img.medscape.comimg.medscape.com/images/828/240/828240_slide.pdf · multiple sclerosis (ms) 101 •...
TRANSCRIPT





Balancing the Risks and
Benefits of Therapy
Scott Newsome, DO
Assistant Professor of Neurology
Director, Neurology Outpatient Services
Johns Hopkins University School of Medicine
Outline
• Multiple Sclerosis (MS) 101
• Clinically Isolated Syndrome (CIS)
• Disease-modifying Therapy Efficacy
• Disease-modifying Therapy Adverse Effects
and Monitoring
Multiple Sclerosis (MS) 101
• Immune-mediated disease of the central nervous
system that is associated with inflammation,
demyelination, axonal loss, and neurodegeneration
• Primary etiology unknown, but likely multifactoral
• Most common cause of nontraumatic disability in
18- to 60-year-old population
• Female predominance with peak incidence between
20 and 40 years old
• Risk factors: low vitamin D, viruses, genetics, smoking,
overweight/obesity, environmental exposures, etc.Calabresi PA, Newsome SD. Multiple Sclerosis; Neurology for the Non-Neurologist. 6th ed.
Lippincott Williams & Wilkins, 2010; 192-221.
Ascherio, A. Expert Rev. Neurother. 2013;13(12 Suppl):3-9.

