id unit presentation: enteric fever in lusaka
DESCRIPTION
DR NCHIMBA. ID UNIT PRESENTATION: ENTERIC FEVER IN LUSAKA. DEFINITIONS. Salmonella is a Gram-negative facultative rod-shaped bacterium belonging to family Enterobacteriaceae , - PowerPoint PPT PresentationTRANSCRIPT
ID UNIT PRESENTATION: ENTERIC FEVER IN LUSAKA
DR NCHIMBA

DEFINITIONS Salmonella is a Gram-negative facultative rod-
shaped bacterium belonging to family Enterobacteriaceae,
Salmonellae live in the intestinal tracts of warm and cold blooded animals. Some species are ubiquitous. Other species are specifically adapted to a particular host. Over 2400 serotypes.
In humans, Salmonella are the cause of two diseases: enteric fever, resulting from bacterial invasion of the
bloodstream, and acute gastroenteritis, resulting from a foodborne
infection/intoxication.

DEFINITIONS
ENTERIC FEVER – includes both typhoid and paratyphoid fevers. Both are caused by Salmonellae that are markedly more invasive and pathogenic than those that cause food poisoning
CAUSAL ORGANISMS – of typhoid fever is Salmonella enterica serotype typhi. S paratyphi A B and C cause paratyphoid fever.

HISTORY OF ENTERIC FEVER 1800 – Typhoid bacillus first observed in spleen
sections and mesenteric lymph-nodes from a patient who had died from typhoid
1881 - Robert Koch cultured the bacterium in lab (but differentiation from other enteric bacteria was uncertain)
1896 – sero-diagnosis made possible. Basis for Widal’s test demonstrated
Early 1900s – enter ‘TYPHOID MARY’ a food handler responsible for infecting at least 78 people and causing the death of 5

EPIDEMIOLOGY strongly
endemic Endemic sporadic
TRANSMISSION
S typhi and S paratyphi have no nonhuman vectors. Modes of transmission: Oral transmission via food or beverages handled
by an individual who chronically sheds the bacteria through stool or, less commonly, urine
Hand-to-mouth transmission after using a contaminated toilet and neglecting hand hygiene
Oral transmission via sewage-contaminated water or shellfish (especially in the developing world)

RISK FACTORS
Ingestion of antacids, H2 blockers, proton-pump inhibitors, gastrectomy
Genetic polymorphisms Environmental/ behavioural
Street vendors’ food Household contact Inadequate washing of hands Drinking unpurified water Home without a toilet Students in hostels with poor hygiene

PROTECTIVE
Protective host mutations occur in cystic fibrosis. Heterozygotes have a mutation which is associated with a decreased susceptibility to typhoid fever, cholera and TB

PATHOGENESIS

All pathogenic Salmonella species are engulfed by phagocytic cells, which then pass them through the mucosa and present them to the macrophages in the lamina propria.
With nontyphoidal salmonellae macrophages recognize pathogen-associated molecular patterns (PAMPs) such as flagella and lipopolysaccharides and then attract T cells and neutrophils with interleukin 8 (IL-8), causing inflammation and suppressing the infection.

S typhi enters the host's system primarily through the distal ileum.
It has specialized fimbriae that adhere to the epithelium over clusters of lymphoid tissue in the ileum (Peyer patches), the main relay point for macrophages traveling from the gut into the lymphatic system.
S typhi has a Vi capsular antigen that masks PAMPs, avoiding neutrophil-based inflammation. The bacteria then induce their host macrophages to attract more macrophages.

S typhi co-opts the macrophages' cellular machinery for its own reproduction as it is carried through the mesenteric lymph nodes to the thoracic duct and the lymphatics and then through to the reticuloendothelial tissues of the liver, spleen, bone marrow, and lymph nodes.
Once there, the S typhi bacteria pause and continue to multiply until some critical density is reached.
Afterward, the bacteria induce macrophage apoptosis, breaking out into the bloodstream to invade the rest of the body

The bacteria then infect the gallbladder via either bacteremia or direct extension of S typhi –infected bile.
Therefore the organism re-enters the GIT in the bile and reinfects Peyer patches or is shed in the stool and is then available to infect other hosts.


CLINICAL MANIFESTATIONS Factors that influence the severity and
overall clinical outcome of the infection: duration of illness before the initiation of
appropriate therapy choice of antimicrobial treatment Age previous exposure or vaccination history virulence of the bacterial strain quantity of inoculum ingested several host factors affecting immune status.

Clinical course if untreated 1st week – gradual onset. Fever,
headache, vomiting. Constipation. Rose spots.
2nd week – distended abd, tympanic note. Splenomegaly. Rales over the bases
3rd week – complication week 4th week – recovery/death
COMPLICATIONS GIT – haemorrhage, perforation
CNS - Encephalopathy, cerebral edema, subdural empyema, cerebral abscess, meningitis, transient parkinsonism, motor neuron disorders, ataxia, seizures, GBS, psychosis
CVS - Endocarditis, myocarditis, pericarditis, arteritis, CCF
PULM - Pneumonia, empyema, bronchopleura fistula
BONE/JOINT – osteomyelitis, septic arthritis
HEPATOBILIARY - Cholecystitis, hepatitis, hepatic abscesses, splenic abscess, peritonitis, paralytic ileus
GUT - Urinary tract infection, renal abscess, pelvic infections, testicular abscess, prostatitis, epididymitis
SOFT TISSUE - Psoas abscess, gluteal abscess, cutaneous vasculitis

