immunoblastic sarcoma arising in child with immunoblastic lymphadenopathy
TRANSCRIPT

747
IMMUNOBLASTIC SARCOMA ARISING IN CHILDWITH IMMUNOBLASTIC LYMPHADENOPATHY
SIR,-Nearly all previous cases of immunoblastic lympha-denopathy’ or angioimmunoblastic lymphadenopathy2-4 haveoccurred in adults beyond middle age; the disease has not pre-viously been reported in children. We have seen a child withthe features of immunoblastic lymphadenopathy which
apparently has progressed to immunoblastic sarcoma.The patient, a 7-year-old boy, had over the preceding 6
months developed a persistent cough, episodes of abdominalpain, and, lately, generalised lymphadenopathy with fever andweight loss. During the next 2-3 weeks his liver and spleen alsobecame palpable. His Hb was 7.8 8 g/dl, white blood-cells80xl0"/l (neutrophils 72%, lymphocytes 21%, monocytes4%), and erythrocyte-sedimentation rate 65 mm in the firsthour. Liver enzymes were normal, but IgG (20-35 g/1), IgA(5-6 g/1), and IgM (4-16 g/1) were persistently raised. A skele-tal survey, catecholamine excretion level, and bone-marrowexamination were normal. Bacteriological and virological stu-dies and serological tests for connective-tissue disorders werenegative. On several occasions analysis of his peripheral-bloodlymphocytes showed severe reduction of T cells.
As the child’s condition was deteriorating rapidly, biopsy ofthe largest cervical lymph-node was done. The histologicalappearances corresponded to descriptions of immunoblasticlymphadenopathy: the normal cortex was atrophied and theinterfollicular and paracortical areas were expanded by a cellu-lar infiltrate which included lymphocytes, plasma cells, andnumerous large immunoblastic cells of variable size with vesi-cular nuclei, prominent nucleoli and intensely pyroninophiliccytoplasm (fig. 1); a deposit of amorphous pale-stainingmaterial separated many cells. There were no Reed-Sternberg
1. Lukes, R. J., Tindle, B. H. New Engl J. Med. 1975, 292, 1.2. Frizzera, G., Moran, E. M. Rappaport, H, Lancet, 1974, i, 1070.3. Frizzera, G., Moran, E. M., Rappaport, H. Am. J. Med. 1975, 59, 803.4. Lancet, 1975, i, 260.
1",<<. 1--Cervical lymph-node: lmmmunoblastic cells with vesicular nuclei,Prominent nucleoli and pyroninophuic cytoplasm.I-’ght microscope x 400.)
Fig. 2-Cervical lymph-node: tilvef imprepation showinø arborisingvascular proliferation.
(Light microscope x 400.)
cells, and only an occasional polymorph and eosinophil wereseen. A striking feature, however, was the proliferation ofsmall blood-vessels assuming an arborising appearance in
places (fig. 2). Because this condition had not previously beenreported in a child we referred the sections to Dr R. J. Lukesat the University of Southern California, who confirmed ourdiagnosis and suggested that in addition the monomorphiccharacter of the immunoblastic proliferation in places was con-sistent with the development of immunoblastic sarcoma (fig.1).He responded well to treatment with prednisolone (40
mg/m2) and vincristine (1.5 mg/m2) with dramatic reductionin the size of his lymph-nodes and abolition of the fever within24 h. When after 2 weeks the chemotherapy was discontinuedthe symptoms recurred within 7 days but the same dramaticimprovement was seen immediately on re-starting chemo-therapy. The immunoglobulin levels returned to normallevels within 2 weeks of commencing chemotherapy.We were hesitant initially to accept the diagnosis of im-
munoblastic lymphadenopathy because of the age of our
patient. In Dr Lukes’ series the youngest patient was 28 yearsold and the median age was 57 years and in the series reportedby Rappaport and his colleagues3 the age ranged from 44 to80 years with a median of 68.
Cervical lymph-node biopsy had been done in another hospi-tal several months earlier and reported as "fibroblastic changessuggestive of persistent infection"; review of this biopsymaterial revealed features of immunoblastic lymphadenopathywithout sarcomatous transformation. This together with thepersistence of areas of immunoblastic lymphadenopathy in thesecond biopsy specimen suggested that the sarcoma hadevolved in lymph-nodes previously affected by immunoblasticlymphadenopathy. Immunoblastic sarcoma was described asthe preterminal event in 3 of the 28 cases described by Lukesbut was not recorded in any of the 24 cases reported by Rappa-port’s group.3 Immunoblastic sarcomas have also been des-cribed in abnormal immunological states such as rheumatoidarthritis, systemic lupus erythematosus,6 Sjogren’s syn-drome and senescence. It seems that the defective immunolo-gical status in these conditions somehow predisposes to sarco-matous transformation.
It has been suggested that immunoblastic lymphadenopathyitself is not a neoplastic disorder but a hyperimmune conditionof B cells arising in an abnormal reactor.’ Our patient had no
5. Lukes, R. J., Collins, R. D. Cancer, 1974, 34, 1488.6. Miller, D. G. Ann. intern. Med. 1967, 66, 507.7. Anderson, L. G., Talal, N. Clin. exp. Immun., 1972, 10, 199.
