ibd and colorectal cancer surveillance - weo · cause of death in 10-15% of ibd crohns colitis...
TRANSCRIPT

IBD and colorectal cancer surveillance
Combined Colorectal Symposium Sunday 24 Sep 2017 Combined Colorectal Symposium S-12 13:30-15:00 Room S426+S427 (4/F)
IBDSydney
Prof Rupert Leong
why screen? when, on whom, how often? how to screen? how to manage dysplasia?
Prof Rupert Leong
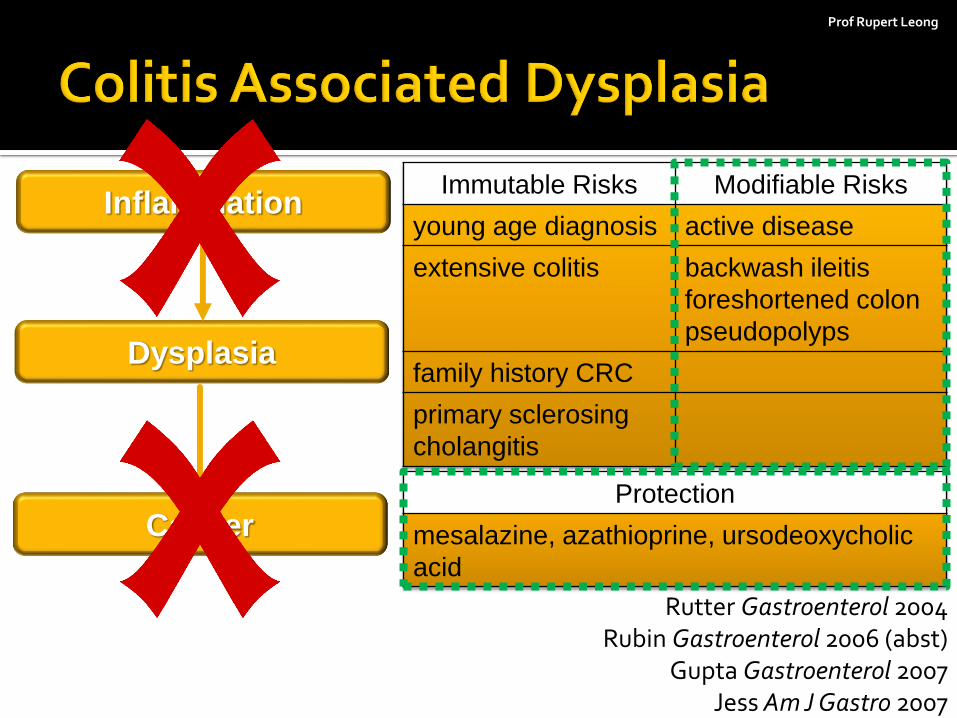
Protection
mesalazine, azathioprine, ursodeoxycholic
acid
Inflammation
Dysplasia
Cancer
Immutable Risks Modifiable Risks
young age diagnosis active disease
extensive colitis backwash ileitis
foreshortened colon
pseudopolyps
family history CRC
primary sclerosing
cholangitis
Rutter Gastroenterol 2004 Rubin Gastroenterol 2006 (abst)
Gupta Gastroenterol 2007 Jess Am J Gastro 2007
Prof Rupert Leong
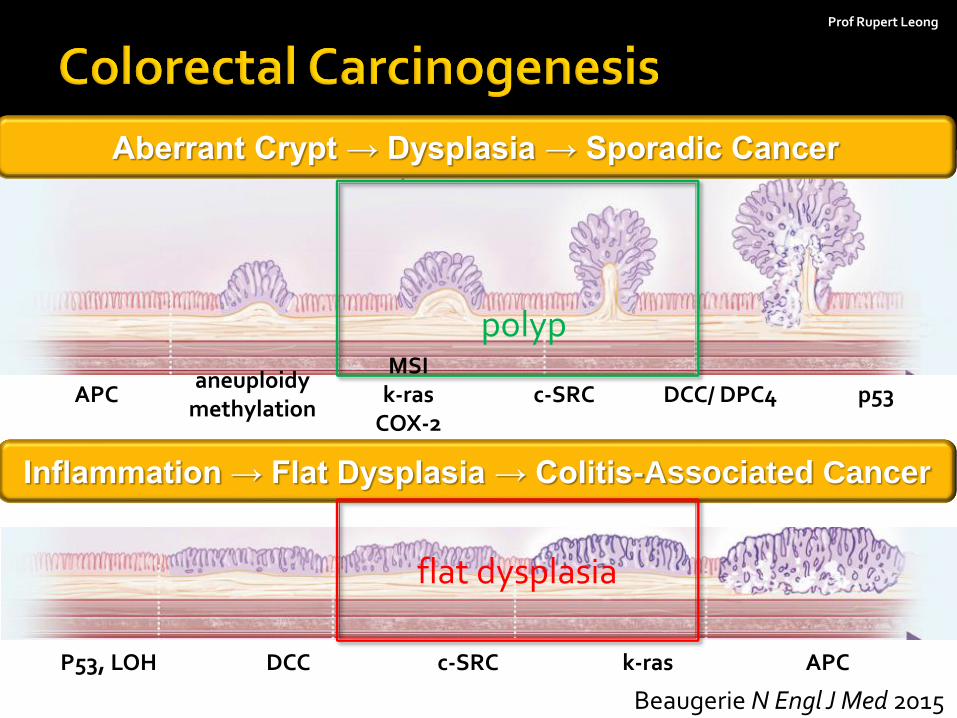
Beaugerie N Engl J Med 2015
Aberrant Crypt → Dysplasia → Sporadic Cancer
Inflammation → Flat Dysplasia → Colitis-Associated Cancer
polyp
flat dysplasia
APC aneuploidy
methylation
MSI k-ras
COX-2 c-SRC DCC/ DPC4 p53
P53, LOH DCC c-SRC k-ras APC
Prof Rupert Leong
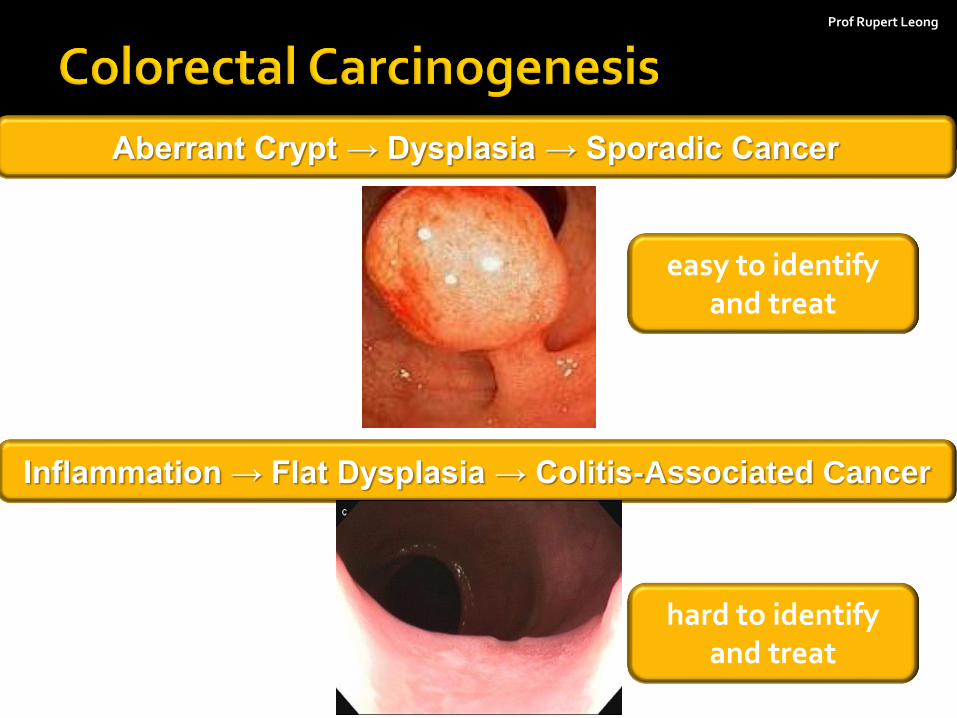
Aberrant Crypt → Dysplasia → Sporadic Cancer
