(identify each visit by a number and a date)
TRANSCRIPT

Mrs SJ
1
Contents
Page 1. Introduction 3
1.1 Key clinical features 3 1.2 Care provided 3 1.3 Outcomes 3 1.4 Plans for future care 3
2. Reason for first visit 4 3. Examination and assessment 4
3.1 Medical History 4 3.2 Dental History 4 3.3 Social History 4 3.4 Extra Oral Examination 4 3.5 Intra Oral Examination 6 3.6 Special Investigations 8 3.7 Results of Special Investigations 9 3.8 Radiographs 10
Figure 1 - Charting and Indices 11
4. Diagnosis 12 5. Treatment plan 13
5.1 Emergency treatment 13 5.2 Stabilisation phase 13 5.3 Reassessment and maintenance 13 5.4 Restorative phase 13 5.5 Continual reassessment and maintenance 13
6. Discussion of treatment plan
6.1 Treatment objectives for stabilisation phase 14 6.2 Patient’s attitude 14 6.3 Discussion of possible alternative treatment plans 14
6.3.1 Restoration of endodontically treated teeth 14 6.3.2 Treatment of 3
rd molars left side 14
6.3.3 Unsatisfactory endodontic treatments 15 6.3.4 Overbuilt crown 15 6.3.5 Missing teeth 15 6.3.6 Restoration of UL1 15 6.3.7 Restoration of UR5 & UL4 16 6.3.8 Presence of fragment LL7 16 6.3.9 Early carious lesions 17
7. Treatment carried out 17
7.1 Visit 1 17 7.2 Visit 2 17 7.3 Visit 3 18 7.4 Visit 4 18
1st hygienist visit 19
2
7.5 Visit 5 20 7.6 Visit 6 20 7.7 Visit 7 22 7.8 Visit 8 23 7.9 Visit 9 25 7.10 Visit 10 26 7.11 Visit 11 27 7.12 Visit 12 28 7.13 Visit 13 and 2
nd hygienist visit 29
8. Appraisal of treatment 30
9. Discussion of any variation from the original plan 30
10. Patient - compliance and attitude 30
11. Prognosis and maintenance 31
11.1 3 months 31 11.2 6 months 31 11.3 12 months 31 11.4 Outstanding problems 31
12. Conclusions 34
13. Note of word count 34
14. References 35
15. Appendices 36
16. Declaration of originality and patients consent back page
3
1. Introduction This case history describes the treatment of Mrs SJ, a 36 year old woman who had extensive caries and a highly cariogenic diet. She is the mother of six children and works in the family business manufacturing and selling furniture. Mrs SJ’s last visit was five years before. She is sometimes anxious about dental treatment.
1.1 Key clinical features
Presenting complaint - pain UR8
Gross caries UR8, UR7, UL4, UL5, UL8, LR4. Gross secondary caries LL8. Caries UL1, Secondary caries UR5, UR4, UL1.
Early carious lesions UR2, LL7, LL3
Unsatisfactory root canal treatments UL6, LR5
Marginal gingivitis
1.2 Care provided The overall approach was one of prevention and stabilisation. More advanced restorative care was considered inappropriate until stability is achieved.
Dietary advice, fluoride advice, oral hygiene instruction.
Scaling and polishing
Extraction of UR8, UL8, LL8
Composite restoration UL1
Root canal therapy UR7, UL5, LR4
Amalgam restorations UR7, UR5, UL4, UL5, LR4
1.3 Outcomes Treatment progressed satisfactorily. Protection of the compromised endodontically treated teeth was achieved using cuspal capping with amalgam. The patient was pleased with the aesthetic improvement to her upper front teeth and seemed to take our advice very seriously.
1.4 Plans for future care
Reassess diet, oral hygiene, compliance with fluoride advice.
Consider further stabilisation as necessary.
Monitor endodontically treated teeth.
Monitor vitality of heavily filled vital teeth. Consider restorative phase of treatment :
Cast restorations for endodontically treated teeth,
Further endodontic therapy for pre-existing root treated teeth Continual reassessment and maintenance
4
2. Reason for first visit Mrs SJ attended the practice for the first time complaining of a constant throbbing toothache from the upper right quadrant.
3. Examination and assessment Examination and assessment were carried out over visits 1 & 2 on 1.9.98 and 4.9.98. The first visit was confined to the taking of a medical history and resolution of the patient’s pain. UR8 was extracted and UR7 dressed with zinc oxide eugenol cement. At the second visit a full examination and assessment was carried out.
3.1 Medical History Mrs SJ takes oral contraceptives. Routine blood tests during pregnancy revealed no abnormality and her blood pressure was reported to be low. This was measured in the surgery and found to be 144/85 with pulse 73. (Appendix A)
3.2 Dental history Previous experiences and attitude
The patient had been an infrequent attender for dental care, her last visit being some 5 years before. She reported that she felt anxious about dental treatment sometimes. (Appendix B)
Dietary habits