748
previous history of hypersensitivity and there was no familyhistory suggestive of any immunological or connective-tissuedisorder. In the 6 months immediately preceding the develop-ment of lymphadenopathy his only drug therapy had been dia-zepam, ’Phensedyl’ (promethazine hydrochloride, codeinephosphate, and ephedrine hydrochloride), and amitriptylinefor persistent cough.The therapeutic management of immunoblastic lympha-
denopathy is not well established. Previous studies suggest theuse of low doses of cytotoxic drugs so that the alreadydiminished resistance of the patient to infection2 is not furthercompromised. At first our patient responded well to a com-bination of vincristine and prednisolone, but within 3 monthsthere was evidence of tumour recurrence. Despite increasedcytotoxic therapy he died with widespread disease, 13 monthsafter initial presentation.
Pædiatric Oncology Clinic,Seacroft Hospital,Leeds LS14 6UH CATHRYN B. HOWARTH
Department of Pathology,School of Medicine,Leeds LS2 9NL C. C. BIRD
PLASMAPHERESIS AND IMMUNOLOGICALCONTROL OF CANCER
SIR,-We read with interest reports by Dr Brown (July 10,p. 96) and Professor Israel (Sept. 18, p. 642) and their col-leagues on the usefulness of plasmapheresis in reversing the im-muno-depression seen in patients with advanced cancer. Weagree with Professor Israel that the inhibitor that is removedby plasmapheresis is probably acting in a non-specific way.Our evidence for this is based on the finding of a factor in thesera of breast-cancer patients which can inhibit E-rosette for-mation by normal T lymphocytes. We have tested sera from140 breast-cancer patients for the presence of this factor andhave found significant inhibition in 74% of these sera-includ-ing all 19 patients with disseminated disease compared withonly 13% of control sera.
This factor can be removed from the surface of normal lym-phocytes previously incubated in cancer sera by extended
washing, overnight incubation, or mild enzyme (papain) diges-tion. These treatments restore E-rosetting ability to lympho-cytes from breast-cancer patients.’ A study of the properties ofthis factor suggest that it is not a normal serum constituent.
2
We would therefore favour a hypothesis that this is a non-spe-cific tumour (cell) breakdown product rather than a tumour-specific factor in any way. A similar effect might also xesultfrom breakdown of non-tumorous tissues. Such a factor whichcan mask E-receptor sites of normal and cancer lymphocytescould easily be envisaged as also masking any tumour-directedsites on the lymphocyte surface.A mechanism of masking of lymphocyte receptors by tissue
breakdown products can be used to explain most instanceswhere immunodepression is known to occur3-5 especiallywhere this has been measured by enumeration of T lympho-cytes. It would also obviate the need to implicate suppressor Tcells in post-traumatic immunosuppression.6University Department of Surgery,Welsh National School of Medicine,Heath Park, Cardiff CF4 4XN
R. H. WHITEHEADC. TEASDALEL. E. HUGHES
1. Whitehead, R. H., Thatcher, J., Teasdale, C., Roberts, G. P., Hughes, L. E.Lancet, 1976, i, 330.
2. Whitehead, R. H., Roberts, G. P., Thatcher, J., Teasdale, C., Hughes, L. E.Unpublished.
3. Messner, R. P., Lindström, F. D., Williams, R. C. J. clin. Invest. 1973, 52,3046.
4. Strickland, R. G., Korsmeyer, S., Soltis, R. D., Wilson, I. D., Williams,R. C. Gastroenterology, 1974, 67, 569.
5. Keller, S. E., Ioachim, H L., Pearse, T., Siletti, D. M. Am. J. clin. Path.
1976, 65, 445.6 Munster, A. M. Lancet, 1976, i, 1329
INACTIVE RENIN IN HUMAN PLASMA
SIR,- We were interested in the paper by Dr Derk and hiscolleagues (Sept. 4, p. 496). Like them we find active and inac-tive renin in human plasma.’ Also like them, we find that acuterenin release-produced in our experiments by saralasin infu-sion-is associated with a rise of active but no change in inac-tive renin concentration. Certain new observations are rele-vant.
