the implementation, development, or improvement of an occupational health and safetymanagement system. As well as providing guidelines for the overall management of occupational healthand safety systems, some specific guidance on risk management is provided, including guidance on riskcontrol measures, adopted within Navy as the ‘Hierarchy of Controls’.
RISK MANAGEMENT PROCESSES
Overview
5.4 Risk management is a structured process whereby managers undertake, in sequence, stepsthat serve to identify and manage risks or hazards facing their organisation. At the upper levels ofcomplexity, risk management can be extraordinarily detailed, requiring specialist tools and advice, butat a lower level it is extremely relevant to the day to day management activities by non-specialists. Anunderstanding of risk management principles is fundamental to all safety management activities, and inmany circumstances is a legislative requirement.
5.5 The outcomes desired from the application of risk management within NAVSAFE are:
a. The identification and management of hazards before safety events occur.
b. Capitalisation upon lessons learned after near miss safety events.
c. Improved efficiency in the resolution of identified hazards through greater awareness,accountability and effective management oversight.
NCELLED


ABR 63035–3
Defence FOI 553/20/21 Item 2 Document 1
5.10 Establish the strategic context. In this process, a definition of the relationship between theoverarching organisation and its environment is established. Factors such as the operational, financial,legal, social, political, and public image environments should be considered. Internal and externalstakeholders should be identified, lines of communication set up with them, and their perceptions takeninto account. Potential stakeholders, in the Navy environment, could include:
a. individuals within Navy in the immediate organisation involved, associatedheadquarters, operational, administrative and training authorities;
b. Senior Navy and Corporate managers;
c. internal support and Enabling Executives;
d. external contractors and service providers;
e. regulators and other government organisations which have authority over the area ofexamination; and
f. through appropriate chains of command, media, interest groups, local communities, andsociety as a whole.
5.11 Establish the organisational context. This process should aim to obtain an understandingof the organisation or process and its capabilities, as well as the goals and objectives and the strategiesthat are in place to achieve them. For instance, if examining a whole of Navy subject, the Navy SafetyPolicy objectives would form part of the context, and in planning an operation, the commanders intentwould be a significant input. This organisational context is important for the following reasons:
a. Risk management takes place in the context of wider organisational goals, objectivesand strategies.
b. The impact of failure to achieve the objectives of the organisation, or the specific activityor project being considered is one of the sets of isk that will have to be managed.
c. The organisational poli y and goals help define the criteria by which the organisationalrisk threshold can e de ermined
5.12 Establish the risk management context. A definition of precisely what part of the activity orprocess that it is intended to manage. This process involves:
a. defining what the project or activity is, and establishing it’s goals and objectives;
b. defining the extent of the project or activity in terms of time and location;
c. identifying any further information, studies or analysis required; and
d. defining the rigour of risk management that is required, including the level ofmanagement that will make risk acceptance decisions, and the degree to which the riskmanagement process will have to examine impact upon other activities.
5.13 Develop evaluation criteria. A decision of the criteria against which risk is to be evaluated.Decisions concerning risk acceptability and risk treatment may be based on operational, technical,financial, legal, social, humanitarian or other criteria. These often depend on an organisation’s internalpolicy, goals, objectives and the interests of stakeholders.
5.14 Structural definition.The project or activity should be divided into separate elements whichwill facilitate the analysis of all aspects of its intended use or purpose. The object of this process is toensure that sufficient detail has been examined in order to ensure that all potential hazards associatedwith the activity will be identified.
Identifying risks
5.15 It is important that the process used to identify hazards or risks is rigorous and meticulous. Awell structured process involving systematic analysis is vital, as hazards or risks that are notidentified in this stage will not be considered in later stages. Lack of application during this phasewill therefore carry a legacy into all remaining stages of risk management, leaving the process open tofailure.
NCELLED






ABR 63035–9
Defence FOI 553/20/21 Item 2 Document 1
Fundamental principles of Operational Risk Management
5.36 The principles of ORM are:
a. Accept risks only when the benefits outweigh the costs.
b. Do not accept any unnecessary risks.
c. Anticipate and manage risks by planning ahead.
d. Risk decisions should be made at the appropriate level (ie elevate decisions ifappropriate, or devolve responsibility to command best placed to execute theresponsibility).
5.37 Some key issues to consider on each of these points:
a. Risk is inherent in war fighting and is involved in every mission.
b. Risk is also related to gain; greater potential gain frequently requires greater risk.
c. Naval tradition is built upon principles of seizing the initiative and taking decisive action.The goal of ORM is not to eliminate risk, but to manage risk so that the mission can beaccomplished with the minimum amount of loss.
d. The acceptance of risk does not equate to the imprudent willingness to gamble. Takeonly risks which are necessary to accomplish the mission.
e. Risks are more easily controlled when identified early in the planning process.
f. Once it has been decided to take a on a risk, the use of ORM should decide on themanagement measures and controls required to red ce the probability of an adverseoutcome.
g. Risk decisions are made by the leader directly responsible for the operation. When theleader responsible for exe uting the mission determines that the risk associated withthat mission is too high or goes beyond the commander’s stated intent, they should seekadditional guidance.
Annexes:A. Hazard assessment—obtaining a Hazard Risk IndexB. Controlling risk—the Hierarchy of ControlsC. Risk management documentationD. Risk management terminologyE. NAVSAFE risk management elements
NCELLED


