in hospital predictive models - take heart...
TRANSCRIPT

In Hospital Predictive Models
Dana P. Edelson, MD MS, FAHA, FHMExecutive Medical Director for Inpatient Quality and Safety
Take Heart America– October 20, 2016
Disclosures
Employment:
• The University of ChicagoResearch support:
• National Heart Lung Blood Institute of NIH
• Philips Healthcare
Ownership interests:
• Founder & CEO, QuantHC
• Patent pending, ARCD.P0535US.P2
Other:
• Immediate Past Chair, Systems of Care Subcommittee,
American Heart Association
• Co-Chair, GWTG-R Adult Research Task Force
• Member, CDC Ward Sepsis Working Group
In-hospital vs out-of hospital cardiac arrest
Predicting IHCA | 3
Out-of-hospital cardiac arrest
VF
In-hospital cardiac arrest
Asystole
PEA

Etiology of in-hospital cardiac arrest
Predicting IHCA | 4
Respiratory failure
Hypotension
Cardiac ischemia
Arrhythmia Metabolic
Other/Unknown
Sandroni, Resus, 2004

Etiology of in-hospital cardiac arrest
Predicting IHCA | 5
Respiratory failure
Hypotension
Cardiac ischemia
Arrhythmia Metabolic
Other/Unknown
Sandroni, Resus, 2004

Hospitalization Time Course

5% of ward patients become unstable…
7
How do we find them quickly and efficiently?

Delays in recognition are costly
• 1 hr delay in ICU transfer
3% increased odds of
hospital death
• Transfer within 6 hrs saves 2
days in the ICU
8

Lessons learned from baseball
9

Traditional baseball stats
10

Sabermetrics: rethinking baseball statistics
11
Wins above replacement (WAR)
Additional wins a player’s team has achieved over expected without
that player
Traditional patient stats
12

What’s our WAR score equivalent?
Hillman, Lancet, 2005 13
Cardiac arrest AUC: 0.63

What’s our WAR score equivalent?
Modified Early Warning Score (MEWS)
14
Score 3 2 1 0 1 2 3
Respiratory rate (RPM) — ≤ 8 — 9-14 15-20 21-29 ≥ 30
Heart rate (BPM) — ≤ 40 41-50 51-100 101-110 111-129 ≥ 130
Systolic BP ≤ 70 71-80 81-100 101-199 ≥ 200
Temperature (°C) — ≤35 — 35.0-38.4 — >38.5 —
AVPU — — — AlertReact to Voice
React to Pain
Unresp
Subbe, QJM, 2001
Cardiac arrest AUC: 0.76

1
5
UK National Early Warning Score (NEWS)
Cardiac arrest AUC: 0.77

But we live in an era of data and computers
16

Running a paper-based tool on a computer is like …
17
Developing a predictive model for clinical deterioration

eCART 2TM – cubic spline logistic regression
n=269,999 admission from five hospitals
Churpek, AJRCCM 2014

