improving peri-operative fluid management can it be … peri-operative fluid management can it be...
TRANSCRIPT

Aminda De Silva
Consultant Gastroenterologist
Royal Berkshire NHS Hospital Trust
Reading
Improving peri-operative fluid managementCan it be done?

Fluid Issues
• How can you take best evidence and apply this in the clinical setting?
• Share our experience
• Members of NSTs already familiar with fluid prescription problems in post-op patients
Consensus Meeting March 07BAPEN Medical, Association of Surgeons, SARS, Intensive Care Society and Renal Association.
Chair Jeremy Powell-Tuck (BAPEN Medical)
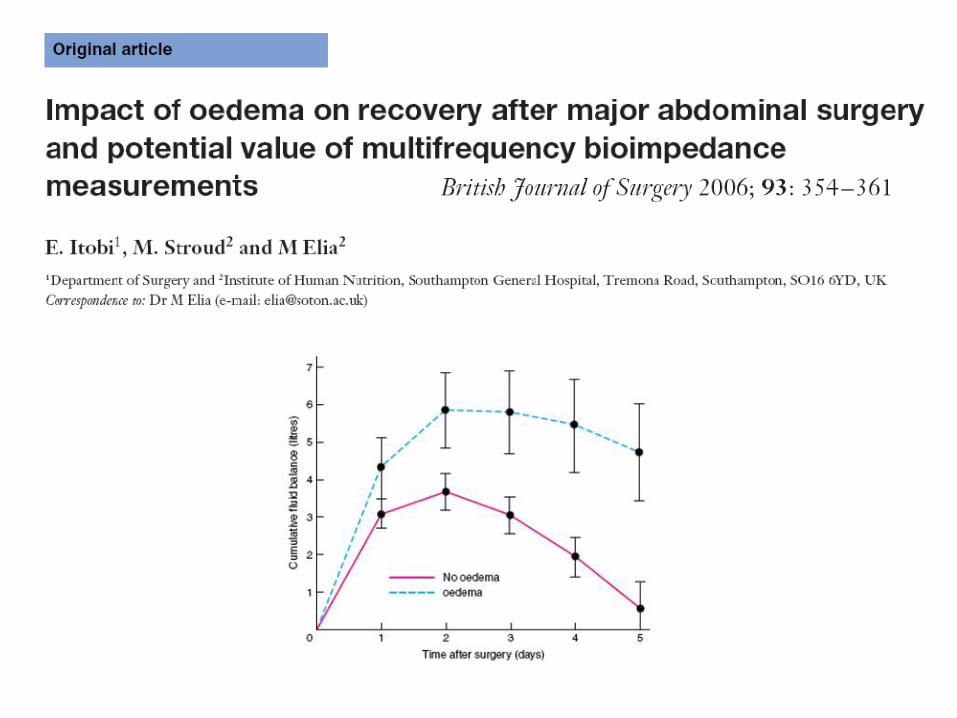
‘Limiting perioperative fluid + early oral intake improves organ function, clinical outcome and l.o.s in hepatic, oesophageal and GI surgery and burns’
Post Operative Fluid Management
Final Guidelines launched November 2008

Southampton University HospitalTrust Executive Committee
Oct 2007
• Possibilities for reducing unnecessary PN usage
• Surgical patients frequently receive too much sodium containing IV fluids
• Tasked with providing working guidelines and education to improve fluid prescription

SUHT Working Group to improve practice in peri-operative fluid prescribing
• Mike Stroud – Lead NST & Chair• Jim Smallwood & Roger House – Surgery• Max Jonas – ITU & Medical School• John Stubbing – Anaesthetics• Karen Hill – MEWS• Peter Austin – Pharmacy• Aminda De Silva – Nutrition Research Fellow
SUHT Fluids Working Group
• Meetings x 6 (Oct 07 – Nov 08)
• Educational initiatives• Local Guidelines• Drug charts• Medical Early Warning Score (MEWS)• Routine use of 0.9% saline

