immune checkpoints sot2016
TRANSCRIPT

© 2016 Envigo envigo.com
Chair: Greg Bannish
Presenters: Lee A. Coney and Mandy Horn
Key considerations in the safety
evaluation of drugs targeting
immune checkpoints

Company overview

We are a global contract research products and
services company dedicated to helping our
customers achieve the potential of their products
which improve human life, advance animal
welfare, and protect the environment and global
food security.
Who We Are

Our Brand Promise
Together, we make the world a
safer and healthier place to live.
Our company places the customer at the center
of everything we do. We focus on what matters
to you, our customer, and work closely with you
to secure the potential of your research and
products. We are dedicated to research that
makes a difference in the lives of people all over
the world.

52 locations Global availability of research
models
and CRO services
5 continents Extensive reach across the
Americas, Europe, Asia, and the
Middle East
3,800 employees Serving over 65 countries
150 years Combined industry experience
$500 million Approximately $500m in annual
revenues
Capacity and Reach

Contract Research Services (CRS) locations
United States of America
+ Princeton, New Jersey
Envigo laboratories are
located in The United
States of America,
Europe and the Middle
East
Europe
Corporate HQ: Huntingdon, England
+ Huntingdon, England
+ Eye, England
+ Ely, England
+ Shardlow, England
+ Rossdorf, Germany
+ Barcelona, Spain
+ Valencia, Spain
Middle East
+ Rehovot, Israel

Research Models and Services (RMS) locations
Envigo production
sites in North
America, Europe, the
Middle East and Asia
North America
+ Dublin, VA
+ Frederick, MD
+ Haslett, MI
+ Houston, TX
+ Indianapolis, IN
+ Livermore, CA
+ Madison, WI
+ Mexico City, Mexico
Europe
+ Blackthorn, UK
+ Bresso, Italy
+ Gannat, France
+ Horst, Netherlands
+ Loughborough, UK
+ Udine, Italy
+ Wyton, UK
Middle East
+ Jerusalem, Israel
+ Rehovot, Israel
+ Yokneam, Israel
India
+ Hyderabad, India
Corporate HQ:
Indianapolis, IN
European Office:
Venray, Netherlands

Key considerations in the safety evaluation of drugs
targeting immune checkpoints

+ What is cancer immunotherapy?
+ What are the potential challenges in the safety assessment
of antibodies targeting immune system checkpoints?
+ Things to consider when designing and running your non-
clinical safety programmes for immune checkpoint targets?
+ Measuring immunotoxicity / immunopharmacology
+ Case study – what if your chosen therapeutic has no
pharmacologically relevant non-clinical safety species?
+ Summary
Presentation overview

Cancer immunotherapy

The utility of the immune system
Heidi L. Nature 2014 508:24

A history of cancer immunotherapy
Kirkwood JM et al. CA Cancer J Clin 2012 62:309

+ There are multiple different platforms of cancer
immunotherapy and many very different target pathways
+ Adoptive cell transfer + TILs, TCR–transfected T-cell, CAR therapy
+ Non-specific immunotherapies + Cytokines (IL-2, IFNa) CD40 agonist mAb, TLR agonist
+ Vaccination strategy + Sipuleucel-T, MAGE-3 ASCL, OncoVEX
+ Immune checkpoint blockade + CTLA-4 blocking mAb, PD-1 blocking mAb
+ The remainder of this talk with focus upon this latter
approach so called immune checkpoint targeting
antibodies
Current state of cancer immunotherapy

+ T-cell killing of tumour cells can be switched on and off + Regulated by signals from other cells of the immune system such as antigen
presenting cells and tumours themselves
+ T-cells are effectively “switched off” by due to signalling
via immunoinhibitory (checkpoint) receptors on activated T
cells
+ T cells can be switched back on in lymph nodes or the
tumour microenvironment by drugs that target checkpoint
receptors
+ There are many such drugs in development and on the
market today with some exciting biology behind them + PD1, CTLA-4, PDL, KIR, IDO1, 4-1BB, OX40, LAG3, B7-H3, CD27, CD70, CD28,
CD30 etc.
Checkpoint inhibitors: Background