eCART is more accurate than MEWS
Predicting IHCA | 20

The strongest predictors of deterioration
38
40
41
43
48
51
63
66
77
100
0 20 40 60 80 100
Glucose
White blood cell count
Blood urea nitrogen
Temperature
Pulse pressure index
Diastolic blood pressure
Systolic blood pressure
Age
Heart rate
Respiratory rate
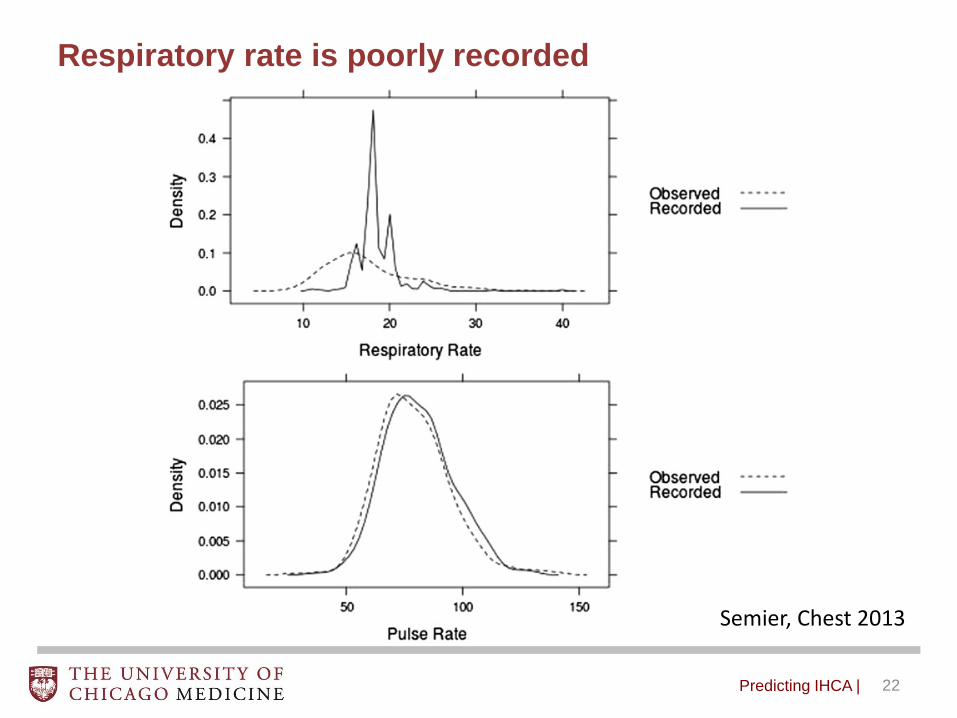
Respiratory rate is poorly recorded
Predicting IHCA | 22
Semier, Chest 2013

Respiratory rate
Ris
k
Churpek, CCM, 2016
Risk associated with respiratory rate is not linear
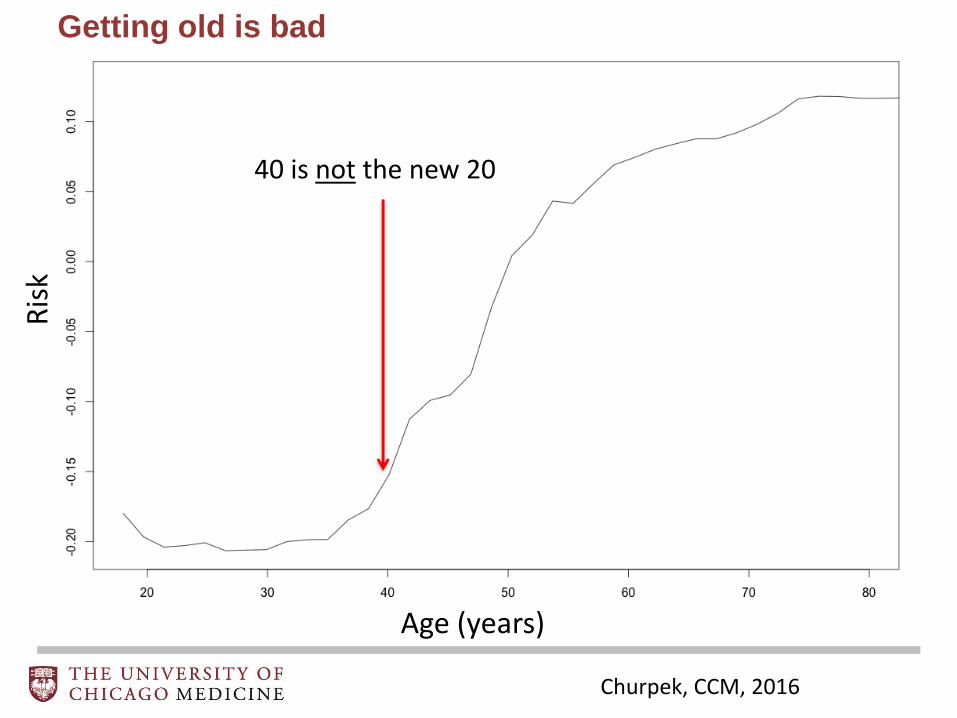
Getting old is bad
40 is not the new 20
Age (years)
Ris
k
Churpek, CCM, 2016

Age
20
40
60
80
100
Respiratory rate 20
40
60
Ris
k o
f Event
1.4
1.6
1.8
Predictors interact with one another

