improving prescribing quality richard seal programme director national collaborative medicines...
Post on 20-Dec-2015
219 views
TRANSCRIPT

Improving prescribing quality
Richard Seal
Programme Director
National collaborative medicines management services programme

Every system is perfectly designed to get the results it achieves ! Don Berwick, Institute for Healthcare Improvement

Unwanted medicines ?
Unwanted effects !
Brain-shakers
The majority of your problems derive from your systems, processes and methods, not from the workers
Changing the system will change what people do, changing what people do will not change the system
The majority of changes in organisations have nothing to do with improvement

Quality in prescribing ?

Prescribing with EASE
Effectiveness
Appropriateness
Safety Economy
Parish PADrug prescribing – the concern of allJ Roy Soc Health 1973;4:213-217
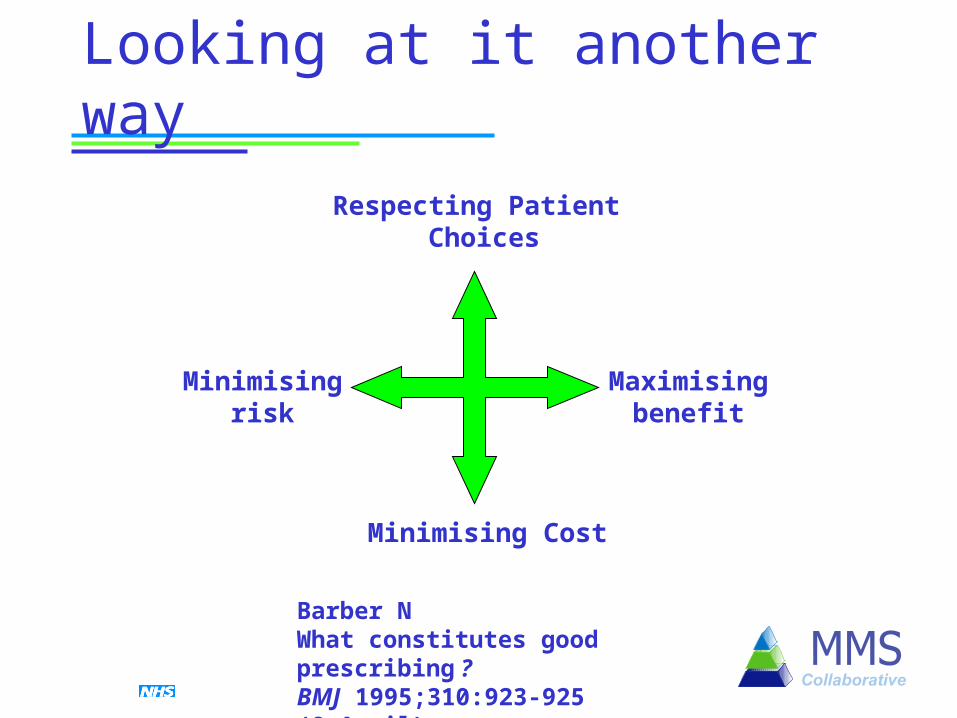
Looking at it another way
Respecting Patient Choices
Minimising Cost
Minimisingrisk
Maximisingbenefit
Barber NWhat constitutes good prescribing ?BMJ 1995;310:923-925 (8 April)

Problems with prescribing
• Inefficient management systems
• Inappropriate variation• Irregular review• Knowledge of the evidence
• Risks vs benefits• Lack of patient involvement
in decision-making• Medication errors

What’s a collaborative ?
“A proven improvement method that relies on spread and adaptation of existing knowledge to multiple settings to accomplish a common goal.”
…hence it is not a research project a passive exercise

The collaborative programme
Key elements of a collaborative
Challenging aims Identifying and sharing ideas which lead to
successful changes Testing and refining small changes Measuring progress Implementing and sustaining change
found to work
Goal and aims
“…optimise prescribing and improve health outcomes and patient experiences, where medicines are involved”– Identify and address unmet pharmaceutical need
– Help patients get more help with their medicines, thereby achieving real improvements in health
– Improve efficiency and reduce waste
– Better access to a range of medicines management services which make better use of skills of pharmacists

