imaging in uveitis - conference design
TRANSCRIPT

Imaging in uveitisAnthony Hall

Causes of Vision Loss in Uveitis
1. Cystoid macular oedema 26%
2. Cataract 19%
3. Glaucoma 11%
4. Permanent macular damage 5%
Rothova et al BJO 1996; 80: 332-336

Macular OCT in uveitis
• CMO• 2/3 of uveitis patients
• The leading cause of visual loss
• Drives treatment decisions
• Others• Permanent outer retinal damage
• ERM
• CNVM

Patterns of OCT thickening in uveitis
• A. Cystic
• B. Diffuse
• C. SRF

OCT markers of visual prognosis
• Loss of outer retinal structures• EZ
• Outer limiting membrane

Non CMO causes of visual loss
• ERM
• CNVM
• Retinitis

CNVM

ERM
• ERM
• PTMH
• FTMH

Syphilitic placoid

Ms GH
• 26 yr old 6 days of pain redness and photophobia.
• OH unremarkable
• GH good
• OE Left AAU with normal fundus

• Treatment • Investigation

• Treatment• Intensive topical steroids
• Investigation• U&E
• LFT
• ACE
• VDRL
• HLA B27

• Review at three weeks
• Pain and redness resolved but VA 6/12


Mr DF
• 21 yr old man
• JIA and ongoing uveitis
• Prednisolone, Humira and methotrexate
• Sec cataract and glaucoma

O/E:
OD OS
6/9 VA 6/36
18 IOP 15
++ cells AC ++ cells
++ cells Vitreous ++ cells
No MO DFE
R>L
Apparent MO
OCT


• Managed with left intravitreal TA 4 mg/0.1 ml





RNFL thickness uveitis pts without glaucoma

RNFL thickness uveitis pts with glaucoma

Syphilitic placoid

Pre and post treatment OCT ASPPE

Mr EW
• 65M admitted under ID for non-tuberculous mycobacterial (Mycobacterium chimera) sternal wound + aortic graft infection on b/g of sternotomy for Type A aortic dissection in March 2016• Treated with imipenem, clarythromycin, moxifloxacin
• ID suggest antimicrobial plan: Clarithromycin 500mg BD, moxifloxacin 400mg nocte, rifabutin 300mg mane, Ethambutol 1.2g mane
• Referred to Ophthalmology OPC with mild floaters in R) eye• Nil pain/ LOV

O/E:
OD OS
6/5 VA 6/4
9 IOP 12
17/17 Ishihara 17/17
D+Q AC D+Q
1+ cells Vitreous Nil cells
multifocal deep white lesions in choroid on posterior pole, not affecting
macula/disc
DFE
R>L
multifocal deep white lesions in choroid on posterior pole, not affecting
macula/disc




• 45 yo man with three days of central visual loss
• GH URTI 3 weeks prior
• 6/6 6/60
• RE all clear
• LE vit cells +/-
• Yellow mac lesion with haemorrhage

FA


1 week

6 weeks

Mrs FI
• 59 yr old woman
• 2 yrs progressive visual loss with floaters
• OH unremarkable
• GH good

O/E:
OD OS
6/18 VA 6/18
9 IOP 12
17/17 Ishihara 17/17
1 + cells AC 1 + cells
++ cells Vitreous ++ cells
Multiple pale outer retinal choroidal lesions with pigmentation
DFE Multiple pale outer retinal choroidal lesions with pigmentation
CT


Mr NK
• 59 yr old man
• 10 yrs progressive uveitis and MFC
• OH unremarkable
• GH good


