impact of tooth replacement strategies on the nutritional status of partially-dentate elders
TRANSCRIPT

Or ig ina l a r t i c l e
Impact of tooth replacement strategies on the nutritionalstatus of partially-dentate elders
Gerald McKenna1, Patrick Finbarr Allen1, Albert Flynn2, Denis O’Mahony3, CristianeDaMata1, Michael Cronin4 and Noel Woods5
1Department of Restorative Dentistry, Cork University Dental School and Hospital, University College Cork, Cork, Ireland; 2School of Food and
Nutritional Sciences, University College Cork, Cork, Ireland; 3School of Medicine, University College Cork, Cork, Ireland; 4School of
Mathematical Sciences, University College Cork, Cork, Ireland; 5School of Policy Studies, University College Cork, Cork, Ireland
Gerodontology 2011; doi: 10.1111/j.1741-2358.2011.00579.x
Impact of tooth replacement strategies on the nutritional status of partially-dentate elders
Objective: To investigate the impact of tooth replacement on the nutritional status of partially dentate
older patients, and, to compare two different tooth replacement strategies; conventional treatment using
removable partial dentures and functionally orientated treatment based on the shortened dental arch.
Background: Amongst older patients, diet plays a key role in disease prevention, as poor diets have been
linked to numerous illnesses. Poor oral health and loss of teeth can have very significant negative effects on
dietary intake and nutritional status for elderly patients. There is evidence that good oral health generally,
has positive effects on the nutritional intake of older adults.
Materials and methods: A randomised, controlled clinical trial was designed to investigate the impact of
tooth replacement on the nutritional status of partially dentate elders. Forty-four patients aged over
65 years completed the trial, with 21 allocated to conventional treatment and 23 allocated to functionally
orientated treatment. Nutritional status was accessed at baseline and after treatment using the Mini
Nutritional Assessment (MNA) and a range of haematological markers.
Results: At baseline, relationships were observed between the number of occluding tooth contacts and
some measures of nutritional status. As the number of contacts increased, MNA scores (R = 0.16), in
addition to vitamin B12 (R = 0.21), serum folate (R = 0.32) and total lymphocyte count (R = 0.35), also
increased. After treatment intervention, the only measure of nutritional status that showed a statistically
significant improvement for both treatment groups was MNA score (p = 0.03). No significant between
group differences were observed from analysis of the haematological data.
Conclusion: In this study, prosthodontic rehabilitation with both conventional treatment and function-
ally orientated treatment resulted in an improvement in MNA score. Haematological markers did not
illustrate a clear picture of improvement in nutritional status for either treatment group.
Keywords: older patients, nutrition, partially dentate, removable dentures, shortened dental arch.
Accepted 4 August 2011
Introduction
Increasingly, it is accepted that there are interre-
lationships between oral health and general health,
particularly the chronic diseases of ageing1. As our
population continues to age, the importance of
understanding these interrelationships takes on
increased significance. Currently, the proportion of
adults over the age of 60 years is expanding rapidly
across European Union countries, including the
United Kingdom and the Republic of Ireland2. As
the older population has grown faster than the total
population, the proportion of older persons relative
to the rest of the population has increased consid-
erably. This trend will have wide ranging effects on
social, political and economic spheres as well as
presenting significant challenges for healthcare
delivery and public healthcare policy3.
From reviewing the current literature, it is
apparent that a number of oral diseases have risk
factors in common with systemic diseases such as
smoking, diet and glycaemic control4–6. However,
� 2011 The Gerodontology Society and John Wiley & Sons A/S 1

research has recently focused on possible bidirec-
tional relationships between oral diseases, particu-
larly inflammation of the periodontal tissues
(periodontal disease), and Cardiovascular Disease,
Diabetes Mellitus and Respiratory Disease.
