immune effector cells: car t and other cytotoxic effector...
TRANSCRIPT
IMMUNE EFFECTOR CELLS: CAR T AND OTHER CYTOTOXIC EFFECTOR CELLS OF THE IMMUNE SYSTEM
Jennifer Peterson MSN, RN, OCN, BMTCN Jennifer Shamai MS, RN, AOCNS, BMTCN How the Experts Treat Hematologic Malignancies Las Vegas, NV March 14, 2018
Disclosures
We have nothing to disclose.
Objectives
• Review basics of immunology and immunotherapy • Introduce use of CAR T-cells in immunotherapy • Present FDA approved CAR T-cell therapies • Discuss monitoring for side effects and managing toxicities • Introduce regulatory standards of immune effector cells • Discuss future directions of immune effector cell therapy • Review educational resources
The Immune System
A complex network of proteins, cells, tissues, and organs aimed at defending the body against infections and other diseases 1) Distinguish self from non-self 2) Identify, target, and eliminate foreign invader
• Major organs – Bone marrow: production of immune cells – Thymus: education of immune cells – Lymph nodes: immune responses are produced – Spleen: immune responses and cell recycling
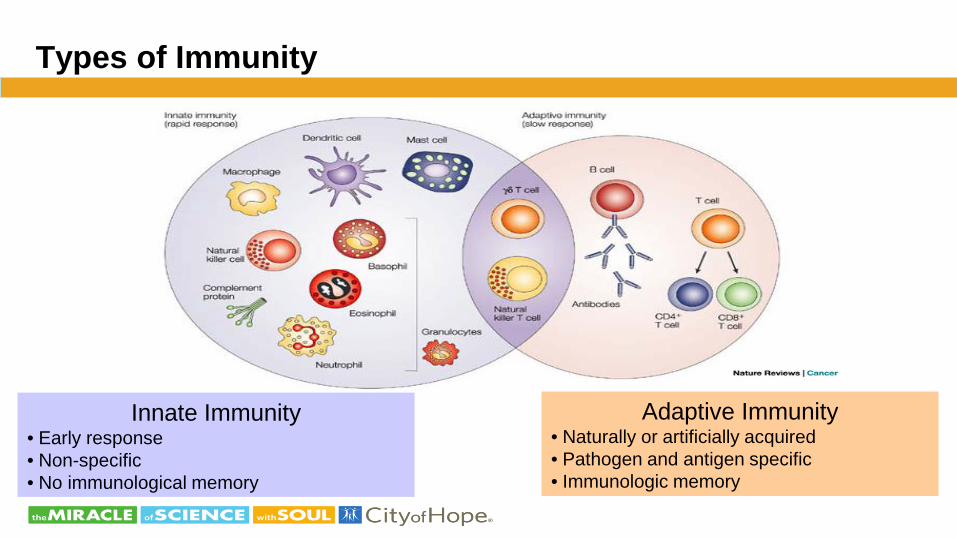
Types of Immunity
Innate Immunity • Early response • Non-specific • No immunological memory
Adaptive Immunity • Naturally or artificially acquired • Pathogen and antigen specific • Immunologic memory
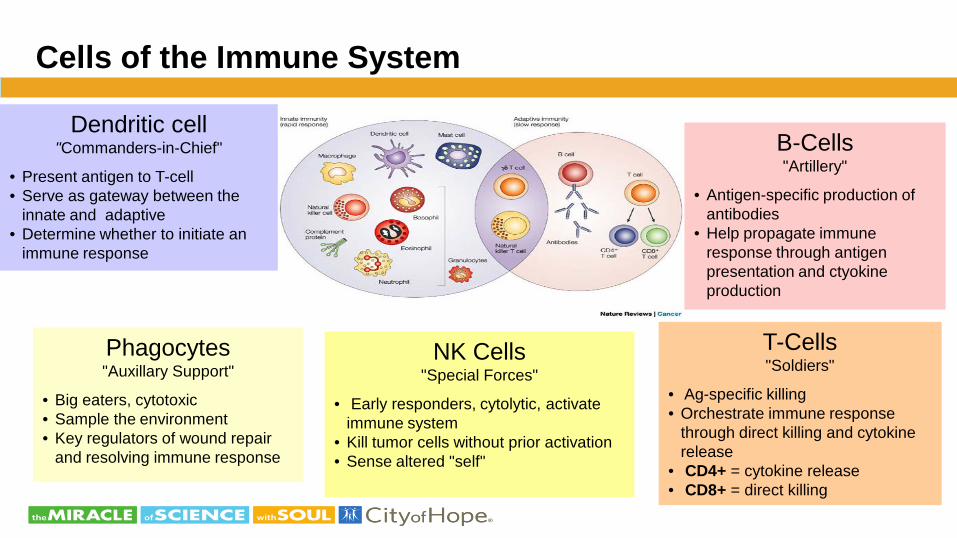
