immunohistochemical localization and correlation of p53 and...
TRANSCRIPT

Indian Journal of Experimental Biology Vol. 38, March 2000, pp. 225-230
Immunohistochemical localization and correlation of p53 and PCNA expression in breast carcinoma
M M Goel, Rashmi Goel, Anju Mehrotra, Pramod Nath, P K Agarwal, Kamlesh Singh* & Raj Mehrotra
Department of Pathology, King George's Medical College, Lucknow 226 003 , India
Received 22 March /999; revised 27 October /999
The object of the present study is to detect the ·p53 tumour suppressor gene and proliferation cell nuclear antigen (PCNA) expression in breast carcinoma by immunohistochemistry and correlate them with the prognostic parameters.Total 35 cases of primary breast carcinoma were studied and classified histologically. Paraffin sections were stained by using monoclonal antibody 007 for p53 protein and PC- lO for PCNA. Out of 35 cases, 16 (45.7%) were p53 positive and 25 (71.4%) were PCNA positive. The mean PCNA labelling index (PCNA LI ± SO) was 58.97 ± 22.72 in tumors positive for both p53+ and PCNA+ while cases negative for p53- and positive for PCNA+ has higher PCNA LI ± SO (59.24 ± 18.97). The difference in the two groups was not significant. Most cases were positive for both p53+ and PCNA+ in the age group < 30 with higher mean PCNA LI±SO (62.2D±27.l3) than in the group> 30 (57.88±18.47). In the pre-menopausal group 57;1 % cases were positive for p53+ with bigher PCNA LI ± SO (59.94±24.22). Maximum p53 and PCNA positivity was observed in grade III tumors (63.2% and 84.2%). The mean PCNA LI ± SO was also highest in grade III carcinomas (66.83±i3.97). No significant correlation was found between p53 and PCNA status with morphological type and tumour size except that logistic regression showed a positive correlation with tumour grade. Therefore the present study suggests that both p53 expression and PCNA are markers of poor differentiation in breast cancer.
Breast cancer is one of the most common cancers among women. Metastatic breast cancer is an incurable disease. Efforts are made to decrease breast cancer mortality by an early detection and an improved treatment. Identification and analysis of a specific genetic susceptibility could permit detection of susceptible women and greatly increase the understanding of the initial step that eventually leads to cancer.
In past few years, most decisions concerning the prognosis and management of breast cancer patients were made on the basis of traditional factors such as tumour size, histological grading, nodal status and histopathological features)-3. However, prognostic factors are being investigated that could identify high risk groups so better treatment can be provided to these patients.
Identification of more accurate prognostic markers, such as expression of mutant p53 protein encoded by the p53 tumour suppressor gene and PCNA that are reproducible, easily assessible and .independent . in predicting clinical outcome would have a beneficial impact on cancer treatment decisions. Therefore the present study was planned to detect overexpression of p53 tumour suppressor gene and PCNA in reported cases of breast cancer by immunohistochemical methods and correlate them with the prognosis of
breast cancer.
Materials and Methods This study was c.onducted on 35 cases of primary
breast carcinoma. These cases were the mastectomy specimens fixed in 10% formalin, received for routine surgical pathology in histopathology laboratory of the King George's Medical College, Lucknow. The available clinical data of the cases were recorded. A meticulous examination of the gross specimen was done. Multiple sections were taken from the tumour area and the axillary lymph nodes. After routine processing and paraffin embedding several sections of 3-4 11m thickness were cut from each case. The sections were stained with haematoxylin and eosin and examined for histological diagnosis.
The .tumours were graded according to the grading system by Bloom and Richardson4 based on ]-3 scoring of tubule formation, nuclear pleomorphism and mitotic counts. Scores of each category were added together and grades were allocated as follows: Tubule formation (l point; tubule formation in majority of the areas, 2 points; moderate degree of tubule formation, 3 points; only mild degree of tubule formation), Nuclear pleomorphism (l point; only mild degree ?f pleomorphism, 2 points; moderate de-
226 INDIAN J EXP BIOL, MARCH 2000
gree of pleomorphism, 3 points; severe degree of pleomorphism), Mitotic counts (Score 1; <1 mitotic figure/ HPF, score 2; 1-2 mitotic figures/ HPF, score 3; >2 mitotic figures/HPF). To obtain the tumor grade, the scores of each category were added together and the grade allocated as follows:
3-5 points : Grade I (well differentiated) 6-7 points : Grade II (Moderately differentiated) 8-9 points : Grade III (poorly differentiated)
Stainingfor P53 protein and PCNA Staining for p53 protein and PCNA was carried
out using monoclonal antibody D07 and PC10 (Novacastra Lab, New Castle, U.K.). Monoclonal antibody PC-10 recognizes tissue fixation and processing-resistant epitope of PCNAs. The antibodies (prediluted 1 :50) were purchased from Histopan (Surat, India). All immu'nohistochemical stainings were done by Streptavidin - Biotin method.
