implementation and execution of civilian rdcr...
TRANSCRIPT

Implementation and execution of civilian RDCR
programs – Minnesota RDCR
Donald H Jenkins, MD FACS Associate Professor of Surgery and Director of Trauma
Division of Trauma, Critical Care and Emergency General Surgery Saint Marys Hospital, Rochester MN
June 2013

Remote Damage Control: Civilian Experience in
the Pre-Hospital Setting
No Disclosures

Objectives
• Indications for treatment with blood products for traumatic hemorrhagic shock in the pre-hospital setting
• Monitoring devices used for coagulopathy and shock • Therapeutics utilized in these patients for pre-hospital
treatment of casualties • Evacuations of long durations compared to rapid ones • Methods of implementation to improve rapid
incorporation of recently initiated changes in practice

Remote Damage Control Resusc
• Austere/rural environment patients • Modified transfusion strategy • Different than those with scene/pre-hospital time < 30
minutes • Limited resources available • Lack of plasma availability • 40% of the population, 60% of the trauma mortality
• Current treatment options for uncontrolled hemorrhage in this environment are very limited
• >75% of combat fatalities occur in the field

Hartford Consensus February 2013
• Leaders in law enforcement, EMS, military and the American College of Surgeons
• Recommendations for civilian organizations to improve survival during active shooter scenarios
• Stress “the importance of early and definitive hemorrhage control to maximize survival in the victims….”

Hartford Consensus THREAT • T - Threat suppression • H - Hemorrhage Control • RE - Rapid Extraction to safety, • A - Assessment by medical providers • T - Transport to definitive care

Coagulopathy on Presentation
• An initial INR ≥ 1.5 reliably predicts those military casualties who will require MT.
• Pts who have a significant injury present with a coagulopathy.
• Severity of injury and mortality is linearly associated with the degree of the initial coagulopathy.
- Schreiber MA, Perkins JP, Kiraly L, Underwood SJ, Wade CE, Holcomb JB. Early Predictors of Massive Transfusion in Combat Casualties. Submitted, J Trauma. - Brohi K, et al. Acute traumatic coagulopathy. J Trauma. 2003.

Background
MacLeod JBA et al. Early Coagulopathy Predicts
Mortality in Trauma J Trauma 2003
Brohi K et al. Acute Traumatic Coagulopathy
J Trauma 2003
By the time of arrival at the ED, 28% (2,994 of 10,790) of trauma patients had a detectable coagulopathy that was
associated with poor outcome

Background
de Biasi et al. Early Coagulopathy Predicts Mortality in Trauma
Transfusion (Epub, Accepted 2010)
Mortality was associated with worse Plasma Deficit &
The efficacy of the Plasma Repletion occurs within hours

DoD Learned About Thawed Plasma
• Thawed plasma is FFP that is kept for up to 5 days at 4°C • This product should be present upon arrival of the casualty in
the ED • should be used as a primary resuscitative fluid started in the ED
• This approach not only addresses the metabolic abnormality of shock, but initiates reversal of the coagulopathy present in the ED.
• Thawed plasma is used in theater • The DoD Level 1 trauma center uses this product
• Decreases waste by 60-70%
- Malone DL, Hess JR, Fingerhut A. Comparison of practices around the globe and suggestion for a massive transfusion protocol. J Trauma, 2006. - Armand R, Hess JR. Treating coagulopathy in trauma patients. Transfus Med Rev 2003.

