il paziente anziano, evidenza e survey nazionale impssibili... · u.o.c. di nefrologia e dialisi...
TRANSCRIPT

dr Carlo Lomonte
U.O.C. di Nefrologia e Dialisi
Ente Ecclesiastico Ospedale Miulli
Acquaviva delle Fonti - Ba
Università La Sapienza
Scuola di Specializzazione in Nefrologia
Prof P. Menè
Meeting di Nefrololgia Interventistica
“L’Accesso Vascolare Impossibile” Roma 23 Marzo 2016
Il paziente anziano, evidenza e survey nazionale

The DOPPS (Dialysis Outcomes and Practice Pattern Study) is a prospective cohort
study of hemodialysis practices based on the collection of observational longitudinal data

3 Pazienti incidenti Pisoni, AJKD 2015

4 Pisoni, AJKD 2015 Pazienti prevalenti

www.dopps.org
68%
86%

www.dopps.org
68%
32%
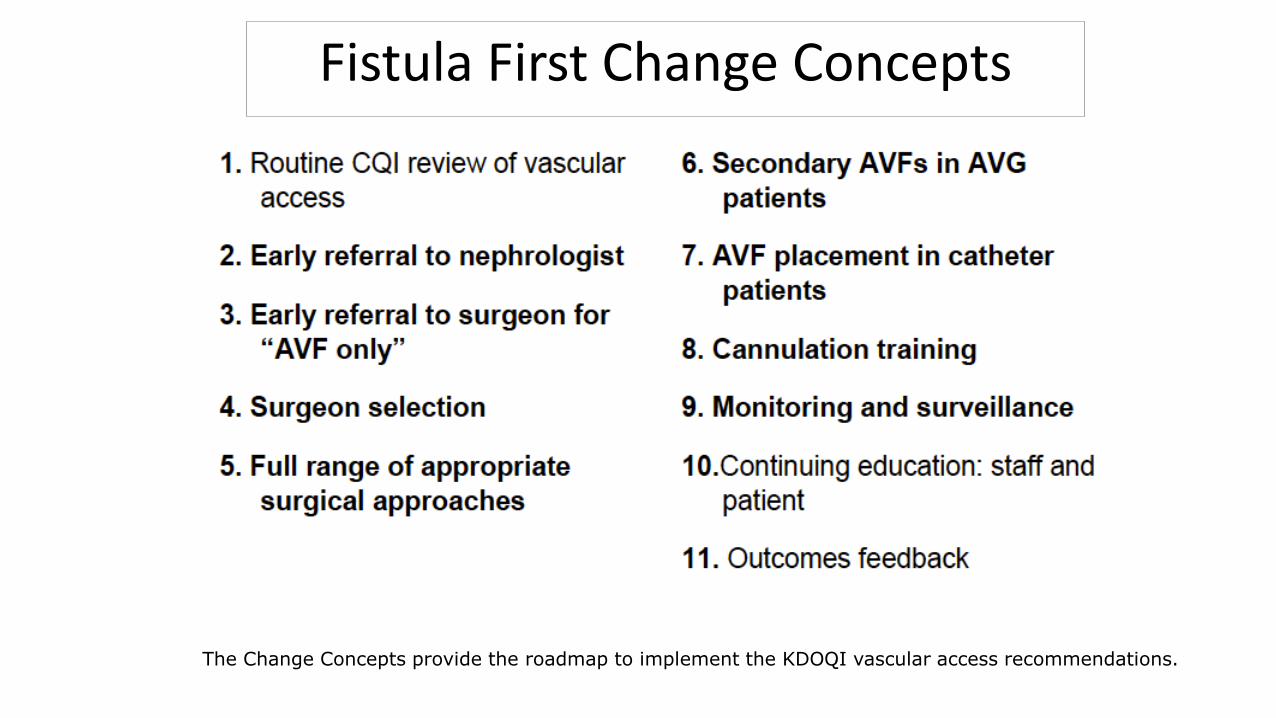
Fistula First Change Concepts
The Change Concepts provide the roadmap to implement the KDOQI vascular access recommendations.