Cells of the Immune System
Phagocytes "Auxillary Support"
• Big eaters, cytotoxic • Sample the environment • Key regulators of wound repair
and resolving immune response
Dendritic cell "Commanders-in-Chief"
• Present antigen to T-cell • Serve as gateway between the
innate and adaptive • Determine whether to initiate an
immune response
NK Cells "Special Forces"
• Early responders, cytolytic, activate immune system
• Kill tumor cells without prior activation • Sense altered "self"
T-Cells "Soldiers"
• Ag-specific killing • Orchestrate immune response
through direct killing and cytokine release
• CD4+ = cytokine release • CD8+ = direct killing
B-Cells "Artillery"
• Antigen-specific production of antibodies
• Help propagate immune response through antigen presentation and ctyokine production
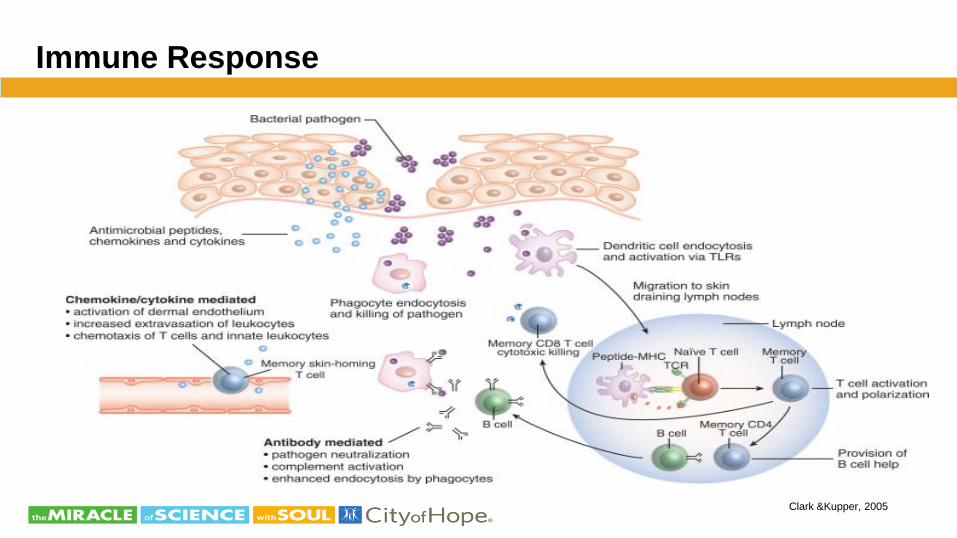
Immune Response
Clark &Kupper, 2005
Immunologic Memory
• Effector T-cells and antibodies persist for weeks to years after exposure to an antigen (protective immunity)
• Second exposure to the same antigen produces a much
faster response (immunologic memory)
The Immune System and Cancer
If cancer is derived from one’s own cells, how does the immune system distinguish self (healthy, normal, uninfected cells) from non-self (cancer cells)?
How do cancer cells evade and suppress the immune system? How can
we combat these mechanisms? How can we boost the immune system?