The patient’s diet record revealed frequent intakes of coffee with two sugars but only gave part of the true picture. Further questioning over future visits showed that she also had frequent sugary snacks that she had not written on her diet sheet such as frequent chocolate bars.
Present oral hygiene measures
Simple cleaning with a toothbrush twice a day. No interdental cleaning
3.3 Social History
Date of birth 12.4.62 Occupation Shop proprietor Marital Status Married Children 6 Tobacco None Alcohol Social, about 6 units per week
3.4 Extra-oral examination
The patient was of normal height and build There were no - visible skin deformities - visible skin lesions - facial swellings, asymmetry or lymphadenopathy (Photographs 1 & 2 pg 5)
5
Photograph 1 Photograph 2
6
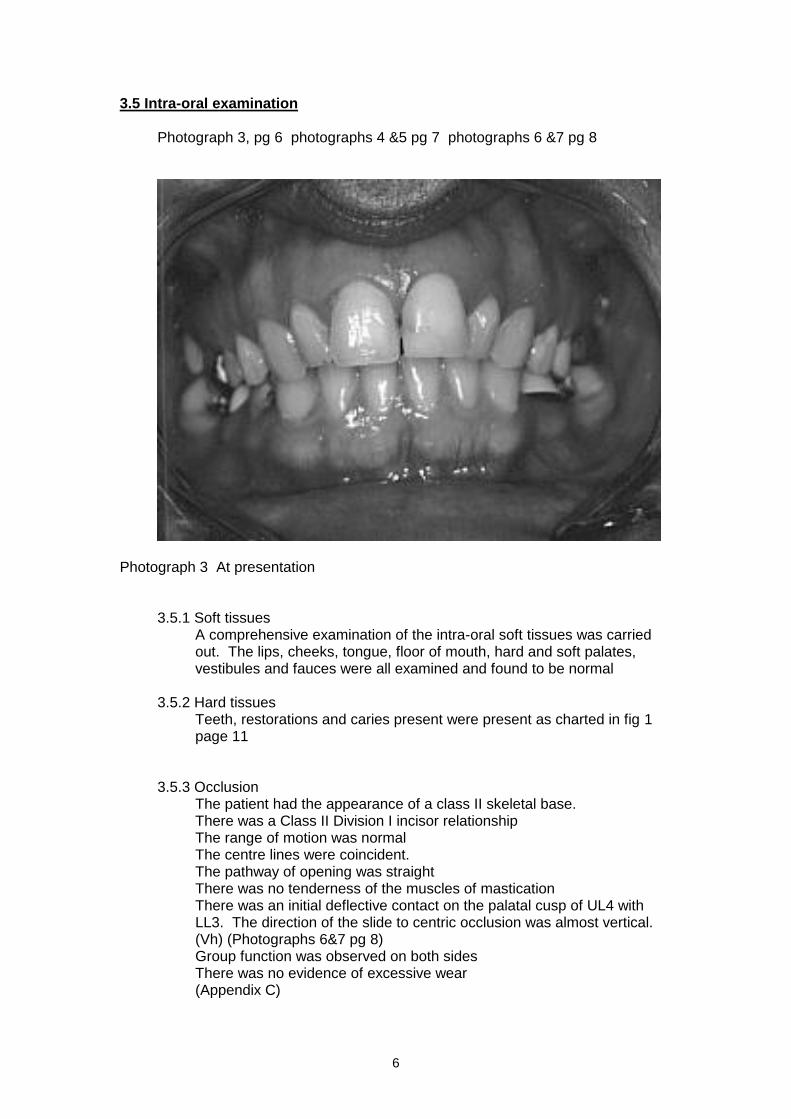
3.5 Intra-oral examination Photograph 3, pg 6 photographs 4 &5 pg 7 photographs 6 &7 pg 8
Photograph 3 At presentation
3.5.1 Soft tissues A comprehensive examination of the intra-oral soft tissues was carried out. The lips, cheeks, tongue, floor of mouth, hard and soft palates, vestibules and fauces were all examined and found to be normal
3.5.2 Hard tissues
Teeth, restorations and caries present were present as charted in fig 1 page 11
3.5.3 Occlusion
The patient had the appearance of a class II skeletal base. There was a Class II Division I incisor relationship The range of motion was normal The centre lines were coincident. The pathway of opening was straight There was no tenderness of the muscles of mastication There was an initial deflective contact on the palatal cusp of UL4 with LL3. The direction of the slide to centric occlusion was almost vertical. (Vh) (Photographs 6&7 pg 8) Group function was observed on both sides There was no evidence of excessive wear (Appendix C)
7
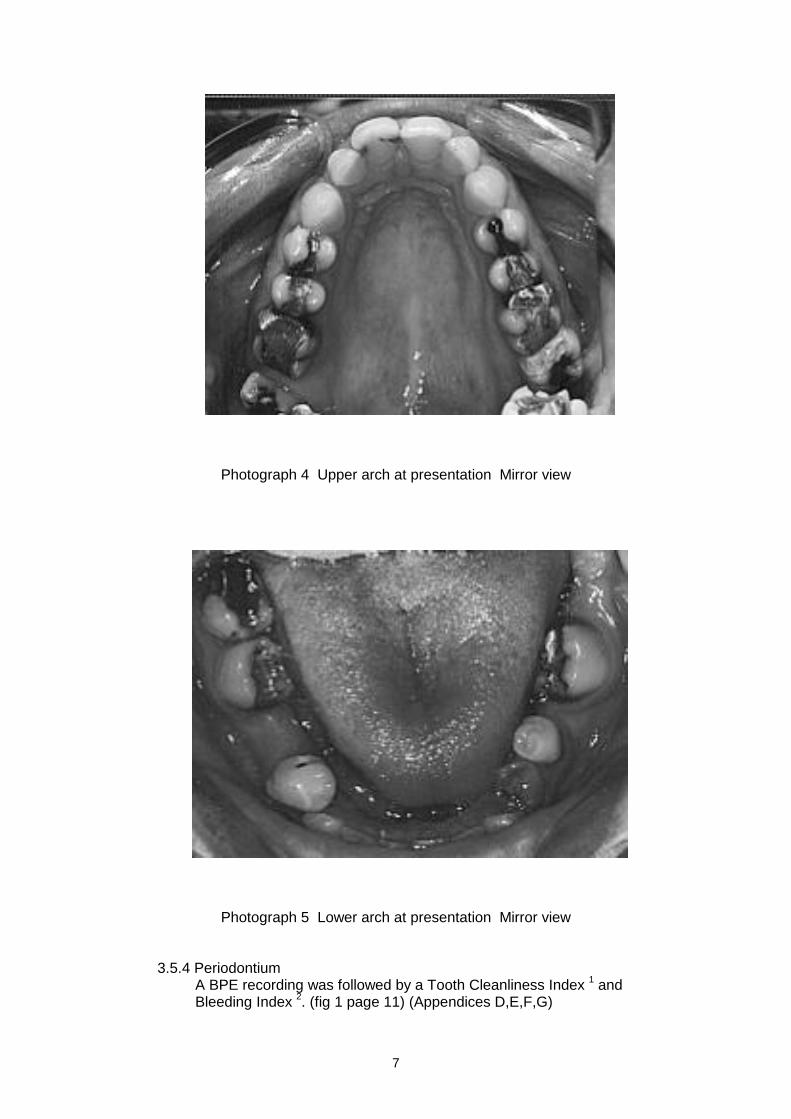
Photograph 4 Upper arch at presentation Mirror view
Photograph 5 Lower arch at presentation Mirror view
3.5.4 Periodontium A BPE recording was followed by a Tooth Cleanliness Index
1 and
Bleeding Index 2. (fig 1 page 11) (Appendices D,E,F,G)
8
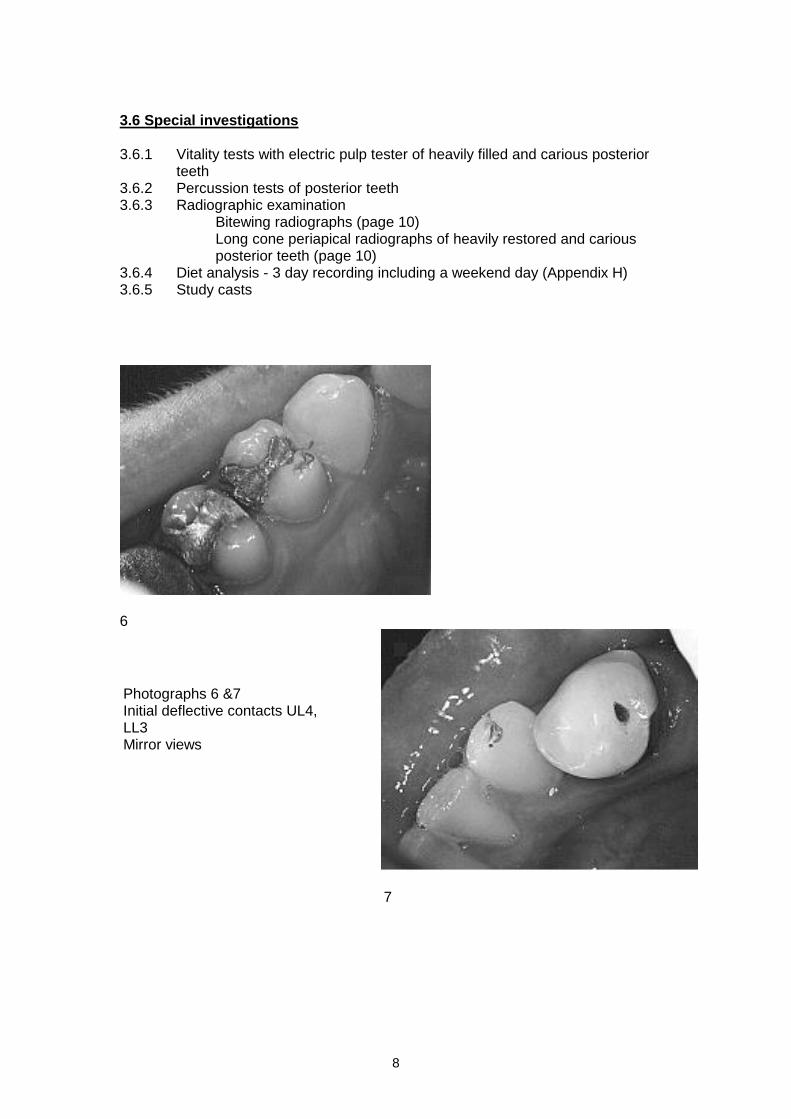
3.6 Special investigations 3.6.1 Vitality tests with electric pulp tester of heavily filled and carious posterior
teeth 3.6.2 Percussion tests of posterior teeth 3.6.3 Radiographic examination
Bitewing radiographs (page 10) Long cone periapical radiographs of heavily restored and carious posterior teeth (page 10)
3.6.4 Diet analysis - 3 day recording including a weekend day (Appendix H) 3.6.5 Study casts
6
7
Photographs 6 &7 Initial deflective contacts UL4, LL3 Mirror views
9
3.7 Results
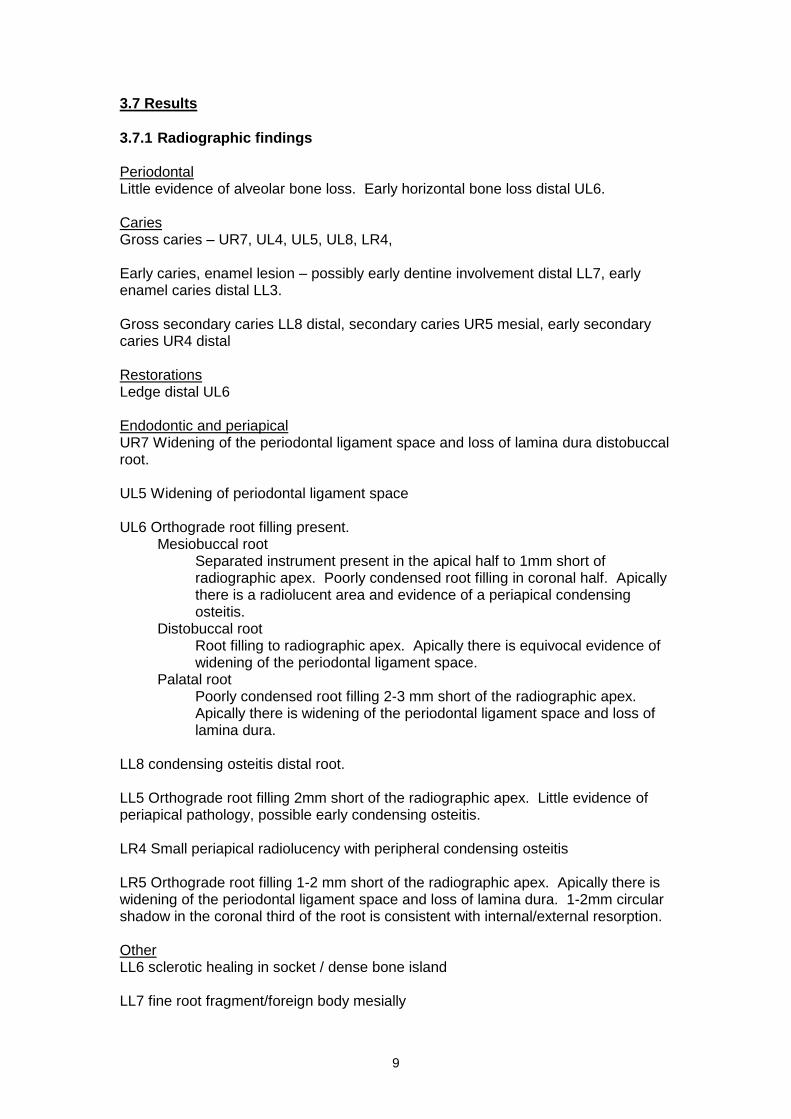
3.7.1 Radiographic findings Periodontal Little evidence of alveolar bone loss. Early horizontal bone loss distal UL6. Caries Gross caries – UR7, UL4, UL5, UL8, LR4, Early caries, enamel lesion – possibly early dentine involvement distal LL7, early enamel caries distal LL3. Gross secondary caries LL8 distal, secondary caries UR5 mesial, early secondary caries UR4 distal Restorations Ledge distal UL6 Endodontic and periapical UR7 Widening of the periodontal ligament space and loss of lamina dura distobuccal root. UL5 Widening of periodontal ligament space UL6 Orthograde root filling present.
Mesiobuccal root Separated instrument present in the apical half to 1mm short of radiographic apex. Poorly condensed root filling in coronal half. Apically there is a radiolucent area and evidence of a periapical condensing osteitis.
Distobuccal root Root filling to radiographic apex. Apically there is equivocal evidence of widening of the periodontal ligament space.
Palatal root Poorly condensed root filling 2-3 mm short of the radiographic apex. Apically there is widening of the periodontal ligament space and loss of lamina dura.
LL8 condensing osteitis distal root. LL5 Orthograde root filling 2mm short of the radiographic apex. Little evidence of periapical pathology, possible early condensing osteitis. LR4 Small periapical radiolucency with peripheral condensing osteitis LR5 Orthograde root filling 1-2 mm short of the radiographic apex. Apically there is widening of the periodontal ligament space and loss of lamina dura. 1-2mm circular shadow in the coronal third of the root is consistent with internal/external resorption. Other LL6 sclerotic healing in socket / dense bone island LL7 fine root fragment/foreign body mesially
10
3.7.2 Results of other special tests
1. UR7 UL8, LL8 & LR4 were negative to electric pulp testing: UR6, UR5, UR4, UL1, UL4, UL5, LR3, were positive to electric pulp testing.