Relapsing-Remitting
Secondary Progressive
Preclinical
Time
Measures of brain volume
Relapses and impairment
MRI burden of disease
MRI activity
Axonal loss
Natural History of MS: Summary
Adapted from Goodkin DE. UCSF MS Curriculum. 1999.
Clinically Isolated Syndrome (CIS)
• CIS is an individual’s initial neurological episode that
occurs due to CNS inflammation/demyelination
• CIS can be:
– A first attack of MS
– An isolated idiopathic episode
– Secondary to another condition (eg, lupus)
• Usually monosymptomatic (eg, optic neuritis), but can
be polysymptomatic
• Can diagnose MS after a single attack with 2010
McDonald criteriaMarcus J, Waubant E. Neurohospitalist. 2013; 3(2): 65–80.
Frohman EM, et al. Arch Neurol. 2006;63(4):614-619.
Polman CH, et al. Ann Neurol. 2011;69(2):292-302.
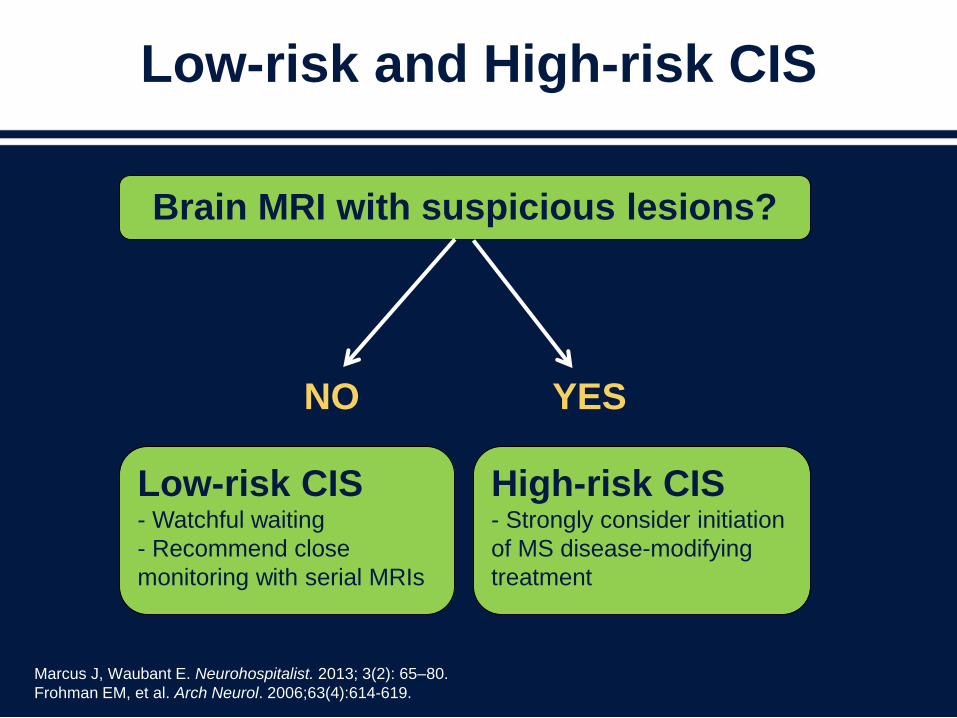
Low-risk and High-risk CIS
Brain MRI with suspicious lesions?
Low-risk CIS- Watchful waiting
- Recommend close
monitoring with serial MRIs
High-risk CIS- Strongly consider initiation
of MS disease-modifying
treatment
NO YES
Marcus J, Waubant E. Neurohospitalist. 2013; 3(2): 65–80.
Frohman EM, et al. Arch Neurol. 2006;63(4):614-619.
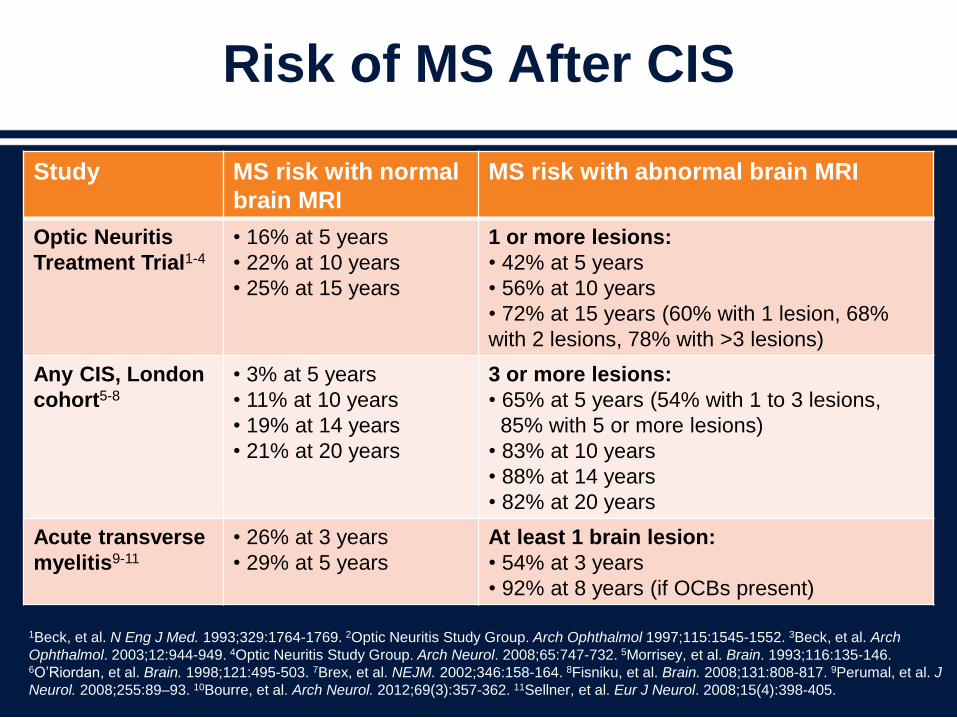
Risk of MS After CIS
1Beck, et al. N Eng J Med. 1993;329:1764-1769. 2Optic Neuritis Study Group. Arch Ophthalmol 1997;115:1545-1552. 3Beck, et al. Arch
Ophthalmol. 2003;12:944-949. 4Optic Neuritis Study Group. Arch Neurol. 2008;65:747-732. 5Morrisey, et al. Brain. 1993;116:135-146. 6O’Riordan, et al. Brain. 1998;121:495-503. 7Brex, et al. NEJM. 2002;346:158-164. 8Fisniku, et al. Brain. 2008;131:808-817. 9Perumal, et al. J
Neurol. 2008;255:89–93. 10Bourre, et al. Arch Neurol. 2012;69(3):357-362. 11Sellner, et al. Eur J Neurol. 2008;15(4):398-405.
Study MS risk with normal
brain MRI
MS risk with abnormal brain MRI
Optic Neuritis
Treatment Trial1-4
• 16% at 5 years
• 22% at 10 years
• 25% at 15 years
1 or more lesions:
• 42% at 5 years
• 56% at 10 years
• 72% at 15 years (60% with 1 lesion, 68%
with 2 lesions, 78% with >3 lesions)
Any CIS, London
cohort5-8
• 3% at 5 years
• 11% at 10 years
• 19% at 14 years
• 21% at 20 years
3 or more lesions:
• 65% at 5 years (54% with 1 to 3 lesions,
85% with 5 or more lesions)
• 83% at 10 years
• 88% at 14 years
• 82% at 20 years
Acute transverse
myelitis9-11
• 26% at 3 years
• 29% at 5 years
At least 1 brain lesion:
• 54% at 3 years
• 92% at 8 years (if OCBs present)
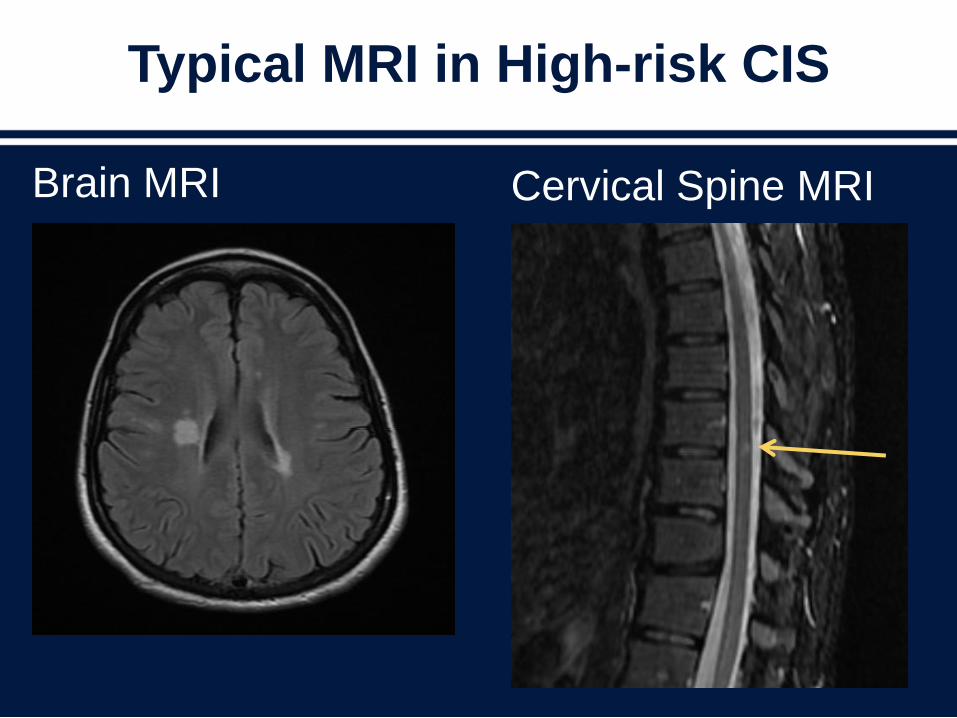
Typical MRI in High-risk CIS
Brain MRI Cervical Spine MRI
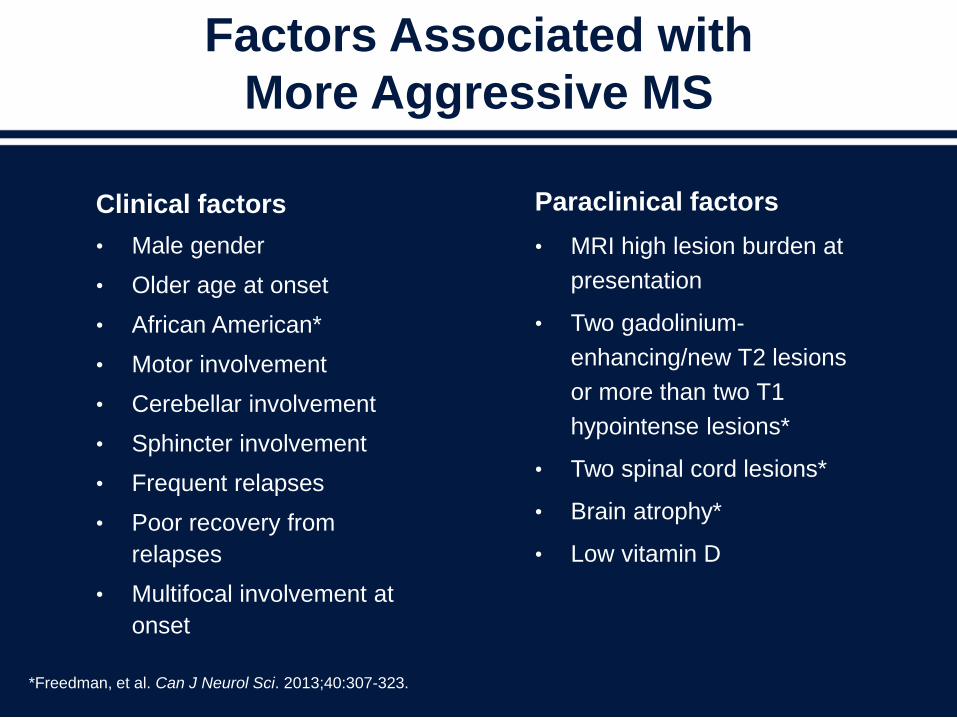
Factors Associated with
More Aggressive MS
Clinical factors
• Male gender
• Older age at onset
• African American*
• Motor involvement
• Cerebellar involvement
• Sphincter involvement
• Frequent relapses
• Poor recovery from
relapses
• Multifocal involvement at
onset
Paraclinical factors
• MRI high lesion burden at
presentation
• Two gadolinium-
enhancing/new T2 lesions
or more than two T1
hypointense lesions*
• Two spinal cord lesions*
• Brain atrophy*
• Low vitamin D
*Freedman, et al. Can J Neurol Sci. 2013;40:307-323.
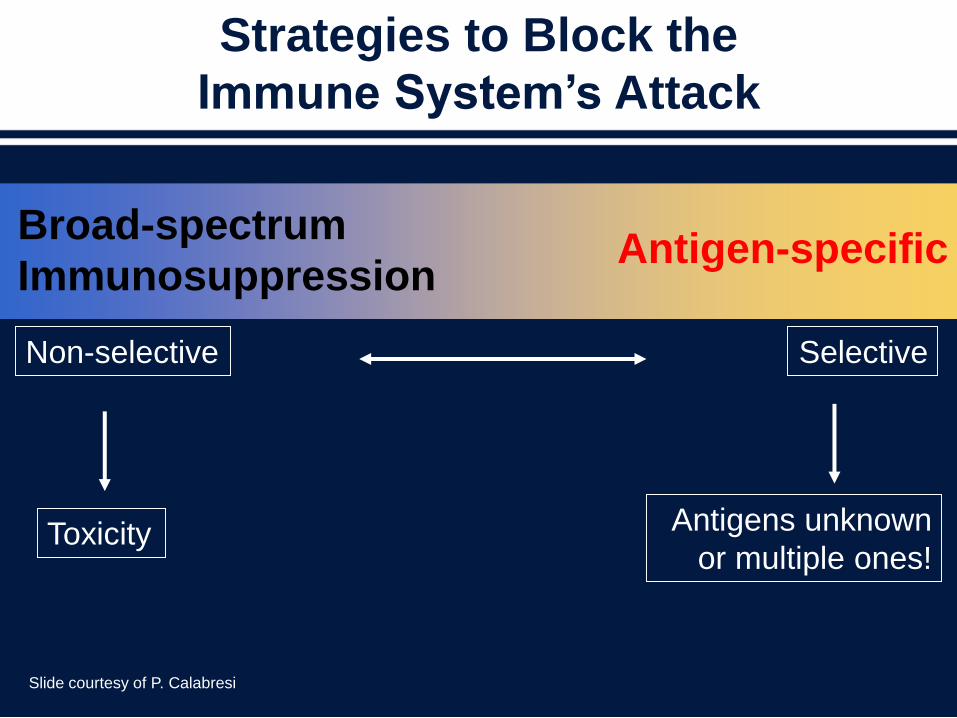
Non-selective Selective
Antigen-specificBroad-spectrum
Immunosuppression
Toxicity Antigens unknown
or multiple ones!
Strategies to Block the
Immune System’s Attack
Slide courtesy of P. Calabresi

