implanted cardiac defibrillator care in radiation oncology patient population
TRANSCRIPT

Int. J. Radiation Oncology Biol. Phys., Vol. 73, No. 5, pp. 1525–1531, 2009Copyright � 2009 Elsevier Inc.
Printed in the USA. All rights reserved0360-3016/09/$–see front matter
doi:10.1016/j.ijrobp.2008.06.1903
CLINICAL INVESTIGATION Implanted Defibrillator
IMPLANTED CARDIAC DEFIBRILLATOR CARE IN RADIATION ONCOLOGYPATIENT POPULATION
DAPHNA Y. GELBLUM, M.D.,* AND HOWARD AMOLS, PH.D.y
Departments of *Radiation Oncology and yMedical Physics, Memorial Sloan-Kettering Cancer Center, New York, NY
Purpose: To review the experience of a large cancer center with radiotherapy (RT) patients bearing implantablecardiac defibrillators (ICDs) to propose some preliminary care guidelines as we learn more about the devices andtheir interaction with the therapeutic radiation environment.Methods and Materials: We collected data on patients with implanted ICDs treated with RT during a 2.5-yearperiod at any of the five Memorial Sloan-Kettering clinical campuses. Information regarding the model, location,and dose detected from the device, as well as the treatment fields, fraction size, and treatment energy was collected.During this time, a new management policy for these patients had been implemented requiring treatment with low-energy beams (6 MV) and close surveillance of the patients in partnership with their electrophysiologist, as theyreceived RT.Results: During the study period, 33 patients were treated with an ICD in place. One patient experienced a defaultof the device to its initial factory setting that was detected by the patient hearing an auditory signal from the device.This patient had initially been treated with a 15-MV beam. After this episode, his treatment was replanned to becompleted with 6-MV photons, and he experienced no further events.Conclusion: Patients with ICDs and other implanted computer-controlled devices will be encountered more fre-quently in the RT department, and proper management is important. We present a policy for the safe treatmentof these patients in the radiation oncology environment. � 2009 Elsevier Inc.
Implanted cardiac defibrillator, Radiotherapy, Patient monitoring.
INTRODUCTION
Recent advances in the field of cardiology have improved the
longevity of patients with acute myocardial infarction and
heart failure. These developments have come from both the
medical and technical arenas, with two trials demonstrating
an advantage in the prophylactic use of implantable cardiac
defibrillators (ICDs). These two studies, the Sudden Cardiac
Death in Heart Failure trial (1) and the Defibrillators in Non-
ischemic Cardiomyopathy Treatment Evaluation (2), demon-
strated a 27% and 23% decrease in sudden death,
respectively, with the prophylactic use of ICDs compared
with medical management alone. The cost-effectiveness of
implanting and maintaining the devices compared with
chronic medical treatment of these patients has also been es-
tablished (3, 4). As a result, Medicare and Medicaid Services
have agreed to expand their coverage of these devices to in-
clude the preventative setting. During the past 10–20 years,
the devices have become smaller, and the implantation proce-
dure has become much less morbid. These factors will
presumably translate into an increased likelihood that these
152
patients will thrive with their cardiac conditions and require
radiotherapy (RT) for a cancer diagnosis in their lifetime.
The proper treatment of these patients in the RT depart-
ment in the era of high-energy linear accelerators is not
well understood. The American Association of Physicists
in Medicine last proposed guidelines for the treatment of pa-
tients with implanted cardiac devices in 1994 (5). This docu-
ment concentrated on the treatment of patients with
implanted cardiac pacemakers and only commented on the
emergence of implantable defibrillators and the need to re-
view their function in the future. Other groups in Europe
have also begun to explore the topic (6, 7) and have suggested
from in vivo testing that some signal detection interference
might occur when the device is placed in the radiation field.
The dose tolerance of the devices has been studied (6, 8, 9),
and it has been shown that the complementary metal oxide
semiconductor used is the most dose-sensitive component.
Within this, the random access memory (RAM) holds the in-
dividual patient pacing and detection threshold information.