Checkpoint inhibitors: Background
Shin DS & Ribas A. Curr Opin Immunol 2015 33:23

+ CD28
+ OX40
+ GITR
+ CD137
+ CD27
+ HVEM
Potential checkpoint targets (not exhaustive)
Activating receptors
+ CTLA-4
+ PD-1
+ TIM-3
+ BTLA
+ VISTA
+ LAG-3
Inhibitory receptors
Inspired by Mellman I et al. Nature 2011 480:480
Agonistic antibodies Blocking antibodies

+ Immunoinhibitory receptors are expressed after normal
MHC class I/II adaptive T cell activation
+ Ligation of CTLA-4 by B7-1/B7-2 or PD1 by PD-L1 or PD-
L2 attenuates normal T cell activation
+ CTLA-4 and PD1 upregulation on chronically activated T
cells makes them less responsive to antigenic stimulation
+ Inhibition of these targets can restore T cell function and
enhance T-cell tumour killing
+ Checkpoint inhibitors play critical roles in maintenance of
peripheral T cell tolerance
+ Drugs that target immune system checkpoints have the
potential to promote inflammation/autoimmunity in humans
Checkpoint inhibitors: Mechanism of action

Characteristic CTLA‐4 pathway PD‐1 pathway
Expression pattern Exclusively T cells
(constitutively on Tregs)
T, B, and NK cells
(activated T cells)
Natural ligands CD80 (B7-1) and CD86
(B7-2)
PD‐L1 and PD‐L2
Expression profile of
ligands
Mainly on antigen
presenting cells (APCs)
APCs and tumour cells
Phenotype of KO mice Early fatal autoimmune
syndrome
(lymphoproliferative
disease)
Strain‐specific
autoimmunity presenting
later in life in some strains
Effect of target blockade Enhanced proliferation of
CD4+ and CD8+ T cells
with increase in ratio to
Treg cells
Enhanced proliferation of
CD8+ T cells greater than
CD4+ T cells and
enhanced cytotoxicity of
CD8+ T cells
CTLA-4 v PD-1 pathways
Greenwald RJ, et al. Ann Rev Immunol. 2005;23:515-548. Chambers CA, et al. Ann Rev Immunol. 2001;19:565-594. Dong H, et al.
Nat Med. 2002;8:793-800. Curran MA, et al. Proc Natl Acad Sci U S A. 2010;107:4275-4280. Pilon-Thomas S, et al. J Immunol.
2010;184:3442-3449.

+ CPIs control central and peripheral immune tolerance to
“self-antigens” + CPIs restrict positive selection in the thymus, inhibit the activation and function of
self-reactive T cells in the peripheral circulation, effect Treg cell development and
their function
+ Therefore inhibition of some CPI pathways may contribute
to the development of immune-mediated disease + Findings consistent with autoimmunity observed in both CTLA-4 and PD-1 KO mice
on certain backgrounds
+ Similar findings seen in humans with genetic anomalies in
certain CPI genes + SLE, RA, MS, Type 1 diabetes
+ Immune-mediated events observed in clinical studies with
CPIs and monitored in post-marketing PV
Predicted risks based on mechanism of action

Checkpoint inhibitors: Mechanism of action
Intlekofer AM et at. J Leukoc Biol 2013 94:25

+ The intended pharmacological action of each therapeutic is
immune system activation – immediate alarm bells!
+ As with most biopharmaceuticals the balance between
therapeutically desired pharmacology and clinical dose-
limiting “exaggerated pharmacology” is a delicate balance
+ Acute effects such as systemic cytokine release may be
manageable in some clinical situations
+ More chronic effects such as induction of autoimmune
disease may be more difficult to model in healthy standard
non-clinical models
+ SPF animals may also lack or have limited target
expression of checkpoint molecules
Challenges in safety assessment