Inflammation → Flat Dysplasia → Colitis-Associated Cancer
easy to identify and treat
hard to identify and treat
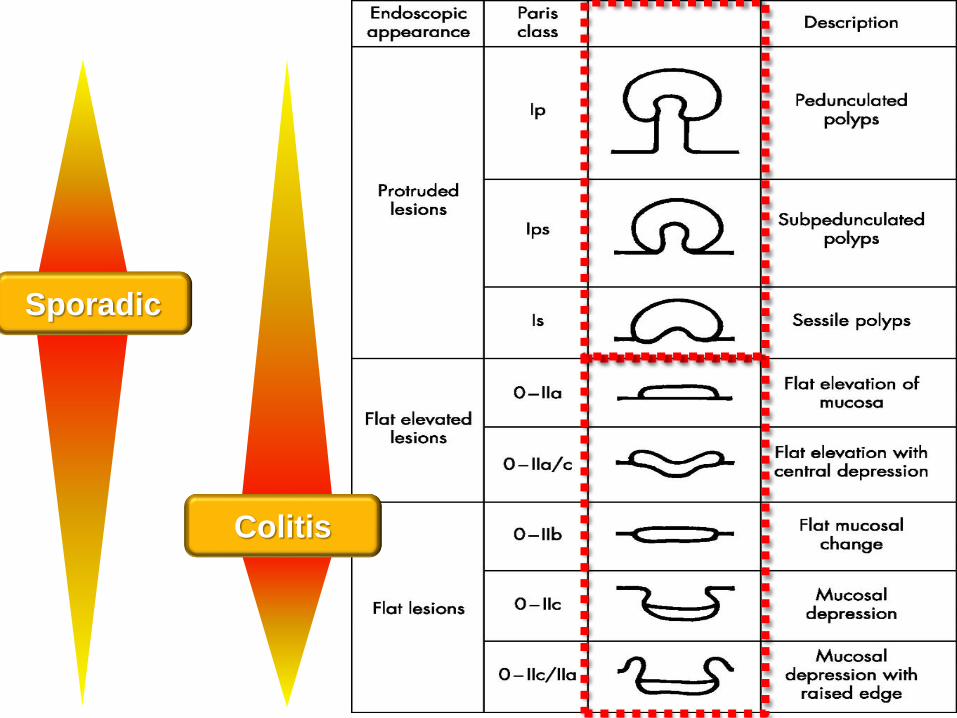
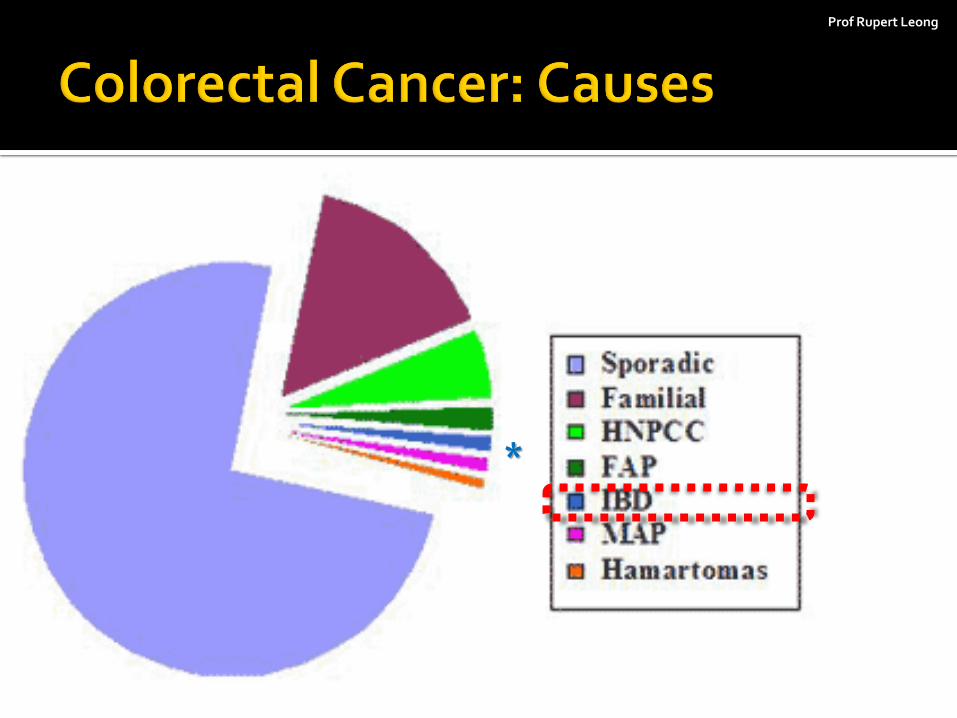
Sporadic
Colitis
Prof Rupert Leong
*
Prof Rupert Leong
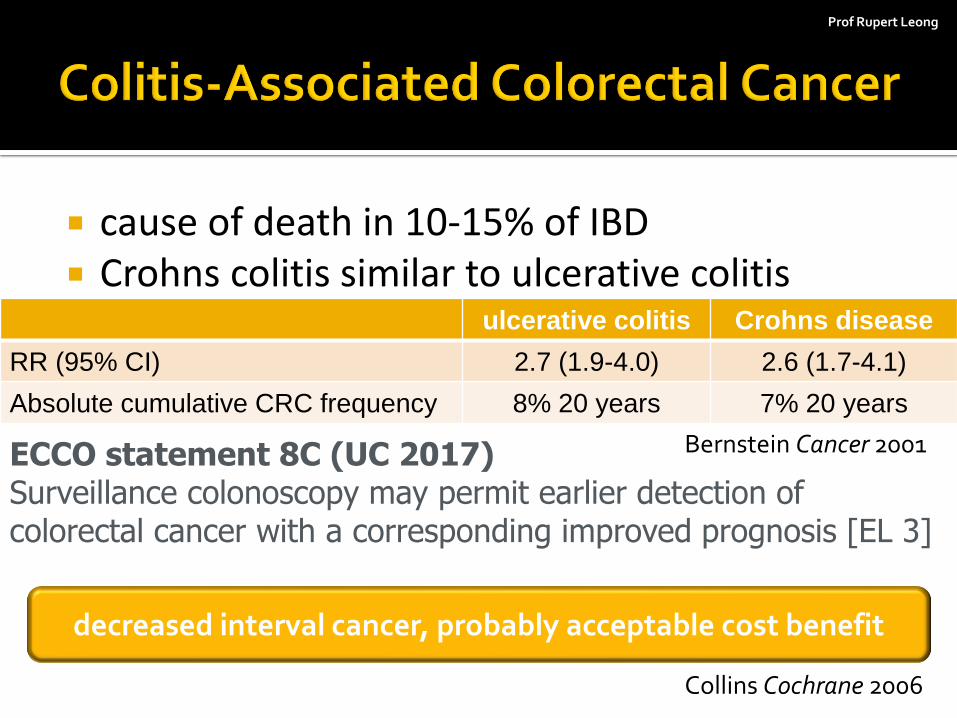
cause of death in 10-15% of IBD Crohns colitis similar to ulcerative colitis
ECCO statement 8C (UC 2017) Surveillance colonoscopy may permit earlier detection of colorectal cancer with a corresponding improved prognosis [EL 3]
ulcerative colitis Crohns disease
RR (95% CI) 2.7 (1.9-4.0) 2.6 (1.7-4.1)
Absolute cumulative CRC frequency 8% 20 years 7% 20 years
Bernstein Cancer 2001
decreased interval cancer, probably acceptable cost benefit
Collins Cochrane 2006
Prof Rupert Leong
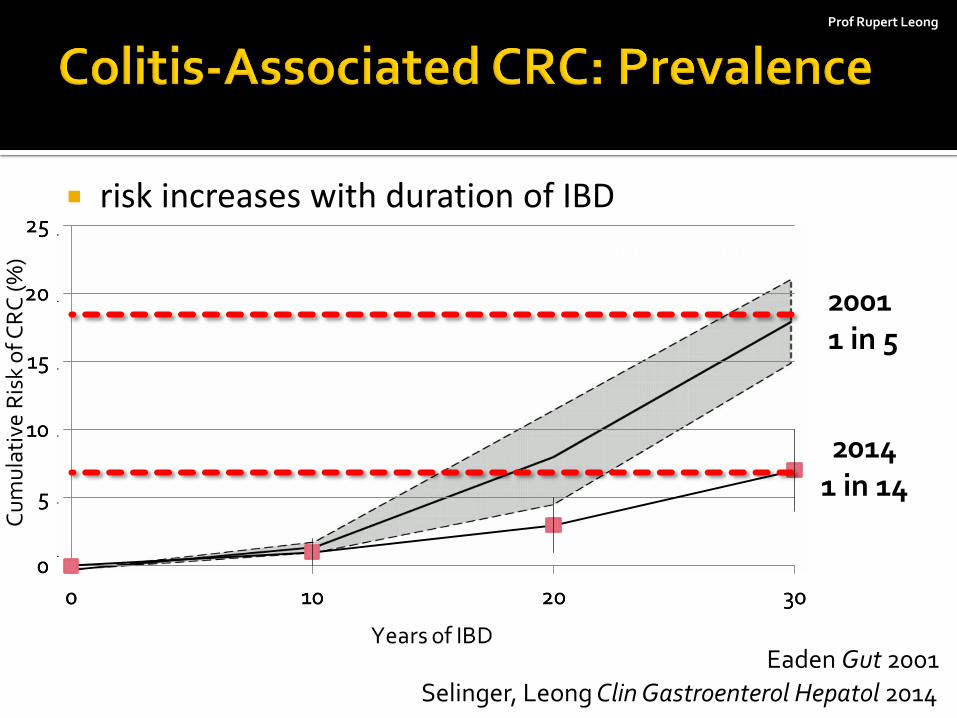
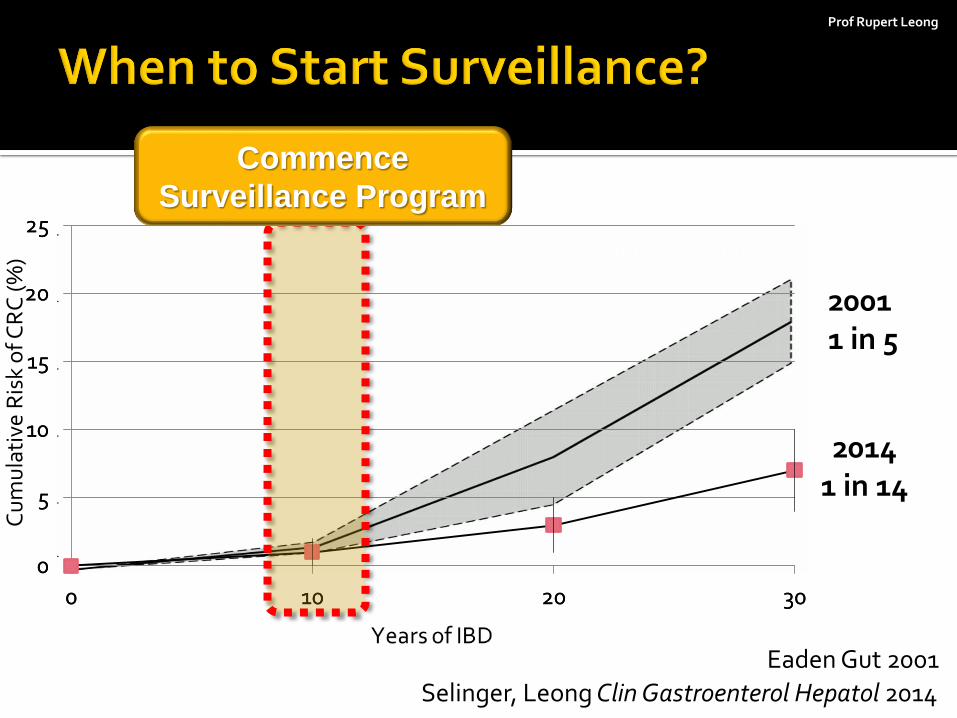
risk increases with duration of IBD
0
5
10
15
20
25
0 10 20 30
Selinger, Leong Clin Gastroenterol Hepatol 2014
Eaden Gut 2001
2001 1 in 5
2014 1 in 14
0
5
10
15
20
25
0 10 20 30
High Low
Cu
mu
lati
ve R
isk
of C
RC
(%
)

Asia Pacific Cohort Prevalence Duration UC
Vellore, India Venkataraman J Gastro Hep 2005
