implantrealities june 04 -...
TRANSCRIPT

Implant RealitiesAchieving success in implant dentistry
Vol. II • issue 3 • 2004
I N T E R N AT I O N A L E S T E A M F Ü R I M P L A N T O L O G I EI N T E R N AT I O N A L T E A M F O R I M P L A N T O L O G Y

Feature articles
4
New Options in Prosthetic Reconstruction
Robert C. Vogel, DDSPalm Beach Gardens, FL
9
Treatment Planning Implications of Implant Dentistry in the Partially Edentulous Patient
Paul A. Fugazzotto, DDSMilton, MA
7
The Use of Extended Healing Caps with the Straumann Dental Implant
Jay Beagle, DDS, MSDIndianapolis, IN
14
Treatment Options in Reconstruction of the Posterior Dentition
Part 2: Planning and Treatment Considerations for Implant-Assisted Restorations in
the Posterior Maxilla: Esthetic
Dean Morton, BDS, MS; Will Martin, DMD, MS; James Ruskin, DMD, MD (University of Florida Center for Implant Dentistry); Todd Fridrich, CDT (Straumann USA, Inc.)

22
Immediate Loading of the Full-Arch Maxilla with Cemented Provisional Restorations
Using Angled synOcta® Abutments
Jeffrey Ganeles, DMD, FACD; Frederic J. Norkin, DMD; Julio Sekler, DMD, MMScBoca Raton, FL
18
An Alternative Abutment for Deep Implant Placements in the Esthetic Zone Utilizing
the synOcta® Meso Abutment
Frank L. Higginbottom, DDSDallas, TX
26
Factors in Implant Supported Mandibular Overdenture Designs
David Todd, DMD, MDLakewood, NY

In every issue
Editor’s Note 1
Editorial 2
Feature Articles 4
Literature Review 29
Upcoming Events 32
Senior Editor: Paul A. Fugazzotto, DDSPlease feel free to contact me with any questions, comments, or submissions at [email protected].
Surgical Editor: Jay Beagle, DDS, MSDWhile the basic protocols for insertion of osseo integrating implants are well established, the field is now characterized by many exciting and innovative modifications of proven techniques. We will explore newer therapies, offer appropriate and helpful clinical “pearls” and remain on the cutting edge. Please contact me with any questions or submissions at [email protected].
Restorative Editor: Frank L. Higginbottom, DDSThe restorative portion of this publication will address common problems, concerns, and interests of usersof the Straumann® Dental Implant System. Both conventional and complex issues will be addressed. This section of the publication is hosted by US ITI members and other serious implant users and will serve as a venue for interesting case presentations as well as a sounding board for questions and answers to actual clinical quandaries. Please feel free to contact us with any concerns you may have at any time. In addition, if you feel you have valuable information to submit for consideration for publication, please e-mailme at [email protected] or phone me at 247/827-1150.
Laboratory Editor: Ira Dickerman, AAS, CDTThe laboratory technician plays an integral role in the success of implant restorative therapy. Beginning with input at the diagnostic and treatment planning phase, the appropriate utilization of the laboratory technician is crucial to the maximization of treatment outcomes. This section of the publication will explore the technical aspects of implant laboratory procedures as well as the role of the laboratory technician in diagnosing and treatment planning of both simple and complex cases. Please call me at 781/828-2808.
Editorial Board: Terry Charters, CDTDavid Cochran, DDS, PHDJeffrey Ganeles, DMD, FACDRobert A. Jaffin, DMDRobert A. Levine, DDS, PCH.P. Weber, DMDArnold S. Weisgold, DDS
Printing: Quinn Printing Co., Newton, MA
The opinions expressed in articles signed by the authors are not necessarily those of the publisheror the editors.

Welcome to Implant Realities
Implant therapy has irreversibly impacted the practice of clinical dentistry. While the opportunity to
utilize newer therapies is obvious, the deep seated influence of implant treatment approaches is
more subtle but no less dramatic. It could be argued that the DNA of clinical dentistry has evolved.
The recrudescent outcomes of many treatment approaches once utilized in attempts to manage
various disease entities due to limitations in treatment options need no longer be tolerated.
This issue of Implant Realities explores the unique manners in which various clinicians have dealt
with clinical challenges through the incorporation of well thought implant treatment modalities into
their clinical armamentaria.
As always, I hope that you enjoy this issue of Implant Realities, and welcome your comments and
manuscript submissions.
Sincerely,
Paul A. Fugazzotto, DDS
Senior Editor, Implant Realities

Past Performance is No Guarantee of Future Results
Arnold S. Weisgold, DDS
The title of this editorial is taken fromthe fine print often found at the bottomof many mutual fund advertisements.Paraphrased, it could very well beused as the heading for a discussionof esthetics and anterior implants,especially the single tooth variety.
If you are a little bewildered andbedazzled by promotional glitzaccompanied by glamorous photo-graphs and computer graphics aswell as intimidated by resonantvoices extolling better-than-life estheticresults, don’t despair - you are notalone! Proudly, but sadly, I must saythat I am too.
The “Holy Grail” of the dental professionis empowerment that it is able totransform a large measure of its owntreatment approach. Surely the adventof the endosseous implant hasachieved this. The forebearers of thisconcept flew in the face of acceptedpractices and made a mark on thelandscape of the profession. They seta standard of excellence by whichfuture efforts will be measured.
Concurrent with the enthusiasmgenerated by the endosseous implanthas been equal excitement engenderedby dental esthetics. By coincidencemore than design, these two areasseem to have become popular aboutthe same time (approximately the midto late 1980s). Originally, their basicobjectives appeared to be ‘worldsapart,’ but over the past decade or so,major advances have come about thathave provided us with the means tomake implants ‘look like teeth.’
My great concern of late is that in oureagerness to achieve the ultimateesthetic result, we may fail to realizethat sometimes this may be impossible.
Often in the lectures that I attend orpapers that I read, I only see outstandingresults. Rarely do I see esthetic failures.Sometimes I wonder if I’m the onlyone who has them!
Clinical practice is as much art andjudgment as it is science, and at timesit is inherently uncertain. Good cliniciansseek up-to-date information and advicefrom the courses they attend and thejournal articles they read. Unfortunately,less than forthright clinicians andquestionable papers found even inpeer-reviewed publications might makedental practice even more uncertain.
Occasionally, I have been asked toreview and comment on papers thathave been submitted for publicationto various journals. I have seensituations where the “post-operative”photograph doesn’t belong to thesame patient as the “pre-operative”one. Other times I have seen porcelainlaminates placed on the teeth adjacent
to the implant, but the author failed tomention that they were placed thereto mask the “black triangles” betweenthe implant and teeth. It is quitedisconcerting to see beautifulphotographs (with lips fully retracted)of the pre-operative condition, surgicaltechniques, interim prostheticprocedures, etc. but the lips not fullyretracted for the post-operative view.As the reader of the paper, do I assumethe result is excellent or otherwise?Fortunately, these situations are rare,but on occasion they do occur.
The linchpin of therapy is diagnosis.Esthetic diagnosis is about strategicissues; treatment is about tactical ones.All successful concepts of dentalesthetics have similarities; allunsuccessful ones are unsuccessful.We all deal with the same problems:thin, delicate tissues that recedeinterproximally, triangular shapedteeth that result in “black triangles,”implants placed too far to the facial or
Implant Realities2

Vol. II • issue 3 • 2004 3
towards the palate, implants positionedtoo close to adjacent natural teeth, and/or implants placed too far apically ornot far enough. All of us are confrontedwith deficient edentulous ridges. About10% of anterior edentulous spaceshave adequate volume to place animplant ideally so as to achieve theultimate esthetic result. But in mostinstances (approximately 90% of thetime) we are faced with less than idealsituations. Once we recognize theseproblems (and see more of them inlectures and journal articles), we willbe better equipped to deal with themor at least inform our patients before-hand that a less than desirable resultmay be in the offing. It will also allowus to take steps (such as ridgeaugmentations) to correct certainproblems.
There used to be a Rolls-Royceadvertisement that states, “The Rolls-Royce automobiles do not break down– however, on occasion they fail toproceed.” Again, to draw a parallel toour profession, “Endosseous implantsusually do not break down – however,on occasion they fail to look life-like.”Auspiciously, the vast majority ofclinicians and authors are highlyprincipled and passionately dedicatedto their work. What we must see aremore of their problems, failures, andclinical compromises (as someonesaid, their “closet cases”). Furthermore,for those clinicians just beginning ontheir ‘journey’ with the single toothanterior implant, my only advice is thatthey not become discouraged – it’sgoing to take a long time to reach anacceptable level of predictability andexpertise. As to my own experience, it surely has been one of the mostdifficult and challenging proceduresI’ve had to learn. Like the gentlemanin New York who asked a passerby,“How do I get to Carnegie Hall?” withthe answer, “Practice, practice,practice,” one has to train the mindand eyes to uncover the varioussubtleties and nuances that are soimportant in dental esthetics.
The endosseous implant has providedus with the opportunity to replace an
anterior tooth without resorting to the“classical” fixed bridge. What a greatinnovation! However, it is not without amodicum of uncertainty and perplexity.Recently I presented a full day seminaron the single tooth anterior implant.Much of the day was spent dealingwith problems (again, I may be theonly one with these difficulties). At theconclusion of my lecture a youngwoman approached the podium,complimented me, and thanked mefor sharing my experiences with theaudience. Her final comment was avery telling one – after listening to mypresentation she was convinced that,“the single tooth maxillary anteriorimplant is not a game for the well-adjusted.” I thought about this for afew days, and you know what? She iscorrect!
The consistent predictability andproven reliability of osseointegratedimplants have opened new possibilitiesin prosthetic reconstruction.
By incorporating today’s technologyand clinical techniques into one ofdentistry’s oldest and often-dreadedprocedures — the removable partialdenture (RPD) — optimal results canbe achieved. This will allow theclinician to provide greater comfortand function for the patient whilehelping to preserve the bone, therebyincreasing the patient’s and clinician’ssatisfaction.
With the introduction of implantdentistry, the indication for RPDs hasdecreased to limited situations andoften only as a last resort treatmentoption. In addition to the lack of idealesthetics, the potential detrimentsfrom removable partial dentures tothe natural dentition and edentulousareas are many: continued oraccelerated bone loss, traumaticfunctional and parafunctional forces,uncontrolled movement transmittedto often compromised abutment teeth,the presence of unsightly clasps, andthe reduction and splinting of naturalteeth for precision attachments. Whileall these compromises can be
addressed by dental implants, thereare still situations when an RPD is aviable option due to such limitationsas health or finances.
Even when a conventional RPD isfabricated to the highest possiblequality, many patients still presentwith ongoing complications. Situationssuch as irregular or thin mucosacovered ridges and resultant chronicirritation of the load-bearing tissuesor increasing tooth mobility fromtraumatic functional or uncontrolledforces can now be successfullytreated with new options.
The incorporation of dental implantsinto this area of prosthetic dentistry
New Options in Prosthetic Reconstruction
Robert C. Vogel, DDS
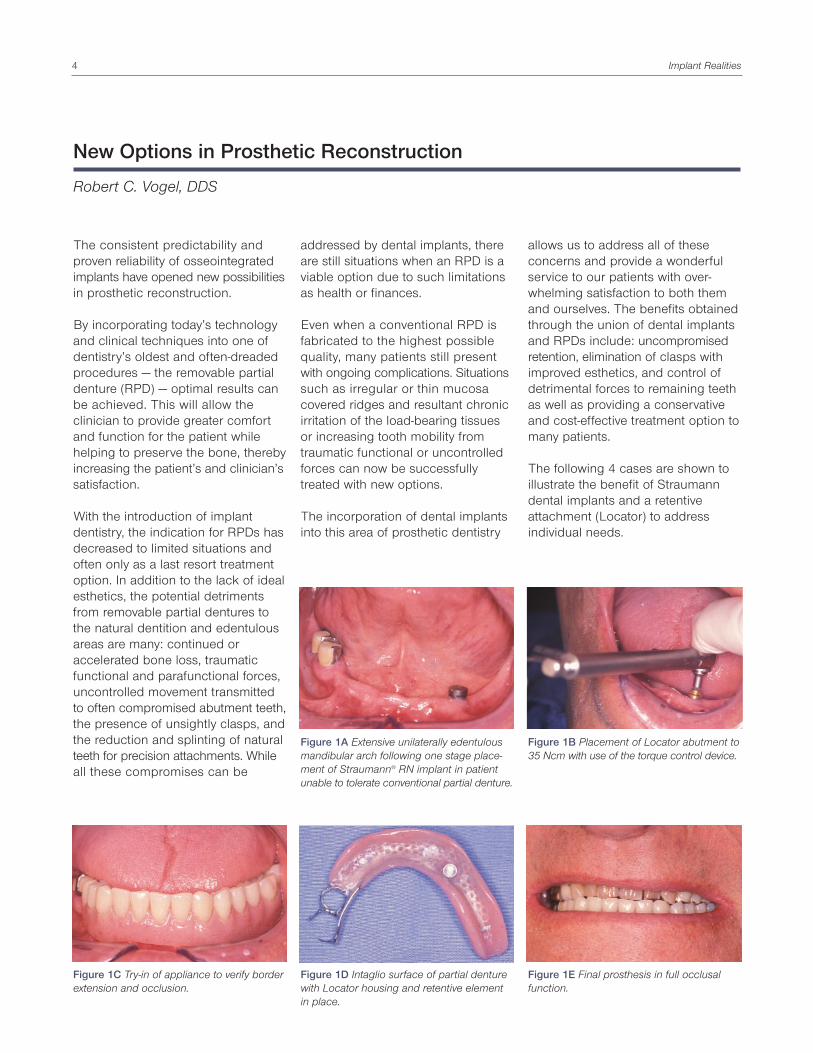
Figure 1C Try-in of appliance to verify borderextension and occlusion.
Figure 1A Extensive unilaterally edentulousmandibular arch following one stage place-ment of Straumann® RN implant in patientunable to tolerate conventional partial denture.
Figure 1E Final prosthesis in full occlusalfunction.
Figure 1D Intaglio surface of partial denturewith Locator housing and retentive elementin place.
Figure 1B Placement of Locator abutment to35 Ncm with use of the torque control device.
allows us to address all of theseconcerns and provide a wonderfulservice to our patients with over-whelming satisfaction to both themand ourselves. The benefits obtainedthrough the union of dental implantsand RPDs include: uncompromisedretention, elimination of clasps withimproved esthetics, and control ofdetrimental forces to remaining teethas well as providing a conservativeand cost-effective treatment option tomany patients.
The following 4 cases are shown toillustrate the benefit of Straumanndental implants and a retentiveattachment (Locator) to addressindividual needs.
Implant Realities4