ABR 63035A–2
Defence FOI 553/20/21 Item 2 Document 1
Step 1—assessing likelihood
4. Having established context, the first step in the hazard assessment process is to assess thelikelihood of an event occurring. There are five levels used in the RAN model as described in table 5A–1below. Units conducting an assessment should look to the likelihood definition applicable to theINDIVIDUAL ITEM, although an assessment of the likelihood for the TOTAL RAN INVENTORY may beappropriate. If appropriate, the reason for arriving at this assessment should be documented.
Table 5A–1: Hazard likelihood
Step 2—assessing severity
5. The second step in the hazard assessment process is to assign an estimate of the severity ofthe outcome should the event being examined transpire. It is possible to have an event that, for example,would be catastrophic in its effect upon personne but render little or no damage to equipment, or havea minimal impact upon the ability to conduct the mission. For this reason the severity tables have beenseparated into hazard severities applicable to PERSONNEL, EQUIPMENT and MISSION. It will benecessary to specify which hazard severity table has been used if doubt may exist. In some cases, useof several Hazard Severity Tables may be warranted. This is described later in this annex.
Table 5A–2: Hazard Severity (Personnel)
DESCRIPTION LEVEL INDIVIDUAL ITEM TOTAL RAN INVENTORY
FREQUENT A Likely to occur REGULARLY.
CONTINUOUSLY experienced in the inventory.
PROBABLE B Will occur SEVERAL TIMES in the life of the item.
Will occur REGULARLY in the inventory.
OCCASIONAL C Unlikely but can be REASONABLY EXPECTED to occur in the life of the item.
Will occur SEVERAL TIMES in the inventory.
REMOTE D UNLIKELY but possible to occur in the life of the item.
Unlikely but can be REASONABLY EXPECTED to occur in the inventory.
IMPROBABLE E So unlikely it MAY NOT BE EXPERIENCED.
UNLIKELY to occur, but possible
DESCRIPTION CATEGORY MISHAP DEFINITION
CATASTROPHIC 1 Failure which could result in death or permanent total disability.
CRITICAL 2 Failure which could result in permanent partial disability, or temporary total disability in excess of 30 days.
MAJOR 3 Failure which could result in temporary partial disability less than 30 days, hospitalisation, emergency medical treatment, injury or illness eligible for compensation.
MINOR 4 Failure which could result in first aid or minor supportive medical treatment.
NCELLED
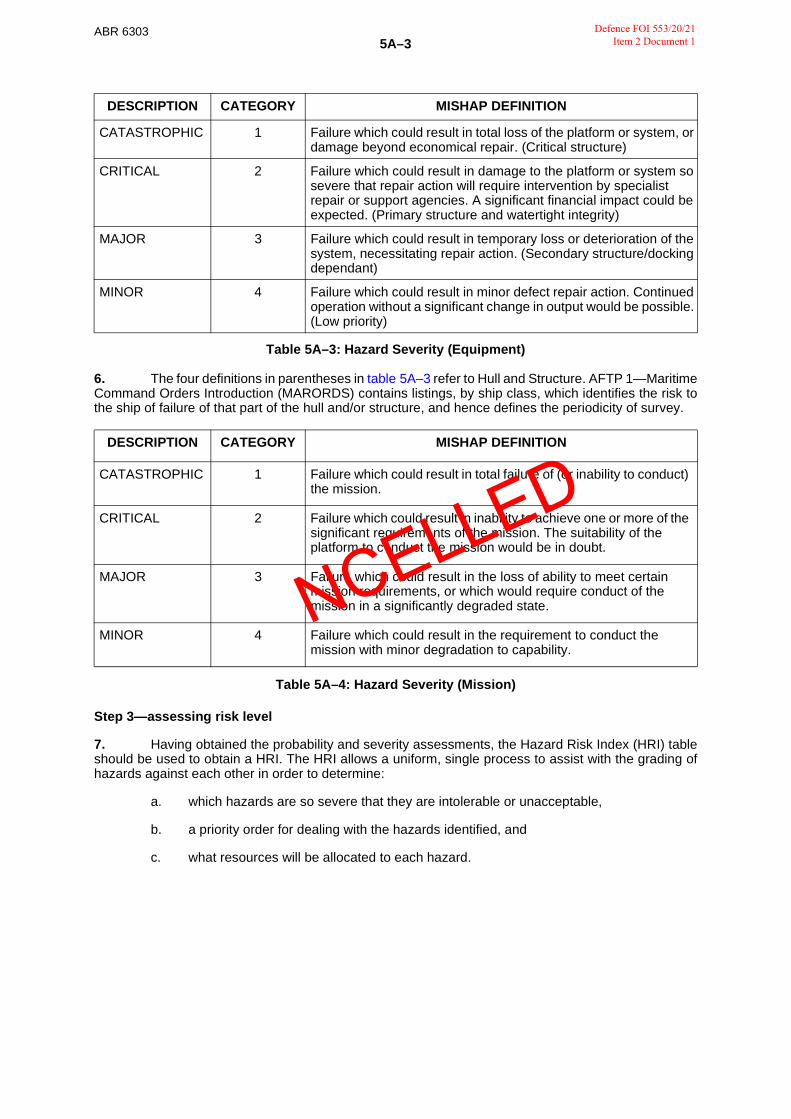
ABR 63035A–3
Defence FOI 553/20/21 Item 2 Document 1
Table 5A–3: Hazard Severity (Equipment)
6. The four definitions in parentheses in table 5A–3 refer to Hull and Structure. AFTP 1—MaritimeCommand Orders Introduction (MARORDS) contains listings, by ship class, which identifies the risk tothe ship of failure of that part of the hull and/or structure, and hence defines the periodicity of survey.
Table 5A–4: Hazard Severity (Mission)
Step 3—assessing risk level
7. Having obtained the probability and severity assessments, the Hazard Risk Index (HRI) tableshould be used to obtain a HRI. The HRI allows a uniform, single process to assist with the grading ofhazards against each other in order to determine:
a. which hazards are so severe that they are intolerable or unacceptable,
b. a priority order for dealing with the hazards identified, and
c. what resources will be allocated to each hazard.
DESCRIPTION CATEGORY MISHAP DEFINITION
CATASTROPHIC 1 Failure which could result in total loss of the platform or system, or damage beyond economical repair. (Critical structure)
CRITICAL 2 Failure which could result in damage to the platform or system so severe that repair action will require intervention by specialist repair or support agencies. A significant financial impact could be expected. (Primary structure and watertight integrity)
MAJOR 3 Failure which could result in temporary loss or deterioration of the system, necessitating repair action. (Secondary structure/docking dependant)
MINOR 4 Failure which could result in minor defect repair action. Continued operation without a significant change in output would be possible. (Low priority)
DESCRIPTION CATEGORY MISHAP DEFINITION
CATASTROPHIC 1 Failure which could result in total failu e of (or inability to conduct) the mission.
CRITICAL 2 Failure which could result n inabi ity to achieve one or more of the significant requirem nts of the mission. The suitability of the platform to c nduct the mission would be in doubt.
MAJOR 3 Fai ur which could result in the loss of ability to meet certain mission requirements, or which would require conduct of the mission in a significantly degraded state.
MINOR 4 Failure which could result in the requirement to conduct the mission with minor degradation to capability.
NCELLED

ABR 63035A–4
Defence FOI 553/20/21 Item 2 Document 1
8. The table used is as follows:
Table 5A–5: Hazard Risk Index
Step 4—assessing acceptability
9. Once the level of risk is determined using the HRI table, the final step in the process is todetermine the acceptability of the risk. Some levels of risk are so high that they are intolerable orunacceptable. These risks require urgent and immediate attention, and cessation of the activity orprocess is warranted in all but the most urgent operations.
Table 5A–6: Ac eptabil ty of Risk
Acceptability definitions
10. Using the system outlined above, hazards will be broadly categorised into the four levels ofRisk Acceptability. A guideline as to the implications of these levels of acceptability is as follows:
• Intolerable. Exposure to the hazard would normally be immediately discontinued except in extreme circumstances. The decision to continue exposure would almost certainly be made at senior levels, with as much risk management rigour as practicable, unless dire operational needs precluded doing so.
• Unacceptable. Exposure to the hazard would normally be discontinued as soon as is reasonably practicable. Continued exposure would only be considered in exceptional circumstances, and the decision to do so would normally be made at senior levels, after due consideration of the cost versus benefit.
• Acceptable with continuous review. Exposure to the hazard is acceptable provided it has been appropriately assessed, has been mitigated to As Low As Reasonably Practicable (ALARP), and is subject to continuous review to ensure the risk does not increase. It would be appropriate that measures to achieve long term further reduction to the risk be considered.
• Acceptable with periodic review. Exposure to the hazard is acceptable, but the hazard must be reviewed periodically to ensure the risk does not increase.
11. It is vital that the Risk Acceptability be considered in the management processes that willfollow. Risk treatment options described in annex B to this chapter should be followed, but forUnacceptable and Acceptable with Review hazards, it may be necessary to implement short-termprotective measures whilst longer term solutions are sought.
Hazard Severity
Hazard Likelihood CATASTROPHIC CRITICAL MAJOR MINOR
FREQUENT 1 3 7 13
PROBABLE 2 5 9 16
OCCASIONAL 4 6 11 18
REMOTE 8 10 14 19
IMPROBABLE 12 15 17 20
HRI Risk Level Risk Acceptability
1 to 5 Extremely high Intolerable
6 to 9 High Unacceptable
10 to 17 Medium Acceptable with cont nuous r view
18 to 20 Low Acceptable with period c eview
NCELLED


ABR 6303ANNEX B TOCHAPTER 5
Defence FOI 553/20/21 Item 2 Document 1
CONTROLLING RISK—THE HIERARCHY OF CONTROLS
1. Risk control can be conducted at a number of levels, and can often be dictated by factors suchas feasibility, financial constraints and operational constraints. Australian Standard/New ZealandStandard 4360:1999—Risk Management provides specific guidance on the options for treating risk,namely:
a. Risk avoidance. Treating the risk by deciding not to proceed with the activity whichgenerates the risk. Whilst appropriate in many circumstances, this process can lead torisk aversion under certain institutional conditions. Risk aversion may introducesignificant risk in itself, as procedures which must be employed or practiced are ignored,increasing the likelihood of failure at subsequent attempts.
b. Reduce likelihood. Reduction techniques designed to reduce the likelihood of anindividual event from occurring.
c. Reduce the consequences. Reduction techniques designed to reduce the impact ofpredicted events when they actually occur.
d. Transfer the risk. Useful predominantly outside the personnel safety environment, thisinvolves transfer of some of the burden for risk to other parties. Financial processessuch as insurance are a good example.
e. Retain risk. This describes the process in which residual risk is accepted and thereforeforms part of the business or procedural processes deliberately adopted by theorganisation.
2. It will not always be practical or feasible to abide by the processes mentioned above. Formateriel and safety management purposes, the processes us d to el minate mitigate known hazardsshould follow a structured process known as the ‘Hierarchy of Controls’ The purpose of this structure isto ensure that the method of treatment is the most effective that is possible in the circumstances.
3. The Hierarchy of Controls, in order of effectiveness, is as follows:
Table 5B–1: The Hierarchy of Controls
Rank Practice Description
1 Elimination A permanent solution that should be attempted in the first instance. Thehazard is eliminated altogether.
2 Substitution The process of replacing the hazard by another that represents lowerrisk. The hazards introduced by the replacement substance orprocedure must be carefully analysed.
3 Engineering Controls
Involves a structural change to the process or environment in order topace a barrier in, or interrupt the transmission path of a hazard.
4 Administrative Controls
Attempts to reduce or eliminate exposure to a hazard by requirementsto adhere to procedures or instructions. This can include changes tooperating procedures, or simple methods such as warning signs. Thevalidity, robustness and longevity of these procedures must beconsidered.
5 Personal Protective Equipment (PPE)
Worn by individuals as the last line of defence against a hazard. Thevalidity of PPE must be carefully monitored, as the hazard is stillpresent, and the protection is likely to be uncomfortable, and oftendebilitating, creating its own hazard.
NCELLED