Interventional nephrology: a new
area of competency in nephrology
• Organization (The American Society of
Diagnostic and Interventional Nephrology – ASDIN,
was established on October 2000)
• Need (dysfunctional access was a major cause of
patient morbidity and mortality)
• Interest (nephrologists have been trained to
address all of the dialysis patient’s problems. The
exception was VA)
G Beathard. History of interventional nephrology in the US In Asif et al: Interventional Nephrology. McGraw-Hill 2012

• There is a substantial need for the establishment of Academic Dialysis Access Centers (ADACs)
• These centers would be essential for transforming IN into a distinct discipline within nephrology similar to transplant nephrology
Roy-Chaudhury et al, CJASN 2012
Academic Interventional Nephrology: A Model
for Training, Research, and Patient Care

Roy-Chaudhury et al, CJASN 2012

Roy-Chaudhury, CJASN 2012
• 35% surgeons
• 30% radiologists
• 25% nephrologists
• 10% anesthesiology and other specialties
vascular access costs

…e in Italia?

2000
Gruppo di Studio degli
Accessi Vascolari

Accessi vascolari prevalenti
FAV nativa
FAV protesica
CVC cuffiato
Censimento SIN 2004
4,6%
11,5%
83,9%

Who is the vascular access manager
Nephrologist 48.8%
Nephrologist and Vascular Surgeon 26.4%
Vascular Surgeon 18.4%
Others 6.4%

Courtesy by Decenzio Bonucchi
Chirurgo Vascolare
Nefrologo
Nefrologo + Chirurgo Vasc.

www.dopps.org
68%
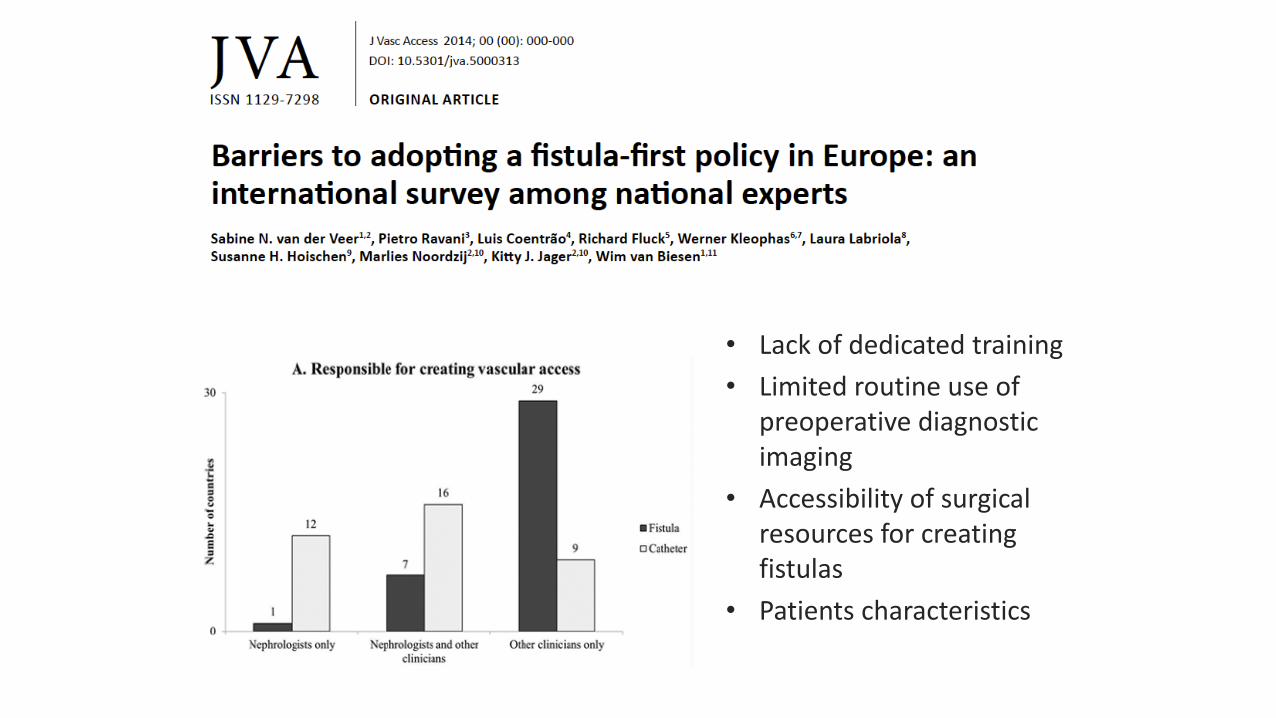
• Lack of dedicated training
• Limited routine use of preoperative diagnostic imaging
• Accessibility of surgical resources for creating fistulas
• Patients characteristics
18