Figure 2A Placement of Straumann dentalimplant and Locator abutment following lossof natural tooth abutment crown andassociated precision attachment.
Figure 2B Final prosthesis with implantattachment in place eliminating the need fortraumatic/unesthetic clasping of lateralincisor while providing ideal retention.
Figure 3A Severely atrophic unilaterallyedentulous ridge with thin mucosa resultingin chronic sore spots and traumatic toothmobility following placement of twoStraumann® RN dental implants.
Figure 3B Placement of two resilient Locatorattachment abutments.
Figure 3C Intaglio surface of appliance withretentive elements in place.
Figure 3D Final appliance ready for delivery.
Case 1
Unilateral distal extension partialdenture with chronic lateral movementresulted in traumatic rotational forcesand lifting of the saddle due to lackof cross arch retention. The Locatorattachment provides ideal retentionand limitation of excessive lateralmovement as well as functionalstimulation of the residual edentulousridge, which helps to preserve bone.
Case 2
Maxillary right cuspid (a tooth criticalfor a partial denture abutment and itsassociated precision attachment) waslost to recurrent decay and fractured tothe gingival level. The Straumanndental implant and Locator attachmentprovide an ideal esthetic solution byeliminating need for an anterior claspand protect remaining natural teethfrom traumatic forces. This can furtherserve as an ideal transitional appliancewhile the patient undergoes sinusaugmentation and additional implantplacement for a posterior fixed bridge.Note: an existing appliance can beimmediately retrofitted to accept thelow profile attachment.
Case 3
Patient presented with a severelyatrophic flat ridge with thin mucosa,chronic sore spots, and toothmobility. Two implants and resilientattachments provide ideal retentionand shared load with the residualridge by limiting traumatic forces tothe teeth and underlying denturebase. This solution can easily betransitioned to a conventionaloverdenture should the remainingteeth be lost and additional implantsplaced.
Case 4
Ideal esthetics and uncompromisedretention are achieved with a clasplesspartial denture; the palatal majorconnector provides support toocclusal forces and reduces stress
Figure 3E Appliance in function for 3 monthswith complete elimination of sore spots andtooth mobility.
Vol. II • issue 3 • 2004 5
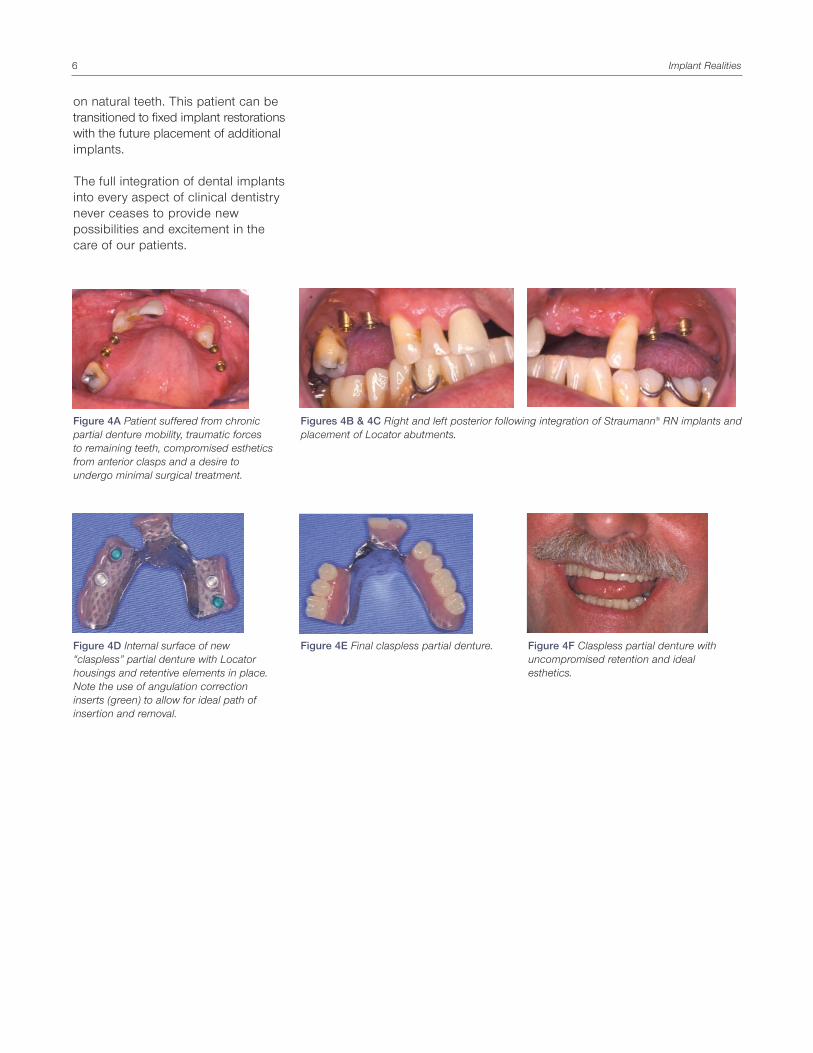
Figure 4E Final claspless partial denture. Figure 4F Claspless partial denture withuncompromised retention and idealesthetics.
on natural teeth. This patient can betransitioned to fixed implant restorationswith the future placement of additionalimplants.
The full integration of dental implantsinto every aspect of clinical dentistrynever ceases to provide newpossibilities and excitement in thecare of our patients.
Figures 4B & 4C Right and left posterior following integration of Straumann® RN implants andplacement of Locator abutments.
Figure 4A Patient suffered from chronicpartial denture mobility, traumatic forcesto remaining teeth, compromised estheticsfrom anterior clasps and a desire toundergo minimal surgical treatment.
Figure 4D Internal surface of new“claspless” partial denture with Locatorhousings and retentive elements in place.Note the use of angulation correctioninserts (green) to allow for ideal path ofinsertion and removal.
Implant Realities6

The Use of Extended Healing Caps with the Straumann Dental Implant
Jay Beagle, DDS, MSD
Since its inception, the Straumann®
Dental Implant System has been theinnovator with regards to non-submerged surgical placement andhealing. Clinical studies have shownthe success of non-submerged implantsto be equal to or greater than thatachieved with traditional submergedsurgical methods.1 Non-submergedtechniques offer the advantages of asingle surgical procedure, preservationof keratinized mucosa, reduced cost,and accelerated soft tissue maturation.
Non-submerged placement ofStraumann dental implants requirespositioning the SLA® surface and thesmooth collar interface at the osseouscrest, with the shoulder of the implantplaced at the level of the soft tissuejunction2 (Figure 1). To preventmigration of the mucosa over the
coronal aspect of the implant, anextended healing cap of appropriateheight is chosen (Figures 2, 3, 4). Theheight should be tall enough tostabilize the soft tissues and maintaina transmucosal healing pattern yetshort enough to prevent any unwantedloading of the implant with the tongue,mastication of food, or the wearing of aremovable prosthesis. An exception tothis technique should be followedwhen implants are placed in Type IVbone quality. In these instances,prevention of premature occlusalloading is paramount. The placementof an internal closure screw is thenindicated, using a semi- or fullysubmerged closure technique. Theclosure screw is then replaced by anextended healing cap at the time ofsecond stage surgery, 12 weeks later.Placement of dental implants
involving the esthetic zone in thepartially edentulous patient oftenprecludes the use of a non-submerged placement technique.Many of these patients present withosseous and soft tissue topographythat is not scalloped, but flat, andwhich does not support the re-creationof interdental papillae. Salama et al.3
suggest that to achieve gingivalharmony with adjacent soft tissues,the interproximal papillae associatedwith dental implants must also bereconstructed. This generally requiresthat the soft tissue be developed notonly horizontally but also vertically.Corn4 suggests that during soft tissueridge augmentation, “dead space”can be created in flap management.He proposed that the space would fillnaturally with soft tissue to enhancethe augmentation procedure. This is
Figure 1 Proper positioning of a Wide Neckhealing cap.
Figure 2 Flaps sutured around 3.0 mm WideNeck healing cap.
Figure 3 Healing caps for Regular NeckStraumann dental implants.
Figure 4 Healing caps for Wide NeckStraumann dental implants.
Figure 5 Beveled healing caps for theStraumann® Dental Implant System.
Figure 6 Buccal view of 3.5 mm beveledhealing cap prior to flap closure.
Vol. II • issue 3 • 2004 7

Figure 7 Occlusal view of 3.5 mm beveledhealing cap prior to flap closure.
Figure 8 Buccal view of semi-submergedclosure with beveled healing cap.
Figure 9 Occlusal view of semi-submergedclosure with beveled healing cap.
Figure 11 Buccal view of customized PEEKhealing cap.
Figure 12 Occlusal view of customized PEEKhealing cap.
much akin to the Buser et al.5, 6
approach to guided boneregeneration in which mini screws areused as “tent poles” to support anePTFE membrane, allowing forosseous regeneration.
By utilizing extended healing caps ofappropriate height, Salama et al.7
have developed a submerged implantprotocol designed to support the softtissues and enable an increase invertical soft tissue height during healing.They have termed this technique, whichis essentially guided tissue regenerationwithout a membrane, “Guided GingivalRegeneration.”
To incorporate this technique in theesthetic zone with a Straumann dentalimplant, 2 mm and 3.5 mm beveledhealing caps can be used (Figure 5).These healing caps are designed witha buccal bevel to reduce the volumeof the cap in the critical zone of thebuccal soft tissues and preventperforation of the mucosal flap duringhealing. This healing cap isadvantageous to use, as it covers theimplant shoulder, supports the softtissues in the approximal area, andpre-shapes a part of the transmucosal
soft tissue tunnel during the initialhealing period.8 It also enables theuse of either a submerged or semi-submerged healing pattern (Figures 6,7, 8, 9).
In esthetic situations where additionalhorizontal or vertical soft tissue supportis needed, custom healing caps canbe created with the two-piece PEEKextended healing cap (Figure 10).These healing caps can be anatomicallyshaped and inserted at the initialsurgery or following second stagemucoplasty allowing the implant tobecome transmucosal for restorativeprocedures (Figures 11 and 12).
Management of the peri-implant softtissues is a critical factor in the successof dental implant procedures. Propertreatment planning is a key factor indeciding when to use a non-submerged,semi-submerged, or fully submergedhealing approach. The opportunity toselect appropriate healing caps willassist the surgeon in providing thepatient an optimal result.
References
1. Buser D, Mericske-Stern R, Bernard JP,Behneke A, Behneke N, Hirt HP, et al. Long-term evaluation of non-submerged ITIimplants. Part 1: 8-year life table analysis ofa prospective multi-center study with 2359implants. Clin Oral Implants Res1997;8(3):161-72.
2. Buser D, von Arx T, ten Bruggenkate C,Weingart D. Basic surgical principles withITI implants. Ibid. 2000;11 Suppl 1:59-68.
3. Salama H, Salama M, Garber D, Adar P.Developing optimal peri-implant papillaewithin the esthetic zone: guided soft tissueaugmentation. J Esthet Dent 1995;7(3):125-9.
4. Corn H. Soft tissue procedures in estheticperiodontal surgery: Annual Meeting;American Academy of Periodontology: 1988.
5. Buser D, Dula K, Belser U, Hirt HP, BertholdH. Localized ridge augmentation usingguided bone regeneration. 1. Surgicalprocedure in the maxilla. Int J PeriodonticsRestorative Dent 1993;13(1):29-45.
6. Buser D, Dula K, Belser UC, Hirt HP,Berthold H. Localized ridge augmentationusing guided bone regeneration. II.Surgical procedure in the mandible. Ibid.1995;15:10-29.
7. Salama H, Salama MA, Li TF, Garber DA,Adar P. Treatment planning 2000: anesthetically oriented revision of the originalimplant protocol. J Esthet Dent1997;9(2):55-67.
8. Buser D, von Arx T. Surgical procedures inpartially edentulous patients with ITIimplants. Clin Oral Implants Res 2000;11Suppl 1:83-100.
Implant Realities8
Figure 10 Two-piece PEEK healing cap.