ABR 6303ANNEX C TOCHAPTER 5
Defence FOI 553/20/21 Item 2 Document 1
RISK MANAGEMENT DOCUMENTATION
Introduction
1. Documentation for risk assessment and hazard management can take many forms. At themost formal level, a Safety Case is used for major acquisitions and projects, is introduced in theformative stages of the endeavour, and is a comprehensive document designed to live and grow throughall stages of design, acquisition, acceptance, service and disposal. Less formal documentation shouldbe as detailed as is necessary in order to fully record the risk management process undertaken, andshould generally comply with the format for a Safety Risk Management Plan as outlined in this annex.For every day activities which are subject to risk management processes, Operational RiskManagement (ORM), which will not normally be accompanied by significant documentation, may beappropriate. It must be stressed however that the level of documentation must be appropriate to the task,it is not acceptable to fail to document risk management processes by reverting to ORM when this is notappropriate.
2. The advantages of documentation in the risk management process are:
a. it provides a means of communicating the decision making process;
b. it assists in ensuring that all facets of the risk assessment process have been followedin a logical order, reducing the likelihood of significant oversight; and
c. it provides an auditable trail of the decision making process, and a defensible positionin the event of mishap.
Types of documentation
3. It is important to align the complexity of the documentation requirement, to the complexity ofthe risk management task. A balance must be struck between the requ rement to document the decisionmaking process, and the need to avoid adding bu densome and nnecessary administrative tasks whennot required. Many documents do not cover the entire gambit of the risk management process, andtherefore require different formats. The fol owing terminology is used on an Australian Defence Forcewide basis:
a. Risk Management Plan. A Risk Management Plan (RMP) is the method by which a riskmanagement endeavour utilising the full ‘six step’ process is formally documented. It isapplicable in Navy for most levels of documentation in which it is sought to demonstratethe rigour of a full risk management activity.
b. Safety Case. Safety Cases are sophisticated and comprehensive documents, whichdemonstrate how safety has been considered with regard to any system or equipment.Safety Cases show how hazards have been identified, managed and monitored throughthe life of the system or equipment. The safety case thus becomes a formal documentwhich demonstrates that due diligence has been given to the Occupational Health andSafety implications of the introduction into service of new equipment or systems, andfacilitates the management of hazards throughout the life of the equipment through todisposal. Further details of the Safety Case can be found in chapter 6—‘The SafetyCase’.
c. ORM. Although no formal documentation is required, it would be prudent to considerdocumenting in planning notebooks or the like, the decision making process used indetermining risk using ORM.
d. Standing Risk Profile (SRP). SRP is a completed risk management documentdesigned to be used as a guide for the conduct of activities within a given context. SRPcan be devised for specific activities that are repeated often, thus allowing minimisationof the time needed to complete risk assessments prior to an activity.
e. Risk Register. A Risk Register details the hazards and risks of a particular organisation,activity or situation, generally at the unit level. This function is currently performed byForm OS 006—Ships Occupational Health and Safety Log in Navy.
NCELLED

ABR 63035C–2
Defence FOI 553/20/21 Item 2 Document 1
f. Risk treatment and action plan. This plan documents the management controls to beadopted for each risk, and lists the person responsible for implementing the plan, theresources to be used, any budgetary allocation, the timetable for implementation, anddetails of the review plan intended.
g. Occupational Health and Safety Incident Report (OHSIR). This is a Navy onlyrequirement, and is used to alert higher authorities, and fellow ships or establishmentsthat might be affected, of any incident, near miss, or risk identification process that hashighlighted the need for management of a hazard. The OHSIR serves as theNavy ‘Exception Report’ (a term used in some Defence risk management processes),and more detail on the OHSIR system can be found in chapter 7—‘Accidents andincidents’.
Elements of a documented risk management process
4. A documented risk management process should include as much information as appropriateto the level formality of the assessment. A guide to the suggested format, appropriate to a fullydocumented risk management processes, is as follows:
a. Background. A description of the circumstances surrounding the risk managementactivity should be given. It is appropriate to describe the key organisations involved, andthe qualifications of personnel if required.
b. Context. This important step defines the environment and relationships of not only thesubject, but the risk assessment process. Detailed contextual guidance can be found inchapter 5—‘NAVSAFE hazard and risk management’.
c. Processes used to identify hazards. Describe fully the processes used to identifyhazards, including techniques and level of research The robustness of this phase iscritical, as hazards which are not identified are not treated later in the process.
d. Hazards identified. Describe each of the hazards that have been identified. It isimportant to list hazards before pr ceeding to the assessment and mitigation phases,as the interrelation between hazards must be clear during the forthcoming phases.
e. Hazard assessmen s. The method of risk analysis must be should described, includingthe tools used to determine likelihood and consequence. The process of evaluationshould then be considered including description of the evaluation criteria.Paragraphs 5.8 to 5.11, describes the assessment process in general and annex A tothis chapter describes the specific Navy hazard assessment process. The end productshould be an ordered list of hazards with rankings, which can be compared against apre-determined set of acceptability criteria.
f. Hazard controls. All control measures should be identified at this stage, even the onesthat at first glance do not seem appropriate, as the optimum solution is often acombination of control measures. It is appropriate to make recommendations, or indeedto decide at this point, as to the control measures to be used. Control measures whichinclude training or operating procedures in the mitigation process must be clearlyidentified.
g. Monitoring and feed back measures. A plan to review or receive feedback as to theeffectiveness of the control measures should be developed.
h. Communication plan. The (two-way) plan to communicate the changes or controlmeasures identified should be established.
i. Emergency procedures. If hazards cannot be eliminated, some level of residual riskwill have to be accepted. If this is the case, emergency procedures to deal with therealisation of residual risk should be identified.
NCELLED