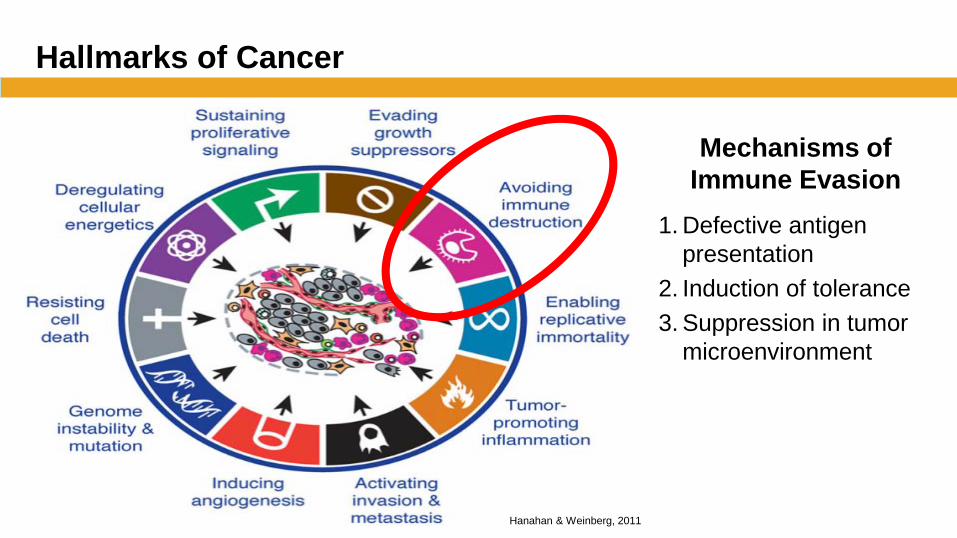
Hallmarks of Cancer
Hanahan & Weinberg, 2011
Mechanisms of Immune Evasion
1. Defective antigen presentation
2. Induction of tolerance 3. Suppression in tumor
microenvironment
Cancer Treatment Modalities
Foundation of cancer therapy for many years: – Surgery – Chemotherapy – Radiation therapy
Newer therapies: – Targeted therapies – Immunotherapy
Immunotherapy, the “Fifth Pillar”
• Immunotherapy is an approach of harnessing a patient's own immune system to fight cancer
• Advantages – Human immune system can distinguish between healthy and unhealthy
cells • Safety profiles that are more manageable or mild than traditional therapies
– Immunotherapy treatment can be dynamic and react to cancer cells as they develop, leading to more lasting results
• Strategies: cancer vaccines, oncolytic viruses, adoptive transfer of T and NK cells, antibodies or proteins that effect the immune checkpoint pathways
Adoptive T-Cell Therapy
Exploits the antitumor properties of lymphocytes 1. Lymphocytes are isolated from the patient 2. Expanded ex-vivo 3. Reinfused back into the patient Why use T-cells? • Ability to specifically target tumor cells that express small peptides • Potentially long clonal lifespan • Potential significant expansion in vivo
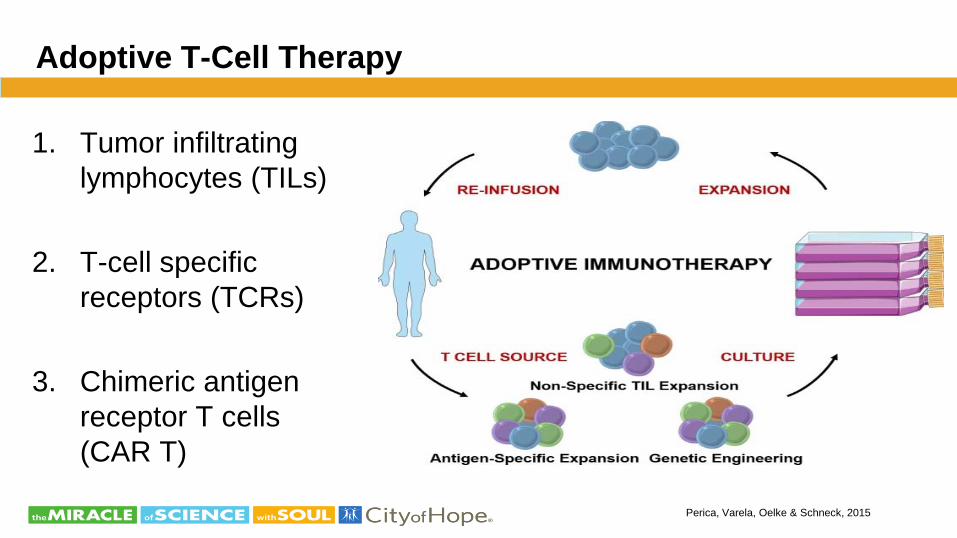
Adoptive T-Cell Therapy
1. Tumor infiltrating lymphocytes (TILs)
2. T-cell specific receptors (TCRs)
3. Chimeric antigen receptor T cells (CAR T)
Perica, Varela, Oelke & Schneck, 2015
History of Immunotherapy and Adoptive Cell Therapy
