importance of communications for ipv introduction · web viewchecklist for monitoring quality of...
TRANSCRIPT

Communication Planning Guide for IPV Introduction and
Routine Immunisation Strengthening
March 2015
1
For further information on IPV introduction, the OPV switch and routine immunization strengthening:
http://www.who.int/immunization/diseases/poliomyelitis/endgame_objective2/en/
Please send any questions or feedback on the materials to: [email protected]
All materials available through this web site are the product of an extensive collaboration between WHO, UNICEF, the Task Force for Global Health, CDC, Gavi, Rotary, and the Bill and Melinda Gates Foundation,
organized under the Immunization systems Management Group (IMG).

What is the purpose of this guide?
This document offers guidance for designing a Communication Plan to support the introduction of the injectable Inactivated Polio Vaccine (IPV) in the Routine Immunisation (RI) programmes of countries.
Included in this document are “pick and use” guidelines, checklists, tools and best practices from previous experiences of new vaccine introduction and routine immunisation communication to enable countries to effectively plan, coordinate, manage and report on the implementation of Communication Plans related to IPV introduction in routine immunisation systems.
This document aims to support national authorities and partners in: I) specifying the programmatic and behavioural objectives of the Communications
Plan; II) identifying key audiences and appropriate channels to reach them; III) developing key messages;IV) highlighting possible barriers and enabling factors to realizing objectives; V) translating messages into effective communication products;VI) monitoring and evaluating communication activities with clear benchmarks.
All of the elements described in this document represent the ideal for communication planning and implementation. However, experience shows that the ideal is sometimes not possible due to time or resource limitations. This resource is meant to give you options based on needs and capacity, but it is recommended that you go through all templates and checklists before deciding what to include or exclude in the final plan. It is also important to emphasise that you should feel free to incorporate your own approaches to communicating about IPV vaccine into the overall plan based on local knowledge and context.
Who will benefit from this guide?
This planning guide is meant to assist Communications Planners as well as Health and Immunisation Managers in Government and partner organisations at national and sub-national levels to plan and implement communication activities for IPV introduction and routine immunisation (RI) strengthening.
Importance of Communications for IPV introduction
This guidance document focuses on two key activities outlined in Objective 2 of the Polio Eradication and Endgame Strategic Plan 2013-2018; specifically,
1) Introduction of at least one dose of inactivated polio vaccine (IPV) in the routine immunization programmes of the 126 countries currently only using trivalent oral polio vaccine (tOPV),
2) Strengthening of immunization programmes in those countries as part of the introduction of at least one dose of IPV into their routine immunization programmes
The communication plan is part of the overall introduction plan that a country develops prior to IPV introduction. Apart from the communication plan, the introduction plan includes technical and operational planning, vaccine-management and cold chain assessment, and monitoring and evaluation tools and reporting mechanisms.
An effective Communications Plan for IPV introduction will at minimum focus on how to promote IPV vaccine acceptance by I) end-users (care-givers and parents), II) influencers (key opinion leaders) and III) actors involved in delivering the vaccine (healthcare providers).
2

Acronyms
CBO: Community Based OrganisationCSO Civil Society OrganisationEPI: Expanded Programme on ImmunisationFGD: Focus Group DiscussionICC: Immunisation Coordination CommitteeIEC: Information, Education and CommunicationIPV: Inactivated Polio VaccineM&E: Monitoring and EvaluationNGO: Non-Governmental OrganisationOPV: Oral Polio VaccinePIE: Post-Introduction EvaluationRI: Routine ImmunisationTOR: Terms of Reference
3

Comprehensive Checklist
While developing a Communication Plan for the introduction of IPV, other new vaccines and routine immunisation, the following checklist will assist you and the planning team to ensure that all the key steps of the planning process have been followed:
☐ Do you have a government-endorsed, multi-agency communications working group in place to support IPV introduction/routine immunisation?
☐ Have you done your situation analysis?
☐ Have you done your behaviour analysis?
☐ Have you planned your messages and materials?
☐ Do you have your strategy planning matrix and plan of action?
☐ Have you pre-tested your communication products/materials?
☐Do you have a distribution plan for the materials?
☐ Do you have a crisis communication plan, including explicitly agreed partner roles and responsibilities and SOPs?
☐Have you identified and trained agreed spokespeople?
☐ Have you secured funding for the implementation of the plan?
4

Communication (C4D) Planning Framework
A number of communication planning frameworks have been developed and they typically follow a series of steps as shown in Figure 1. This may also be applied to the IPV introduction Communication Plan as well as any other new vaccine or RI Communication Plan.
Figure 1: The Key Steps in Communications Planning
Each of these steps are described in detail below, with a linear step-by-step guide to preparing your Communications Plan.
5
1. Coordination & Preparation
2. Communication Analysis
3. Strategic Planning & Design
4. Creative Strategy & Material
Development
5. Monitoring & Evaluation

NAVIGATION PAGE
1. Coordination & Preparation 71.1 Establish or Reactivate Communication Committee 71.2 Establish Roles for Partners and Allies 7
2. Communication Analysis 72.1 Problem/Situational Analysis 7
2.1.1 Formative Research 72.1.2 Focus Group Discussions with Caregivers 72.1.3 Sample Template for Problem/Situational Analysis 8
2.2 Behaviour Analysis 82.2.1 Sample Template for Behaviour Analysis 9
2.3 Channel Analysis 102.3.1 Sample Template for Channel Analysis 10
3. Strategic Planning & Design 113.1 Develop SMART Objectives 113.2 Develop M&E Indicators 11
3.2.1 Sample Template for SMART Objectives 113.3 Strategy Planning Matrix 12
4. Creative Strategy and Materials Development 124.1 Message Development 12
4.1.1 Sample Template for Message Development 134.1.2 Checklist for Good Messages 13
4.2 Materials Development 144.2.1 Sample Template for Materials Development 14
4.3 Pretesting and Revising 154.3.1 How to conduct a pre-test? 15
5. Monitoring & Evaluation 155.1 Monitoring 15
5.1.1 Checklist for Monitoring Implementation 165.1.2 Checklist for Monitoring Quality of Interpersonal Communication
before RI session 165.1.3 Checklist for Monitoring Traditional & Local Media before RI session 165.1.4 Checklist for Monitoring Programme Interventions during RI session 16
5.2 Evaluation 175.2.1 Steps in carrying out an evaluation 17
6. Annexes 18Annex 1 – Suggested Composition of a Communication Committee 18Annex 2 – Suggested Terms of Reference of an IPV Communication Committee 18Annex 3 – Guidelines for Formative Research for IPV Introduction 19Annex 4 – Study Guide: For Focus Group Discussions with Caregivers 21Annex 5 – In-depth Interview Questionnaire with Service Providers 26Annex 6 – Multiple Injection Questionnaire 28Annex 7 – Sample M&E Indicators for Routine Immunisation and IPV 30
6