+ Binds human CTLA-4 in vitro with high affinity
+ Inhibits in vitro binding of B7.1 (CD80) and B7.2 (CD86) to
human CTLA-4
+ CDC and ADCC activity investigated in vitro and in vivo
+ Colon carcinoma studies in human CTLA-4 transgenic
mouse
+ Extensive TDAR investigation in cynomolgus monkey + Hepatitis B surface antigen (HBsAg) vaccine, a melanoma cell-based vaccine (Sk-
mel), DNP (2,4-Dinitrophenyl)-Ficoll, keyhole limpet hemocyanin (KLH) and simian
immunodeficiency virus (SIV), DNA vaccines (purified plasmid DNA) expressing the
proteins for the gag (pSIVgag), env (pSIVenv), and pol (pSIVpol) portions of SIV. In
one study, the SKmel tumour line was transfected to express GM-CSF.
+ Extensive immunophenotypic analysis of T cells and subsets in these studies
+ Extensive assessment of humoral immune responses to TDAR antigens
Yervoy (Ipilimumab) anti-CTLA-4 antibody
EMA Assessment Report For Yervoy (ipilimumab)

+ Tissue cross reactivity studies
+ Safety pharmacology included as part of repeat dose
toxicity programme
+ Combination studies with anti-CD137 and anti-PD-1
antibodies conducted in cynomolgus monkeys
+ Single species toxicology programme conduced in
cynomolgus monkey as only pharmacologically relevant
species
+ Studies up to 6 months in duration at a variety of dose
levels conducted
+ No reproductive, developmental or juvenile toxicology
studies were submitted for registration purposes
Yervoy (Ipilimumab) anti-CTLA-4 antibody
EMA Assessment Report For Yervoy (ipilimumab)

+ Most findings considered adverse seen in combination
toxicity or exploratory (TDAR) pharmacology studies not
anti-CTLA-4 alone GLP studies
+ Low incidence of immune-meditated toxicities + Colitis, dermatitis, or infusion reactions
+ Responses consistent with proposed MOA of CTLA-4 in maintaining self-tolerance
+ Findings in cynomolgus monkeys correlated with findings
in humans, although with less frequently – under predict?
+ CTLA-4 blocking did result in an over stimulation of the T-
cell compatment + Few meaningful changes in immunophenotype or autoimmune organ pathology
(with exception of colitis and dermatitis)
+ Increased TDAR was observed demonstrating expected pharmacodynamics
Yervoy (Ipilimumab) anti-CTLA-4 antibody
EMA Assessment Report For Yervoy (ipilimumab)
+ Agonist antibodies + Systemic cytokine release
+ Hepatotoxicity
+ Antagonist (blocking) antibodies + Immune system activation and autoimmunity
+ Dermatitis, colitis, hepatitis, thyroiditis, hypophysitis, uveitis, pneumonitis
+ Adverse events observed in clinic include: pneumonitis,
colitis, skin effects (rash, pruritis, vitiligo), conjunctivitis,
uveitis, hepatotoxicity, thyroid toxicity, nephritis
+ Normal cynomolgus monkeys not predictive of all clinical
findings – how do we increase the potential to translate
understanding from non-clinical to clinical?
Clinical experience

+ Can studies in normal animals (were lower expression of
checkpoint receptors since lower numbers of activated T
cells) predict adverse events in cancer patients?
+ Do the immune changes in normal animals adequately
reflect the risk of immune-mediated pathology in humans?
+ Should greater focus be on safety studies in models of
autoimmunity, cancer, vaccination, where more activated T
cells & checkpoint expression / activity is higher?
+ Could these models then become over predictive?
+ Is it useful to understand relative risk of combos of
checkpoint inhibitors to monotherapy; benchmark new
therapies to anti-CTLA-4 & anti-PD-1 marketed products?
Checkpoint inhibitors: Key considerations for safety

+ “Classical” NOAEL approach less relevant for molecules
targeting check point inhibitors
+ First in human dosing likely to be based on extensive non-
clinical investigations + In vitro potency assessment including relative potency between human and non-
clinical species
+ Receptor occupancy
+ FIH dose likely to be based on PAD and / or MABEL. Generally clinical dose setting
will be conservative with slow dose escalation in the clinic
+ Extensive PK/PD modelling to inform clinical dosing and dose escalation.
Challenging given huge diversity in clinical subjects T-cell populations
Increasing the translation of non-clinical to clinical