1950s – Adoptive immunity first described 1950s-1960s – Development of allogeneic HSCT 1970s – Graft versus leukemia effect established 1988 – Earliest trials using TILs 1989 – First CAR T was conceived and developed 2010 – First successful CAR T-cell therapy 2010 – First cancer vaccine Sipuleucel-T approved 2017 – Two CAR T-cell therapies were approved

CAR T-Cell Therapy
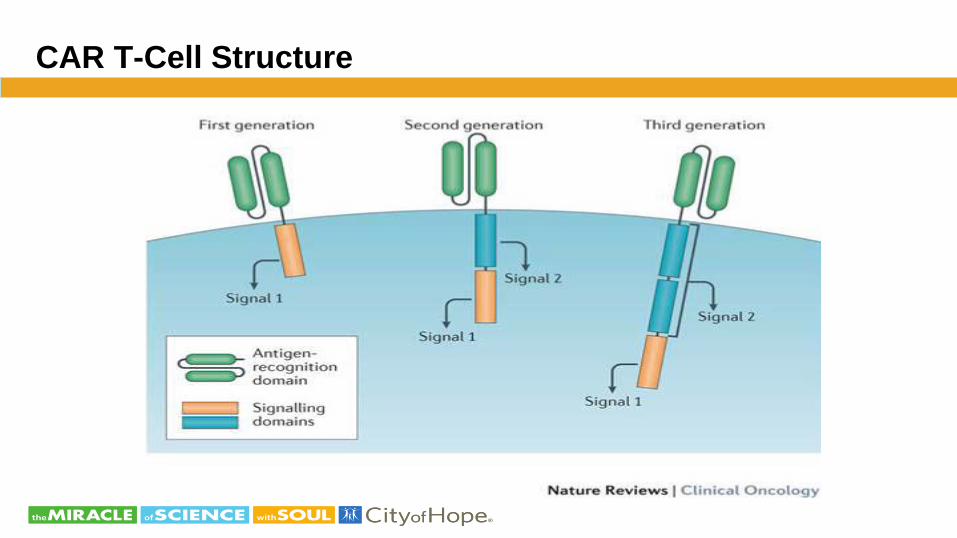
CAR T-Cell Structure
CAR T- Cells for Hematologic Malignancies
FDA approved products for B-cell malignancies in 2017
– Tisagenlecleuel (Kymriah™) indicated for the treatment of patients up to 25 years of age with B-cell precursor acute lymphoblastic leukemia (ALL) that is refractory or in second or later relapse
– Axicabtagene ciloleucel (Yescarta™) indicated for non-Hodgkin lymphoma: Diffuse large B-cell lymphoma (DLBCL), primary mediastinal B-cell lymphoma and transformed follicular lymphoma
Cell Collection and Lymphodepletion
• Cell collection via leukopheresis • Cell manufacturing
– Viral vector and chimeric antigen receptors • Lymphodepletion
– Fludarabine and cyclophosphamide • Yescarta™: fludarabine and cyclophospahmide administered on
the fifth, fourth and third day prior to T-cell infusion • Kymriah™: fludarabine for 4 days and cyclophosphamide for 2
days starting with the first dose of fludarabine – Infuse Kymriah 2 to 14 days after completion of the lymphodepleting
chemotherapy
Response to Therapy
• Response rates in clinical trials for B-cell ALL were reported as 70-93% complete response and 60-86% complete molecular response
• Response rates in clinical trials for lymphoma were reported as 82% complete or partial response, with 54% of patients achieving complete response