Amongst older patients, diet also plays a key role
in disease prevention, as poor diets have been
linked to illnesses such as osteoporosis, athero-
sclerosis and bowel disease7. Although nutritional
state is influenced by factors such as age, socio-
economic status and general health, it would
appear that dental status is also significant. Poor
oral health and loss of teeth can have very signifi-
cant negative effects on dietary intake and nutri-
tional status for elderly patients8. As a result, the
American Dietetic Association9 recently stated that
oral health and nutrition have a synergistic bidi-
rectional relationship. There is evidence that good
oral health generally has very positive effects on
the nutritional intake of older adults10.
The aim of this study was to investigate the im-
pact of tooth replacement on the nutritional status
of partially dentate older patients, and, to compare
two different tooth replacement strategies. There
are currently no previously reported randomised
controlled clinical trials that compare the impact of
prosthodontic rehabilitation strategies on nutri-
tional status.
Materials and methods
Partially dentate patients attending Cork University
Dental Hospital seeking dental treatment were in-
vited to participate in the research study (Fig. 1).
Patients were included if they were aged 65 years
and older, had a minimum of six remaining natural
teeth in one arch, no evidence of dementia, were
able to have routine treatment in a dental chair and
could communicate in the English language. Par-
ticipants were each given an information sheet
detailing the proposed treatment options, and each
provided written informed consent. Patients were
randomly allocated to one of two treatment groups
using a random number generator stratified for age
and gender. Patient allocation was performed by a
member of staff not directly involved in the
research project.
Each patient received a detailed oral examination
with dental status recorded using the International
Caries Detection and Assessment System, Basic
Periodontal Examination, number of occluding
contacts, bleeding score and plaque score. Prior to
prosthodontic rehabilitation, all patients received
routine dental care as required including standar-
dised oral hygiene instruction, extraction of teeth
with a hopeless prognosis, periodontal treatment
and restoration of caries. Full ethical approval was
provided by the Cork University Teaching Hospitals
Ethics Committee.
Patients assigned to Group 1 (Conventional
treatment) had all missing natural teeth replaced
using a removable cobalt-chromium partial den-
ture (Fig. 2). Those assigned to Group 2 (Func-
tionally orientated treatment) were restored to 10
occluding tooth contacts using Resin Bonded
Bridgework (RBB) (Fig. 3). RBB was provided
using a standardised protocol that included mini-
Figure 1 Partially dentate female patient aged 74 years
before prosthodontic rehabilitation.
Figure 2 Sixty-seven-year-old female patient with
removable partial dentures replacing missing teeth (con-
ventional treatment).
Figure 3 Partially dentate patient aged 68 years reha-
bilitated using resin bonded bridgework (functionally
orientated treatment).
� 2011 The Gerodontology Society and John Wiley & Sons A/S
2 G. McKenna et al.

mal preparation of abutment teeth, adequate
thickness of retentive wings (minimum 0.7 mm),
chairside sandblasting of the bridgework and cemen-
tation using a composite resin cement (Panavia� F;
Kuraray Co. Ltd, Kita-Ku, Osaka, Japan).
Assessments of nutritional status were conducted
at baseline (prior to any prosthodontic rehabilita-
tion) and 1 month after treatment was completed.
Nutritional status was assessed using the Mini
Nutritional Assessment (MNA), which included
anthropometrical measurements in addition to a
global assessment, and using haematological bio-
markers. Blood samples were taken from patients
and analysed for a range of markers including a full
blood count, serum folate, vitamin B12, ferritin,
albumin and vitamin D.
Data were collated and entered using Microsoft
Excel (Microsoft� Office Excel 2000). At baseline,
correlations between the number of occluding
tooth contacts and nutritional status were analysed
using a Pearson’s Correlation Coefficient and a
Chi-squared Test. After prosthodontic rehabilita-
tion, pre-operative and post-operative nutritional
measures were compared using a Student’s T-test.
Data were analysed using SPSS� (SPSS, IBM
Corporation, Armonk, NY, USA) and statistical
significance was determined at p £ 0.05.
Results
Descriptive statistics
In total, 44 patients completed the trial in Cork
University Dental Hospital (Fig. 4). Eighty-six pa-
tients from were invited to participate in the study.