To protect this element, it has been proposed that the total
dose seen by the defibrillator should not exceed 2–5 Gy,
Reprint requests to: Daphna Y. Gelblum, M.D., Department ofRadiation Oncology, Memorial Sloan-Kettering Cancer Center,650 Commack Rd., Commack, NY 11725. Tel: (631) 623-4200;Fax: (631) 864-5786; E-mail: [email protected]
Conflict of interest: none.Received Jan 25, 2008, and in revised form June 19, 2008.
Accepted for publication June 20, 2008.
5

1526 I. J. Radiation Oncology d Biology d Physics Volume 73, Number 5, 2009
depending on the report. Company literature reflects these
findings as well (10–12), and some manufacturers have
been unwilling to quote a minimally acceptable dose.
Three potential interactions can occur between the ICD
and radiation generation and therapy delivery. The first is re-
lated to the radiation dose delivered to the device. The second
is the unintentional firing of the device during treatment as
a result of radiofrequency interference from the linear accel-
erator. Third, and perhaps most important, is the possible re-
programming of the device from some poorly understood
interference from the linear accelerator or the radiation
beam itself. The problem of reprogramming the defibrillators
is a stochastic event that we have now encountered on two
occasions in 2 separate patients during the past 3 years.
At Memorial Sloan-Kettering Cancer Center, we are en-
countering greater numbers of these patients and as a result
have looked to the manufacturers’ data and company techni-
cal support more closely for guidelines on how to handle
these patients safely. We have found a broad spectrum of
opinion with few supportive data. One school of thought is
that no interference has been documented between the
high-energy linear accelerators used in oncology and the
function of the defibrillator devices. Thus, beyond a discus-
sion with the treating cardiologist, no further special monitor-
ing has been advised, aside from minimizing the dose to the
device and interrogating it before the start, and after the com-
pletion, of the RT course. On the more conservative side,
other sources have suggested daily suspension of tachycardia
detection and therapy delivery by magnet placement during
RT sessions and frequent device interrogation to confirm
continued functioning. Published cardiac device malfunction
registries only track devices that require explantation and re-
placement, which is typically not required in the radiation set-
ting; thus, they do not capture the events of concern in our
patient population (13, 14). A survey of current practice in
the United States was undertaken by Solan et al. in 2004
(15). Their review underscored the lack of understanding
that exists in the clinical office practice of radiation oncology
and has prompted us to study this issue further.
METHODS AND MATERIALS
The sentinel case in our department that prompted our policy re-
vision was witnessed in a patient found to have a malfunctioning
ICD who had been treated for prostate cancer. As was our standard
policy at the time for all patients with implanted cardiac devices, a di-
ode was placed on his defibrillator (which was positioned outside of
the radiation portal in his left chest) on the first day of his RT ses-
sions to document the dose delivered to the device on a daily basis.
Additionally, a rhythm strip was run to confirm normal cardiac
rhythm during RT. He was treated with 15-MV photons and re-
ceived a total dose of 8,640 cGy in 48 fractions uneventfully. On
a follow-up visit with his cardiologist, it was found that his cardio-
defibrillator had reverted back to its initial factory programmed set-
tings. From the ICD’s memory, it was established that the
reprogramming had occurred immediately after one of his daily
RT visits. The device was reprogrammed and interrogated, with
the finding that the patient had not experienced any cardiac events
during that time, and he has not experienced any subsequent events.
In an attempt to quantify the incidence of these devices in our pa-
tient population and to capture any RT-associated malfunctions, a re-
view of our patients was conducted. After obtaining permission
from the institutional review board, all physicians in our main facil-
ity in Manhattan, as well as in our four regional offices, were asked
to complete a brief questionnaire documenting the specifics of the
case and submit it to a central data collection site when they encoun-
tered and treated patients with ICDs. This report presents our expe-
rience between June 2005 and December 2007. The data collection
began after an ad hoc committee, composed of radiation oncologists,
radiation nurses, cardiologists, and physicists, had already estab-
lished new patient management guidelines in light of the recent ex-
periences in the department (Fig. 1). It was decided that every
patient’s case would be individually discussed with their electro-
physiologist and that, at a minimum, no patient would be treated
with an energy >6 MV to prevent stray neutron emission, a suspected
cause of electrical interference. On the first day of treatment, a ther-
moluminescent dosimeter would be placed on the device to docu-
ment the dose delivered to the device, and a rhythm strip would
also be run during the entire first treatment delivery to visualize
the cardiac rhythm. Additional manipulation and monitoring of
the device was then individualized according to the specific manu-
facturer’s recommendations and the recommendations of the pa-
tient’s private electrophysiologist. This additional monitoring
ranged from daily post-treatment device interrogation in patients
deemed to be device dependent and who had a history of proper de-
vice firing in the past, to educating patients with self-check devices
to use the magnet to verify proper ICD functioning themselves, to
weekly interrogation by a company representative.
