i. best in show: useful vignettes from the 2010 uscap meeting
TRANSCRIPT
I. Best in show: useful vignettes from the 2010 USCAP meeting.
Michael R. Pins, MDDirector, Anatomic Pathology
Advocate Lutheran General HospitalMay 18, 2010

RCH-GIP Society Companion Meeting: “H. pylori-negative gastritis” (Robert M. Genta, MD UT Southwestern University)
(Not the “Roger C. Haggitt Memorial Lecture given in memory of Harvey Goldman”)
Table 1: Causes of Helicobacter pylori-negative chronic active gastritis.> Crohn’s disease> Focal active (“enhanced”) gastritis
(non-specific)> Lymphocytic gastritis with an
active component> Reflux carditis> Drug (e.g. NSAIDs)> Infectious (CMV, Staph, syphilis)
Table 2: Possible reasons for failure to detect Helicobacter pylori.> Diagnostic error
> Not seen> Misdiagnose chronic active
gastritis> Sampling error
> PPIs shift bacteria from antrum> Altered environment
> Intestinal metaplasia> Ulcer
> Suppression from other drugs (antibiotics, PPIs, etc)

RCH-GIP Society Companion Meeting: “H. pylori-negative gastritis” (Robert M. Genta, MD UT Southwestern University)
(Not the “Roger C. Haggitt Memorial Lecture given in memory of Harvey Goldman”)
Helicobacter pylori colonization?> Dr. Genta estimates 1:3000 gastric biopsies
will show H. pylori in the absence of gastritis.
> These rare cases may represent non-specific staining of the generally used (polyclonal?) H. pylori antibody.
> A more specific (monoclonal?) antibody exists but it does not stain H. heilmannii.
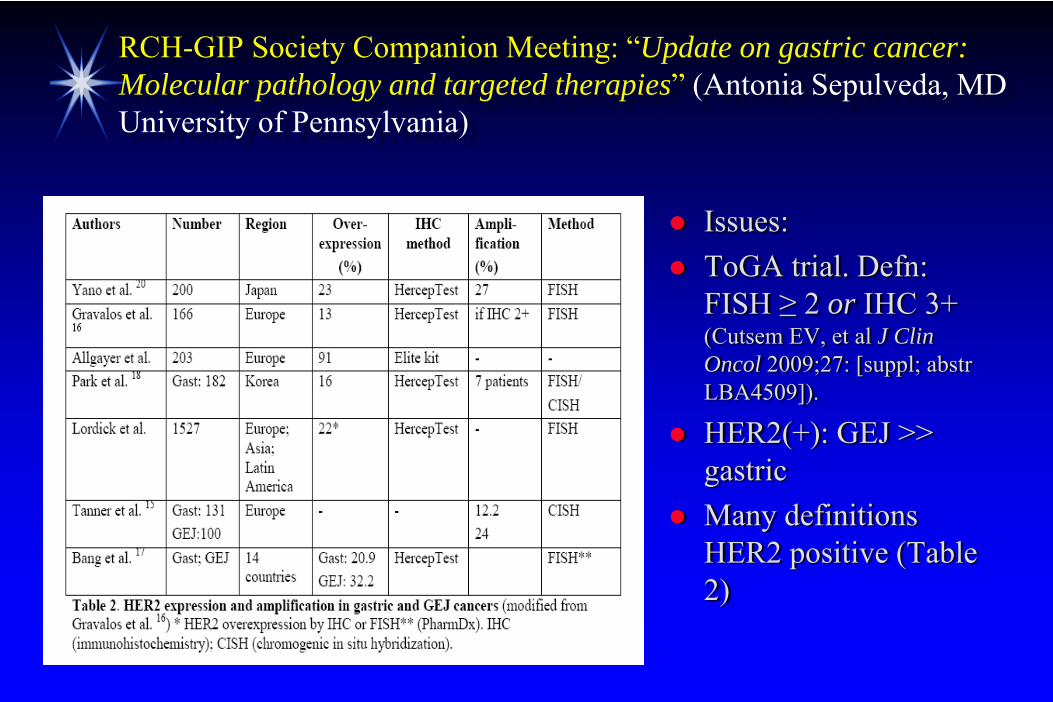
RCH-GIP Society Companion Meeting: “Update on gastric cancer: Molecular pathology and targeted therapies” (Antonia Sepulveda, MD University of Pennsylvania)
Issues:ToGA trial. Defn: FISH ≥ 2 or IHC 3+(Cutsem EV, et al J ClinOncol 2009;27: [suppl; abstrLBA4509]).
HER2(+): GEJ >> gastricMany definitions HER2 positive (Table 2)

Gynecological Pathology Evening Specialty Conference: “Ovarian Cancer” (Moderator, Robert J Kurman, MD Johns Hopkins)
Type I: serous (l.g.), endometrioid(l.g.), clear cell, mucinous, transitional cell.> Indolent (precursors), earlier stage, p53 (-), genomically
stable
Type II: serous (h.g.), undifferentiated, MMMT.
Aggressive (no precursors), advance stage, p53 (+), genomically unstable
Kurman RJ and Shih IM. The origin and pathogenesis of epithelial ovarian cancer: A proposed unifying theory Am J Surg Pathol 2010;34:433-443.