Sixteen patients did not meet the inclusion criteria
for the trial and were excluded, whereas 26 did not
complete the initial operative phase of treatment.
The patient pool consisted of 28 women and 16
men with an average age of 68.2 years (range
65–82 years). Twenty-one patients were allocated
to conventional treatment (Group 1) compared
with 23 who were allocated to functionally orien-
tated treatment (Group 2) (Table 1). All the mem-
bers of the conventional treatment group received
their allocated treatment; however, two patients
from the functionally orientated group refused their
allocated treatment and received conventional
treatment instead. These patients were analysed
according to the intention to treat principle.
Baseline findings
Within the sample of 44 patients, a range of 4–9
occluding contacts was recorded at baseline.
Occluding contacts were recorded where there was
contact between natural teeth in addition to nat-
ural teeth occluding against fixed or removable
prostheses that were not scheduled for replace-
ment.
Analysis of the haematological data illustrated
that as the number of occluding contacts increased,
there was a corresponding increase in levels of
vitamin B12, serum folate and total lymphocyte
count. The same relationships were not recorded
for serum ferritin, albumin or cholesterol.
For vitamin B12, all the samples recorded at
baseline were within the normal range (120–
650 ng/l). With an increase in occluding tooth
contacts, the levels of vitamin B12 also increased
giving an R value of 0.21 calculated using a Pear-
son’s correlation coefficient (Fig. 5). When the
results recorded for the minimum (four contacts)
and maximum number of occluding contacts (nine
contacts) were compared using a chi-squared test,
there was a highly statistically significant difference
(p < 0.001). Three patients were deficient in serum
folate at baseline (normal range 2.3–20 ng/l). As
the number of occluding contacts increased, serum
folate levels also increased with an R value of 0.32
recorded (Fig. 6). For serum folate, there was not a
statistically significant difference between the
results recorded for the minimum and maximum
number of occluding units (p = 0.82). A similar
relationship was found between number of
occluding contacts and total lymphocyte count. The
trendline illustrated that as the number of occlud-
ing contacts increased, the total lymphocyte count
also increased. An R value of 0.35 was calculated
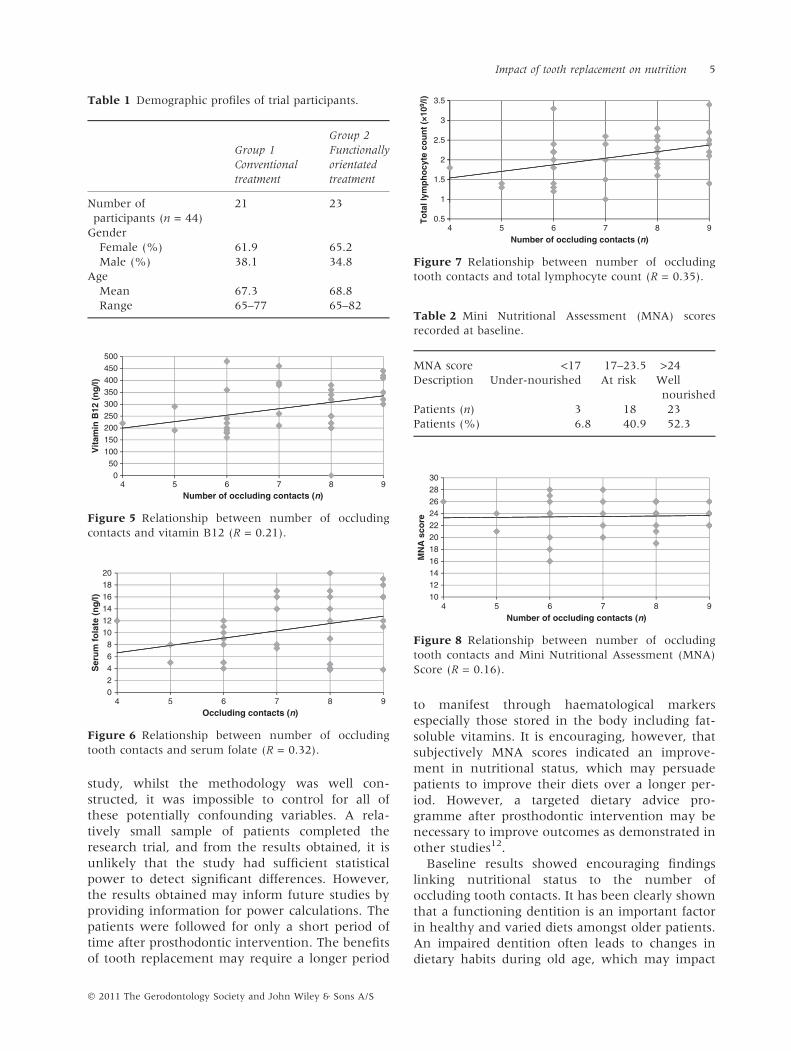
for this relationship with a p-value of 0.80 (Fig. 7).