The immunostaining was done as per the manufacturer's instructions in the Histospan Kit. The sections were incubated with the -primary antibody for two hours at 37°C. Positive staining was identified as a brown coloured reaction product. The positivity of the PS3 was graded into three categories: <10%, 10-50% arid >50% after scanning the entire slide6
.
Positive and negative controls for p53 immunohistochemical staining
Paraffin embedded sections of a case of Hodgkin's lymphoma (Lymphocytic depletion type), known to be positive for p53 mutations by molecular hybrid i- _ zation, were used as positive control for all staining batches and sections from a case of primary breast carcinoma, known to be positive for p53, stained with negative control antibody (1 % Non-immune serum) was used as negative control.
Positive and negative controls for PCNA immunohistochemical staining
Positive control : PCNA positivity is considered to be high in actively proliferating cells in the body e.g. intestinal villi, tongue and germinal centres of the lymph node. Thin paraffin embedded sections of the base of tongue were utilised as a positive control for PCNA staining in all batches. The basal cells of the stratified squamous lining, which have a high proliferation rate, gave a positive brown reaction product in their nuclei as well as in the cytoplasm. The mature non dividing cells of the superficial epithelium were
stained negatively. Negative control: A case of breast carcinoma,
known to be positive for PCNA, was stained with negative control antibody (l % non-immune serum). No brown coloured staining was produced in any of the cells.
Calculation of PCNA labelling index 1000 cells were counted in the tumour section and
the PCNA labelling index calculated as follows:
No. of cells showing positive staining peNAL! xlOO
Total No. of tumour cells counted
Statistical analysis All the observations were pooled and statistical
analysis was done to find out the correlations between p53 and PCNA status with other prognostic variabJes. Student's t test was done to find out .correlations of various parameters with PCNA LJ and the Chi square test was used to test the significance of the correlations of P53 positivity with various parameters in this univariate analysis. If the P value was 0.05 or less, it was considered to be significant. Multiple logistic regression was done using "MULTLR" software at Department . of Clinical Epidemiology Unit, K.G.M.C., Lucknow.
Results The present study was conducted in 35 cases of
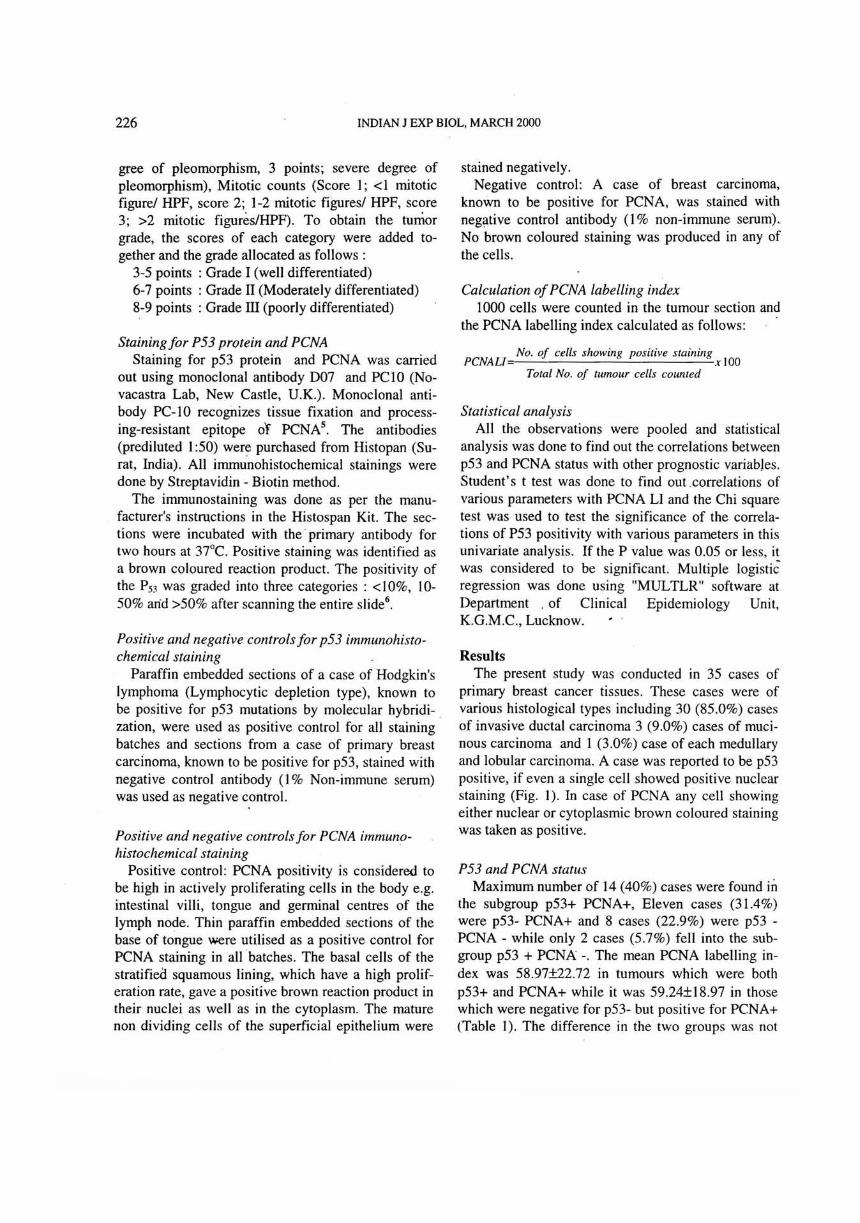
primary breast cancer tissues. These cases were of various histological types including 30 (85.0%) cases of invasive ductal carcinoma 3 (9.0%) cases of mucinous carcinoma and 1 (3.0%) case of each medullary and lobular carcinoma. A case was reported to be p53 positive, if even a single cell showed positive nuclear staining (Fig. 1). In case of PCNA any cell showing either nuclear or cytoplasmic brown coloured staining was taken as positive.