Education
• Key intervention
• Top down – Consultants• Bottom Up – Junior Doctors
– Structured 30 min presentation– Key evidence– Repeated!!!– Induction

Education
• At the end of a session– Understand why fluid balance is important– When & when not to use 0.9% saline– Be able to assess a patient– Incorporate biochemistry– Prescribe effectively
• Not enough on its own…
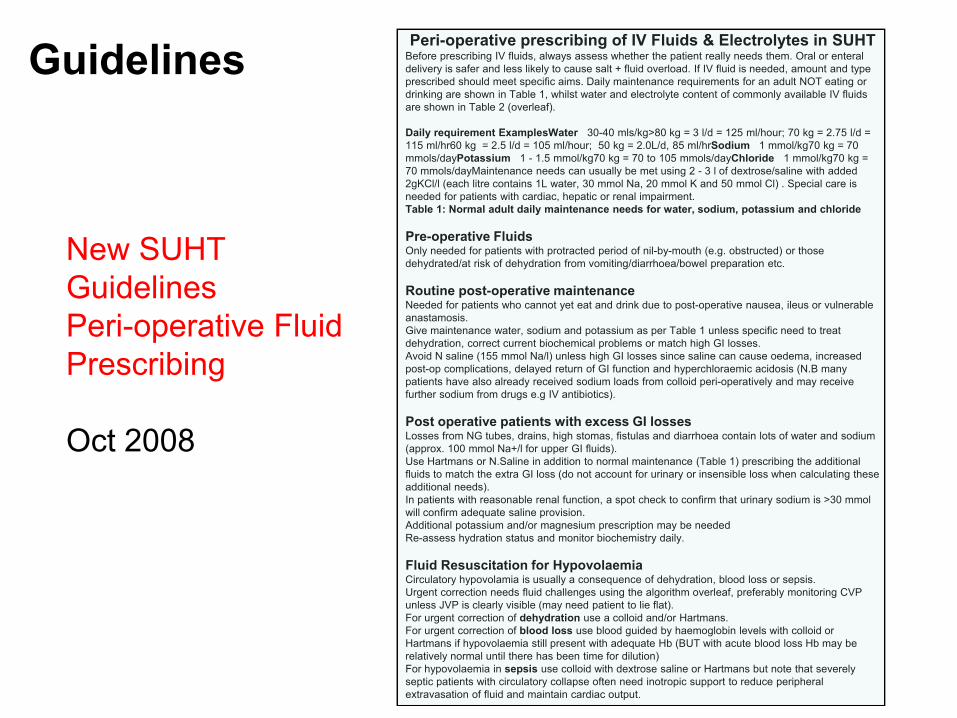
Peri-operative prescribing of IV Fluids & Electrolytes in SUHTBefore prescribing IV fluids, always assess whether the patient really needs them. Oral or enteral delivery is safer and less likely to cause salt + fluid overload. If IV fluid is needed, amount and type prescribed should meet specific aims. Daily maintenance requirements for an adult NOT eating or drinking are shown in Table 1, whilst water and electrolyte content of commonly available IV fluids are shown in Table 2 (overleaf).
Daily requirement ExamplesWater 30-40 mls/kg>80 kg = 3 l/d = 125 ml/hour; 70 kg = 2.75 l/d = 115 ml/hr60 kg = 2.5 l/d = 105 ml/hour; 50 kg = 2.0L/d, 85 ml/hrSodium 1 mmol/kg70 kg = 70 mmols/dayPotassium 1 - 1.5 mmol/kg70 kg = 70 to 105 mmols/dayChloride 1 mmol/kg70 kg = 70 mmols/dayMaintenance needs can usually be met using 2 - 3 l of dextrose/saline with added 2gKCl/l (each litre contains 1L water, 30 mmol Na, 20 mmol K and 50 mmol Cl) . Special care is needed for patients with cardiac, hepatic or renal impairment.Table 1: Normal adult daily maintenance needs for water, sodium, potassium and chloride
Pre-operative FluidsOnly needed for patients with protracted period of nil-by-mouth (e.g. obstructed) or those dehydrated/at risk of dehydration from vomiting/diarrhoea/bowel preparation etc.
