“i will never forget”: what we learned from medical student reflections on a palliative care...
TRANSCRIPT

‘‘I Will Never Forget’’: What We Learned from MedicalStudent Reflections on a Palliative Care Experience
Barbara A. Head, Ph.D.,1 Lori A. Earnshaw, M.D.,1 Ruth B. Greenberg, Ph.D.,2
Robert C. Morehead, M.D.,1 Mark P. Pfeifer, M.D.,1 and Monica Ann Shaw, M.D.2
Abstract
Purpose: To use reflective writing to evaluate a new required palliative care experience for third year medicalstudents.Method: The authors used a constant comparison method based on grounded theory to conduct a thematicanalysis of reflective writings produced by third-year medical students completing a mandatory week-longclinical rotation in palliative care during academic year 2010 at the University of Louisville.Results: Two broad thematic categories were identified: what the students learned and what the students ex-perienced. Student writings revealed learning about palliative care (pain management, family meetings, goals ofcare, patient-family centered care, timing of palliative care, and delivering bad news); being a doctor (knowledge,communication, presence, empathy, not giving false hope, and person-focused care); the patient (importance offamily, the experience of dying, and the uniqueness of each patient); and themselves (need to be non-judgmental,ability to do palliative care, self-limitations, becoming a better physician, and dealing with death). Student re-flections centered on encounters with patients and families, internal emotional responses, and self-transformation.Conclusions: Systematic analysis of reflective writing provides educators with valuable data about students’learning experiences. These results may inform the design and modification of the curriculum.
Our patients aren’t just objects that we are supposed to fix, but
instead they are people with values and ideals that we must respect.
This is a lesson that I learned while on that rotation that I will neverforget .I will never forget her facial expression or her verbalization of pain
and how scared she was. I will also never forget how much I wanted to
do something for her to alleviate her suffering.
– reflections of third-year medical students
Introduction
Clinical experiences with seriously ill and dyingpatients are vital to physician education in palliative
medicine. Too often, preparation to care for such patientsconsists entirely of preclinical didactic lectures. Studentsthemselves believe that care of the dying requires learningfrom direct clinical experience,1 but meaningful contact withseriously ill and dying patients is often absent from themedical school experience.2
Experiential learning involves interpreting and integratingexperience into existing knowledge structures to produce newknowledge.3 D.A. Kolb refers to this as the experiential
learning cycle.4 According to Kolb, the learner emotionallytransforms the experience into something meaningfulthrough either (a) gaining new information by thinking, an-alyzing, or planning (abstract conceptualization or thinking)or (b) experiencing the concrete, tangible, felt qualities of theworld (concrete experience or feeling).
Reflecting on experience is essential for self-discovery, self-regulation, and the therapeutic use of self in clinical situationsand is important for professional development.5 The aim ofreflection is to inform future actions so they can be morepurposeful and deliberate.3 Reflection cultivates the self-awareness crucial to those providing compassionate care forseriously ill and dying patients.1 Reflective writing, one toolfor reflection, is an established method for teaching empa-thetic patient interactions6 and has been linked to effective useof feedback and improved diagnostic accuracy.7
Reflective activities have also been shown to provide a richsource of information about the ‘‘informal and hidden cur-riculum,’’ those things that are learned during the everydayexperiences of students outside of the formal curriculum.8,9
Experiences in the clinical setting may well determine per-ceptions of acceptable behaviors and values as students enterthe medical profession.10,11 Evaluations of student reflections
1Department of Medicine, Division of General Internal Medicine, Palliative Medicine, and Education, 2Department of Medical Education,University of Louisville School of Medicine, Louisville, Kentucky.
Accepted December 12, 2011.