Early Use of Blood in the Pre-hospital Setting
• Mayo Clinic Experience • 1993-96 retrospective review • Criteria: Hgb<10, shock, hypotension after
resuscitation • ~2100 helicopter flights, 94 patients received
PRBC’s (4%, 91% interfacility transfer) • 48% trauma patients, 25% GI bleed, 38% AAA • Hgb increased from 8.9 to 10.2 after 2 PRBC • No transfusion reactions or complications • Average 12 u PRBC after admision • Age of RBC is < 14 days
Air Med J 1998 Zietlow and Berns
Age of Blood and Procoagulant Microparticles
• Historically, PCMP increases with age of blood
• 52 trauma patients vs 22 volunteers • Higher PCMP with injury; no difference
between transfused (n=19)/not transfused • 24 hour PCMP decreased with transfusion
• No decrease if no transfusion • Difference widened with increasing transfusion
Spinella Crit Care 2009 Jy Transfusion 2011 Rubin Transfusion 2010-12

Catchment Area
Rationale Coagulopathy & the “Golden
Hour”
• Trauma Induced Coagulopathy (TIC) predicts mortality
• Plasma and RBC resuscitation should occur early in the hemorrhagic / coagulopathic pt
• Catchment area / Rural location provides geographic obstacles
• Regional plasma deficiency

Protocol – ED Phase • Thawed Plasma Program • Developed in Feb 2008 with input from:
- Blood Bank Team - Transfusion Medicine - Medical Transport - Trauma, Critical Care and General Surgery
• Initial 9 months were restricted to in-hospital Emergency Department use
• Medical and Surgical emergencies - Safety concerns - Utilization of resources

• Product immediately available in the Trauma Resuscitation Area: - 4 units thawed plasma (A+) - 4 units PRBCs (0 negative)
• Order of transfusion for trauma patients was: • 2 units PRBC • 2 units thawed Plasma • 2 units PRBC • 2 units thawed Plasma
Protocol – Helicopter Phase
pRBC + Plasma 1. Hypotension (single reading
of systolic blood pressure < 90mmHg)
2. Tachycardia (single reading of heart rate ≥ 120)
3. Penetrating mechanism 4. Point of care lactate ≥ 5.0
mg/dl 5. Point of care INR ≥ 1.5
Indications for PRBC and Plasma administration in adult trauma patients
Plasma Alone 1. Point of care INR ≥ 1.5 2. Stable Hemodynamics


Waste Prevention Division of Transfusion Medicine monitors
usage
- Thawed plasma is removed from the satellite blood refrigerator on Day #3 and sent to the Operating Theater for immediate use.

Mayo Helicopter Transfusion Criteria

RESULTS
• 5 for hemorrhage • 3 required massive transfusion (> 10 units/24 hours)
• 5 pts transfused for history of trauma and coumadin use
• All 4 deaths were in this group
• All pts entered into protocol required ongoing blood product transfusion after arrival to the hospital.
10 TRAUMA PATIENTS TRANSFUSED IN FLIGHT 2/2009 – 9/2010
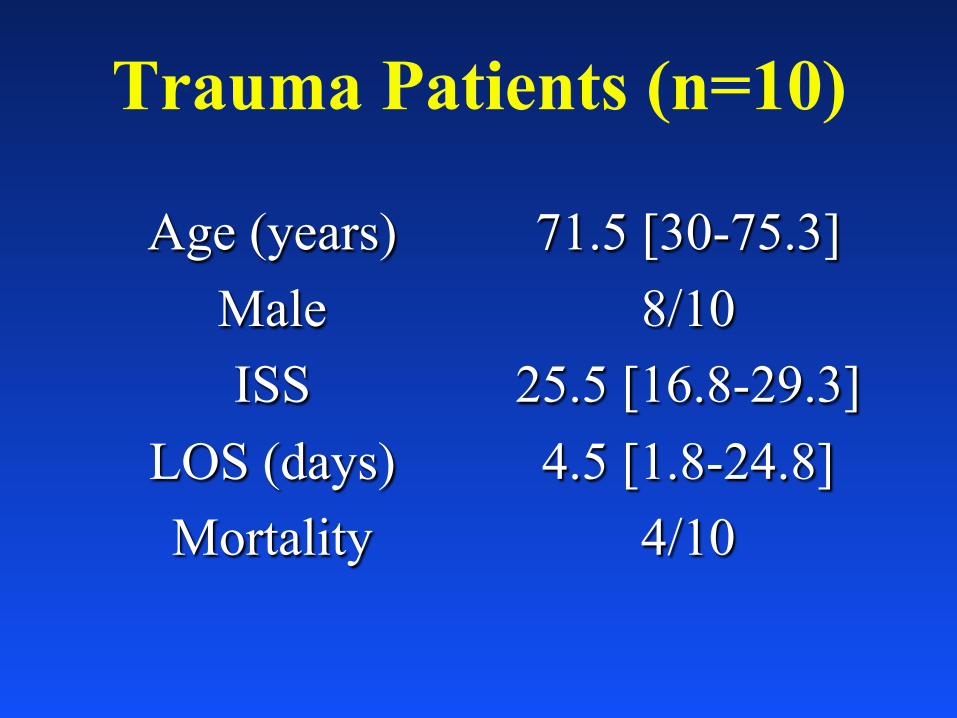
Trauma Patients (n=10)
Age (years) Male ISS
LOS (days) Mortality
71.5 [30-75.3] 8/10
25.5 [16.8-29.3] 4.5 [1.8-24.8]
4/10