1. Coordination & Preparation
1.1 Establish a Communication teamSupporting the establishment or reactivation of a communication coordination committee/subgroup for IPV introduction at national and sub-national levels can contribute significantly towards ensuring Government ownership and partner buy-in throughout the planning and implementation process.
The IPV Communication Committee should be fully integrated within the existing national Immunization Coordination Committee (ICC) or the country’s National Immunization Programme and should include all relevant stakeholders to ensure effective mobilization of partners, community support and resources. It should include multidisciplinary teams of communication experts, social scientists, clinicians, health workers, and community representatives, as well as representatives of the ministry of health, line ministries, key partner agencies and community institutions considered important to the implementation of the communication component of the programme. See Annex 1 for a more thorough suggested composition.
1.2 Establish roles for partners and allies Failure to clarify collective and individual roles of collaborating partners can result in inactive and unfocused participation. See Annex 2 for the suggested Terms of Reference of IPV Coordination Committee (within the Immunisation Coordination Committee). The IPV committee will also be responsible for identifying, training and supporting the Spokesperson to prepare and deliver messages in case of AEFIs.
2. Communication Analysis
2.1 Problem/Situational Analysis
The situational assessment should include gathering and analysis of secondary (e.g., desk review) and primary (e.g., interview or focus group) data to describe the scope and status of the current immunization situation, the anticipated impact of IPV introduction, and the associated programme objectives.
2.1.1 Formative ResearchFormative research is likely to reveal key barriers or facilitators to be taken into consideration while developing the Communications Plan. Whether the collection and analysis of data is led by partners or a contracted consultant or agency will depend upon the scope of work, timeframe, and resources. See Annex 3 for guidelines to conduct formative research for IPV introduction.
For example, research in one community might point to a high acceptance for injectable vaccines among caregivers and radio programming and political will as the main facilitators for high routine immunisation coverage and the acceptance of new vaccines. While in another area, negative attitude of health workers and frequent vaccine stock-outs might be identified as the main barrier for low RI demand and distrust in the health system. These findings are key for communication planning.
2.1.2 Focus Group Discussions with Caregivers If conducting formative research is not possible due to time or resource constraints, countries are encouraged to conduct Focus Group Discussions (FGDs) with both caregivers and health workers to generate information and variance based on geographical, ethno-linguistic, infrastructural, or other
7

differences. See Annex 4 for a FGD guide for caregivers and Annex 5 for an In-depth Interview guide for service providers.
In-depth interviews with health workers might reveal their concerns related to the new vaccine introduction. For example, healthworkers might express concern about administering multiple injections to a child in one visit, heavy workload or other capacity related matters. Such findings can better inform training materials and respond to specific gaps in healthworker capacity, important not only for IPV introduction but also for the strengthening RI systems.
With the introduction of IPV, planned introduction of other new vaccines and the routine immunisation schedule, multiple injections in one health facility visit is likely to generate discussions and also raise concerns among healthworkers and caregivers. In order to develop evidence based communication and healthworker training plans to address the issue of multiple injections, countries are strongly encouraged to conduct research on the issue. See Annex 6 for a brief questionnaire on multiple injections.
2.1.3 Sample Template for Problem/Situational AnalysisWhile undertaking a problem/situation analysis, the following questions should be kept in mind:
What barriers, behavioural and otherwise, might prevent achieving programme objectives associated with the vaccine introduction?
Which people will likely be affected and how that might influence programme objectives?
What inputs/resources, activities, outputs and outcomes will likely need to be achieved in order to effectively integrate IPV into the routine immunization programme (including political will to adequately finance all necessary activities to support successful introduction, including communication and social mobilization)?
The following is only a sample template in which the problem/situational analysis for only one target audience (caregivers, particularly mothers) has been outlined. A fully developed problem/situational analysis should also address other target groups as identified in the formative research. These can be specific family members, health workers, religious leaders and community elders.
Audience (Caregivers
, Health workers, Family,
etc.)
Problem Impact Causes
Caregivers related System/Service related
Caregivers, particularly mothers of children under 5 years of age.
IPV non-immunisation or under immunisation of children in accordance with national immunisation schedule.
Increased risk of morbidity and mortality from vaccine preventable diseases among children.
Parental knowledge (not knowing child’s age, when and where to go, hours of operation, value of immunisation and benefits of IPV)
Fear of side effects from IPV or other vaccines
Religious/cultural/social
Lack of resources, stock outs that affects reliability, cold chain
Reliability (no cancellation of sessions – both fixed and outreach)
Distance/travel conditions to reach catchment area
Health staff’s motivation, performance/compete
8

beliefs/norms and rumours
Distance/travel conditions, access
nce, behaviour and ability to communicate with mothers.
2.2 Behavior AnalysisFrom step 2.1.3 problem analysis, determine which of those problem behaviors to focus on and analyze those in order to understand your key problems and a potential response better.Questions to keep in mind:
Target audience groups that will be affected by and might affect IPV introduction and associated programme objectives
Their existing behaviors/practices that might help or hinder achieving programme objectives
The communication channels that are accessible and preferred by each audience group.
2.2.1 Sample Template for Behaviour Analysis
A sample behaviour analysis for primary caregivers (mothers of children under 5 years) is presented below. A fully developed behaviour analysis should also address other target groups as identified in the formative research. These can be specific family members, health workers, religious leaders and community elders.
Desired Behaviour Actual Behaviour Feasible Behaviour Factors Encouraging Ideal Behavior
Caregivers bring their children for IPV/RI to service delivery points at the ages recommended in the national schedule with immunisation card
Many caregivers take their children for complete immunisation at some point in time.
Delay in first immunisation based on practice of “staying in the home” after delivery and health workers not remembering to advise mothers.
Caregivers unable to locate vaccination cards.
Caregivers bring their children only one time to get the immunisation.
Most caregivers take their children to get fully immunized
Are aware of and follow the immunisation schedule
Maintain the Immunisation card
Understanding of the benefits of IPV and immunisation for the child
Awareness of immunisation schedule, place and date
Proximity to health facility.
Positive attitude of health staff towards caregivers.
9