JOURNAL OF PALLIATIVE MEDICINEVolume 15, Number 5, 2012ª Mary Ann Liebert, Inc.DOI: 10.1089/jpm.2011.0391
535

can be an important tool for end-of-life curriculum planning,evaluation, and reform.1,9,12
In 2007, the University of Louisville School of Medicineredesigned the curriculum to integrate palliative care into all 4years of medical school. With the assistance of mentors fromthe Medical College of Wisconsin, the project team evaluatedthe components of the existing curriculum, reworked thepreclinical curriculum, developed novel educational materi-als, and developed a one-week required palliative care clinicalrotation during the third-year Medicine clerkship. During thisrotation, students were assigned to a palliative care programin a hospital setting where they rounded with the physician,provided medical care for palliative patients, completedlearning modules on topics such as pain, symptom manage-ment, and communication, and responded to a structuredclinical vignette designed to teach palliative care principles.
The new curriculum included a writing assignment inwhich students reflected on a patient interaction or experiencerelated to palliative care. The assignment had two purposes:(1) to provide an opportunity for student reflection and (2) toprovide evidence of the impact of the revised curriculum. Theaim of this study was to use students’ reflective writings toexplore the value of this new mandatory palliative care ex-perience for third-year medical students. Approval to conductthe research was granted by the University of Louisville’sHuman Subject Protection Program. The study was deter-mined to be exempt as it was research conducted in an es-tablished educational setting for the purpose of evaluatinginstructional effectiveness and the identity of the students wasnot revealed to the research team.
Method
Data source
The assignment. For the reflective writing assignment,students were instructed to: (1) summarize a specific doctor-patient experience/encounter involving palliative care (atelling of the story without interpretation); (2) explore/inter-pret the possible meanings of the event; and (3) describe/predict how the knowledge gained from the encounter couldbe used professionally in the future. This assignment structurereflected the four phases of the experiential learning cycle asconceptualized by D.A. Kolb: (1) the learner has an experi-ence; (2) the learner reflects on the experience; (3) the learnermakes an attempt to understand his or her actions or reactionsto the experience; and (4) the learner applies the new knowl-edge.4 Papers were to be approximately one page in lengthand were submitted online.
All third-year medical students (academic year 2009–2010,n = 155) completed the palliative care rotation during theirmedicine clerkship and submitted the required assignment atany chosen point before the end of the clerkship.
Sample selection. Student names were removed fromthe essays and the essays were copied to a computer disk. Amember of the research team (BH) who had no previouscontact with the students or their essays selected 40 essaysrandomly from the group of 155. It was believed that 40 essayswould be manageable for in-depth analysis. The researchteam agreed that if data saturation was not evident after an-alyzing these essays, more would be selected and analyzed.The essays were assigned numbers, copied, and distributed tothe six members of the research team.
Ensuring trustworthiness
The six members of the research team represented diversebackgrounds and included four Department of Medicinefaculty members (three M.D.s and one Ph.D./social worker),the Associate Dean for Medical Education, and a Medicineresident. Each team member read the essays several times.Dialogue and peer debriefing ensured reliability of the overallfindings. Random selection of the essays contributed to thedata being representative of the whole. The process of con-ceptualizing categories, agreeing on domains and themes,and developing an overall scheme was documented at eachmeeting using flip charts, thereby providing a clear audit trail.
Analysis
Analysis proceeded using a constant comparison approachbased on grounded theory.13 Steps in the analysis follow:
(1) A ‘‘naı̈ve’’ first reading of all essays. Researchers readall essays while ‘‘bracketing’’ or putting aside anypreexisting ideas or thoughts about what should ormight be revealed. Researchers noted themes thatthey observed separate from the data.
(2) A second reading of essays and identification ofquotes related to themes by coding in the margins.Both the first and second readings were done by eachmember of the team in isolation.
(3) Development of an exhaustive list of themes. Theteam reached consensus regarding the dominantthemes. The team concluded that data saturation hadbeen achieved (no new themes emerged; repetition ofthose identified was evident).
(4) Identification of two core domains encompassing thethemes: what the students experienced and what thestudents learned.
(5) Division of the team into two smaller groups, eachassigned to one of the two domains.
(6) Small-group ‘‘deconstruction’’ of the data by selectingquotes representative of the themes within each domain.
(7) Small-group presentation of findings to the researchteam.
(8) Development of consensus about the themes andquotes to include as representative of each domain.