P53 and PCNA status Maximum number of 14 (40%) cases were found in
the subgroup p53+ PCNA+, Eleven cases (31.4%) were p53- PCNA+ and 8 cases (22.9%) were p53 -PCNA - while only 2 cases (5.7%) fell into the subgroup p53 + PCNA -. The mean PCNA labelling index was 58.97±22.72 in tumours which were both p53+ and PCNA+ while it was 59.24±18.97 in those which were negative for p53- but positive for PCNA+ (Table I). The difference in the two groups was not

GOEL et al.: P53 & PCNA IN BREAST CARCINOMA 227
significant.
p53 and PCNA status and patient's age The findings of p53 and PCNA status with differ
ent prognostic factors are given in Table 2. The patients were divided' into two age groups,
those below and those above 30 years of age. 8 cases (23%) belonged to the former .group while 27 (77%) were of the latter. A higher number of cases were positive for both p53 and PCNA in the age group < 30 years and the mean PCNA LI was also higher in this group (62.20±27.13) than in the group> 30 years. The difference however, was not statistically significant in any of the variables.
p53 and PCNA status and menopausal status Twenty one, out of the 35 cases studied (60%)
were premenopausal while the rest 14 (40%) were postmenopausal. A higher number of cases were positive for p53 in the pre-menopausal group
Fig. I-Histological section from a poorly differentiated carcinoma of breast showing positive immunostaining (dark brown) for p53 (500x).
(57.1 %). The mean PCNA LI was also higher in this group (59.94±24.22). The difference however was not significant in any of the cases.
p53 and PCNA status and tumour size Five cases (14%) had tumour size <2 cm, 7 cases
(20%) had tumour of 2.1 - 5 cm size and 23 (66%) cases had tumour of >5 cm size. No significant correlation was found between p53 and PCNA positivity and tumour size.
p53 and PCNA status and axillary lymph node status Eight, out of the 35 cases studied (23%) were
lymph node negative. Three cases (35.3%) were p53 positive in this group and 6 cases (77.8%) were PCNA positive with a mean PCNA labelling index of 65.63 ± 13.28. Twenty seven cases (77%) were lymph node positive with varying number of lymph nodes involved. A higher number of cases were positive for both p53 and PCNA in the lymph node positive group. The mean PCNA LI was also higher in this group 73.88±11 .06. The difference however, was not significant.
p53 and PCNA status and histological type No significant correlation was found between the
p53 and PCNA status with morphological t)IPe of tumors.
p53 and PCNA status and histological grade Of the 35 cases studied, 7 were diagnosed as grade
I (20%), 9 as grade II (26%) and 19 as grade III (54%). Maximum p53 and PCNA positivity was observed in grade III carcinomas (63.2% and 84.2%). The mean PCNA LI was also highest in grade III carcinomas (66.83 ± 13.97). A significant correlation was found between the status of p53 and PCNA positivity and histological grade.