Admission Laboratory Values Coumadin 5/10 (50%) Lactate 2.8 [1.7-5.7] Base -4.1 [-12.5- -0.5] PLT 149 [114-180] PTT 30 [28-42] HgB 10.8 [10.1-13.5] Post-Flight INR 1.6 [1.3-2.8] Pre-Flight INR 2.7 [1.6 – 4.0]

Feasibility
• Excellent utilization • No discarded units of plasma to date
• No transfusion reactions documented to date; use of product parallels massive transfusion in the standard setting

Protocol Evolution
• During the study period, total of 771 flights • Only two pts received all 4 units of PRBC
during transport • Product Order and Ratio
• 2009: 2 PRBC, 2 Plasma, 2 PRBC • 2010: 2 Plasma, 2 PRBC, 2 PRBC • 2011: 3 Plasma, 3 PRBC

Hemostatic Resuscitation in Our Trauma Center
• Pre-hospital plasma and POC testing • INR/Lactate pre-hospital
• Early Diagnosis in ED – StO2/i-Stat • 1:1 ratio (thawed plasma to RBC)
• Plasma-first transfusion sequence • ED use of PCC?
• Frequent TEG and early platelet use • Minimal crystalloid • Repeated doses of PCC and/or transfusion
in OR and ICU as required by TEG • Young red cells (<14 days)

Ratios / Plasma Balance PTP (n=9) Control (n=50) p
En Route P:RBC 1.3 : 1.0 N/A <0.001 30 min P:RBC 1.3 : 1.0 0.14 : 1.0 <0.001 6 hr P:RBC 1.0 : 1.0 0.42 : 1.0 <0.001 24 hr P:RBC 1.0 : 1.0 0.45 : 1.0 <0.001 En Route Plasma Deficit - 0.4 - 1.0 0.32 30 min Plasma Deficit - 1.2 - 2.0 0.37 6 hr Plasma Deficit - 1.7 - 5.3 0.06 24 hr Plasma Deficit - 1.0 - 5.7 0.04

Time & the ‘Geographic Plasma
Deficit’
PTP (n=9) Control (n=50) p Facility Transfer 100% 54% 0.002 Transport à Trauma Ctr (min) 40 39 0.78 Injury à First Plasma (min) 194 231 0.58 Trauma Ctr arrivalàPlasma (min) - 34 97 0.013

• ABO-identical preferred • Universal plasma donor
• Group AB • Lacks anti-A/anti-B • Pan-ABO compatible • Rarest blood group
Group A Plasma Transfusion Introduction
Inaba K et al. Arch Surg 2010
Group A Plasma Transfusion Group AB supply
• Recent safety data • ABO incompatible platelets
• 1 – 2 plasma units
• 1 in 9000 hemolysis
• Group O
• Immunosuppression
Isaak EJ et al. Immunohematology 2011 Josephson CD et al. Transfus Apher Sci 2010