Results
Initial coding of the data into themes delineated two broaddomains: what the students learned and what the studentsexperienced. These two domains reflect Kolb’s two methods oftransforming experience into meaning: (1) thinking, analyzingor planning (our domain of what the student learned) and (2)experiencing the felt qualities of the world (our domain of whatthe students experienced). Within each domain, further themesemerged during the constant comparison process.
What students learned
This domain encompassed the development of knowledgeor skill and the modification of a behavioral tendency by ex-perience. Student learning was further categorized into fourtopical areas or subdomains: learning about palliative care(Table 1); learning about being a doctor (Table 2); learningabout the patient (Table 3); and learning about oneself (Table
536 HEAD ET AL.
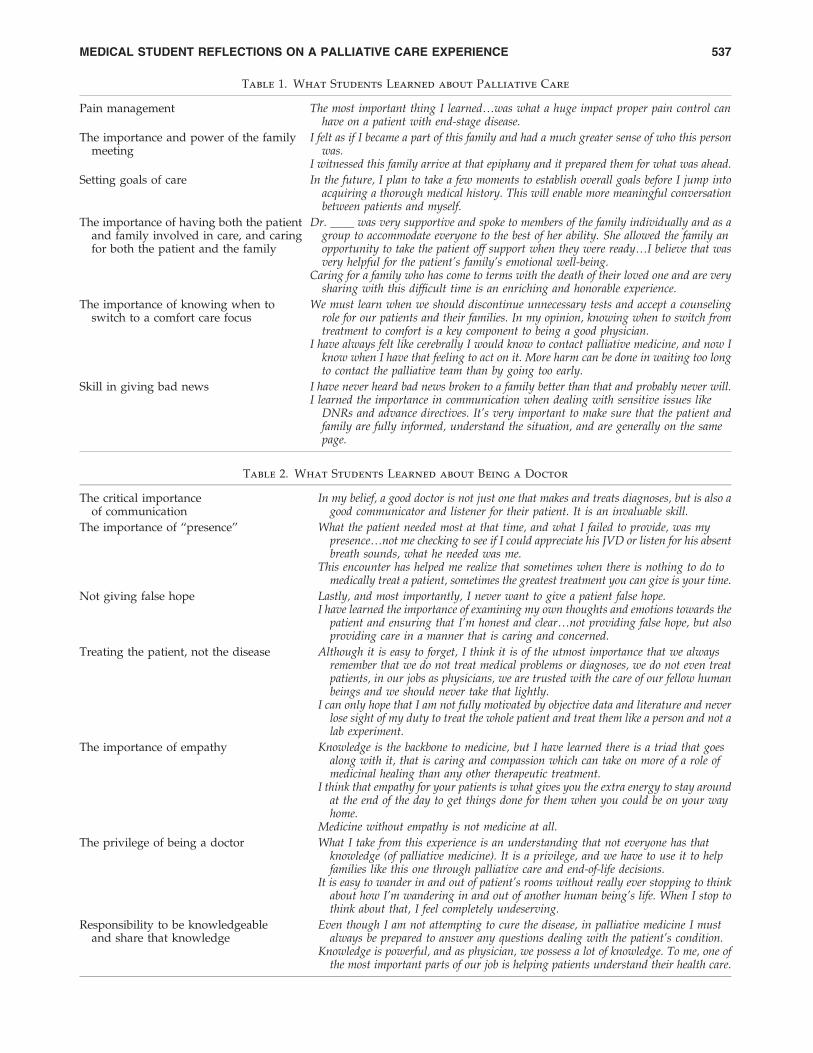
Table 1. What Students Learned about Palliative Care
Pain management The most important thing I learned.was what a huge impact proper pain control canhave on a patient with end-stage disease.
The importance and power of the familymeeting
I felt as if I became a part of this family and had a much greater sense of who this personwas.
I witnessed this family arrive at that epiphany and it prepared them for what was ahead.
Setting goals of care In the future, I plan to take a few moments to establish overall goals before I jump intoacquiring a thorough medical history. This will enable more meaningful conversationbetween patients and myself.