Based on the communication needs and the research available, a similar analysis can be undertaken for different audience groups. These may include:
Primary audience – These may include, heads of households, Fathers and Guardians (includes grandparents and mothers-in-law) and extended family members.
Tertiary audience groups: This include decision makers at the national and sub-national level. At the provincial and district level (sub-national) these may include, provincial and district government leaders, administrators, local health authorities, health professionals in the private and public sector, academics, business leaders and local media. At the national level, tertiary audience may include, public policymakers, parliamentarians, national government officials and national media and advocacy groups.
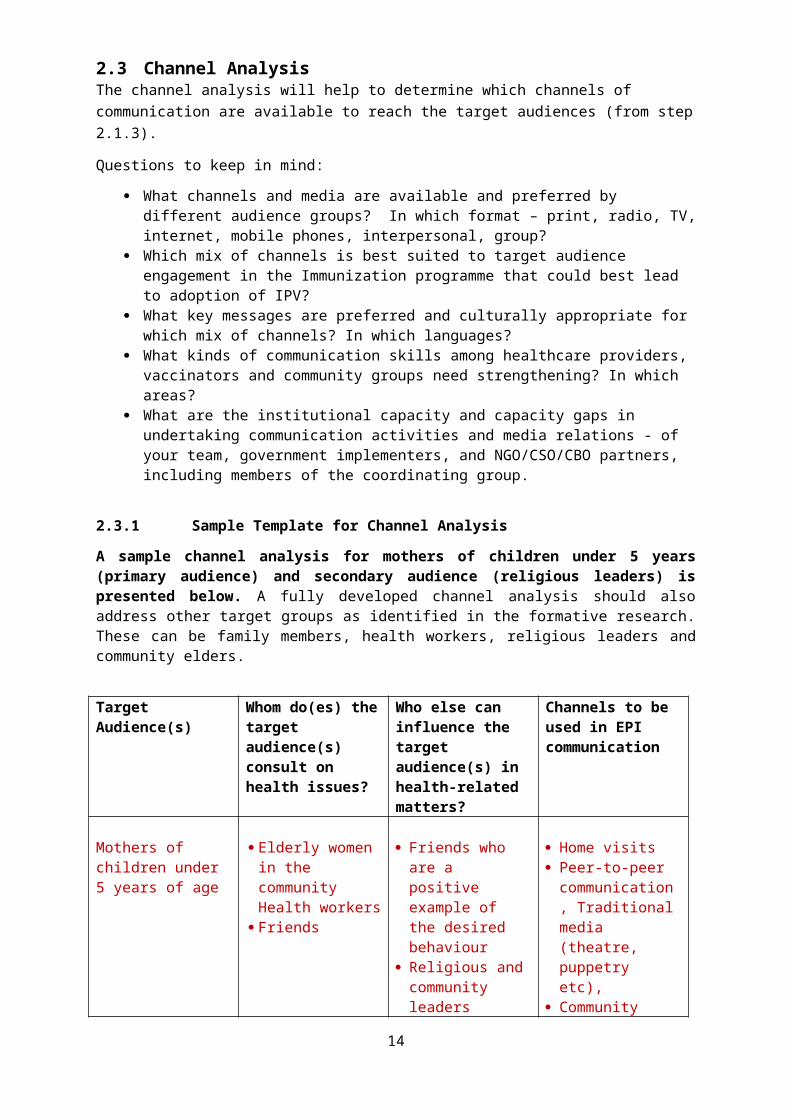
2.3 Channel AnalysisThe channel analysis will help to determine which channels of communication are available to reach the target audiences (from step 2.1.3).
Questions to keep in mind:
What channels and media are available and preferred by different audience groups? In which format – print, radio, TV, internet, mobile phones, interpersonal, group?
Which mix of channels is best suited to target audience engagement in the Immunization programme that could best lead to adoption of IPV?
What key messages are preferred and culturally appropriate for which mix of channels? In which languages?
What kinds of communication skills among healthcare providers, vaccinators and community groups need strengthening? In which areas?
What are the institutional capacity and capacity gaps in undertaking communication activities and media relations - of your team, government implementers, and NGO/CSO/CBO partners, including members of the coordinating group.
2.3.1 Sample Template for Channel Analysis
A sample channel analysis for mothers of children under 5 years (primary audience) and secondary audience (religious leaders) is presented below. A fully developed channel analysis should also address other target groups as identified in the formative research. These can be family members, health workers, religious leaders and community elders.
Target Audience(s) Whom do(es) the target audience(s) consult on health issues?
Who else can influence the target audience(s) in health-related matters?
Channels to be used in EPI communication
Mothers of children under 5 years of age
Elderly women in the community Health workers
Friends
Friends who are a positive example of the desired behaviour
Religious and community leaders (social norms
Home visits Peer-to-peer
communication, Traditional media (theatre, puppetry etc),
Community 10
Secondary audience groups – These may include, community leaders, family members including grandparents and mothers-in-law, health workers, vaccinators, NGO and CSO workers, religious leaders/groups and social networks.

related to new vaccines/RI)
dialogue involving elderly women.
Religious leaders Other/senior religious leaders
Senior health workers
District level administrators
Politicians
Community meetings
Religious gatherings Flyers Religious radio and
TV broadcasts
3. Strategic Planning & Design
This section explains how to develop actionable plans based on the guidance presented in Step 2 above.
3.1 Develop SMART ObjectivesAn objective is a way to articulate the change you want to make – in our case, this change might be from a problematic behaviour to a desired behaviour (e.g. non-vaccination to vaccination). Objectives must be specific and stated in a clear way. They should not be vague and should not be open to multiple interpretations. A good way to test whether the objectives you’ve set are appropriate is to ensure that they are SMART:
Specific: Who? (Target population and persons doing the activity) and What? (Action/activity)
Measurable: How much change is expected and how will you measure it? Achievable: Can it be realistically accomplished given current resources and constraints,
including time restraints? It is important to be realistic. Realistic and relevant: Does it address the problem and propose reasonable programmatic
steps? Time-bound: Does it provide a timeline indicating when the objective will be met?
For more guidance on how to formulate SMART objectives, go to: http://www.cdc.gov/phcommunities/docs/evaluate_smart_objectives_template.doc
3.2 Develop M&E IndicatorsMonitoring provides a basis to track programme progress; Evaluation measures programme progress. Examples of indicators are shown in Annex 7. More information on the implementation of monitoring and evaluation can be found in Step 5.
3.2.1 Sample Template for SMART Objectives, Strategy, Activities, and M&E Indicators
The following sample template is only for one communication objective. It should be used for each of the communication objectives of the IPV introduction and RI strengthening communication plan.
Objective By October 2012, X% of mothers in a given community in high priority district Y of state Z have been met by a community health volunteers and informed about the benefits of IPV
Strategy Interactions with community health volunteers through planned home visits and in social settings, supported by information, education and communication materials.
Activities 1) Training of community health volunteers using IPV RI communication modules
11