• 10,206 patients over study period • Trauma patient • July 2008 – June 2012 • ≥ 1 unit emergency release plasma (group A
plasma) • 258 emergency release plasma (2.5%)
• 4 died prior to blood grouping
Group A Plasma Transfusion Results
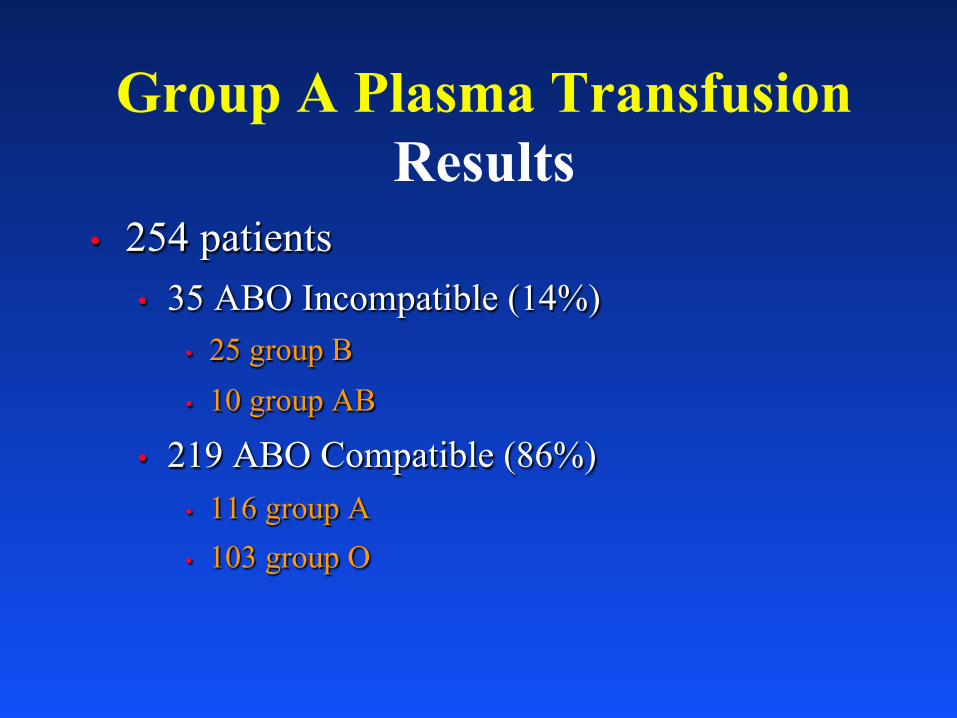
• 254 patients • 35 ABO Incompatible (14%)
• 25 group B • 10 group AB
• 219 ABO Compatible (86%) • 116 group A • 103 group O
Group A Plasma Transfusion Results