532 UC 0.9% CRC 4.4% <20yr 5.8% >20yr
extent
Mumbai, India
Desai World J Gastro 2015 430 UC 2.8% CRC extent duration
active colitis
New Dehli, India
Bopanna UEGJ 2017 1,012 2.0% CRC 1.5% 10yr 7.2% 20yr
23.6% 30yr
KASID, Korea
Kim B J Gastro Hep 2009 7,061 UC 0.37% CRC 0.7% 10yr 7.9% 20yr
33.2% 30yr
Guangzhou, China
Gong Dig Dis Sci 2012 3,922 UC 0.87% CRC 1.2% 10yr 3.6% 20yr
14.4% 30yr
Taipei, Taiwan
Wei J Chin Med Assoc 2013 406 UC 1.5% CRC
Sydney, Australia
Selinger Clin Gastro Hep 2014 504 UC 4.8% CRC 1% 10yr 3% 20yr 7% 30 yr
Prof Rupert Leong
0
5
10
15
20
25
0 10 20 30
Selinger, Leong Clin Gastroenterol Hepatol 2014
Eaden Gut 2001
2001 1 in 5
2014 1 in 14
0
5
10
15
20
25
0 10 20 30
High Low
Cu
mu
lati
ve R
isk
of C
RC
(%
)
Commence
Surveillance Program
Prof Rupert Leong
at least distal colitis 8 years following symptom onset
primary sclerosing cholangitis: annual
This Photo by Unknown Author is licensed under CC BY-SA
ECCO e-guide 2017
Prof Rupert Leong
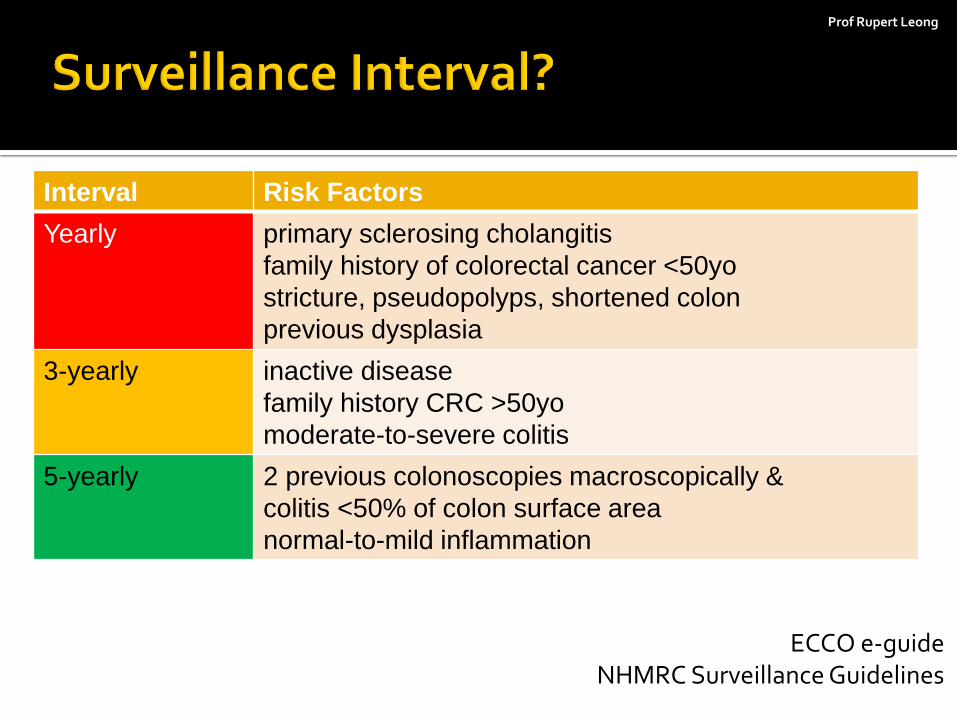
Interval Risk Factors
Yearly primary sclerosing cholangitis
family history of colorectal cancer <50yo
stricture, pseudopolyps, shortened colon
previous dysplasia
3-yearly inactive disease
family history CRC >50yo