Routine post-operative maintenanceNeeded for patients who cannot yet eat and drink due to post-operative nausea, ileus or vulnerable anastamosis.Give maintenance water, sodium and potassium as per Table 1 unless specific need to treat dehydration, correct current biochemical problems or match high GI losses. Avoid N saline (155 mmol Na/l) unless high GI losses since saline can cause oedema, increased post-op complications, delayed return of GI function and hyperchloraemic acidosis (N.B many patients have also already received sodium loads from colloid peri-operatively and may receive further sodium from drugs e.g IV antibiotics).
Post operative patients with excess GI lossesLosses from NG tubes, drains, high stomas, fistulas and diarrhoea contain lots of water and sodium (approx. 100 mmol Na+/l for upper GI fluids).Use Hartmans or N.Saline in addition to normal maintenance (Table 1) prescribing the additional fluids to match the extra GI loss (do not account for urinary or insensible loss when calculating these additional needs). In patients with reasonable renal function, a spot check to confirm that urinary sodium is >30 mmol will confirm adequate saline provision. Additional potassium and/or magnesium prescription may be neededRe-assess hydration status and monitor biochemistry daily.
Fluid Resuscitation for HypovolaemiaCirculatory hypovolamia is usually a consequence of dehydration, blood loss or sepsis.Urgent correction needs fluid challenges using the algorithm overleaf, preferably monitoring CVP unless JVP is clearly visible (may need patient to lie flat). For urgent correction of dehydration use a colloid and/or Hartmans.For urgent correction of blood loss use blood guided by haemoglobin levels with colloid or Hartmans if hypovolaemia still present with adequate Hb (BUT with acute blood loss Hb may be relatively normal until there has been time for dilution) For hypovolaemia in sepsis use colloid with dextrose saline or Hartmans but note that severely septic patients with circulatory collapse often need inotropic support to reduce peripheral extravasation of fluid and maintain cardiac output.
New SUHT GuidelinesPeri-operative Fluid Prescribing
Oct 2008
Guidelines