ABR 6303ANNEX D TOCHAPTER 5
Defence FOI 553/20/21 Item 2 Document 1
RISK MANAGEMENT TERMINOLOGY
ALARP As Low As Reasonably Practicable.
Benefit The gain that is expected or achieved from the successful completion of an activity.
Consequence The outcome of an event expressed qualitatively or quantitatively, being a loss, injury, disadvantage or gain. There may be a range of possible outcomes associated with an eve.
Cost Cost of activities, both direct and indirect, involving any negative impact, including money, time, labour, disruption, goodwill, political and intangible losses.
Dangerous Occurrence An incident arising from an activity or task that could have resulted in death or serious personal injury.
Frequency A measure of the rate of occurrence of an event expressed as the number of occurrences of an event in a given time.
Hazard A source of potential harm, or a situation with a potential to cause loss.
Likelihood A qualitative description of probability or frequency.
Probability The likelihood of a specific event or outcome, measured by the ratio of specific events or outcomes to the total number of events or outcomes. Probability is expressed as a number between 0 and 1, with 0 indicating an impossible event or outcome, and 1 indicat ng an event or outcome that is certain.
Residual Risk The remaining level of risk after ri k trea ment measures have been taken.
Risk The chance of som thing h ppening that will have an impact upon objectives. It is measured in erms of consequence and likelihood.
Risk Acceptance An informed decisi n to accept the consequences and likelihood of a particular risk.
Risk Analysis A systematic use of available information to determine how often specified events may occur, and the magnitude of their consequences.
Risk Assessment The overall process of Risk Analysis and Risk Evaluation.
Risk Aversion A tendency of personnel to avoid risk without reference to organisational objectives or the reason for conducting an activity.
Risk Avoidance An informed decision not to become involved in a risk situation
Risk Control That part of risk management which involves the implementation of policies, standards, procedures and physical changes to eliminate or minimise adverse events.
Risk Decision The informed decision to accept, avoid or refer the residual risk associated with an activity; made by a commander, leader or individual responsible for assessing that activity.
Risk Evaluation The process used to determine risk management priorities by comparing the level of risk against predetermined standards, target risk levels or other criteria.
Risk Identification The process of determining what can happen, why and how.
Risk Level A qualitative or quantitative measure of risk, resulting from an assessment of potential damage to equipment or personnel; degradation of capability; sub-optimal completion of mission; or an adverse effect upon morale or professional image.
Risk Management The culture, processes and structures that are directed towards the effective management of potential opportunities and adverse effects.
NCELLED
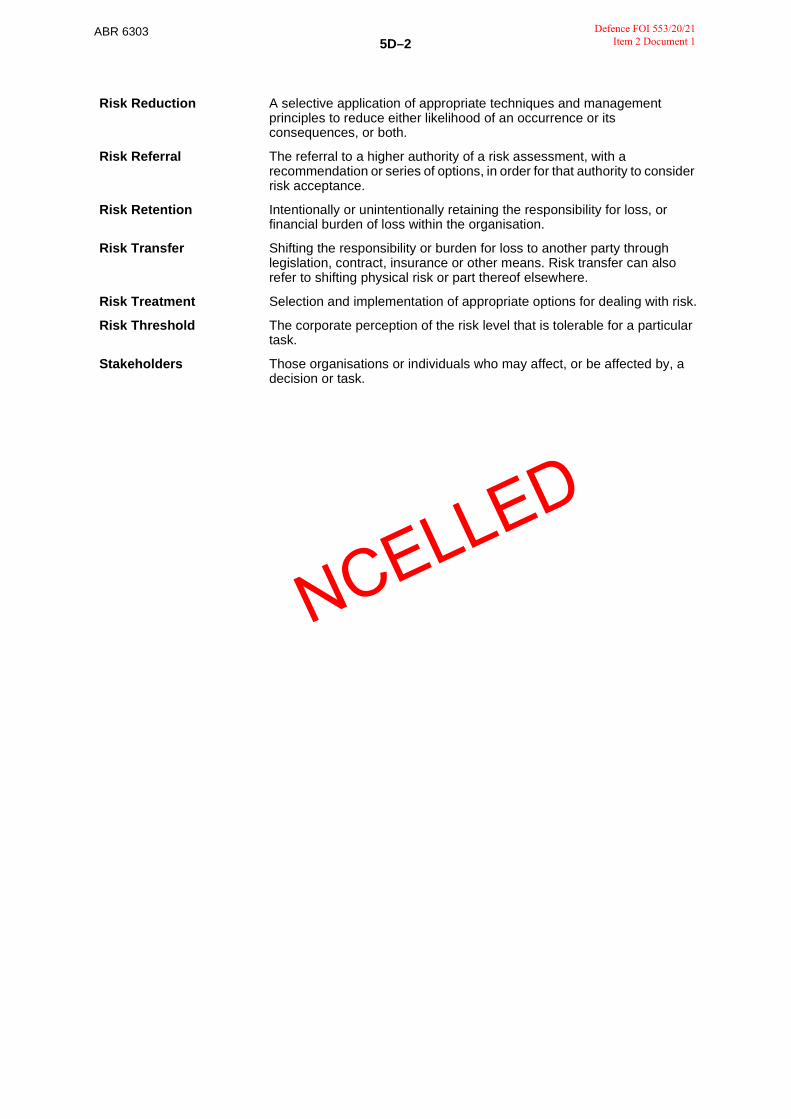
ABR 63035D–2
Defence FOI 553/20/21 Item 2 Document 1
Risk Reduction A selective application of appropriate techniques and management principles to reduce either likelihood of an occurrence or its consequences, or both.
Risk Referral The referral to a higher authority of a risk assessment, with a recommendation or series of options, in order for that authority to consider risk acceptance.
Risk Retention Intentionally or unintentionally retaining the responsibility for loss, or financial burden of loss within the organisation.
Risk Transfer Shifting the responsibility or burden for loss to another party through legislation, contract, insurance or other means. Risk transfer can also refer to shifting physical risk or part thereof elsewhere.
Risk Treatment Selection and implementation of appropriate options for dealing with risk.
Risk Threshold The corporate perception of the risk level that is tolerable for a particular task.
Stakeholders Those organisations or individuals who may affect, or be affected by, a decision or task.
NCELLED


ABR 6303 Defence FOI 553/20/21 Item 2 Document 1
CHAPTER 6
THE SAFETY CASE
OVERVIEW
What is a Safety Case?
6.1 Safety Cases are sophisticated and comprehensive documents, which demonstrate howsafety has been considered with regard to any system or equipment. Safety Cases show how hazardshave been identified, managed and monitored through the life of the system or equipment. The safetycase thus becomes a formal document which demonstrates that due diligence has been given to theOccupational Health and Safety implications of the introduction into service of new equipment orsystems1, and facilitates the management of hazards throughout the life of the equipment through todisposal.
6.2 The concept of the Safety Case was developed in the United Kingdom (UK) within industrieswhich were required to manage major industrial hazards, especially the nuclear and chemical industries.Their use has become widespread, and Safety Cases have been formally adopted by the2 UK Ministryof Defence for the design, construction, management, maintenance, operation and disposal of ships.
6.3 The Safety Case has a unique characteristic in that it is an acceptance that the directresponsibility for the ongoing management of safety is the responsibility of the operators, not theregulator. The Safety Case is, however, identical in concept to other less sophisticated risk managementdocumentation and accords with Australian Standard (AS)/New Zealand Standard (NZS) 4360:1999—Risk Management. The Safety Case serves two main purposes:
a. The regulator is provided with a confidence that the operator has the ability, commitmentand resources to properly assess and effectively control risks to the health and safetyof its personnel, and the general public.
b. The Safety Case provides a compr hensiv working document which facilitates audit ofthe safety management process The regulator and operator can check, using theSafety Case, that t e accep ed risk control measures and safety management systemshave been properly set up and are performing their intended function throughout the lifeof the platform or sys em.
Requirements of Safety Cases
6.4 It is a key requirement of the NAVSAFE system that initial ship or establishment facilities,systems and equipment designs, and any subsequent design changes are, and remain, inherently safegiven their role and purpose. They are also to be capable of safe maintenance and safe operation in theirintended role. This requirement has been recognised in more recent acquisition activities, which havemandated the requirement to adhere to the United States (US) Military Standard(MIL–STD)–882C—System Safety Program Requirements—January 19963. This standard was detailedand prescriptive, and was adopted commonly for acquisition within Defence. This standard has beensuperseded by US MIL–STD–882D—Standard Practice for System Safety, which takes a lessprescriptive approach.
6.5 It should be noted that safety cases are not yet a mandatory requirement for the acquisitionprocess. Goods and services delivered to Navy must satisfy legislative obligations under theOccupational Heath and Safety (Commonwealth Employment) Act 1991 (OHS(CE) Act 1991), and theassociated OHS(CE) (National Standards) Regulations, and the Navy Safety Case is the preferredmethod of demonstrating such compliance, for complex acquisition projects.
1 The Acceptance Into Naval Service (AINS) process is descr bed in Australian Book of Reference 6205—The Naval Test,Evaluation and Acceptance Manual.
2 JSP 430—Ministry of Defence Ship Safety Management Code.
3 US MIL–STD–882C.
NCELLED

ABR 63036–2
Defence FOI 553/20/21 Item 2 Document 1
6.6 Navy also has a requirement for an effective safety management system, and the adoption ofproven standards (Royal Australian Navy (RAN), commercial or in use with allied navies) is seen assensible practice. Notwithstanding, foreign safety management standards do not meet all Australianrequirements, and as such the Navy Safety Case has been modified from its parent documents in orderto ensure compliance with the following:
a. OHS(CE) Act 1991;
b. OHS(CE) (National Standards) Regulations—Statutory Rules 1994;
c. AS/NZS 4360:1999;
d. AS/NZS 4804:1997—Occupational health and safety management system—Generalguidelines on principles, systems and supporting techniques;
e. AS/NZS 4801: 2001—Occupational health and safety managementsystems—Specifications with guidance for use.
ELEMENTS OF THE NAVY SAFETY CASE
Core components
6.7 The Navy Safety Case contains the following elements, as a minimum:
a. Ship/facility description.
b. Formal Safety Assessment (FSA), incorporating:
(1) hazard identification,
(2) hazard analysis,
(3) risk evaluation,
(4) hazard control.
c. safety management system;
d. emergency/contingency arrangements;
e. Safety Case report; and
f. communication plan.
Ship/facility description
6.8 The first element of any risk management process, as outlined in AS/NZS 4360:1999, is toestablish the context within which the hazard management process will be conducted. A thoroughunderstanding of the strengths, weaknesses, intended employment and threats to the system isrequired. The ship/facility description should therefore define the context for the Safety Case.
6.9 The ship/facility description should consider the various contexts affecting the subject of theSafety Case, in accordance with AS/NZS 4360:1999. There is no requirement for the analysis of contextto form a distinct and separate section of the ship/facility description, provided the following contextsfrom AS/NZS 4360:1999 are considered fully:
a. The strategic context—the relationship between the equipment or organisation and itsenvironment, considering factors such as finance, operations, political implications,public image, and legal aspects.
b. The organisational context—the capabilities, structures and goals of the organisationwithin which the equipment or system will operate. This will enable the consideration ofrisk management within the context of the wider goals of the parent organisation. It willalso highlight the implications of failure of the equipment or system on the organisation,and establish the criteria by which it is decided whether a risk is acceptable or not.
NCELLED

