identifying and preventing medical errors in patients … 1 welcome to the disparities solutions...
TRANSCRIPT

12/30/2015
1
Welcome to the Disparities Solutions Center’s Web Seminar Series
Identifying and Preventing Medical Errors in Patients with
Limited-English Proficiency: New Tools for the Field
Tuesday, October16, 20121:00PM – 2:30PM ET
This web seminar will start momentarily
Identifying and Preventing Medical Errors in Patients with Limited-English Proficiency: New Tools for the Field
PresentersPresenters
Joseph Betancourt, MD, MPHDirector, The Disparities Solutions Center at Massachusetts General Hospital
Cindy Brach, MPP Senior Health Policy Researcher, Agency for Healthcare Research and Quality
Anabela Nunes, MBA Director of Medical Interpreter Services,Massachusetts General Hospital
John Cowden, MD, MPHInterim Section ChiefGeneral Pediatrics, Medical DirectorOffice of Equity and DiversityChildren's Mercy Hospitals and Clinics

12/30/2015
2
The Hospital Guide and LEP T STEPPSLEP TeamSTEPPS
Module
Available at:http://www.ahrq.gov/teamsteppstool
s/lep/index.html
Cindy Brach, MPP
Cindy Brach, MPP, is a Senior Health Policy Researcher y , , yat the Agency for Healthcare Research and Quality (AHRQ). She conducts and oversees research on health literacy, cultural and linguistic competence, system design innovations, and Medicaid and SCHIP. Cindy leads AHRQ’s health literacy and cultural competence activities, such as the development of the a TeamSTEPPS module for improving care to patients with limited English proficiency and adapting tools to improve the hospital discharge process for diverse patients. She serves on the Institute of Medicine Roundtable on H lth Lit d b f th N ti lHealth Literacy and was a member of the National Project Advisory Committee for updating the National Standards for Cultural and Linguistic Competence. Her publications include “Integrating Literacy, Culture, and Language to Improve Quality of Health Care for Diverse Populations” and “Crossing the Language Chasm, and she was the editor of “Setting the Agenda for Research on Cultural Competence in Health Care.”

12/30/2015
3
Anabela Nunes, MBAAnabela Nunes, MBA, is the director of Medical Interpreter Services at theMedical Interpreter Services at the Massachusetts General Hospital (MGH), Boston, Massachusetts. She oversees a complex operation which integrates the delivery of language services in a variety of modalities, face‐to‐face, telephonic and video using state of the art scheduling system that facilitates the efficient allocation of resources across a large sprawling urban campus. She leads a group of 36 staff medical interpreters and 50 freelance interpreters who provide interpreting services in over 30 languages. During her tenure, Ms. Nunes has been part of a number of initiatives to enhance accessibility to and increase utilization of professional medical interpreters through the creation and deployment of I‐POPs (Interpreter Phone on Pole) and more recently V‐POPs (video medical interpreting).
John Cowden, MD, MPHJohn Cowden, MD, MPH, is Interim Section Chief of General Pediatrics at Children's Mercy yHospitals and Clinics. He also serves as Medical Director of Children's Mercy's Office of Equity and Diversity, which guides the organization's efforts toward cultural competency and health equity. He is founder and co‐director of CHICOS and Enlaces, a Spanish language resident care clinic and a medical resident Spanish class, respectively. Dr. Cowden’s research interests include provider‐patient communication, provider bias, and access to health care for minorities specifically those who do not speakminorities, specifically those who do not speak English. In his bilingual clinical practice, he serves Spanish‐speaking families throughout the Kansas City metropolitan area. He teaches medical students from the University of Kansas City –Missouri and pediatric residents at the Children’s Mercy Hospitals and Clinics.