Summary of fluid guidelines
• Maintenance– Avoid ‘normal’ saline– restrict use to high gastric, stoma and other GI losses– 4%/0.18% dextrose saline + KCl maintenance
but flag danger of water overload– Consider Hartmann's solution
• Blood Loss– Colloid + Hartmann’s / Blood
• Sepsis– Colloid, Hartmann’s + inotropes
• Main difference from consensus– 4%/0.18% dextrose saline vs Hartmann’s

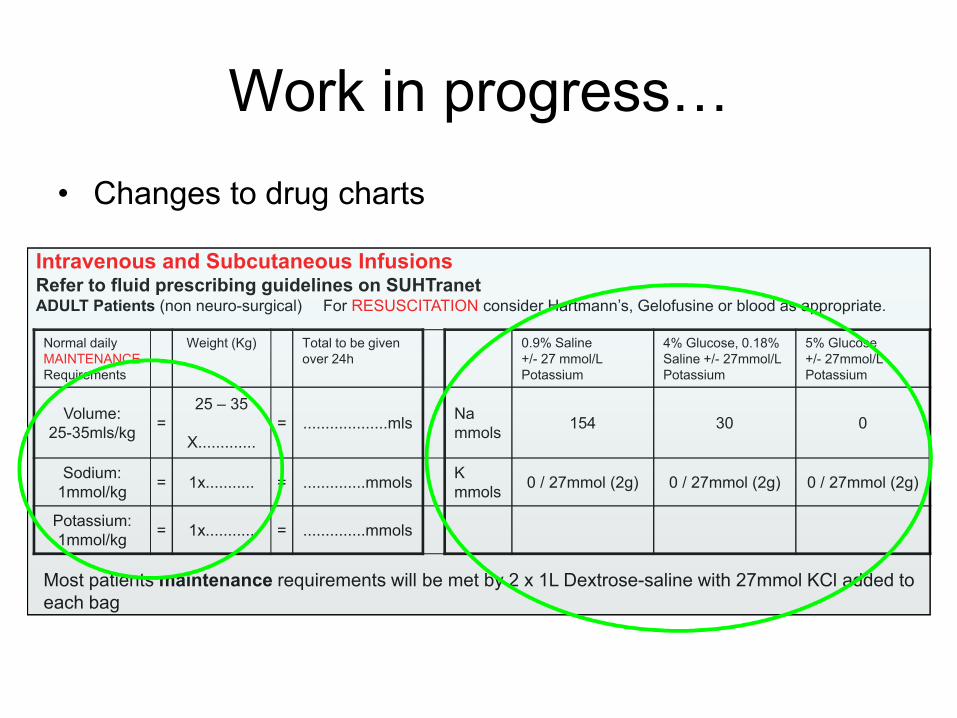
Work in progress…• Changes to drug charts
Normal dailyMAINTENANCERequirements
Weight (Kg) Total to be givenover 24h
0.9% Saline +/- 27 mmol/LPotassium
4% Glucose, 0.18%Saline +/- 27mmol/LPotassium
5% Glucose+/- 27mmol/LPotassium
Volume: 25-35mls/kg =
25 – 35
X............. = ...................mls Na
mmols 154 30 0
Sodium:1mmol/kg = 1x........... = ..............mmols K
mmols 0 / 27mmol (2g) 0 / 27mmol (2g) 0 / 27mmol (2g)
Potassium:1mmol/kg = 1x........... = ..............mmols
Intravenous and Subcutaneous InfusionsRefer to fluid prescribing guidelines on SUHTranetADULT Patients (non neuro-surgical) For RESUSCITATION consider Hartmann’s, Gelofusine or blood as appropriate.
Most patients maintenance requirements will be met by 2 x 1L Dextrose-saline with 27mmol KCl added to each bag
Work in progress…• Changes to drug charts
Normal dailyMAINTENANCERequirements
Weight (Kg) Total to be givenover 24h
0.9% Saline +/- 27 mmol/LPotassium
4% Glucose, 0.18%Saline +/- 27mmol/LPotassium
5% Glucose+/- 27mmol/LPotassium
Volume: 25-35mls/kg =
25 – 35
X............. = ...................mls Na
mmols 154 30 0
Sodium:1mmol/kg = 1x........... = ..............mmols K
mmols 0 / 27mmol (2g) 0 / 27mmol (2g) 0 / 27mmol (2g)
Potassium:1mmol/kg = 1x........... = ..............mmols
Intravenous and Subcutaneous InfusionsRefer to fluid prescribing guidelines on SUHTranetADULT Patients (non neuro-surgical) For RESUSCITATION consider Hartmann’s, Gelofusine or blood as appropriate.
Most patients maintenance requirements will be met by 2 x 1L Dextrose-saline with 27mmol KCl added to each bag

Work in progress…• Changes to drug charts
Normal dailyMAINTENANCERequirements
Weight (Kg) Total to be givenover 24h
0.9% Saline +/- 27 mmol/LPotassium
4% Glucose, 0.18%Saline +/- 27mmol/LPotassium
5% Glucose+/- 27mmol/LPotassium
Volume: 25-35mls/kg =
25 – 35
X............. = ...................mls Na
mmols 154 30 0
Sodium:1mmol/kg = 1x........... = ..............mmols K
mmols 0 / 27mmol (2g) 0 / 27mmol (2g) 0 / 27mmol (2g)
Potassium:1mmol/kg = 1x........... = ..............mmols
Intravenous and Subcutaneous InfusionsRefer to fluid prescribing guidelines on SUHTranetADULT Patients (non neuro-surgical) For RESUSCITATION consider Hartmann’s, Gelofusine or blood as appropriate.
Most patients maintenance requirements will be met by 2 x 1L Dextrose-saline with 27mmol KCl added to each bag