• Multifactorial: – Tumor type – Cell dose infused – Design of the chimeric antigen receptor (CAR) – Pre-infusion conditioning regimen
Relapse: Loss of CD-19 expression of the malignant cells was noted
Davila, M., 2017
Monitoring and Managing Toxicities of CAR T-Cell Therapy
• Cytokine release syndrome (CRS)-boxed warning for both FDA approved CAR T-cells
• Neurologic toxicities-boxed warning for both FDA approved CAR T-cells
• Other potential side effects

Cytokine Release Syndrome
• Associated with – Monoclonal antibody infusion – Bi-specific antibodies for leukemia – Haploidentical stem cell transplant – CAR T-cell therapy
• Occurs when large number of lymphocytes and/or macrophages are activated and release cytokines that activate other immune cells
• Interleukin (IL) 6, tumor necrosis factor, IL-2, IL-8 and IL-10 levels are elevated
• C-reactive protein and ferritin levels used as markers
Lee et al., 2014
Cytokine Release Syndrome
• Onset and severity depend on causative agent and degree of immune cell activation
• Incidence and severity greater with larger disease burden • Primary anticipated side effect after T-cell therapy • Occurs in approximately 90% of patients receiving CAR T-cell therapy
– Can range from mild to life threatening • Indicator of response to therapy • Fever is the hallmark sign • Monitoring is crucial
Callahan, C., Baniewicz, D., and Ely, B., 2017

Symptoms of Cytokine Release Syndrome
• Fever-often mimics infection • Cardiac • Respiratory • Neuro • Renal • Hepatic • Gastrointestinal • Coagulopathies
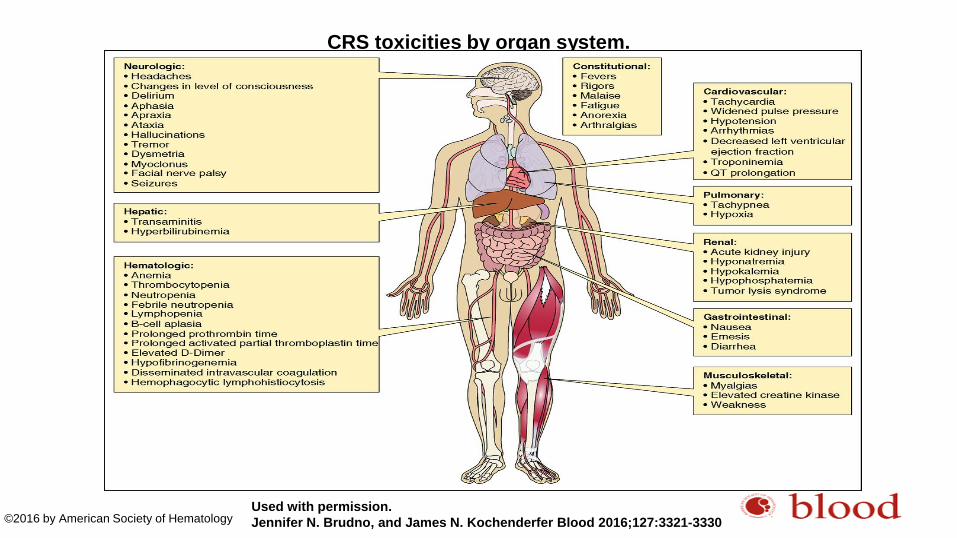
