improving good ideas -...
TRANSCRIPT
( PRACTICE FORUM JImproving Good Ideas
Edited by Patricia M. Byron, MA, OTRlL, CHT
Over the years, hand therapists have refined the art of innovation , always finding ways to make the good even better. Thisissue's Practice Forum submissions areperfect examples of this quest to improve and refine. The first article, by Judy Colditzand Anne Marie Schneider, offers one solution to the difficult task of improving proximal interphalangeal joint extensionfor the little finger. The second contribution also tackles the proximal interphalangeal joint, this time with a reoision of asplint designed for early mobilization of the unstable intra-articular fracture .
MODIFICATION OF THE DIGITALSERIAL PLASTERCASTING TECHNIQUE
Judy C. Colditz, OTRlL, CHTAnne Marie Schneider, OTRILHand and Orthopaedic Rehabilitation AssociatesP. O. Box 30263Raleigh, NC 27622
Serial plaster-of-Paris casting as described byBrand I is recognized as an effective technique forregaining proximal interphalangeal joint extension.However, the inability of the serial cast to "purchase"the full length of the proximal phalanx decreases thelength of the proximal lever arm available to extendthe joint. Additionally, when the distal interphalangeal joint is hyperextensible, the length of thedistal lever arm is limited to the length of the middlephalanx. Care must be taken to avoid hyperextensionof the distal interphalangeal joint when the proximalinterphalangeal joint is molded into extension. Wehave observed this mechanical inefficiency to be par- .ticuiarly marked in the little finger because of the
FIGURE 1. The middleand distal phalanges are wrapped witha thin layerof plaster. The proximal interphalangeal joint creasemust be clear.
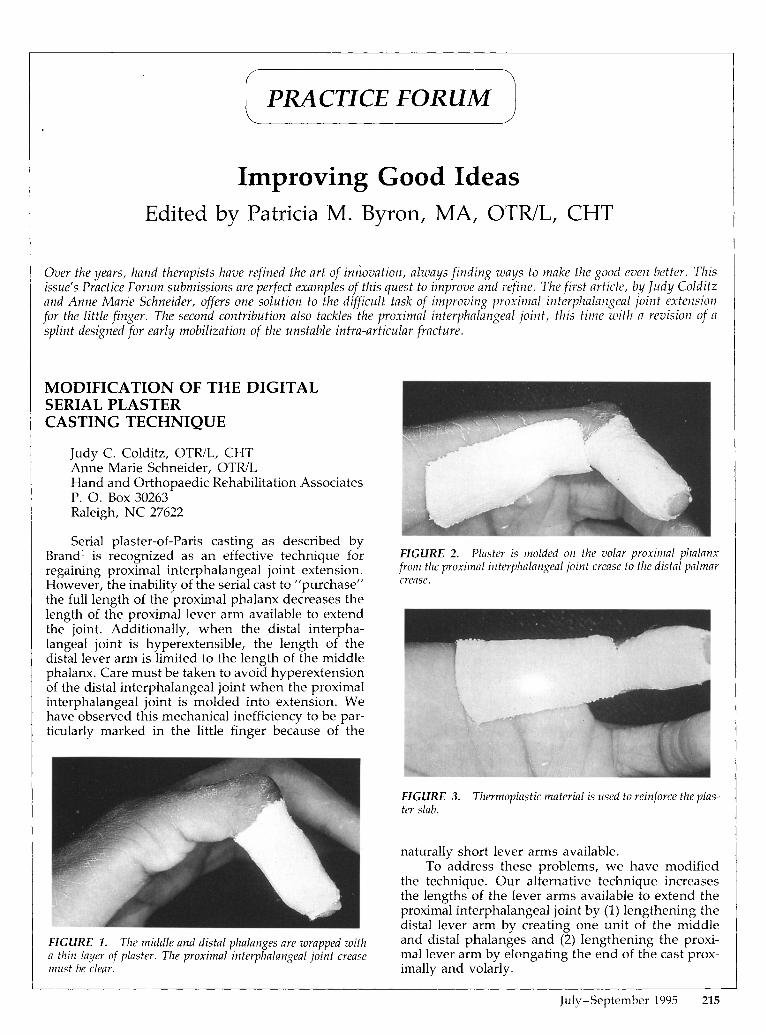
FIGURE 2. Plaster is molded on the volar proximal phalanxiront the proximal interphalangeal joint crease to the distal palmarcrease.