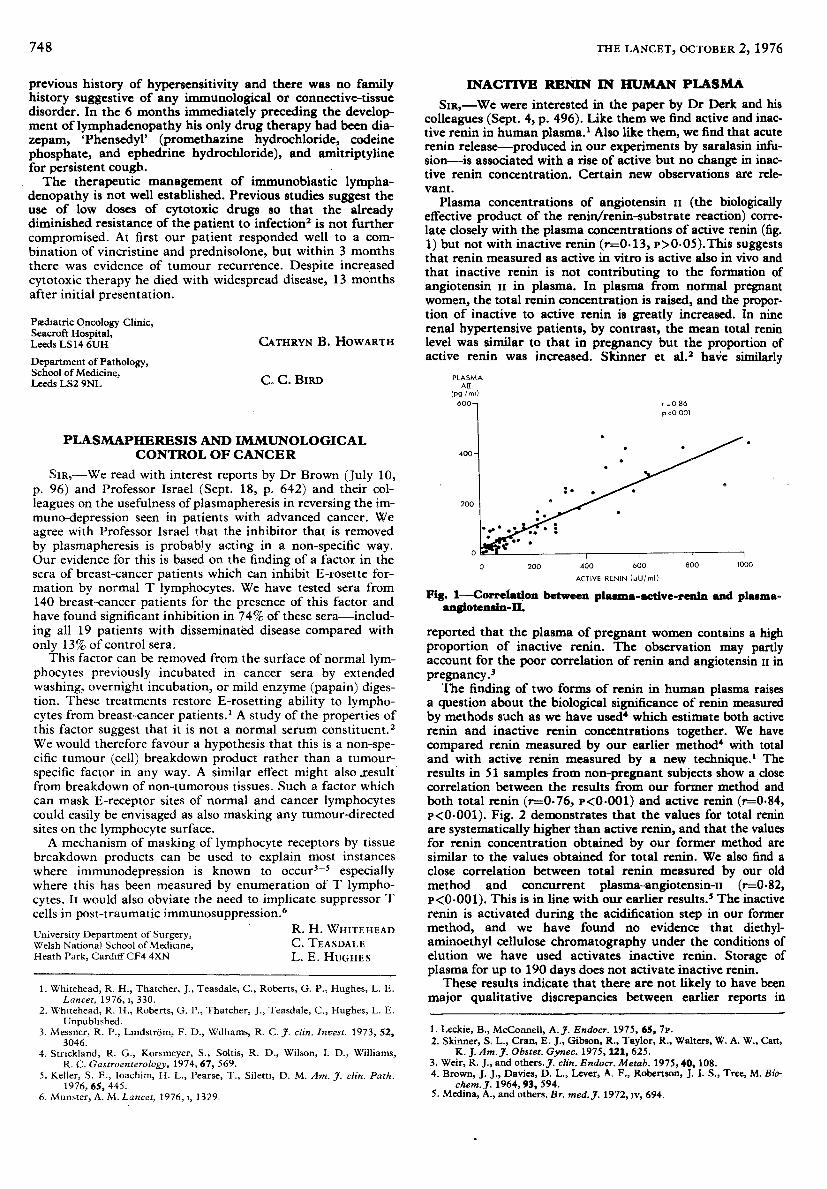
Plasma concentrations of angiotensin ii (the biologicallyeffective product of the renin/renin-substrate reaction) corre-late closely with the plasma concentrations of active renin (fig.1) but not with inactive renin (r=0.13, p)O.05).This suggeststhat renin measured as active in vitro is active also in vivo andthat inactive renin is not contributing to the formation ofangiotensin n in plasma. In plasma from normal pregnantwomen, the total renin concentration is raised, and the propor-tion of inactive to active renin is greatly increased. In ninerenal hypertensive patients, by contrast, the mean total reninlevel was similar to that in pregnancy but the proportion ofactive renin was increased. Skinner et al.2 have similarly
Fig. 1—Coffeltttiom between piMmtt-Mtive-fenin and plasma-angiotensin-n.
reported that the plasma of pregnant women contains a highproportion of inactive renin. The observation may partlyaccount for the poor correlation of renin and angiotensin 11 inpregnancy. 3The finding of two forms of renin in human plasma raises
a question about the biological significance of renin measuredby methods such as we have used which estimate both activerenin and inactive renin concentrations together. We havecompared renin measured by our earlier method4 with totaland with active renin measured by a new technique.’ Theresults in 51 samples from non-pregnant subjects show a closecorrelation between the results from our former method andboth total renin (r=0.76, p<O.001) and active renin (r=084,P<0.001). Fig. 2 demonstrates that the values for total reninare systematically higher than active renin, and that the valuesfor renin concentration obtained by our former method aresimilar to the values obtained for total renin. We also find aclose correlation between total renin measured by our oldmethod and concurrent plasma-angiotensin-tt (r=082,r<0.001). This is in line with our earlier results.’ The inactiverenin is activated during the acidification step in our formermethod, and we have found no evidence that diethyl-aminoethyl cellulose chromatography under the conditions ofelution we have used activates inactive renin. Storage ofplasma for up to 190 days does not activate inactive renin.
These results indicate that there are not likely to have beenmajor qualitative discrepancies between earlier reports in
1. Leckie, B., McConnell, A. J. Endocr. 1975, 65, 7P.2. Skinner, S. L., Cran, E. J., Gibson, R., Taylor, R., Walters, W. A. W.. Catt,
K. J. Am. J. Obstet. Gynec. 1975, 121, 625.3. Weir, R. J., and others. J. clin. Endocr. Metab. 1975, 40, 1084. Brown, J. J., Davies, D. L., Lever, A. F., Robertson, J. I. S., Tree, M. Bio.
chem. J. 1964, 93, 594.5. Medina, A., and others. Br. med. J. 1972, iv, 694.