The Treatment Planning Implications of Implant Dentistry in the PartiallyEdentulous Patient
Paul A. Fugazzotto, DDS
Introduction
Both the predictability of osseo-integrated implant therapy and itsimpact upon the practice of clinicaldentistry are well recognized. Fromthe replacement of less predictableprocedures, through the utilization ofless invasive procedures, to theprovision of previously undreamt oftreatment options, the impact ofimplant therapy on everyday practicecontinues to evolve and increase.
It is imperative that implant therapybe viewed neither as a panacea nora replacement for proven, predictabletherapies. Implant therapy must beappropriately integrated into patienttreatment planning and execution ofcare.
Utilization of implant reconstructivetherapy does not allow the clinician toabandon the basic tenets of diagnosis,case work up, treatment planning,and meticulous performance oftherapy. The concepts and foundationsof appropriate surgical and restorativeintervention and the reality of the needto establish both microbiologic andforce equilibriums are of paramountimportance to maximize the longevityof performed care.
The purpose of this paper is tohighlight various areas in whichimplant therapy significantly impactsand many times alters our patienttreatment planning.
Comprehensive examination, caseworkup, and diagnosis
The introduction of implant therapyinto the treatment armamentarium
does not simplify diagnosis, caseworkup, or treatment planning. Byaffording newer avenues of care inaddition to traditional approaches,implant therapy places additionaldemands upon diagnosis and caseworkup in order to appropriatelyexplore all treatment plan options. Inmost instances, such a case workupincludes face bow mounted modelsand 1 or more laboratory diagnosticwax-ups to help fully identify thescope of the oral health problemspresent and to enumerate not only thetreatment options but the reasonableexpectations from each option.
The importance of joint consultationsbetween all restorative dentists,specialists, and laboratory techniciansinvolved in the treatment of the casecannot be overemphasized. It is onlythrough such sharing of knowledgeand specific viewpoints that the mostappropriate treatment plan for a givenpatient, as well as viable options, willevolve.
Replacing less predictable therapeuticoptions
The periodontally involved furcationhas long represented a significantchallenge to conscientious clinicians.A periodontally involved furcationcannot be predictably maintainedthrough professional and patient oralhygiene measures. Periodontallyinvolved multi-rooted furcated teethdemonstrate further attachment lossand are lost more frequently than theirnon-furcated counterparts. Thisunderstanding has led to a variety oftreatment approaches.
While Class I furcation involvements
are easily eliminated through the useof odontoplasty, providing the patientwith an environment more amenableto home care measures and thus moremaintainable over time, Class IIperiodontally involved furcationscannot be treated predictably in sucha manner. The resultant deep toothindentations evident after eliminationof a Class II periodontally involvedfurcation via odontoplasty poseplaque control difficulties in and ofthemselves.
These facts led to the development ofvarious root resective techniques toseparate the roots of teeth with deeplyinvolved periodontal furcations, retain1 or more of the separated roots,perform necessary endodontic therapy,and utilize the root or roots as partialsupport for fixed prosthetics. Whileroot resection and subsequentrestoration in appropriately diagnosedand executed scenarios can bepredictably maintained long term, thelevel of diagnosis and technicalexpertise required, in addition topossible post therapeutic sequellae ofroot fracture and/or carious involvement,remain daunting. In addition, thefinancial ramifications of root resectivetherapy, endodontic treatment, postand core build up, and fixed prostheticrestoration often render such atherapeutic option unrealistic for manypatients.
Guided Tissue Regenerative therapy(GTR) offers an alternative to rootresective techniques. Histologic andclinical reports have demonstrated theability to regenerate lost attachmentapparatus and supporting alveolarbone following the exclusion ofepithelial cells from a failing periodontally
Vol. II • issue 3 • 2004 9

represent a financial commitmentbeyond many patients’ means. Insuch situations, implants may beutilized to help stabilize removablepartial prostheses, improve comfortand function, and lessen forces beingapplied to abutment teeth.
In the instance of a bilateral distalextension removable partial prosthesis,placement of single implants in firstmolar positions and utilization ofoverdenture abutments in the implantsand various attachment designs in theundersurface of the prosthesis easilyaccomplishes such goals with a lesserfinancial commitment.
Implants may be employed at lesserpoints along a removable partialprosthesis to improve retention,function, and comfort and to lessenforce application to remaining abutmentteeth. For example, a patient with noteeth anterior to the bicuspids mayfind that placement of 1 - 2 implants inthe anterior segment is highlybeneficial for the aforementionedreasons. The same is true of a patientattempting to utilize a unilaterallyretained removable partial prosthesisdue to a lack of natural abutments in agiven quadrant.
In many cases, the implants andabutments may be placed and theattachments “retrofitted” to the under-surfaces of an existing removablepartial prosthesis to lessen further thefinancial impact to the patient.
Replacement of more invasivetherapies
Use of implants to replace singlemissing teeth has greatly expandedover the last decade. Once controversial,such implant application is now viewedas preferable when faced with a singlemissing tooth and intact, non-restoredteeth mesial and distal to the edentulousspace. The advent of various implantbody surfaces often allows therestoration of single implants 6 - 8weeks after insertion thus further
involved furcation area, thus allowingrepopulation of the periodontal defectwith the desired periodontal ligamentand osseous precursor cells. GTRtherapy is highly diagnostic andtechnique specific. Unfortunately, theliterature has also demonstrated theunpredictability of GTR therapy inmany periodontally involved furcationswhen utilized inappropriately.
While both resective techniques andGTR therapy offer viable means forresolution of periodontally involvedfurcations in many situations, theapplication and utilization of thesetreatment modalities must be carefullyconsidered before embarking upon afinal course of therapy. The feasibilityof the overall treatment plan, thepredictability of treatment of a giventooth and lesion through root resectiveor GTR techniques, the financialramifications of care, and the ability ofthe patient to exercise appropriatepost therapeutic plaque controlmeasures are all factors that may resultin less than ideal treatment outcomes.
The introduction of implantreconstructive therapy, with or withoutconcomitant Guided Bone Regenerativetechniques (GBR), affords the cliniciana highly predictable means by whichto reconstruct posterior sextants in theface of deeply periodontally involvedfurcations. As our understanding ofimplant surgical techniques, implantbody surfaces, and force distributionhave evolved, implant use in maxillaryand mandibular posterior regions hasdemonstrated high levels of predictabilityunder function over time. Theimportance of the advent ofregenerative therapy in the utilizationof implants in posterior areas cannotbe overemphasized. The introductionof various rough surfaced implantbodies has led to increased implant tobone surface area, a shortening of thetime necessary to achieve osseo-integration before implant loading,and increased implant survival both atthe time of implant uncovering andunder function. Appropriately
executed GBR treatment allows thepredictable rebuilding of damagedalveolar bone at the time of toothremoval, with or without concomitantimplant placement; the regeneration ofatrophic ridges post tooth extractionand resorptive healing; and theaugmentation of pneumatized sinusareas to afford bone for implantplacement in previously untenablesites.
Although similar success rates for upto 15-21 years between root resectiveand restored molars and molarposition implants have been reported,it is important to recognize 2significant caveats. The first is that theindications described for theutilization of root resective andrestorative techniques were found tobe less universal than those forimplant placement in posterior regions.The second caveat involves patientfinancial challenges. Tooth removaland replacement with individualimplants and crowns often entails lessof a financial commitment than rootresective and restorative therapy,which may mandate a full archreconstruction to afford thenecessary strength to be gainedunder function through cross archessplinting.
When faced with a scenario ofposterior edentulism, there is nodoubt that implant placement andrestoration provide a much morestable result with regard to patientcomfort and function and in terms oflessening of forces being placedupon remaining anterior teeth thanthe “more conventional” treatmentoption of a bilateral distal extensionremoval partial prosthesis.
Improving treatment outcomes of“conventional” prosthetic options
While often less financially dauntingthan root resective therapy andresultant full arch reconstruction,implant-supported fixed reconstructivetreatment modalities may still
Implant Realities10

underscoring the desirability of such a treatment approach when comparedto preparation and invasion of adjacentunaffected teeth.
When faced with deeply decayednatural teeth, tooth extraction andimplant placement, with or withoutconcomitant regenerative therapydepending upon the situation, may be preferable to crown lengtheningosseous surgery, endodontic therapy,post and core build up, and fullcoverage restoration of the tooth inquestion. Should the aforementioneddecay be interproximal, the necessarycrown lengthening osseous surgeryoften results in removal of extensiveosseous support from the adjacenttooth. If the subgingival decay is onthe buccal or interproximal aspects ofa tooth in the patient’s esthetic zone,the required crown lengtheningosseous surgery often results in anesthetically unacceptable treatmentoutcome. In such a situation, orthodonticsuper eruption of the tooth prior tocrown lengthening osseous surgerycould be considered. However, theclinician is now adding an additionaltreatment modality and expense to analready questionable situation.
Expense must be factored in to thecomparison of various treatmentmodalities. It is a reality of clinicalpractice that, while many treatmentapproaches are technically feasible,the time and expense necessitated by such therapeutic modalities maybe difficult to justify when simpler, less expensive, and as predictablealternative therapeutic options exist.
These arguments should never beconstrued as a justification for implantplacement in all situations. Often toothretention is preferable to removal andreplacement with an implant due tocertain indications such as: the lack ofneed for endodontic therapy,endodontic therapy having alreadybeen performed prior to examination;the location of the carious lesions onthe buccal or lingual aspects of the
tooth, which is easily exposed withoutjeopardizing support to adjacentteeth; the unsuitability of the patient toundergo implant therapy due tosystemic reasons, psychologicalconcerns, smoking habits, etc.; or thepatient’s stated desire to maintainnatural teeth wherever possible. Inaddition, the necessity to performextensive regenerative therapies toeffect appropriate implant placement,or the presence of various limitinganatomical structures, may indicatethat a fixed prosthesis is preferable toan implant and a single crown in thereplacement of a single missing tooth.For example, if tooth # 3 is missingand a significantly pnuematized sinusis noted in this area, resulting ininadequate bone coronal to the floorof the sinus for implant placement, a3-unit fixed splint may be preferable toperformance of a sinus augmentationprocedure, subsequent implantplacement, and eventual implantrestoration.
Conclusions
There is no doubt that the introductionof predictable implant reconstructivetherapy has significantly altered thelandscape of comprehensive patienttreatment planning. However, ratherthan being viewed as a replacementfor predictable conventional treatmentmodalities, implant therapy must beconsidered as an adjunct to ouralready existing treatmentarmamentarium.
Treatment planning decisions regardingutilization of implants or “moreconventional” therapeutic approachesmust be based upon a given patient’sneeds, desires, and clinical scenarios.Such decisions should never bemotivated by manufacturer claims, a clinician’s desire to perform “moreexciting” therapies, or questions offinancial renumeration.
Case 1
A 43-year-old male presented with fiveremaining maxillary teeth. The maxillaryarch had previously been restored witha conventional removable partialprosthesis due to financial limitations.The unfavorable force distributionunder function was resulting inincreasing mobility of the abutmentteeth. Following periodontal regenerativetherapy to rebuild alveolar bone andattachment apparatus around theremaining five teeth, Straumannimplants were placed in the maxillaryanterior region. Locator attachmentswere placed on the implants and thefemale housings for the attachmentswere retrofitted into the existingremovable partial prosthesis. Theresult was a more stable andmechanically favorable outcome witha minimum of financial commitment.
Vol. II • issue 3 • 2004 11
Figure 1 Two Straumann implants with Locatorattachments in the anterior region.
Figure 2 The attachments have beenretrofitted into the existing removableprosthesis to lessen the financial impact oftherapy. Restorative dentistry by Dr. JohnMurphy, Milton, MA.