The importance of having both the patientand family involved in care, and caringfor both the patient and the family
Dr. ____ was very supportive and spoke to members of the family individually and as agroup to accommodate everyone to the best of her ability. She allowed the family anopportunity to take the patient off support when they were ready.I believe that wasvery helpful for the patient’s family’s emotional well-being.
Caring for a family who has come to terms with the death of their loved one and are verysharing with this difficult time is an enriching and honorable experience.
The importance of knowing when toswitch to a comfort care focus
We must learn when we should discontinue unnecessary tests and accept a counselingrole for our patients and their families. In my opinion, knowing when to switch fromtreatment to comfort is a key component to being a good physician.
I have always felt like cerebrally I would know to contact palliative medicine, and now Iknow when I have that feeling to act on it. More harm can be done in waiting too longto contact the palliative team than by going too early.
Skill in giving bad news I have never heard bad news broken to a family better than that and probably never will.I learned the importance in communication when dealing with sensitive issues like
DNRs and advance directives. It’s very important to make sure that the patient andfamily are fully informed, understand the situation, and are generally on the samepage.
Table 2. What Students Learned about Being a Doctor
The critical importanceof communication
In my belief, a good doctor is not just one that makes and treats diagnoses, but is also agood communicator and listener for their patient. It is an invaluable skill.
The importance of ‘‘presence’’ What the patient needed most at that time, and what I failed to provide, was mypresence.not me checking to see if I could appreciate his JVD or listen for his absentbreath sounds, what he needed was me.
This encounter has helped me realize that sometimes when there is nothing to do tomedically treat a patient, sometimes the greatest treatment you can give is your time.
Not giving false hope Lastly, and most importantly, I never want to give a patient false hope.I have learned the importance of examining my own thoughts and emotions towards the
patient and ensuring that I’m honest and clear.not providing false hope, but alsoproviding care in a manner that is caring and concerned.
Treating the patient, not the disease Although it is easy to forget, I think it is of the utmost importance that we alwaysremember that we do not treat medical problems or diagnoses, we do not even treatpatients, in our jobs as physicians, we are trusted with the care of our fellow humanbeings and we should never take that lightly.
I can only hope that I am not fully motivated by objective data and literature and neverlose sight of my duty to treat the whole patient and treat them like a person and not alab experiment.
The importance of empathy Knowledge is the backbone to medicine, but I have learned there is a triad that goesalong with it, that is caring and compassion which can take on more of a role ofmedicinal healing than any other therapeutic treatment.
I think that empathy for your patients is what gives you the extra energy to stay aroundat the end of the day to get things done for them when you could be on your wayhome.
Medicine without empathy is not medicine at all.
The privilege of being a doctor What I take from this experience is an understanding that not everyone has thatknowledge (of palliative medicine). It is a privilege, and we have to use it to helpfamilies like this one through palliative care and end-of-life decisions.
It is easy to wander in and out of patient’s rooms without really ever stopping to thinkabout how I’m wandering in and out of another human being’s life. When I stop tothink about that, I feel completely undeserving.
Responsibility to be knowledgeableand share that knowledge
Even though I am not attempting to cure the disease, in palliative medicine I mustalways be prepared to answer any questions dealing with the patient’s condition.
Knowledge is powerful, and as physician, we possess a lot of knowledge. To me, one ofthe most important parts of our job is helping patients understand their health care.
MEDICAL STUDENT REFLECTIONS ON A PALLIATIVE CARE EXPERIENCE 537

4). Key points for each area evolved as the data were furtheranalyzed. For most subdomains, there were five or more re-lated quotes by students. The Tables include only key quotesselected to be representative of the students’ thinking in eachtopical area. Students’ writing was not edited.
What students experienced
Analysis revealed that the required palliative care experi-ence was also an emotional experience for the students. Thisdomain addressing what they experienced included three
subdomains: intimate encounters with patients and families,internal emotional responses, and transformation and journeyin patient experiences. Representative quotes from the dataare displayed in Table 5.