Multiple logistic regression The logistic regression (Table 3) did not show sig-
Table I-Combined p53 and PCNA positivity in breast cancer
Tumour status No. of cases (%)
pS3 +PCNA+ p53 + PCNAp53 -PCNA+ p53 -PCNA-
P<O.l
14 (40,0) 2 (5.7)
II (31.4) 8 (22.9)
Mean PCNA LI ± SD
58.97 ± 22.72
59.24 ± 18.97

228 INDIAN J EXP BIOL, MARCH 2000
nificant correlation of P53 positivity with age, menopausal status, tumour size, number of lymph nodes and histological types except a positive correlation with tumour grade indicating P53, a marker of poor differentiation .
Discussion The magnitude of breast cancer problem highlights
the need to determine the best possible predictors of prognosis so that appropriate therapy can be selected for women suffering from this common and dreaded disease.
Alterations of p53 have been found to be the most common genetic anomaly involved in breast cancer. In the present study, 45.7% cases of breast cancer were found to be p53 positive. This was quite close to the previous observations of 42.5%7, 52%8 and 53%9. In contrast few authors lO
•12 have reported very low
positivity of 19% and 24.8%. This variability in the results may be attributed to the diversity of procedures and reagents used by different investigators. Significant differences have been reported 13 in the p53 immunoreactivity depending upon the antibody
used. In this study, we used the monoclonal antibody 007. However a number of workers l4
•15 have ac
cepted that antibody Pab 1801 work more efficiently on paraffin embedded sections in comparison to the other antibodies.
Another important difference among the reported studies was the lack of a standardized immunohistochemical criteria to classify a carcinoma as p53 positive. Davidoff et al.2 classified those tumours as posi-
Table 3--Correlation ofP53 positivity with different prognostic parameters by multiple logistic regression
Parameters Coeffi-cient
Age -1.317 Menopausal -0.775 status Tumour size -0.1841 No. of lymph 0.1508 nodes Histological 1.0906 grades
Odds ratio (95% confidence
interval)
0.268 (0.04, 1.9) 0.461 (0.09,2.3)
0.832 (0.47, 1.48) 1.163 (0.69, 1.96)
2.976 (1.004, 8.83)
P value
0.1876 0.349
0.531 0.569
0.049
Table 2--Correlation of p53 and PCNA positi vity with different prognostic factors
Prognostic parameter No. of p53 positivity (%) PCNA positivity MeanPCNA cases (%) (%) U±SD
Gr. I Gr.II Gr.III Age (Years) <30 8 (23.0) 1 4 I 6 (75.0) 7 (87.5) 62.20 ± 27.13 > 30 27 (77.0) 2 5 3 10 (37.0) 18 (66.7) 57.88 ± 18.47
P= 0.07 P=0.71 Menopausal Pre 21 (60.0) 2 8 2 12 (57.1) 14 (66.7) 59.94 ± 24.22 Post 14 (40.0) 2 4 (28.6) II (78 .6) 58.00 ± 16.32
P = 0.19 P=0.81 Tumour size <2 5 (14.0) I 1 1 3 (60.0) 4 (80.0) 68.97 ± 9.71
2.1 - 5 7 (20.0) 0 2 I 3 (42.9) 5 (71.4) 51.68 ± 30.64 >5 23 (66.0) 2 6 2 10 (43.5) 16 (69 .6) 58.93 ± 19.33
P= 0.78 P == 0.48 No. of positive lymph nodes 0 8 (23.0) I 3 (35.3) 6 (77.8) 65.63 ± 13.28 I - 3 3 (9.0) 0 2 0 2 (66.6) 3 (100.0) 73.88 ± 11.06 4 24 (68.0) 2 6 3 11 (46.0) 16 (65.2) 53.87 ± 28.86
P=0.69 P = 0.215 Hi stological grade 1 7 (20.0) 0 I 0 1 (14.3) 5 (71.4) 43.28 ± 30.68 II 9 (26.0) 2 1 0 3 (33.3) 4 (44.4) 47.88 ± 17.39 III 19 (54.0) J 7 4 12 (63 .2) 16 (84.2) 66.83 ± 13 .97
P = 0.05 P=0.035

GOEL et al.: P53 & PCNA IN BREAST CARCINOMA 229
tive that showed intense nuclear staining throughout malignant epithelium, while other workers showed l6
at least 10% of the nuclei to be reactive for p53. Those cases were taken as positive in which more than 5% nuclei showed immunoreactiviti 4
• A carcinoma was considered to be positive if any cell showed nuclear staining8.1"'. In this study, we considered a case positive if even a single cell had positive nuclear staining. In our results 45.7% cases were positive, which was consistent with the findings of the above investigators using the same criteria.