At baseline, the MNA indicated that 52.3% of the
participants were ‘well nourished’, with 40.9% ‘at
risk of malnutrition’ and 6.8% ‘undernourished’
(Table 2). In general, it was found that as the
number of occluding contacts increased, the MNA
scores also improved with an R value of 0.16
recorded and a p-value of 0.84 (Fig. 8).
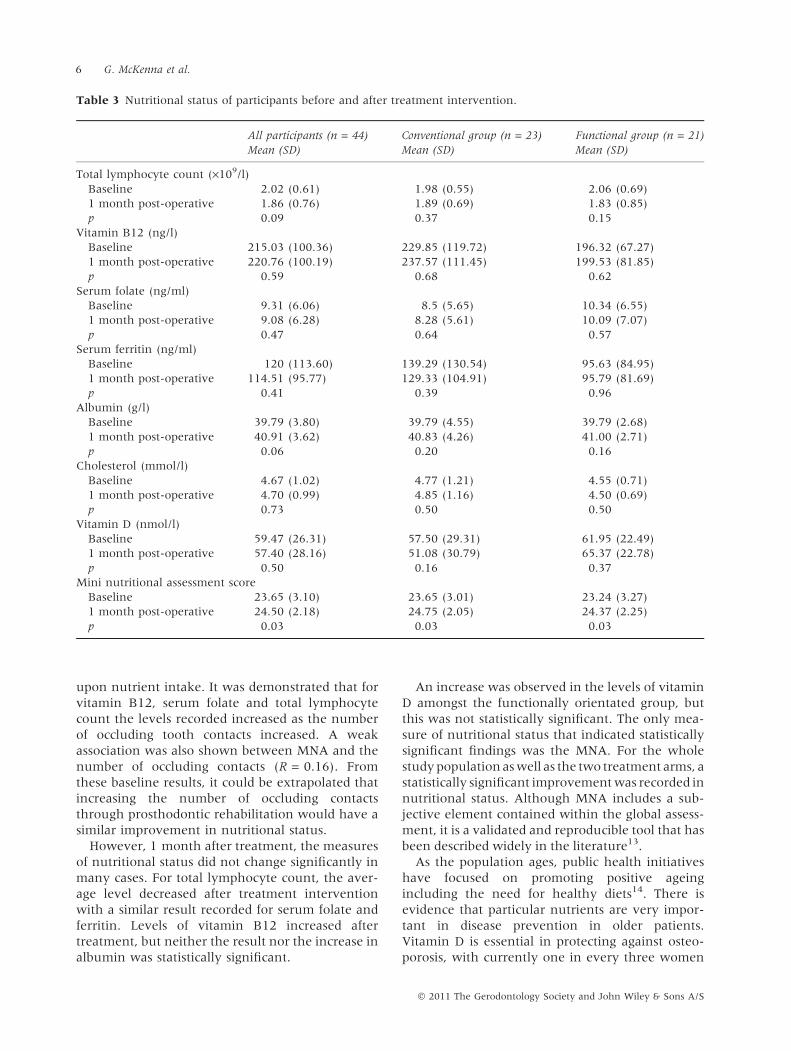
Findings after treatment intervention
One month after prosthodontic intervention, the
MNA and haematological samples were repeated
(Table 3). For total lymphocyte count, the average
level declined for all patients from 2.2 · 109/l at
baseline to 1.86 · 109/l, 1 month after treatment
intervention. For vitamin B12, the average result
increased from 215.03 to 220.76 ng/l. A larger in-
crease in average level was found in the con-
ventional treatment group (229.85–237.57 ng/l),
but the results were not statistically significant
� 2011 The Gerodontology Society and John Wiley & Sons A/S
Impact of tooth replacement on nutrition 3

(p = 0.68). For both serum folate and ferritin, the
levels decreased after treatment was completed, but
the results were not statistically significant for the
entire study population or the treatment sub-
groups. A decrease in the levels of vitamin D was
also recorded for the conventional treatment group
and for the entire study sample, but in the func-
tionally orientated group, average levels of vitamin
D increased from 61.95 nM at baseline to 65.37 nM
post-operatively (p = 0.37). For albumin, an in-
crease in levels was recorded for both intervention
groups, but neither result was statistically signifi-
cant. For cholesterol, the average level recorded
increased for the conventional group, but
decreased for the functionally orientated group
(from 4.55 to 4.50 mM).
For the MNA, the whole study population
recorded an average of 23.65 pre-operatively,
which increased to 24.50 after treatment inter-
vention (p = 0.03). A similar finding was recorded
for the conventional group where an average
baseline score of 23.65 increased to 24.75
(p = 0.03). For the functionally orientated group,
the average baseline score of 23.24 improved to
24.37 after treatment (p = 0.03). MNA was the
only measure that indicated a statistically signifi-