2) Development of IEC materials related to IPV/RI – posters, flipcharts3) Home visits by community health workers to interact with caregivers4) Community dialogue sessions with community elders, including women
Process Indicators
# of community health volunteers trained on IPV/RI Communications# of IPV and RI posters developed & distributed# of RI flipcharts developed & distributed# of home visits conducted by community health volunteers# of community dialogue sessions organized by community health volunteers
Outcome Indicators
Knowledge - X% of mothers in a given community in high priority district Y of state Z can correctly state at least 2 benefits of IPV/RI
Attitude - % of mothers who believe that children should receive IPV/be immunized according to RI schedule
Source of Information - X% of mothers in a given community in high priority district Y of state Z that identify the community health volunteers as main source of information on IPV/RI
Impact Indicators
By December 2012, immunisation coverage in a given community in high priority district Y of state Z has increased from 60% to 70%.
3.3 Strategy Planning MatrixThis communication plan matrix is intended to offer an outline of the communications activities that should be considered in preparing to introduce IPV and a proposed timeline based on a November IPV introduction. The plans that you have developed so far can be put in the attached planning template, which also includes space for budgeting and assigning task responsibility.
Not all types of activities are essential although recommended to support a successful introduction. If desired a column for indicators can be added.
The communication plan template should guide the Communication Committee to review progress against plans and take corrective actions where needed.
4. Creative Strategy & Material Development
Message and material development should be based on the analysis done in step 2. Effective communication entails tailoring your messages according to the level/knowledge gaps/needs of your target audience.
Plans for the messages should be developed at this stage. Determine basic message concepts based on the areas in which messages should be developed. In addition, determine the communication approach (should it be informing, entertaining, persuading, educating, empowering or a combination of these?) and the appeal and tone (should it be positive/negative, rational/emotional, definite/open-ended, etc.?).
12

4.1 Message DevelopmentThe process of message development will allow you to narrow down what the audience would want to hear from the communication and how it needs to be positioned in order to prompt/motivate them to act.
Message development involves:
1. Identifying areas in which to develop messages 2. Determine the communication approach 3. Determine media, materials, and editorial format.4. Drafting messages and concepts.5. Review, pre-test, and revise text and concepts
4.1.1 Sample Template for Message Development The following template presents the variety of factors to be taken into consideration during the message design process. Formative research or FGDs will provide information on the “Factors Influencing adoption.”
The draft messages developed out of this process should be pre-tested and finalised.
Audience(s)
Behavior to Promote
Factors Influencing Adoption
Message Concepts
Approach Tone
Caregivers, particularly mothers of children under 5
Most caregivers take their children to receive IPV/ get fully immunized
Follow the immunisation schedule
Maintain the immunisation card
IPV and immunisation is a free service.
IPV will make your child stronger.
Mild negative side effects from IPV/immunisation are normal
Immunisation prevents serious child sickness, including polio
IPV + OPV provides greatest protection against polio.
Lifelong protection to the child.
Immunisation card is like an identity card for a child.
Parents want their children to be healthy.
Male support for accessing lifesaving health services
Informing, entertaining, persuading
Positive, Emotional
Community elders
Support caregivers to ensure child is taken to the health centre
IPV and immunisation is free
Mild negative side effects from IPV/immunisation are normal
Immunisation prevents
Healthy children will make a healthy community
Male support for accessing lifesaving health services
Informing, entertaining, persuading
Positive, Emotional, Supportive (acknowledging existing beliefs and attitudes)
13
serious child sickness, including polio
4.1.2 Good Messages ChecklistEffective messages should have certain characteristics as shown in the checklist below.
☐ Reinforce positive factors identified in formative research☐ Address misunderstandings and areas of deficient knowledge☐ Address attitudes☐ Give the benefits of the behaviours being promoted☐ Urge specific actions☐ State where to find the services being promoted☐ State where to find help, if needed☐ Address barriers to action
Key resource documents to support IPV message development can be found here.
4.2 Material DevelopmentGood communication materials express ideas simply, clearly, and directly, using language, images, and examples that target audiences are familiar with. And ultimately, it should be a call for action. The materials developed should be thoroughly reviewed, pre-tested, and revised if necessary based on feedback.
For further reference, IPV Communication Materials from Nepal can be viewed here.
4.2.1 Sample Template for Materials Development The following materials development template suggests the different materials by audience and communication channel that could be needed for IPV introduction in countries. In the use of this template, local contexts and research data should be used to best identify what materials would be most suitable.
Strategy Audience(s) Materials to DevelopMass Media Group Settings One-on-one
Behaviour Change
Caregivers (mothers and fathers)
Radio and TV drama, SMS content
Flipcharts Flyers Posters Banners Scripts for
theatre and puppet shows,
Facilitator notes for community dialogue sessions
Flipcharts Flyers
Social Mobilization
Community Self Help Groups, Community elders, school
Radio and TV drama, Public Service
Announcements SMS content
Banners, Flyers Posters Scripts for
14

children, Media theatre and puppet shows
Advocacy Senior religious leaders, district administrators, Media, policy makers and professional associations
Radio and TV drama, Public Service
Announcements Scripts for Talk
Shows/Panel Discussions
Flyers Posters Advocacy
folder with inserts
Advocacy folder with inserts
Training Health Workers Radio and TV drama, Public Service
Announcements
Presentations IPV/RI
training video clips showing best practice
IPV Job Aids
Job Aids Posters
(with technical guidelines)
Health worker training modules on IPV and RI can be viewed under “Training” here.
4.3 Pre-testing & RevisingPre-testing is a critical step in your message development, using a sample of your audience to determine the impact that your materials will have prior to production and dissemination. Your aim is to identify any elements that need to be changed or improved to make your material more effective. Pre-test to ensure that your messages and materials have the five elements of effectiveness:
1. Understandable – Is the message clearly explained and easy to understand?2. Attractive – Is the message attractive enough to hold attention and be remembered?3. Acceptable – Does the message contain anything that is culturally offensive, annoying or
false?4. Involving – Does the audience feel that the message/material speaks to them and is about
them? 5. Persuasive – Does the message convince the audience to take the recommended action?
4.3.1 How to conduct a pre-test?Pre-testing can be done through organising Focus Group Discussions, with a maximum of 15 people per group. The facilitator should show the participants the materials developed and get their feedback on the key elements mentioned above. Care should be taken to get feedback from a cross –section of people in the community i.e. mothers, fathers, community elders, social mobilisers etc. Mixed groups might not be conducive for pre-testing as some individuals are likely to feel constrained in airing their views. Therefore, as much as possible the facilitator should try and organise FGDs with a similar group i.e. religious leaders, mothers of caregivers under 5 years, social mobilisers. If needed, follow up interviews can also be conducted with specific individuals.
5. Monitoring & Evaluation (M&E)
Monitoring is used to measure if a communication intervention is progressing as planned, and to make in-course adjustments or changes if necessary in order to achieve the intended behaviour outcomes among specific audience groups.
Evaluation is done after a pre-determined period of time has elapsed, known as an “end line” to ask “how did we do?”, i.e., to measure the expected outcomes from a communication intervention assessed against any relevant “baseline” data and indicators.
15