Case 2
A 42-year-old female presented to theoffice with severe carious breakdownof teeth #’s 2, 4, and 5. Treatmentoptions included the following:
A. Removal of teeth #’s 2, 4, and 5,and fabrication of a unilateralremovable partial prosthesis. Suchan approach was unacceptable interms of comfort, function, andlong term stability.
B. Fabrication of a fixed splint onteeth #’s 2, x, 4, and 5: The longterm prognosis of such aprosthesis was highly questionabledue to the compromised nature ofthe abutment.
C. A conventional fixed splint on teeth#’s 2, x, 4, 5, 6: While the additionof tooth #6 would add support tothe prosthesis, it would entailinvolvement of an unaffected tooth.In addition, tooth #2 would still beill suited to serve as a terminalabutment for the fixed prosthesis.
Implant Realities12
Figure 6 Tooth #3 is fractured. Note theminimal amount of bone coronal to thefloor of the sinus.
Figure 7 Two Straumann implants wereplaced at the time of tooth extraction andaugmentation, and subsequently restored.This radiograph demonstrates stability after3 yeas in function. Restorative dentistry byDr. Richard Baker, Braintree, MA.
Figure 3 Teeth #’s 2, 4, and 5 are severelydecayed.
Figure 4 Three Straumann implants (a WideNeck, a Tapered Effect, and a Regular Neck)have been placed at the time of toothremoval, and subsequently restored.
Figure 5 A clinical view of the final restorations.Restorative dentistry by Dr. Thomas Analletto,Needham, MA.
Case 3
A 77-year-old male presentedwith a hopeless tooth #3. Ratherthan consider either edentulismin this area or utilization of adistal extension removable partialprosthesis, tooth #3 wasextracted and augmentationtherapy was performed at thetime of tooth removal.Subsequent to maturation of theregenerating hard tissues, two4.1 mm wide x 9 mm longStraumann implants were placedin the positions of teeth #’s 2 and3, and restored with singlecrowns.
D. Removal of teeth #’s 2, 4, and 5,and placement of implants in thepositions of #’s 3, 4, and 5 at thetime of tooth removal: This optionwas chosen. No implant wasplaced in the position of tooth # 2as tooth # 31 was absent. A WideNeck Straumann implant wasplaced in the position of tooth #3; a4.1 Tapered Effect Straumannimplant was placed in the positionof tooth #4; and a Regular Neck 4.1 mm Straumann implant wasplaced in the position of tooth #5.The implants were restored withsolid abutments and single crowns.
Vol. II • issue 3 • 2004 13
Case 4
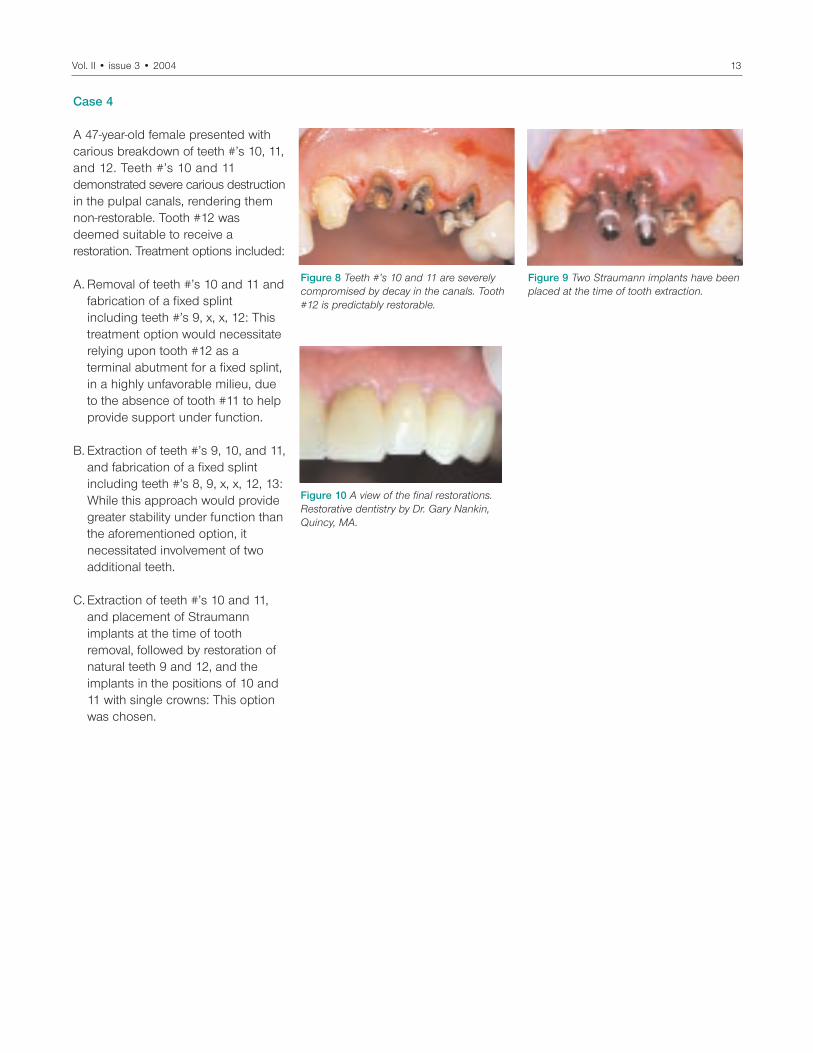
A 47-year-old female presented withcarious breakdown of teeth #’s 10, 11,and 12. Teeth #’s 10 and 11demonstrated severe carious destructionin the pulpal canals, rendering themnon-restorable. Tooth #12 wasdeemed suitable to receive arestoration. Treatment options included:
A. Removal of teeth #’s 10 and 11 andfabrication of a fixed splintincluding teeth #’s 9, x, x, 12: Thistreatment option would necessitaterelying upon tooth #12 as aterminal abutment for a fixed splint,in a highly unfavorable milieu, dueto the absence of tooth #11 to helpprovide support under function.
B. Extraction of teeth #’s 9, 10, and 11,and fabrication of a fixed splintincluding teeth #’s 8, 9, x, x, 12, 13:While this approach would providegreater stability under function thanthe aforementioned option, itnecessitated involvement of twoadditional teeth.
C. Extraction of teeth #’s 10 and 11,and placement of Straumannimplants at the time of toothremoval, followed by restoration ofnatural teeth 9 and 12, and theimplants in the positions of 10 and11 with single crowns: This optionwas chosen.
Figure 8 Teeth #’s 10 and 11 are severelycompromised by decay in the canals. Tooth#12 is predictably restorable.
Figure 9 Two Straumann implants have beenplaced at the time of tooth extraction.
Figure 10 A view of the final restorations.Restorative dentistry by Dr. Gary Nankin,Quincy, MA.

Treatment Options in Reconstruction of the Posterior DentitionPart 2: Planning and Treatment Considerations for Implant-AssistedRestorations in the Posterior Maxilla: Esthetic
Dean Morton, BDS, MS; Will Martin, DMD, MS; James Ruskin, DMD, MD; Todd Fridrich, CDT
Although restoration of the posteriorregions of the mouth often presentsunique difficulties for the treatmentteam, implant survival remains high.Challenges encountered whentreating the posterior maxilla arerelated to the anatomic characteristicsof the area. Reduced bone qualityand quantity and the consequent softtissue deficiency often lead to theneed for enhancement procedures, toprovide adequate implant support,and to establish an environmentcapable of sustaining an esthetic andfunctional restoration. Implants maybe positioned immediately on extractionof the teeth, thus limiting or preventingbone and soft tissue loss. The demandsof the patient, the number andposition of missing teeth, and thefunctional and occlusal requirementsof the restorations are also influential
in the formulation of the final treatmentplan and the achievement of anesthetic outcome.
Magne and Belser (2002) have listedobjective and subjective criteria to beconsidered when assessing a patientwith esthetic demands. Several of thecriteria address the supporting softtissues (gingival health, inter-dentalclosure, zenith of the gingival contour,and balance of the gingival levels),while others directly relate to the teeth(axis, level of inter-dental contact,relative tooth dimensions, tooth formand character, surface texture, color,incisal edge configuration, lip line, andsmile symmetry). Treatment planningfor implant-based therapy must becognizant of these factors, and thefinal outcome must be assessed inrelation to them.
Case Report
The patient presented with chiefconcerns related to esthetics (Figure 1)and functional inadequacy (Figure 2).Intraoral evaluation revealedapproximately 6 mm of inter-occlusalspace at rest (Figure 3). Lateral viewsillustrated the disrupted incisal andocclusal planes, and retaineddeciduous teeth. Inter-occlusal spaceis demonstrated in between theposterior teeth with the patient at rest(Figures 4 and 5). Radiographicanalysis confirmed the absence ofmost permanent teeth and detailed noevidence of disease or pathology(Figure 6).
The esthetic evaluation revealed amultitude of concerns. Although thegingival tissues were healthy and of
Figure 1 A pre-operative smile view. Figure 2 A pre-operative anterior view ofmaximum intercuspation.
Figure 3 A pre-operative anterior view at restposition.
Figure 4 A pre-operative right view at restposition.
Figure 5 A pre-operative left view at restposition.
Figure 6 A pre-operative panoramic radiograph.
Implant Realities14

appropriate color, the gingivalarchitecture was problematic as aresult of missing and mal-positionedteeth. The planned restorations wouldneed to establish appropriate toothproportion and symmetry, and developharmony with the supporting softtissues if an improvement to thedeficient smile was to be realized.
After considering several treatmentoptions, the patient chose to pursueimplant-based rehabilitation. Thetreatment plan included several stages:
1. Extraction of the deciduous teethand immediate implant placement.
2. Immediate loading of the implantswith two short span provisionalfixed partial dentures in the maxillaand a complete arch provisionalrestoration in the mandible.
3. Subsequent to implant healing,definitive restoration of the maxillawith metal-ceramic fixed prostheses,and restoration of the mandible witha fixed-detachable (hybrid)prosthesis.
The deciduous teeth were removedwith a minimum of trauma to the boneand surrounding soft tissues (Figure 7).Surgical templates, fabricated fromthe diagnostic wax-up, communicatedthe desired three-dimensional positionof the implants (Figure 8) to the surgeon.Tapered Effect implants werepositioned in the maxilla to maximizeimplant stability, and wide bodyimplants were utilized in the mandibleto maximize both implant stability andsupport for the future prosthesis(Figure 9). Polyvinyl siloxaneimpressions were made of both archesto relate the implants, and modifiedbaseplates and wax rims used to obtaininter-occlusal articulation records.
The casts were articulated, andprovisional restorations were laboratoryfabricated and delivered within 48hours of implant placement. Themaxillary provisional restorations werecement-retained on angled synOcta®
abutments, chosen to idealize thepath of placement. The mandibularprovisional fixed-detachable restorationwas screw-retained by synOcta® (forbridge) titanium abutments (Figure 10).
The provisional restorations remainedin place for eight weeks while theimplants healed (Figure 11). Thedefinitive restoration of the mandibulararch was undertaken first, to provide astable arch against which the maxillaryrestorations could be fabricated.Further, the bone in the maxilla wasconsidered less ideal, and as suchwas afforded additional healing time.
Subsequent to removal of theprovisional restoration the tissueswere evaluated (Figure 12) and animplant-level polyvinyl siloxaneimpression was made (Figure 13). Thedefinitive mandibular restoration wasfabricated on synOcta® 2.5 abutments,which were positioned and torqued to35 Ncm (Figure 14) prior to delivery ofthe prosthesis. The mandibular fixedprosthesis was evaluated for fit,adaptation to the soft tissues, andocclusion. Subsequent to assessmentof the patient’s satisfaction, therestoration was torqued to place withSCS occlusal screws (Figure 15).The restoration of the maxillary archbegan with a polyvinyl siloxaneimpression of the implants and the
Figure 7 Minimally traumatic extractionshave been carried out in the maxilla.
Figure 8 The surgical template is in place. Figure 9 A panoramic radiograph postplacement.
Figure 10 A view of the mandibularprovisional prosthesis and titanium temporarysynOcta® abutments for bridge.
Figure 11 A view of the provisional restorations8 weeks post implant placement.
Figure 12 A view of the mandibular implants8 weeks post implant placement.
Vol. II • issue 3 • 2004 15

soft tissue contours (Figure 16). Shadecommunication was improved throughclinical photographs that identified theappropriate base shade (Figure 17)and displayed the surface texture ofadjacent teeth (Figure 18). The mastercast incorporated implant analogs(Figure 19) and was articulated againsta cast of the opposing mandibularrestoration (Figure 20). A cast of themaxillary provisional restorations wascross-articulated against the mandibularcast to illustrate the appropriate toothpositions and lengths to the dentaltechnician (Figure 21).
Using matrices fabricated from thecast of the provisional restorations,two-piece cementable abutments
were chosen, positioned, and adjustedto facilitate fabrication of the metal-ceramic restorations (Figures 22-24).The restorations were checked orallyfor adequacy of fit, occlusion, andesthetics. Subsequent to confirmationof the patient’s satisfaction with theesthetic result, the restorations weredefinitively cemented (Figures 25 and26).
The two-week follow-up appointmentconfirmed soft tissue healing with theimproved contour and adaptation ofthe definitive restorations (Figure 27).Lateral views confirmed the estheticresults which were possible (Figures28 and 29). Note the pink ceramicpapilla developed between teeth 5
and 6. The final radiographic resultconfirmed implant and tooth health(Figure 30).
Figure 13 Final impression and tissueanalog - mandible.
Figure 14 Positioning and torquing synOcta®
2.5 abutments.Figure 15 Mandibular definitive prosthesis.
Figure 16 Final impression and tissueanalog - maxilla.
Figure 17 Base shade communication isperformed.
Figure 18 Surface texture and shadecommunication is carried out.
Figure 19 A view of the maxillary master cast. Figure 20 A view of the articulated maxillarymaster cast.
Figure 21 A view of the cross articulatedcast of provisional restorations.
Implant Realities16

Vol. II • issue 3 • 2004 17
Figure 22 A lateral view of the adjustedabutments.
Figure 23 A palatal view of the adjustedabutments.
Figure 24 A buccal view of the adjustedabutments.
Figure 25 An occlusal view of the definitiverestorations on the day of placement.
Figure 26 An anterior view of the definitiverestorations on the day of placement.
Figure 27 An anterior view of the definitiverestorations two weeks post placement.
Figure 28 A left lateral view of the definitiverestorations two weeks post placement.
Figure 29 A right lateral view of the definitiverestorations two weeks post placement.
Figure 30 A panoramic radiograph of thecompleted restorations.