RESULTS
During the study period, 12,972 patients were treated at the
radiation oncology department of Memorial Sloan-Kettering
Cancer Center. Of these patients, 33 had ICDs (Table 1). Of
the 33 patients, 22 had been treated with definitive intent and
11 palliatively. Two patients required relocation of the device
out of the proposed radiation portal before starting RT. Three
patients were treated sequentially to two separate fields for
multifocal disease. Two patients had their prescribed treat-
ment dose limited because of dose constraints posed by the
presence of the defibrillator. The total dose to the ICDs was
1–299 cGy (Table 1). The patient management policy
followed is outlined in Fig. 1.
During the study period, 1 additional patient experienced
a resetting of his device during therapy (Patient 5, Table 1).
This patient was receiving treatment of rectal cancer and
again had been treated with 15-MV photons. He had a Med-
tronic device, which is built to send an audible alert when the
device reverts to the factory settings. This occurred after only
four treatments, although the patient stated that he was not
aware of the tone for an additional 5 days. The device had
been located well out of the radiation portal in the left chest
and had been interrogated before and after his first RT session
without incident. After consultation with this patient’s elec-
trophysiologist, the company representative was called,
who reprogrammed the device. He completed therapy with
6-MV photons. For the remainder of the RT, a rhythm strip

Defibrillator care in radiation d D. Y. GELBLUM AND H. AMOLS 1527
Fig. 1. Newly adopted patient management guidelines for patients with implantable cardiac defibrillators who are under-going treatment in the Department of Radiation Oncology at Memorial Sloan-Kettering Cancer Center (New York, NY).
was run and observed daily at the treatment machine, and the
company representative was on site for daily, post-RT inter-
rogation of the defibrillator. He completed his cancer therapy
successfully to a total dose of 50.4 Gy in 28 fractions and has
had no further issues. This patient was treated at the time that
the institutional policy was being formulated and was ini-
tially treated with 15-MV beams. Since then, we have treated
all patients with ICDs with low-energy 6-MV beams and
have not had any further events. We are confident with the
treatment plan defined.
The ICD in 3 patients was exposed to >2 Gy without expe-
riencing ICD malfunction, supporting our hypothesis that
this is not a dose-driven effect.
DISCUSSION
As implantable medical devices become more common
and successful in permitting the population to age, the fre-
quency of these encounters in RT departments will increase.
It is incumbent on the radiation oncologist to understand the
interaction of our linear accelerators with these devices to en-
sure the safety of our patients. The total dose delivered to the
device is known to be a hazard to the function of any mechan-
ical device located in or near a radiation field; thus, all im-
planted devices (e.g., pacemakers, infusion pumps, ICDs)
should be kept outside the primary radiation beam. Clinicians
and scientists unfamiliar with therapeutic radiation have ad-
vised ‘‘shielding the device’’ if it is in the direct beam. In
the case of a typical 6-MV beam, >5 cm of lead would be nec-
essary to attenuate the beam by 90%; thus, a simple lead
apron would not be effective and might even increase the po-
tential for scatter dose. With the increased use of intensity-
modulated RT, an often forgotten introduction of increased
photon scatter propagated from the head of the linear acceler-
ator has occurred. More conformal treatment delivery has
also permitted dose escalation, which also leads to increased
scatter. Thus, the only solution is to physically separate the
device from the radiation portal, in some cases requiring sur-
gical relocation of the device.
The issue of possible aberrant firing of the defibrillator
is of most concern with St. Jude’s medical products (11).