CJASN 2013


Annual Report of ERA-EDTA Registry 2012
• 65-74 years = 22%
• >75 years = 20%

Timely VA placement in the elderly
- Older patients lose renal function at slower rates than
youngers one (Vachharajani, CJASN 2011)
- The elderly patients may be more likely to die before
benefiting from an AVF (Hod, JASN 2015)
- The elderly patients with CKD should be referred later
to reduce the risk of creating an AVF that is never used
(Gomes, JASN 2013)

23 Hod et al, J Am Soc Nephrol 2015

VA in elderly patients: recent findings
• There is currently no general consensus as to the best
dialysis VA for elderly patients with ESRD
• The creation and use of a VA in elderly patients requires
the complex integration of patients, biological and surgical
factors because the VA type might be a key factor
influencing their survival




More vein, less plastic
Criteria for the ideal VA device
• Safe
• Reliable performance and adequate blood flow
• Durable long-term function
• Internal
• Free from complications
• Acceptable to the patients
• Simple to create
• Inexpensive to create and maintain
• Vein preservation is paramount in patients who can be identified as being in the early stage of CRF
• A culture of vein preservation has to be developed in renal and surgical units and among venipuncture nurses, anesthetists etc.
28 D Francis, Nephrology 2005

Detailed History
29
• Previous CVC (temporary or tunneled)
• Hospitalization for major events (trauma, ICU)
• Scars on the chest
• Previously failed VA
• Cardiac rhythm devices
• Swelling of the arm, shoulder, chest, brest, face
• Collaterals veins
Salman & Beathard, CJASN 2013

30
Physical examination (summary)
• Presence of a superficial vein (straight of at least 8-10 cm)
• Good arterial pulse (not diminished or absent)
• Negative Allen’s test (patent palmar arch)
• Difference < 10 mm Hg in blood pressure in 2 arms (normal)
Asif et al, J Nephrol 2007 32

31
The Necessity for Routine Pre-operative Ultrasound Mapping
Before Arteriovenous Fistula Creation: A Meta-analysis
Giorgiadis et al, Eur J Vasc Endovasc Surg. 2015
Randomized clinical trial of selective versus routine preoperative
duplex ultrasound imaging before arteriovenous fistula surgery.
Smith, Br J Surg. 2014

33
Elsharawy, J Vascular Access 2006

34
Three steps in order to increase the pool of eligible patients can be individualized:
1) process of care, which includes three fundamental items:
- the VA team
- early VA education
- timely VA surgical referral
2) preoperative evaluation
3) surgical strategy

Surgical strategy in elderly patients

- A recent meta-analysis examining studies from 2000 to
2012 reported a primary failure rate (defined as non
usable AVF for dialysis up to 6 months post creation) of
23 % (Al-Jaishi, AJKD 2014)
- AVF failure increases by 1% for every year above the
age of 67 years (Hod, Hemodial Int 2014)
- Patients over 65 years have a fistula failure rate double
that of younger patients (Lok, JASN 2006)
Primary failure

Clinical use of the score system
Lok, JASN 2006

38
» All patients with risk factors for central venous stenosis should have a venogram regardless of score
Lok, JASN 2006

39

40
Masengu, CKJ 2016

41
J Vasc Surg 2007
An Italian perspective
• AVF still remains the dialysis access with highest prevalence also in older patients, with an excellent survival rate (Venturelli et al JN 2013; Pirozzi et al JVA 2014)
• In Italy, among patients with > 4 months pre-ESRD care prior to starting chronic HD, 71% had AVF (DOPPS)

Ethier et al, NDT 2008

• …we believe that dialysis VA selection in the elderly should
be guided by patient’s preference and surgeon’s
experience, based on comprehensive, balanced and
unbiased information, adopting an individualized approach
that strives to achieve the best outcomes regardless of age.
Conclusion

Key messages
1. Renal replacement therapy in the elderly raises several issues.
2. The VA planning in the elderly is different from that in younger patients:
elderlies could be referred later to reduce the risk of creating an AVF that is
never used.
3. The elderly with limited life expectancy may be less likely to benefit from an
AVF first approach.
3. The patient’s preference for the type of VA should be taken into account.
4. We advice to adopt an individualized approach, regardless of age.

FAV PROSSIMALE
Revisione FAV PROTESICA
CATETERE long term
CVC TEMPORANEO
FAV PROTESICA
FAV “DISPERATA”
F.G.
- Il nefrologo ha sempre “titolo” per fare gli accessi! ?
Riabbocco FAV DISTALE
FAV DISTALE
Superficializzazione/Trasposizione V.nativi
CATETERE long term
FAV Prossimalizzata