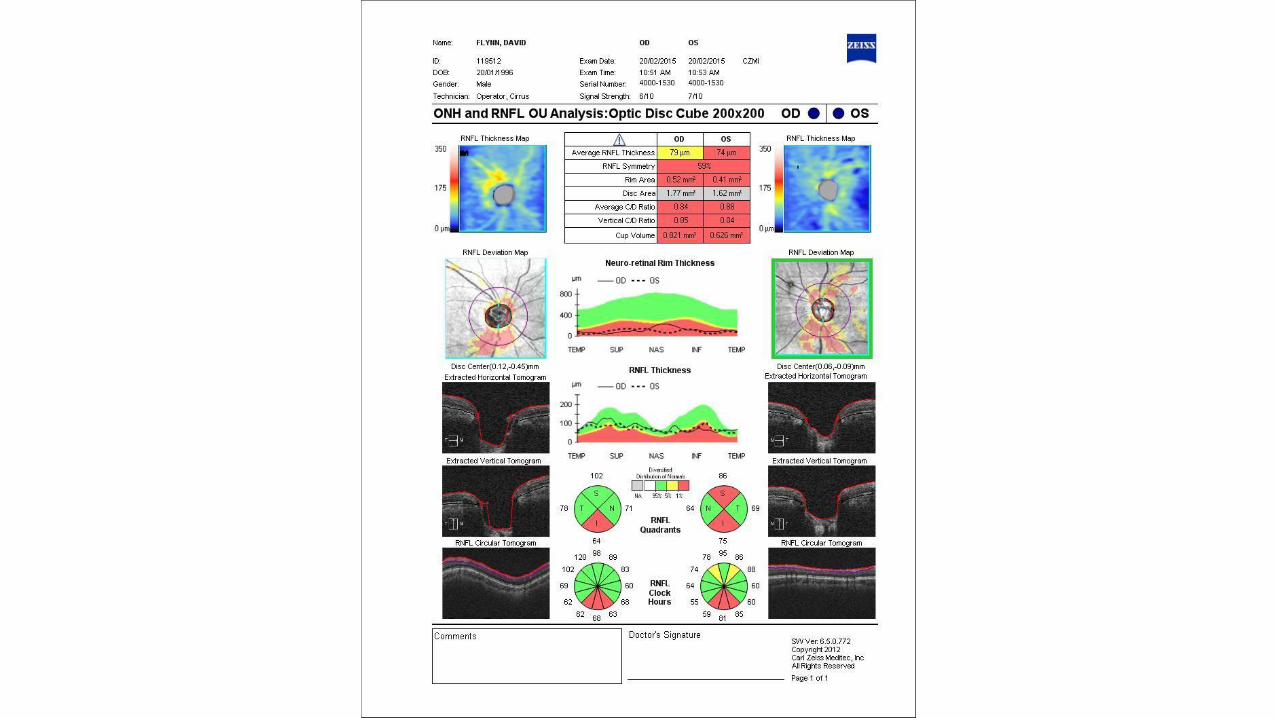
Ms FW
• 28 yr old woman
• URTI followed by painless paracentral scotoma

O/E:
OD OS
6/7.5 VA 6/7.5
9 IOP 12
17/17 Ishihara 17/17
+ cells AC D+Q
1+ cells Vitreous + cells
Confluent pale outer retinal lesions with early pigmentation
DFEConfluent pale outer retinal lesions with
early pigmentation
OCT


Mr TN
• 38 yr old Vietnamese man
• 2 weeks of headache
• 1 Week bilateral central visual loss

O/E:
OD OS
6/36 VA 6/60
7 IOP 5
17/17 Ishihara 17/17
++ cells AC ++ cells
++ cells Vitreous ++ cells
Disc swellingMultifocal cloudy serous detachment
DFE Disc swellingMultifocal serous detachment
OCT


VKH
• Acute phase• Prodrome with HA, meningism,
hearing changes then
• Acute bilat uveitis• Serous detachment
• Disc swelling
• Acutely steroid responsive
• Convalescent phase• Vitiligo and poliosis
• Retinal depigmentation
• Relapsing remitting or chronic uveitis

Mrs VH
• 85 yr old woman presents with 1 week of right sided orbital ache and mild visual loss
• OH bilat cat ext
• GH severe RA, treated with MTX and ritux
• Recent RA related pneumonitis treated with short course of steroids

O/E:
OD OS
6/7.5 VA 6/7.5
9 IOP 12
17/17 Ishihara 17/17
D+Q AC D+Q
1+ cells Vitreous Nil cells
Large single raised mass inferiorly DFE NAD
CT




Causes of Scleritis(n = 188, Foster et al, 1994)
43%
19%
9%
8%
6%
3%
12%
idiopathic
RA
infections
GPA
Rel Pol
PAN/Hep B
Others

Scleritis DDx
Mild Episcleritis, atopy (esp limbal), inflamed pingueculum or pterygium
Moderate HZO, iritis, sinus disease
Severe ACG, HZO, uveitis
Necrotizing SCC, radionecrosis (+/- infection)
Posterior CSR, VKH, uveal effusion syndrome, choroidal primary or secondary,IOI, TED, optic neuritis

Mrs CA
• 31 yr old woman presented with unilateral central distortion

O/E:
OD OS
6/5 VA 6/18
19 IOP 19
D+Q AC D+Q
quiet Vitreous Occ cell only
NAD DFE Multiple quiet flat white lesions around posterior pole
Single raised lesion with surrounding pigment





PIC
• Essex et al
• 136 patients with PIC
• 93% female
• Ave -4 dioptres
• 46% unilateral
• 12% recurrent PIC lesions
• 22% new CNVM
• Median final VA 6/24

Mrs RW
• 45 yr old woman
• Referred with long standing R>L intermediate uveitis
• No longer responding to rptorbital steroids
• GH good


Thank you