Work in progress…• Changes to drug charts
Normal dailyMAINTENANCERequirements
Weight (Kg) Total to be givenover 24h
0.9% Saline +/- 27 mmol/LPotassium
4% Glucose, 0.18%Saline +/- 27mmol/LPotassium
5% Glucose+/- 27mmol/LPotassium
Volume: 25-35mls/kg =
25 – 35
X............. = ...................mls Na
mmols 154 30 0
Sodium:1mmol/kg = 1x........... = ..............mmols K
mmols 0 / 27mmol (2g) 0 / 27mmol (2g) 0 / 27mmol (2g)
Potassium:1mmol/kg = 1x........... = ..............mmols
Intravenous and Subcutaneous InfusionsRefer to fluid prescribing guidelines on SUHTranetADULT Patients (non neuro-surgical) For RESUSCITATION consider Hartmann’s, Gelofusine or blood as appropriate.
Most patients maintenance requirements will be met by 2 x 1L Dextrose-saline with 27mmol KCl added to each bag
NPSA – ? National Drug Charts incorporating fluid guidance

Work in progress…• Changes to MEWS criteria
– Often found that low urine output overnight triggers automatic fluid prescription reflex
• Changing routine use of 0.9% Sodium Chloride to 5% Glucose as diluent for IV drugs- providing it is stable

Assessing impact of changes…• Pharmacy Records
• Historical data 2002
• Prospective audits of elective major LGI / HPB / UGI surgical patients 2008 & 2009
– Pt demographics & surgical data– Detailed fluid balance (days 0-5)– Daily observation & oedema scoring– Daily weights– Complication rates– Daily biochemistry

Pharmacy Records
• Survey of quantities and type of fluid supplied to surgical wards– 1000 and 500 ml bags only– Not including colloid
• Problems– No account for case numbers– No account for case mix

0
10
20
30
40
50
60
70
80
90
100
Jan toMar 07
Apr toJun 07
Jul to Sep07
Oct toDec 07
Jan toMar 08
Apr toJun 08
Jul to Sep08
Oct toDec 08
Jan toMar 09
Time period
Perc
enta
ge o
f eac
h flu
id is
sued
in ti
me
peri
od
0.9% Sodium Chloride 5% Glucose Dextrose-saline Hartmanns
General Surgery Care Group1000ml and 500ml IVI bags issued
Audit Results
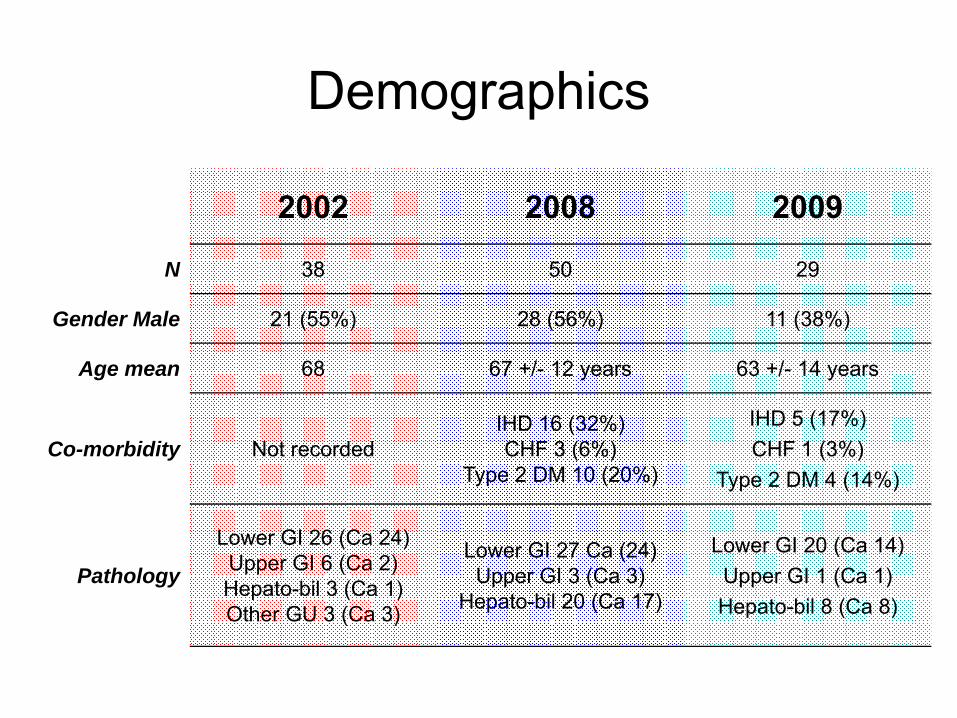
Demographics
2002 2008 2009
N 38 50 29
Gender Male 21 (55%) 28 (56%) 11 (38%)
Age mean 68 67 +/- 12 years 63 +/- 14 years
Co-morbidity Not recordedIHD 16 (32%)CHF 3 (6%)
Type 2 DM 10 (20%)
IHD 5 (17%)CHF 1 (3%)
Type 2 DM 4 (14%)
Pathology
Lower GI 26 (Ca 24)Upper GI 6 (Ca 2)Hepato-bil 3 (Ca 1)Other GU 3 (Ca 3)
Lower GI 27 Ca (24)Upper GI 3 (Ca 3)
Hepato-bil 20 (Ca 17)
Lower GI 20 (Ca 14)Upper GI 1 (Ca 1)Hepato-bil 8 (Ca 8)