2. UR8 was tender to percussion 3. Diet analysis indicated possible problem areas in the diet but did not give
the whole story. The patient reported that she had already decided to cut down on sugary snacks and drinks and that this was reflected in the diet sheet
4. Study casts indicated occlusal contacts and assisted with planning of post treatment stability.
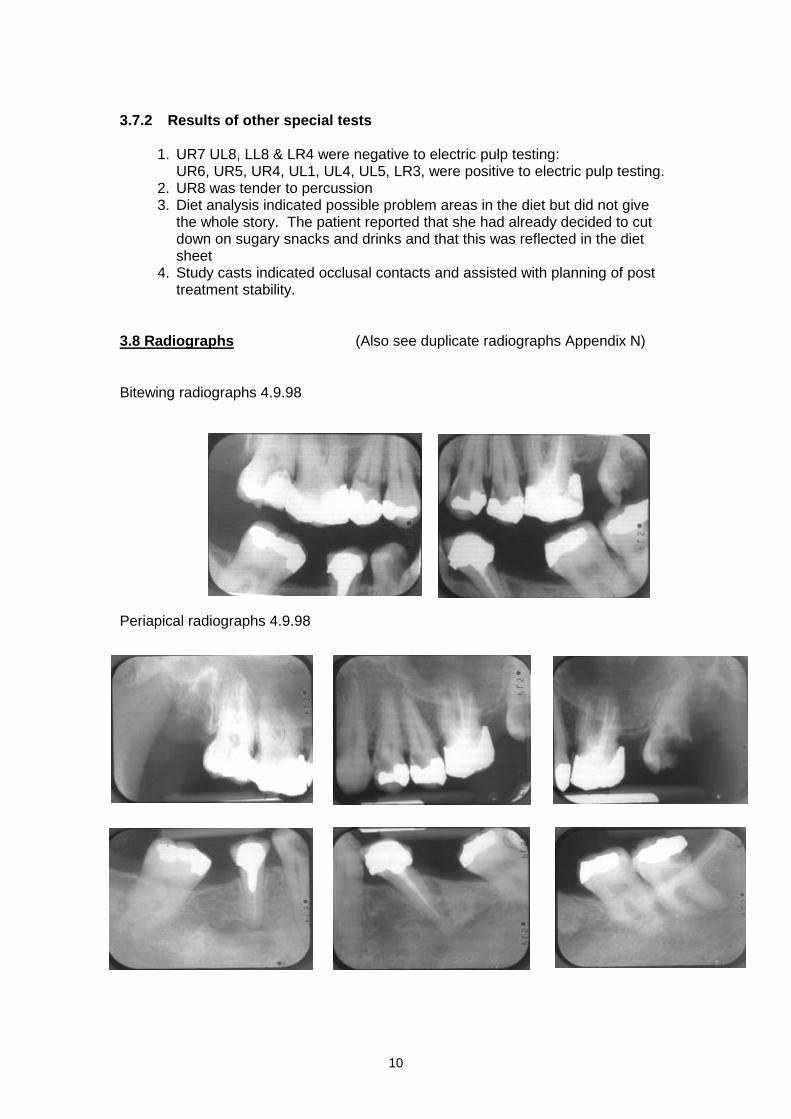
3.8 Radiographs (Also see duplicate radiographs Appendix N)
Bitewing radiographs 4.9.98
Periapical radiographs 4.9.98
11
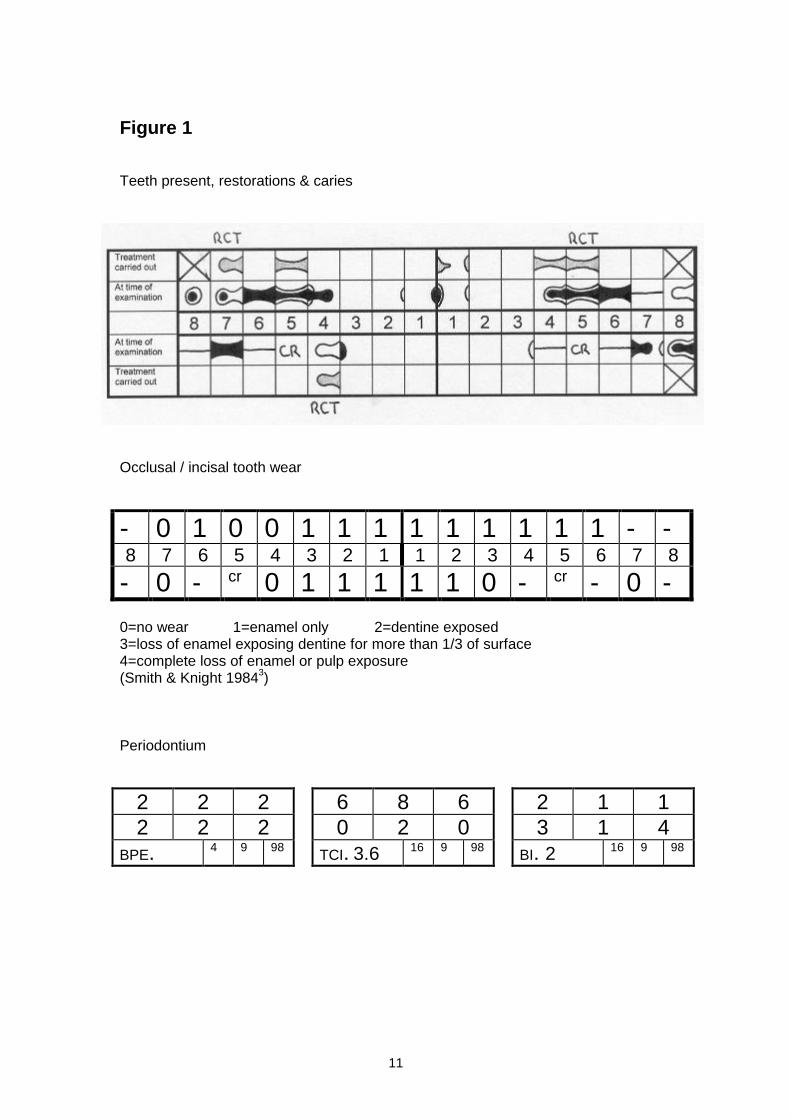
Figure 1 Teeth present, restorations & caries
Occlusal / incisal tooth wear
- 0 1 0 0 1 1 1 1 1 1 1 1 1 - - 8 7 6 5 4 3 2 1 1 2 3 4 5 6 7 8
- 0 - cr 0 1 1 1 1 1 0 - cr - 0 - 0=no wear 1=enamel only 2=dentine exposed 3=loss of enamel exposing dentine for more than 1/3 of surface 4=complete loss of enamel or pulp exposure (Smith & Knight 1984
3)
Periodontium
2 2 2
2 2 2
BPE. 4 9 98
6 8 6
0 2 0
TCI. 3.6 16 9 98
2 1 1
3 1 4
BI. 2 16 9 98
12
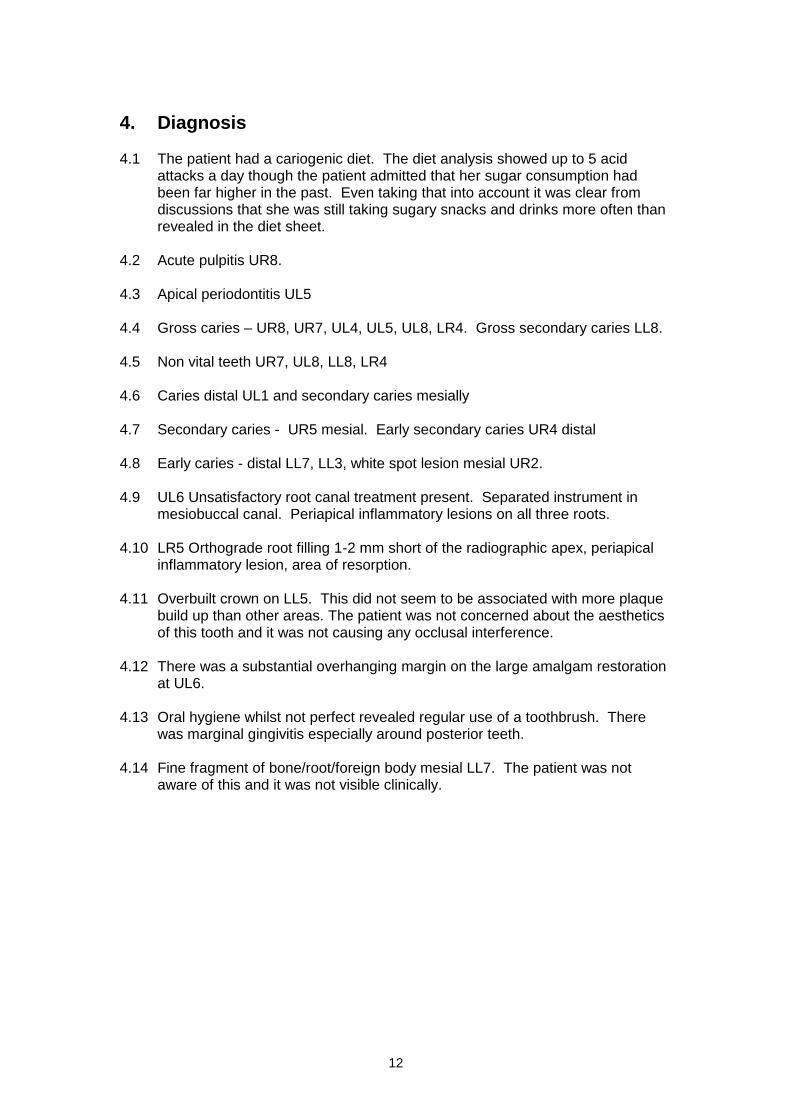
4. Diagnosis 4.1 The patient had a cariogenic diet. The diet analysis showed up to 5 acid
attacks a day though the patient admitted that her sugar consumption had been far higher in the past. Even taking that into account it was clear from discussions that she was still taking sugary snacks and drinks more often than revealed in the diet sheet.
4.2 Acute pulpitis UR8. 4.3 Apical periodontitis UL5 4.4 Gross caries – UR8, UR7, UL4, UL5, UL8, LR4. Gross secondary caries LL8. 4.5 Non vital teeth UR7, UL8, LL8, LR4 4.6 Caries distal UL1 and secondary caries mesially 4.7 Secondary caries - UR5 mesial. Early secondary caries UR4 distal 4.8 Early caries - distal LL7, LL3, white spot lesion mesial UR2. 4.9 UL6 Unsatisfactory root canal treatment present. Separated instrument in
mesiobuccal canal. Periapical inflammatory lesions on all three roots. 4.10 LR5 Orthograde root filling 1-2 mm short of the radiographic apex, periapical
inflammatory lesion, area of resorption. 4.11 Overbuilt crown on LL5. This did not seem to be associated with more plaque
build up than other areas. The patient was not concerned about the aesthetics of this tooth and it was not causing any occlusal interference.
4.12 There was a substantial overhanging margin on the large amalgam restoration
at UL6. 4.13 Oral hygiene whilst not perfect revealed regular use of a toothbrush. There
was marginal gingivitis especially around posterior teeth. 4.14 Fine fragment of bone/root/foreign body mesial LL7. The patient was not
aware of this and it was not visible clinically.
13
5. Treatment plan
5.1 Emergency treatment 5.1.1 Extraction of UR8
5.2 Stabilisation phase 5.2.1 Preventive measures
Diet advice Fluoride advice Oral hygiene instruction
5.2.2 Extraction of teeth of hopeless prognosis UL8, LL8
5.2.3 Removal of iatrogenic factors Removal of ledge UL6
5.2.4 Non surgical periodontal treatment Scaling and polishing
5.2.5 Endodontic treatment UR7, UL5, LR4
5.2.6 Preliminary restoration of carious teeth UR7 UR5, UL1, UL4, UL5, LR4
5.3 Reassessment and maintenance 6 months 5.3.1 Reassess diet 5.3.2 Reassess oral hygiene 5.3.3 Assess compliance with fluoride advice 5.3.4 Bitewing radiographs 5.3.5 Review
Early carious lesions UR4, UR2, LL7, LL3, Overbuilt crown LL5 Fragment mesial LL7
5.3.6 Consider Further diet advice Further scaling and oral hygiene instruction Further stabilisation as necessary
5.4 Reassessment and maintenance 12 months As in 5.3 In addition :
5.4.1 Periapical radiographs of all endodontically treated teeth 5.4.2 Review endodontically treated teeth
Treated by candidate in last course of treatment Pre-existing root canal treatments External resorption LR5
5.4.3 Consider further endodontic treatment
5.5 Restorative phase 5.5.1 Consider
Cast restorations for endodontically treated teeth New crown LR5, LL5
5.6 Continual reassessment and maintenance
THIS CASE IS PRESENTED AT THE COMPLETION OF THE
STABILISATION PHASE.