Diagnosis of typhoid fever by culture and serology
18
Wk 1 Wk 2 Wk 3 Wk 4 Wk 5 Wk 6 Wk 7 Wk 80102030405060708090
100
BloodStoolUrineSerum agglutinins
Weeks of Illness
Perc
ent
of P
atie
nts
Wit
h Po
s-it
ive
Cult
ures

TREATMENT
Resistance to chloramphenicol well documented
MDR typhoid have necessitated the the use of Quinolones (drug of choice) and 3rd generation cephalosporins
Supportive care (fluid/electrolyte balance, fevers)
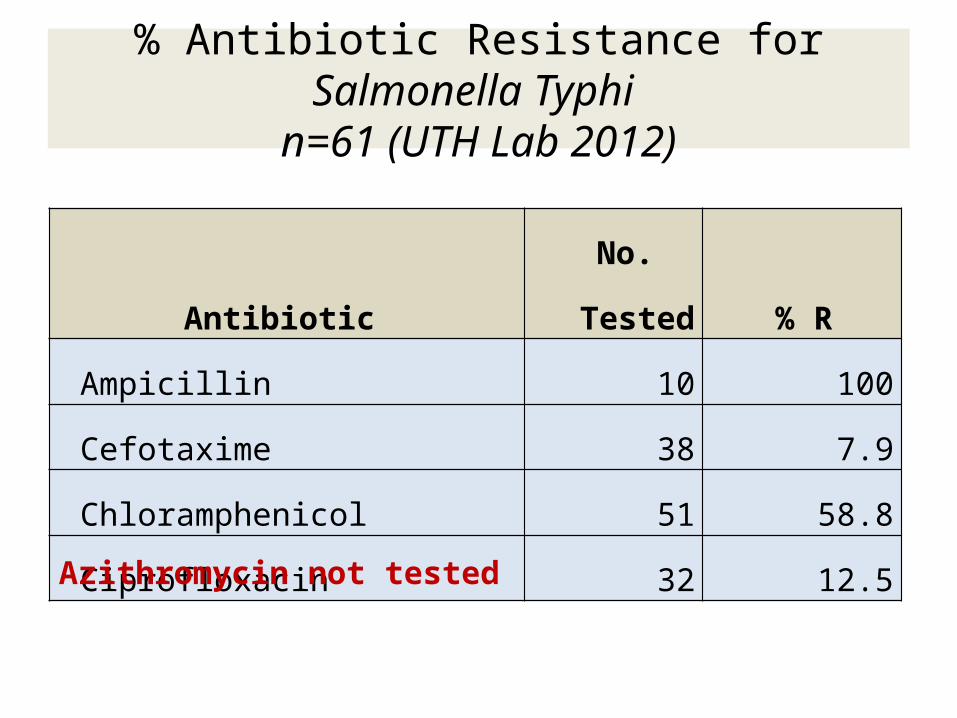
Antibiotic No.
Tested % R Ampicillin 10 100Cefotaxime 38 7.9Chloramphenicol 51 58.8Ciprofloxacin 32 12.5
% Antibiotic Resistance for Salmonella Typhi n=61 (UTH Lab 2012)
Azithromycin not tested
PROGNOSIS
Despite appropriate therapy, 2–4% of infected children may relapse after initial clinical response to treatment
Individuals who excrete S. Typhi for ≥3
mo after infection are regarded as chronic carriers.
Children with schistosomiasis can develop a chronic urinary carrier state.

CHALLENGES FACED
CHALLENGES ON THE WARD Diagnostic challenges (blood culture
bottles; delay in getting results) ??Treatment and resistance Policy for screening for carriers after
treatment not effective

CHALLENGES IN THE COMMUNITY Patients go back to the same
environment; continue getting exposed to the same contaminated water and food
Water and sanitation crisis in Lusaka’s residential areas
Practices do not change much Do we have carriers in the
community???

CARRIERS
The human-to-human spread by chronic carriers is important, and attempts should therefore be made to target food handlers and high-risk groups for S. Typhi carriage screening.
Once identified, chronic carriers must be counseled as to the risk for disease transmission and given advice on handwashing and preventive strategies.



ANYTHING NEW? Traditionally, 2 vaccines. An oral, live-attenuated
preparation of the Ty21a strain of S. Typhi has been shown to have good efficacy (67–82%) for up to 5 years.
The Vi capsular polysaccharide can be used in people ≥2 yr of age. It is given as a single intramuscular dose, with a booster every 2 yr and has a protective efficacy of 70–80%.
The vaccines are currently recommended for traveling into endemic areas.

ANYTHING NEW…. Vi-polysaccharide conjugate typhoid vaccine (TCV): It
is a Vi-capsular polysaccharide conjugate typhoid vaccine conjugated with tetanus toxoid
The vaccine has been licensed by the Drug Controller General of India (DCGI) in August, 2013 for clinical use in India
This vaccine has been approved for use in children below 1 years of age. Seroconversion rates of 98.05% have been reported with this vaccine.
The Indian Academy of Pediatrics recommends that the TCV can be given below one year of age, preferably between 9-12 months