Feature ABO Incompatible n = 35 ABO compatible
n = 219 P
Age (years) 56 (39-79) 59 (32-79) 0.944 Male sex 63% 63% 0.973 ISS 25 (16-37) 22 (12-30) 0.199 TRISS 0.86 (0.26-0.97) 0.93 (0.34-0.97) 0.880 Scene transfer 34% 38% 0.710 Time from injury to trauma
bay admission (mins) 145 (54-185) 172 (92-230) 0.214 Time in trauma bay (mins) 24 (20-35) 26.5 (20-36) 0.883 Time at referring hospital 119 (96-144) 121 (70-172) 0.920
Group A Plasma Transfusion Results
Group A Plasma Transfusion Results
ABO Incompatible n = 35 ABO compatible
N = 219 P
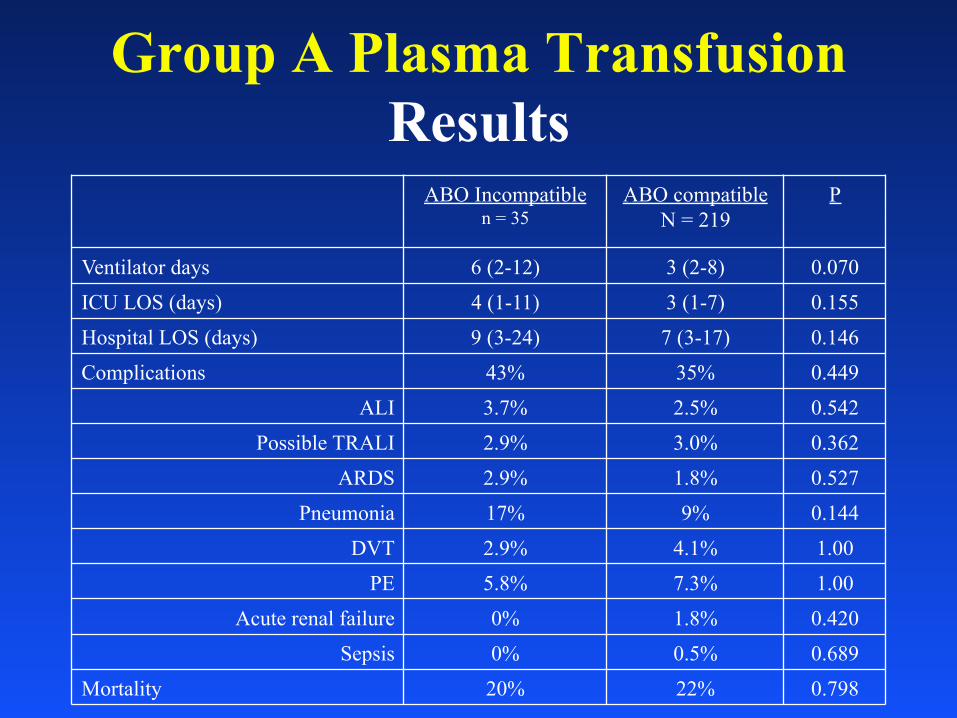
Ventilator days 6 (2-12) 3 (2-8) 0.070 ICU LOS (days) 4 (1-11) 3 (1-7) 0.155 Hospital LOS (days) 9 (3-24) 7 (3-17) 0.146 Complications 43% 35% 0.449
ALI 3.7% 2.5% 0.542 Possible TRALI 2.9% 3.0% 0.362
ARDS 2.9% 1.8% 0.527 Pneumonia 17% 9% 0.144
DVT 2.9% 4.1% 1.00 PE 5.8% 7.3% 1.00
Acute renal failure 0% 1.8% 0.420 Sepsis 0% 0.5% 0.689
Mortality 20% 22% 0.798

Group A Plasma Transfusion Results
ABO Incompatible n = 35
ABO compatible N = 219
P
Ventilator days 6 (2-12) 3 (2-8) 0.070 ICU LOS (days) 4 (1-11) 3 (1-7) 0.155 Hospital LOS (days) 9 (3-24) 7 (3-17) 0.146 Complications 43% 35% 0.449
ALI 3.7% 2.5% 0.542 Possible TRALI 2.9% 3.0% 0.362
ARDS 2.9% 1.8% 0.527 Pneumonia 17% 9% 0.144
DVT 2.9% 4.1% 1.00 PE 5.8% 7.3% 1.00
Acute renal failure 0% 1.8% 0.420 Sepsis 0% 0.5% 0.689
Mortality 20% 22% 0.798