14
6. Discussion of treatment plan 6.1 Treatment objectives for stabilisation phase
Relief of pain
Motivation of the patient in prevention of further dental disease
Resolution of marginal gingivitis
Restoration of carious teeth to form, function and aesthetics where possible and appropriate
6.2 Patient’s attitude
The patient seemed motivated and determined to make a fresh start with her oral health. The candidate was encouraged by the patient’s request for information about sugar free snacks even before a diet sheet was issued. Mrs SJ did not appear anxious during treatment and even seemed to enjoy her visits. She is intelligent, understood the advice very easily and has begun to examine food labels for sugar content. It is hoped that this enthusiasm is maintained and that it will yield benefits for her future oral health.
6.3 Discussion of possible alternative treatment plans
The rationale for this treatment plan was to stabilise the oral condition and ensure compliance with preventive measures before proceeding to more complex restorative work. At the same time it was planned to keep options for future care open by avoiding extraction where appropriate.
The following aspects were considered:
6.3.1 Restoration of the endodontically treated teeth UR7, UL5, LR4 These teeth were severely weakened firstly by caries and subsequently by endodontic procedures.
4,5 The aim of restoration was therefore to protect the
remaining tooth structure. Two options were considered: Cast restorations:
These have the advantage of maximum protection and control over the occlusion. However it was felt that cast restorations were inconsistent with the aim of stabilisation and review before proceeding with complex restorative work:
Amalgam restorations incorporating cusp capping
These have the disadvantage of difficulty in establishment of good contour and occlusion. However they were felt to provide sufficient protection, were consistent with the aim of stabilisation and review, keep open the option of a partial coverage cast restorations at a later stage and are relatively inexpensive.
6.3.2 Treatment of the third molars on the left side The prognosis for the grossly carious UL8 was considered very poor. Although restoration was theoretically possible it was in practice considered unrestorable. The caries was gross and subgingival. There was very little remaining tooth structure and any endodontic therapy would be complicated by difficult access and sclerosed root canals.

15
Having made the decision to extract UL8 the treatment of LL8 was considered. This tooth had gross secondary caries distally. Restoration was possible but would be complicated by deep subgingival caries and possibly the need for endodontic therapy. Having made the decision to extract UL8, LL8 had no opposing tooth and it was decided that the best interests of the patient would be served by extraction.
6.3.3 Unsatisfactory endodontic treatment UL6, LR5 These teeth had existing root canal treatments which appeared unsatisfactory. There is a fractured instrument in the mesiobuccal canal of UL6 and the root filling at LR5 seemed poorly condensed. Both had associated periapical radiolucencies. However both teeth were symptomless and there was no sinus or buccal tenderness. Furthermore it was not known whether the periapical radiolucencies were becoming larger, smaller or staying the same. In addition there are the difficulties associated with re-treatment and the removal of the cast post at LR5. Under these circumstances further endodontic therapy was felt to be inconsistent with the aim of stabilisation and review and it was decided that further radiographs in 1 year would be the most appropriate course.
6.3.4 Consideration of overbuilt crown LL5 Although the crown at LL5 is overbuilt it is not associated with marginal gingivitis any more than other areas. Mrs SJ is not concerned by the appearance and it is not causing occlusal interference. It was therefore decided that it was satisfactory at this stage of the treatment plan
6.3.5 Missing teeth from lower arch LL4, LL6, LR6 Mrs SJ had not expressed any wish to have these missing teeth replaced and was unconcerned about the aesthetic effect of the spaces. There were no unopposed teeth which might over-erupt. It was considered that in the absence of good oral hygiene a partial denture would be damaging and fixed restorations would not be appropriate to the stabilisation phase of treatment. Further it was not felt that there was any good reason for replacement. The remaining teeth were functional, aesthetic, stable and more than met the requirements of the shortened dental arch
6 and satisfaction with oral function.
7
6.3.6 Restoration of UL1 The existing restoration on UL1 involved the mesial incisal angle. There was secondary caries around this restoration and a new lesion distally. The following options were considered: Glass ionomer
This material has the advantage of fluoride release but comparatively poor aesthetics It’s mechanical properties and relatively weak bond to tooth substance would not allow it to be used for the load bearing mesial incisal angle.
Cast gold
This material would have good mechanical properties. However it has a number of disadvantages: The appearance of gold anteriorly is unacceptable to many people. Its use in a large complex situation would be time consuming and involve further destruction of tooth substance for retentive features. It’s use would be inconsistent with the aim of

16
stabilisation and review before proceeding with complex restorative work. It would also have added considerably to the expense to the patient
Crown/veneer.
The pattern of caries in this tooth was not suitable for veneer placement and both a crown and a veneer were considered unnecessarily destructive. Good appearance could be achieved by indirect methods.
Composite resin
Composite resin was considered the ideal material for use in this situation. It has a good bond to tooth substance and it’s mechanical properties allow it to be used in a load bearing situation. It’s bond to tooth would avoid unnecessary tooth preparation and it has superior aesthetics.
6.3.7 Restoration of UR5 & UL4 Alternatives were: Direct composite restorations
The restorations were medium to large and had occlusal stops present. Wear is therefore of importance. In addition it is difficult to establish good contour and contact points with composite resin
Indirect alternatives Gold, composite or porcelain inlays would give good control over contact points, contour and occlusion. Gold would enable protection of weakened cusps, in particular the compromised buccal cusp of UR5. However the indirect option was rejected on the following grounds:
Indirect techniques were inconsistent with the aim of stabilisation and review.
Indirect techniques would add considerably to the cost
The patient was unconcerned about a cosmetic solution for these teeth.
Future endodontic treatment may be necessary for these heavily filled teeth.
Poor success rate of porcelain and composite inlays.
Amalgam restorations Amalgam restorations were chosen for the following reasons:
Ability to establish good contact points and contour
Long term success rate.
Inexpensive
Ability to support the occlusion
Good wear characteristics
6.3.8 Presence of fragment mesial LL7 Mrs SJ was unaware of this fragment and it was not evident clinically. Other matters were considerably more pressing. Mrs SJ was made aware of this fragment and it was agreed that this would be reviewed with a view to removal in the next course of treatment.

17
6.3.9 Early carious lesions Early carious lesions were present at UR4, UR2, LL7, & LL3. The decision was therefore to treat operatively or preventively. UR2 was a white spot lesion which was directly visible and not cavitated. The secondary caries at UR4 was confined to enamel radiographically. The caries at LL3 was confined to enamel radiographically. The most advanced lesion radiographically was the distal lesion on LL7. The planned extraction of LL8 would enable a direct examination of the lesion to confirm or disprove cavitation and also change it’s environment considerably. It was therefore decided that these lesions would be treated preventively and reviewed in six months.
7. Treatment carried out 7.1 Visit 1 1.9.98 - pain relief, extraction of UR8 Mrs SJ attended the practice as an emergency complaining of a constant throbbing pain on the upper right side. A medical history form was completed. (Appendix A) Mrs SJ clearly indicated that UR8 was the painful tooth. This was grossly carious. UR8 was exquisitely sensitive to cold air and painful to light percussion. UR7 was also grossly decayed. However this tooth was not tender to percussion or sensitive to cold air. A diagnosis of acute pulpitis of UR8 was made. UR8 was unopposed and the candidate elected to extract this tooth. There was food trapping in UR7 and a sharp edge to the cavity. A dressing of zinc oxide eugenol cement was placed in UR7. A 2% solution of lignocaine hydrochloride with 1 in 80,000 adrenaline was administered using an aspirating syringe. This agent and pattern of syringe were subsequently used whenever a local anaesthetic was given to Mrs SJ. In this case infiltration local anaesthetic was applied buccally and palatally to UR8. Some 1.5 mls was used. The extraction was performed uneventfully using straight elevators and bayonet forceps. Haemostasis was obtained. Post operative instructions were given both verbally and in writing. (Appendix I). A 3 day diet sheet was issued (Appendix H)
The candidate’s priority at this visit was to alleviate the patient’s pain whilst leaving open options for further treatment. A second appointment was made for a comprehensive examination and assessment.