Discussion
What we learned
What we learned about the students. Analysis re-vealed that the students’ experiences with dying patients andtheir exposure to palliative care left them with positive
Table 3. What Students Learned about the Patient
The importance of family I saw the impact of having people who love you around in times of need. This man physically didbetter when his wife was around. The nurses had less calls to his room. The man’s vitalsstabilized. He simply looked and was more comfortable with his wife there.
Families are just worried about their loved one. These are not simply patients, but rathersomeone’s trust blanket.
The experience of dying Even as their bodies fail them and they appear apathetic to the world around them, these patientsretain a great deal of their personality, and they are just as susceptible to fear and anxiety asanyone else.
The uniqueness of each patient This patient encounter made me realize that different patients have different needs.The experience made me realize that every one deals with the dying process differently. To
Mr. Smith, living a life in bed all the time wasn’t really a life worth living, so I think thatplayed a large part in his decision to be DNR.
Table 4. What Students Learned about Themselves
The need for a nonjudgmental approach Overall, I think I need to remind myself not to assume what a patient or his/herfamily will want, and I should try to approach every patient with a clean slate so Idon’t let prior experiences cloud my judgment.
‘‘I can do’’ palliative care I felt natural talking with a patient quietly and for a long time as they meanderedtheir way across their points with only gentle guidance and comments fromme.With this patient’s encouragement, I was able to practice this gentlemedicine that feels so natural to me.
Through all of this I learned that I can handle myself in tough situations, that I canbe proud of the way I handled things, even if others might disagree.
Taking the time to sit down with the patient, making sure the family was present,answering all of her questions, and really talking to her was a completely differentand refreshing experience. It made me remember why I had initially wanted topursue medicine.
Self-limitations We will never beat death, but we can cheat it. We fight death, yet it is a part ofeverything living, and sometimes it is the best way. We cheat when we can, butsometimes we shouldn’t.
I realize that I cannot fix a patient’s personality or alter the way they react to stressbut I can help with direct medical and/or palliative issues.
On being a better physician I will try to keep this person and experience with me with every person I see, and tryto remember the person in front of me has a mother or brother or daughter wholoves them, sees them for who they are, as a person, not the disease they presentedwith.
This experience made an impact on me and I think it will make me a betterphysician.it taught me to learn to listen to my patients and make sure they arecomfortable and feel that they are aware of what is going on and why.
Witnessing this type of end-of-life amends making process will no doubt benefit mein my future practice. I will be able to talk about such issues with dying patientsand can hopefully facilitate, at least in some small way, their preparations fordeath.
Dealing with death as part of doctoring No matter what we, as medical professionals, do, we will always lose, and a patientwill always die..a physician merely plays an infinitesimal intermediary betweenlife and eternity, trying when we can to stave the course of fate.
I know how fleeting life is, but that is one lesson no one is ever truly preparedfor..I’m not sure I will ever be completely equipped for that situation, but I havelearned it is a part of life, and part of being a doctor.
538 HEAD ET AL.

attitudes related to the practice of palliative care. Specifically,they learned that the physician-patient encounter can providehealing and help prepare patients and families for life-changing experiences.
Similar to other studies,8,14 we found that both positiveand negative observations shape student perceptions of theprofession and its values. These observations also contributeto development of their professional identities and shapetheir views about the physicians they want to become. Theirwritings conveyed realization of the privilege of being aphysician and the immense responsibility that accompaniesthis role.
The writings provide evidence that the clinical experiencein palliative care made them more prepared. They learnedfirst-hand about pain management, the power of the familymeeting, and giving bad news. They experienced empathy asthey identified with patient situations (‘‘he is a young manaround my age which wasn’t something I was preparedfor .’’, ‘‘I sat down on his bed like he was my brother.’’), and
reflected on mortality (‘‘I know how fleeting life is,’’ ‘‘we willnever beat death.’’).
Many students reflected upon medicine’s tendency toevaluate patients based upon objective measures (patient’soutward physical appearance, vital signs, physical exam,or lab results) and ‘‘lump’’ them into disease categories.After this clinical exposure, students realized they oftenlost sight of the uniqueness of the individual. The pallia-tive care experience served as a reminder of how physi-cians should actually relate to and treat ‘‘our fellow humanbeings.’’