ABR 63036–4
Defence FOI 553/20/21 Item 2 Document 1
6.14 This process must include analysis of what can happen, then how and why it can happen. Acomprehensive list of events which might occur should be constructed, then an analysis of the ways inwhich an event can be initiated should be conducted. All parts of the system must be examined, includingdesign, maintenance, and operation. All hazards should be presented, including those consideredremote.
Hazard analysis
6.15 All hazards should then be analysed, with the aim of establishing the following:
a. the existing controls in place;
b. the likelihood of the hazard or risk being realised;
c. the consequence(s) of the hazard or risk being realised; and
d. from this an estimate of the level of risk.
Hazard evaluation
6.16 Hazards should be analysed with their existing hazard controls and evaluated using anappropriate Hazard Risk Index (HRI) which complies with AS/NZS 4360:1999. The RAN preferredHRI table is demonstrated in chapter 5—‘NAVSAFE hazard and risk management’, but any analysis toolappropriate to the Safety Case at hand may be used. The combined effect of interrelated hazards shouldalso be considered, especially the cumulative effect of seemingly minor hazards which could betriggered simultaneously or sequentially.
Hazard controls
6.17 The options for the treatment of the hazards should then be determined. Measures used toremove, mitigate or control the consequences should be documented. Particular attention must be paidto the key hazards and features of emergency sys ems Any hazards which will be controlled by trainingor operating procedures should be clearly dentified at this stage, as they will form an essential part ofthe Safety Case report. Any quantitat ve or quali ative analysis of hazard treatment options, andassumptions made, is to be included in the Safety case report.
6.18 Appropriate hazard controls should be determined through the use of the Hierarchy ofControls, which is described in detail in chapter 5. Summarised, they are (in order of priority):
a. elimination of the hazard,
b. substitution of the hazard,
c. engineering controls,
d. administrative controls, and
e. personal protective equipment.
6.19 It must be borne in mind that at the concept and design phase, reaching the higher levels ofthe Hierarchy of Controls involves significantly less cost than later in the process, especially afterconstruction. Once the ship or equipment has been constructed it becomes significantly more difficult tomake elimination of a hazard through design change possible. There is therefore a financial, as well assafety management, obligation to identify and manage hazards early in the acquisition process.
6.20 The mitigated HRI for all hazards must then be re-assessed with the controls in place. The newrisks inherited as a result of the proposed mitigation measures must be identified and assessed(omission of this step is a frequent and potentially hazardous error in risk management). All hazardsmust be reduced to levels ALARP. The principle of ALARP is described in chapter 5 and figure 5–1.
NCELLED

ABR 63036–5
Defence FOI 553/20/21 Item 2 Document 1
Safety management system
6.21 This section is to contain a written description of the safety management system to beestablished in order to ensure the requirements of the Safety Case are met. The safety managementsystem must be consistent with the NAVSAFE system, but should address the specific requirements ofthe ship/facility to ensure specific and unambiguous delineation of responsibility with respect to:
a. authority and responsibility for management of the Safety Case throughout the life of theship/facility; and
b. authority and responsibility for maintenance, Integrated Logistic Support, ConfigurationManagement and Certification of the ship/facility;
Monitoring and feedback measures
6.22 Measures should be determined to monitor and feedback the effectiveness of hazard controls.Feedback must be used to review and update the Safety Case. The process must facilitate amanagement and audit process, and must include the following:
a. A means by which hazards are recorded which is visible to key stakeholders.
b. A means by which the assessment process, including hazard analysis and hazardevaluation, is documented.
c. A facility to record the control measures decided upon.
d. A facility to track the implementation of the control measures, through to closure,including updated status reports which can be examined by man gers and auditors.
e. Details of residual risk which has been accepted, and any control measures put in placeto mitigate this risk. Control measures which i volve aining or operating proceduresmust be clearly identified.
Emergency procedures
6.23 Not all hazards can be elimin ted. For the residual hazards, emergency procedures andcontingency arrangements should be determined for response to the hazard eventuality. Emergencyarrangements must include equipment, operating procedures and training requirements as appropriate,and the requirements of each carefully examined to ensure maximum effectiveness in the actualenvironment in which the hazard could be realised.
Safety Case report
6.24 A Safety Case report is a summary document which references all key supportingdocumentation and shall contain the following:
a. An executive summary.
b. The hazards identified and their control measures.
c. Feedback, monitoring and reporting arrangements.
d. Emergency and contingency arrangements.
6.25 The Safety Case report is supplied to the ship or system controller as appropriate and willenable the operator to fully understand the hazards associated with the equipment or system. Bydefinition, the safety report must be dynamic, and must be capable of being updated as new hazards areidentified throughout the life of the system.
6.26 All hazards which have been mitigated through programs involving training or operatingprocedures must be highlighted and fully documented so that trainers and operators are completelyconversant with the requirements placed upon them.
NCELLED

ABR 63036–6
Defence FOI 553/20/21 Item 2 Document 1
Communication plan
6.27 A plan for communicating the contents of the Safety Case to stakeholders in the acquisition,operation, maintenance and management of the system must be developed. This must be a high projectmanagement priority.
NCELLED


ABR 63037–2
Defence FOI 553/20/21 Item 2 Document 1
h. Document the ship/unit and personnel activities for the previous 48 hours, to enabledetermination of factors such as fatigue or other stressors.
INCIDENT AND ACCIDENT REPORTING REQUIREMENTS
Statutory requirements
7.3 Section 68 of the Occupational Health and Safety (Commonwealth Employment) Act 1991(OHS(CE) Act 1991) requires that the following incidents be reported to Comcare:
a. An accident that causes the death of, or serious personal injury to, any person.
b. An accident that causes an employee who performs work in connection with theundertaking to be incapacitated from performing work for a period of 30 days.
c. A dangerous occurrence (which could have resulted in events described insubparagraphs a. or b.
7.4 Section 7 of the OHS(CE) Act 1991 ensures that the Act is not prejudicial to Australia’sdefence. This section allows the Chief of Defence Force (CDF) to exercise the right to declare thatcertain provisions of the Act do not apply or apply subject to modification and adaptation. With respectto reporting requirements, CDF has declared that Section 68 of the Act does not apply to members ofthe Australian Defence Force (ADF) who are involved in:
a. ADF operational deployments;
b. ADF deployments in support of the United Nations (UN), or;
c. organised ADF sporting activities.
Comcare and Defence Safety Management Agency functions
7.5 Comcare is the authority establ shed under the Safety, Rehabilitation and CompensationAct 1998 and is responsible for reg lating compliance with the OHS(CE) Act 1991 Comcare require thereporting of incidents outlined in paragraph 7.1. Comcare are also charged with powers to investigate,and to make recommendations or rulings based on the outcome.
7.6 The Defence Safety Management Agency (DSMA) is the authority responsible for collatingaccident and injury data for the ADF. This is managed through a system known as DEFCARE. TheDEFCARE database provides information on compensation and rehabilitation, and is used to assesstrends and developments in ADF injury rates. It is therefore essential that all reportable incidents beentered into this database.
Australian Defence Force reporting requirements
7.7 The single form used to record accidents and incidents (to satisfy ADF wide requirements) isForm AC 563—Incident and Fatality Report. The additional Navy specific reporting requirements,designed to facilitate proactive hazard reduction, are described later in this chapter.
Command responsibility
7.8 Commands are to ensure that an effective system is in place that ensures all reportingrequirements outlined in this chapter are met.
Defence Report—Form AC 563
7.9 Form AC 563 must be completed to record any workplace injuries in the ADF. The form isrendered to DSMA on all occasions, and to Comcare for instances of death, serious personal injury,incapacity or near miss events which could have resulted in the aforementioned. This requirement isoutlined in table 7–1.
NCELLED