7.2 Visit 2 4.9.98 - examination and assessment. Mrs SJ reported that her pain had gone completely. A full history and examination were carried out as follows:
Extra oral examination
Intra oral soft tissue examination
Bilateral bitewing radiographs using film holders. (Page 10)
Periapical radiographs UR7, UL4, UL8, LL8, LL5, LR4, LR5, using film holders. (Page 10)
BPE recording (Page 11)

18
Charting of teeth, restorations and caries present, (Page 11)
Articulatory system examination (Appendix C)
Alginate impressions for study casts
Photographs
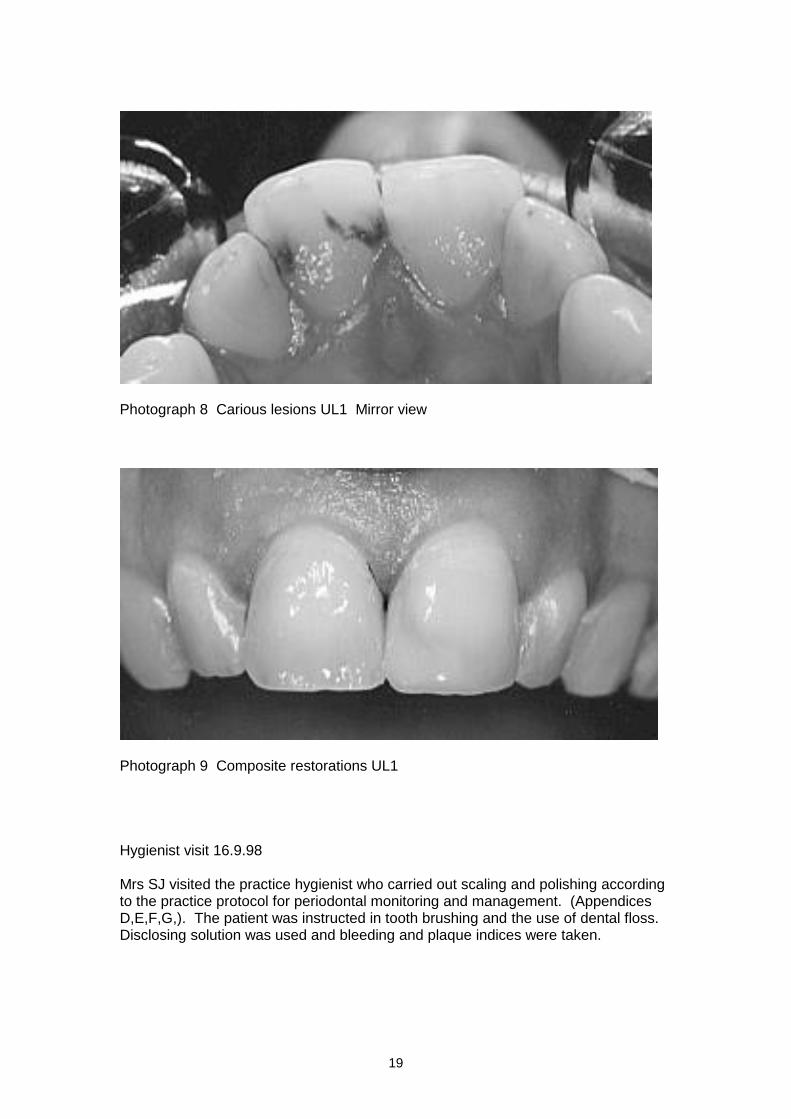
Vitality testing (see 3.7.2 page 10) The patient was given a fluoride mouth rinse 0.05% and instructed to use this twice a day, morning and afternoon. Mrs SJ was also advised to continue using a fluoride toothpaste first thing in the morning and last thing at night. The proposed treatment plan was discussed with the patient who agreed to the suggestions made. It was agreed that the patient would be treated under the terms of the National Health Service. Mrs SJ was referred to the practice hygienist under a prescription from the candidate. 7.3 Visit 3 7.9.98 - Extraction LL8, UL8 Infiltration local anaesthesia was administered buccally and palatally to UL8. Inferior dental block and long buccal anaesthesia was administered on the left side. Some 4 mls was used in total. The extractions of UL8 and LL8 were performed using elevators and forceps. Some difficulty was encountered with the extraction of LL8, the apical 2-3mm turning severely buccally. However the whole tooth was delivered with no apical fragment being retained. Haemostasis was obtained. Post operative instructions were given both verbally and in writing (Appendix I) A visual examination of the distal surface of LL7 revealed that the early carious lesion was not cavitated. 7.4 Visit 4 11.9.98 - Discussion of diet sheets, restoration of UL1 The patient returned the diet sheets. These were analysed and discussed. It was clear that the diet sheets did not tell the whole story and the patient reported that she had recently changed her dietary habits, cutting out sugary snacks and drinks between meals. However it was shown that the patient was taking frequent cups of coffee with two sugars. She also admitted to eating chocolate bars more frequently than shown on the diet sheet. Specific advice was given in these regards and recorded on a practice leaflet which was given to the patient. A copy was kept in the records so that the advice could be discussed further and reviewed at future appointments. (Appendix J) Mrs SJ was also given a copy of the practice leaflet ‘Sugar the Hidden Enemy’.(Appendix K). Mrs SJ enquired specifically about alternatives to sugary snacks and was given a copy of the practice leaflet ‘Top ten safe snacks for teeth’ .(Appendix L) Buccal infiltration local anaesthesia was applied to UL1 and rubber dam fitted. Cavity preparation was carried out for class 3 cavities mesially and distally and a separate class 4 cavity mesio incisally. (Photograph 8 pg 19). 37% phosphoric acid was applied to the enamel for 20 seconds and the dentine for 10 seconds. After washing and partial drying a dentine bonding agent was applied and blown dry. Unfilled resin sealer was then applied and blown dry. This was cured with a curing light for 20 seconds. A light cured hybrid composite was used to restore the tooth. (Photograph 9 pg 19). The patient was delighted with the new appearance of this tooth and it was believed that this helped to motivate the patient.
19
Photograph 8 Carious lesions UL1 Mirror view
Photograph 9 Composite restorations UL1 Hygienist visit 16.9.98 Mrs SJ visited the practice hygienist who carried out scaling and polishing according to the practice protocol for periodontal monitoring and management. (Appendices D,E,F,G,). The patient was instructed in tooth brushing and the use of dental floss. Disclosing solution was used and bleeding and plaque indices were taken.

20
7.5 Visit 5 21.9.98 - restoration of UL4, UL5 The badly decayed UL4 UL5 were investigated. Both teeth had tested positively to electric pulp testing. Buccal infiltration local anaesthesia was administered and rubber dam fitted. Removal of the existing amalgam fillings with a water cooled high speed handpiece revealed the extensive soft decay below. (Photograph 10 pg 20) Decay was initially removed with steel round headed burs in a slow handpiece. The deeper parts were excavated by hand using excavators. Even a careful removal of only soft decay by hand revealed an exposure of the pulp on UL5. (Photograph 11 pg 20) The root canal of UL5 was then opened and one wide canal was identified. The canal orifice was widened using Gates Glidden burs. (photograph 12 pg 21) The root length was determined using an electronic apex locator and checked with a diagnostic radiograph at 19mm. This was precisely at the radiographic apex of the tooth and thus the candidate decided on a working length of 18mm Although not exposed there was some stained dentine at the base of the cavity at UL4. In this case the candidate decided to apply an indirect pulp cap of light cured calcium hydroxide cement over the deepest part of the cavity followed by an overall lining of glass ionomer
8 A matrix band was fitted and adapted gingivally with
wooden wedges. The cavity was restored with a high copper, spherical amalgam alloy. (Photograph 12 pg 21). After removal of the dam the occlusion was checked with Hanel articulating paper and shimstock held in Miller’s forceps. The patient was warned that the restoration was deep and may give postoperative discomfort for a few days. Mrs SJ was advised to take an ibuprofen 200mg tablet up to six times per day initially if there was discomfort. The patient was also advised to telephone the practice if symptoms worsened. The UL5 was temporarily dressed with non setting calcium hydroxide, a sterile cotton wool pledget and reinforced zinc oxide eugenol cement. (Radiographs pg 21)
10
11
Photographs 10,11, Treatment of UL4, UL5 Mirror views
21
4.9.98 21.9.98
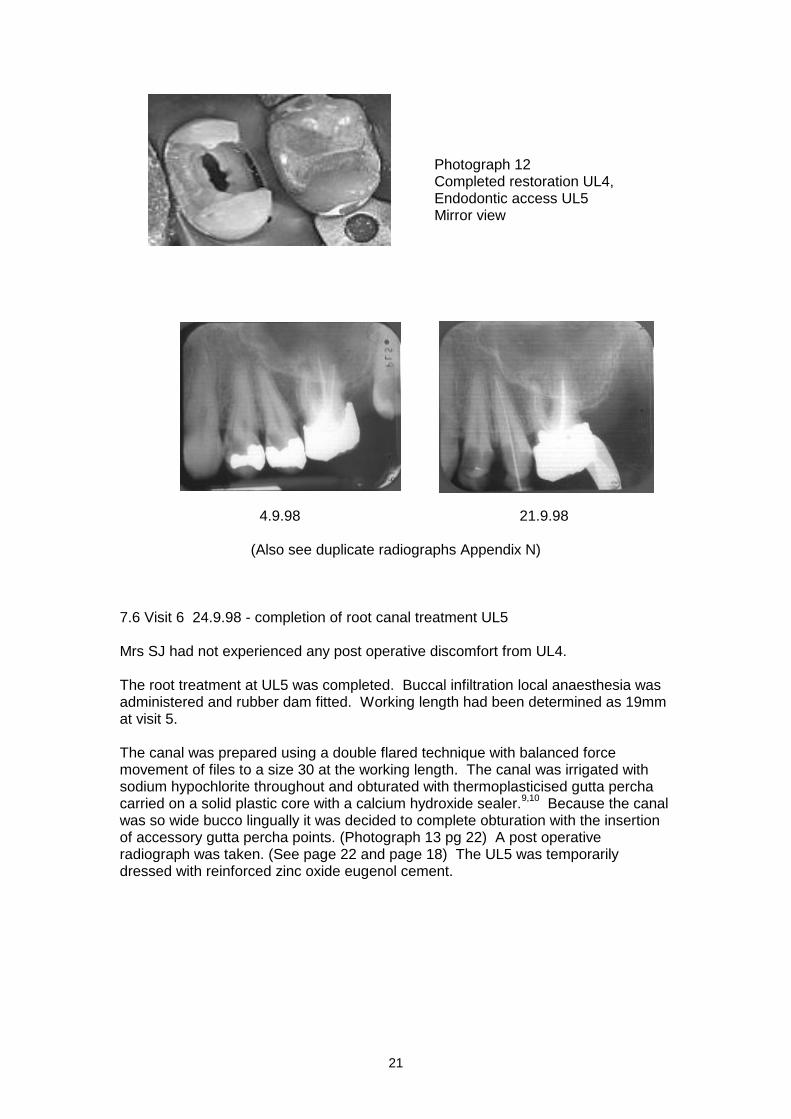
(Also see duplicate radiographs Appendix N) 7.6 Visit 6 24.9.98 - completion of root canal treatment UL5 Mrs SJ had not experienced any post operative discomfort from UL4. The root treatment at UL5 was completed. Buccal infiltration local anaesthesia was administered and rubber dam fitted. Working length had been determined as 19mm at visit 5. The canal was prepared using a double flared technique with balanced force movement of files to a size 30 at the working length. The canal was irrigated with sodium hypochlorite throughout and obturated with thermoplasticised gutta percha carried on a solid plastic core with a calcium hydroxide sealer.
9,10 Because the canal
was so wide bucco lingually it was decided to complete obturation with the insertion of accessory gutta percha points. (Photograph 13 pg 22) A post operative radiograph was taken. (See page 22 and page 18) The UL5 was temporarily dressed with reinforced zinc oxide eugenol cement.
Photograph 12 Completed restoration UL4, Endodontic access UL5 Mirror view

22
Photograph 13 Completion of endodontic treatment UL5 Mirror view 7.7 Visit 7 28.9.98 - restoration of UL5 in amalgam Local anaesthetic was not administered on this occasion but the patient was advised to raise her hand if she felt discomfort. Rubber dam was applied to UL5. 3mm of the root canal was used for resistance and retention. Since this was an MOD cavity there were no marginal ridges and the remaining buccal and palatal cusps were higher than they were wide. For this reason they were considered at high risk of fracture and were reduced. A matrix band was used with wooden wedges. (Photograph 14 pg 22) and an amalgam restoration was placed capping the buccal and palatal cusps.(Photograph 15 pg 22) The occlusion was checked.