12/30/2015
4
Tools for Identifying and Preventing Medical Errors in Patients with
Limited-English ProficiencyJoseph R. Betancourt, M.D., M.P.H.
Director, The Disparities Solutions CenterSenior Scientist, Mongan Institute for Health Policy
Director for Multicultural Education, Massachusetts General Hospital
Associate Professor of Medicine, Harvard Medical School
g y
Quality Health Care
Health care should be
– Safe
– Effective
– Patient-centered
– Timely
– Efficient
– Equitable

12/30/2015
5
Background: Disparities, LEP and Patient Safety
Approximately 24 million (8.5% of the U.S. population) are defined as having Limited English Proficiency (LEP)
Adverse events affect LEP patients more frequently and severely than they affect English speaking patients
LEP patients more likely to experience medical errors d t i ti bl th E li h kidue to communication problems than English speaking
LEP patients more likely to suffer from physical harmwhen errors occur
Project Overview
Goal: Develop, test, and implement two new tools to reduce patient harm due to language barriers and cross-cultural care communication problems
Hospital Guide on preventing, identifying, and reporting medical errors due to language barriers and cross-cultural communication problems
A new TeamSTEPPS training module, focused on team behaviors to improve safety in LEP and culturally diversebehaviors to improve safety in LEP and culturally diverse patient populations
Funded by the Agency for HealthCare Research and Quality (AHRQ) and conducted by Abt Associates, Inc. and the Disparities Solutions Center at
Massachusetts General Hospital

12/30/2015
6
Research and Development Team
Disparities Solutions CenterMegan Renfrew MPH– Megan Renfrew, MPH
– Aswita Tan-McGrory, MPH, MBA
– Lenny Lopez, MD, MPH, Mdiv
– Alexander R. Green, MD, MPH
ABT AssociatesMelanie Wasserman PhD– Melanie Wasserman, PhD
– Mark Spranca, PhD
AHRQ– Cindy Brach, MPP
Methodology and Data Sources
IMP
Adverse Events Database
Advisory Board
Key Informant Interviews
Preliminary Hospital Guide
Interviews Frontline Staff
Environmental Scan
Field Testing
Preliminary Team STEPPS
Final Hospital Guide
Final Team STEPPS
LEMENTATI
Interpreter Pilot Results
ION
Identify Role of Language Barriers in Pt Safety Events
Document how Hospitals are Addressing LEP Errors
Background
Preliminary Tool Development
Testing and Validation
Final Product Development
Dissemination and Adoption
Town Meeting

12/30/2015
7
Adverse Events Database From 2006-8, 840 events in LEP patients (of 16,708 total)
LEP patients more likely to have adverse events attributable to medication errors (57% vs 50%) and procedure consent errors (.12% vs .07%) compared to English speaking patients*compared to English speaking patients
Adverse Events Attributable to Procedure Consent Errors in English Speaking and LEP
Patients
0.10%
0.15%
rcen
t
52%
54%
56%
58%
erc
en
t
Adverse Events Attributable to Medication Errors in English Speaking and LEP
Patients
0.00%
0.05%
English speaking Limited Englishproficiency
per
46%
48%
50%
English speaking Limited Englishproficiency
pe
Betancourt JR, Renfrew MR, Green AR, et al. Improving patient safety systems for patients with limited English proficiency: a guide for hospitals. (Prepared by the Disparities Solutions Center, Mongan Institute for Health Policy at Massachusetts General Hospital and Abt Associates, Cambridge, MA, under Contract No. HHSA290200600011I). Rockville, MD: Agency for Healthcare Research and Quality; July 2012. AHRQ Publication No. 12-0041. September 2012.
MGH Interpreter Pilot Project
Overview of Key Themes – Misuse of interpreter services
No interpreter present, use of family members, providers using l kill )poor language skills)
– Miscommunication between patients and providers Poor communication skills, not listening to patients’ complaints,
lack communication between patient and broader care team
– Cultural issues Inappropriate questions posed to patients (e.g. religion);
Providers’ lack of understandingg
– ProfessionalismRudeness to interpreters and not respecting or understanding
their role
– Informed Consent Consent signed without interpreter present