Collaborative StructureEach organisation will work towards the collaborative objectives
by developing and implementing their own locally acceptable models of work
‘EXPERT’Panel
0 41 to 3
Report & Rollout
Five Learning Sessions
LocalActions
LocalActions
LocalPrep
Support from core team

3 waves of activity
Wave 1 site
Wave 2 site
Wave 3 site
London Region

Improvement measures
Improvement not performance management
Reflect improvement activities in a number of areas
Teams develop additional local measures
4 practice level– Polypharmacy (med reviews from wave 2), equivalence and
compliance, safety, satisfaction
3 PCT level– Med review in NH, VFM & health improvement, discharge,

Practice level
Collected monthly from the 5 practices initially involved in the programme
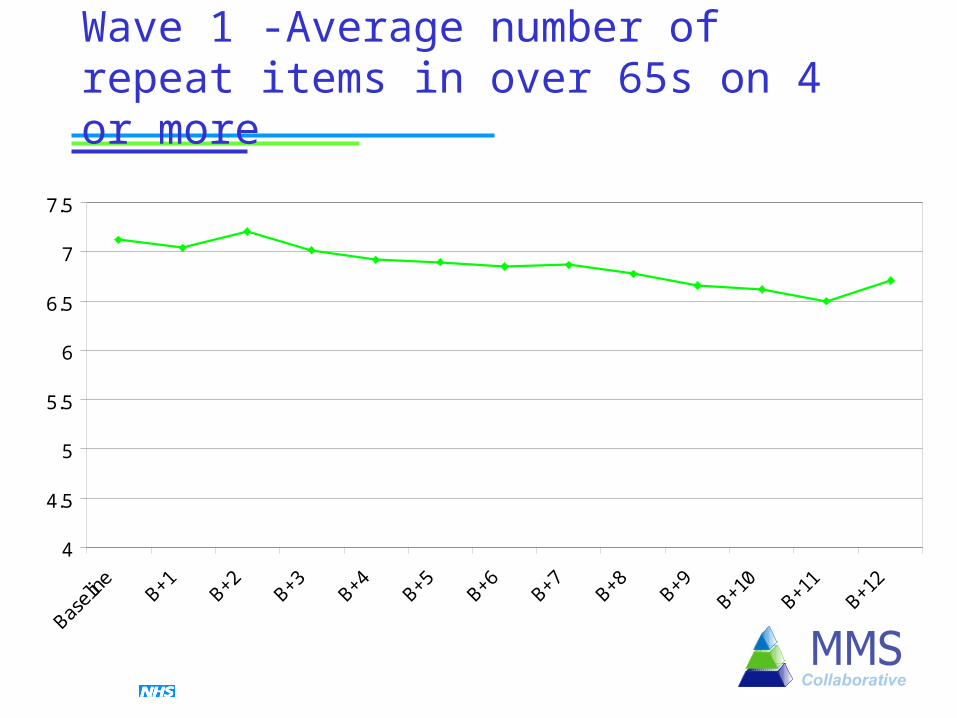
Wave 1 -Average number of repeat items in over 65s on 4 or more
4
4.5
5
5.5
6
6.5
7
7.5
Baseli
ne B+1 B+2 B+3 B+4 B+5 B+6 B+7 B+8 B+9B+1
0B+1
1B+1
2

Wave 2 - % over 65s with documented medication review in past 12 months
0
5
10
15
20
25
30
35
40
45

% scripts each month where not all regular items are requested
0
10
20
30
40
50
60
Wave 1Wave 2

% scripts leaving surgery without specific dose instructions
0
5
10
15
20
25
Wave 1Wave 2