moderate-to-severe colitis
5-yearly 2 previous colonoscopies macroscopically &
colitis <50% of colon surface area
normal-to-mild inflammation
ECCO e-guide NHMRC Surveillance Guidelines

Prof Rupert Leong
detect & enhance flat lesions
Class Dye
contrast: topography • indigocarmine 0.1 – 0.5%
absorptive: vital • methylene blue 0.1% (intestinal)
• crystal violet 0.1% (intestinal, gastric)
• Lugol’s 3% (glycogen)
reactive: chemical • acetic acid 3% (keratin)
• Congo red (pH)
Prof Rupert Leong
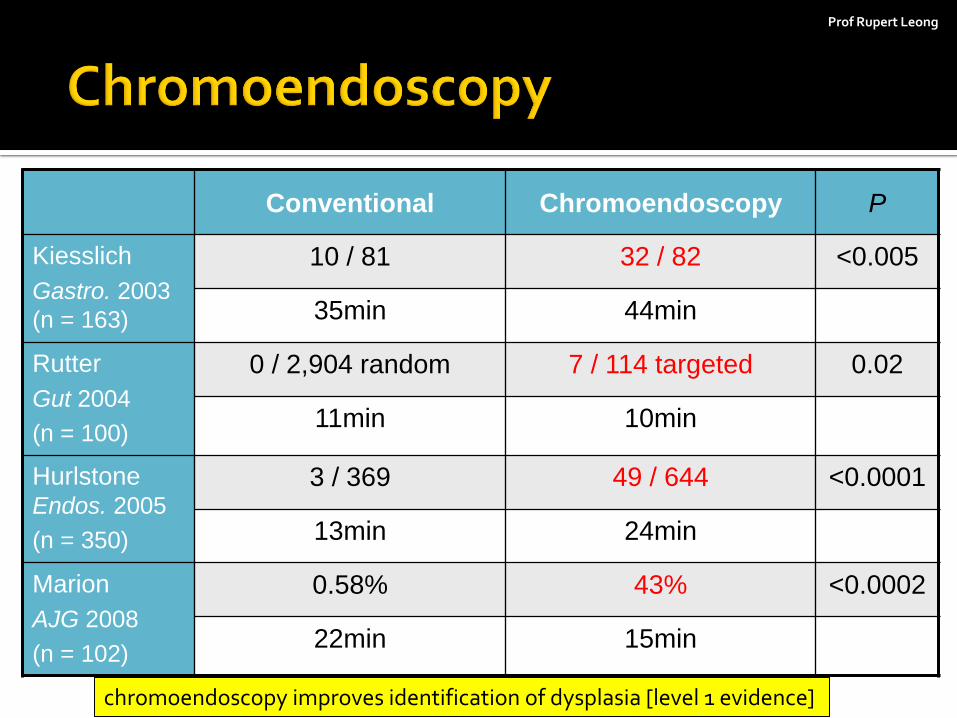
Conventional Chromoendoscopy P
Kiesslich
Gastro. 2003
(n = 163)
10 / 81 32 / 82 <0.005
35min 44min
Rutter
Gut 2004
(n = 100)
0 / 2,904 random 7 / 114 targeted 0.02
11min 10min
Hurlstone Endos. 2005
(n = 350)
3 / 369 49 / 644 <0.0001
13min 24min
Marion
AJG 2008
(n = 102)
0.58% 43% <0.0002
22min 15min
chromoendoscopy improves identification of dysplasia [level 1 evidence]
Prof Rupert Leong
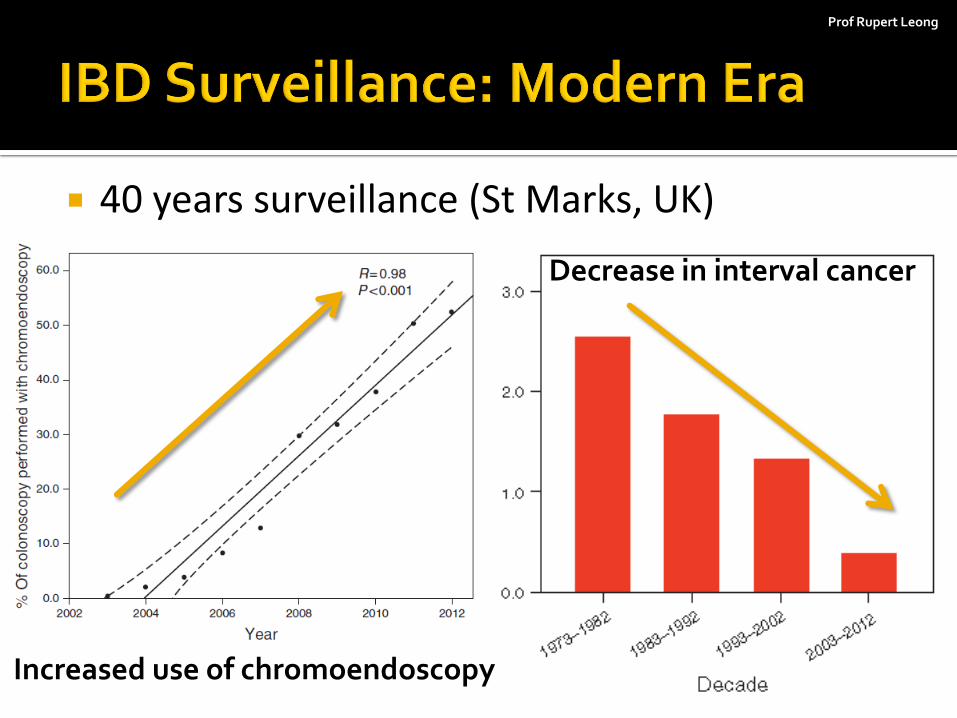
40 years surveillance (St Marks, UK)
Increased use of chromoendoscopy
Decrease in interval cancer
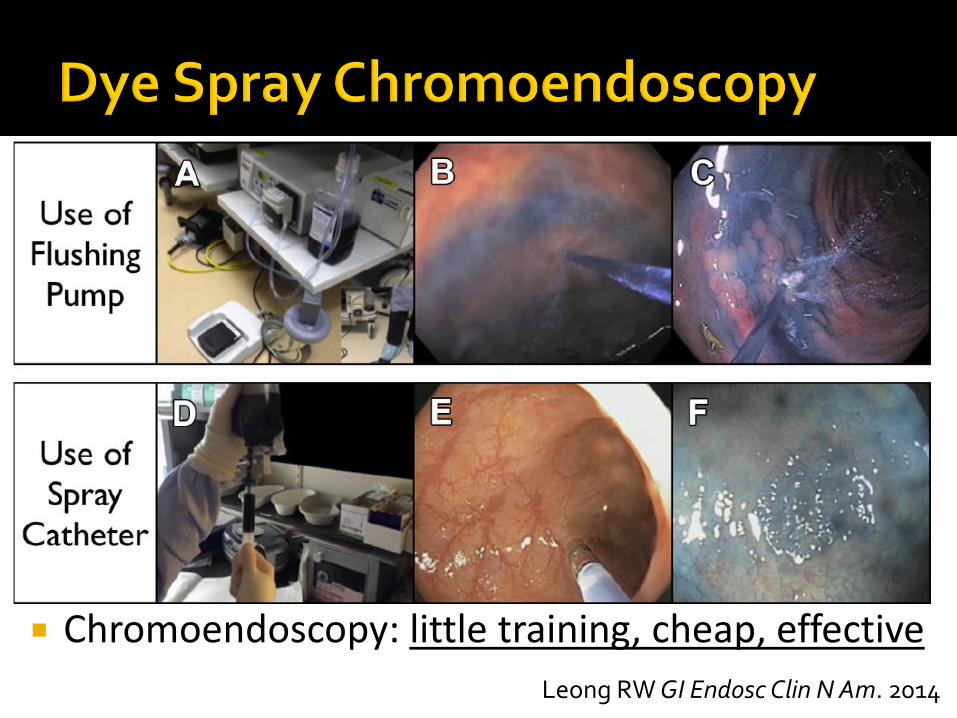
Chromoendoscopy: little training, cheap, effective
Leong RW GI Endosc Clin N Am. 2014