M&E indicators should have been created during the planning phase.
5.1 MonitoringSome of the monitoring methods are periodic review of programme action plans, regular audits of materials to ensure they are being distributed and used correctly, spot checks at public places where target audience members are found (check whether they remember some of the messages in the media), exit interviews at routine immunization sessions, group discussions, etc. It is key to prepare a monitoring schedule for implementation prior to RI sessions and at RI sessions.
The key areas to be monitored (and the checklist for each area) can be divided into are listed below:
5.1.1 Checklist for Monitoring Implementation
☐ Planned programme activities being implemented prior to RI sessions and at RI session.☐ IPV and RI materials distributed and used as plannedMethods that can be used to monitor include regular progress reports from the field, regular audits of materials, supervision visits/checklists, etc.
5.1.2 Checklist for Monitoring Quality of Interpersonal Communication before RI Session
☐ Interpersonal communication activities being carried out (adequate promotion of Routine Immunization sessions via Social Mobilization activities)☐ Quality of interpersonal communication between clients and workers is high; clients are satisfied and interacting well☐ Clients receiving the key information that they should receive during interpersonal interactions☐ Front line workers being adequately trained in Inter-Personal Communication Skills☐Quality of interpersonal communication between communication trainers and trainees is high
Methods that can be used to monitor include observations, exit interviews, group discussions with appropriate audience categories, etc.
5.1.3Checklist for Monitoring Traditional & Local Media before RI session
☐ Number of local groups involved is adequate☐ The groups are viewed and received well in the community☐ The groups involved and the media are managed well☐ The impact of the messages is monitored and reviewed
5.1.4 Checklist for Monitoring Programme Interventions during RI session
☐ Key Messages being given at Routine Immunization sessions☐People understand the messages☐ People accept the messages. If they reject, measures taken to improve.☐ People find that it is possible to implement the actions being proposed in the messages☐ Changes are taking place in knowledge, attitudes, or behaviour among the target audiences☐ Interventions are making gains
16

☐Caregiver recall of key messages via Information, Education and Communication (IEC) materials (posters, leaflets, Public Service Announcements) or via frontline health workers (to provide in-course guidance as to the most effective way to reach caregivers)
5.2 EvaluationThere are three types of evaluation. These are process evaluation (short-term achievements: were activities implemented as planned?), outcome evaluation (medium-term effects: did any change take place?), and impact evaluation (long-term effects: change in morbidity, morality, health status, quality of life).
5.2.1 Steps in Carrying out an Evaluation Establishing evaluation indicators: This should have been done in the planning phase. Establish evaluation objectives: This should be determined based on how you want to use
the answers from the evaluation. You should also determine what needs to be measured to get this information.
Determine design and methods. Also determine sample size. Collect data Analyze data Utilize research data: Summarize key findings and share with appropriate people. Use the
findings to develop improved strategies.
The New Vaccine Post-Introduction Evaluation (PIE) Tool provides a systematic method for evaluating the impact of the introduction of a vaccine on the existing immunization system in a country, and includes “Advocacy, Communications and Acceptance” as an evaluation area. A PIE should be done between 6 and 12 months after introduction of the new vaccine.
At the very least, countries should attempt to evaluate the outcomes of IPV introduction communication activities (against Knowledge, Attitude and Practice indicators) two months after the introduction.
17

ANNEXES
Annex 1:Suggested Composition of a RI/IPV/NV Communication Committee
NATIONAL LEVEL
RI/IPV/NV Communication Coordinating Group (subgroup of ICC)Chair:
Ministry of Health (e.g., Health Education and Communication Chief) If relevant, additional partners may serve as Co-chair or Vice Chair (e.g. UN, NGOs,
Rotary)Secretary:
Ministry of Health StaffMembers: (responsible for advocacy, social mobilization, community engagement and media relations)
PROVINCIAL/STATE/DISTRICT LEVEL
Provincial/State/District Health/ Social Mobilization Team Health Executive Officer and/or Deputy District Immunization Officers or EPI Mid-level managers Other line department sub-national officers from Education, Information and
Communication, Social Welfare, Interior and Community Development Local government authorities – Office of the Governor, District Chief, Mayor Religious leaders Representatives from relevant NGOs
Annex 2:Suggested Terms of Reference of an RI/IPV/NV Communication Committee
The role of the IPV Communication Group is to serve as the team of technical communication advisers and specialists who will:
1. Agree on terms of reference of the Group; roles and responsibilities of specific member agencies; regularity and venue of meetings, and format for record of meetings and reporting to National Committee; follow-up on action points; timelines for individual and team tasks.
2. Identify and appoint a full-time communication professional, with a support team and a base agency for communication operations, who will act as the focal point, and manage and perform day to day communication operations as per the communication action plan.
3. Develop TOR and MOUs of implementing agencies, cooperating partners and local government authorities describing agency tasks/roles and accountabilities for transparent coordination mechanisms.
4. Oversee, facilitate and monitor the development and successful implementation of an integrated communication strategy (including AEFI Risk Communication Plan) and provincial/state/district level action plans for cholera prevention and IPV introduction in pre-emptive and reactive modes.
5. Facilitate the formation of lower level IPV Communication Group structures at state/provincial/municipal/community levels to support the communication activities with corresponding TOR and communication plans.
6. Oversee AEFI-related communication protocols and setting roles and responsibilities for media management in the event of AEFIs.
18