cant difference in nutritional status after treatment
intervention.
Discussion
Evidence suggests that nutritional status is a
multifactorial condition. Whilst dental status may
have a role to play, other factors including socio-
economic class, income levels and learned behav-
iour patterns are also very important11. In this
ExcludedNot meeting inclusion criteria (16)Declined to participate (26)
Randomised (44)stratified for:
AgeGender
Allocated to FUNCTIONAL TREATMENT(n = 23)
Received allocated treatment (n = 21)Did not receive allocated treatment (n = 2)2 Patients declined functional treatment. Received conventional treatment
1 month post treatmentLost to Follow Up (n = 0)
Treatment discontinued (n = 0)
Analysed (n = 23)Excluded from analysis (n = 0)
Treatment discontinued (n = 0)
Allocated to CONVENTIONAL TREATMENT (n = 21)
Received allocated treatment (n = 21)Did not receive allocated treatment (n = 0)
1 month post treatmentLost to Follow Up (n = 0)
Treatment discontinued (n = 0)
Analysed (n = 21)Excluded from analysis (n = 0)
Treatment discontinued (n = 0)
Enrollment
Allocation
Follow-Up
Analysis
Assessed for eligibility(n = 86)
Figure 4 Study flow diagram.
� 2011 The Gerodontology Society and John Wiley & Sons A/S
4 G. McKenna et al.
study, whilst the methodology was well con-
structed, it was impossible to control for all of
these potentially confounding variables. A rela-
tively small sample of patients completed the
research trial, and from the results obtained, it is
unlikely that the study had sufficient statistical
power to detect significant differences. However,
the results obtained may inform future studies by
providing information for power calculations. The
patients were followed for only a short period of
time after prosthodontic intervention. The benefits
of tooth replacement may require a longer period
to manifest through haematological markers
especially those stored in the body including fat-
soluble vitamins. It is encouraging, however, that
subjectively MNA scores indicated an improve-
ment in nutritional status, which may persuade
patients to improve their diets over a longer per-
iod. However, a targeted dietary advice pro-
gramme after prosthodontic intervention may be
necessary to improve outcomes as demonstrated in
other studies12.