Prof Rupert Leong
chromoendoscopy is suggested rather than white-light colonoscopy – Dye based contrast improve epithelial surface detail – targeted biopsies less costly, more effective than
WLC with random biopsies – increase duration of colonoscopy by 11 minutes
Laine Gastroenterol 2015
Prof Rupert Leong
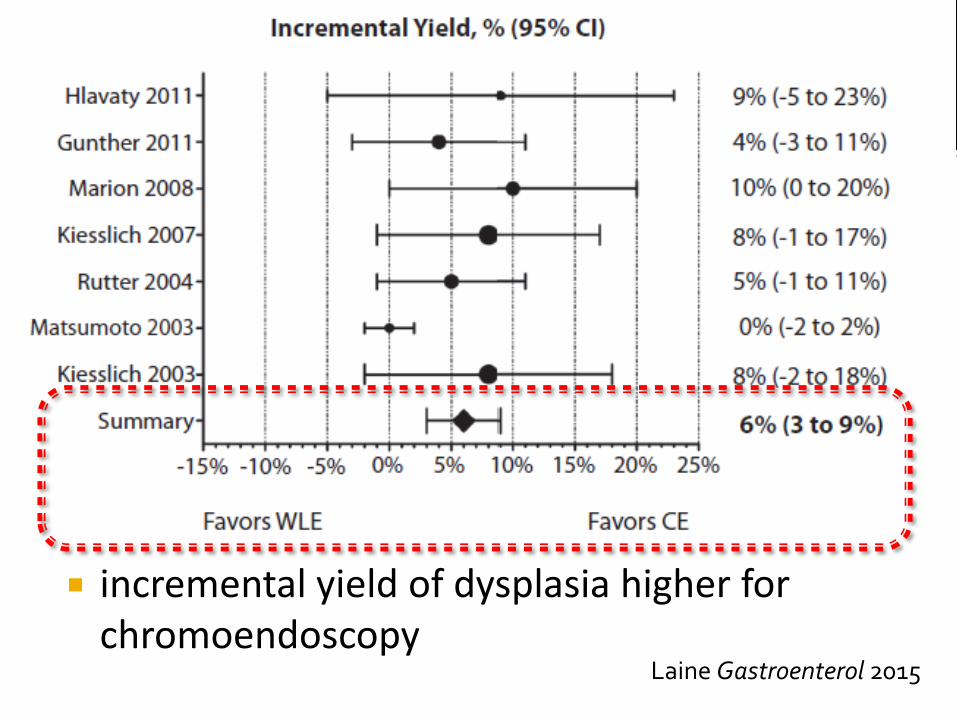
incremental yield of dysplasia higher for chromoendoscopy
Laine Gastroenterol 2015
Prof Rupert Leong
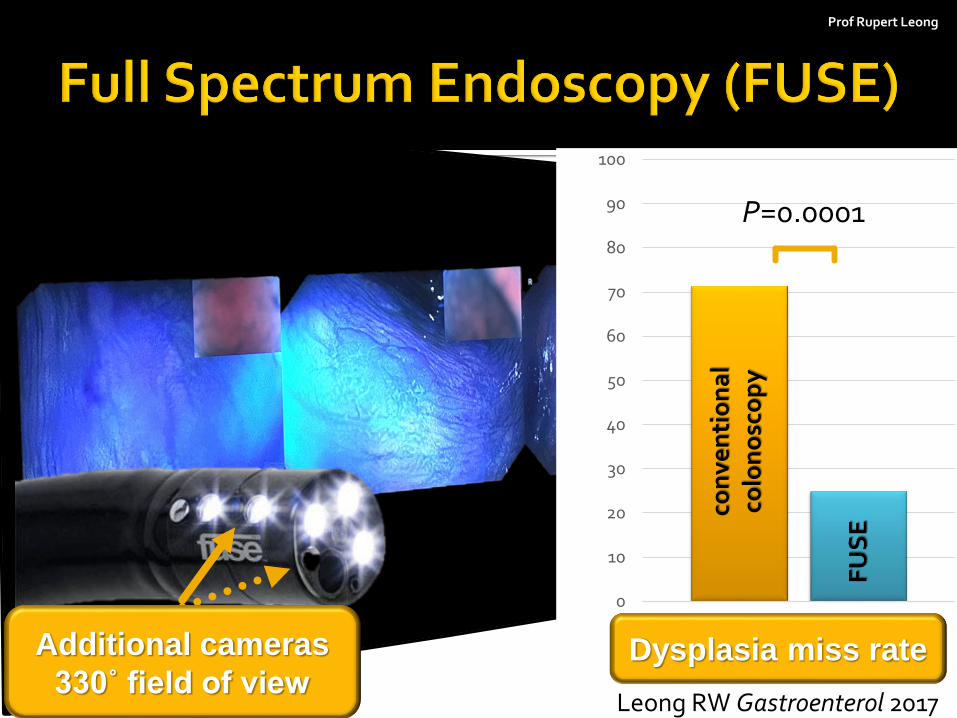
Additional cameras
330˚ field of view Leong RW Gastroenterol 2017
0
10
20
30
40
50
60
70
80
90
100
Dysplasia Miss Rate
con
ven
tio
na
l co
lon
osc
op
y
FU
SE
P=0.0001
Dysplasia miss rate
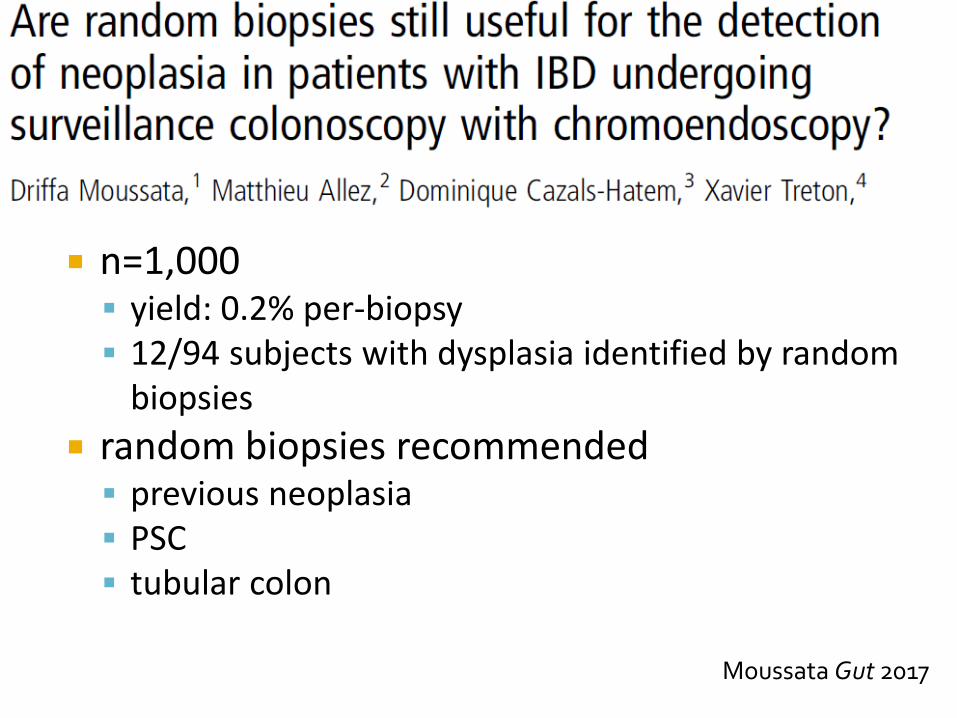
n=1,000 yield: 0.2% per-biopsy 12/94 subjects with dysplasia identified by random
biopsies
random biopsies recommended previous neoplasia PSC tubular colon
Moussata Gut 2017
Prof Rupert Leong
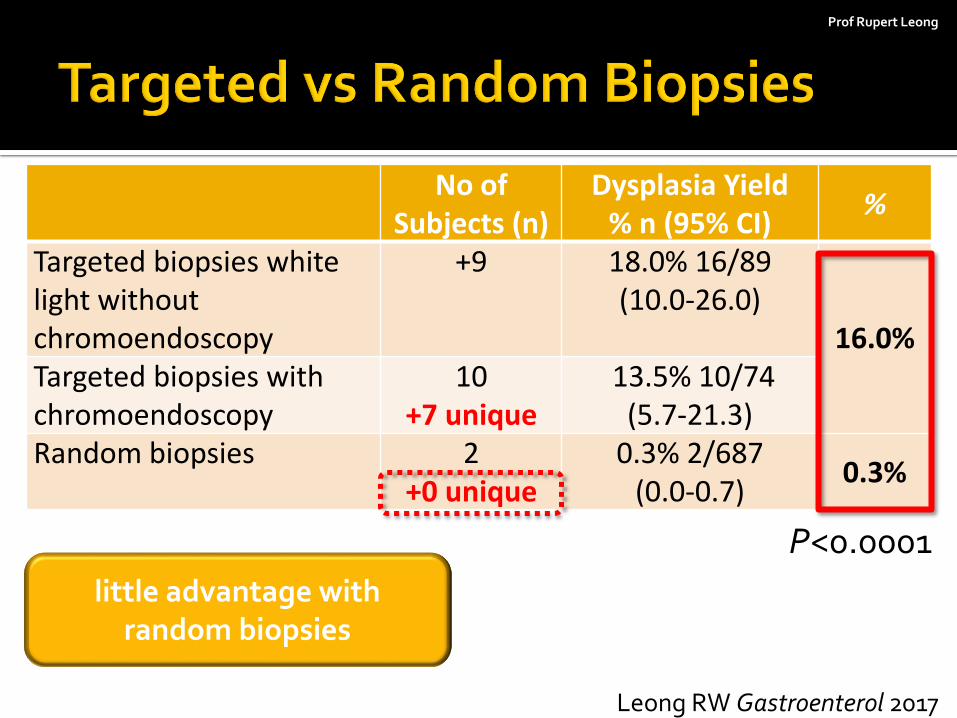
No of Subjects (n)
Dysplasia Yield % n (95% CI)
%
Targeted biopsies white light without chromoendoscopy
+9
18.0% 16/89 (10.0-26.0)
16.0% Targeted biopsies with chromoendoscopy
10 +7 unique
13.5% 10/74 (5.7-21.3)
Random biopsies 2 +0 unique