7. Regularly review, update and where necessary recommend changes to the IPV introduction communication strategy and action plan at provincial/state/district levels.
8. Develop an operational monitoring checklist to detect issues/bottlenecks/gaps in implementation, management and coordination. Take appropriate measures to close the gaps.
9. Designate representatives to participate in regular meetings of other sub-committees/groups and report on actions and identified bottlenecks, e.g., resource gaps, issues and challenges for immediate action.
Annex 3:Guidelines for Formative Research – IPV Introduction
This section provides formative research guidance – including the research framework, target groups and behavioural outcomes for developing an IPV communications plan.
Within the process of undertaking formative research, value clarifications and consensus among stakeholders for IPV introduction is an important first output. Value clarification workshops are ideal to achieve consensus and build support among stakeholders. The workshop is an opportunity to further develop and refine the overall global approach to the formative research; to design and plan critical country-level research; to develop and refine country-level key research questions and global research conceptual framework (discussed below); and, local country level experiences, variations and different research needs and priorities for IPV introduction.
Formative research is a recognized activity in the World Health Organization’s framework for new vaccine introduction. The formative research should cover a variety of topics, therefore research teams needed to be interdisciplinary.
Research aim and objectivesBased on the outcomes of value clarification workshop and discussions with stakeholders, the research aims need to be developed. Country programs are encouraged to develop research objectives based on their need and context.
Research AimTwo general questions to guide objectives of formative research are likely to be-
1. What factors are most likely to result in end-users having a positive disposition towards receiving IPV vaccine?
2. What factors are most likely to foster healthcare providers’ ability for successful IPV vaccine delivery?
Research Objective: Based on the above research aims; following research objectives should be formulated
1. To understand the concerns and fears of care-givers towards their child’s susceptibility to disease, disease severity, benefits and risks of treatment through IPV and multiple injections
2. To understand the perceptions of health workers towards multiple injections including IPV introduction.
3. Determine information needs of various stakeholder regarding IPV vaccine and immunization in general.
4. Identify key sociocultural factors that could influence acceptance or rejection of the IPV vaccine
5. Assess communication skills capacity of healthcare providers in offering IPV vaccine to caregivers.
6. Review the current communications initiatives and efforts in increasing routine immunization coverage, with a specific focus on best practices and lessons learned.
19

Research topics of enquiryEach level includes salient research topics that are appropriate for the overall study objectives. Research topics may be identified in a number of ways i.e., review of literature or the past and most recent quantitative and qualitative research studies on immunization, findings from demographic health surveys, routine immunization coverage survey, and/or questions generated during value clarifications workshop. Researchers and practitioners with expertise in the different areas of inquiry should be also consulted.
Table 1 presents the key areas of inquiry or research topics explored within each study component and the corresponding levels described in the conceptual framework and target groups.
Levels in conceptual framework
Target Group Ares of Inquiry
Personal/parental beliefs andInteraction with healthcare providers.
Caregivers/parents Knowledge and perception: Understanding of immunization, immunization schedule, vaccine preventable diseases, routine versus campaign immunization, risk-benefit analysis of immunization for decision, trust and confidence in vaccine (self-efficacy)Knowledge and Perception: Understanding of Polio and IPV, perceived benefits, concerns regarding IPV (safety and efficacy)Quality of care and access: Experience with vaccine providers, access to vaccine service pointsSocial norms: Role of key authority figures in vaccination decisionInformation source: Media sources for immunization, vaccines, access to communications channels, preferred and trusted media sources and channelsLocal terminologies of diseases, vaccine and immunization schedule.
Institutional factors Healthcare providers Knowledge and perception of immunization, understanding of immunization schedule, knowledge of community practices, outreach strategies to improve vaccination coverageUnderstanding of IPV vaccine, association of IPV vaccine positives and negatives, concerns in offering IPV to children (multiple injections, adding a new vaccine in the schedule)Negotiation skills: Communicating with caregivers on multiple injections, vaccine safety and efficacyMotivations: Strategies/tools to improve healthcare provider efficiency and productivity in offering IPV in the community
Social/community factors Community leaders Knowledge and perception of immunizationPerception of immunization servicesPractices for community mobilization
Interpersonal – role of male
Social support, inter spousal communications
20

Annex 4:Study Guide: For Focus Group Discussions with Caregivers (mothers, fathers or grandmothers)
Introduction
►Explain the reason for discussion (to improve immunization services and protection for children)►Explain how the discussion will proceed: ground rules (turn off cell phones, everyone should participate, one person talking at a time, etc.)►Request that everyone share opinions and experiences: explain that no one is being judged or evaluated►Express appreciation for everyone’s participation►Repeat that participation is voluntary and that participants’ names and individual opinions will not be shared with anyone[Hand out name tags with first names only]
Main Topics Key Questions Possible Probing Questions
Introduction of participants: talk about their families
Can each of you please tell us:►Who are the members of your family?►How long you have lived in your community or neighbourhood?►Can you please tell us something interesting or unusual about your family?
Note: You can modify these questions. The purpose is to help people feel comfortable with each other and with speaking out. Write these questions on a flip chart.
Concept of vaccination
►What is the purpose of vaccination?►How important is it for children to get all of their vaccinations?►Do you have any concerns about having your children vaccinated?
Note: If you believe that concern about vaccine safety is a major issue, you can add a question such as: How safe do you feel that vaccination is?
►What diseases does vaccination protect against?►Do you think that getting vaccinated guarantees that the person will never get the disease?
Practical Knowledge of Vaccination
►How many vaccination visits do you think a child needs?
►By what age should a baby receive all of the basic vaccinations?
Experiences with and feelings about vaccination services
Next we’d like to discuss your experiences in getting your children vaccinated:►Can each of you please tell us if your child has received most of his vaccinations in a health center, health post, or outreach site?►Can you please tell us about your experiences when you brought your
►What have you liked about your experiences?►What aspects of getting your children vaccinated have been difficult or unpleasant? (Please be frank because we are asking this so we can learn how to improve the services.)
21

Main Topics Key Questions Possible Probing Questions
children for vaccination?Note: You can call on various participants to share experiences. Ask if anyone else has had a similar experience.►How satisfied are you with the way in which the vaccinators treat you and your child?►How much have your experiences getting your child vaccinated encouraged or discouraged you to bring your child back for additional vaccinations?
►How friendly is the vaccinator?►What does the vaccinator normally tell you when s/he vaccinates your child?►How easy is it to understand what the vaccinator says to you?►Does the vaccinator invite questions from you?►How confident are you with the vaccinator’s competence?
Reasons for current vaccination status
Note: Choose the appropriate category: All of you have young children who have (1) some but not all of the vaccinations they should have received [or] (2) are fully vaccinated or up to date with their vaccinations.
Can you please explain the reasons why your child has:* only some of the vaccinations he is eligible to receive* all of his/her vaccinations?
Note: This section can be deleted if your concern is only with the HW/caregiver interactions.
Probe about any of the following areas that the group does not cover well without prompting:►Do others in your family encourage or discourage your child from getting vaccinated?►Did other community members or leaders influence your decision to have or not have your child vaccinated? If so, please tell us what they said.►How convenient for you are the days and hours when vaccinations are offered?►What, if any, problems do you have in getting off from work to bring your children for vaccination?►Does it cost you any money to get your child vaccinated?►Are you concerned about bad things that people say about vaccination?►Do you and your family leave your community during some times of the year? Does your travel affect your ability to bring your child for vaccinations?►Have you ever brought your child for vaccination but not been able to receive it? [If so] why?►Are you concerned about side effects from vaccination? Have any of you not brought your child because of this concern?
Family and Community Support
Do family members encourage or support caretakers to take their children for immunization?
In what situation do you ask for permission to take your child for immunization? From who?
If “yes” What kind of support do they give? (Probe: Encouragement, Transport, Reminders, others …)
If ‘no’, why do you think they do not support caregivers?
22