CRS toxicities by organ system.
Used with permission. Jennifer N. Brudno, and James N. Kochenderfer Blood 2016;127:3321-3330 ©2016 by American Society of Hematology
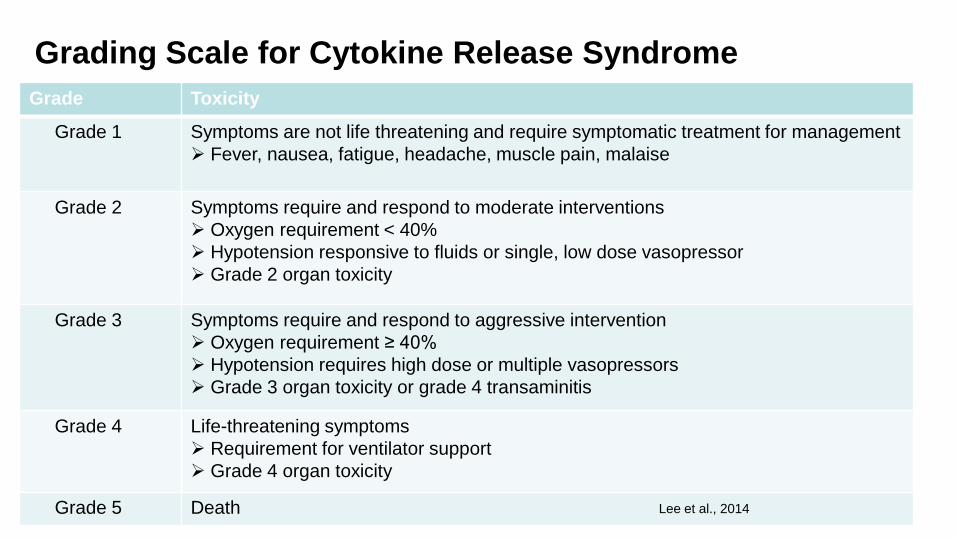
Grading Scale for Cytokine Release Syndrome Grade Toxicity
Grade 1 Symptoms are not life threatening and require symptomatic treatment for management Fever, nausea, fatigue, headache, muscle pain, malaise
Grade 2 Symptoms require and respond to moderate interventions Oxygen requirement < 40% Hypotension responsive to fluids or single, low dose vasopressor Grade 2 organ toxicity
Grade 3 Symptoms require and respond to aggressive intervention Oxygen requirement ≥ 40% Hypotension requires high dose or multiple vasopressors Grade 3 organ toxicity or grade 4 transaminitis
Grade 4 Life-threatening symptoms Requirement for ventilator support Grade 4 organ toxicity
Grade 5 Death Lee et al., 2014
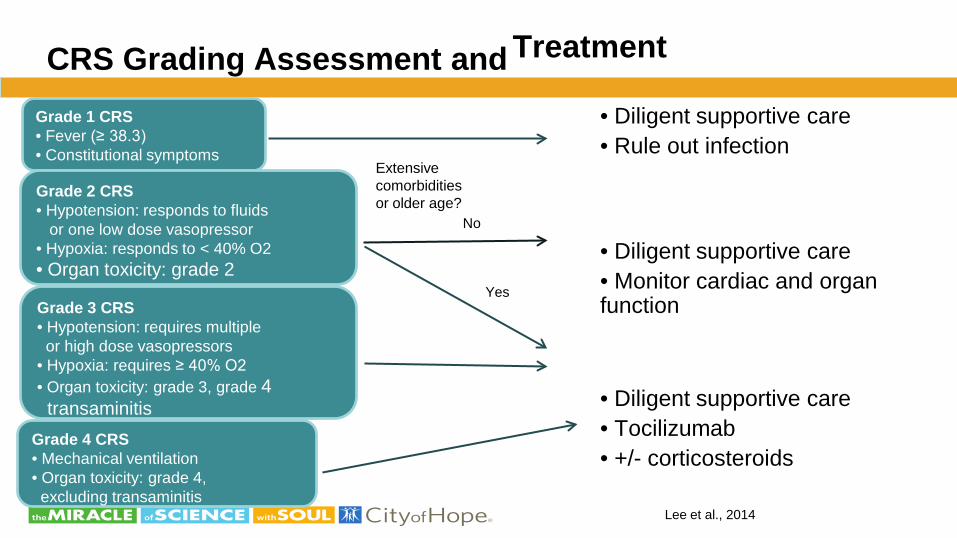
Treatment CRS Grading Assessment and
• Diligent supportive care • Rule out infection
• Diligent supportive care • Monitor cardiac and organ function
• Diligent supportive care • Tocilizumab • +/- corticosteroids
Grade 1 CRS • Fever (≥ 38.3) • Constitutional symptoms
Grade 2 CRS • Hypotension: responds to fluids or one low dose vasopressor • Hypoxia: responds to < 40% O2 • Organ toxicity: grade 2
Grade 3 CRS • Hypotension: requires multiple or high dose vasopressors • Hypoxia: requires ≥ 40% O2 • Organ toxicity: grade 3, grade 4 transaminitis
Grade 4 CRS • Mechanical ventilation • Organ toxicity: grade 4, excluding transaminitis
Extensive comorbidities or older age?