% patients experiencing problems with repeat medicines
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
Wave 1Wave 2
PCT level
Collected monthly from practices across the PCT
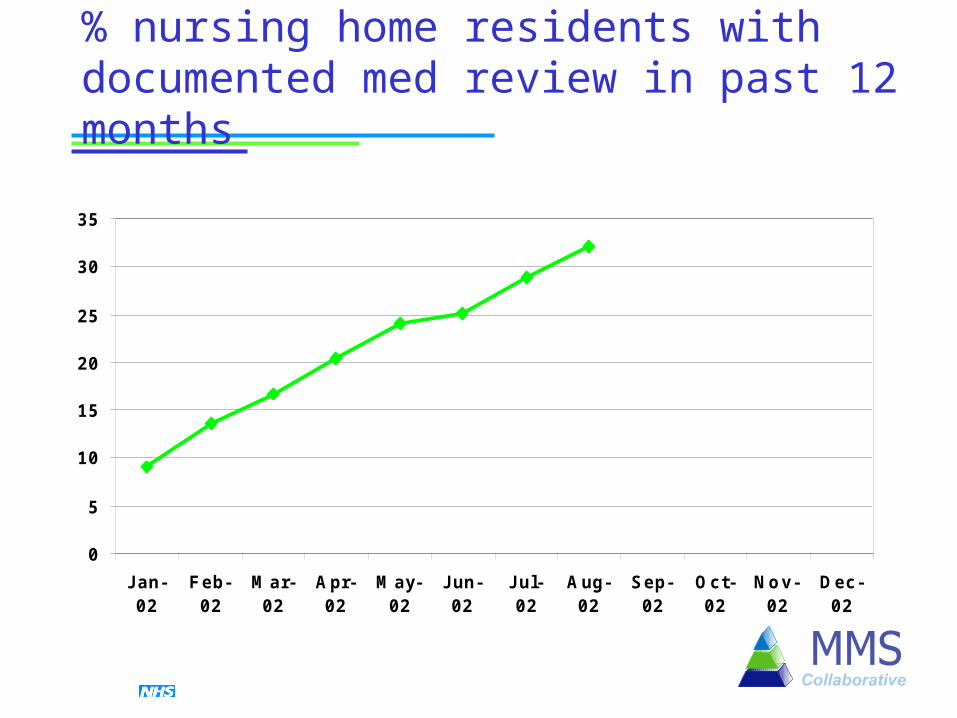
% nursing home residents with documented med review in past 12 months
0
5
10
15
20
25
30
35
J an-02
Feb-02
Mar-02
Apr-02
May-02
J un-02
J ul-02
Aug-02
Sep-02
Oct-02
Nov-02
Dec-02

Receipt of discharge info for 90% of patients before next request for medicines
0
10
20
30
40
50
60
J an-02
Feb-02
Mar-02
Apr-02
May-02
J un-02
J ul-02 Aug-02
Sep-02
Oct-02
Nov-02
Dec-02

Areas of improvement activity
General Practice
CommunityPharmacy
PCT
• Repeat prescribing processes• Medication review• Drug monitoring• Practice staff empowerment• Telephone consultations
• Medicines managers• Incentivised medicines management• Formulary development• Practice-based pharmacists• HIMP & NSF priorities• Care home services• Interface issues• Multidisciplinary teams
• Patient involvement• Workshops
• Prescription interventions• Medication review• Minor ailments• Services to practices• Enhanced DUMP campaigns• Patient education• Case-finding
What next
Range of spread activities
– Regional events and networks
– Partnership working
Wave 4 planning
Evaluation Identification of key
improvements for roll-out – Medication review
– Prescription intervention schemes
– Minor ailment schemes
– Repeat prescribing systems
– Medicines management in NSFs

Things to think about
All improvements require change but not all changes lead to improvement
Changes travel through conversation and interaction between trusted peers
Ideas that spread more rapidly– Relative advantage – “better than it is now”
– Compatible with existing beliefs and values
– Simple to understand and implement
– Easily tested before committing fully
– Observable difference

Final thought
“Great discoveries and improvements invariably involve the co-operation of many minds”
Alexander Graham Bell