This seems to be a hypothetical occurrence that, according
to all three of the leading manufacturers in the United
States, has never been known to have occurred. The con-
cern is that the radiofrequency generated at the head of the
linear accelerator as the photon beam is generated would
cause the ICD to inappropriately deliver therapy in the ab-
sence of cardiac arrhythmia. Because other environmental
settings exist in which ICDs can misfire, we have thought
that protecting against this possibility might not be war-
ranted, although educating the patient and staff about
this possibility is.
1528 I. J. Radiation Oncology d Biology d Physics Volume 73, Number 5, 2009
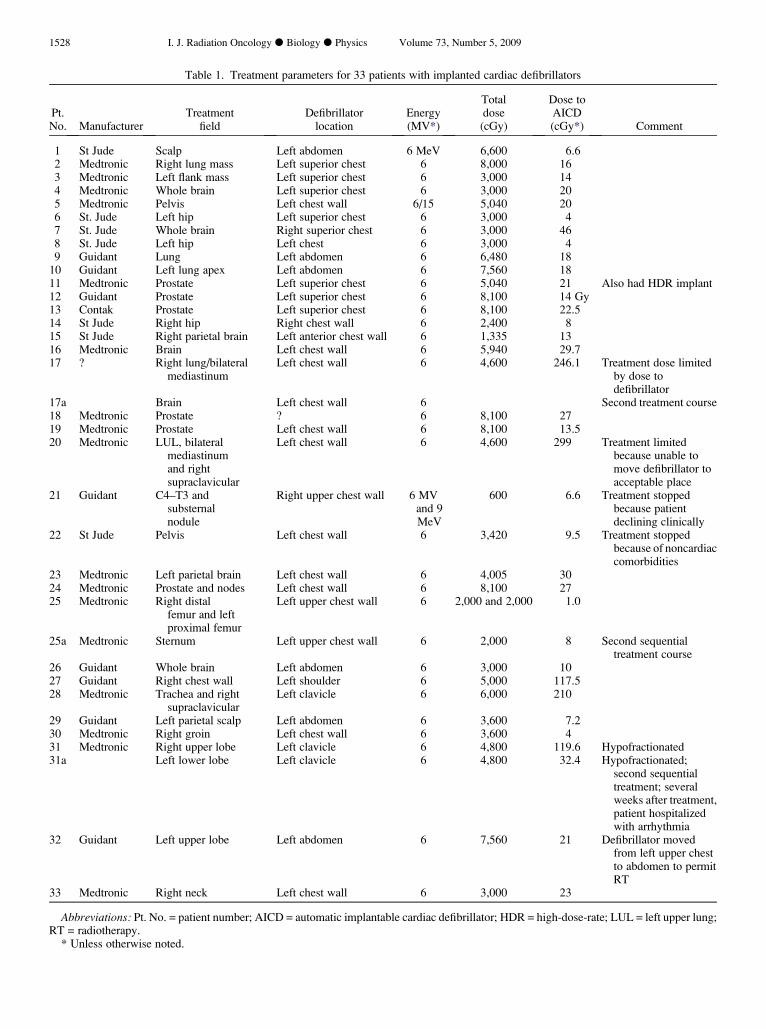
Table 1. Treatment parameters for 33 patients with implanted cardiac defibrillators
Pt.No. Manufacturer
Treatmentfield
Defibrillatorlocation
Energy(MV*)
Totaldose(cGy)
Dose toAICD(cGy*) Comment
1 St Jude Scalp Left abdomen 6 MeV 6,600 6.62 Medtronic Right lung mass Left superior chest 6 8,000 163 Medtronic Left flank mass Left superior chest 6 3,000 144 Medtronic Whole brain Left superior chest 6 3,000 205 Medtronic Pelvis Left chest wall 6/15 5,040 206 St. Jude Left hip Left superior chest 6 3,000 47 St. Jude Whole brain Right superior chest 6 3,000 468 St. Jude Left hip Left chest 6 3,000 49 Guidant Lung Left abdomen 6 6,480 18
10 Guidant Left lung apex Left abdomen 6 7,560 1811 Medtronic Prostate Left superior chest 6 5,040 21 Also had HDR implant12 Guidant Prostate Left superior chest 6 8,100 14 Gy13 Contak Prostate Left superior chest 6 8,100 22.514 St Jude Right hip Right chest wall 6 2,400 815 St Jude Right parietal brain Left anterior chest wall 6 1,335 1316 Medtronic Brain Left chest wall 6 5,940 29.717 ? Right lung/bilateral
mediastinumLeft chest wall 6 4,600 246.1 Treatment dose limited
by dose todefibrillator
17a Brain Left chest wall 6 Second treatment course18 Medtronic Prostate ? 6 8,100 2719 Medtronic Prostate Left chest wall 6 8,100 13.520 Medtronic LUL, bilateral
mediastinumand rightsupraclavicular
Left chest wall 6 4,600 299 Treatment limitedbecause unable tomove defibrillator toacceptable place
21 Guidant C4–T3 andsubsternalnodule
Right upper chest wall 6 MVand 9MeV
600 6.6 Treatment stoppedbecause patientdeclining clinically
22 St Jude Pelvis Left chest wall 6 3,420 9.5 Treatment stoppedbecause of noncardiaccomorbidities
23 Medtronic Left parietal brain Left chest wall 6 4,005 3024 Medtronic Prostate and nodes Left chest wall 6 8,100 2725 Medtronic Right distal
femur and leftproximal femur
Left upper chest wall 6 2,000 and 2,000 1.0
25a Medtronic Sternum Left upper chest wall 6 2,000 8 Second sequentialtreatment course
26 Guidant Whole brain Left abdomen 6 3,000 1027 Guidant Right chest wall Left shoulder 6 5,000 117.528 Medtronic Trachea and right
supraclavicularLeft clavicle 6 6,000 210