No
Yes
Lee et al., 2014
Neurotoxicity
• Changes may be subtle • Symptoms can range from mild to severe • May occur with CRS symptoms or independent of CRS
symptoms • Pathogenesis unclear • Education for patient and caregivers is essential
Bayer et al., 2017
Neurotoxicity
• Symptoms may include: – Headache – Word finding difficulty/aphasia – Seizures – Tremors – Obtundation – Confusion/altered mental status – Altered gait
Lee et al., 2014
CARTOX 10 Neurotoxicity Assessment
• Developed by MD Anderson • A simple and quick method to flag development of neurotoxicity • The 10-point test asks a patient:
– Oriented to year, month, city, hospital, and president/prime minister of their home country (5 points)
– Ability to write a standard sentence (1 point) – Name three nearby objects (3 points) – Count backward from 100 by tens (1 point)
http://www.ascopost.com/News/58061,
2017

MD Anderson 10 Point Neurotoxicity Grading
• Normal: 10 points • Mild toxicity: 7-9 points • Moderate toxicity: 3-6 points • Severe toxicity: 1-2 points • Critical toxicity: obtunded, new onset motor
weakness, cerebral edema on imaging or status epilepticus
Kebriaei, P., 2017
Management of Neurotoxicity
• Neurology consult • Rule out other causes with imaging • Seizure prophylaxis • Immunosuppression with dexamethasone is standard
treatment • May depend on concurrent CRS present or not
Treatment of CRS and Neurotoxicity
• Monitoring and treatment may require higher level of care • Dependent on grade of CRS • Tocilizumab
– Humanized anti-IL-6 monoclonal antibody • Corticosteroids • Siltuximab
Other Potential Side Effects
• B cell aplasia – Target CD-19
• Tumor lysis syndrome – High tumor burden prior to therapy
• Graft-Versus-Host Disease – Immunologic response
• Relapsed disease due to short persistence of CAR T-cells and antigen loss
• Psychosocial effects – Relapse/refractory disease – Travel to treatment institution – Cost for stay (approximately 6 weeks)
Callahan, C., Baniewicz, D. and Ely, B., 2017
Smith, L. And Venella, K., 2017
Regulatory Requirements
• Products are restricted to certified healthcare facilities • Facilities must be enrolled and comply with the Risk Evaluation and
Mitigation Strategy (REMS) – Authorized hospital representative designated and trained – Providers who prescribe, dispense, or administer must be trained
regarding the management of CRS and neurotoxicity – Immediate access to 2 doses of tocilizumab – Provide patient wallet card – Report adverse effects
FACT Immune Effector Cell (IEC) Standards
Why develop IEC standards? • Novel therapy with unique toxicity profile • Administration requires significant collaboration with
various members of the healthcare team • Coordination of therapy requires a robust clinical
infrastructure
Maus & Nikiforow, 2017
FACT Immune Effector Cell (IEC) Standards
• New standards and an accreditation program for IECs published early 2017 – “Cells used to modulate, elicit, or mitigate an immune response for
therapeutic intent” – Includes dendritic, NK, T or B cells
• Standards apply to the process, not the science – Donor workup, apheresis collection, labeling, storage,
documentation, product administration, and chain of custody – Quality management program – Education
Maus & Nikiforow, 2017l; Nikiforow, n.d.; FACT, 2017
FACT Immune Effect Cell (IEC) Standards
• Pharmacies shall have access to medications adequate to treat expected complications of IECs, including CRS
• Training and competency for nurses, APPs, and physicians shall include – CRS – Tumor lysis syndrome – Cardiac dysfunction – Respiratory distress – Neurologic toxicity – Renal and hepatic failure – Disseminated intravascular coagulation – Anaphylaxis
FACT, 2017
FACT Immune Effect Cell (IEC) Standards
• Procedures shall include: – Written policies for the detection and management of
complications, including CRS and neurotoxicity – Process for rapid escalation of care – Timely communication to clinical staff, intensive care units,
emergency departments and pharmacies • Clinical program shall have written guidelines for management of
complications
FACT, 2017
Other Considerations
• Establishing standards of care • Capturing the acuity level of care to adjust staffing levels • Creating documentation forms for clinical care, care plans, and patient
education
Halton, Llerandi, Diamonte, Guintanilla & Maile-Mayer, 2017
At What Cost?