+ Non-standard approaches to safety assessment will
continue to be evolved to increase the predictiveness of
non-clinical models + Vaccination / antigen challenge in non-clinical studies
+ Host defense approach adapted for safety evaluation
+ Comprehensive analysis of T-cell subsets by flow cytometry (Treg, Tem, Teff, Tcm,
Th1, Th2 in addition to normal panels)
+ Receptor occupancy in blood and other lymphoid tissue
+ In vitro and in vivo cytokine analysis (large multiplex panels)
+ RO, PAD/MABEL, in vitro / in vivo (EC50s), integrate exposure/PD/efficacy/safety;
close patient monitoring
+ The sample burden on animals is likely to be extensive,
increases the requirement for microsampling /
microanalysis even in non-rodent species
Increasing the translation of non-clinical to clinical

Measuring immunotoxicity / immunopharmacology

Immunotoxicology synopsis
Normal
animals
Immunosuppression Immunostimulation
Infection / cancer risk Hypersensitivity
& Autoimmunity
Morbidity
potential
Morbidity
potential

Immunotoxicology focus for immune checkpoints
Normal
animals
Immunosuppression Immunostimulation
Infection / cancer risk Hypersensitivity
& Autoimmunity
Morbidity
potential
Morbidity
potential

+ There is no single assay or suitable biomarker to measure
all aspects of immunotoxicology
+ A weight of evidence approach is undertaken + Existing understanding of drug pathway engagement / pharmacological properties
+ Immune system effects observed in animal toxicity and clinical safety studies
+ Drugs with a high predicted risk will require immune
function testing to characterise that risk and understand
dosing limitations
Measuring immunotoxicology

+ Inclusion of immunotoxicology / pharmacology endpoints in
toxicity studies aids us in… + …demonstrating the relevance of the tox species
+ …preclinical toxicity study dose selection
+ …TK / PD demonstrates durable pharmacology and exposure in studies
+ …understanding applicability of immunogenicity
+ …identifies translatable biomarkers for clinic
+ …interpretation of dose-response relationship with toxicity and identification of
clinical doses
Immunotoxicology v pharmacology

+ Can biomarkers of immune activation improve our
nonclinical models? + Understand relevance of the non-clinical model
+ Demonstrate PD and maintenance of PD in presence of immunogenicity
+ Potentially increase target expression when it requires immune activation for
expression
+ Establish pharmacodynamic range
+ Help set doses for toxicity studies
+ Help define FIH starting dose
+ Immunotoxicity – extension of the pharmacology
+ Help identify and/or understand adverse findings
+ Cytokines, complement activation, immune complexes, auto-antibodies
Immune activation biomarkers?

+ Immune system over stimulation can cause pathological
changes + Immune complex deposition
+ Hypersensitivity
+ Activation of pre-existing disorders
+ Autoimmune cross-reactivity
+ Inflammatory responses
+ How do we predict autoimmunity in animal models?
+ Molecular mimicry + Pathogen (or vaccine antigen) contains a similar linear T cell epitope or
conformational B cell epitope to host leading to a cross reactive immune response
to healthy tissue
Autoimmune cross-reactivity

Disease Implicated agent Mechanism?
Rheumatic heart disease Group A Streptococcus T cell mimicry (GAS Prt-M
with vascular heart protein)
Guillain-Barre Syndrome Campylobacter jejuni B cell mimicry (LPS
oligosaccharides cross react
with gangliosides)
Chronic Lyme arthritis Borrelia burgdorferi T cell mimicry (OspA cross
reactivity with human LFA-1
Idiopathic thrombocytopenia VZV, EBV, Rubella B cell mimicry (viral epitopes
cross reactivity with platelet
glycoprotein IIb/IIIa
Reactive arthritis Chlamydia trachomatis T cell mimicry (epitope cross
reactivity with HLA-B27)
Type I Diabetes Rotavirus/ Enterovirus Epidemiological evidence
(trigger effect?)
Infection and autoimmune disease
+ Haematology: total & absolute differential leukocyte counts
(incl. macrophages)
+ Clinical chemistry - globulin levels and A/G ratios
+ Gross pathology of lymphoid organs and tissues
+ Organ weights - thymus, spleen, lymph nodes etc.
+ Histopathology of lymphoid organs (bone marrow, spleen,
lymph node, thymus etc.)
+ Flow cytometry of T, B & NK cells
+ All included within most general toxicology studies study
General immune status