29 Guidant Left parietal scalp Left abdomen 6 3,600 7.230 Medtronic Right groin Left chest wall 6 3,600 431 Medtronic Right upper lobe Left clavicle 6 4,800 119.6 Hypofractionated31a Left lower lobe Left clavicle 6 4,800 32.4 Hypofractionated;
second sequentialtreatment; severalweeks after treatment,patient hospitalizedwith arrhythmia
32 Guidant Left upper lobe Left abdomen 6 7,560 21 Defibrillator movedfrom left upper chestto abdomen to permitRT
33 Medtronic Right neck Left chest wall 6 3,000 23
Abbreviations: Pt. No. = patient number; AICD = automatic implantable cardiac defibrillator; HDR = high-dose-rate; LUL = left upper lung;RT = radiotherapy.
* Unless otherwise noted.

Defibrillator care in radiation d D. Y. GELBLUM AND H. AMOLS 1529
Few reports have been published documenting the possi-
ble interactions between RT and ICDs, although a few case
reports have been submitted. Thomas et al. (16) reported in
a cardiac journal, a case report of a patient with a history of
coronary artery disease, myocardial infarction, coronary ar-
tery bypass, hypertension, atrial fibrillation, and right upper
lung cancer. The patient had had an ICD implanted in the
left chest wall. After 56 Gy delivered to his right-sided
lung cancer in 2.0-Gy/d fractions with 18-MV photons, he
was seen by his cardiologist. On interrogation of the ICD,
it was found to have reset to its fallback setting 9 days earlier
during RT session (determined by comparing the date and
time of the stored event and the patient’s therapy schedule).
No other malfunction was found in the device after additional
testing. They speculated that not only is direct or scattered
dose to the device of concern, but also the potential for elec-
tromagnetic interference of the ICD from the linear accelera-
tor. Hoecht et al. (17) in a letter to the editor briefly
mentioned an ICD malfunction that had occurred in a patient
undergoing RT in their department. The exact details of the
treatment parameters were not discussed, but they did men-
tion that the ICD was seated in a pectoral pocket, and the
RT was delivered to the patient’s pelvis. The malfunctioning
device was found to have gone into a fallback programming
to the fixed detection area and a fixed pace rate of 50/min.
Nemec (18) published a case report of a patient treated to
a thoracic tumor in the left chest with a Guidant ICD also
seated in the left chest, as documented by an accompanying
X-ray film. The radiation energy used for treatment was not
documented, and mention was made that the treating physi-
cians did not find it necessary to relocate the ICD before treat-
ment. During the third session (180-cGy fractions), the
patient collapsed and was found to have wide complex tachy-
cardia. The patient recovered, and the device interrogation
after explantation because of feared radiation damage failed
to show any malfunction. The manufacturer suspected a scat-
tered radiation effect on the RAM. The total radiation dose to
the device was not known.