Photographs 14 & 15 Amalgam restoration UL5 Mirror views
Post operative radiograph Endodontic treatment UL5 24.9.98 (Also see duplicate radiographs appendix N)

23
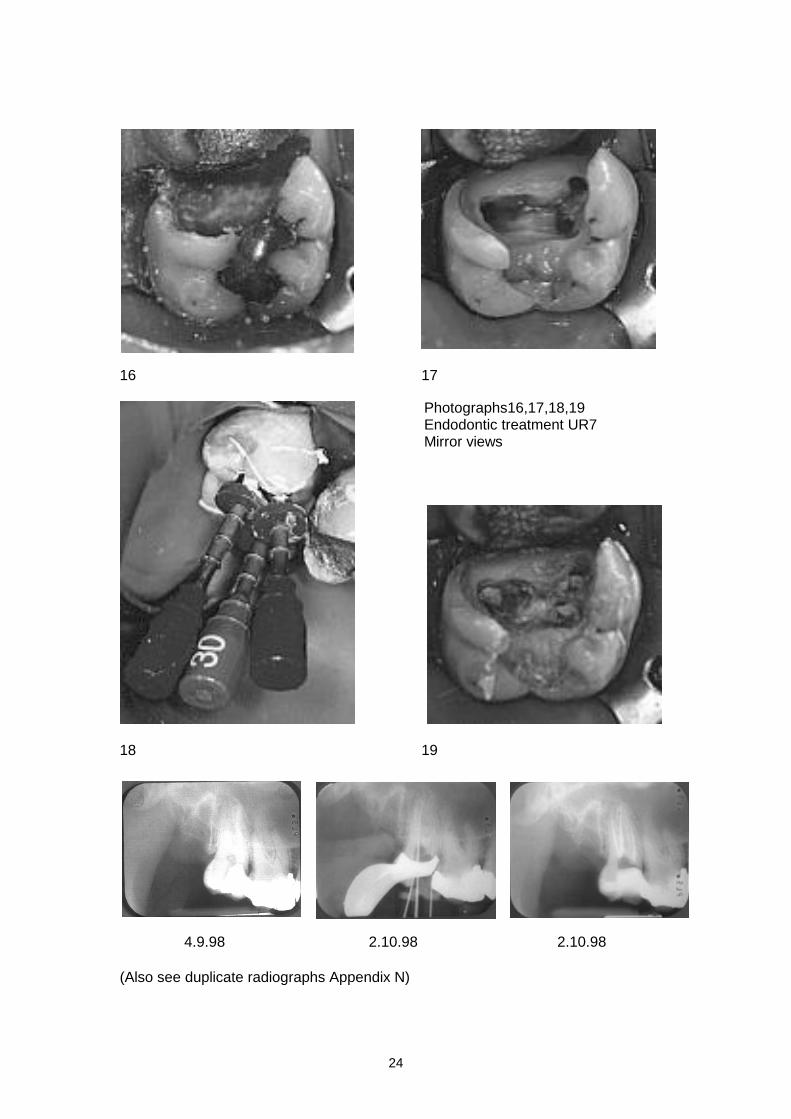
7.8 Visit 8 2.10.98 - root canal treatment UR7 Buccal infiltration local anaesthesia was administered to UR7 and rubber dam fitted. The zinc oxide eugenol dressing was removed and the extent of the decay revealed (Photograph 16 pg 24) . Removal of the decay revealed at an early stage that the pulp chamber was involved and that the tooth was non vital with a necrotic pulp as indicated by electric pulp testing. An access cavity was opened and three canals opened. The candidate checked for the presence of a second mesiobuccal canal. The canal orifices were widened using Gates Glidden burs. (photograph 17 pg 24) Working lengths were determined using an electronic apex locator and checked with a diagnostic radiograph. These were considered to be acceptable working lengths. They were: palatal canal 19mm, mesiobuccal canal 18mm and distobuccal canal 20mm. The canals were prepared using a double flared technique with balanced force movement of files. The palatal canal was prepared to a size 30 at the working length and the buccal canals to size 25 at the working length. The canals were irrigated with sodium hypochlorite throughout and they were obturated with thermoplasticised gutta percha carried on a solid plastic core with a calcium hydroxide sealer.
9,10 (Photographs 18 & 19, radiographs page 24). A post operative
radiograph was taken. The UR7 was temporarily dressed with a sterile cotton wool pledget and reinforced zinc oxide eugenol cement.
24
16 17
18 19
4.9.98 2.10.98 2.10.98
(Also see duplicate radiographs Appendix N)
Photographs16,17,18,19 Endodontic treatment UR7 Mirror views
25
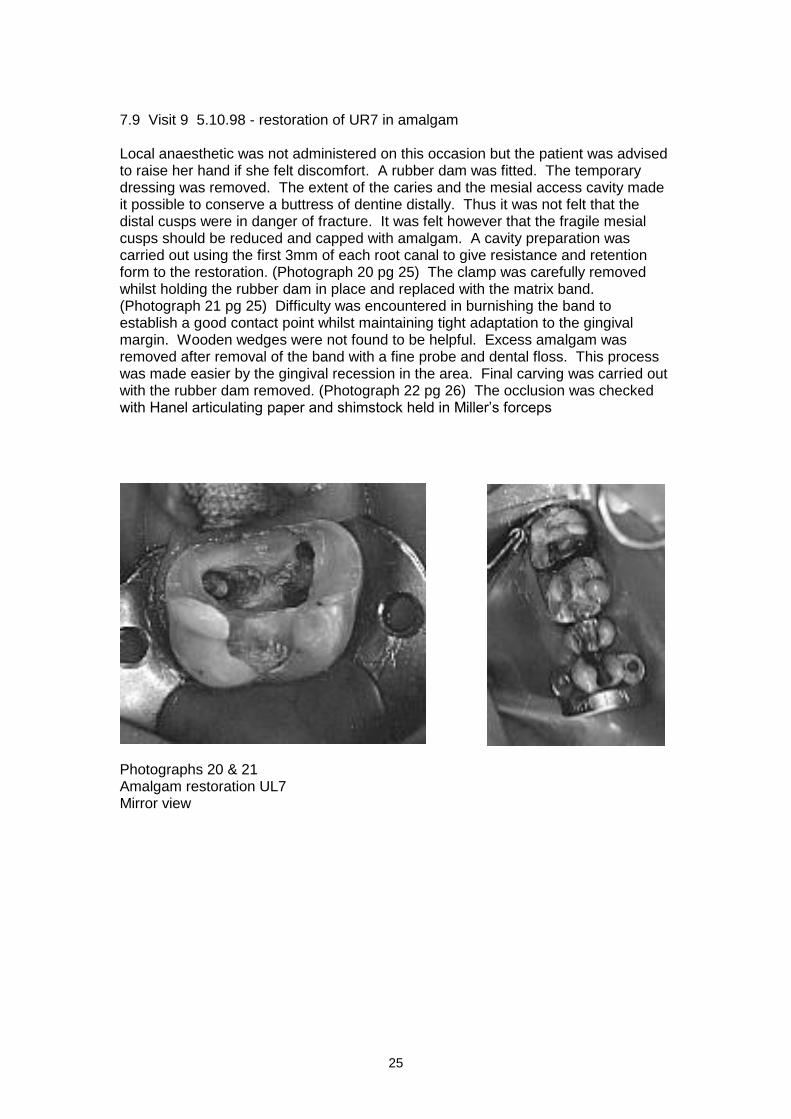
7.9 Visit 9 5.10.98 - restoration of UR7 in amalgam Local anaesthetic was not administered on this occasion but the patient was advised to raise her hand if she felt discomfort. A rubber dam was fitted. The temporary dressing was removed. The extent of the caries and the mesial access cavity made it possible to conserve a buttress of dentine distally. Thus it was not felt that the distal cusps were in danger of fracture. It was felt however that the fragile mesial cusps should be reduced and capped with amalgam. A cavity preparation was carried out using the first 3mm of each root canal to give resistance and retention form to the restoration. (Photograph 20 pg 25) The clamp was carefully removed whilst holding the rubber dam in place and replaced with the matrix band. (Photograph 21 pg 25) Difficulty was encountered in burnishing the band to establish a good contact point whilst maintaining tight adaptation to the gingival margin. Wooden wedges were not found to be helpful. Excess amalgam was removed after removal of the band with a fine probe and dental floss. This process was made easier by the gingival recession in the area. Final carving was carried out with the rubber dam removed. (Photograph 22 pg 26) The occlusion was checked with Hanel articulating paper and shimstock held in Miller’s forceps
Photographs 20 & 21 Amalgam restoration UL7 Mirror view
26
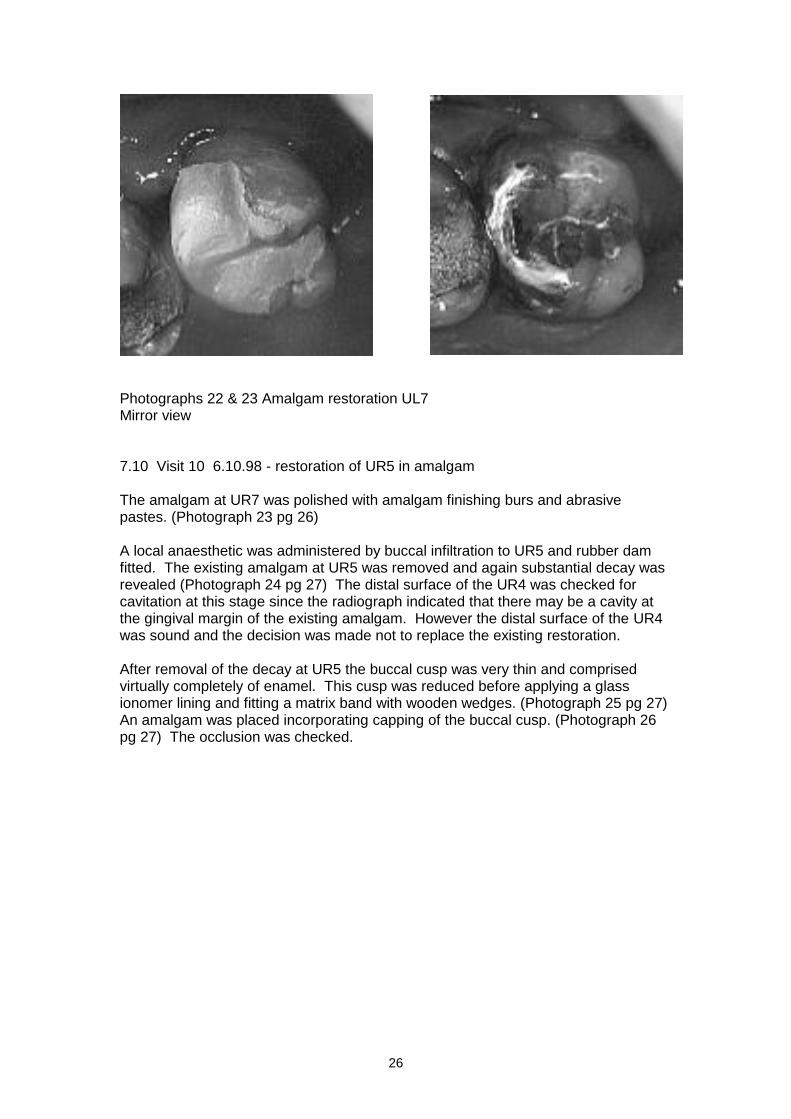
Photographs 22 & 23 Amalgam restoration UL7 Mirror view 7.10 Visit 10 6.10.98 - restoration of UR5 in amalgam The amalgam at UR7 was polished with amalgam finishing burs and abrasive pastes. (Photograph 23 pg 26) A local anaesthetic was administered by buccal infiltration to UR5 and rubber dam fitted. The existing amalgam at UR5 was removed and again substantial decay was revealed (Photograph 24 pg 27) The distal surface of the UR4 was checked for cavitation at this stage since the radiograph indicated that there may be a cavity at the gingival margin of the existing amalgam. However the distal surface of the UR4 was sound and the decision was made not to replace the existing restoration. After removal of the decay at UR5 the buccal cusp was very thin and comprised virtually completely of enamel. This cusp was reduced before applying a glass ionomer lining and fitting a matrix band with wooden wedges. (Photograph 25 pg 27) An amalgam was placed incorporating capping of the buccal cusp. (Photograph 26 pg 27) The occlusion was checked.