12/30/2015
8
Broad Key Themes Interviews & Town Hall Meeting:Current Hospital Strategies/Efforts to Address
Linguistic and Cultural Sources of Error Language data collection – not systematic or routine across
hospitalsp
Safety reporting systems often do not include fields to identify “language” or “interpreter” as playing a role –precludes stratification of errors and impedes root cause analyses
Hospitals do not routinely monitor medical errors for LEP and rarely generate reports for high risk scenarios
Challenges with data collection (merging of databases not designed for this purpose)
Broad Key Themes Interviews & Town Hall Meeting:Common Causes of Medical Errors for LEP
Use of non-qualified interpreters
Use of family members/friends or house staff
Provider use of basic language skills to “get by”
Cultural beliefs/values impacting patient care

12/30/2015
9
Broad Key Themes Interviews & Town Hall Meeting:High Risk Scenarios
Medication Reconciliation
Informed Consent Processes
Patient Discharge
Emergency Department Visits
Pre, Peri and Post-Operative Care
Hospital Guide Educate leaders with background
and evidence on medical errors that occur due to LEP
Present strategies and training tools Present strategies and training tools to create systems and an organizational culture to better identify, report and prevent medical errors that occur due to LEP in a variety of hospital settings
Provide a set of practical case Provide a set of practical case examples that solidify learning
Provide resources which can be useful in developing an LEP patient error reporting and response system

12/30/2015
10
The LEP ModuleCindy Brach, AHRQ

12/30/2015
11
TeamSTEPPS
Health Care and Teamwork
Communication failures account for the overwhelming Communication failures account for the overwhelming majority of adverse events
Medical care is complex and human performance has inherent limitations
Effective teamwork can prevent mistakes
Embedding evidence-based training and team behaviors can enhance safety
Team training has a positive impact on work force retention
TEAMSTEPPS 05.2Mod 1 05.2 Page 21Mod 1 05.2 Page 21
Team training has a positive impact on work force retention
TeamSTEPPS
AHRQ/DoD Partnership Activities began in 2002 Expert Panel Expert Panel Comprehensive literature
review and case study analysis
Clinical measures of teamwork
Medical Team Training Curriculum TeamSTEPPS
Edited Handbook
Evidence-Based
Methods
Tools for
Principles andGuidelines
TEAMSTEPPS 05.2Mod 1 05.2 Page 22Mod 1 05.2 Page 22
National ImplementationTools for
Training andMeasurement

12/30/2015
12
TeamSTEPPS
National Implementation Project
Created a national infrastructure to support the adoption of TeamSTEPPS
Quality Improvement Organizations
Hospital Engagement Networks
ACTION Partners
Academic Medical Centers
Other Countries (Japan, Australia, Netherlands)
Spread TeamSTEPPS: trained over 5000 Master Trainers
TEAMSTEPPS 05.2Mod 1 05.2 Page 23Mod 1 05.2 Page 23
Spread TeamSTEPPS: trained over 5000 Master Trainers who trained 25,000 trainees to date
TeamSTEPPS
Products and Materials
Core TeamSTEPPS Core TeamSTEPPS Rapid Response
Systems (RRS) Module
Limited English Proficiency (LEP) Module
TEAMSTEPPS 05.2Mod 1 05.2 Page 24Mod 1 05.2 Page 24
Module
Long-term Care
Primary Care

12/30/2015
13
TeamSTEPPS
Benefits of including interpreter on the care team
Receive more complete and accurate information
Facilitate better clinical decisions
Receive support from a cultural broker who is also an advocate for the patient
Meet the new Joint Commission patient-centered
TEAMSTEPPS 05.2Mod 1 05.2 Page 25Mod 1 05.2 Page 25
pcommunication standards (in effect July 1, 2012)
TeamSTEPPS
How the LEP module can help
1.5 hour staff training module so unit staff and interpreters can:
Understand the risks to LEP patients
If LEP call a professional medical interpreter
Identify and raise patient communication issues
4 hour train the trainer program:
TEAMSTEPPS 05.2Mod 1 05.2 Page 26Mod 1 05.2 Page 26
4-hour train-the-trainer program:
Hospitals train their own staff