• Tisagenlecleucel: $475,000 • Axicabtagene ciloleucel: $373,000 • Tocilizumab: ~$4,800 per dose
• Patient support programs are available • Insurance policies provide coverage
Future Directions in Immune Effector Cell Therapy
• Other diseases – Hematology: Multiple myeloma, acute myelogenous leukemia, chronic
lymphocytic leukemia – Solid tumors: Glioblastoma, pancreatic, lung, malignant mesothelioma,
and prostate (lethal neuroendocrine prostate cancer) • Dual target therapy: CD-19 and CD-22 for ALL and CD-33 and CD-123
for AML • Allogeneic CAR T-cells for patients who are at high risk for relapse or
who relapse post stem cell transplant • Universal CAR T-cells
Future Directions in Immune Effector Cell Therapy
• Tumor- infiltrating lymphocytes – Advanced colorectal cancer, liver cancer and melanoma
• T-cell receptors – Demonstrating positive results in melanoma and sarcoma
• Virus specific T-cells – Epstein-Barr, adenovirus, cytomegalovirus, BK virus
and human herpes virus 6 • Bi-specific antibodies
Tzannou, I. et al., 2017 www.cancer.gov/about-cancer/treatment/research/car-t-cells
Future Directions in Immune Effector Cell Therapy
• As of 2/2/18: – Open T-cell based cellular therapy clinical trials around
the world: ~2,345 – Open NK-cell based cellular therapy clinical trials
around the world: ~300
Clinicaltrials.gov

Resources
Nurse resources • Oncology Nursing Society
– https://www.ons.org/practice-resources/cancer-therapies/immunotherapy-resources
• CAR T-cell Therapy: The Nurse’s Role in Treating Patients – http://www.mlicme.org/P17053/index.php – 1.5 CE contact hours
• Society for Immunotherapy of Cancer (SITC) – https://www.sitcancer.org/connected/home
Resources
Patient resources • National Cancer Institute
– https://www.cancer.gov/about-cancer/treatment/research/car-t-cells • Leukemia and Lymphoma Society
– http://www.lls.org/treatment/types-of-treatment/immunotherapy/chimeric-antigen-receptor-car-t-cell-therapy
– Video: https://youtu.be/NEt9BmvSl0k • International Myeloma Foundation • American Cancer Society
– https://www.cancer.org/treatment/treatments-and-side-effects/treatment-types/immunotherapy/car-t-cell1.html
• Kite – Kite Konnect program • Novartis – Kymriah Cares program
References Brudno, J. and Kochenderfer, J. (2016). Toxicities of chimeric antigen receptor T cells: recognition and management. Blood, 127(26), 3321-3330. Callahan, C. , Baniewicz, D. and Ely, B. (2017) CAR T-cell therapy. Clinical Journal of Oncology Nursing, Supplement to volume 21, 22-28. Clark, R. and Kupper, T. (2005). Old meets new: the interaction between innate and adaptive immunity. Journal of Investigative Dermatology, 125(4), 629-637. Davila, M. (2017). The latest advances in CAR T-cell therapy for refractory and relapsed lymphomas and leukemias. Journal of the Advanced Practitioner in Oncology, 8(supplement 2), 3-13. Foundation for the Accreditation of Cellular Therapy. (2017). Standards for immune effector cells (1st ed.). Hanahan, D. and Weinberg, R. (2011). Hallmarks of cancer: the next generation. Cell, 144(5) 636-674. Maus, M. & Nikiforow, S. (2017). The Why, what, and how of the new FACT standards for immune effector cells. Journal for Immunotherapy of Cancer, April 18(5). Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5394615/ Nikiforow, S. (n.d.). Introducing the FACT standards for immune effector cells. Retrieved from http://www.factwebsite.org/uploadedFiles/Educational_Opportunities/Immune%20Effector%20Cell%20Standards.pdf Lee, D., Gardner, R., Porter, D., Louis, C., Ahmed, N., Jensen, M., Grupp, S., and Mackall, C. (2014). Current concepts in the diagnosis and management of cytokine release syndrome. Blood, 124(2), 188-195. Perica, K., Varela, JC., Oelke, M., & Schneck, J. (2015). Rambam Maimonides Medical Journal, eCollection 2015 Jan. Smith, L. and Venella, K. (2017). Cytokine release syndrome: Inpatient care for side effects of CAR T-cell therapy. Clinical Journal of Oncology Nursing, supplement to volume 21, 29-34.
References
Tzannou, I., Papadopoulou, A., Nail, S., Leung, K., Martinez, C., Ramos, C., Carrum, G., Sasa, G., Lulla, P., Watanabe, A. Kuvalekar, M., Gee, A., wu, M., Liu, H., Grilley, B., Krance, r., Gottschalk, S., Brenner, M., Rooney, C., Heslop, H., Leen, A. ,and Omer, B. (2017). Off-the –shelf virus specific T-cells to treat BK virus, human herpesvirus 6, cytomegalovirus, Epstein- Barr virus, and adenovirus infections after allogeneic hematopoeitic stem-cell transplantation. Journal of Clinical Oncology, 35(31), 3547-3557. Zeltsman, M., Dozier, J., McGee, E., Ngai, D., and Adusumilli, P. (2017). In-depth review: Chimeric antigen receptor T cell- based therapies. Translational Research, 187, 1-8. The National Cancer Institute. CAR T cells: Engineering patients’ immune cells to treat their cancers. Retrieved from https://www.cancer.gov/about-cancer/treatment/research/car-t-cells