An Alternative Abutment for Deep Implant Placements in the Esthetic Zone Utilizing the synOcta® Meso Abutment
Frank L. Higginbottom, DDS
Today the most frequently employedrestorative option for the partiallyedentulous patient when using theStraumann® Dental Implant System isthe solid abutment supporting acemented crown. This approach maybecome problematic when the implantmust be placed more deeply in theanterior region. Such placement oftenresults in an interproximal shoulderdepth of 5-7 mm or more, dependingupon the severity of the gingival scallop.In these instances, a cement-retainedrestoration with a deep interproximalmargin would result in a marginalplacement that presents a problem forcement removal by the dentist andoral hygiene measures for the patient.
For these reasons it is advisable to placea screw-retained crown in cases withdeeper implant placements. This maybe achieved with a single crownretained by an occlusal screw.However, many times the anatomy ofthe anterior maxilla will not allow theuse of this simple solution, due to ascrew access position that is notlingual to the lingual incisal edge of an upper incisor.
One option is Straumann’s synOcta®
gold abutment, a cast-to abutmentdesigned for the fabrication of customrestorations where the laboratorytechnician waxes the abutment anddirectly casts onto it.
Another option is the use of asynOcta® meso abutment, which is aone-piece titanium component that fitsdirectly into the implant (Figures 1 and2) and retained to the implant with abasal screw. The meso abutment fitsinto the internal octagon connectionof the implant and contacts theimplant shoulder. The abutment screw
is torqued to 35 Ncm. The synOcta®
meso abutment allows for angulationcorrection and marginal placementcontrol with one component.
The meso abutment is available forboth the 4.8 mm and the 6.5 mmimplant shoulders. A synOcta® implantlevel impression is first taken with eitheran open tray synOcta® impressioncoping or the traditional impressioncap and synOcta® positioning cylinder.When the implant is placed subgingival,it is recommended that an open trayimpression coping is used to helpensure complete seating onto theimplant shoulder. An impression ismade and a provisional restoration isfabricated. The impression is forwardedto the laboratory technician for thefabrication of the final restoration. Thetechnician fabricates a soft tissue castand shapes the peri-implant space.
An alternative approach is to completethe model work in the dental office andhave the patient return when the peri-implant tissues have been shaped by aprovisional restoration. The provisionalrestoration is then used to fabricate asoft tissue cast union exactly resemblingthe contours created in the mouth. Thetechnician selects the appropriatesynOcta® meso abutment and shapes
it to create a uniform cement line that is 2 mm below the gingival margin. Itis crucial that the tissue model beaccurate. The soft tissue contoursshould be allowed to stabilize for onemonth prior to fabrication of the softtissue cast.
After laboratory fabrication of the finalrestoration, the synOcta® mesoabutment and finished cementablecrown are returned to the dentist forplacement. The provisional restorationand abutment are removed and thesynOcta® meso abutment is seated anddouble torqued to 35 Ncm. The finalcrown is fitted and the occlusion andcontacts adjusted. When the crown isacceptable, the crown is seated withappropriate cement.
Case 1
A 51-year-old male patient presentedwith a non-restorable maxillary rightcentral incisor. The tooth was removedand an implant placed in a mature siteafter 45 days of healing. Proper implantpositioning dictated a deep shoulderplacement. A solid abutment was notconsidered appropriate due to thedepth of placement. A synOcta® meso
Figure 1 Illustrations of the synOcta® mesoabutments in the 4.8 mm and the 6.5 mmshoulder configurations.
Figure 2 The synOcta® meso abutment is aone-piece abutment with a basal screw. Theabutment screw is titanium alloy with nobiumand aluminum. The screw has a tapered broadneck, producing a good frictional contact withthe mating surface of the abutment.
Implant Realities18

Vol. II • issue 3 • 2004 19
Figure 4 The healing abutment is removed,note the immature peri-implant space.
Figure 5 A synOcta® screw-retainedimpression coping is seated.
Figure 6 A view of the working cast with thesoft tissue analog in place.
Figure 7 A view of a synOcta® meso abutmentfor the standard shoulder prior to itscustomization to adjust the marginal depth of the cement line and angulation.
Figure 8 Various SHP burrs and discs areused to machine the synOcta® meso abutment.
Figure 10 A facial view of the shapedsynOcta® meso abutment.
Figure 11 An occlusal view of the shapedsynOcta® meso abutment.
Figure 12 A view of the finished synOcta®
meso abutment.
Figure 9 The synOcta® meso abutment isseated on the master cast.
Figure 13 The finalized custom synOcta®
meso abutment and a single PFM crown forcementation has been fabricated.
Figure 16 A view of the peri-implant spacecreated by the emergence profile provisionalrestoration.
Figure 14 The patient’s provisional restorationis used to shape the gingival tissues.
Figure 15 A solid abutment is used as theinterim abutment for the provisional restoration.
abutment was selected to changeangulation and raise the cement line toa manageable level for a cementedcrown (Figures 3-19).
Figure 3 A transmucosal healing abutment isin place at twelve weeks post surgery.

Figure 17 The synOcta® meso abutment isseated and double torqued to 35 Ncm.
Figure 18 The final PFM crown is seated,and cemented with the cement of theclinician’s choice.
Figure 19 A final radiograph of the restoredimplant.
Figure 20 The patient presents with afractured maxillary right canine.
Figure 21 The radiograph demonstratesexternal root resorption.
Figure 22 A view of the customized synOcta®
meso abutment.Figure 23 Views of the porcelain fused tohigh noble metal and shaped synOcta®
meso abutment.
Figure 24 A view of the provisionalrestoration shaped peri-implant space, with the provisional restoration removed.
Figure 25 The synOcta® meso abutment is seated and torqued to 35 Ncm.
Figure 26 A view of the final cementedporcelain fused to metal crown.
Figure 27 A radiograph of the restoredimplant.
Implant Realities20
Case 2
A 55-year-old male patient presentedwith a maxillary right caninedemonstrating external resorption,following endodontic treatment andsubsequent fracture. This situationnecessitates deep implant placement,resulting in a deep interproximalmargin placement. The restorativesolution involves correcting themarginal placement for a cementedcrown with the use of a synOcta®
meso abutment (Figures 20-27).
Case 3
A 63-year-old female patientpresented with a fixed partial denture,and non-restorable anterior abutments.Implants were placed in the canineand premolar positions. The fact thatthe implant in the canine position wasan immediate placement necessitatedit being placed more deeply, andresulted in a marginal placement thatwas not appropriate for a traditionalcemented margin. A synOcta® mesoabutment was used to facilitate theplacement of a cemented porcelainfused to metal crown (Figures 28-36).
Case 4
A 70-year-old patient presented at amaintenance visit with a failing postand core. It was not deemed advisableto fabricate a fixed bridge from the pre-molar implant to the lateral incisor.Immediate implant placement and loadwas accomplished using a Wide Neckimplant. A cemented crown was utilizedwith a synOcta® meso abutment as theretentive element (Figures 37-42).

Vol. II • issue 3 • 2004 21
Figure 30 An occlusal view of the completedsynOcta® meso abutment.
Figure 31 Comparison of the pre-machinedsynOcta® meso abutment and the completedabutment is instructive.
Figure 32 A view of the completed synOcta®
meso abutment and porcelain fused to metalcrown.
Figure 33 An occlusal view of the peri-implantspace shaped by the provisional restoration.
Figure 34 The synOcta® meso abutment isseated and abutment screw is double torquedto 35 Ncm.
Figure 35 The final porcelain fused to metalcrown is cemented to place.
Figure 36 A radiograph of the restoredimplant.
Figure 37 A radiographic view of the non-restorable maxillary right canine.
Figure 38 A view of the healed and shapedperi-implant space after provisionalization.
Figure 39 Views of the final shaped abutmentand porcelain fused to metal crown.
Figure 40 The synOcta® meso abutment isseated and torqued twice to 35 Ncm.
Figure 41 The final cemented restoration seated. Figure 42 A radiograph of the final results.
Figure 29 A view of the master cast withsynOcta® meso abutment placed prior to themachining process.
Figure 28 The maxillary left canine isunrestorable, and the lateral incisor isunfavorable as an abutment for a fixed bridge.

Immediate Loading of the Full-Arch Maxilla with Cemented ProvisionalRestorations Using Angled synOcta® Abutments
Jeffrey Ganeles, DMD, FACD; Frederic J. Norkin, DMD; Julio Sekler, DMD, MMSc
The immediate loading and restorationof dental implants has been shown tobe successful in well over 100 scientificpapers during the last decade.Summarizing these papers anddrawing conclusions from them wasthe mission of one of the sections ofthe ITI Consensus Conference held inGstaad, Switzerland in August 2003.The results of this meeting will soon bepublished as a special supplement tothe International Journal of Oral andMaxillofacial Implants. A significantnumber of case series and reportsexist for different clinical case types.However, an area of study with relativelylittle documentation is immediateloading of the full-arch maxilla.
Traditionally, full-arch maxillary caseshave been perceived as being moredifficult or presenting more obstaclesthan full-arch mandibular cases.Impediments to successful treatmentinclude qualitative and quantitativedifficulties in maxillary bone ascompared to mandibular bone.Another factor is that the shape of theedentulous maxilla often precludesparallel placement of dental implants,while mandibles often lend themselvesto straight alignment.
In an article published in 2001,Ganeles et al.1 identified several differentoptions for creating immediately loadedprovisional restorations. In that articleand in subsequent practice, thepreferred technique for full-archprovisional restorations was theLaboratory Processed, Cemented(LPC) version. Advantages of thistechnique include the ability toprovide an accurate, passively fitting,easily adjustable, and estheticprovisional restoration given the tighttime constraints of immediate loading.One of the requirements for using this
technique is aligning the implants sothat there is a path of insertion on theStraumann® solid abutments. Theexternal taper of these abutments is6˚, so that for a restoration to seatproperly, implants must all be withinapproximately 16˚ of parallel. Thisrequirement can be modified byreducing the precision of fit of arestoration, creating more spaceinternally around an abutment that issignificantly out of alignment. Creatinga looser fit increases the tolerance toseat a restoration significantly butreduces the retention and stability,both key elements in successfulimmediate loading.
In maxillary immediate loading cases,implants are selected and placed inorder to maximize implant surfacearea and engage optimal bonedensity. Frequently, 3-dimensionalradiographic imaging, planning, and(eventually) image-guided surgery areused in order to place the implants.Most often, the apices of the implantsare directed palatally towards thejunction of the palatal vault, maxillarysinus, and floor of the nose in order togain maximum stability. The net effectof this positioning is that implants arefrequently more than 30-40˚ out ofalignment, beyond the ability toreasonably create a path of insertionon solid abutments with rigidprovisional restorations. To solve thisdilemma, alternatives include use ofscrew retention, which also haslimited alignment correction ability,use of custom abutments, or use ofsynOcta® angled abutments. Customabutments or synOcta® Mesoabutments are impractical in animmediate loading context, as theyrequire significant laboratory time tofabricate or modify, interfering with theobjective of delivering a full-arch
provisional restoration in a timelymanner.
The following case report illustratesthe techniques necessary to satisfythe conflicting objectives of providinga rigid, accurate, esthetic, laboratory-processed, cement-retained,immediately loaded provisionalrestoration on implants thatsignificantly diverge.
Case 1
AC is a 45-year-old, healthy malesuffering from advanced periodontitisin the maxillary arch, caries, andposterior bite collapse, including lossof occlusal vertical dimension andposterior support. His desire was toreplace his failing dentition with a newmaxillary fixed prosthesis supportedby dental implants. The remainingmaxillary teeth were deemed to behopeless or not valuable to a newmaxillary restoration. Missingmandibular posterior teeth were alsoto be replaced with implant-supportedrestorations. Caries in remainingmandibular teeth were to be treatedwith appropriate operative andprosthodontic procedures. Othertreatment goals included avoiding aremovable prosthesis duringtreatment and minimizing the amountof treatment time and dentalappointments due to severe anxiety.
After clinical and radiographicevaluation (Figures 1 and 2), it wasdetermined that he had adequatebone available anterior to the maxillarymolars to permit immediate loading ofan adequate number of implants tosupport a full arch provisionalrestoration. Further, it was determinedthat with appropriate modification ofhis vertical dimension, a therapeutic
Implant Realities22