No significant correlation of p53 and peNA positivity was found with the age of the patients which was consistent with the results of other investigators I5
•18
. Most groups have found no significant correlation of p53 overexpression with the menopausal
1419 Th d . h .. status '. e ata In t e present senes are In agree-ment with them. On the contrary, Friedrichs et al. 3
observed a significantly higher positivity in the premenopausal than in the postmenopausal group.
Our findings supported the views of other workers ll
,I9 that tumor size was not correlated with the p53 positivity .. However, a high p53 positivity with an increasing tumour size has been r~ported by some workers20
. The axillary lymph node status is generally considered to be the most important predictor of prognosis in breast cancer but, almost all studies have failed to demonstrate any associatIOn between the nodal status and p53 1
1.19. Our study also depicts similar findings .
A few histological types of breast cancer e.g. mucinous, medullary and tubular types have a better prognosis than the more common invasive ductal carcinoma, not otherwise specified (NOS) type. However, most investigators have found a higher immunoreactivity in the medullary carcinomas than in the invasive ductal carcinoma NOS type and very low positivity in the mucinous type l5
. Our findings are also consistent with them.
Majority of the studies 11 .15.21 have demonstrated a positive correlation between p53 overexpression and poor histological grade of the tumour. We have also obtained similar results based on multiple logistic regression. A significant positive correlation, was found between the increasing peNA LI and a poor histological grade. These observation were consistent with the findings of most other investigators22
•23
•
However, our conclusion could not be drawn in the case of histological type because of an unequal distribution of the cases.
Overexpression of p53 has been found to be associated with early disease recurrence and decreased overall survival rates24
. peNA has also been shown to have a poor prognostic value25
•26
. In most of the studies, no correlation of peNA could be found with the recurrence free survival or the overall survivaf2
•23
• No conclusions could be drawn regarding the role of p53 and peNA in the overall prognosis of breast cancer of a short interval between the time of presentation by the patient and the study undertaken.
Management of patients with breast cancer requires an individualized approach that is based on a careful weighing of a variety of prognostic consideration. The relative importance of these factors will require further large scale prospective multiparameteric studies. Although results from such studies are awaited, an understanding of the clinical heterogeneity of breast cancer must be based on a mUltiplicity of observations, each of which characterizes in a limited way, the biology of the disease. Therefore present study suggests that both p53 overexpression and peNA are markers of poor differentiation in breast cancer. But, whether p53 expression or peNA will carry predictive power independent of the more traditional variables awaits accumulation of large series with adequate follow up.
References I Caleffi M, Teague M W, Jensen R A & Vnencak Jones C L,
P53 gene mutations and steroid receptor status in breast cancer. Clinicopathologic correlations and prognostic assessment. Cancer, 73 (1994) 2147.
2 Davidoff A M, Herndon J E'. Glover N S, Kerns B J, Pence J C, Iglehart J D & Marks J R, Relation between P53 overexpression and established prognostic factors in breast cancer. Surgery, 110(2) (1991) 259.
3 Freidrichs K, Gluba S. Eidtmann H & Jonal W, OVf:rexpression of P53 and prognosis in breast cancer. Cancer, 72 (1993) 3641.
4 Bloom H J G & Richardson W W, Histological grading and prognosis in breast cancer, Br J Cancer, II (1957) 359.
5 Waseem N H & Lane D P, Monoclonal antibody analysis of the proliferatoin cell nuclear antigen (PCNA) structural conservation and detection of a nucleolar form, J Cell Sci. 26 (1990) 121.
6 Ming Tee, Aileen Wee & Gangaraju C R, An immunohistochemical study of PS3 protein in gall bladder and extra hepatic bile duct/ampullary carcinoma, Cancer, 74(5) (1994) 1543.
7 Poller D N, Hutchings C E & Galea M, P53 protein e~pression in human breast carcinoma. Relationship to expression of epidermal growth factor receptor, C-erb-2 protein overexpression and oesotrogen receptor, BI' J Cancer, 66 (1992) 583.