0.3% 2/687 (0.0-0.7)
0.3%
P<0.0001
Leong RW Gastroenterol 2017
little advantage with random biopsies
Prof Rupert Leong
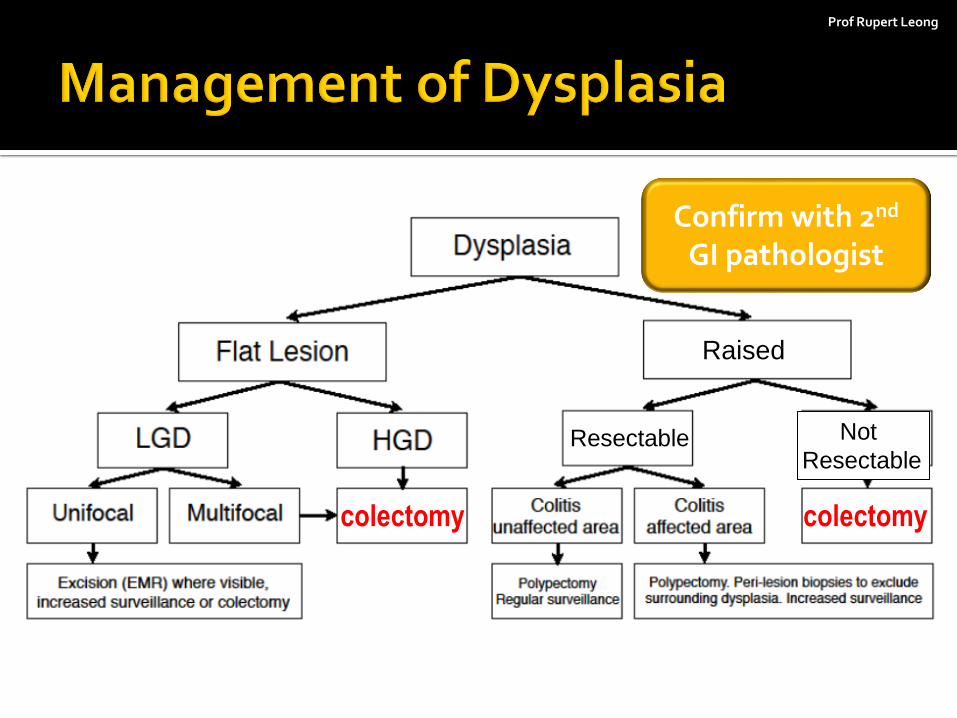
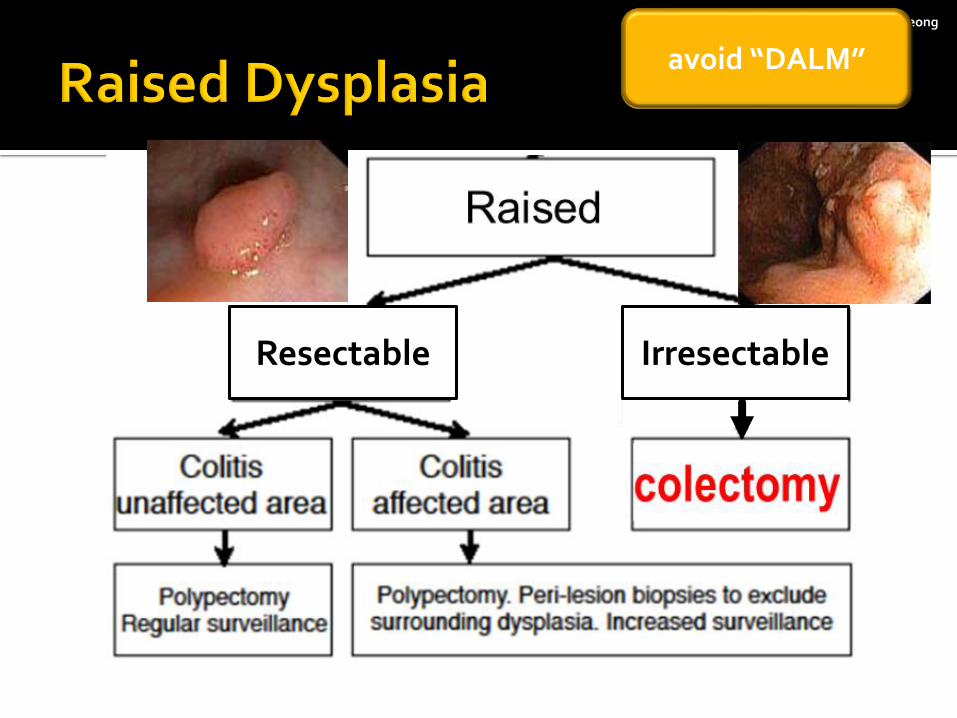
Raised
Resectable Not
Resectable
colectomy colectomy
Confirm with 2nd GI pathologist
Prof Rupert Leong
Resectable Irresectable
avoid “DALM”
Prof Rupert Leong
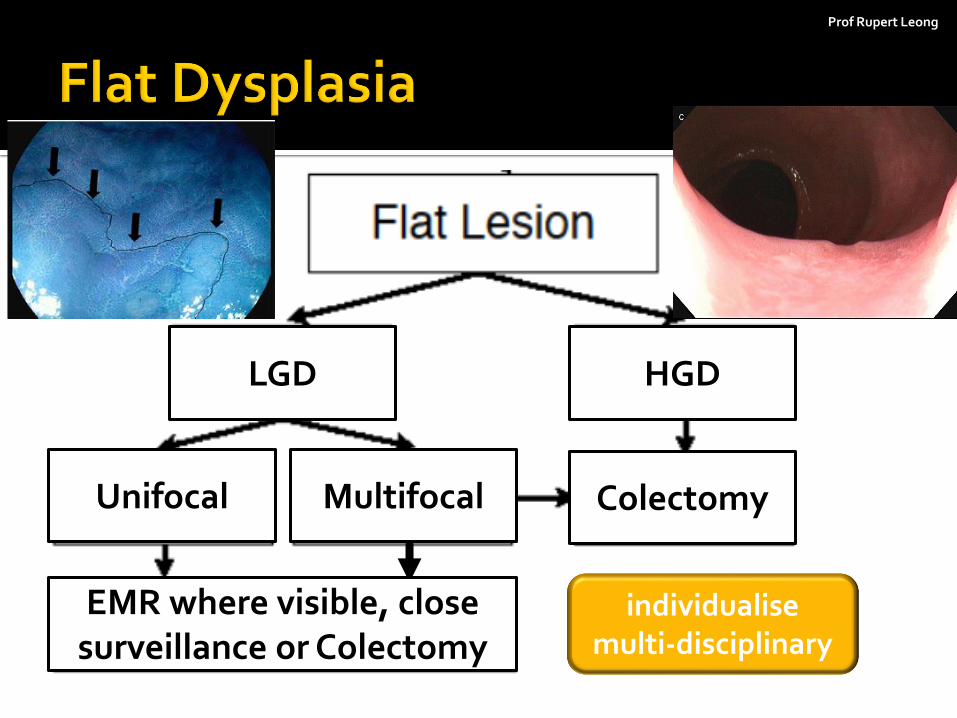
Colectomy Multifocal Unifocal
EMR where visible, close surveillance or Colectomy
LGD HGD
individualise multi-disciplinary
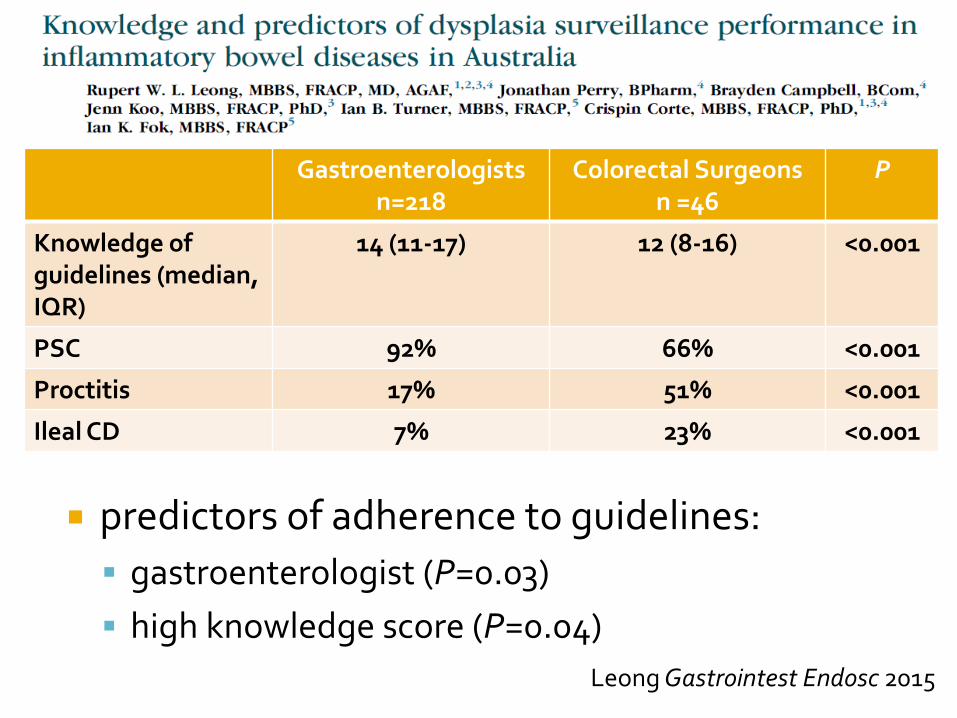
Gastroenterologists n=218
Colorectal Surgeons n =46
P
Knowledge of guidelines (median, IQR)
14 (11-17) 12 (8-16) <0.001
PSC 92% 66% <0.001
Proctitis 17% 51% <0.001
Ileal CD 7% 23% <0.001
predictors of adherence to guidelines:
gastroenterologist (P=0.03)
high knowledge score (P=0.04)
Leong Gastrointest Endosc 2015
Prof Rupert Leong
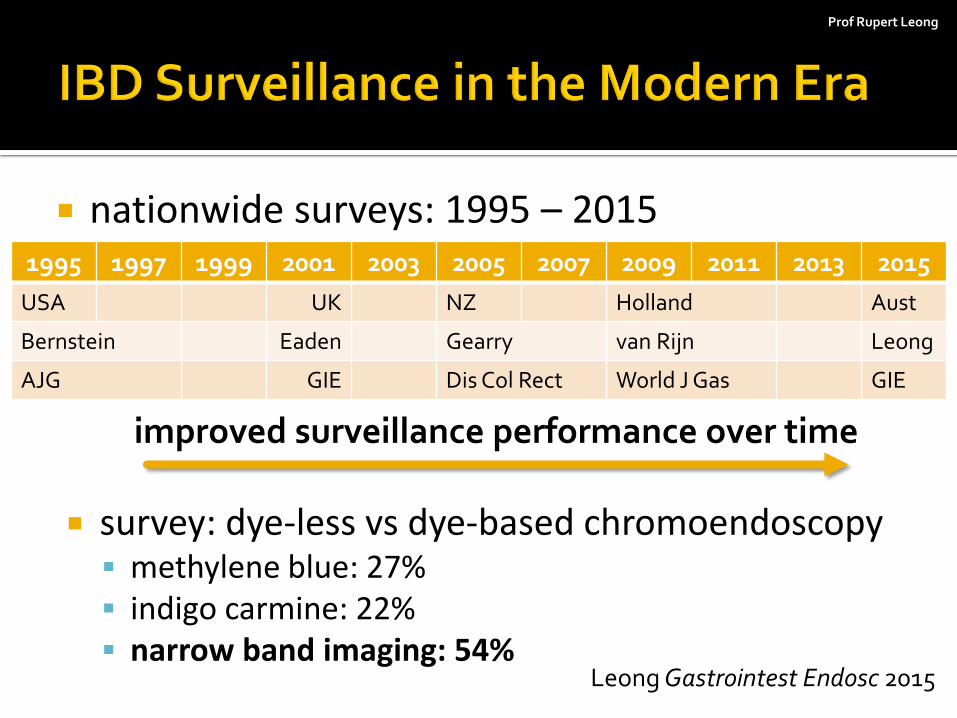
survey: dye-less vs dye-based chromoendoscopy methylene blue: 27% indigo carmine: 22% narrow band imaging: 54%
Leong Gastrointest Endosc 2015
1995 1997 1999 2001 2003 2005 2007 2009 2011 2013 2015
USA UK NZ Holland Aust
Bernstein Eaden Gearry van Rijn Leong