Vol. II • issue 3 • 2004 23
occlusion would be obtained againstthe existing mandibular teeth.
Pre-operative prosthetic preparationincluded analysis of mounted diagnosticmodels and fabrication of a clear acrylicocclusal registration device that wasverified and modified intraorally withadditional acrylic (Figure 3). The devicewas constructed to have positive tissuecontact on the tuberosities and palateat the desired new vertical dimension.It was also constructed to have positiveocclusal contact with the opposingdentition at the correct verticaldimension. It was further modified toserve as a rudimentary surgical guideto assist in implant positioning andorientation during surgery.
At the time of surgery, vertical
dimension of occlusion was recordedextraorally by marking and measuringthe distance between the nose andchin with the registration device inplace (Figure 4). Appropriate surgicaltechniques were used to extract teethand place 8 Straumann implants,leaving the central incisors in place(Figure 5). Standard, threaded implantswere selected to maximize the lengthand width of the implants seated inavailable bone. No attempt was madeto place the implants parallel. Instead,implants were positioned with the goalof placing them with optimal stability,often resulting in palatal inclination ofthe apices of the implants. Insertiontorque was measured for all implantsusing the ratchet and torque controldevice during implant insertion. Theobjective was to obtain a minimum of35 Ncm torque resistance for allimplants to be immediately loaded.
The distal-most implants were placedin conjunction with osteotome sinusaugmentation procedures usingautogenous bone recovered from theosteotomy sites. These implants were
sealed with appropriate closure screwsand allowed to heal without prostheticloading.
Prior to suturing, impression copingsand synOcta® positioning cylinderswere snapped onto the implants to beloaded (Figure 6). A polyvinylsiloxane(PVS) impression was taken, capturingthe impression assemblies. synOcta®
angled abutments were tried in themouth with the objective of creating aparallel path of insertion between thedivergent implants. Abutments can beselected either by using the Straumann®
prosthetic planning kit with plasticplanning parts or by sequentiallytrying in actual abutments in themouth. In this case, “A” and “B” typesof angled abutments as well as straightabutments were sequentially tried untila reasonably parallel insertion pathwas created (Figure 7). Once selectedand hand-tightened in the implants,the abutments were notched at theirfacial-occlusal surfaces for futurerepositioning in the analog models(Figure 8).
Figure 1 Radiograph shows adequate boneavailable anterior to the maxillary molars.
Figure 3 A clear acrylic occlusal registrationdevice is fabricated then verified andmodified intraorally with additional acrylic.
Figure 4 Vertical dimension of occlusion isrecorded extraorally with the registrationdevice in place.
Figure 6 Prior to suturing, impressioncopings and synOcta® positioning cylindersare snapped onto the implants to be loaded.
Figure 5 Teeth are extracted, leaving centralincisors in place, and 8 Straumann implantsare placed.
Figure 2 Pre-operative facial view showinganterior flaring, loss of occlusal verticaldimension, and bone loss.
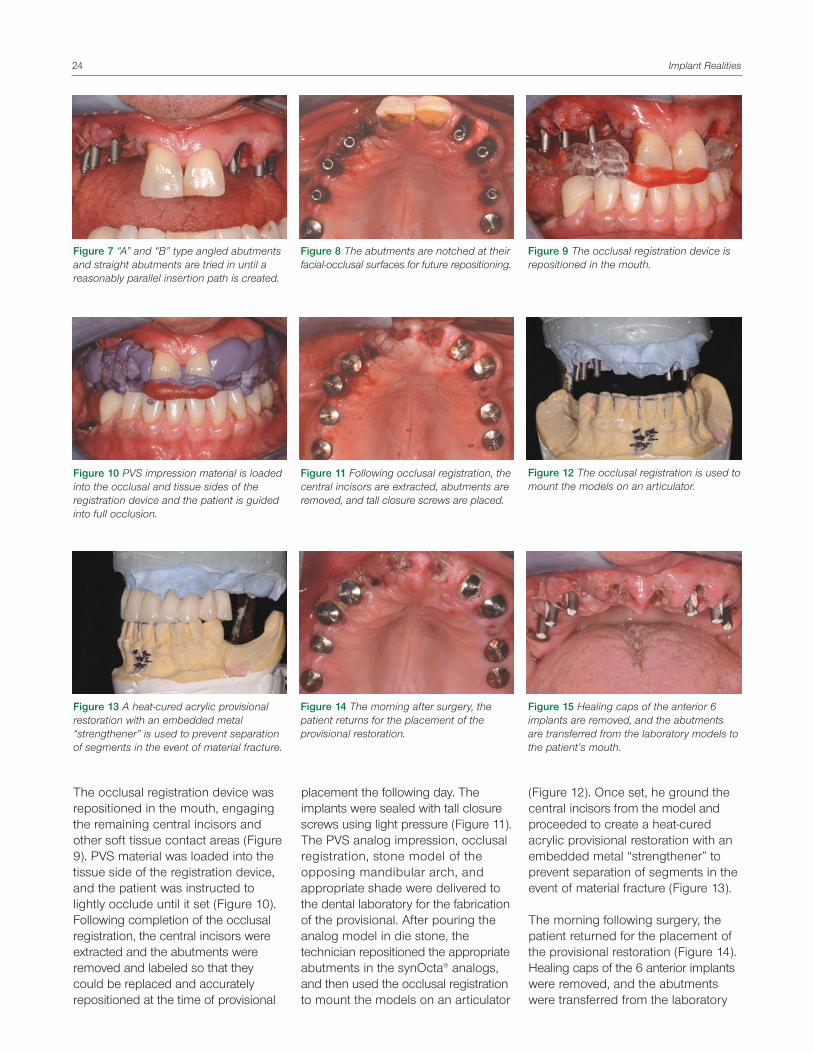
The occlusal registration device wasrepositioned in the mouth, engagingthe remaining central incisors andother soft tissue contact areas (Figure9). PVS material was loaded into thetissue side of the registration device,and the patient was instructed tolightly occlude until it set (Figure 10).Following completion of the occlusalregistration, the central incisors wereextracted and the abutments wereremoved and labeled so that theycould be replaced and accuratelyrepositioned at the time of provisional
placement the following day. Theimplants were sealed with tall closurescrews using light pressure (Figure 11). The PVS analog impression, occlusalregistration, stone model of theopposing mandibular arch, andappropriate shade were delivered tothe dental laboratory for the fabricationof the provisional. After pouring theanalog model in die stone, thetechnician repositioned the appropriateabutments in the synOcta® analogs,and then used the occlusal registrationto mount the models on an articulator
(Figure 12). Once set, he ground thecentral incisors from the model andproceeded to create a heat-curedacrylic provisional restoration with anembedded metal “strengthener” toprevent separation of segments in theevent of material fracture (Figure 13).
The morning following surgery, thepatient returned for the placement ofthe provisional restoration (Figure 14).Healing caps of the 6 anterior implantswere removed, and the abutmentswere transferred from the laboratory
Figure 7 “A” and “B” type angled abutmentsand straight abutments are tried in until areasonably parallel insertion path is created.
Figure 8 The abutments are notched at theirfacial-occlusal surfaces for future repositioning.
Figure 9 The occlusal registration device isrepositioned in the mouth.
Figure 10 PVS impression material is loadedinto the occlusal and tissue sides of theregistration device and the patient is guidedinto full occlusion.
Figure 13 A heat-cured acrylic provisionalrestoration with an embedded metal“strengthener” is used to prevent separationof segments in the event of material fracture.
Figure 15 Healing caps of the anterior 6implants are removed, and the abutmentsare transferred from the laboratory models tothe patient’s mouth.
Figure 14 The morning after surgery, thepatient returns for the placement of theprovisional restoration.
Figure 11 Following occlusal registration, thecentral incisors are extracted, abutments areremoved, and tall closure screws are placed.
Figure 12 The occlusal registration is used tomount the models on an articulator.
Implant Realities24
Vol. II • issue 3 • 2004 25
models to the patient’s mouth andtightened with strong finger pressure(Figure 15). All access holes in theabutments were sealed with a cottonpellet and sealer. The provisionalrestoration was seated in the mouthwithout anesthetic and adjusted toensure a passive and accurate fit.Occlusion was carefully adjusted toensure even contact on all implants incentric closure and to minimizevertical rise in lateral movements.Posterior working and non-workingcontacts were removed, and thecantilever pontics were completelyrelieved from contact.
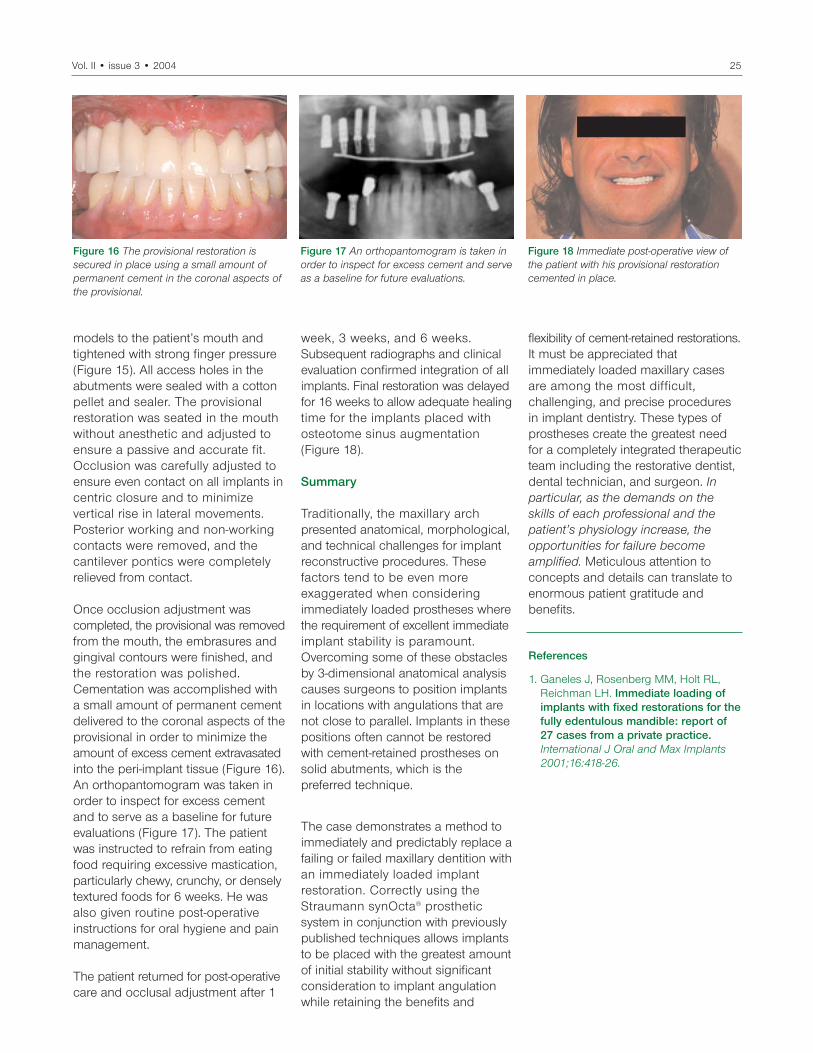
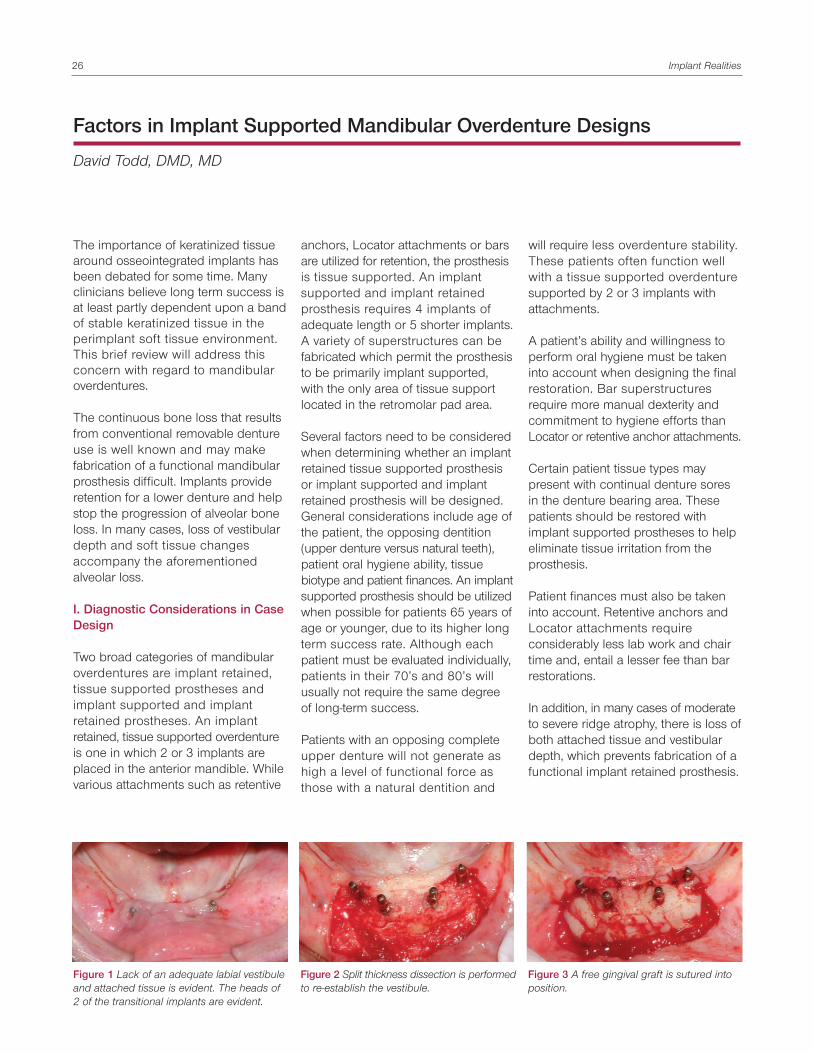
Once occlusion adjustment wascompleted, the provisional was removedfrom the mouth, the embrasures andgingival contours were finished, andthe restoration was polished.Cementation was accomplished witha small amount of permanent cementdelivered to the coronal aspects of theprovisional in order to minimize theamount of excess cement extravasatedinto the peri-implant tissue (Figure 16).An orthopantomogram was taken inorder to inspect for excess cementand to serve as a baseline for futureevaluations (Figure 17). The patientwas instructed to refrain from eatingfood requiring excessive mastication,particularly chewy, crunchy, or denselytextured foods for 6 weeks. He wasalso given routine post-operativeinstructions for oral hygiene and painmanagement.
The patient returned for post-operativecare and occlusal adjustment after 1
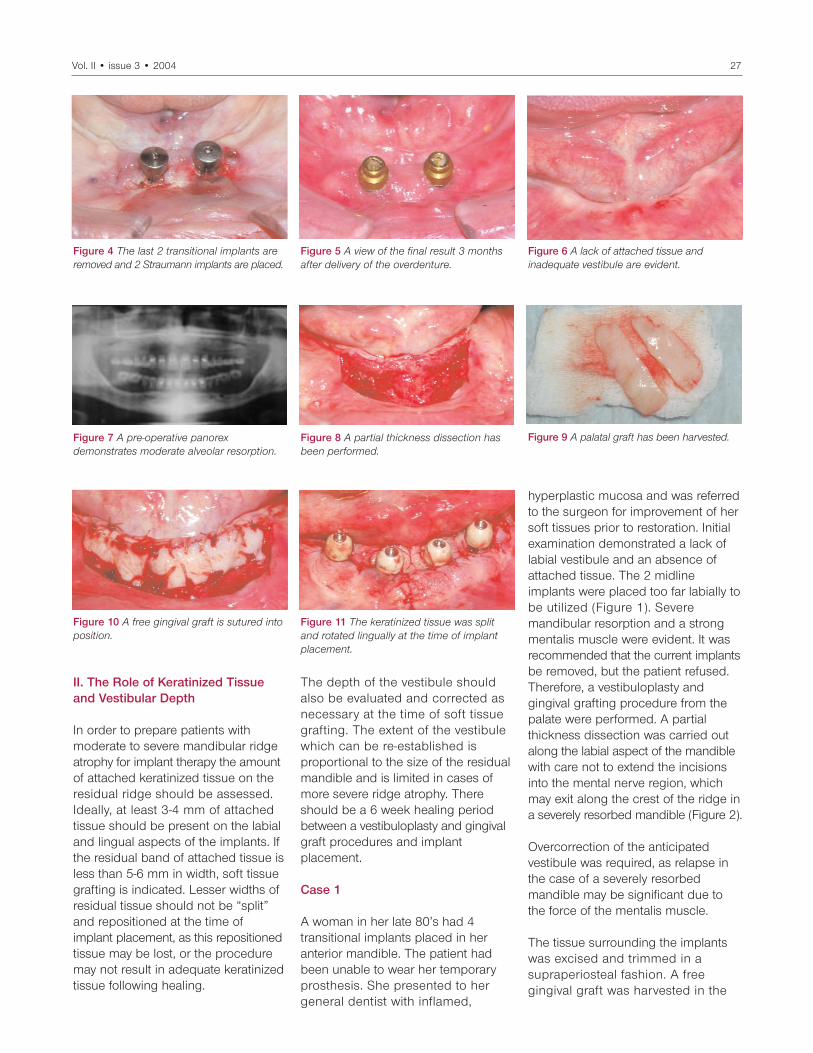
week, 3 weeks, and 6 weeks.Subsequent radiographs and clinicalevaluation confirmed integration of allimplants. Final restoration was delayedfor 16 weeks to allow adequate healingtime for the implants placed withosteotome sinus augmentation (Figure 18).
Summary
Traditionally, the maxillary archpresented anatomical, morphological,and technical challenges for implantreconstructive procedures. Thesefactors tend to be even moreexaggerated when consideringimmediately loaded prostheses wherethe requirement of excellent immediateimplant stability is paramount.Overcoming some of these obstaclesby 3-dimensional anatomical analysiscauses surgeons to position implantsin locations with angulations that arenot close to parallel. Implants in thesepositions often cannot be restoredwith cement-retained prostheses onsolid abutments, which is thepreferred technique.
The case demonstrates a method toimmediately and predictably replace afailing or failed maxillary dentition withan immediately loaded implantrestoration. Correctly using theStraumann synOcta® prostheticsystem in conjunction with previouslypublished techniques allows implantsto be placed with the greatest amountof initial stability without significantconsideration to implant angulationwhile retaining the benefits and
flexibility of cement-retained restorations. It must be appreciated thatimmediately loaded maxillary casesare among the most difficult,challenging, and precise proceduresin implant dentistry. These types ofprostheses create the greatest needfor a completely integrated therapeuticteam including the restorative dentist,dental technician, and surgeon. Inparticular, as the demands on theskills of each professional and thepatient’s physiology increase, theopportunities for failure becomeamplified. Meticulous attention toconcepts and details can translate toenormous patient gratitude andbenefits.
References
1. Ganeles J, Rosenberg MM, Holt RL, Reichman LH. Immediate loading of implants with fixed restorations for thefully edentulous mandible: report of 27 cases from a private practice.International J Oral and Max Implants 2001;16:418-26.
Figure 16 The provisional restoration issecured in place using a small amount ofpermanent cement in the coronal aspects ofthe provisional.
Figure 18 Immediate post-operative view ofthe patient with his provisional restorationcemented in place.
Figure 17 An orthopantomogram is taken inorder to inspect for excess cement and serveas a baseline for future evaluations.
will require less overdenture stability.These patients often function wellwith a tissue supported overdenturesupported by 2 or 3 implants withattachments.
A patient’s ability and willingness toperform oral hygiene must be takeninto account when designing the finalrestoration. Bar superstructuresrequire more manual dexterity andcommitment to hygiene efforts thanLocator or retentive anchor attachments.
Certain patient tissue types maypresent with continual denture soresin the denture bearing area. Thesepatients should be restored withimplant supported prostheses to helpeliminate tissue irritation from theprosthesis.
Patient finances must also be takeninto account. Retentive anchors andLocator attachments requireconsiderably less lab work and chairtime and, entail a lesser fee than barrestorations.
In addition, in many cases of moderateto severe ridge atrophy, there is loss ofboth attached tissue and vestibulardepth, which prevents fabrication of afunctional implant retained prosthesis.
The importance of keratinized tissuearound osseointegrated implants hasbeen debated for some time. Manyclinicians believe long term success isat least partly dependent upon a bandof stable keratinized tissue in theperimplant soft tissue environment.This brief review will address thisconcern with regard to mandibularoverdentures.
The continuous bone loss that resultsfrom conventional removable dentureuse is well known and may makefabrication of a functional mandibularprosthesis difficult. Implants provideretention for a lower denture and helpstop the progression of alveolar boneloss. In many cases, loss of vestibulardepth and soft tissue changesaccompany the aforementionedalveolar loss.
I. Diagnostic Considerations in CaseDesign
Two broad categories of mandibularoverdentures are implant retained,tissue supported prostheses andimplant supported and implantretained prostheses. An implantretained, tissue supported overdentureis one in which 2 or 3 implants areplaced in the anterior mandible. Whilevarious attachments such as retentive
anchors, Locator attachments or barsare utilized for retention, the prosthesisis tissue supported. An implantsupported and implant retainedprosthesis requires 4 implants ofadequate length or 5 shorter implants.A variety of superstructures can befabricated which permit the prosthesisto be primarily implant supported,with the only area of tissue supportlocated in the retromolar pad area.
Several factors need to be consideredwhen determining whether an implantretained tissue supported prosthesisor implant supported and implantretained prosthesis will be designed.General considerations include age ofthe patient, the opposing dentition(upper denture versus natural teeth),patient oral hygiene ability, tissuebiotype and patient finances. An implantsupported prosthesis should be utilizedwhen possible for patients 65 years ofage or younger, due to its higher longterm success rate. Although eachpatient must be evaluated individually,patients in their 70’s and 80’s willusually not require the same degreeof long-term success.
Patients with an opposing completeupper denture will not generate ashigh a level of functional force asthose with a natural dentition and
Factors in Implant Supported Mandibular Overdenture Designs
David Todd, DMD, MD
Figure 1 Lack of an adequate labial vestibuleand attached tissue is evident. The heads of2 of the transitional implants are evident.
Figure 2 Split thickness dissection is performedto re-establish the vestibule.
Figure 3 A free gingival graft is sutured intoposition.
Implant Realities26
Vol. II • issue 3 • 2004 27
hyperplastic mucosa and was referredto the surgeon for improvement of hersoft tissues prior to restoration. Initialexamination demonstrated a lack oflabial vestibule and an absence ofattached tissue. The 2 midlineimplants were placed too far labially tobe utilized (Figure 1). Severemandibular resorption and a strongmentalis muscle were evident. It wasrecommended that the current implantsbe removed, but the patient refused.Therefore, a vestibuloplasty andgingival grafting procedure from thepalate were performed. A partialthickness dissection was carried outalong the labial aspect of the mandiblewith care not to extend the incisionsinto the mental nerve region, whichmay exit along the crest of the ridge ina severely resorbed mandible (Figure 2).
Overcorrection of the anticipatedvestibule was required, as relapse inthe case of a severely resorbedmandible may be significant due tothe force of the mentalis muscle.
The tissue surrounding the implantswas excised and trimmed in asupraperiosteal fashion. A freegingival graft was harvested in the
Figure 4 The last 2 transitional implants areremoved and 2 Straumann implants are placed.
Figure 5 A view of the final result 3 monthsafter delivery of the overdenture.
II. The Role of Keratinized Tissueand Vestibular Depth
In order to prepare patients withmoderate to severe mandibular ridgeatrophy for implant therapy the amountof attached keratinized tissue on theresidual ridge should be assessed.Ideally, at least 3-4 mm of attachedtissue should be present on the labialand lingual aspects of the implants. Ifthe residual band of attached tissue isless than 5-6 mm in width, soft tissuegrafting is indicated. Lesser widths ofresidual tissue should not be “split”and repositioned at the time ofimplant placement, as this repositionedtissue may be lost, or the proceduremay not result in adequate keratinizedtissue following healing.
The depth of the vestibule should also be evaluated and corrected asnecessary at the time of soft tissuegrafting. The extent of the vestibulewhich can be re-established isproportional to the size of the residualmandible and is limited in cases ofmore severe ridge atrophy. Thereshould be a 6 week healing periodbetween a vestibuloplasty and gingivalgraft procedures and implantplacement.
Case 1
A woman in her late 80’s had 4transitional implants placed in heranterior mandible. The patient hadbeen unable to wear her temporaryprosthesis. She presented to hergeneral dentist with inflamed,
Figure 6 A lack of attached tissue andinadequate vestibule are evident.
Figure 7 A pre-operative panorexdemonstrates moderate alveolar resorption.
Figure 8 A partial thickness dissection hasbeen performed.
Figure 9 A palatal graft has been harvested.
Figure 10 A free gingival graft is sutured intoposition.
Figure 11 The keratinized tissue was splitand rotated lingually at the time of implantplacement.
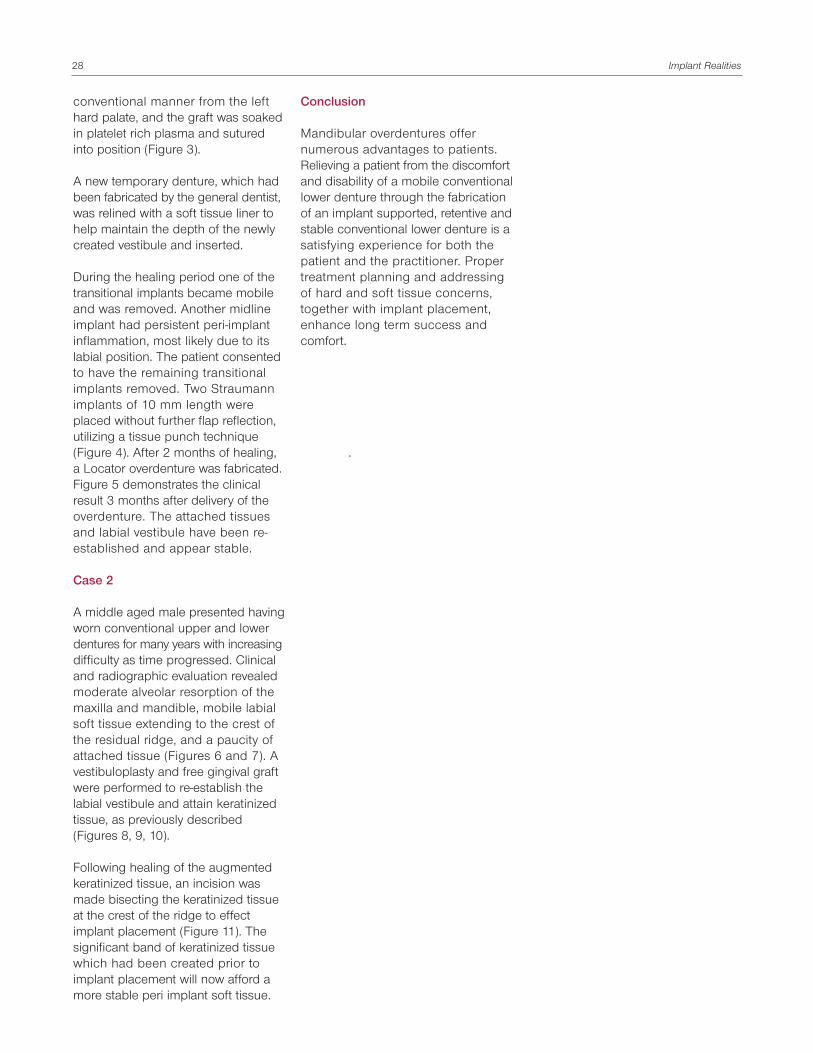
conventional manner from the lefthard palate, and the graft was soakedin platelet rich plasma and suturedinto position (Figure 3).
A new temporary denture, which hadbeen fabricated by the general dentist,was relined with a soft tissue liner tohelp maintain the depth of the newlycreated vestibule and inserted.
During the healing period one of thetransitional implants became mobileand was removed. Another midlineimplant had persistent peri-implantinflammation, most likely due to itslabial position. The patient consentedto have the remaining transitionalimplants removed. Two Straumannimplants of 10 mm length wereplaced without further flap reflection,utilizing a tissue punch technique(Figure 4). After 2 months of healing,a Locator overdenture was fabricated.Figure 5 demonstrates the clinicalresult 3 months after delivery of theoverdenture. The attached tissues and labial vestibule have been re-established and appear stable.
Case 2
A middle aged male presented havingworn conventional upper and lowerdentures for many years with increasingdifficulty as time progressed. Clinicaland radiographic evaluation revealedmoderate alveolar resorption of themaxilla and mandible, mobile labialsoft tissue extending to the crest ofthe residual ridge, and a paucity ofattached tissue (Figures 6 and 7). Avestibuloplasty and free gingival graftwere performed to re-establish thelabial vestibule and attain keratinizedtissue, as previously described(Figures 8, 9, 10).
Following healing of the augmentedkeratinized tissue, an incision wasmade bisecting the keratinized tissueat the crest of the ridge to effectimplant placement (Figure 11). Thesignificant band of keratinized tissuewhich had been created prior toimplant placement will now afford amore stable peri implant soft tissue.
Conclusion
Mandibular overdentures offernumerous advantages to patients.Relieving a patient from the discomfortand disability of a mobile conventionallower denture through the fabricationof an implant supported, retentive andstable conventional lower denture is asatisfying experience for both thepatient and the practitioner. Propertreatment planning and addressing of hard and soft tissue concerns,together with implant placement,enhance long term success andcomfort.
.
Implant Realities28