12/30/2015
14
TeamSTEPPS
Training Module Content
Slid d k ith id d i Slide decks with videos and exercises
Train-the-Trainer materials, including instructor guides, readiness assessment , and handouts
Hospital Guide
Evaluation Guide, with provider behavior and patient outcome surveys
TEAMSTEPPS 05.2Mod 1 05.2 Page 27Mod 1 05.2 Page 27
p y
TeamSTEPPS
Tools
Assemble the team Assemble the team
CUS
Two Challenge Rule
Brief
Psychological Safety
Check-Back
TEAMSTEPPS 05.2Mod 1 05.2 Page 28Mod 1 05.2 Page 28
Teach Back

12/30/2015
15
TeamSTEPPS
Stop the Line: CUS
(insert video clip of CUS here)
TEAMSTEPPS 05.2Mod 1 05.2 Page 29Mod 1 05.2 Page 29
TeamSTEPPS
Field Test
Module implemented in all 3 hospitalsp p Settings:
3 hospitals in MO, DE and NC Labor and Delivery Emergency Department, OB/Gyn Pediatric primary care
TeamSTEPPS/non-TeamSTEPPS hospital
TEAMSTEPPS 05.2Mod 1 05.2 Page 30Mod 1 05.2 Page 30
268 staff members trained including doctors, nurses, interpreters, registration staff

12/30/2015
16
TeamSTEPPS
Field Test Findings Focus for each hospital was different:
U f lifi d i t Use of a qualified communicator
Briefs with interpreters
Phone interpreter use if no in-person interpreter
Catalyst for institutional changes
Reorganize/reallocate interpreters
TEAMSTEPPS 05.2Mod 1 05.2 Page 31Mod 1 05.2 Page 31
Reorganize/reallocate interpreters
Clarify interpreter use policies
Bilingual provider training/certification
TeamSTEPPS
Field Test Results
Qualitative results: Clinical staff more aware of need to call interpreter Interpreters more empowered to raise and address
communication issues with clinical team
Quantitative results: Hospital 1: pre-test convinced leadership no post-test
Hospital 2: High satisfaction, increase in knowledge, R/E/L d t lit i i t t d t bl
TEAMSTEPPS 05.2Mod 1 05.2 Page 32Mod 1 05.2 Page 32
R/E/L data quality issues interpreter use data unusable
Hospital 3: High satisfaction, increase in knowledge scores, R/E/L data quality issues interpreter use data unusable

12/30/2015
17
TeamSTEPPS
Conclusions
Module can be implemented in a variety of Module can be implemented in a variety of settings
TeamSTEPPS/non-TeamSTEPPS
Hospital/ primary care clinic
Catalyst for change
R/E/L data Collection/use still a barrier to formal
TEAMSTEPPS 05.2Mod 1 05.2 Page 33Mod 1 05.2 Page 33
evaluation
TeamSTEPPS
More Information
To access the TeamSTEPS Module for Limited English Proficiency, go to: http://www.ahrq.gov/teamsteppstools/lep/index.html
For more information about TeamSTEPPS, go to: http://teamstepps.ahrq.gov/
TEAMSTEPPS 05.2Mod 1 05.2 Page 34Mod 1 05.2 Page 34
http://teamstepps.ahrq.gov/