AJG GIE Dis Col Rect World J Gas GIE
nationwide surveys: 1995 – 2015
improved surveillance performance over time

Prof Rupert Leong
NBI has similar sensitivity than chromoendoscopy
NBI: 8 minutes faster (P<0.001)
per lesion neoplasia detection P=0.79 OR 1.09 (0.6-2.0)
Chromo-endoscopy
n=66
NBI n=65
total neoplastic lesions
31 21
% lesions neoplastic
17.4% 16.3%
Bisschops Gut 2017
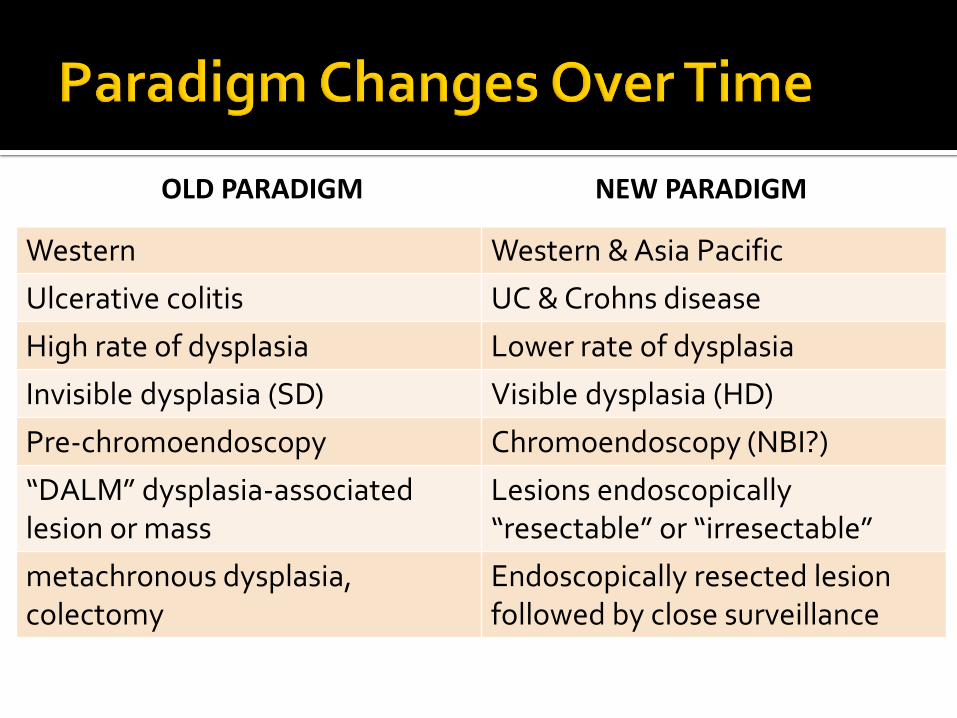
Old Paradigm New Paradigm
Western Western & Asia Pacific
OLD PARADIGM NEW PARADIGM
Old Paradigm New Paradigm
Western Western & Asia Pacific
Ulcerative colitis UC & Crohns disease
OLD PARADIGM NEW PARADIGM
Old Paradigm New Paradigm
Western Western & Asia Pacific
Ulcerative colitis UC & Crohns disease
High rate of dysplasia Lower rate of dysplasia
OLD PARADIGM NEW PARADIGM

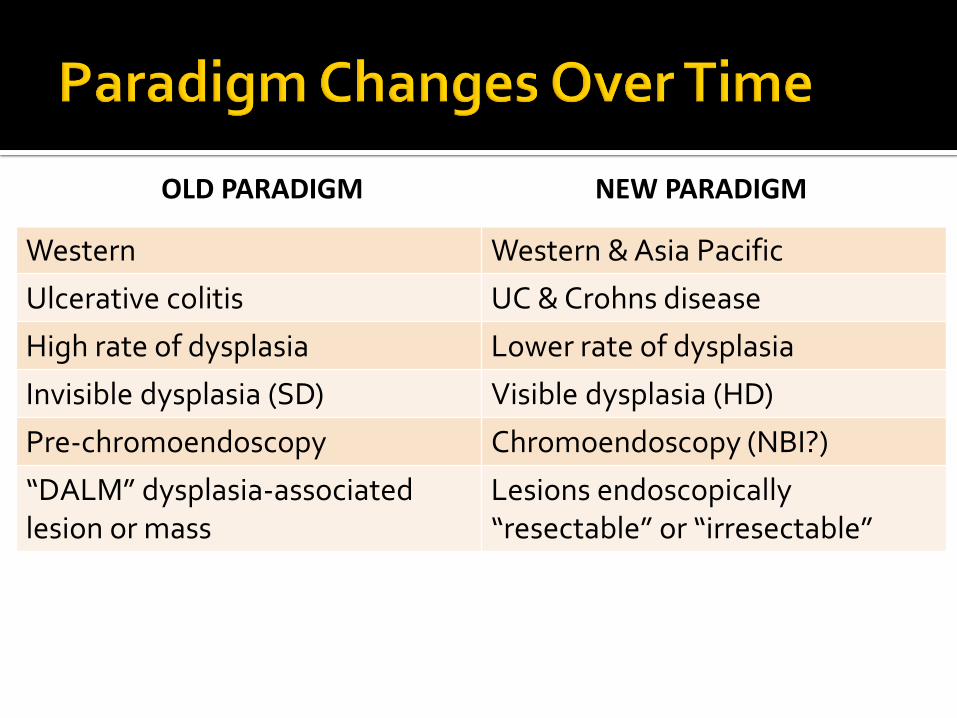
Old Paradigm New Paradigm
Western Western & Asia Pacific
Ulcerative colitis UC & Crohns disease
High rate of dysplasia Lower rate of dysplasia
Invisible dysplasia (SD) Visible dysplasia (HD)
Pre-chromoendoscopy Chromoendoscopy (NBI?)
OLD PARADIGM NEW PARADIGM
Old Paradigm New Paradigm
Western Western & Asia Pacific
Ulcerative colitis UC & Crohns disease