Group A Plasma Transfusion Results
ABO Incompatible n = 35
ABO compatible N = 219 P
Ventilator days 6 (2-12) 3 (2-8) 0.070 ICU LOS (days) 4 (1-11) 3 (1-7) 0.155 Hospital LOS (days) 9 (3-24) 7 (3-17) 0.146 Complications 43% 35% 0.449
ALI 3.7% 2.5% 0.542 Possible TRALI 2.9% 3.0% 0.362
ARDS 2.9% 1.8% 0.527 Pneumonia 17% 9% 0.144
DVT 2.9% 4.1% 1.00 PE 5.8% 7.3% 1.00
Acute renal failure 0% 1.8% 0.420 Sepsis 0% 0.5% 0.689
Mortality 20% 22% 0.798

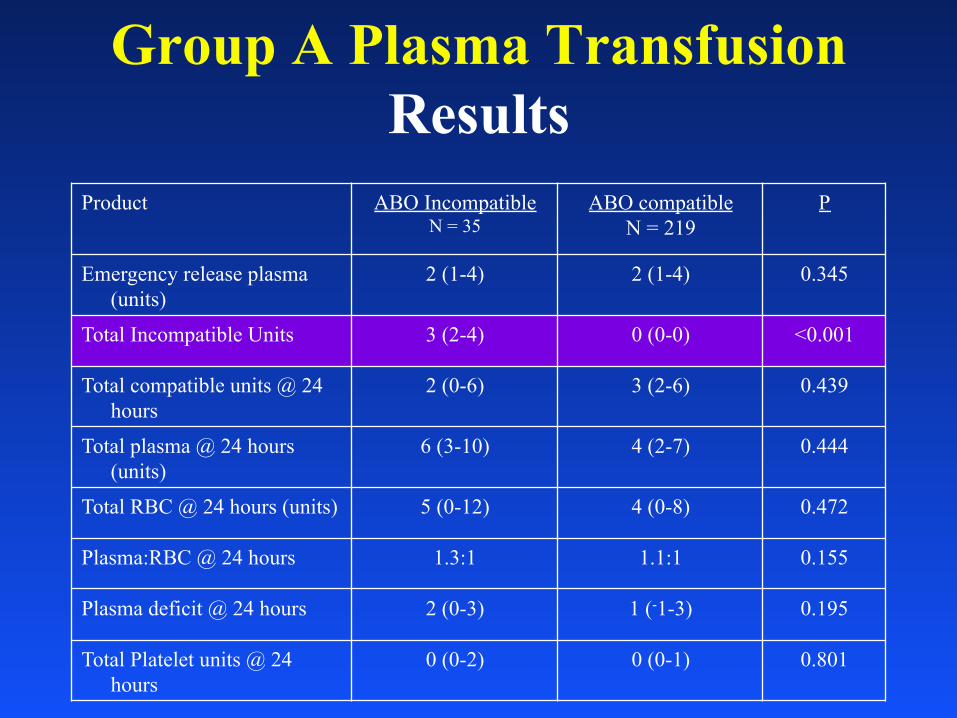
Product ABO Incompatible N = 35
ABO compatible N = 219
P Emergency release plasma
(units) 2 (1-4) 2 (1-4) 0.345 Total Incompatible Units 3 (2-4) 0 (0-0) <0.001 Total compatible units @ 24
hours 2 (0-6) 3 (2-6) 0.439 Total plasma @ 24 hours
(units) 6 (3-10) 4 (2-7) 0.444 Total RBC @ 24 hours (units) 5 (0-12) 4 (0-8) 0.472 Plasma:RBC @ 24 hours 1.3:1 1.1:1 0.155 Plasma deficit @ 24 hours 2 (0-3) 1 (-1-3) 0.195 Total Platelet units @ 24
hours 0 (0-2) 0 (0-1) 0.801
Group A Plasma Transfusion Results
Product ABO Incompatible N = 35
ABO compatible N = 219
P Emergency release plasma
(units) 2 (1-4) 2 (1-4) 0.345 Total Incompatible Units 3 (2-4) 0 (0-0) <0.001 Total compatible units @ 24
hours 2 (0-6) 3 (2-6) 0.439 Total plasma @ 24 hours
(units) 6 (3-10) 4 (2-7) 0.444 Total RBC @ 24 hours (units) 5 (0-12) 4 (0-8) 0.472 Plasma:RBC @ 24 hours 1.3:1 1.1:1 0.155 Plasma deficit @ 24 hours 2 (0-3) 1 (-1-3) 0.195 Total Platelet units @ 24
hours 0 (0-2) 0 (0-1) 0.801
Group A Plasma Transfusion Results