Currently Approved MS Disease-modifying Therapies
Generic Name (Brand Name) Approval
Year
Route Known Main Mechanism(s) of Action
IFNβ-1b (Betaseron) 1993 SC QODReduce T-cell activation/proliferation, reduce
secretion of MMPs, inhibit interferon gamma
release, and reduce expression of HLA
IFNβ-1a (Avonex) 1996 IM QW Same as above
Glatiramer acetate (Copaxone) 1996 SC QD Th1 to Th2 shift & blocking MHC peptide antigen
Mitoxantrone (Novantrone) 2000IV every 3
months
DNA topoisomerase II inhibitor; suppresses
proliferation of T cells, B cells, and macrophages
IFNβ-1a (Rebif) 2002 SC TIW Same as other interferon agents
Natalizumab (Tysabri) 2004IV
monthly
Targets alpha-4 integrin on immune cells which
prevents cell interaction with vascular endothelium
and transmigration into CNS
IFNβ-1b (Extavia) 2009 SC QOD Same as other interferon agents
Fingolimod (Gilenya) 2010 PO QD
Sphingosine 1-phosphate receptor modulator;
prevents activated lymphocytes egress out from
secondary lymphoid organs to peripheral
circulation
Teriflunomide (Aubagio) 2012 PO QDInhibits dihydro-orotate dehydrogenase; decreases
proliferation of activated immune cells
Dimethyl fumarate (Tecfidera) 2013 PO BIDTh1 to Th2 shift & activates Nrf2 transcriptional
pathway
Glatiramer acetate (Copaxone) 2014 SC TIW Same as Glatiramer acetate above
See prescribing information for each agent; O'Connor PW, Oh J. Handb Clin Neurol. 2014;122:465-501.

Disease-modifying Treatment in High-risk CIS
Agent Study Name Entry Criteria Results
IM IFNβ-1a 30 mcg
weekly (Avonex)
CHAMPS/CHAMPIONS(NEJM. 2000;343:898-904;
Neurology. 2006;66: 678-684)
2 or more MRI
lesions
Lower rate of MS dx at
3 years (35% vs. 50%)
SC IFNβ-1a 22 mcg
weekly (low-dose
Rebif)
ETOMS(Lancet. 2001;357:1576-1582)
4 or more MRI
lesions or 3
lesions if one
enhancing or
infratentorial
Lower rate of MS dx at
2 years (34% vs. 45%)
SC IFNβ-1a 44 mcg
TIW (Rebif)
REFLEX(Lancet. 2012;11:33-41)
2 or more MRI
lesions
Lower rate of MS dx at
2 years (21% vs. 38%)
SC IFNβ-1b 250 mcg
qod (Betaseron)
BENEFIT (Neurology. 2006;67: 1242-
1249; Lancet. 2007;370:389-
397)
2 or more MRI
lesions
Lower rate of MS dx at
2 years (28% vs. 45%);
decreased disability
development
Glatiramer acetate
20 mg SC daily
(Copaxone)
PreCISe(Lancet. 2009;374:1503-1511)
2 or more lesions Lower rate of MS
diagnosis
(45% reduction at 36
months)