Sepe et al. (19) reported on their experience treating a pa-
tient for larynx cancer with 6-MV photons to a total dose of
60 Gy. During the course of therapy, the ICD received a cu-
mulative dose of 2.5 Gy. They continually monitored the
device throughout the therapy and immediately after comple-
tion of the RT course and found no adverse effects. They sug-
gested a similar management policy as put forth in the present
report, with the exception of a blanket recommendation to
disarm the ICD on a daily basis for treatment, with continual
electrocardiographic monitoring.
It is not only the direct photon exposure of a device that
must be considered, but also the potential for a single hit neu-
tron particle interaction. Much like radiation damage to a liv-
ing cell, radiation damage to ICDs and similar solid state
devices can, theoretically, manifest by way of two physically
different pathways, the so-called somatic or stochastic path-
ways. Somatic effects, such as skin erythema or loss of infor-
mation stored in the ICD’s memory, can result from
accumulation of a low-energy transfer (LET) dose, for which
no threshold dose has been established and for which the
magnitude of the effect is proportional to the absorbed
dose. Catastrophic or stochastic events, such as cell mutation
or total ICD failure, however, can also result from the passage
of a few, or even a single high LET particle through a cell nu-
cleus or an ICD chip. Stochastic effects are usually all or
nothing bimodal events—either the catastrophic happens or
it does not. Another example of a random catastrophic ICD
effect would be emitting a high-voltage shock without detec-
tion of cardiac arrhythmia. Unlike somatic effects, the prob-
ability of occurrence of a stochastic event is dose dependent,
but the magnitude of the damage or failure is not.
Published data have documented that relatively high radi-
ation doses (>1 Gy) do indeed cause cumulative damage to
ICDs, and virtually every manufacturer has recommended
that ICDs not be placed directly in the radiation beam, even
if it requires surgical repositioning. When such precautions
are taken, none of our findings nor any published reports
that we are aware of have suggested that small (<1 Gy) radi-
ation doses should be of concern to RT patients with ICDs.
Similarly, we know of no documented cases of ICD failure
resulting from the electromagnetic fields produced by high-
energy linear accelerators. Nonetheless, scattered cases
have been reported, including our own, of ICD failure, mem-
ory loss, reprogramming, and so forth, occurring during or
shortly after a RT session. In the events reported in the pres-
ent study, the failure was a reprogramming error (the ICD re-
programmed to its default values) occurring sometime during
the RT course.
Bradley and Normand (20) have reported on extensive
measurements of so-called single event upsets (i.e., sto-
chastic events) in ICDs. Because of the paucity of data
for RT patients, the study by Bradley and Normand was
based entirely on ICD failures observed in the general pop-
ulation that were caused, presumably, by background radi-
ation, plus direct irradiation of ex vivo ICDs under
controlled laboratory conditions. Their data suggested
that the RAM is the subsystem in the ICD most sensitive
to radiation damage because of the small amount of charge
stored in the RAM and its resulting high volatility. Perhaps
more significantly, they reported that the cross-section of
probability of single event upsets is strongly dependent
on LET, increasing by approximately three orders of mag-
nitude as the LET increases from 2 MeV-cm2/mg to 15
MeV-cm2/mg. X-rays and electrons have LETs of about
2 MeV-cm2/mg, and neutrons have LETs of approximately
5–10 MeV-cm2/mg. Although highly speculative, this is
consistent with ICD events observed in vivo in RT patients
only for the high-energy 15-MV X-ray beam for which
neutron contamination is about 0.1% of the total dose.
We speculate that the ICD events observed in RT patients
who have received relatively low radiation doses might be
caused by neutrons rather than by X-rays or other electro-
magnetic radiation. The total dose seen by the defibrillator
in the 2 patients in our study who experienced reprogram-
ming was low, and those few patients in whom the ICD
was exposed to >2 Gy had no issues.