Product ABO Incompatible N = 35
ABO compatible N = 219
P Emergency release plasma
(units) 2 (1-4) 2 (1-4) 0.345 Total Incompatible Units 3 (2-4) 0 (0-0) <0.001 Total compatible units @ 24
hours 2 (0-6) 3 (2-6) 0.439 Total plasma @ 24 hours
(units) 6 (3-10) 4 (2-7) 0.444 Total RBC @ 24 hours (units) 5 (0-12) 4 (0-8) 0.472 Plasma:RBC @ 24 hours 1.3:1 1.1:1 0.155 Plasma deficit @ 24 hours 2 (0-3) 1 (-1-3) 0.195 Total Platelet units @ 24
hours 0 (0-2) 0 (0-1) 0.801
Group A Plasma Transfusion Results
Group A Plasma Transfusion Discussion
• Emergency plasma use is increasing
• Limited access
• “New” universal
donor resulted in 97.6% reduction in AB plasma use

Group A Plasma Transfusion Discussion
• Group A plasma has equivalent outcomes to group AB • Incompatible transfusions occurred • No hemolytic reactions • Similar mortality • Similar immunogenic complications
• Limitations
• Small comparison group
• Type II error potential
• Post-hoc analysis

43
CRASH-2 Study Lancet, Online Article, 2010
• Prospective, randomized controlled trial • 20,211 patients • TXA significantly reduced all cause mortality from 16.0% to
14.5% • TXA significantly reduced death due to bleeding from 5.7% to
4.9% 43

44

45


StO2

Beilman Study • Over a 15-month period, seven Level I trauma centers in
the USA enrolled 383 patients, 50 of whom developed MODS
• StO2 below 75% indicates serious hypoperfusion in trauma patients
• 78% of patients who developed MODS, and 91% of patients who died, had StO2 below 75% in the first hour
• Trauma patients who maintained StO2 above 75% within the first hour had an 88% chance of MODS-free survival
J Trauma 2006

Can early StO2 predict the need of blood product requirement in trauma
population?
Total 632 level 1 trauma 325 patients with recorded StO2

Variable StO2< 65
n=23 StO2>65
n=302 p
Systolic blood pressure, (SD) NS Heart rate, (SD) NS
Scene Assessment

Variable StO2< 65
n=23 StO2>65
n=302 p
Systolic blood pressure, (SD) 0.23 Heart rate, (SD) 0.39 Respiratory rate, (SD) 0.06 O2 saturation, (SD) 0.2
Temperature, (SD) 36.1 (1.2) 36.6 (0.7) Trauma score, (SD) 9 (2) 10 (2) Glasgow coma score, (SD) 7.7 (6) 10 (6)
Emergency Department Assessment

Variable StO2< 65
n=23
StO2>65 n=302
p
Hemoglobin, (SD) NS Hematocrit, (SD) NS pH, (SD) NS Base deficit, (SD) NS Lactate, (SD) 3.9 (3.2) 2.4 (2.1) FAST done NS Positive FAST NS
Laboratory Results and FAST