ABR 63037–4
Defence FOI 553/20/21 Item 2 Document 1
7.16 An OHSIR should be raised in any of the following circumstances:
a. a hazard is realised; ie a person or persons are injured;
b. a hazard near miss event occurs; or
c. a hazard is identified; ie a potential hazard is detected through inspection, riskassessment or any other appropriate method.
7.17 It is important to note that the OHSIR system is not to be used to lay blame. The OHSIR shouldbe raised in support of the Navy Safety Policy objective of an open reporting regime.
7.18 The OHSIR should take the following format:
a. Paragraph 1 should detail the reporting unit name, and the sequential number of theOHSIR for the calendar year.
b. Paragraph 2 should give brief details of the date, time and location of the accident (ifappropriate), or detail of the method of risk analysis that led to the detection of thehazard.
c. Paragraph 3 should describe the serial, evolution or work being done at the time of theaccident or near miss (if appropriate), or detail the circumstances in which the identifiedhazard could be realised.
d. Paragraph 4 should give a ‘headline’ account of the consequences of the accident, nearmiss or identified hazard. The aim should be to identify the general category of thehazard for use in data collection and analysis.
e. Paragraph 5 should give a detailed account of the manner in which the hazard was (orcould be) realised, including precursors, contributing factors and sequence of events.
f. Paragraph 6 should outline the Command assessment of the failures which did (orcould) contribute to the h zard. It is important that this paragraph is not used to layblame. Thought sh uld be given to all of the contributing factors, including any one ofthe following: managem nt failures, design deficiencies, maintenance deficiencies,Integrated Logistics Support deficiencies, physical precursors (fatigue/alcohol/drug/strength etc), psychological precursors (mood/emotion etc), supervision, trainingdeficiencies, briefing deficiencies, process deficiencies or contractor/contractdeficiencies.
g. Paragraph 7 should outline the immediate actions taken, and that should be taken byother units exposed to the hazard, in order to effect immediate mitigation. Longer termactions should be listed in paragraph 10.
h. Paragraph 8 requires a statement as to whether a Comcare report has been submitted.Care should be taken that this paragraph is consistent with the reporting requirementsoutlined earlier in this chapter. An explanation of the reasons for this decision may beappropriate (eg a ship operating in support of the UN would report that a Comcare reportwas not raised, in accordance with paragraph 7.11).
NCELLED

ABR 63037–5
Defence FOI 553/20/21 Item 2 Document 1
i. Paragraph 9 requires that a Hazard Risk Analysis be conducted. It is important to notethat this requirement is satisfied by stepping through all aspects of the risk assessmentor Operational Risk Management process as appropriate. A Hazard Risk Index (HRI)cannot be properly assigned without looking at all aspects of the risk assessmentprocess. When assigning a HRI, the following must be considered:
(1) When determining Hazard Likelihood, the decision making process should bedetailed when it is not readily apparent.
(2) When determining Hazard Severity, the Hazard Severity Table used(PERSONNEL, EQUIPMENT, or MISSION) should be stated (seesub-subparagraph (3) below). The selection process should be detailed when itis not readily apparent.
(3) The overall HRI assigned (there may be more than one if risks to PERSONNEL,EQUIPMENT and/or MISSION are considered) may be abbreviated using theterms HRI(P), HRI(E) or HRI(M).
j. Paragraph 10 should identify whether or not it is within the capability of the individualunit to eliminate the hazard, or mitigate it to As Low As Reasonably Practicable(see chapter 5—‘NAVSAFE hazard and risk management’). If not, recommendations forelimination or mitigation should be made.
7.19 Addressees for the OHSIR should be as follows:
a. ACTION: The appropriate command or headquarters.
b. INFORMATION: Other units likely to be affected by the hazard, he appropriate ForceElement Group commander(s) of units affected by the hazard, other relevant operating,support and maintenance authorities, Maritime Headquarters Australia (MHQAUST) ifnot the action addressee, and DGNCSA. Inclus on of the latter two addressees ensuresthe information is entered into r levant databases. In all cases where MHQAUST isrequested to action Comcare repo ting requirements, it is to be an action addressee.HMAS WATSON should be an information addressee for OHSIR that should receiveSHORESAFE atte tion.
7.20 The SIC code used should be W2M/LAL/I2B. Precedence should be appropriate to the needto alert the relevant authorities and other units, and should ensure it matches Comcare reporting timeframes if appropriate. The message should be UNCLASSIFIED if possible, bearing in mind sensitivitiesthat may apply when personnel have been injured, and normal security protocols. Names of individualsshould not be mentioned in the OHSIR.
INCIDENT INVESTIGATION
Basic Elements
7.21 The key aim of an accident investigation is to identify control measures that will effectivelyprevent it happening again, or at least to minimise the likelihood of re-occurrence. Equally, considerationmust be given to developing a strategy that will assist the speedy rehabilitation of the injured worker(s),back into the work force.
7.22 The implementation of control measures will, in some way incur costs. It is therefore essentialthat an appropriate representative of management is involved in the investigation (to an appropriatedegree), to ensure decisions, in relation to expenditure of costs can be made to initiate the preventativeaction. There is no use in the investigation team recommending a control measure that is costprohibitive.
7.23 Instructions for completing accident or dangerous occurrence forms are contained in thischapter. The head of the ships safety team should assess each accident or dangerous occurrence anddetermine whether the accident or dangerous occurrence should be investigated by the entire team orby designated members. The findings of accident or dangerous occurrence investigations should includerecommendations for devising appropriate safety measures to prevent a similar occurrence.
NCELLED

ABR 63037–6
Defence FOI 553/20/21 Item 2 Document 1
Technique
7.24 Investigation team if an investigation team has not already been established, eg as a matterof ship’s standard procedure, the first thing required is the formation of such a team. The level of severityof the accident will assist to determine this; ie a fatality will require a high level of expertise, whereas aminor injury may only require a single investigator.
7.25 The most appropriate source of investigators will be the ship’s safety team plus personnel withparticular expertise in relation to the incident being investigated.
7.26 The investigation team may also be assisted by appropriate reference documents, egAustralian Book of Reference (ABR), Maintenance Schedules, Australian Standards (AS),Defect Records, Accident Records and Training Records.
7.27 Once a team has been formed, they should record details of the accident, visit the site andconsider taking photos or sketches. They should also make a recommendation on whether theequipment, etc involved in the accident can continue to be used in the immediate future.
Purpose of investigation
7.28 It is essential that all personnel are confident that the Navy’s purpose of investigatingaccidents/incidents is to prevent a re-occurrence and not to apportion blame. If this confidence exists,personnel are more inclined to assist with accurate information for the investigation. It should be notedthat the RAN also has a statutory responsibility to investigate accidents/incidents.
Witnesses
7.29 One of the most crucial elements to the success of the investigat on is to obtain, as soon aspossible, the names of any eye witnesses. Note that any person who heard about the accident fromanother person, is not an eyewitness, their account of the event is hea say’. Statements should beobtained from witnesses as a matter of priority.
7.30 The purpose of taking witness names is to eventually interview them, however, before anyinterview, the emotional state of the witness should be considered. The information you gather may bedistorted because the witness is emotionally upset from seeing the accident occur or they may be a closefriend of the victim, etc. Whilst cons dering this, it is also important to interview witnesses as soon aspossible to capture the events while they are still clear in their minds. The injured victim(s) of the accidentis also a witness.
7.31 When interviewing witnesses, investigators should try and re-construct the events occurringimmediately prior to the accident. As a guide, the following questions and examples, may assist:
• Overhead question, to open discussion, eg Where shall we start?
• Direct question, to gain information, eg Were you trained to operate ...?
• Relaxing question, to gain opinion, eg Would you like to comment?
• Reverse question, to encourage thought, eg Tell me your experiences?
• Factual question, to get the facts, eg When, how, who?
• Broadening question, to broaden discussion, eg What other factors were involved?
• Justifying question, to gauge a further perspective, eg Is that important though?
• Hypothetical question, to change discussion, eg Did we ever consider?
• Alternative question, to decide an alternative, eg What is the best solution?
NCELLED