Students also realized the importance of being ‘‘present’’for the patients. We were struck by how descriptive theirwritings were. They were truly in the moment with theirpatients, and evidence of the depth of their presence mani-fested itself in the richness of their descriptions. Many stu-dents indicated that being able to spend time with patients,learning their stories, and relating to them as fellow humanbeings were the reasons why they became physicians. They
Table 5. What Students Experienced
Intimate encounters with patients andfamilies
I realized that the way he turned his hand when I approached was his signal that hewanted to hold my hand while I talked and examined him.
At that moment I sat down on his bed like he was my brother. I really got to know him.I knew his whole story, right down to the fact that he liked to watch cartoons in themorning.
He asked me to hold his hand and to pray with him. I did. Maybe some physicians willtell me that I was wrong to, that it was inappropriate or too personal of a gesture. I’ddo it again..I’m not the most religious person, but I am aware of the significance ithas on someone who believes. How could I have turned him down?
I developed a genuine fondness for his family and many times I would feel a lump in mythroat after speaking with them.
Internal emotional responses I found it easy to dehumanize him. It sounds awful, but at first he seemed to me to be acadaver in waiting.
I was nervous. In my mind, this was going to be tough. I was afraid to see people soweak and hopeless. I was scared to see an actively dying patient.This was a verypowerful experience. Some lessons you learn aren’t great or profound. They’re ugly,nasty, and painfully real. The encounter was terribly upsetting for me. It had beenquite some time since I had been so shaken by a patient encounter.
I teared up in the car on my drive home..He was the first patient that I had really beentaking care of myself who had died..This was the first time that it felt reallypersonal to me.
Why me? Why do I get to be part of a very intimate event in their lives?To watch on rounds as the doctors basically evaluated her like cattle angered me as few
things in life do.I can’t interpret accurately in my young career what exactly I understand about our
visit that day. I do know that I felt good in many ways. I was happy about my placein medicine, and glad about my role.
I questioned whether medical school had made me jaded or calloused to my gut feelings.I sympathized with how foreign this place must be and how scared it must be to not
understand what everyone was saying.I sat and held his hand through these painful moments, and attempted to hold back
tears..I sensed his loneliness and wanted to cry with him. In fact, I did cry as soonas I hit the door.
Transformation and journey in patientexperiences
I came to understand Mr. Smith more. To me, he became a person and not just a patientto try and fix.
As I started to work with him I found there was a very real person beneath it.A patient that I never actually talked to had taught me about trust, loyalty, and family.
These are all things that I have not learned much about during my training.I wondered how I could confront my own mortality.Witnessing this type of end-of-life amends making process will no doubt benefit me in
my future practice. I will be able to talk about such issues with dying patients andcan hopefully facilitate, at least in some small way, their preparations for death.
MEDICAL STUDENT REFLECTIONS ON A PALLIATIVE CARE EXPERIENCE 539

rediscovered their initial motivation and interest in medicineduring their palliative care experience.
What we learned about the curriculum. Previous au-thors have suggested that didactic training in palliativemedicine is not adequate preparation to enable students toprovide such care.1,8 Students also need role models and ex-periences with both positive and negative behaviors. In ouranalysis, we found this to be true. Students were extremelyimpressed by their observations of palliative care physiciansin action, and their eyes were opened to improper treatmentof seriously ill patients, be it poor pain management, inade-quate education, discrimination, or an unwillingness to bepresent to the patient’s suffering. In many of their reflectivewritings, the students clearly state they had learned both whatto do and not do on the basis of their observations of medicalpractitioners. According to Karniele-Miller and colleagues,these experiences compose the ‘‘informal curriculum’’ thatshapes students’ perceptions of professionalism.8
Students reported observing essential skills (i.e., giving badnews, conducting a family conference, or setting goals of care)
that will provide guidance to them in future practice. Mostwould agree that students should not be expected to use a skillthey haven’t observed,1 but without a palliative care rotation,most students’ medical education would be void of such ex-posure. Pain management was frequently cited as an area ofnew learning, whereas management of other symptoms wasnot viewed as noteworthy by these students. Perhaps thisreflects an area of medical practice (pain management) that isseverely neglected during the course of medical educationunless it is taught during exposure to palliative care.