12/30/2015
18
Limiting Medical Errors among the Limiting Medical Errors among the Limited English ProficientLimited English Proficient
Anabela NunesAnabela NunesDirector MGH Medical Interpreter ServicesDirector MGH Medical Interpreter Services
MGH InterpretationsMGH Interpretations
82,464
75 792
80,000
90,000
Inpatient: 27%
Inpatient: 28%
Inpatient: 26%
40,168
49,248
57,062
65,551
75,792
40,000
50,000
60,000
70,000
To
tal N
um
be
r o
f E
nc
ou
nte
rs
Inpatient: 28%
Inpatient: 25%
Inpatient: 23%
20,000
30,000
FY 06 FY 07 FY 08 FY 09 FY 10 FY11

12/30/2015
19
Anecdotally…Anecdotally…
Near missesNear misses
Wrong languageWrong language
Incorrect or improper careIncorrect or improper care
“Getting by”“Getting by”
LEP Safety InitiativesLEP Safety Initiatives
Quality and Safety RoundsQuality and Safety Rounds Interpreter Services leadership included inInterpreter Services leadership included in Interpreter Services leadership included in Interpreter Services leadership included in
Executive Quality and Safety RoundsExecutive Quality and Safety Rounds Standard script for staffStandard script for staff Identify safety concerns for LEP patientsIdentify safety concerns for LEP patients
Successes Successes In progressIn progress
•• Tentative start date in the Fall 2012Tentative start date in the Fall 2012
ChallengesChallenges•• Frequency of roundsFrequency of rounds•• Competing goalsCompeting goals

12/30/2015
20
LEP Safety InitiativesLEP Safety Initiatives
Interpreter RoundsInterpreter Rounds Standard scriptStandard scriptpp Inform patients of right and access to interpreter servicesInform patients of right and access to interpreter services Assess how language needs are metAssess how language needs are met
Successes Successes •• More rounds done than anticipatedMore rounds done than anticipated•• Valuable data gathering will help identify new initiativesValuable data gathering will help identify new initiatives•• Rounding on any languageRounding on any language
In progressIn progress In progressIn progress•• Data collection and analysis for evaluationData collection and analysis for evaluation
ChallengesChallenges•• Standardize interpreter roundsStandardize interpreter rounds•• Round on all patientsRound on all patients•• Coordinate rounds with other disciplinesCoordinate rounds with other disciplines
LEP Safety InitiativesLEP Safety Initiatives
Interpreter TrainingInterpreter Training Quality & Safety 101 including reportingQuality & Safety 101 including reporting Quality & Safety 101, including reportingQuality & Safety 101, including reporting
Successes Successes •• Increased awareness of their role in LEP patient safetyIncreased awareness of their role in LEP patient safety•• Greater understanding of value of reportingGreater understanding of value of reporting•• Increased number of reports being submittedIncreased number of reports being submitted
In progressIn progress•• Training and implementation on specific communication skillsTraining and implementation on specific communication skills
ChallengesChallenges•• Empowering interpreters to speak up in the moment Empowering interpreters to speak up in the moment •• Recognition as a member of the medical teamRecognition as a member of the medical team