Baseline results showed encouraging findings
linking nutritional status to the number of
occluding tooth contacts. It has been clearly shown
that a functioning dentition is an important factor
in healthy and varied diets amongst older patients.
An impaired dentition often leads to changes in
dietary habits during old age, which may impact
100
150
200
250
300
350
400
450
500
0
50
4 5 6 7 8 9
Vit
amin
B12
(n
g/l)
Number of occluding contacts (n)
Figure 5 Relationship between number of occluding
contacts and vitamin B12 (R = 0.21).
0
2
4
6
8
10
12
14
16
18
20
4 5 6 7 8 9
Ser
um
fo
late
(n
g/l)
Occluding contacts (n)
Figure 6 Relationship between number of occluding
tooth contacts and serum folate (R = 0.32).
0.5
1
1.5
2
2.5
3
3.5
4 5 6 7 8 9
To
tal l
ymp
ho
cyte
co
un
t (×
109 /
l)
Number of occluding contacts (n)
Figure 7 Relationship between number of occluding
tooth contacts and total lymphocyte count (R = 0.35).
Table 1 Demographic profiles of trial participants.
Group 1
Conventional
treatment
Group 2
Functionally
orientated
treatment
Number of
participants (n = 44)
21 23
Gender
Female (%) 61.9 65.2
Male (%) 38.1 34.8
Age
Mean 67.3 68.8
Range 65–77 65–82Table 2 Mini Nutritional Assessment (MNA) scores
recorded at baseline.
MNA score <17 17–23.5 >24
Description Under-nourished At risk Well
nourished
Patients (n) 3 18 23
Patients (%) 6.8 40.9 52.3
10
12
14
16
18
20
22
24
26
28
30
4 5 6 7 8 9
MN
A s
core
Number of occluding contacts (n)
Figure 8 Relationship between number of occluding
tooth contacts and Mini Nutritional Assessment (MNA)
Score (R = 0.16).
� 2011 The Gerodontology Society and John Wiley & Sons A/S
Impact of tooth replacement on nutrition 5
upon nutrient intake. It was demonstrated that for
vitamin B12, serum folate and total lymphocyte
count the levels recorded increased as the number
of occluding tooth contacts increased. A weak
association was also shown between MNA and the
number of occluding contacts (R = 0.16). From
these baseline results, it could be extrapolated that
increasing the number of occluding contacts
through prosthodontic rehabilitation would have a
similar improvement in nutritional status.
However, 1 month after treatment, the measures
of nutritional status did not change significantly in
many cases. For total lymphocyte count, the aver-
age level decreased after treatment intervention
with a similar result recorded for serum folate and
ferritin. Levels of vitamin B12 increased after
treatment, but neither the result nor the increase in
albumin was statistically significant.
An increase was observed in the levels of vitamin
D amongst the functionally orientated group, but
this was not statistically significant. The only mea-
sure of nutritional status that indicated statistically
significant findings was the MNA. For the whole
study population as well as the two treatment arms, a
statistically significant improvement was recorded in
nutritional status. Although MNA includes a sub-
jective element contained within the global assess-
ment, it is a validated and reproducible tool that has
been described widely in the literature13.
As the population ages, public health initiatives
have focused on promoting positive ageing
including the need for healthy diets14. There is
evidence that particular nutrients are very impor-
tant in disease prevention in older patients.
Vitamin D is essential in protecting against osteo-
porosis, with currently one in every three women
Table 3 Nutritional status of participants before and after treatment intervention.