1530 I. J. Radiation Oncology d Biology d Physics Volume 73, Number 5, 2009
The whole body effects of neutron contamination from
high-energy photon beams have been shown by Hall et al.(21). In their work, they demonstrated that when a phantom
was radiated to the pelvis in fields similar to those used for
standard four-field treatment of cervical cancer, the dose re-
ceived by scatter to the breasts was more significant when
the treatment was administered with 20-MV than with
6-MV beams. The dose seen by thermoluminescent dosime-
ter measurements placed in tissue at the level of the breast
was 0.26 Gy for 6-MV and 0.55 Gy for 20-MV treatment
when 70.2 Gy was delivered in a fractionated manner to
the pelvis. A bubble meter was used to quantitate the neutron
dose and detected a 0.005-Gy neutron dose to the tissue flask
in the breast location. This correlated with the calculated ex-
pected maximal neutron dose of 0.015 Gy, assuming a maxi-
mal neutron production rate of 3� 1012 neutron/Gy of X-rays
delivered. This form of radiation delivery to implanted de-
vices cannot be protected against by external blocking mech-
anisms and can only addressed by altering the treatment
delivery to minimize the chance of these interactions occur-
ring. We, therefore, advocate that patients with ICDs be
treated with low energy (<10-MV) photons whenever possi-
ble. Since the institution of that policy, we have not detected
any further reprogramming events. We also continue to vig-
ilantly observe these patients, together with their cardiolo-
gists, as they go through treatment.
The sensitivity of modern devices to RT has not been well
documented. The three leading American manufactures have
failed to establish a ‘‘safe’’ or acceptable dose to the ICD, ac-
knowledging that the remaining issue is scattered dose,
which is difficult to quantitate. To date, the only group to
have studied and published on dose tolerances is Uiterwaal
et al. (22) from The Netherlands. They reported their obser-
vations after irradiating 11 devices from four manufacturers
(the three major American companies and Biotronik, which
is European based). They used 6-MV photon beams to a cu-
mulative dose of 20 Gy. Of the 11 devices they observed, 4
devices had ‘‘complete loss of function’’ after only 1.5 Gy.
They concluded that these are devices are very radiosensitive
and that new guidelines for the treatment of these patients are
indicated. As we await these parameters, we have been suc-
cessful in implementing the policy put forth in the present
report.
CONCLUSION
The complexity of patient treatment in the radiation oncol-
ogy department continues to increase as technology prog-
resses. As evidenced in the present report, the advances
made in other fields of medicine can directly effect how we
function in our departments. The hypothesis that ICD dam-
age is caused by high LET neutron scatter has been proposed
by several investigators, and the clinical evidence presented
in our report supports this theory. We will continue to watch
our patients carefully and urge other centers to do so as well.
When a patient event is witnessed in which the ICD was not
exposed to excessive radiation as a result of therapy and the
ICD malfunctions, this should be reported.
We have adopted and advocate a patient management pol-
icy for patients with ICDs who require RT. We suggest treat-
ment with low-energy beams (<10 MV), keeping the ICD as
far from the treatment field as possible, discussing each indi-
vidual patient’s care with their cardiologist, and determining
the optimal practice. Interrogation should always occur be-
fore and after the initial fraction and again with some fre-
quency thereafter, as determined in consultation with the
patient’s electrophysiologist. A thorough discussion must
be held with the patient to educate them about the issue as
it applies to them and their specific device. The 2006 Journal
of the American Medical Association cardiac patient educa-
tion sheet does not mention RT in their section on ‘‘Concerns
for patients with an ICD’’ (23). It might also be determined
that a patient is so dependent on the defibrillator that they
should not be considered for RT.
The treatment of these patients using proton machines
requires a separate review.
REFERENCES
1. Bardy GH, Lee KL, Mark DD, et al. Amiodarone or and im-plantable cardioverter-defibrillator for congestive heart failure.N Engl J Med 2005;352:225–237.
2. Sanders GD, Hlatky MA, Owens DK. Cost-effectiveness of im-plantable cardioverter-defibrillators. N Engl J Med 2005;353:1471–1480.
3. Glodman L. Cost-effectiveness in a flat world—Can ICDs helpthe United States get rhythm? N Engl J Med 2005;353:1513–1515.