Disease-modifying Therapy Efficacy
Agent Relapse MRI
12-week
Disability
Progression
Initial Pivotal
Clinical Trials
(Placebo Controlled)
IFNβ-1a (low dose) ARR: ↓ 18%Gd+ lesions: ↓50%
T2 lesions: no effect↓ 37%
Multiple Sclerosis Collabrative
Research Group. Ann Neurol.
1996;39(3):285-294.
IFNβ-1a (high dose) ARR: ↓ 33% Gd+ lesions: ↓84%
T2 lesions: ↓78%↓ 30%
PRISMS. Lancet. 1998;352:
1498–1504.
IFNβ-1b ARR: ↓ 34% Gd+ lesions: ↓83%
T2 lesions: ↓75%
Barely
significant
IFNB Multiple Sclerosis Study
Group. Neurology. 1993;43(4):
655-661.
Glatiramer acetate ARR: ↓ 29%Not adequately
assessedNot significant
Copolymer 1 Multiple Sclerosis
Study Group. Neurology
1995;45:1268-1276.
Natalizumab ARR: ↓ 68%Gd+ lesions: ↓92%
T2 lesions: ↓83%↓42%
AFFIRM. N Engl J Med.
2006;354(9):899-910.
Mitoxantrone
(12 mg/m2)ARR: ↓ 68%
Gd+ lesions: + trend
T2 lesions: ↓85%↓43%
MIMS Trial. Lancet. 2002;360:
2018–2025.
Fingolimod ARR: ↓ 54%Gd+ lesions: ↓82%
T2 lesions: ↓74%↓ 32%
FREEDOMS. N Engl J Med.
2010;362:387-401.
Teriflunomide
(14 mg)ARR: ↓ 32%
Gd+ lesions: ↓80%
Lesion volume: ↓67%↓ 30%
TEMSO. N Engl J Med.
2011;365:1293-1303.
Dimethyl fumarate ARR: ↓ 53%Gd+ lesions: ↓90%
T2 lesions: ↓85%↓ 38%
DEFINE. N Engl J Med.
2012;367:1098-1107.
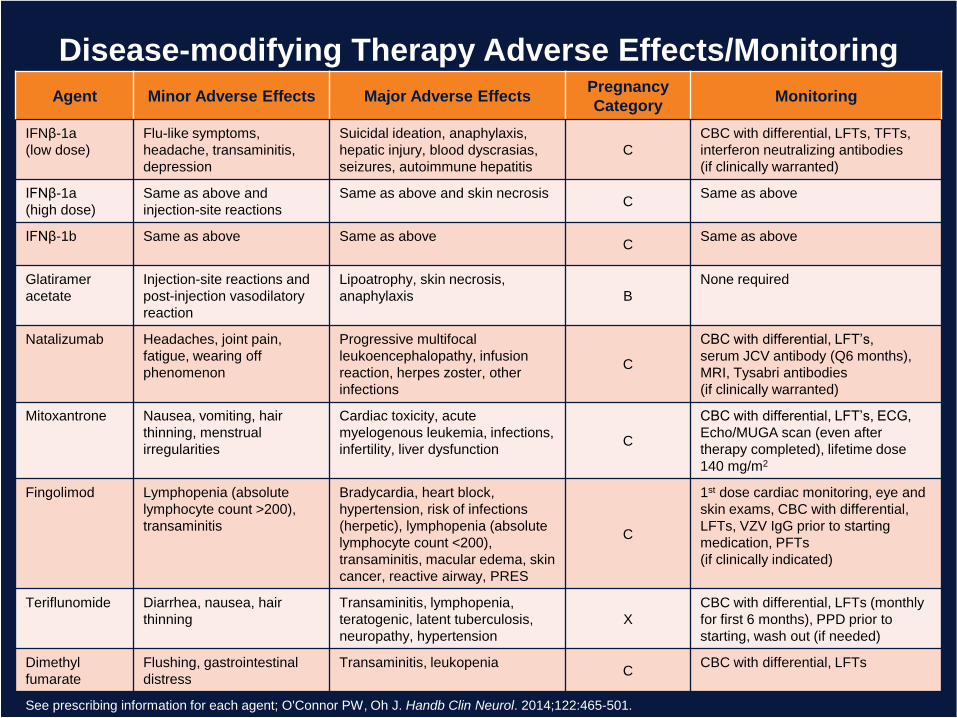
Disease-modifying Therapy Adverse Effects/Monitoring
Agent Minor Adverse Effects Major Adverse EffectsPregnancy
CategoryMonitoring
IFNβ-1a
(low dose)
Flu-like symptoms,
headache, transaminitis,
depression
Suicidal ideation, anaphylaxis,
hepatic injury, blood dyscrasias,
seizures, autoimmune hepatitis
C
CBC with differential, LFTs, TFTs,
interferon neutralizing antibodies
(if clinically warranted)
IFNβ-1a
(high dose)
Same as above and
injection-site reactions
Same as above and skin necrosisC
Same as above
IFNβ-1b Same as above Same as above C
Same as above
Glatiramer
acetate
Injection-site reactions and
post-injection vasodilatory
reaction
Lipoatrophy, skin necrosis,
anaphylaxis B
None required
Natalizumab Headaches, joint pain,
fatigue, wearing off
phenomenon
Progressive multifocal
leukoencephalopathy, infusion
reaction, herpes zoster, other
infections
C
CBC with differential, LFT’s,
serum JCV antibody (Q6 months),
MRI, Tysabri antibodies
(if clinically warranted)
Mitoxantrone Nausea, vomiting, hair
thinning, menstrual
irregularities
Cardiac toxicity, acute
myelogenous leukemia, infections,
infertility, liver dysfunctionC
CBC with differential, LFT’s, ECG,
Echo/MUGA scan (even after
therapy completed), lifetime dose
140 mg/m2
Fingolimod Lymphopenia (absolute
lymphocyte count >200),
transaminitis
Bradycardia, heart block,
hypertension, risk of infections
(herpetic), lymphopenia (absolute
lymphocyte count <200),
transaminitis, macular edema, skin
cancer, reactive airway, PRES
C
1st dose cardiac monitoring, eye and
skin exams, CBC with differential,
LFTs, VZV IgG prior to starting
medication, PFTs
(if clinically indicated)
Teriflunomide Diarrhea, nausea, hair
thinning
Transaminitis, lymphopenia,
teratogenic, latent tuberculosis,
neuropathy, hypertension
X
CBC with differential, LFTs (monthly
for first 6 months), PPD prior to
starting, wash out (if needed)
Dimethyl
fumarate
Flushing, gastrointestinal
distress
Transaminitis, leukopeniaC
CBC with differential, LFTs
See prescribing information for each agent; O'Connor PW, Oh J. Handb Clin Neurol. 2014;122:465-501.
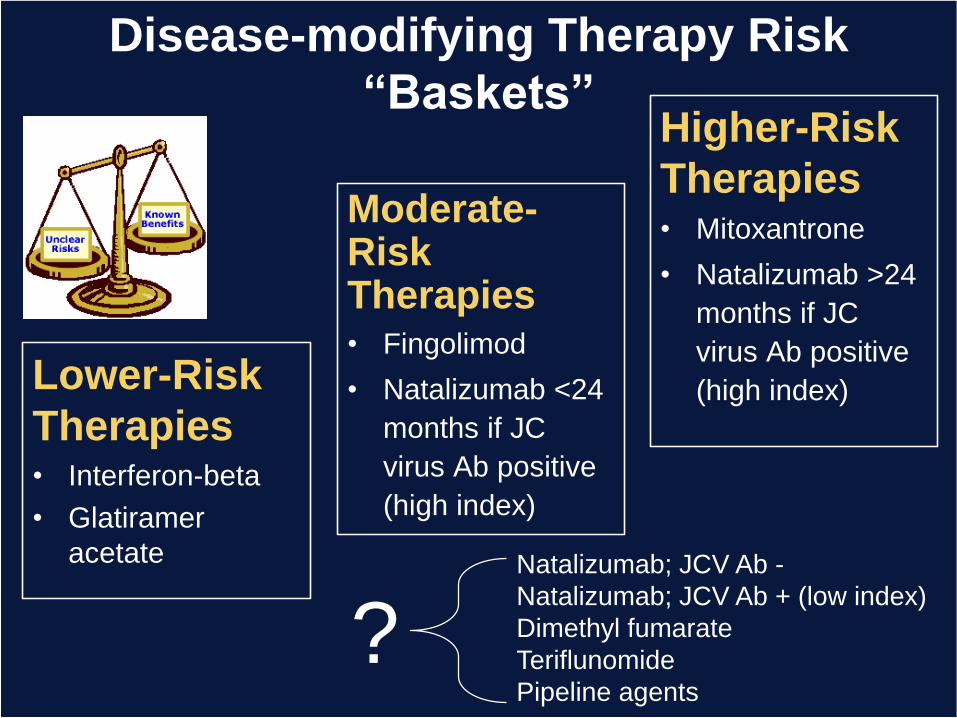
Lower-Risk
Therapies• Interferon-beta
• Glatiramer
acetate
Moderate-Risk Therapies• Fingolimod
• Natalizumab <24
months if JC
virus Ab positive
(high index)
Higher-Risk
Therapies• Mitoxantrone
• Natalizumab >24
months if JC
virus Ab positive
(high index)
Natalizumab; JCV Ab -
Natalizumab; JCV Ab + (low index)
Dimethyl fumarate
Teriflunomide
Pipeline agents
?
Disease-modifying Therapy Risk
“Baskets”