+ General immunophenotyping of cellular component of
immune system by flow cytometric methods
+ T-cell-dependent antibody response (TDAR) to model
antigens e.g. KLH, SRBC, TT, OVA, flu' immunised during
dosing & after recovery + Measure primary (IgM/IgG) & secondary (IgG) antibody response
+ Measure cellular response to vaccination with viral / DNA / tumour vaccines
+ T cell responses + DTH responses, LLNA
+ NK activity
+ Macrophage function
Measuring immunomodulation

+ Increases in in vitro cytotoxicity, receptor expression, T cell
proliferative / cytokine responses to mitogens, NK activity
+ Histopathology of target tissues for autoimmunity
+ Serum cytokine levels
+ Show immune system returns to / towards normal on
cessation of dosing / removal of drug
+ Activation quantified by increase in in vitro cytotoxicity,
cytokine secretion, receptor expression (flow cytometry)
+ General immune status- flow cytometry of T and B cells,
monocytes, histopathology of lymphoid organs,
haematology
Immune system activation

TDAR principle
1st Vaccination 2nd Vaccination
IgM
IgG

General immunophenotyping
SSC
FS
C
CD14
SS
C
CD3
CD
20
CD4
CD
8
CD3
CD
16
Lymphocytes
Monocytes
NK
T helper
T cell
B cell
T cytotoxic

Unstimulated PHA Unstained
(Isotype controls)
CD25
Fo
xP
3
Treg Treg
+ Intracellular staining: Increased CD4+CD25+foxP3+ Tregs
following stimulation of whole blood from cynomolgus
macaque
Treg cell staining by flow cytometry
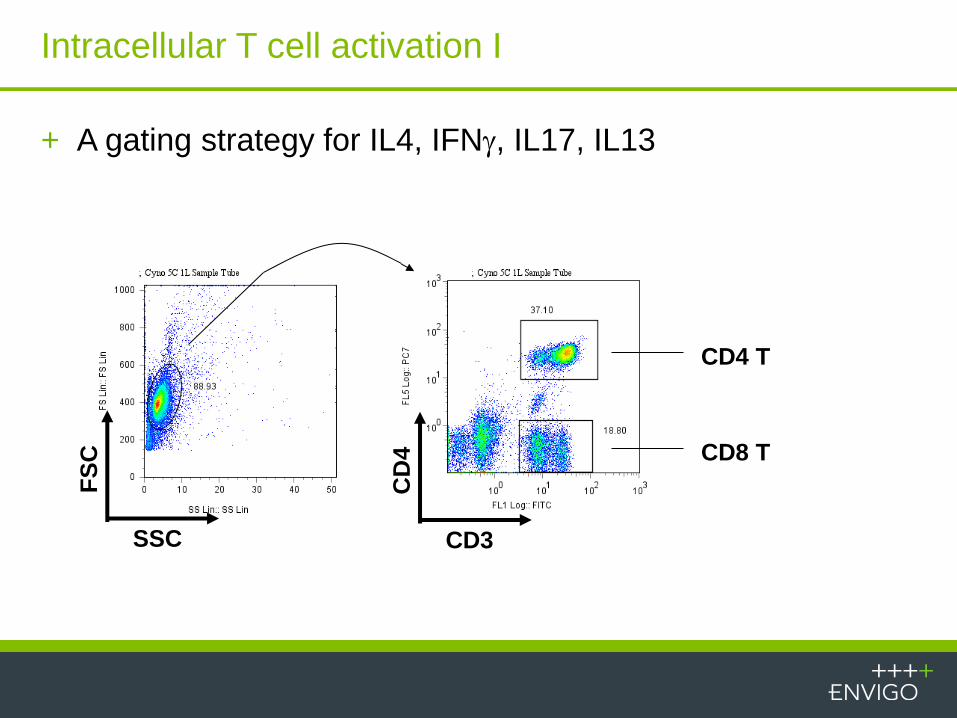
CD8 T
CD4 T
CD3
CD
4
SSC
FS
C
+ A gating strategy for IL4, IFNg, IL17, IL13
Intracellular T cell activation I