27
24 25
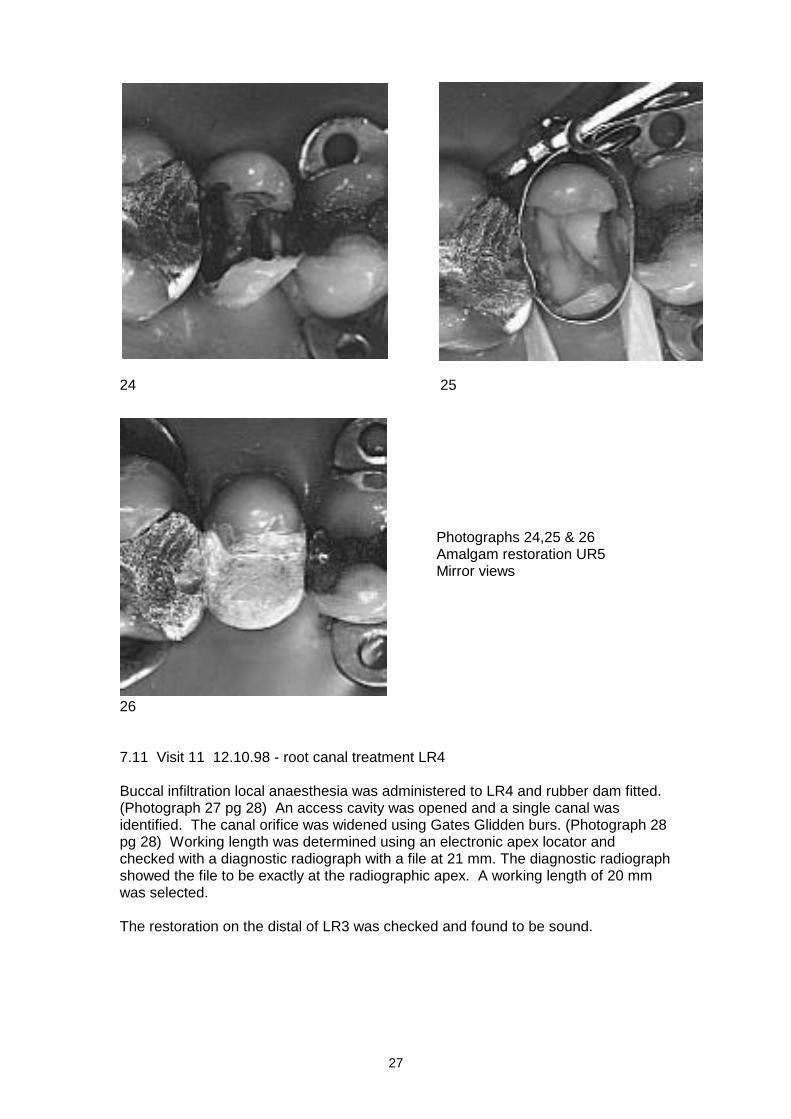
Photographs 24,25 & 26 Amalgam restoration UR5 Mirror views
26
7.11 Visit 11 12.10.98 - root canal treatment LR4 Buccal infiltration local anaesthesia was administered to LR4 and rubber dam fitted. (Photograph 27 pg 28) An access cavity was opened and a single canal was identified. The canal orifice was widened using Gates Glidden burs. (Photograph 28 pg 28) Working length was determined using an electronic apex locator and checked with a diagnostic radiograph with a file at 21 mm. The diagnostic radiograph showed the file to be exactly at the radiographic apex. A working length of 20 mm was selected. The restoration on the distal of LR3 was checked and found to be sound.
28
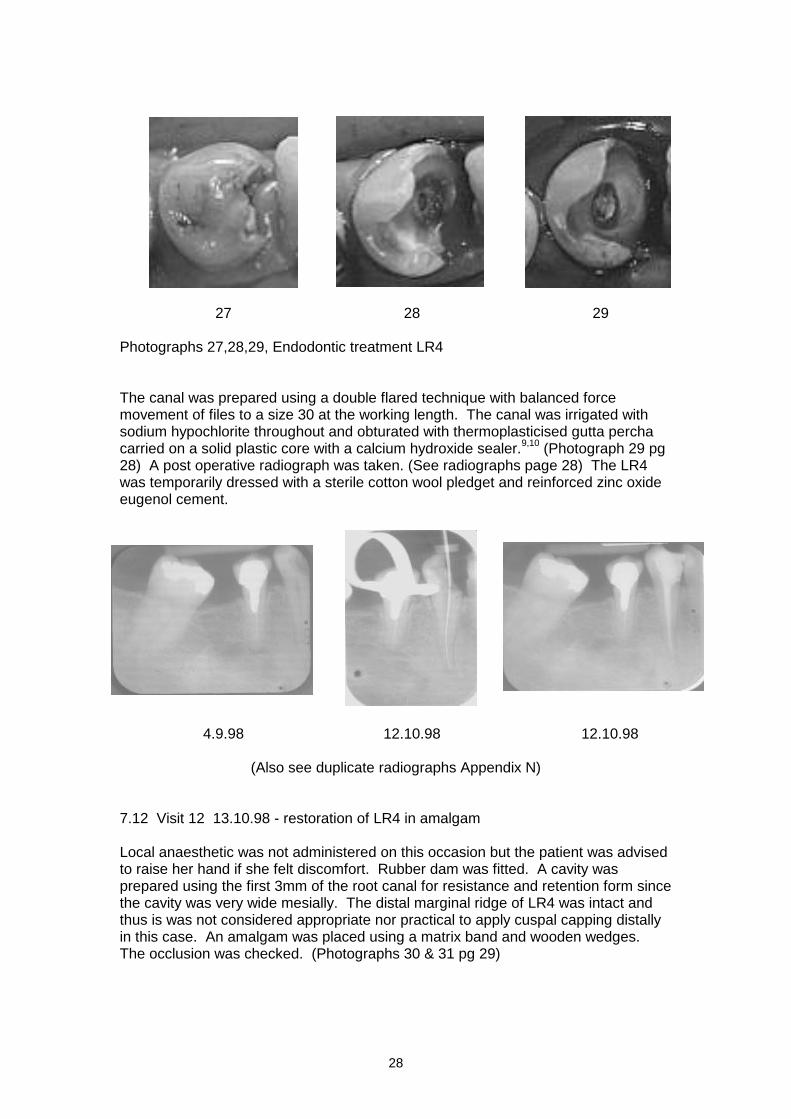
27 28 29 Photographs 27,28,29, Endodontic treatment LR4 The canal was prepared using a double flared technique with balanced force movement of files to a size 30 at the working length. The canal was irrigated with sodium hypochlorite throughout and obturated with thermoplasticised gutta percha carried on a solid plastic core with a calcium hydroxide sealer.
9,10 (Photograph 29 pg
28) A post operative radiograph was taken. (See radiographs page 28) The LR4 was temporarily dressed with a sterile cotton wool pledget and reinforced zinc oxide eugenol cement.
4.9.98 12.10.98 12.10.98
(Also see duplicate radiographs Appendix N)
7.12 Visit 12 13.10.98 - restoration of LR4 in amalgam Local anaesthetic was not administered on this occasion but the patient was advised to raise her hand if she felt discomfort. Rubber dam was fitted. A cavity was prepared using the first 3mm of the root canal for resistance and retention form since the cavity was very wide mesially. The distal marginal ridge of LR4 was intact and thus is was not considered appropriate nor practical to apply cuspal capping distally in this case. An amalgam was placed using a matrix band and wooden wedges. The occlusion was checked. (Photographs 30 & 31 pg 29)

29
30 31 Photographs 30,31, Amalgam restoration LR4 Mirror views 7.13 Visit 13 16.10.98 - polishing amalgam, reinforce dietary advice. , removal of ledge UL6 The patient’s amalgams were polished using steel amalgam finishing burs in a slow handpiece and finished with a nylon brush and abrasive pastes. The large overhanging ledge on the UL6 was trimmed with diamond burs until flush with the tooth surface. Final photographs were taken. Diet was discussed with the patient again who seemed to take the advice very seriously. She had begun to choose sugar free snacks and drinks and to check labels for sugar content. Hygienist visit 21.10.98 Mrs SJ attended for a second hygienist appointment where an improvement in oral hygiene was noted. Further scaling and polishing was carried out and oral hygiene reinforced. (Appendix F)

30
Photograph 32 Completion of stabilisation phase
8. Appraisal of treatment Treatment progressed very satisfactorily for this patient. The candidate encountered some difficulty in manipulation of amalgam where the cusps were capped especially on the premolars. It was however possible to maintain reasonable control over the occlusion.
Root canal treatments The root canal treatment at UL5 appeared ideal radiographically at 1mm short of the radiographic apex and well condensed. The result at LR4 had a small escape of sealant from the apex although this was considered an acceptable result. The root canal fillings at UR7 appeared to be some 2mm short of the apex on both buccal roots. This is not inconsistent with success. Follow up radiographic and clinical examination will be necessary for all the root treated teeth for Mrs SJ.
9. Discussion of any variation from the original plan From the radiographic appearance it was thought likely that root canal treatments would be necessary on both UL4 and UL5. However the pattern of reactive dentine formation on UL4 made this unnecessary. It will however be necessary to monitor the vitality of this previously heavily carious tooth.
10. Patient - compliance and attitude The patient was enthusiastic enough to complete 13 visits in a little over 6 weeks. Mrs SJ has become enthusiastic about her oral health during the course of dental care. Her requests for further information were encouraging and it is to be hoped that this enthusiasm is maintained to the benefit of her oral health.

31
11. Prognosis and maintenance The key to this treatment plan has been prevention. There have been two visits to the practice hygienist with disclosing and toothbrush instruction, Fluoride advice has been given and a 0.05% fluoride mouth rinse prescribed. A diet sheet was issued, returned and discussed. Diet advice was re-inforced with practice leaflets. (Appendices J,K & L). The initial patient response appears good in this respect although the candidate appreciates the need for constant vigilance. Maintenance schedule
11.1 3 months Hygienist visit
11.2 6 months Reassess diet Reassess oral hygiene, take bleeding and plaque indices Assess compliance with fluoride advice Bitewing radiographs
Review Early carious lesions UR4, UR2, LL7, LL3, Overbuilt crown LL5 Fragment mesial LL7
Consider Further diet advice Further scaling and oral hygiene instruction Further stabilisation as necessary
11.3 12 months As in 11.2 In addition : Periapical radiographs of all endodontically treated teeth Review endodontically treated teeth
Treated by candidate in last course of treatment Pre-existing root canal treatments Resorption LR5
Consider further endodontic treatment
11.4 Outstanding problems Protection of root treated teeth
An outstanding problem following this course of stabilisation is the presence of three posterior teeth which have undergone endodontic treatment, UR7, UL5 and LR4. These teeth have lost a considerable amount of their structure and are thus more prone to fracture.