ABR 63037–7
Defence FOI 553/20/21 Item 2 Document 1
The facts
7.32 Once witnesses have been interviewed and the accident scene inspected, the investigationteam should establish the accepted drill and procedure for what was being undertaken at the time of theaccident/incident and then compare the method used by those involved. The differences should revealany deficiencies in the document drill or procedure.
7.33 To establish the accepted drill or procedure, the investigation team may need to refer to writtendocumentation, ABR, Codes of Practice, AS, Industry Standards, etc or other RAN sources of expertise.
7.34 Other factors that may have contributed to the accident should also be gathered, such as:
• how long had the injured worker(s) been in the job;
• what training was given, (was it appropriate);
• environmental issues, eg heat, noise;
• design issues, eg height of working surface, location of controls;
• systems, eg lack of supervision;
• human issues, eg fatigue, disregarding (reasonable) instructions; and
• external stressors, eg family or financial problems.
The report
7.35 Once the investigation is complete, a report should be prepared that inc udes conclusions andrecommendations. The recommendations must set out pract cal solutions for the prevention of futureaccidents/incidents; an achievable time frame to implement the changes; and what interim measuresmay be implemented until the permanent solution is insta led.
7.36 For example, an accident/incident involvi g an unguarded machine will mean fitting it with aguard. The availability of the part, time nvolved n fitting it and the cost, could set back resolving thedeficiency in the short term. Given the fact that one person has already been injured, because of the lackof guarding, an interim measure must be suggested to prevent accidents/incidents until a permanentguard can be fitted. A suggested measure may include developing a written procedure with appropriatetraining for users of the machine and closer supervision until the matter is resolved. The riskmanagement processes outlined in chapter 5 should be used.
7.37 In preparing the report, the investigation team must be conscious of the fact that this document,when completed, is an official account of the accident/incident and will be made available to externalagencies (external to the ship), eg Maritime Command, Comcare, DGNCSA, and DSMA. This is not tosuggest they should omit sensitive elements of the report, however they should be prepared to stand bywhat has been presented as fact.
Royal Australian Navy marine incident investigators
7.38 The RAN has a number of trained marine incident investigators. These investigators mayassist in accident and incident investigations. MHQ or DGNCSA should be contacted to provideinvestigators if required.
COMCARE investigation
7.39 Comcare are the administrator of Commonwealth Occupational Health and Safety (OHS)legislation, and as such undertake regulatory, advisory and reporting activities and perform many of theSafety, Rehabilitation and Compensation Commission’s functions. Comcare have the right underSection 40 of the OHS(CE) Act 1991 to appoint a member of staff of Comcare, or other person havingOHS knowledge and experience, to investigate accidents and incidents and conduct audits ofDefence units. Such persons will carry an identity card, which identifies them as an investigator, carriestheir name, photograph and signature, and is signed and dated by the Chief Executive Officer ofComcare.
NCELLED

ABR 63037–8
Defence FOI 553/20/21 Item 2 Document 1
7.40 Navy ships and establishments are defined workplaces under the OHS(CE) Act 1991. A dulyappointed Comcare investigator may, to the extent that it is reasonably necessary to do so in connectionwith the investigation:
a. Enter at any reasonable time during the day or night, a workplace, and:
(1) search the workplace;
(2) inspect, examine, take measurements or conduct tests concerning the workplaceor any plant, substance or thing at the workplace; or
(3) take photographs, or make sketches, of the workplace or any plant, substance orthing at the workplace.
b. Require the owner, occupier, employee or contractor at the workplace to give theinvestigator reasonable assistance, to answer any questions put by the investigator, andto produce any documents requested by the investigator, in connection with the conductof the investigation.
c. Take possession of the plant substance or thing and remove it from the workplace, ortake samples of the substance or thing and remove it from the workplace.
d. Remove an immediate threat to the health and safety of any person.
e. Direct, in writing, that a workplace, plant or substance not be disturbed for a periodnecessary to allow inspection, examination, measuring or testing to take place.
f. Issue a Prohibition Notice.
g. Issue an Improvement Notice.
7.41 Classified compartments, and other a eas and systems governed by restricted accessprocedures, as laid down in the Security Manual (SECMAN) documents, cannot be entered without theappropriate security clearance and access control procedures. Requests to enter such areas should bepassed through appropriate command cha n, as should requests for release of classified documents.Defence Security Authority will ultimately deal with such requests, and will issue approvals or denials inwriting.
7.42 Formal communications between Comcare and the Australian Defence Organisation areaddressed to Head Defence Personnel Executive (HDPE), and staffed through DSMA. Requests forinformation from Navy will then be directed through Director Navy Safety Systems (DNAVSAFE).Generally, the appropriately delegated employer representative, HDPE, must sign responses toComcare. When commands are approached directly for information by Comcare, they should cooperatewith the request. DNAVSAFE should be informed and included as an information addressee oncorrespondence.
Annexes:A. Personnel safety event—checklistB. Occupational Health and Safety Incident Report format
NCELLED

ABR 6303ANNEX A TOCHAPTER 7
Defence FOI 553/20/21 Item 2 Document 1
PERSONNEL SAFETY EVENT—CHECKLIST
Event Action
Events which occur in areas not exempted by Chief of the Defence Force (CDF) declaration. For events where the CDF declaration is applicable, Commission for the Safety, Rehabilitation and Compensation of Commonwealth Employees (Comcare) is not informed, but all other reporting requirements are applicable.
Death • Make Safe (paragraph 7.1).
• Secure Evidence (paragraph 7.2).
• Fatal Casualty Message in accordance with Defence Instruction (General) (DI(G)) PERS 11–2—Notification of Service and Civilian Casualties (DI(N) PERS 31–39).
• Comcare and Defence Safety Management Agency (DSMA) by telephone (or through Maritime Headquarters if not possible) within two hours.
• Part 1 of Form AC 563—Incident and Fatality Report to DSMA within 24 hours.
• Occupational Health and Safety Incident Report (OHSIR) to inform other units of hazard (if appropriate).
• Part 2 to DSMA within 28 days.
Incapacity(30+ days)
• Make Safe (paragraph 7.1).
• Secure Evidence (paragraph 7.2).
• Notification of Casualty (NOTICAS) Message in accordance with DI(G) PERS 11–2 (DI(N) PERS 31–39) if appropriate.
• Comcare and DSMA to be facsimiled part 1 of Form AC 563 within 24 hours.
• OHSIR to inform othe u its of hazard.
• Part 2 of Form AC 563 to DSMA within 28 days.
Serious Personal Injury
• Make Safe (paragraph 7.1).
• Secure Evidence (paragraph 7.2).
• NOTICAS Message in accordance with DI(G) PERS 11–2 (DI(N) PERS 31–39) if appropriate.
• Comcare and DSMA to be facsimiled part 1 of Form AC 563 within 24 hours.
• OHSIR to inform other units of hazard.
• Part 2 of Form AC 563 to DSMA within 28 days.
Near Miss involving potential for above events
• Make Safe (paragraph 7.1) if appropriate.
• Secure Evidence (paragraph 7.2) if appropriate.
• Comcare and DSMA to be facsimiled part 1 of Form AC 563 within 24 hours.
• OHSIR to inform other units of hazard.
• Part 2 of Form AC 563 to DSMA within 28 days.
Incapacity (5 days or more, but 30 days or less)
• Make Safe paragraph 7.1if appropriate.
• Secure Evidence (paragraph 7.2) if appropriate.
• DSMA to be facsimiled part 1 of Form AC 563 within 24 hours if practicable, or at next reasonable opportunity.
• OHSIR to inform other units of hazard.
• Part 2 of Form AC 563 to DSMA within 28 days.
Minor accident or injury
Exposure to hazard
Disease
NCELLED

ABR 6303ANNEX B TOCHAPTER 7
Defence FOI 553/20/21 Item 2 Document 1
OCCUPATIONAL HEALTH AND SAFETY INCIDENT REPORT FORMAT
PRECEDENCE: ROUTINE or PRIORITY as applicable
FROM: Unit
TO: Appropriate Command Headquarters
INFO: Other units which may be affected by the hazardFEG Commanders affected by hazardAny other affected operating authoritiesAny appropriate project or sustainment officeDGNAVCERTSAFEMHQAUST (if not action addressee)HMAS WATSON (for matters affecting SHORESAFE)TA–LOG
CLASSIFICATION: (UNCLAS if possible)
SIC: W2M/LAL/I2B
SUBJ: HMAS (SHIP NAME) OHSIR
A. ABR 6303 chapter 7—‘Accidents and incidents’
1. Reporting unit name, and the sequential number of the OHSIR for the alendar year.
2. Brief details of the date, time and location of the accident ( f appropriate), or detail of the method of risk analysis that led to the detection of th hazard.
3. The serial, evolution or work being d ne at the t me of the accident or near miss (if appropriate), or detail the cir umstances in which the identified hazard could be realised.
4. ‘Headline’ account of the consequences of the accident, near miss or identified hazard. The aim should be to identify t e general category of the hazard for use in data collection and analysis.
5. Detailed account of the manner in which the hazard was (or could have been) realised including precursors, contributing factors and sequence of events.
6. Command assessment of the failures which did (or could have) contribute to the hazard. It is important that this paragraph is not used to lay blame. Thought should be given to all of the contributing factors, including any one of the following: management failures, design deficiencies, maintenance deficiencies, ILS deficiencies, physical precursors (fatigue/alcohol/drug/strength etc), psychological precursors (mood/emotion etc), supervision, training deficiencies, briefing deficiencies, and process deficiencies, or contractor/contract deficiencies.
7. Outline of the immediate actions taken, and that should be taken by other units exposed to the hazard, in order to affect immediate mitigation. Longer term actions should be listed in paragraph 10.
8. Statement as to whether a Comcare report has been submitted. Care should be taken that this paragraph is consistent with the reporting requirements outlined in ABR 6303, table 7–1. An explanation of the reasons for this decision may be appropriate (eg a ship operating in support of the UN would report that a Comcare report was not raised, in accordance with paragraph 7.11 of ABR 6303).
NCELLED