Conclusions
• MS therapeutics is dynamic and becoming
more complicated (↑ efficacy = ↑ risks)
• Low-risk CIS needs close monitoring while
high-risk CIS should be treated
• Clinical and MRI data are critical for
assessing treatment success or failure
• Ongoing need to balance efficacy and
safety of therapeutic interventions
CASE: 32-year-old Woman
• A 32-year-old woman with migraine headaches and
a brain MRI suggestive of CNS demyelination
• Referred for an abnormal brain MRI
• She has had occasional migraine headaches since
adolescence but recently developed more frequent
headaches several times a month prompting an
MRI by her primary physician to rule out a tumor or
vascular anomaly

CASE: Continued
• Probing questioning elicits no history of
prior neurologic symptoms other than the
headaches and some associated visual
scintillations
• She is otherwise healthy
• Neurological exam is normal
CASE: Continued
• Brain MRI shows ten T2 lesions in the periventricular,
and central hemispheric white matter
– Three lesions are ovoid and have the appearance of
“Dawson’s fingers”
– One lesion is juxta-cortical
– None of the lesions enhance following contrast infusion
• MRI of the cervical spinal cord obtained and is normal
• Serologic and metabolic testing for conditions
associated with white matter lesions reveals no
abnormalities

Your diagnosis would be:
1. Multiple sclerosis
2. Clinically isolated syndrome
3. Radiologically isolated syndrome
4. Other

If this patient had a silent partial segmental lesion in
the cervical spinal cord, but still had a normal
neurological examination, your next step be:
1. Spinal fluid exam
2. Start treatment with a disease modifying
agent
3. Repeat the brain MRI in 6 months
CASE: Continued
• The patient is not treated with a DMT
• Treated with a beta blocker and a change in birth
control pills results in reduction in the frequency of her
migraine headaches
• Six months later, a follow-up MRI of the brain shows a
new T2 hyper-intensity in the left central white matter
which does not enhance following contrast infusion
– She has had no new neurological symptoms
– Her neurological exam still normal
– She has no spinal cord lesion

Your next step would be:
1. Spinal fluid exam
2. Start treatment with a disease modifying
agent
3. Repeat the brain MRI in another 6 months
CASE: For the Panel
• Do you ever treat patients with DMTs on their first presentation
with RIS?
• What factors influence your decision to treat patients with RIS?
• Do you treat patients with RIS on appearance of a new lesion
on follow-up brain MRI regardless of clinical symptoms or
findings?
• Do you believe the natural history of patients with RIS as a
cohort is different from patients presenting with CIS, or is RIS
simply the accidental discovery of a group of patients of whom
most will become symptomatic in the future?
CASE: Summary
• RIS represents the incidental discovery of patients with imaging
characteristics typical of CNS demyelination in whom no clinical
history of symptoms compatible with CNS demyelination is
present, or has occurred in the past
• The long term natural history of such patients is currently
unknown and may differ from the newly identified symptomatic
MS patient, potentially including a group of patients destined to
have clinically benign MS who would not require treatment
• The presence of silent spinal cord disease is known to increase
the likelihood of a future symptomatic demyelinating event in a
patient with RIS
MS Therapeutic Strategies:
What to Use, In Whom, and
When to Switch
Robert Bermel, MD
Staff Neurologist and Medical Director
Mellen Center for Multiple Sclerosis
Cleveland Clinic
Cleveland, OH
The Clinical Situation in RRMS
• We are well-equipped to treat and monitor the
inflammatory component of RRMS
– 10 (11) approved therapies
– Widespread availability of MRI for monitoring
• Early treatment is emphasized
• DMTs are variably effective in individuals
• No biomarker to prospectively predict efficacy of specific
treatments in individual patients
• Choosing and monitoring a therapy (clinically and with
MRI) is common, though there are no standards or
defined targets in the clinic
• Symptomatic treatment and wellness play a large role