4. Kadish A, Dyer A, Daubert JP, et al. Prophylactic defibrillatorimplantation in patients with nonischemic dilated cardiomyop-athy. N Engl J Med 2004;350:2151–2158.
5. Marbach JR, Sontag MR, Van Dyk J, et al. for the American As-sociation of Physicists in Medicine. Management of radiationoncology patients with implanted cardiac pacemakers: Reportof AAPM Task Group No. 34. Med Phys 1994;21:85–90.
6. Uiterwaal GJ, Springorum BGF, Scheepers E, et al. Influence oftherapeutic irradiation on the latest generation of implantablecardioverters/defibrillators. Europace Supplements 2004;6:96.
7. Uieterwaal GJ, Hurkmans CW, Springorum BF, et al. Interfer-ence signals detection by implantable defibrillators induced bytherapeutic radiation therapy [Abstract]. Heart Rhythm 2004;1:S78.
8. Niehaus M, Tebbenjohanns J. Electromagnetic interference inpatients with implanted pacemakers or cardioverter-defibrilla-tors. Heart 2001;86:246–248.
9. Hurkmans CW, Scheepers E, Springorum BG, et al. Influenceof radiotherapy on the latest generation of implantable cardi-overter-defibrillators. Int J Radiat Oncol Biol Phys 2005;63:282–289.
10. Medtronic CRM Technical Services. Medtronic company liter-ature on radiation tolerance of their implantable cardiac pace-makers and implantable cardiac defibrillators. Minneapolis,MN: Medtronic; 2006.
11. St. Jude Medical Cardiac Rhythm Management Division.St. Jude company literature on radiation tolerance of theirimplantable cardiac pacemakers and implantable cardiac defi-brillators. Austin, TX: St. Jude; 2006.

Defibrillator care in radiation d D. Y. GELBLUM AND H. AMOLS 1531
12. Guidant Corporation, Cardiac Rhythm Management Technical
Services. Guidant company literature on radiation tolerance of
their implantable cardiac pacemakers and implantable cardiac
defibrillators. Indianapolis, IN: Guidant Corporation; 2006.13. Maisel WH, Moynahan M, Zuckerman BD, et al. Pacemaker
and ICD generator malfunctions: Analysis of Food and Drug
Administration reports. JAMA 2006;295:1901–1906.14. Maisel WH. Pacemaker and ICD generator reliability: Meta-
analysis of device registries. JAMA 2006;295:1929–1934.15. Solan AN, Solan MJ, Bednarz G, et al. Treatment of patients
with cardiac pacemakers and implantable cardioverter-defibril-
lators during radiotherapy. Int J Radiat Oncol Biol Phys 2004;
59:897–904.16. Thomas D, Becker R, Katus HA, et al. Radiation therapy-in-
duced electrical reset of an implantable cardioverter defibrillator
device located outside the irradiation field. J Electrocardiol
2004;37:73–74.
17. Hoecht S, Rosenthal P, Sancar D, et al. Implantable cardiac de-fibrillators may be damaged by radiation therapy. J Clin Oncol2002;20:2212–2213.
18. Nemec J. Runaway implantable defibrillator—A rare complica-tion of radiation therapy. Pace 2007;30:716–718.
19. Sepe S, Schaffer P, Krimmel K, et al. Irradiation treatment oflaryngeal cancer in a patient with an implantable cardioverter-defibrillator (ICD). Onkologie 2007;30:378–380.
20. Bradley PD, Normand E. Single event upset in implantable car-dioverter defibrillators. IEEE Trans Nuclear Sci 1998; 452929–2940.
21. Hall EJ, Martin SG, Amols H, et al. Photoneutrons from med-ical linear accelerators—Radiobiological measurements andrisk estimates. Int J Radiat Oncol Biol Phys 1995;33:225–230.
22. Uiterewaal GJ, Springorum BGF, Scheepers E, et al. Influenceof therapeutic irradiation on the latest generation of implantablecardioverter/defibrillators. Eurospace 2004;6(Suppl.):96.
23. JAMA Patient Page: Implantable cardioverter-defibrillators.JAMA 2006;295:1964.