Vol. II • issue 3 • 2004 29
Soon after the introduction of the root-form implant and the phenomenon ofosseointegration, there was muchspeculation about the therapeuticfuture of root resections as a viablemodality for the treatment of thefurcated molar. A number of papersdealing with the success of root-resected teeth were published beforethe advent of predictable dentalimplant therapy, thus eliminatingimplant dentistry from the diagnosticdecision tree. In an effort to moreproperly address the issue of rootresection vs. implant placement, thisliterature review includes three paperswritten since the advent of “modern”implant dentistry, two case series andone review article.
Carnevale G, Di Febo G, Tonelli MP,Marin C, Fuzzi MA. A RetrospectiveAnalysis of the Periodontal-ProstheticTreatment of Molars with Inter-radicular Lesions. Int J PeriodontRest Dent 1991; 11:189-205.
This retrospective study wasundertaken to report on thesuccess/failure of root resectiontherapy of 500 teeth over a period of3 to 11 years. Root amputation orhemisection was performed on 407grade II or III furcated teeth, 81 teethpresenting with deep osseousdefects, 11 teeth with endodonticlesions and one carious tooth. Teethincluded were maxillary (174) andmandibular (140) first molars,
maxillary (101) and mandibular (72)second molars, maxillary (4) andmandibular (6) thirds molars andmaxillary first premolars (3). All 500teeth were restored: 309 terminalabutments, 127 intermediateabutments, and 64 as single crowns.All patients were recalled forperiodontal maintenance and re-examination, at 1 month (1%), 3month (95.5%), or 6 month (3.5%)basis. Treatment failures included:loss of cementation, root fracture,abutment fracture, progressiveprosthesis mobility or solder-jointfailure, probing depth >5 mm,untreatable endodontic failure, andcaries.
488 teeth were evaluated (12 wereunavailable). 303 were followed for 3-6 years, and 185 for 7 to 11 years.The overall failure rate was 5.7%. The3 to 6 year group showed a 6.9%failure rate and the 7 to 11 year groupa 3.8% failure rate. When comparedto other teeth selected as controls,differences in probing depths werenot significantly different; plaque indexand gingival indices were low for both,but statistically better in the controlgroup.
Due to the retrospective nature of thisstudy, it is impossible to make generalconclusions about all furcated teeth,as some may have been strategicallyremoved early in treatment, and thereis no true control group. However,
within the limitations of this study, rootresection therapy seems to be aneffective means of treating certainperiodontal, endodontic, and carieslesions. They pointed out that most ofthe teeth in this study were treatedbecause of periodontal breakdown(97.6%), and only three teeth (0.6%)showed probing depths beyond 5 mmafter treatment. The majority of thefailures were of non-periodontaletiology: caries, root fracture, cementwashout, and untreatable endodonticproblems. These findings underscorethe technique-sensitivity of rootresection and the importance ofproper execution of all phases oftreatment, optimal oral hygiene, andmaintenance therapy.
Fugazzotto PA. A Comparison of theSuccess of Root Resected Molarsand Molar Position Implants inFunction in a Private practice:Results up to 15-Plus Years.J Periodontol 2001;72:1113-1123.
This retrospective case series studywas undertaken to assess the long-term results of root resection andsubsequent restoration or molarimplant placement and subsequentrestoration in a single private practicesetting. The treatment groupsincluded 701 root-resected molarsand 1,472 molar implants evaluatedafter 15 and 13 years respectively. Allsurgical and maintenance therapies(for at least 5 years postoperatively)
Carnevale G, Di Febo G, Tonelli MP, Marin C, Fuzzi MA. A Retrospective Analysis of the Periodontal-ProstheticTreatment of Molars with Interradicular Lesions. Int J Periodont Rest Dent 1991; 11:189-205.
Fugazzotto PA. A Comparison of the Success of Root Resected Molars and Molar Position Implants in Function in aPrivate Practice: Results up to 15-Plus Years. J Periodontol 2001;72:1113-1123.
Kinsel RP, Lamb RE, Ho D. The Treatment Dilemma of the Furcated Molar: Root Resection Versus Single ToothImplant Restoration. A Literature Review. Int J Oral and Maxillofac Implants 1998;13:322-332.
Literature Review:Root Resection Versus the Dental Implant: A Diagnostic Dilemma
Philip R. Melnick, DMD; Paulo M. Camargo, DDS, MS