Therapeutic Options: 2014
Monitoring off therapy
Injectables:
Interferon beta-1b
Interferon beta-1a IM
Interferon beta-1a SC
Glatiramer acetate qd
Glatiramer acetate tiw
Orals:
Fingolimod
Teriflunimide
Dimethyl fumarate
Infusions/MAbs:
Natalizumab (JCV Ab +)
Natalizumab (JCV Ab -)
Therapeutic Options:
2014 Overly Simplifying Efficacy
Monitoring off therapy
Injectables:
Interferon beta-1b
Interferon beta-1a IM
Interferon beta-1a SC
Glatiramer acetate qd
Glatiramer acetate tiw
Orals:
Fingolimod
Teriflunimide
Dimethyl fumarate
Infusions/MAbs:
Natalizumab (JCV Ab -)
Natalizumab (JCV Ab +)
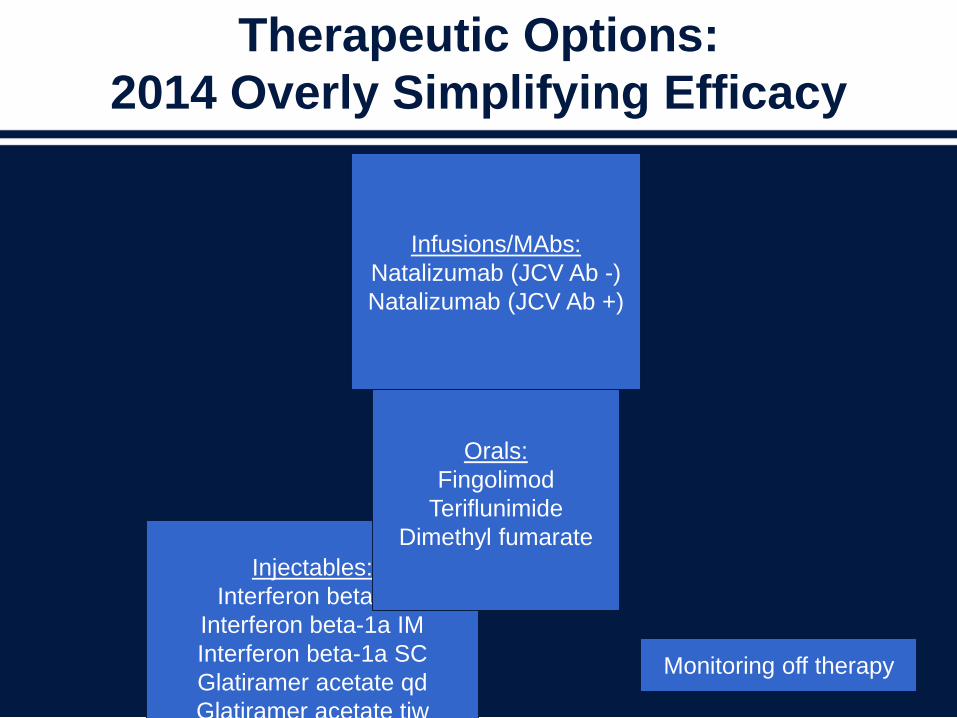
Therapeutic Options:
2014 Overly Simplifying Efficacy
Monitoring off therapy
Injectables:
Interferon beta-1b
Interferon beta-1a IM
Interferon beta-1a SC
Glatiramer acetate qd
Glatiramer acetate tiw
Orals:
Fingolimod
Teriflunimide
Dimethyl fumarate
Infusions/MAbs:
Natalizumab (JCV Ab -)
Natalizumab (JCV Ab +)
Therapeutic Options:
2014 Overly Simplifying Safety
Monitoring off therapy
Injectables:
Interferon beta-1b
Interferon beta-1a IM
Interferon beta-1a SC
Glatiramer acetate qd
Glatiramer acetate tiw
Orals:
Fingolimod
Teriflunimide
Dimethyl fumarate
Infusions/MAbs:
Natalizumab (JCV Ab -)
Natalizumab (JCV Ab +)
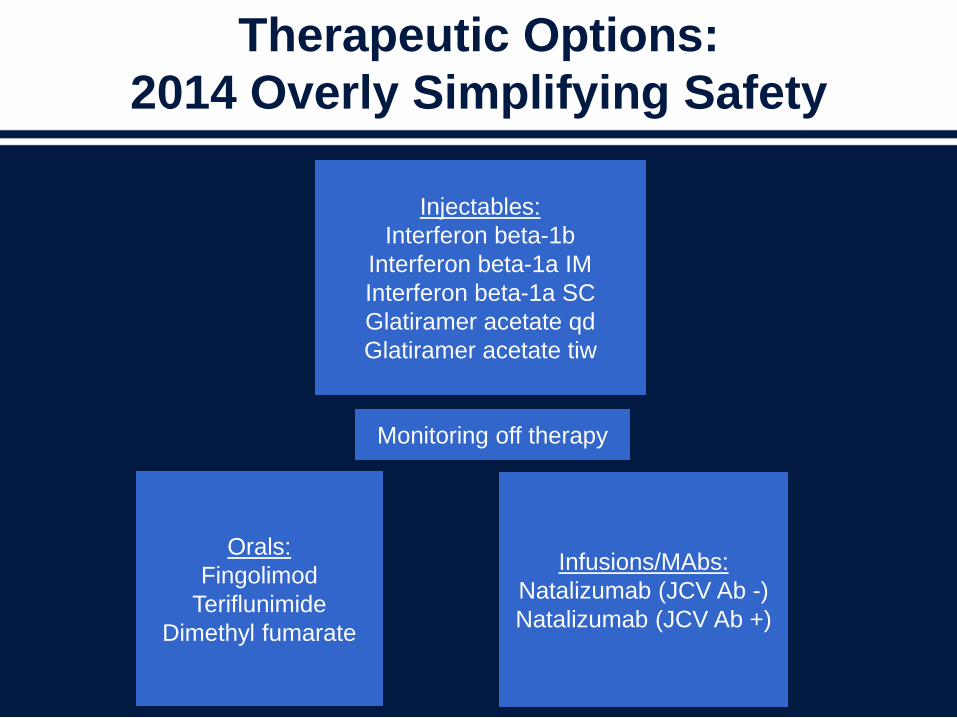
Therapeutic Options:
2014 Overly Simplifying Safety
Monitoring off therapy
Injectables:
Interferon beta-1b
Interferon beta-1a IM
Interferon beta-1a SC
Glatiramer acetate qd
Glatiramer acetate tiw
Orals:
Fingolimod
Teriflunimide
Dimethyl fumarate
Infusions/MAbs:
Natalizumab (JCV Ab -)
Natalizumab (JCV Ab +)

Key Considerations
• Disease severity/burden/prognosis
– Recovery from prior relapses, MRI lesion burden
• Disease activity
– Relapse frequency, MRI activity
• What have they been on in the past?
• JCV Ab status
• Pregnancy plans?
• Patient and physician preference and risk tolerance

Therapeutic Options:
2014 More Realistic
Inje
cta
ble
s:
Inte
rfero
n b
eta
-1b
Inte
rfero
n b
eta
-1a I
M
Inte
rfero
n b
eta
-1a S
C
Gla
tira
mer
aceta
te q
d
Gla
tira
mer
aceta
te t
iw Infu
sio
ns/M
Abs:
Nata
lizum
ab
(JC
V A
b +
)
Nata
lizum
ab
(JC
V A
b -)Individual
Patient
Monitoring off
therapyOrals:
Fingolimod
Teriflunimide
Dimethyl fumarate
How can we evaluate an individualized
treatment plan for success?
Treating to Target in MS
• What do we expect of our current
therapies?
• Do we discuss it with our patients?
• How do we know if we are achieving the
desired result?
• Model from rheumatoid arthritis and
diabetes
One Possible Treatment Target
• No new or enlarging T2 lesions
• No new Gad+ lesions
• No relapses
• No confirmed EDSS worsening
No Evidence of Disease Activity• Previously defined in analysis of clinical trials
• Can it be applied to the MS clinic?
When to Switch?
• Common situations:– Noncompliance
– Symptoms or “Global Impression”
– Definite relapses
– Exam changes/disability progression
– Neutralizing antibodies
– Gad lesions
– New/enlarging T2 lesions
Does subclinical disease activity on treatment matter?