4 The candidate felt that whilst cast
restorations are ideal they were inappropriate on the grounds of a high caries rate. These teeth were restored using the pulp chamber and first 3mm of the root canals as retention for complex amalgams involving cuspal capping
11
This has the advantage of giving time to evaluate the success of the endodontic treatments on these teeth. Nevertheless the candidate would prefer to advance to cast restorations on these teeth as soon as oral stability and the success of the endodontic therapies can be demonstrated.

32
In addition the UL6 had undergone root treatment some 8 or 10 years before and has an MOD amalgam restoration in place. The candidate decided to continue to monitor this tooth and review in the light of the patient’s response to preventive measures.
Root fragment mesial LL7
Mrs SJ was unaware of the presence of a fragment and it was not detectable clinically. It was decided that it would be a simple procedure to remove the fragment if it appeared on the mucosal surface and it would be left in place until that time.
Existing endodontic treatments
UL6. Several options exist for the future management of this tooth including re-endodontic treatment, surgical endodontics, root resection and extraction. Further options exist for the coronal restoration such as amalgam or cast restoration. LR5. It cannot be said with certainty whether the radiographic appearance in the coronal third of the root represents previous internal or external resorption. An external lesion could not be detected clinically. The root canal treatment is some 1-2 mm short of the radiographic apex and there is widening of the periodontal membrane. LL5. There is little evidence of periapical pathology associated with this tooth. The overbuilt crown whilst unaesthetic is acceptable clinically and the appearance is not causing the patient any concern.
The candidate decided to continue to monitor these teeth and review in the light of the patient’s response to preventive measures.
Early carious lesions
Early carious lesions were present at UR2, LL7 and LL3. There was early secondary caries on the distal of UR4. The most extensive of these was the distal lesion on LL7. However this was not found to be cavitated on examination after the extraction of LL8. The removal of the LL8 would be expected to dramatically change the environment of the lesion. It was decided that an opportunity would be given for preventive measures to succeed.
33
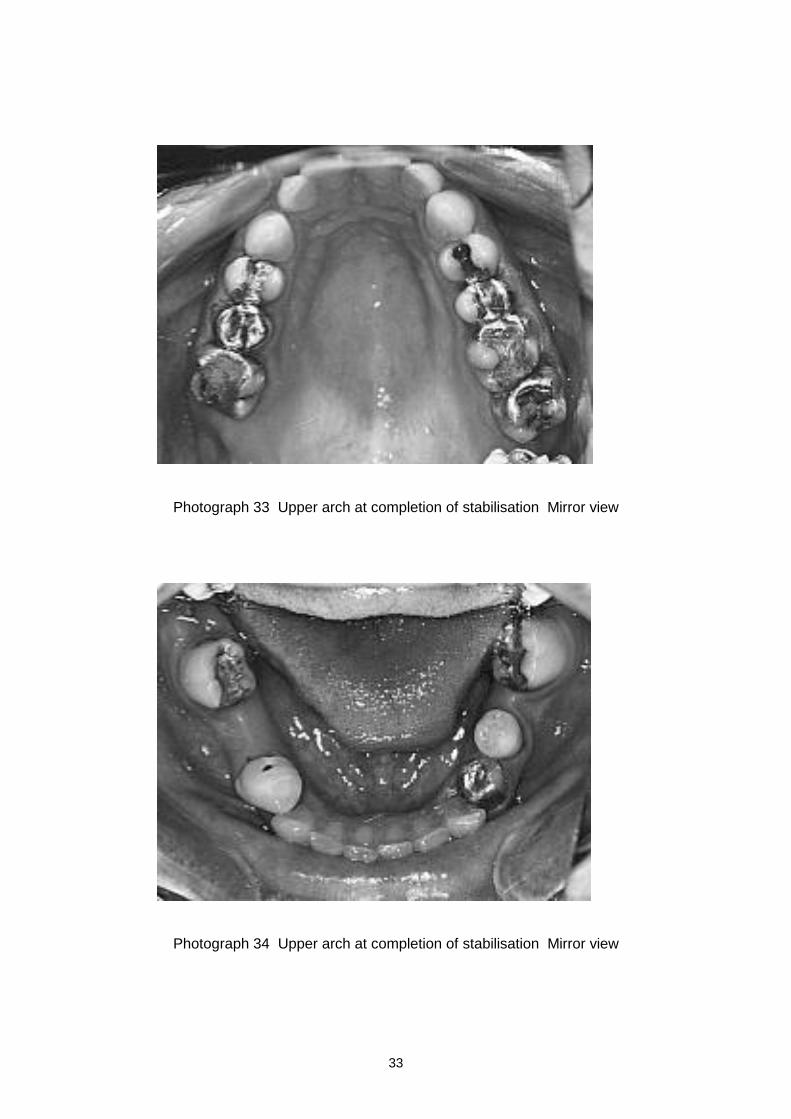
Photograph 33 Upper arch at completion of stabilisation Mirror view
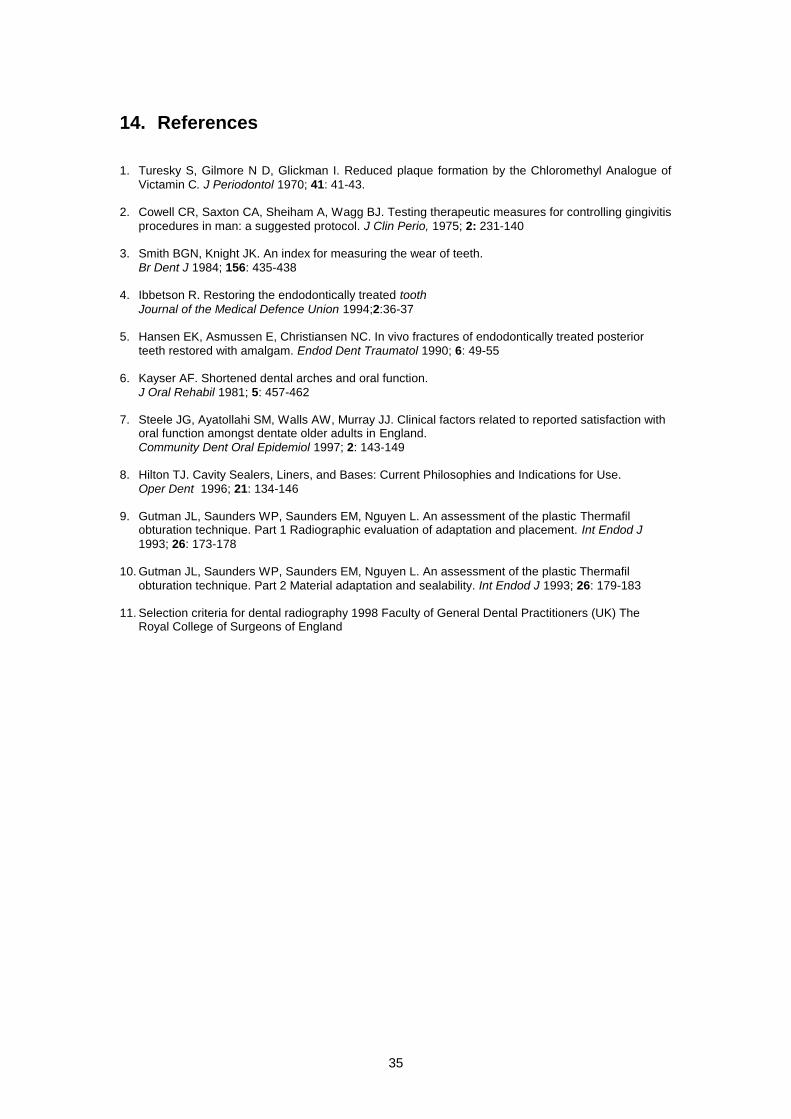
Photograph 34 Upper arch at completion of stabilisation Mirror view

34
12. Conclusions In the space of 6 weeks this patient has changed her diet and oral hygiene habits. She has acquired 6 restorations, three root canal treatments and lost three teeth. Future care will be dictated by the health of the pulps of the heavily restored teeth, the success of the old and new root canal treatments and her maintenance of a suitable diet and oral hygiene measures. Hopefully close monitoring and guidance will yield positive results and consideration can be given to further restorative work.
13. Note of word count 4972
35
14. References 1. Turesky S, Gilmore N D, Glickman I. Reduced plaque formation by the Chloromethyl Analogue of
Victamin C. J Periodontol 1970; 41: 41-43. 2. Cowell CR, Saxton CA, Sheiham A, Wagg BJ. Testing therapeutic measures for controlling gingivitis
procedures in man: a suggested protocol. J Clin Perio, 1975; 2: 231-140 3. Smith BGN, Knight JK. An index for measuring the wear of teeth.
Br Dent J 1984; 156: 435-438 4. Ibbetson R. Restoring the endodontically treated tooth
Journal of the Medical Defence Union 1994;2:36-37 5. Hansen EK, Asmussen E, Christiansen NC. In vivo fractures of endodontically treated posterior
teeth restored with amalgam. Endod Dent Traumatol 1990; 6: 49-55 6. Kayser AF. Shortened dental arches and oral function.
J Oral Rehabil 1981; 5: 457-462 7. Steele JG, Ayatollahi SM, Walls AW, Murray JJ. Clinical factors related to reported satisfaction with
oral function amongst dentate older adults in England.
Community Dent Oral Epidemiol 1997; 2: 143-149 8. Hilton TJ. Cavity Sealers, Liners, and Bases: Current Philosophies and Indications for Use.
Oper Dent 1996; 21: 134-146 9. Gutman JL, Saunders WP, Saunders EM, Nguyen L. An assessment of the plastic Thermafil
obturation technique. Part 1 Radiographic evaluation of adaptation and placement. Int Endod J
1993; 26: 173-178 10. Gutman JL, Saunders WP, Saunders EM, Nguyen L. An assessment of the plastic Thermafil
obturation technique. Part 2 Material adaptation and sealability. Int Endod J 1993; 26: 179-183 11. Selection criteria for dental radiography 1998 Faculty of General Dental Practitioners (UK) The
Royal College of Surgeons of England
36
15. Appendices A. Medical history form B. Dental history form C. Articulatory system examination form D. Outline of practice protocol for periodontal monitoring E. Leaflets
. Gum disease fact sheet (given to Mrs SJ)
. Treatment of gum disease A (not given to Mrs SJ)
. Treatment of gum disease B (given to Mrs SJ)
. Treatment of gum disease C (not given to Mrs SJ)
. Personal plaque control programme (given to Mrs SJ) F. Hygienist record card including dentist's prescription G. Pages from visual aid 'Understanding Gum Disease' H. Diet record Mrs SJ I. Post operative advice leaflet for extractions and surgery J. Personal diet advice record K. Leaflet 'Sugar the Hidden Enemy' L. Leaflet 'Top ten safe snacks for teeth' M. Copies of clinical records N. Duplicate radiographs
16. Declaration of originality and patients consent