During analysis, themes emerged that reflect student ex-posure to all six core competency domains defined by theAmerican Academy of Hospice and Palliative Medicine workgroup15 and adopted by the Accreditation Council of Grad-uate Medical Education (ACGME) as standards for palliativemedicine education16 (see Table 6). Learning objectivesguiding the revised curriculum were structured to address allof these domains. The reflective writing analysis validatedprogress toward student mastery of the objectives.
Student exposure to interdisciplinary teams was an initialgoal of the curricular redesign. Although some students did
Table 6. Qualitative Responses Related to ACGME Competency Domains
Competency Domain Related Qualitative Responses in Student’s Reflective Writing
Patient and Family Care I came away from the family meeting with such gratitude for the work of thepalliative service.
Listening to the family’s questions and arguments.made me realize how importantfamily meetings are.
Caring for a family who has come to terms with the death of their loved one and arevery sharing with this difficult time is an enriching and honorable experience.
I witnessed this family arrive at that epiphany and it prepared them for what wasahead.
Medical Knowledge I learned the proper way to dose and escalate opioids for pain and delirium.Even though I am not attempting to cure the disease, in palliative medicine I must
always be prepared to answer any questions dealing with the patient’s condition.The most important thing I learned was what a huge impact proper pain control can
have on a patient with end stage disease.Knowledge is powerful, and as physician, we possess a lot of knowledge. One of our
most important jobs is getting patients to understand their healthcare.
Practice-based Learning and Improvement I have a greater appreciation for what palliative medicine does after being on thatrotation
Not everyone has that knowledge of palliative medicine.
Interpersonal and Communication Skills In my belief, a good doctor is a good communicator and listener for their patient.I learned the importance in communication when dealing with sensitive issues such
as DNRs and advance directives.This experience confirmed once again how important communication is when
taking care of people.Effective communication is the only way to customize a patient’s care when so
many.are involved.Empathy for your patients is what gives you the extra energy to stay around at the
end of the day to get things done.
Professionalism I think it is of the utmost importance that we always remember that we do not treatmedical problems or diagnoses, we do not even treat patients; in our jobs asphysicians, we are trusted with the care of our fellow human beings and weshould never take that lightly.
I can only hope that I am not fully motivated by objective data and literature andnever lose sight of my duty to treat the whole patient and treat them like a person.
Systems-Based Practice More harm can be done in waiting to contact the palliative team than by going tooearly.
Knowing when to switch from treatment to comfort is a key component to a goodphysician
540 HEAD ET AL.

refer to the ‘‘team,’’ this did not evolve as a significant themein the coding process. Realizing the need for interdisciplinarylearning, our research team has since received funding for thedevelopment and testing of an interdisciplinary palliativecare curriculum involving students from medicine, nursing,social work, and chaplaincy in interdisciplinary learningopportunities.
Limitations
One significant limitation of our study is that the data aredrawn from a single academic center. In addition, the reflec-tions were written at different times during the medicalclerkship as students rotated through palliative medicine atvarious points during the 12-week experience. Experienceseither before or after the week in palliative medicine couldhave had an impact on their essays, which is unaccounted forin the analysis.
Conclusion
Our in-depth qualitative analysis of the reflective writingsof third-year medical students completing a mandatory week-long rotation in palliative care supports the call for ‘‘hands on’’teaching and role modeling via a clinical experience1 and‘‘reflective time’’17 as essential components of palliativemedical education. If physicians are to effectively care for thedying, they must participate in the clinical care of the dying aspart of their educational experience.18 Such exposure teachesnot only the skills and knowledge required in palliative carebut also compassionate, person-centered care crucial to allmedical practice. The reflections of these students providedinsight into learning not easily measured by traditional eval-uation techniques (i.e., pre-test, post-test, knowledge-basedquestions)—learning that, in their own words, they will neverforget.