All participants (n = 44)
Mean (SD)
Conventional group (n = 23)
Mean (SD)
Functional group (n = 21)
Mean (SD)
Total lymphocyte count (·109/l)
Baseline 2.02 (0.61) 1.98 (0.55) 2.06 (0.69)
1 month post-operative 1.86 (0.76) 1.89 (0.69) 1.83 (0.85)
p 0.09 0.37 0.15
Vitamin B12 (ng/l)
Baseline 215.03 (100.36) 229.85 (119.72) 196.32 (67.27)
1 month post-operative 220.76 (100.19) 237.57 (111.45) 199.53 (81.85)
p 0.59 0.68 0.62
Serum folate (ng/ml)
Baseline 9.31 (6.06) 8.5 (5.65) 10.34 (6.55)
1 month post-operative 9.08 (6.28) 8.28 (5.61) 10.09 (7.07)
p 0.47 0.64 0.57
Serum ferritin (ng/ml)
Baseline 120 (113.60) 139.29 (130.54) 95.63 (84.95)
1 month post-operative 114.51 (95.77) 129.33 (104.91) 95.79 (81.69)
p 0.41 0.39 0.96
Albumin (g/l)
Baseline 39.79 (3.80) 39.79 (4.55) 39.79 (2.68)
1 month post-operative 40.91 (3.62) 40.83 (4.26) 41.00 (2.71)
p 0.06 0.20 0.16
Cholesterol (mmol/l)
Baseline 4.67 (1.02) 4.77 (1.21) 4.55 (0.71)
1 month post-operative 4.70 (0.99) 4.85 (1.16) 4.50 (0.69)
p 0.73 0.50 0.50
Vitamin D (nmol/l)
Baseline 59.47 (26.31) 57.50 (29.31) 61.95 (22.49)
1 month post-operative 57.40 (28.16) 51.08 (30.79) 65.37 (22.78)
p 0.50 0.16 0.37
Mini nutritional assessment score
Baseline 23.65 (3.10) 23.65 (3.01) 23.24 (3.27)
1 month post-operative 24.50 (2.18) 24.75 (2.05) 24.37 (2.25)
p 0.03 0.03 0.03
� 2011 The Gerodontology Society and John Wiley & Sons A/S
6 G. McKenna et al.

and one in every 12 men aged 55 years and older
affected in the United Kingdom15. Studies from
around the world have clearly demonstrated that
poor vitamin D status is common amongst older
adults, particularly those from Northern Eur-
ope16,17. Amongst the study population reported in
this article, 74% of participants were deficient in
Vitamin D at baseline compared with 71% after
treatment intervention. There is also further
evidence that vitamin D may play an important
role in the prevention of osteoarthritis18.
Despite the rise of obesity throughout the general
population, malnutrition remains common in older
patients, particularly those living in nursing
homes19. In this study of free living older adults,
whilst only 6.8% of the population could be clas-
sified as ‘malnourished’ at baseline, a further
40.9% were classified as being ‘at risk of malnu-
trition’. As malnutrition represents a deficiency of
all nutrients, and not just the calories, this can be
accompanied by a range of health problems
including impaired immune response, poor wound
healing and an increased risk of hospital admis-
sions.
Dental health surveys indicate that the oral
health of our older population is improving with
more natural teeth retained into old age20. How-
ever, factors such as xerostomia, polypharmacy
and reduced manual dexterity can mean that
preservation of these teeth can be challenging.
Given these circumstances, it is important that
practitioners consider treatment options for par-
tially dentate older patients, which can be main-
tained without contributing to further dental
disease and tooth loss. Unfortunately, it has been
shown that removable partial dentures can in-
crease the potential for dental disease including
caries and periodontitis. As an alternative treat-
ment strategy, the shortened dental arch can pro-
vide a functional dentition without the need for a
removable prostheses21. Given the fact that the
change in nutritional status was broadly similar for
both treatment groups, the positive attributes of
the shortened dental arch should still encourage
practitioners to consider this strategy for partially
dentate elders.
Conclusions
Nutrition and diet are important factors in disease
prevention especially amongst the elderly popula-
tion. In this study, patients indicated that after
prosthodontic rehabilitation with either a conven-
tional or functionally orientated approach, their
nutritional status improved according to the MNA.
Apart from this measure of nutritional status,
which contains a subjective element, haematolog-
ical biomarkers did not demonstrate a clear picture
of improvement for either treatment group.