Fluid Input & Balance (0-5d)

Presence of Oedema
Period Any Oedema (%)
2002 52
2008 40
2009 38

2002 2008 2009
Oedema Nooedema Oedema No
oedema Oedema Nooedema
Number of subjects 20 18 20 30 11 18
Total Fluid inputover 5 days (L) 21.6 20.6 17.1 15.9 17.2 12.4
Mean daily fluid input (L) 4.3 4.1 3.4 3.1 3.4 2.5
Total Na inputover 5 days
(mmol)1401 1192 1457 947
Fluid AdministrationBreakdown by presence of oedema
Severity of Oedema
Oedema Scores
1 = no oedema2 = detectable (mild)3 = moderate (significant but localised)4 = severe (extensive)

Percentage of patients with any oedema and oedema score ≥ 3
53
25
40
4
0
10
20
30
40
50
60
Oedema Oedema score ≥ 3
2002
2008
2009
38
14
%

Clinical outcomes 2002 vs 2008 vs 2009
2002 2008 2009
Number of subjects 38 50 29
5 day post op fluids (L) 21.1 16.4 14.2
PN Requirement 4 (8%) 0 (0%)
Days to solid food 6 (5 – 25) 3 (1 – 14)* 3 (1 – 11) *
Days to BO 6 (1 – 17) 3 (1 – 13)* 4 (1 – 11) *
L.O.S days 13 (4 – 59) 11 (3 – 66)* 10 (3 – 36) *
*p<0.05

Take home messages…• Exercise has underlined value of continuous audit
• There do appear to be clear trends– Reduction in Na & fluid provision– Improvement in oedema rates, complications and LOS
• It does seem possible to improve peri-operative fluid prescribing
• Requires considerable sustained efforts across many specialities
• Key interventions– Education Education Education! Know why– Guidelines Know how– Both Together Change in practice

The dangers of inappropriatefluid input…

Acknowledgements• Tina Scibelli Surgical Research Fellow• Emmanuel Itobi Surgical Research Fellow• Peter Austin Senior Pharmacist• Mo Abu-Hilal HPB Surgeon• Steve Wootton Senior Lecturer• Mike Stroud Gastroenterologist