Real-time data-driven decision support in action

The University of Chicago Medical Center
617 beds
28,726 inpatient admissions
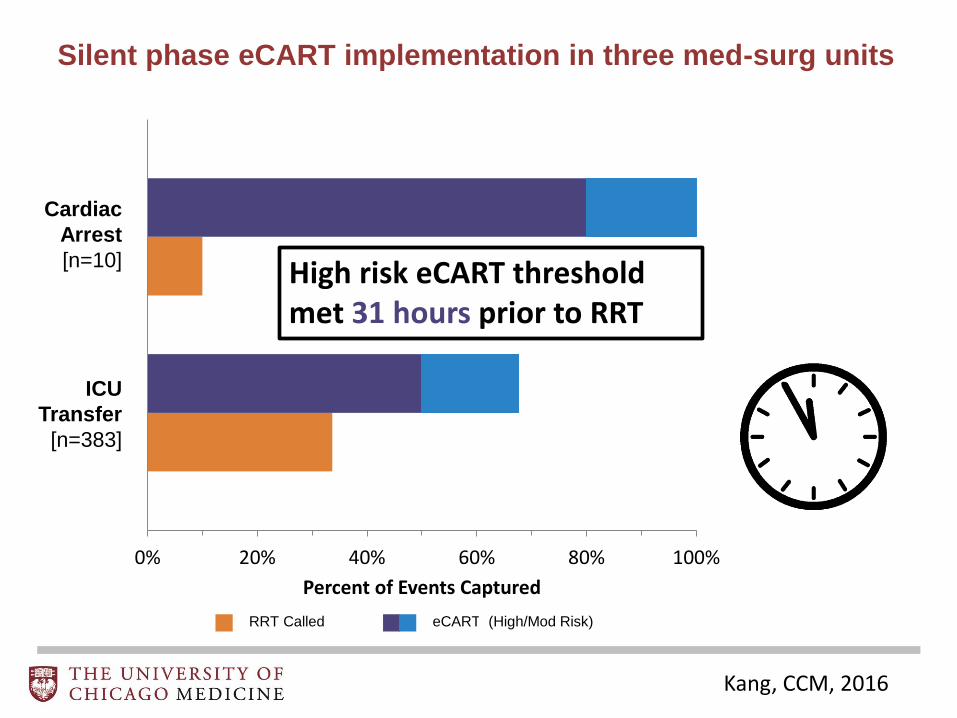
0% 20% 40% 60% 80% 100%
Percent of Events Captured
RRT Called
ICU
Transfer
[n=383]
eCART
Cardiac
Arrest
[n=10] High risk eCART threshold met 31 hours prior to RRT
(High/Mod Risk)
Silent phase eCART implementation in three med-surg units
Kang, CCM, 2016

Integrating risk prediction into the clinical workflow

Real-time Patient Dashboard

Integrating eCART into the EMR

Where does sepsis fit it?
Predicting IHCA | 32

3
3
SIRS criteria
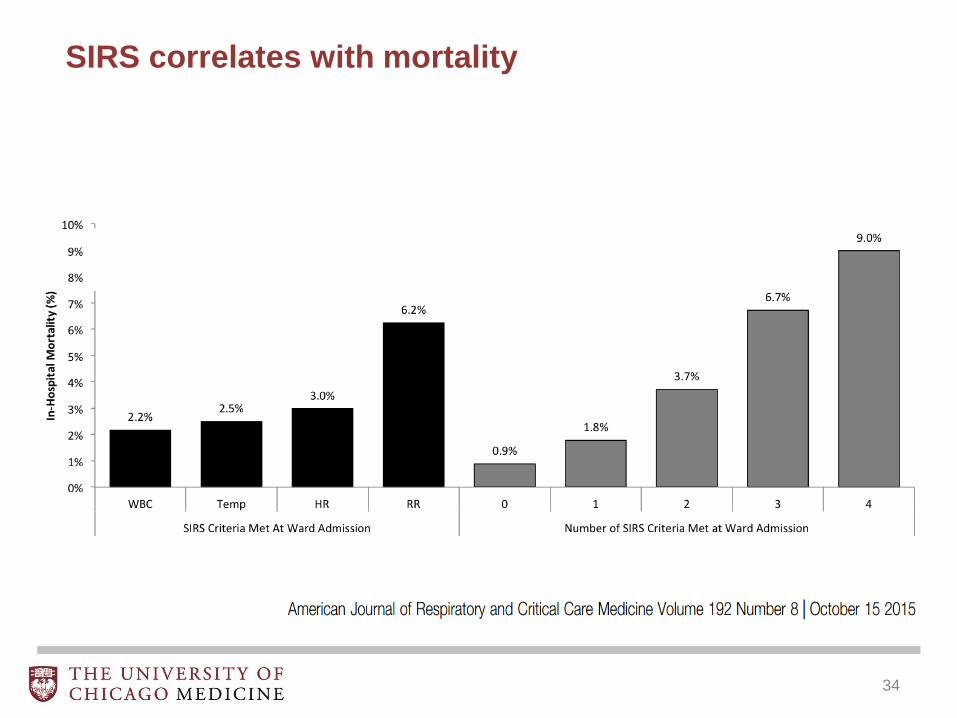
SIRS correlates with mortality
34