References
1. McKenna G, Allen PF, O’Mahony D et al. The
importance of oral health for the systemic well being
of an ageing population. Ir Med J 2009; 102: 202–204.
2. Fitzgerald J. Ireland – an Ageing Multicultural
Economy. Working Paper Number 157. Dublin, Ire-
land: The Economic and Social Research Institute,
2004.
3. United Nations Department of Economic and
Social Affairs, Population Division. World Popu-
lation Ageing: 1950–2050. New York: United Nations,
2002.
4. Jin LJ, Chiu GK, Corbett EF. Are periodontal dis-
eases risk factors for certain systemic disorders – what
matters to medical practitioners? Hong Kong Med J
2003; 9: 31–37.
5. Seymour RA. Does periodontal treatment improve
general health? Dent Update 2010; 37: 206–212.
6. Tonetti MS, D’Aiuto F, Maurizio S et al. Treat-
ment of periodontitis and endothelial function. N Engl
J Med 2007; 356: 911–920.
7. Moynihan PJ. The relationship between nutrition
and systemic and oral well-being in older people. J
Am Dent Assoc 2007; 138: 493–497.
8. Sheiham A, Steele JG, Marcenes W et al. The
relationship among dental status, nutrient intake, and
nutritional status in older people. J Dent Res 2001; 80:
408–413.
9. American Dietetic Association. Position of the
American Dietetic Association: Oral Health and
Nutrition. J Am Diet Assoc 2007; 107: 1418–1428.
10. Walls AW, Steele JG. The relationship between oral
health and nutrition in older people. Mech Ageing Dev
2004; 125: 853–857.
11. Steen B. Preventive nutrition in old age – a review. J
Nutr Health Aging 2000; 4: 114–119.
12. Bradbury J, Thomasson JM, Jepson NJ et al.
Nutrition counselling increases fruit and vegetable
intake in the edentulous. J Dent Res 2006; 85: 463–
468.
13. Bleda MJ, Bolibar I, Pares R et al. Reliability of the
mini nutritional assessment (MNA) in institutiona-
lised elderly people. J Nutr Health Aging 2002; 6: 134–
137.
14. British Nutrition Foundation. Healthy Ageing: The
Role of Nutrition and Lifestyle. London: Wiley, 2009.
15. Cooper C. Bone mass, muscle function and fracture of
the proximal femur. Br J Hosp Med 1989; 42: 277–280.
16. Hill TR, Flynn A, Kiely M et al. Prevalence of
suboptimal vitamin D status in young, adult and
elderly Irish subjects. Ir Med J 2006; 99: 48–49.
17. Cashman KD, Wallace JM, Horigan G et al. Esti-
mation of the daily requirement for vitamin D in free
� 2011 The Gerodontology Society and John Wiley & Sons A/S
Impact of tooth replacement on nutrition 7

living adults >64 years. Am J Clin Nutr 2009; 89:
1366–1374.
18. Heidari B, Heidari P, Hajian-Tilaki K. Association
between serum vitamin D deficiency and knee
osteoarthritis. Int Orthop 2011; 35: 1627–1631.
19. Smoliner C, Norman K, Wagner KH et al. Mal-
nutrition and depression in the institutionalised
elderly. Br J Nutr 2009; 102: 1663–1667.
20. Whelton H, O’Mullane D, Woods N et al. Oral
Health of Irish Adults 2000–2002. Dublin: Department
of Health and Children, 2007.
21. Kayser AF. Shortened dental arches and oral func-
tion. J Oral Rehabil 1981; 8: 457–462.
Correspondence to:
Gerald McKenna, Department of Restorative
Dentistry, Cork University Dental School and
Hospital, University College Cork, Cork, Ireland.Tel.: +353 021 420 5033
Fax: +353 021 490 1193
E-mail: [email protected]
� 2011 The Gerodontology Society and John Wiley & Sons A/S
8 G. McKenna et al.