FIGURE 3. Thermoplastic material is used to reinforce the plaster slab.
naturally short lever arms available .To address these problems, we have modified
the technique. Our alternative technique increasesthe lengths of the lever arms available to extend theproximal interphalangeal joint by (1) lengthening thedistal lever arm by creating one unit of the middleand distal phalanges and (2) lengthening the proximal lever arm by elongating the end of the cast proximally and voiarly.
July-September 1995 215

FIGURE 4. The plaster cast is applied over the proximal anddistal segments.
FIGURE 5. The finger is gently stretched into extension .
Technique
First , the middle and di stal phalanges are encompasse d in a th in layer of plaster of Pari s that iswrapped circumferentially from the end of the digitto the proximal interphalangeal joint crease (Fig. 1).Next, eight layers of 'l-In wide wet plaster of Pari sare applied volarly on th e d igit from the proximalinterphalan geal joint crease proximall y to the distalpalmar crease, po sitioning th e metacarpophalangealjoint in zero degrees of extens ion (Fig . 2). The pla steris gently molded to the palmar con tour of the digit.The d istal circumfere n tial cas t and th e proximal volarslab mu st meet exactly at the proximal interphalangea l joint crease (join t axis) . The volar piec e of plasteris then rein forced by addi ng a sma ll piece of thin (1/16 in) thermoplastic mat erial molded d irectly overthe hardening plaster slab (Fig . 3). It is importantthat the edge of th e pla stic mat erial does not touchthe pati ent's skin.
Once these segme nts ar e in place, a pla ster castis applied circumferentially ove r th em using the technique described by Bell-Krotoski (Fig . 4) .2 With th eparti ally hardened components under th e serial cast ,the proximal interphalangeal joint can be ge n tly positioned toward extens ion without risk of creating a
216 JOURNAL OF HAND TH ERAPY
pressure area over the proximal interphalangeal joint(Fig. 5). Excessive force must be avoided when molding the cast for proximal interphalan geal joint extension, as th e dorsal proximal edge of the di stal circumferential piece can be tilted , creating a pressurepoint on the dorsum of the proxima l interphalan gealjoint.
This modified techniqu e is particularly useful forresistive joints whe re th e uninjured metacarp ophalan geal and distal interphalangeal joint are hypermobile. It is also effective for sho rt digits w he re thereis restri cted len gth ava ilable to hold onto th e proximaland middle phalanges adequa te ly with circumferential plaster. Thi s modifi ed techniqu e increases th emechanical efficiency of the cast application.
REFERENCES
1. Bran d PW: The recon st ruction of the hand in lep rosy. Ann RColi Surg Eng l 11:350, 1952.
2. Bell-Krotoski JA: Plaster cylinder casting for con tractures of theinterpha langeal joints . III Hunter JM, Schneide r LH, MackinE). Callahan AD (eds): Reh abilitation of the Hand, 3rd ed . St.Louis, MO, C. V. Mos by, 1990.
A MODIFIED DYNAMIC TRACTIONSPLINT FOR UNSTABLEINTRA-ARTICULAR FRACTURESOF THE PROXIMALINTERPHALANGEAL JOINT
Anne Byrne, Bsc OT, Dip COTTarry Yau, PDOTOccupational Therap y Dep artmentScarborough General Hospital3050 Lawrence Avenue EastScarboroughOntario MIP 2V5Canada
Adopting the Dennys et a1. 1 and Schenck? splinting concept in our facility has resulted in a modification of the Dennys splin t (Fig. 6). The original de-
FIGURE 6. A modified dynamic traction splint for unstableintra-articular fractures of the proximal interphalangeal joint.