Most ward patients meets SIRS criteria at some point
35

New definitions for sepsis proposed
36


Predicting IHCA | 38
Don’t ditch your early warning scores for
SIRS or qSOFA!
Am J Respir Crit Care Med. 2016 Sep 20. [Epub ahead of print]

One size rarely fits all
39

From: A Prospective Study of Nighttime Vital Sign Monitoring Frequency and Risk of Clinical Deterioration
JAMA Intern Med. 2013;():-. doi:10.1001/jamainternmed.2013.7791
Nighttime vital sign monitoring
Predicting IHCA | 40
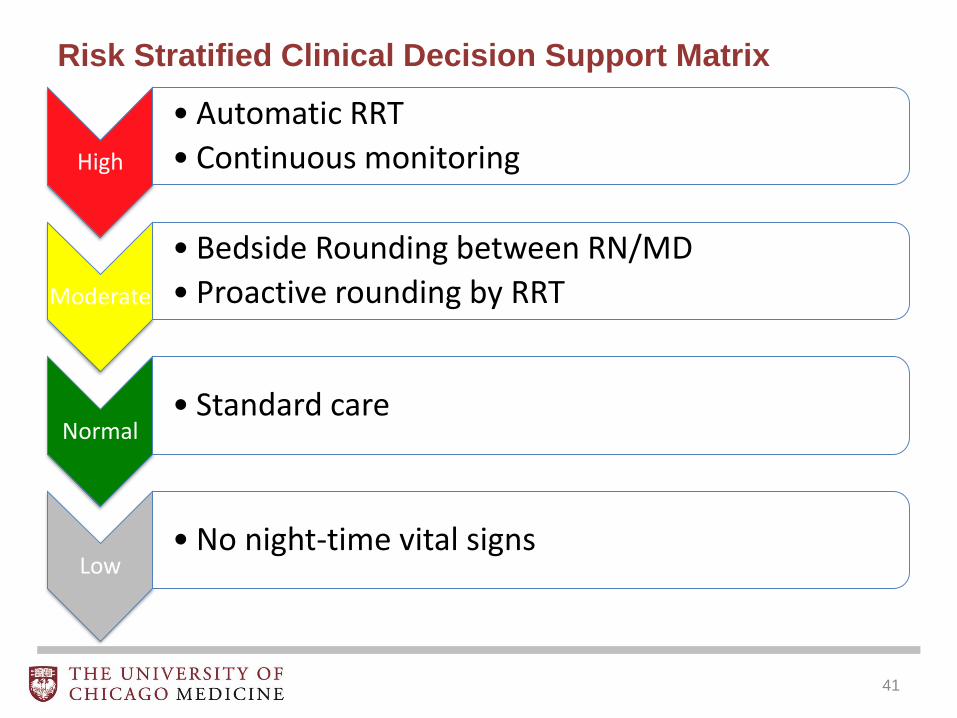
Risk Stratified Clinical Decision Support Matrix
High
• Automatic RRT
• Continuous monitoring
Moderate
• Bedside Rounding between RN/MD
• Proactive rounding by RRT
Normal• Standard care
Low• No night-time vital signs
41

Summary:
Cardiac arrest in the hospital is often
predictable and preventable
Real-time, data-driven decision support
to is possible today
Stop driving your Lamborghini in traffic!

ChicagoMay 11-12, 2017
hosted by
The 13th International Conference on Rapid
Response Systems and Medical Emergency Teams