Variable StO2< 65
N=23
StO2>65 N=302
p
ICU days, (SD) NS Hospital length of stay, (SD) NS Mortality NS
Surgical interven.on 18 (78%) 152 (50%) Morbidity 11 (48%) 68 (23%)
Outcomes
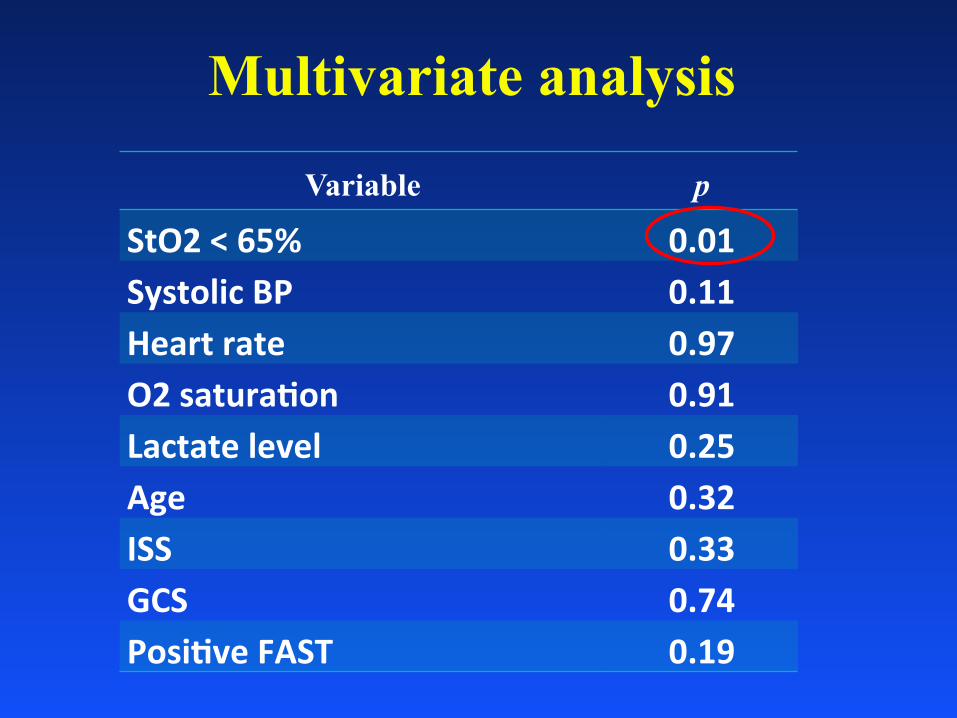
Multivariate analysis
Variable p
StO2 < 65% 0.01 Systolic BP 0.11 Heart rate 0.97 O2 satura.on 0.91 Lactate level 0.25 Age 0.32 ISS 0.33 GCS 0.74 Posi.ve FAST 0.19

Current Status • All 3 Mayo helicopter bases carrying 3 PRBC
and 3 thawed plasma • All 3 use same transfusion triggers • All 3 use i-Stat INR and ABG cartridges • All 3 carry TXA; uses similar triggers but has
some limitations for use • Just added StO2 as a trigger • Limited waste at all 3 sites • No crystalloid for those with hemorrhage • Tourniquets and Combat Gauze on all 3 ships

The Future • Freeze dried plasma? • Whole blood? • Platelets? • Prothrombin complex concentrates?

Why Freeze Dried Plasma?
Remote Damage Control Resuscitation!


Implementation of Change • Consensus • Review of the literature and our own data • Practicality and safety are first order of
business with best interest of patient in mind • Continuous monitoring of program • Education of all health care providers • Willingness of blood bank and transfusion
medicine to consider novel use of products

Overall System Results • Current era (2011) compared to the era
before pre-hospital plasma • Referrals up (838 vs 998*) • ISS up (9 vs 12*) • Mortality same (2.5% vs 2.2%) • Observed decline open abdomen (under study) • Observed decline in massive tx (under study) • Arrival TEG improved? (under study)

Summary • Trauma patients die from shock • Our job is to limit preventable trauma death • First, identify the patient in shock • Pre-hospital resuscitation with plasma can
prevent the trauma induced coagulopathy and limit the risk of death due to hemorrhage
• Making dried plasma available in the rural and pre-hospital/austere environment will save lives

Thank You!

Questions?