Early MRI Activity on IFN Predicts
Poor Long-term Outcome
Reprinted with Permission from Bermel RA, et al. Ann Neurol. 2013;73(1):95-103.
MRI activity and relapses predicted future disability in patients treated with IFNβ
ASSURANCE Study (15-year f/u of IM IFN beta1a) ─ Results:
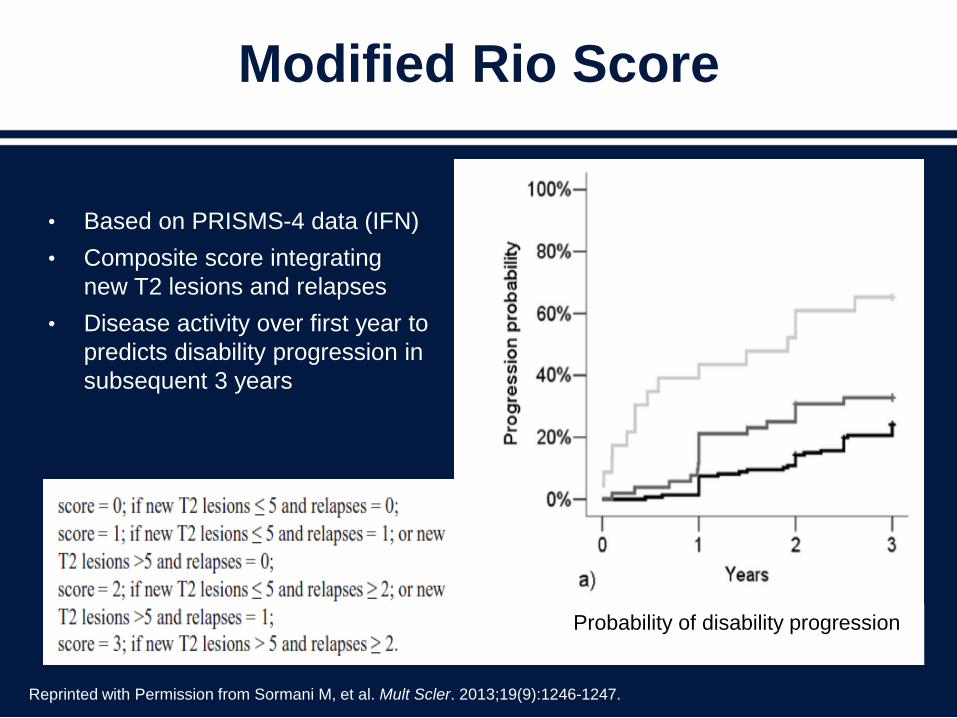
Modified Rio Score
• Based on PRISMS-4 data (IFN)
• Composite score integrating
new T2 lesions and relapses
• Disease activity over first year to
predicts disability progression in
subsequent 3 years
Reprinted with Permission from Sormani M, et al. Mult Scler. 2013;19(9):1246-1247.
Probability of disability progression
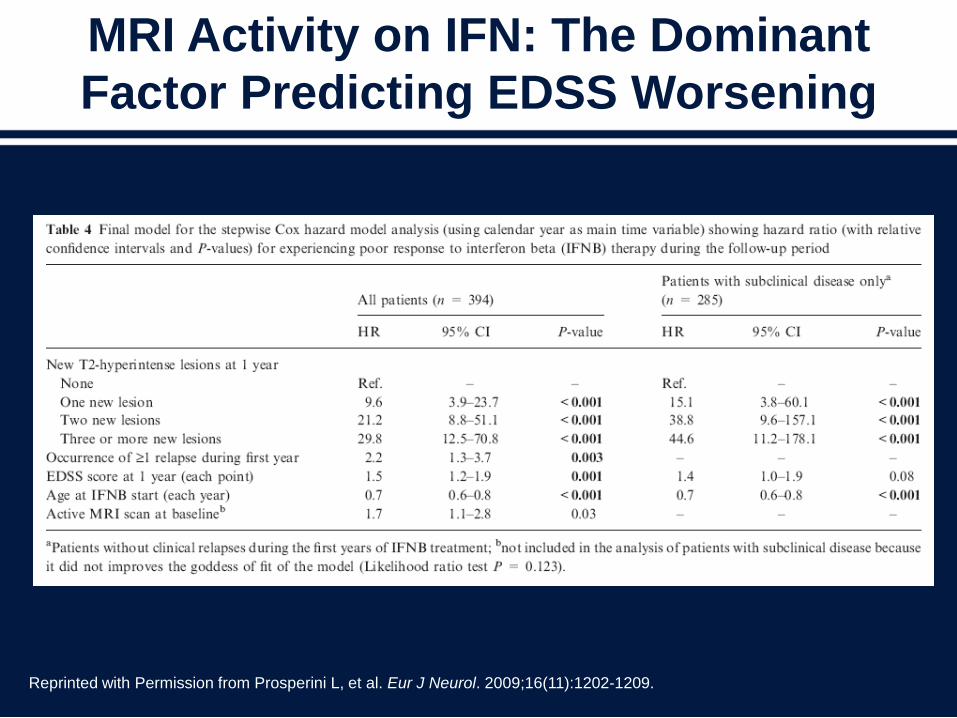
MRI Activity on IFN: The Dominant
Factor Predicting EDSS Worsening
Reprinted with Permission from Prosperini L, et al. Eur J Neurol. 2009;16(11):1202-1209.
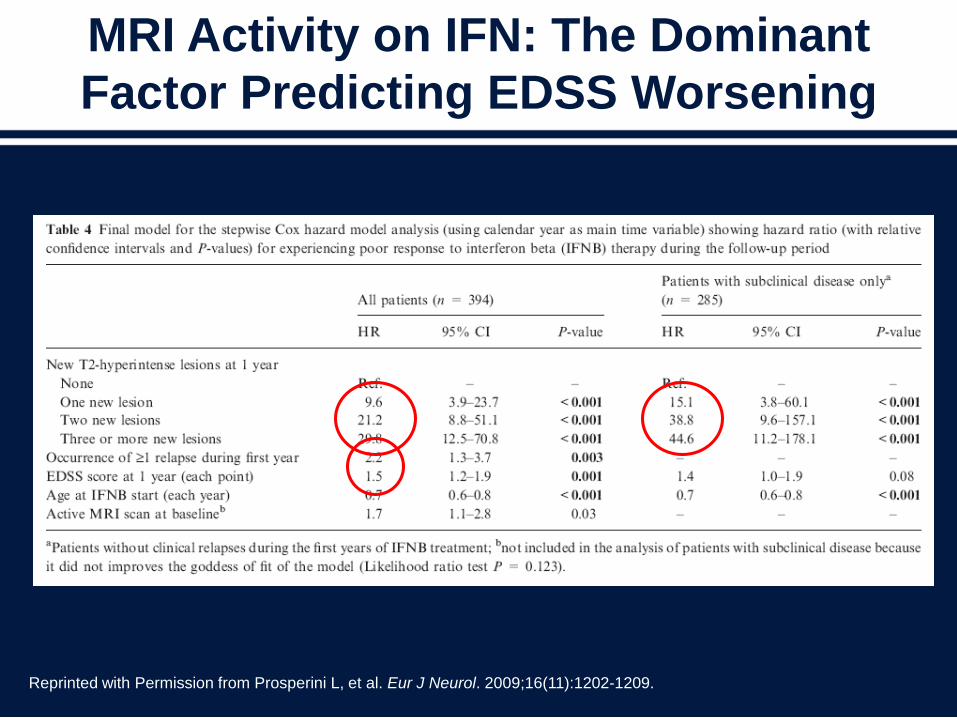
MRI Activity on IFN: The Dominant
Factor Predicting EDSS Worsening
Reprinted with Permission from Prosperini L, et al. Eur J Neurol. 2009;16(11):1202-1209.
Complexities: Monitoring
• Monitoring disease activity is complex
– Reestablishing the baseline for MRI monitoring
– How to appropriately analyze MRI
– No easy way to track the components of NEDA in most
electronic medical records
– Threshold to act (and what to do) is unclear
• Implementing in the clinic may be facilitated by
enlisting radiology colleagues, and using
technology
NEDA=No Evident Disease Activity
A Consistent Strategy
• There is no “one size fits all” treatment
• Choice of initial therapy depends on multiple factors
• Regardless of choice, monitoring for tolerability,
adherence and efficacy is important
• A “treat-to-target” approach may be reasonable, though
more research guiding this strategy is needed
• If breakthrough disease, switching mechanisms of
action makes sense, though largely based on data from
interferon long-term follow-up
• Do not forget symptomatic therapy and wellness