12/30/2015
21
Children's Mercy Hospitals & ClinicsKansas City, Missouri
John D. Cowden, MD, MPH
Enhancing Safety for Patients withwith
Limited English Proficiency
12/30/2015
22
Pediatric Care CenterYellow Clinic (1 of 4 colors)Spanish Language Focus
LEP™
Check-Back is…
TEAMSTEPPS 05.2Mod 6.11.10 Page 44
12/30/2015
23
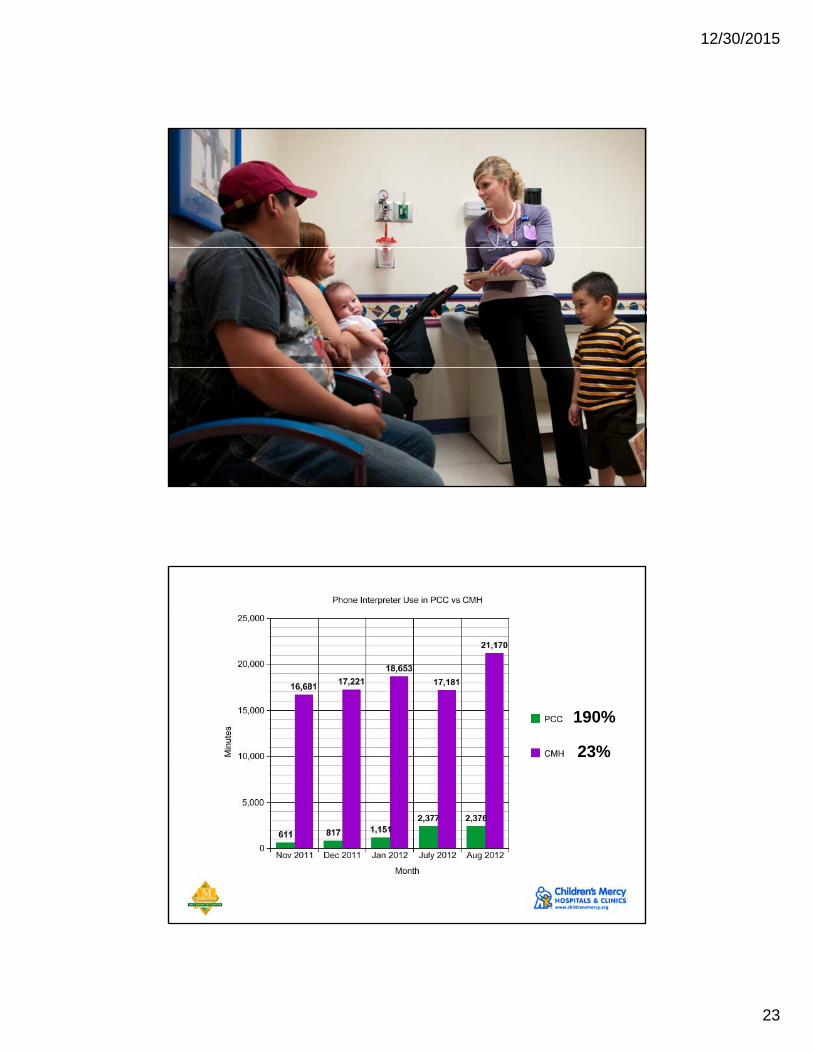
190%
23%

12/30/2015
24
http://seccioneuropea.files.wordpress.com/2010/09/imagen-1.png
Please help us further improve our web seminars byPlease help us further improve our web seminars by taking a moment to complete an evaluation of today’s
event. Please click the link below and complete the evaluation on your web browser.
Take the Survey!Take the Survey!
Find the Survey at https://www.surveymonkey.com/s/LEPWebinar if the above link does not properly function

12/30/2015
25
Question and Answer Period
Please submit your questions online by typing them into the Question box on the right side of the screen and clicking the “Send” button. The panelists will try to answer the questions as succinctly as they can.
Depending on the size of the audience, we may not be able to answer all questions.q
Presenters
Identifying and Preventing Medical Errors in Patients with Limited-English Proficiency: New Tools for the Field
Presenters
Joseph Betancourt, MD, MPHDirector, The Disparities Solutions Center at Massachusetts General Hospital
Cindy Brach, MPP Senior Health Policy Researcher, Agency for Healthcare Research and Quality
Anabela Nunes, MBA Director of Medical Interpreter Services,Massachusetts General Hospital
John Cowden, MD, MPHInterim Section ChiefGeneral Pediatrics, Medical DirectorOffice of Equity and DiversityChildren's Mercy Hospitals and Clinics

12/30/2015
26
The Hospital Guide and LEP T STEPPSLEP TeamSTEPPS
Module
Available at:http://www.ahrq.gov/teamsteppstool
s/lep/index.html

12/30/2015
27
Thank you for your participation!
www.MGHDisparitiesSolutions.org