Main Topics Key Questions Possible Probing Questions
In your opinion, what contribution can fathers make towards successful routine immunization?
What resources do you have in this community that will enable you to inform caretakers to emphasize the importance and need to take their children for routine immunization?
If the no structures/ resources are mentioned, probe if the role of: local councils, community groups, Revolving Funds for prevention of Malaria, Religious organizations, CBO’s)
General understanding of Polio Vaccination
What do you know about the polio disease?
What do you think causes polio? How can one treat polio? Is it curable? How can you protect yourself and
children from polio? What do you know about the oral polio
vaccine? How safe do you think this vaccine is? How effective do you think the vaccine
is in terms of protecting you and your children from polio?
Do you have any concerns with a vaccine that is given into the mouth? Why?
Introducing IPV
We discussed about the polio vaccine that is given as drops into the mouth, we would like to discuss your opinion about the injectable polio vaccine – one that is given through a needle. This vaccine will soon be available to your children who are under five years old. First a child will receive 1st does of oral polio vaccine – (the drops), and then at 14th week along with DPT3 and 2nd dose of oral polio vaccine an injectable vaccine will be given to your child, this will be followed by a 3rd does of oral polio vaccine.
What do you think about this new idea- giving children in your community another polio vaccine, which is an injection along with oral polio drops?
What do you think about an injectable polio vaccine?
Do you have any concerns about this new polio injection?
What are opinions about the “polio injection” versus “oral polio drops”? What do you think the difference is?
After your child had received the “polio 23

Main Topics Key Questions Possible Probing Questions
drops” with “polio injection”, will you continue to give your child additional polio drops in future?
What do you think of other people in your community would think about giving the “injectable vaccine” in addition to the “polio drops”?
Can you think of any issues which can make giving the “injectable vaccine” along with “polio drops” to children difficult?
Sources of Information
1. In this community, what are your sources of information about immunization?
2. Of those that you have mentioned, what sources of information on immunization do you think caretakers trust most? What about you?
3. Have you heard someone in this community talking against taking children for immunization?
4. Do you/ caretakers in the community have child health cards?
Probe: 1Who tells you about routine immunization?Who tells you about NIDs?
Probe: 2What kind of person would best convince caretakers in this community to take their children for routine immunization in order to complete their children’s immunization schedule?What sources of information do you prefer?
Probe:3What have you heard?Do you think some people in the community believed them? Why do you think they believed them?Do you think what they said was true or false? Why?How can we convince caretakers that immunization is good for protecting a child against diseases?Who in the community can best convince caretakers?In your opinion, what key messages must caretakers know in order to be convinced to take their children regularly for routine immunization?
Probe:4Who gave them to you?What were you told about the card?Did you understand what you are supposed to do with the card?Did you share immunization
24

Main Topics Key Questions Possible Probing Questions
information from the card with your spouse? With a family member?
Suggestions ►Please let us know your ideas for how vaccination services could be improved?►Do you have any suggestions for how interactions with the vaccinators can be improved?
Closing Thank the participants and ensure them that a summary of their experiences and suggestions will be shared with the health official, who will consider what you have said in planning improvements in vaccination services and how they are promoted.
If possible wait until the end to serve refreshments. You can also break in the middle, but try to break at a time when the discussion has slowed down.
Do you have any final questions or concerns about vaccinations or vaccine-preventable diseases that you would like to ask?
Annex 5:In-depth Interview – Health Service Providers
Section A: Interviewee’s ParticularsName of Zone………………..Region ………….…District……………….Ward…………… Name of Health Facility…………………..Date: ____/____/_____Start Time: ____/_____ End time: ____/____ (Total Time spent: _______) Name of Interviewer: ……………………
Section B: Respondents’ Particulars
Respondents ID Age Sex
Designation
Section C: Perceptions and Attitudes
1. Do you know the current national immunization schedule?1. Yes2. No
2. Can you mention types of vaccine given and the respective scheduled time for each? (Tick all that are mentioned)
Type of Vaccine When to be given Tick if mentioned
BCG At birth or first contact
25

OPV1, DTP-HepB-Hib 1,PCV1, Rotavirus 1 6 WeeksOPV2, DTP-HepB- Hib2, PCV2, Rotavirus 2 10 WeeksOPV3, DTP-HepB-hib3, PCV3 14 Weeks
MCV1 9 Months of age
MCV2 18 monthsVitamin A – 1st dose 9 Months of ageVitamin A – 2nd dose 15 Months of ageVitamin A – 3rd dose 21 Months of ageTT 1 First contactTT 2 1 Month after the 1st
doseTT 3 6 Months after the 2nd
doseTT 4 1 Year after the 3rd
doseTT 5 1 Year after the 4th
dose
3. What do you think about current immunization schedule? a. With regard to number of visits by the care givers to health facility (Tick if mentioned)
I. Too many visits II. No problem
III. No commentIV. Any other Comment_______________________
b. With regard to number of injections per visit (Tick if mentioned)
I. Too many injectionsII. No problem
III. No commentIV. Other( Mention)________________________
4. How many injections do you think can be given to a child at one visit?
I. Only 1II. Upto 2
III. Upto 3IV. More than 3
5. Do you receive any concerns/ complain from parents/care givers with regard to immunization schedule?
I. Yes II. No
What are their concerns (list down)
I. --------------------------------II. …………………………………………….
III. ………………………………………………..6. Who are the most affected by the concerns, how? (Tick and write explanation)
I. The Government II. Service Providers
III. Parents/caretakersIV. Children
26