+ Expression of IFNg in CD4T and CD8 T cells
Intracellular T cell activation II
CD4 T CD8 T
Unstim
Stim.
IL4
IFN
g

+ Expression of IL17 in CD4 T cells
Intracellular T cell activation III
Unstim
Stim.
IL17
IL13
CD4 T CD8 T

Control Dosed
IL-4
IFN
-g
Draining
LN
Non-
Draining LN
PBMC
Intracellular expression of IL-4 and IFNg in total CD3 T
lymphocytes

Intracellular expression of IL-4 and IFNg in CD4 T
lymphocytes
Control Dosed
IL-4
IFN
-g
Draining
LN
Non-
Draining LN
PBMC

Intracellular expression of IL-4 and IFNg in CD8 T
lymphocytes
Control Dosed
IL-4
IFN
-g
Draining
LN
Non-
Draining LN
PBMC

TEM
TCM
TNaive
TEM
TCM
TNaive
Cyno DTH - increased TEM in CD8+
Case study – What if your chosen therapeutic has no
pharmacologically relevant non-clinical safety
species?

+ The novel antibody needs a safety package but does not
bind to the checkpoint inhibitor (CPI) in any standard
toxicity species
+ An academic group has a transgenic mouse model
expressing the CPI (KO/KI) that may be suitable for safety
assessment of the therapeutic
+ The transgenic model is a good well characterised one,
the transgene expression and distribution of the CPI is
consistent with the human expression profile
+ Initiated a project to breed the transgenic mouse for use in
toxicity studies
Challenges with a checkpoint blocking antibody

+ The transgenic mouse model is on a C57BL/6N
background + One mutation is x-linked
+ One mutation is somatic
+ Currently maintained in academic institution with
unacceptable health status and poor availability due to
small colony size
Transgenic mouse model background

+ Rederive model to acceptable health status
+ Develop breeding colony + Genetic testing required to confirm genotype in offspring and future breeders
+ Model maintained mating heterozygous / hemizygous males x heterozygous /
homozygous females
+ Expand colony for provision of acceptable numbers of
animals at requested frequency
Next steps

Breeder genotype
FEMALE BREEDER
n/+
XmXm
MALE BREEDER
n/+
XmY

n
Xm
n
Xm
+
Xm
+
Xm
n
Y
n/n
XmY
n/n
XmY
n/+
XmY
n/+
XmY
n
Xm
n/n
XmXm
n/n
XmXm
n/+
XmXm
n/+
XmXm
+
Y
n/+
XmY
n/+
XmY
+/+
XmY
+/+
XmY
+
Xm
n/+
XmXm
n/+
XmXm
+/+
XmXm
+/+
XmXm
Preferred mating scheme
Female (n/+ XmXm)
Male
(n/+
Xm
Y)
+ 50% to be selected as
future breeders
+ 25% proper genotype for
research studies
+ 25% discarded due to
incorrect genotype

+ Colony mice positive for pinworms and Helicobacter spp
+ 5 x 10 breeding pairs provided for rederivation via embryo transfer
+ Females superovulated; embryos collected, pooled, washed, then surgically transferred into recipient pseudopregnant females of an approved health status
+ Pups born and genotyped; health monitoring performed to confirm approved health status
+ 4 females and 6 males provided
Rederivation