CASE: 27-year-old Woman
• A 27-year-old woman has been taking glatiramer
acetate for the past four and a half years
• Her symptoms began with an episode of optic neuritis
5 years ago
• Her brain MRI showed five T2 hyper-intense lesions
including periventricular lesions with the appearance of
“Dawson’s fingers”
• She was started on interferon beta but did not tolerate
the flu-like symptoms and was switched to glatiramer
acetate
CASE: Continued
• Surveillance brain MRI reveals 2 new lesions compared
to her last image about a year prior
• Prior monitoring MRIs have been stable
• Neurologic exam reveals left optic disc pallor with visual
acuity of 20/25 corrected, and mild vibratory loss in her
left foot, unchanged from her initial exam 6 years ago
• EDSS is 1.5
• No new symptoms since presentation
• No comorbid medical conditions
• Previous imaging of her cervical spinal cord was normal
In counselling this patient, what
would you recommend next?
1. Change in DMT therapy
2. Continuation of current therapy and repeat
brain MRI in 6 months
3. Continuation of current therapy and repeat
brain MRI in a year
4. Repeat cervical MRI
CASE: Continued
• A year goes by and she has another small
new lesion in the right hemispheric white
matter on a follow-up surveillance MRI
• Her exam is unchanged
• She has had no new neurologic symptoms
• She has now been on glatiramer acetate for
5.5 years
At this time what would you advise?
1. Continue glatiramer acetate unless she
has a new clinical event
2. Switch to an alternate DMT
3. Continue to monitor MRIs to see if she
develops more lesions
4. Switch DMTs if a new silent lesion
develops in the brainstem or spinal cord
In a clinically stable mildly affected MS patient,
how many new MRI lesions would prompt you
to switch DMTs?
1. 1
2. 2
3. 3
4. 4
5. 5 or more
6. I would not change treatment based only on new MRI lesions
CASE: For the Panel
• How often do you obtain surveillance MRIs?
• How many lesions are sufficient to prompt you to change DMTs
in a clinically stable patient?
• Does the timing of new lesions in relation to the duration of MS
and the current DMT treatment affect your decision making?
• Does the severity of the patient’s existing (stable) clinical
condition affect your decision making when a new lesion
appears?
• Does any new relapse warrant a switch in DMTs, or does the
duration of stability prior to the event affect your decision?

Adherence: Monitoring,
Achieving, and Optimizing
Kathleen Costello, ANP-BC, MSCN, MSCS
National Multiple Sclerosis Society
Johns Hopkins Medicine
New Information About Adherence
Really?
Adherence
“The extent to which a person’s behavior –
taking medication, following a diet, and/or
executing lifestyle changes – corresponds
with agreed recommendations from a health
care provider.”1
1World Health Organization. (2003). Adherence to Long-term Therapies: Evidence for Action. Geneva: WHO.

What Do We Know
About Nonadherence?
• The number of patients who are nonadherenthas reached epidemic proportions.1
• 3.8 billion prescriptions written/year yet >50% are taken incorrectly or not at all.2
• A survey of 1000 patients, nearly 75%, admitted to partial or nonadherence.3
• Among the chronically ill, who regularly fill their prescriptions, only 1/2 of the doses are taken.4
1Chesanow N, Medscape. 2014; 2Osterberg L and Blaschke T. NEJM. 2005;353:487-489.3National Council on Patient Information and Education 2007; 4Fischer M, et al. J Gen Intern Med. 2010;25(4):284–90.

Impact on Health
• Increasing the effectiveness of adherence,
interventions may have a greater impact on
long-term health benefits than
improvements in specific medical
treatments.
World Health Organization. (2003). Adherence to Long-term Therapies: Evidence for Action. Geneva: WHO.
Adherence to MS Medications
• A substantial affect (N=2446) on the clinical
and economic impact of adherence to
DMTs
– Less likelihood of hospitalization
– Less likelihood of relapse, particularly severe
relapse
– Less medical costs overall
Tan H, et al. Adv Ther. 2011;28:51-61.

Nonadherence to DMTs
• Several large DMT adherence studies in MS
1. Treadaway K, et al. J Neurol. 2009: N=798
Nonadherence over 3 questionnaire periods or waves:
39%, 37%, and 36%
2. Devonshire V, et al. Eur J Neurol. 2011: N=2648
(4 weeks)
Overall nonadherence: 25%
3. Arroyo E, et al. Eur J Neurol. 2011: N=254 (2 years)
Overall nonadherence: 18%
Reasons Cited for
DMT Nonadherence
1. Forgetting to take the medication
2. Injection related reasons
3. Did not feel like it
4. Lack of perceived benefit
Treadaway K, et al. J Neurol 2009;256:568-576; Devonshire V, et al. Eur J Neurol. 2011;18:69-77;
Arroyo E, et al. Eur J Neurol. 2011;65:59-67.
Adherence to DMTs
• A study of 55 multiple sclerosis patients that looked at
various neuropsychological factors and adherence to
DMTs over an 8-week time frame
• Results indicated that
– MS patients with current mood or anxiety disorders were
nearly 5 times as likely as MS patients with no psychiatric
diagnosis to exhibit problems adhering to treatment.
– Poor adherence was also associated with memory
difficulties, anxiety, depression, neuroticism, and low
conscientiousness.
Bruce J, et al. J Behav Med. 2010;33:219–227.
Adherence to DMTs
• A UK study of 2390 patients, conducted for several years, assessed factors that influence persistence with IFN β-1a SC treatment
• Overall 24% of patients discontinued treatment
• Associated with discontinuation:– Feeling unwell on treatment (adverse effects)
– Feeling poorly informed at the start of treatment
Bruce J, et al. J Behav Med. 2010;33:219–227.
What is Being Done
to Improve Adherence?
• >40,000 peer-reviewed papers on the
subject – yet the estimated rate of poor
adherence has not changed over the past
several decades.
Honigberg R, et al. Utilization Review Accreditation Commission. 2011.
Steps in Initiation and Adherence
1. Prescription written/explained
2. Prescription filled
– The first 6 months are the most critical time for adherence
3. Individual factors for nonadherence
– Forgetfulness (25%)
– Insurance/Cost (17%)
– Adverse events (20%)
– Perception of need (14%)
4. Consider that the patient spends a few hours with the provider
each year – but 5000 hours living without us
– A lot can happen to influence adherence!

HCP Role in Adherence
• Education/re-education
– Purpose
– Expectations
– Adverse effects/management
• Insurance pre-authorization/appeals
• Followup
– Several studies indicate improved adherence with nurse
phone f/u1
• Assess/address individual factors affecting adherence
1Caon C, et al. Journal of Neuroscience Nursing. 2010;42(5 suppl):S5-S9.
Addressing Individual Factors
• Forgetfulness
– Simplified dosing regimen
– Frequent followup
– Maximize support network
– Telephone counseling
• Adverse effects
– Assess ISR
– Aggressively assess and treat
– Change treatment if
interventions exhausted
– Frequent followup
• Treatment fatigue
– Discuss with patient
– Enlist family/other support
– Change treatment if needed
– Motivational interviewing
• Cost
– Assist with resource
identification
– Appeals to insurance
Remington G, et al. International Journal of MS Care. 2013;15:36-45.
Summary
• Adherence continues to be a problem despite our
best efforts
• The MS adherence literature suggests that from
20% to 40% of patients are nonadherent
• Numerous contributing factors have been identified
• Adherence plans that address individual
nonadherence factors, with attention to close
followup may improve adherence to DMTs