Acknowledgments
The Robert Wood Johnson Foundation funded the revisionof the curriculum discussed in this article. Ethical approvalwas granted by the University of Louisville’s Human SubjectProtection Program.
Author Disclaimer Statement
No competing financial interests exist.
References
1. Wear D: ‘‘Face-to-face with it’’: Medical students’ narrativesabout their end-of-life education. Acad Med Apr 2002;77:271–277.
2. Gibbins J, McCoubrie R, Forbes K: Why are newly qualifieddoctors unprepared to care for patients at the end of life?Med Educ 2011;45:389–399.
3. Sandars J: The use of reflection in medical education: AMEEGuide No. 44. Med Teach 2009;31:685–695.
4. Kolb DA: Experiencial Learning: Experience as the Source ofLearning. Upper Saddle River, NJ: Prentice Hall, 1984.
5. Fischer MA, Harrell HE, Haley HL, Cifu AS, Alper E, JohnsonKM, Hatem D: Between two worlds: A multi-institutionalqualitative analysis of students’ reflections on joining themedical profession. J Gen Intern Med 2008;23:958–963.
6. DasGupta S, Charon R: Personal illness narratives: Using re-flective writing to teach empathy. Acad Med 2004;79:351–356.
7. Wald HS, Reis SP: Beyond the margins: Reflective writingand development of reflective capacity in medical educaitonJ Gen Intern Med 2010;25:746–749.
8. Karnieli-Miller O, Vu R, Holtman M, Clyman S, Inui TS:Medical students’ professionalism narrative: A window onthe informal and hidden curriculum. Academic Med2010;85(1):124–133.
9. Gaufberg EH, Batalden M, Sands R, Bell S. The hiddencurriculum: What can we learn from third-year medicalstudent narrative reflections? Acad Med 2010;85:1709–1716.
10. Inui TS: A Flag in the Wind: Educating for Professionalism inMedicine. Washington, D.C.: Association of American Med-ical Colleges, 2003.
11. Hafferty FW: Professionalism and the socialization of med-ical students. In: Creuss RI, Creuss SR, Steinert Y (eds):Teaching Medical Professionalism. Cambridge, UK: CambridgeUniversity Press, 2008, pp. 53–72.
12. Rosenbaum ME, Lobas J, Ferguson K: Using reflection ac-tivities to enhance teaching about end-of-life care. J PalliatMed 2005;8:1186–1195.
13. Creswell JW: Qualitative Inquiry and Research Design: Choos-ing among Five Tradiations. Thousand Oaks, CA: Sage, 1998.
14. Ratanawongsa N, Teherani A, Hauer KE: Third-year medi-cal students’ experiences with dying patients during theinternal medicine clerkship: Qualitative study of the infor-mal curriculum. Acad Med 2005;80:641–647.
15. American Academy of Hospice and Palliative Medicine(AAHPM): Hospice and Palliative Medicine Core Competencies,Vol Version 2.3. Glenview, IL: AAHPM, 2009.
16. Accreditation Council of Graduate Medical Education(ACGME): ACGME Program Requirements for Graduate Med-ical Education in Hospice and Palliative Medicine. Chicago, IL:ACGME, 2008.
17. Weissman DE, Quill T, Block SD: Missed opportunities inmedical student education. J Palliait Med 2010;13:489–490.
18. Anderson WG, Williams JE, Bost JE, Barnard D: Exposure todeath is associated with positive attitudes and higherknowledge about end-of-life care in graduating medicalstudents. J Palliat Med 2008;11:1227–1233.
Address correspondence to:Barbara A. Head, Ph.D.
Interdisciplinary Program for PalliativeCare and Chronic Illness
University of LouisvilleMedical Dental Research Building, Suite 110
511 South Floyd StreetLouisville, KY 40202
E-mail: [email protected]
MEDICAL STUDENT REFLECTIONS ON A PALLIATIVE CARE EXPERIENCE 541