+ Breeding pairs received into flexible
film isolator to maintain approved
health status
+ Based on feedback from original
institution, mice maintained on 18%
protein, 6% fat diet and wood pulp
bedding
+ Mice maintained for six weeks with
only three females pregnant and one
cannibalized litter
Develop breeding colony

+ Housing and husbandry reviewed; mice switched to higher
fat diet (19% protein, 9% fat) and crinkle paper enrichment
added to cages
+ The addition of enrichment and diet change improved
breeding; however, two females died unexpectedly, leaving
6 breeding males and 2 breeding females in the
Foundation Colony
Root cause analysis #1
+ Concept of backcrossing discussed with geneticist
+ C57BL/6N females at an approved health status were
available
+ Females were introduced into male breeding cages (1x2)
+ Breeding efficiency improved, but now more extensive
record keeping and genetic testing needed to confirm
which mice are acceptable for future breeder selection
Root cause analysis #2

+
X+
n
Xm
n/+
XmX+
n
Y
n/+
X+Y
+
Xm
+/+
XmX+
+
Y
+/+
X+Y
Backcross generation 1
Female (+ X+)
Male
(n/+
Xm
Y)
+ 50% to be selected as
future breeders
+ 50% discarded due to
incorrect genotype
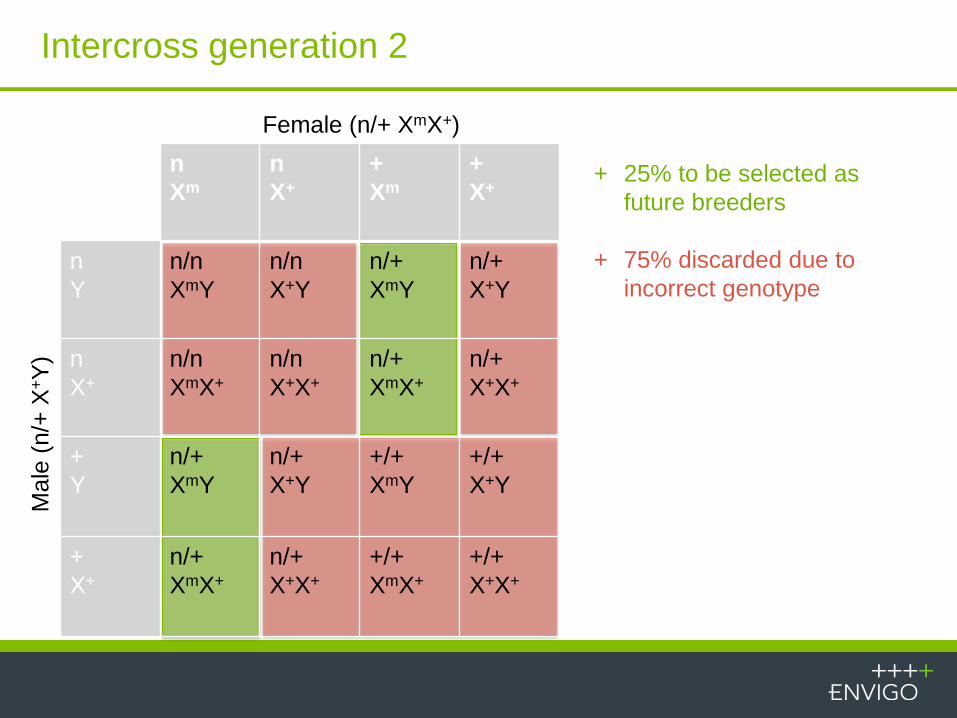
Intercross generation 2
Female (n/+ XmX+)
Male
(n/+
X+Y
)
+ 25% to be selected as
future breeders
+ 75% discarded due to
incorrect genotype
n
Xm
n
X+
+
Xm
+
X+
n
Y
n/n
XmY
n/n
X+Y
n/+
XmY
n/+
X+Y
n
X+
n/n
XmX+
n/n
X+X+
n/+
XmX+
n/+
X+X+
+
Y
n/+
XmY
n/+
X+Y
+/+
XmY
+/+
X+Y
+
X+
n/+
XmX+
n/+
X+X+
+/+
XmX+
+/+
X+X+