ABR 63037B–2
Defence FOI 553/20/21 Item 2 Document 1
9. Hazard Risk Analysis conducted. It is important to note that this requirement is satisfied by stepping through all aspects of the risk assessment or ORM process as appropriate. An HRI cannot be properly assigned without looking at all aspects of the risk assessment process. When assigning an HRI, the following must be considered:
a. When determining Hazard Likelihood, the decision making process should be detailed when it is not readily apparent.
b. When determining Hazard Severity, the Hazard Severity Table used (PERSONNEL, EQUIPMENT, or MISSION) should be stated (see subparagraph c. below). The selection process should be detailed when it is not readily apparent.
c. The overall HRI assigned (there may be more than one if risks to PERSONNEL, EQUIPMENT and/or MISSION are considered) may be abbreviated using the terms HRI(P), HRI(E) or HRI(M).
10. Assessment as to whether or not it is within the capability of the individual unit to eliminate the hazard, or mitigate it to As Low As Reasonably Practicable (see chapter 5—‘NAVSAFE hazard and risk management’). If not, recommendations for elimination or mitigation should be made.
NCELLED
ABR 6303 Defence FOI 553/20/21 Item 2 Document 1
GLOSSARY
Accident An undesired event which results in harm to people, damage to property/environment orloss to process. For the purposes of the Act, a reference to an accident also includes areference to the contracting of a disease. (Source: Defence Instruction (General)(DI(G)) PERS 19–2—Occupational Health and Safety (Commonwealth Employment)Act 1991—Implementation within the ADF).
Accident investigation team A team of personnel, directed to investigate an accident or dangerous occurrence, and todetermine to the best of their ability the causes of the accident or dangerous occurrence, andmake recommendation to prevent a recurrence. Refer chapter 7, annex B for details oninvestigation technique.
Appointing officer/authority The officer, under Defence (inquiry) regulations who appoints a Board of Inquiry.
AuditA systematic and independent examination to determine whether (safety) activities and relatedresults comply with the planned arrangements, and whether these arrangements areimplemented effectively, and are suitable to achieve objectives.
Certification A formal regime and set of processes to ensure the worthiness, fitness for service and safety ofmateriel during acquisition and in-service.
Contractor A private sector enterprise or the organisational elemen of Department of Defence (DoD) or anyother Government agency engaged to provide services o products within agreed limits specifiedby the Commonwealth of Australia.
Command climate Refers to all aspects of the ommand posture. This includes among other things the commandattitude, at all levels, toward safety nd the maintenance of standards, adherence to policies andprocedures, and the fair and honest (or at least consistent) enforcement of regulations, includingpunishment. The commanding officer squarely sets the tone for the command climate throughgoals and objectives and their implementation.
Consequence The outcome of an event or situation expressed qualitatively or quantitively, being a loss, injury,disadvantage or gain.
Convening officer/authority The officer, under this instruction, that convenes an Accident Investigation Team.
Dangerous occurrence an occurrence that places at risk, the health or safety of an employee at a workplace; oran occurrence that:a. arises from operations carried on at a workplace; andb. places at risk, the health or safety of another person at or near the workplace.
Without limiting the generality of this definition, the Occupational Health and Safety (CE) Act, Section 3 (2) specifies dangerous occurrences.
Employee Where the terms ‘employee’ and ‘personnel’ are used they refer to both uniformed members ofthe RAN and to civilian employees of DoD working in the Navy Group.
NCELLED

ABR 63032
Defence FOI 553/20/21 Item 2 Document 1
Executive words Executive words are used throughout this document to determine the required level of compliancewith the individual instructions contained herein:
Shall—Mandatory. All organisations and individuals must comply with the intent of the instruction.
Should—Highly Desirable. Compliance is not mandatory, however, organisations and individuals are advised to comply.
Fail safe A design feature that ensures that the system remains safe, or in the event of a failure will causethe system to revert to a state which will not cause an accident.
Hazard A condition that has the potential to cause injury or illness to personnel, or damage to equipment.
Hazardous substance Means a substance: a. that is described in the List of Designated Hazardous Substances [NOHSC: 10005 (1994)];
or b. that has been determined to be a hazardous substance by its manufacturer, in writing and
in accordance with the ‘Approved Criteria for Classifying Hazardous Substances’[NOHSC: 1008 (1994)].
Injury categories As per DI(G) PERS 19–2—Occupational Health and Safety (Commonwe lth Employment) Act1991 Implementation within the ADF.
InspectionA self examination of part or all of systems designed to manage safety within ships, submarines,establishments or other RAN units.
NAVSAFE The generic title of the RAN Safety Management Program and its major components. For exampleRAN Safety Council, SHIPSAFE Board, etc. It was introduced by Defence Instruction(Navy) OPS 60–20—The RAN Safety Program and is formalised by this Australian Book ofReference.
Near miss See definition for dangerous occurrence.
Probability The ratio of specific outcomes to the total number of possible outcomes.
Program A plan or policy to be followed.
Reasonably practicable When considering what is reasonably practicable the following should be considered: a. the severity of the hazard or risk in question; b. the state of knowledge about that hazard or risk and any ways of removing or mitigating that
hazard or risk; c. the availability and suitability of ways to remove or mitigate that hazard or risk; and d. the cost of removing or mitigating that hazard or risk.
Risk The probability and possible consequences of occurrence of injury or illness to personnel anddamage or loss of naval systems and equipment.
Risk assessment The process of evaluating the probability and consequences of injury or illness arising fromexposure to an identified hazard or hazards.
NCELLED

ABR 63033
Defence FOI 553/20/21 Item 2 Document 1
Safety The control of recognised hazards to attain an acceptable level of risk.
Safety case The demonstration, via written documentation, that a project has a safety management systemthat is capable of continually and systematically identifying hazards, conducting systematic riskassessment, and in so far as is reasonably practicable, eliminating or controlling the risk topersonnel or facilities.
Safety critical A system or function which is critical to the safe operation of platforms and systems, and theabsence or malfunction of which would pose an unacceptable level of risk to personnel orplatforms or other systems in the performance of assigned roles and missions.
Safety management system A structured and documented system for managing safety which outlines safety objectives,standards and adherence to standards which will allow personnel to effectively implement safetypolicy.
System A composite, at any level of complexity, of personnel, processes, procedures, materials, tools,equipment, facilities and software. The elements of this composite entity are used together in theintended operational or support environment to provide a capability to perform a given task orachieve a specific purpose, support, or mission requirement.
System safety The application of engineering and management principles, criteria and techniques to optimise allaspects of safety within the constraints of operational effectiveness, t me and cost throughout allphases of the system life-cycle.
System safety management A management discipline that defines sys em safety program requirements and ensures theplanning, implementation and accomplishment of system safety tasks and activities consistentwith the overall program req irements.
System safety manager Person responsible to program management for setting up and managing the system safetyprogram.
System safety program The combined tasks and activities of system safety management and system safety engineeringimplemented by project managers.
NCELLED

ABR 6303 Defence FOI 553/20/21 Item 2 Document 1
ACRONYMS AND ABBREVIATIONSABR Australian Book of Reference
ASOR Air Safety Occurrence Report
BOI Board of Inquiry
CN Chief of NavyCO Commanding Officer
DCN Deputy Chief of NavyDGNCSA Director-General Navy Certification Safety and Acceptance AgencyDSMA Defence Safety Management Agency
ISM Code International Safety Management Code for Ships
MFU Major Fleet UnitMHQ Maritime HeadquartersMWV Minor War Vessel
NAVSAFE The Navy Safety Management SystemNCSA Navy Certification Safety and Acceptance Agency
OHS Occupational Health and Safety OHS(CE) Act 1991 Occupational Health and Safety (Commonwealth Employment) Act 1991OHSIR Occupational Health and Safety Incident ReportORM Operation Risk Management
RADHAZ Radio Frequency Radiation Hazard
SST Ship’s Safety Team
NCELLED