V. All above7. What challenges do you face as a service provider with regard to the current immunization
schedule? (list below)I. ……………………………………………………………………
II. ………………………………………………………………….
III. …………………………………………………………………..
IV. …………………………………………………………………
8. Are you aware of plans to introduce IPV/ additional injection in the current Immunization schedule?
i. Yes II. No
8.1 IF YES, What are the details/ What do you know about it: ___________________________
_______________________________________________________________________________
9. What do you think will be the challenges of introducing multiple injections in the current immunization schedule?
I. Resources II. Storage
III. Human resourceIV. Parental concernsV. Risks of AEFI
VI. Other: ___________________10. Do you think introducing additional injection into the current immunization schedule will have
any effect to your work? I. Yes
II. NoExplain: ________________________________________________________________
11. What do you foresee as benefits of additional multiple polio injection in the immunization schedule?
I. Protecting Children II. Fewer vaccination visits
III. Increasing Efficiency IV. Other: ______________
11.1 What do you think are disadvantages of additional IPV injection in the current immunization schedule?
I. ____________________________________________II. ____________________________________________
III. ____________________________________________
12. Are you comfortable administering multiple injections to children at one visit? If not why?
I. ___________________________________________
II. ___________________________________________
13. How many injections have you been administering to a child in one single visit? Are you administering all injections as per the immunization schedule?
27

14. Up to how many injections are you willing to administer to a child on one single visit?
15. Agree or disagree with each of the following statement
I. Children Respond to Multiple Vaccines Given at the Same Time in a Manner Similar to Individual Vaccines _________________
II. Multiple Vaccines Overwhelm or Weaken the Infant’s Immune System _____________
III. Infants Have the Capacity to Respond to an Enormous number of Antigens___________
IV. Children are Exposed to Fewer Antigens in Vaccines today than in the past__________
16. Who do you think parents/caregivers listen to and believe in when receiving health/immunization information?
17. After vaccinating the child do you explain key messages to care/givers about immunization? If yes what do you tell them?
18. What do you think are the key messages to give to caregivers after their children receive IPV vaccination?
19. Before we close up our discussion, do you have any opinion or any issue you would want to address with regard to introduction of multiple injections in the current immunization schedule? ______________________________________________________________________________
______________________________________________________________________________
**THANK YOU**
Annex 6:Multiple Injection Questionnaire
The purpose of this brief questionnaire is to survey key immunization staff as well as caregivers to assess experiences related to administering and receiving multiple injections.
VACCINATOR Questions:
1. What is the age of the VACCINATOR? ______________ years
2. How many years of practice does the VACCINATOR have? _____________ years
3. What is the typical amount of time it takes for the vaccination visit in the EPI program (including administration of all vaccines, informing caretaker on next visit, record updating, and dispensing the syringe and vial)?
a. < 5 minutesb. 5-10 minutesc. 10-15 minutesd. 15-20 minutes
28

4. When is the record updated?a. After administration of each vaccineb. After administration of all vaccines
5. Does the vaccinator update immunization records or is there usually a second person who does the recording during an immunization visit?
a. Yesb. Noc. Don’t know
6. What was the VACCINATORS’ general attitude towards multiple injections during the first six months after the vaccine introduction?
a. No concernsb. Some concernsc. Moderate concernsd. Strong concerns
7. What was the VACCINATORS’ general attitude towards multiple injections AFTER the first six months of vaccine introduction?
a. No concernsb. Some concernsc. Moderate concernsd. Strong concerns
8. What are the VACCINATORS’ reasons for concern over multiple injections?a. Vaccine reactogenicityb. Adverse events following immunization (AEFI)c. Pain during multiple injectionsd. Caretaker would not bring child back for repeat visitse. Lack of data on efficacy of vaccine or burden of diseasef. Other: _________________________________________
9. What training for IPV introduction received by the VACCINATOR?a. Yesb. Noc. Don’t know
10. Did the VACCINATORS receive any guidance or recommendations on simultaneous injections from medical organizations or the MOH?
11. How many injections do the VACCINATORS think are too many to give in a single visit? ____________________
CARETAKER Questions:
12. What was the CARETAKERS’ general attitude towards multiple injections DURING the first six months after the vaccine introduction?
a. No concernsb. Some concernsc. Moderate concernsd. Strong concerns
29

13. What was the CARETAKERS’ general attitude towards multiple injections AFTER the first six months of vaccine introduction?
a. No concernsb. Some concernsc. Moderate concernsd. Strong concerns
14. What are the CARETAKERS’ reasons for concern over multiple injections?a. Vaccine reactogenicityb. Adverse events following immunization (AEFI)c. Pain during multiple injectionsd. Lack of VACCINATOR support on need for multiple injectionse. Lack of data on efficacy of vaccine or burden of diseasef. Other: _________________________________________
15. How many injections do the CARETAKERS think are too many to give in a single visit? ____________________
16. Do the CARETAKERS prefer to get all 3 shots during one visit or prefer separate visits?a. One visitb. More than one visitc. Don’t know
Annex 7:Sample M&E Indicators for Routine Immunisation and IPV
Programme and Process Indicators
Number of communication committees established Number of meetings held by each committee. Number of provinces using this guide for planning EPI activities. Number of districts developing integrated EPI/NID/Surveillance plans instead of free
standing NIDs plans. Number of committees commencing communication plans at least 8 months in advance of
NIDs. Quality of monitoring, documentation and reporting (e.g. reports received on time and
correctly completed). Type and quality of data received from the field for decision making. How data collected are used. Availability of structures and processes that promote joint planning, consultation and
information sharing between different EPI departments.
Knowledge
Percentage of caregivers reached by immunisation messages. Percentage of caregivers who know the minimum number of times they need to bring a child
for vaccination by age one year. Percentage of caregivers who know the linkage between RI and supplemental immunisation. Percentage of caregivers who can recognise the symptoms of AFP. Percentage of community leaders who know why they should report cases of AFP Percentage of community workers who can correctly identify the process for reporting AFP.
Attitudes
30

Percentage of caretakers who believe children should be immunised Percentage of caretakers who are convinced that immunisations given during RI sessions and
those given during NIDs are:- Use the same vaccine- Have the same effectiveness- Are both safe- Are both necessary
Percentage of caretakers convinced that it is necessary to notify health workers about children with AFP within 24 hours
Behaviour
Percentage of caretakers bringing children under one year to receive RI according to the vaccination schedule.
Percentage of caretakers bringing children under 5 years of age for both rounds of NIDs immunisations.
Partners and organisations participating in at least 80 per cent of the committees for NIDs and RI.
Training & Capacity Building
Percentage of planned training and capacity building activities:- Implemented - Implemented on time
The number of training activities using participatory training methods Number of people trained Number of supportive supervision activities carried out by the national level and district
teams Level of funds committed to training and capacity building
Sustainability
Level of political and leadership support. Level of government funding and donor funding. Structures established to support communications at different levels: national, district and
community. How often research data is used for planning communication activities. Quality of long range communication programmes developed. Level of community involvement in planning, funding, implementation, monitoring and
evaluation of communication activities. Level of decentralisation of resource allocation and programme management
31

32