Intercross generation 3
Female (n/+ XmX+)
Male
(n/+
Xm
Y)
+ 25% to be selected as
future breeders
+ 12.5% proper genotype for
research studies
+ 62.5% discarded due to
incorrect genotype
n
X+
n
Xm
+
X+
+
Xm
n
Y
n/n
X+Y
n/n
XmY
n/+
X+Y
n/+
XmY
n
Xm
n/n
XmX+
n/n
XmXm
n/+
XmX+
n/+
XmXm
+
Y
n/+
X+Y
n/+
XmY
+/+
X+Y
+/+
XmY
+
Xm
n/+
XmX+
n/+
XmXm
+/+
XmX+
+/+
XmXm
+ Backcross complete!
+ Adequate number of future breeders available to expand
colony rapidly
+ Genetic testing still necessary to confirm pups carrying
transgenes
+ Health monitoring performed quarterly to ensure
appropriate health status
Colony expansion

+ CPI expressed on activated T lymphocytes
+ Harvest spleens from naïve and transgenic mice
+ Stimulate with PMA + Ionomycin for 24 hours
+ Flow cytometry analysis of activated T lymphocytes to
evaluate endogenous and human CPI
Verification of CPI expression in T cells of Tg mouse

FSC-A
SS
C-A
0 65536 196608-2523
63644
129810
195977
262144
LM
FSC-W
FS
C-A
0 65536131072 2621440
65536
131072
196608
262144
Single_Cells
CD3AF488 FITC-A
Count
100
101
102
103
104
105
0
298
596
893
1191
T Cells
Single Cells Lymphocytes T Lymphocytes
Verification of CPI expression in T cells of Tg mouse:
Gating Strategy

PD-1 PerCP-Cy5-5-A
Count
100
101
102
103
104
105
0
9
19
28
37
CPI,
30.26
PD-1 PerCP-Cy5-5-A
Count
100
101
102
103
104
105
0
60
119
179
238
CPI,
1.75
PD-1 PerCP-Cy5-5-A
Count
100
101
102
103
104
105
0
8
16
24
32
CPI,
44.59
Isotype PerCP-Cy5-5-A
Count
100
101
102
103
104
105
0
10
19
29
38
CPI,
0.09
Naïve Mouse Transgenic
Mouse
Mouse CPI
Human CPI
no
endogenous
expression
Transgene
expressed
Verification of CPI expression in T cells of Tg mouse
CPI CPI
CPI

CD4 PE-A
CD
8 V
500-A
-103
-102
103
104
105
-102
102
103
104
105
CD4 T
CD8 T
CD28 PE-Cy7-A
CD
95
V4
50
-A
-10210
210
310
410
5
-102
102
103
104
105
46.72%0.38%
42.80%10.10%
FoxP3 PE-A
CD
25
Pa
cific
Blu
e-A
-10210
210
310
410
5
-102
102
103
104
105 CD4TregFoxP3
CD3+CD4+
T helper
CD3+CD4+
T helper
(total T)
CD
25
CD
62L
CD
8
CD4 FoxP3 CD44
T naive Tcm Tem CD8 T CD4 T T reg
Other T cell subsets evaluated for CPI expression

Rederivation
•~ 3 months
Breeding Colony Development
•~ 3 months
Backcrossing Project
•~ 6 months
Colony Expansion
•~ 5 months
Receipt of Animals
Conclusions
0 3 6 9 15 18
+ Process is time consuming and labor intensive
+ Genetic testing and proper record keeping paramount to success of
colony development and expansion
+ Provision of high quality mice approximately 17 months after initiation
of project

Summary

+ Immunomodulatory biologics are increasing in complexity
+ A translational approach to safety assessment with focus
upon the biologics mechanism of action is essential in
designing fit for purpose safety packages
+ Although standard species offer enormous value in
determining the safety profiles of drugs that target CPIs,
new approaches are being considered all the time to
produce clinically translatable data
+ Biology…biology…biology…
Summary

Thank You