•

230 INDIAN 1 EXP BIOL, MARCH 2000
8 Allred D C, Clark G M & Elledge R, Association of P53 protein expression with tumor cell proliferation rate and clinical outcome in node negative hreast cancer, J NaIL Cancer IIISI, 85 (1993) 200.
9 Horak E, Smith K, Bromley L, Lejeune S, Greenall M & Lane D, Mutant PSJ , EGF receptor and C-erb B-2 expression in human breast cancer, Ollcogelle, 6 (1991) 2277.
10 Barnes D M, Dublin E A, Fisher C 1, Levison D A & Millis R R, Immunohistochemical detection of P53 protein in mammary carcinoma: An important new independent indicator of prognosis, Human Palhol, 24(5) (1993) 469.
II Rosanelli G P, Steindorfer P, Wirnsberger G H & Klimpfinger M, Ratschek Mutant P53 expression and DNA analysis in human breast cancer comparison with conventional clinicopathological parameters, Anticancer Res, 15(2) (1995) 581.
12 Hanzel E, Gitsch G, Koulberger F, Dadak C & Miechowiecka B G, Immunohistochemical detection of mutant P53 suppressor gene product patients with breast cancer influence on metastasis free survival, Anlicancer Res, 12(68) (1992) 2325 .
13 Cattoretti G, Rilke F, Andreola S, D'Amato L & Delia D, po.l expression in breast cancer, Inl J Cancer, 41 (1988) 178.
14 Silvestrini R, Benini E & Daidone M G, P03 as an independent prognostic marker in lymph node - negative breast cancer patients, J Noll Cancer Insl, 85 (1993) 965.
15 Rosen P P, Lesser M L & Arroyo C D, PS3 in node negative breast carcinoma: An immunohistochemical study of epidemiologic risk factors , histologic features, and prognosis, J Clin Oncol, 13 (1995) 821.
16 Barbareschi M, Leonardi E, Mauri F A, Serio G & Palma P D, Po3 and C-erb 8-2 protein expression in breast carcinoma. An immunohistochemical study including correlations with receptor status, proliferation markers and clinical stage in human breast cancer, Am J Clin Palhol, 98 (1992) 408.
17 Thor A D, Moore D H & Edgerton S M, Accumulation of P53
tumor suppressor gene protein : An independent marker of prognosis in breast cancers, J Noll Cancer Insl, 84 (1992) 845.
18 Anelli A, Anelli T F, Youngson B, Rosen P P & Borgen P I, Mutations of po) gene in male breast cancer, Cancer, 75 (1995) 2233.
19 Bhargava V, Thor A & Deng G, The association of P53 immunopositivity with tumor proliferation and other prognostic indicators in breast cancer, Mod Palhol, 7 (1994) 361.
20 Stenmark A M, Stal 0 & Sullivan S, Cellular accumulation of P53 protein: An independent prognostic factor in stage II breast cancer, ElIr J Cancer, 30A (1994) 175.
21 Sasa M, Kondo K, Komaki K, Morimoto T & Monden Y, PS3 alterations correlates with negative ER, negative PgR and high histologic grade in breast cancer, J Surg On col, 56 (1994) 46.
22 Schonborn I, Zschiesche W, Minguillon C, Spitzer E, Mohner M, Ebeling K & Grosse R, Prognostic value of proliferating cell nuclear antigen and C-erb-2 compared with conventional histopathological factors in breast cancer, J Cancer Res Clin On col, 121 (1995) 115.
23 Cummings M C, Furnival C M, Parsons P G & Townsend E, PCNA immunostaining in breast cancer, Ausl NZJ Surg , 63 (1993) 630.
24 Stenmark A M, Stal 0, Oslen K & Nordenskjold B, PS3 as a prognostic factor in stage 1 breast cancer. South East Sweden breast cancer group, Br J Cancer, 72 (1995) 715.
25 Aaltomaa S, Lipponcr . Papinaho S & Syrjanen K, Proliferating cell nuclear antIgen (PC 1 0) immunolabelling and other proliferation indices as prognostic factors in breast cancer, Cancer Res Clin Oil col, 119 (1993) 288 .
26 Tahan S R, Neuberg D S, Dieffenhach A & Yacoub L, Prediction of early relapse and shortened survival in patients with breast cancer by proliferating cell nuclear antigen score, Cancer, 71 (1993) 3552.