were completed in the author’spractice.
Cumulative success rates were 96.8%for root-resected molars and 97.0% formolar implants. Treatment success inboth groups was statistically related toother clinical issues, such as positionof the tooth or implant in the arch,splinted versus non-splintedrestorations, and occlusal forces.Lowest success rates in eachcategory were, for resected teeth,distal root of mandibular molar (75%),and for the implants the lone standingimplant in the second molar position(85%). Lone standing terminalabutments in both groups showed thehighest failure: 30.4% (7 of 23) forresected teeth and 37.8% (17 of 45)for implants. The author attributed thehigher failure rate to untreatedparafunction. First molars did betterthan second molars with maxillarysecond molars showing the lowestsuccess rates at 92.9% and maxillaryfirst molars the highest success rate at97.6%.
The author suggested that rootresection be undertaken only aftercarefully analyzing all clinicalparameters involved in treatment:periodontal, endodontic, restorative,and occlusal. He concluded that highsuccess rates can be achieved whenthere is adequate remaining toothstructure, protection within an intactarch or as part of a splintedprosthesis, and when occlusal forcesare controlled.
The success of molar implants rangedfrom 84% in the mandibular secondmolar location to 98.4% in themandibular first molar position. Thissignificant difference was attributed topossible trauma at insertion orparafunctional forces. Consequently,control of these factors and minimalbacterial contamination wouldimprove the expectation of long-termsuccess.
The author concluded that while bothmodalities show comparable successrates, they are not necessarilyinterchangeable. Many factors must
be considered in the treatmentselection as they relate to generalpatient considerations (e.g. generalhealth, plaque control, psychological),and site-specific issues (e.g. cariesrate, dental morphology, prior boneloss, endodontic feasibility). These areto be viewed in the context of acomprehensive diagnosis andtreatment plan, with an eye on long-term predictability, cost-effectiveness,and preventive care.
Kinsel RP, Lamb RE, Ho D. TheTreatment Dilemma of the FurcatedMolar: Root Resection Versus SingleTooth Implant Restoration. ALiterature Review. Int J Oral andMaxillofac Implants 1998; 13:322-332.
There is substantial evidence thatmolar teeth have a predilection forperiodontal breakdown. Interradicularanatomy has been implicated as bothsecondarily etiologic to the diseaseprocess and a complicating factor toits treatment. Treatment options, non-surgical and surgical, have met withvarious levels of success. With theexception of one study, all othersreviewed herein describe continuingattachment loss over time. This paperhighlights the treatment of thefurcated molar with root resectiontherapy and the molar implant.
Indications for root resection included:1) severe vertical bone loss involvingone root, 2) furcation bone loss in amaxillary molar inaccessible to plaquecontrol 3) root proximity whichinterferes with maintenance of Class Ior II furcation invasions, 4) furcationcompromised by bone loss or carieswhich cannot be properly restoredand maintained, 5) fixed partialdenture abutments or piers withnegative prognosis due to periodontalbreakdown, 6) individual root fracture,7) endodontically involved teeth notamenable to conventional or surgicalendodontic therapy.
The authors reported a wide disparityin long-term outcomes resulting fromroot resection, with failure/complicationrates ranging from 11.8% to 38%. Atthe time of publication, there were
limited studies on single, independentimplant restorations. Single molartooth implants reviewed were reportedto have a failure rate ranging from 0 to10%.
The authors attempted to answer thequestion “when should a furcatedmolar be extracted, and when shoulda root resection be employed?” Theyproposed a number of negativefactors to be considered in rootresection prognosis: decreased bonesupport for all roots, combined withreversed crown to root ratio, deepvertical defects combined with a ClassII or III furcation invasion, fused roots,untreatable endodontic problem, poorremaining root anatomy, poor plaquecontrol ability, tooth unrestorability,and tooth hypermobilty. Situationsfavoring implant placement wouldinclude: sufficient bone quality, heightand width to support anticipatedocclusal forces, adequate interdentaland interarch distance, absence ofmedical contraindications, or personalhabits, and adequacy of oral hygiene.
When deciding on a treatmentmodality the prognosis will bedetermined by a number of factors,including: root anatomy, endodonticpredictability, occlusal forces, initialmobility, skills of the therapist, andpatient compliance. The authorssuggest that if these factors are lessthan optimal, the long-term retentionof furcated molars via root resection isquestionable. On the other hand,evidence seems to indicate thatsuccessful placement and restorationof dental implants are less reliant onthe experience or skill of the therapist,and may be the treatment of choice incompromised situations.
Conclusion
All three papers discussed agree thatroot resection can be a successfuland predictable treatment for thefurcated molar in certain situations.However, high levels of diagnostic,treatment planning and therapeuticskill seem to be required. Whereas,the potential for success with rootresection seems to be much more
Implant Realities30

Vol. II • issue 3 • 2004 31
narrowly defined, the data presentedsuggest that dental implants in themolar positions are a predictable andperhaps less technically demandingprocedure. Nevertheless, care mustbe exercised in the decision-makingprocess to be sure that whichevertreatment is undertaken it is part of a well thought out, patient and sitespecific treatment plan.

2004 Courses
Comprehensive Implant Prosthetics and Predictable Anterior EstheticsSeptember 17 • Ft. Collins, COSeptember 18 • Colorado Springs, COOctober 9 • Newport Beach, CANovember 19 • Newport Beach, CADr. Robert Vogel
Esthetic Solutions for Fully and Partially Edentulous PatientsSeptember 10 • Newport Beach, CANovember 12 • Newport Beach, CADr. Gary Solnit
Dental Assistant Training: RestorativeSeptember 15 • Newport Beach, CANovember 4 • Newport Beach, CAPascale Hartmann, RDH Swiss
Basic Restorative Procedures for Dental ImplantsSeptember 17 • Malvern, PAOctober 2 • New Brunswick, NJDr. David Felton
Immediate Placement and Advanced Surgical TechniquesSeptember 17 - 18 • Newport Beach, CA (SOLD OUT) October 15 - 16 • Newport Beach, CADr. Jay Beagle
Advanced Surgical Techniques for Immediate PlacementSeptember 17 - 18 • Newport Beach, CA (SOLD OUT)October 14 - 15 • Newport Beach, CADr. Jay Beagle
Multiple Posterior Implant Placement and Sinus GraftingSeptember 24 - 25 • Newport Beach, CA (SOLD OUT)December 3 - 4 • Newport Beach, CADr. Jay Beagle
Immediate Loading on Partially and Fully Edentulous PatientsOctober 1 • Newport Beach, CA Dr. Robert Jaffin
Dental Hygiene CourseOctober 8 • Newport Beach, CA Pascale Hartmann, RDH Swiss
Clinical Realities of Periodontal Regenerative and Root Coverage Procedures: A Live Surgical CourseOctober 15 • Milton, MADr. Paul Fugazzotto617/696 7257
US ITI Congress 2004October 23 - 24 • Chicago, IL
Clinical Realities of Ridge and Sinus Augmentation: A Live Surgical CourseOctober 27 • Milton, MA December 8 • Milton, MADr. Paul Fugazzotto617/696 7257
Clinical Realities of Immediate LoadingOctober 28 • Milton, MADecember 9• Milton, MA Dr. Paul Fugazzotto, Dr. Richard Baker, and Mr. Ira Dickerman617/696 7257
Simplifying Esthetic and Implant DentistryDecember 3 - 4 • Las Vegas, NVDrs. James Ruskin, Dean Morton, and Will Martin
Upcoming events
For all course information, please contact Straumann’s Training and Education Department at 800/448 8168 (unless otherwise noted).




Implant Realities© August 2004Printed in USA
IR 204