High rate of dysplasia Lower rate of dysplasia
Invisible dysplasia (SD) Visible dysplasia (HD)
Pre-chromoendoscopy Chromoendoscopy (NBI?)
“DALM” dysplasia-associated lesion or mass
Lesions endoscopically “resectable” or “irresectable”
OLD PARADIGM NEW PARADIGM
Old Paradigm New Paradigm
Western Western & Asia Pacific
Ulcerative colitis UC & Crohns disease
High rate of dysplasia Lower rate of dysplasia
Invisible dysplasia (SD) Visible dysplasia (HD)
Pre-chromoendoscopy Chromoendoscopy (NBI?)
“DALM” dysplasia-associated lesion or mass
Lesions endoscopically “resectable” or “irresectable”
metachronous dysplasia, colectomy
Endoscopically resected lesion followed by close surveillance
OLD PARADIGM NEW PARADIGM
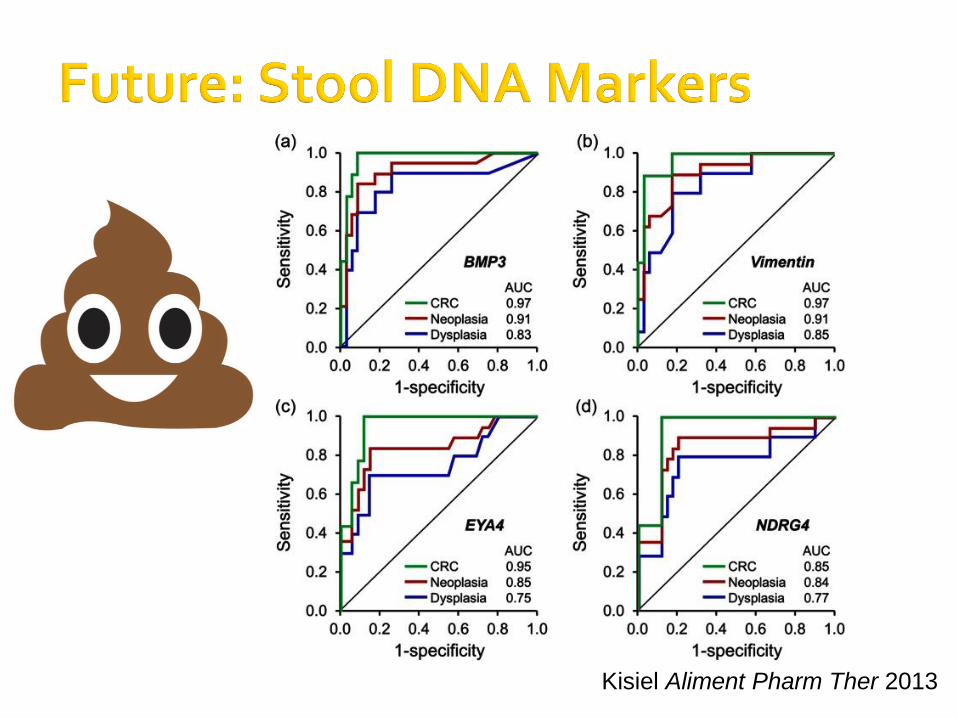
Kisiel Aliment Pharm Ther 2013
Prof Rupert Leong
control inflammation: mucosal healing high risk: PSC, foreshortened colon, prior
dysplasia quality surveillance, chromoendoscopy if high
risk increasing in Asia Pacific
IBDSydney
Prof Rupert Leong
Prof Rupert Leong
biomarkers: risk prediction systems eg faecal DNA testing
can image-enhanced surveillance increase surveillance intervals?
cost effectiveness change natural history in era of biological
agents?