Gynecological Pathology Evening Specialty Conference: “Ovarian Cancer” (Moderator, Robert J Kurman, MD Johns Hopkins)

ISUP Companion Meeting: “Renal tumors with eosinophiliccytoplasm” (Jesse K. McKenney, MD Stanford University)
CC RCC, eosinophilic var. CK, EMA, CD10, RCC -3p, CH3-3p-CH3
Papillary RCC (type 2) CK7, AMACR +7, +17, -Y
Chromoph. RCC, eos var CK7 (patchy), CD117, Ksp-cadherin, claudin7, EpCam -1,2,6,10,13,17,21 and Y
Oncocytoma CD117, Ksp-cadherin - 1,Y, rarely t(5;11) or t(9;11)
Collecting duct carcinoma Varies Varies
Xp11 (TFE3) RCC TFE3, melanocytic markers f(+); CKs (-) Xp11
t(6;11) RCC TFEB, melanocytic markers f(+); CKs (-) t(6;11)
Acquired (dialysis) RCC AMACR +1,2,3,6,7,16,10, and Y (few cases)
Epithelioid AML SMA, melanocytic markers 9q34 (TSC1), 16p13.3 (TSC2)
Hereditary leiomyomatosis RCC
See papillary RCC (type 2) 1q42-43 (fumarate hydratase)
Birt-Hogg-Dube See oncocytoma, chromophobe, CC RCC 17p11.2 (BHD)
RCC post neuroblastoma EMA, vimentin, CKs Too few cases

ISUP Companion Meeting: “Renal tumors with eosinophiliccytoplasm” (Jesse K. McKenney, MD Stanford University)
Issues:> Subtyping has prognostic and therapeutic
implications.> IHC of limited utility in morphologically
equivocal cases.> Stanford karyotypes all of their renal tumors
<40> Karyotype all grossly unusual tumors?

APS-SSP Companion Meeting: “Placenta potpourri: thepernicious, picayune and pervasive” (Phyllis C Huettner, MD Washington University)
New Topics / Twists:Fetal inflammatory response syndrome> Fetal complications
Maternal inflammatory response (Stage 1,2,3; Grade 1,2)(Redline RW, et al. Pediatr Dev Pathol 2003;6:435-448)
Fetal inflammatory response (Stage 1,2,3; Grade 1,2)(Redline RW, et al. Pediatr Dev Pathol 2003;6:435-448)
CMV most common cause of infectious (non-immunologic) villitis

II. Pathologic examination of the placenta: Indications and potential maternal and fetal
implications.
Michael R. Pins, MDDirector, Anatomic Pathology
Advocate Lutheran General HospitalMay 18, 2010

Placental Pathology - Outline
Indications for Placental examination> ACOG and CAP> Advocate Risk Management Patient Safety Initiative
What we do – documentation> Photographic> Systematic gross and microscopic> Anatomical approach
> Umbilical cord> Membranes> Disk
Processes (with specific examples): Infectious, Neoplastic, Vascular, Developmental, Mechanical, Hereditary, Inflammatory, Iatrogenic, Idiopathic, Others

Placental Pathology - Indications
American College of Obstetricians and Gynecologists. Placental Pathology. Committee Opinion 125. Washington, DC: ACOG; 1993.“declined recommending any individual indications for placental examination in live births, expressing concern that there were insufficient data to support the use of such a policy.”
College of American Pathologists (CAP) consensus guidelines.Langston C, et al. Arch Pathol Lab Med 1997;121:449-476.Maternal indications and fetal indicationsStrong Memorial Hospital (Obstet Gynecol 2007;109:35-41).> Expected: 37.5%> Actual: 18.2%

Placental Pathology – CAP Indications
Maternal> Fever> Pre-eclampsia, HTN> Hx. Recurrent loss> Bleeding> Systemic disorders
> Diabetes> Collagen vascular> Hematologic> Etc
Fetal / Neonatal> IUGR> Prematurity> Hydrops> Developmental /
chromosomal> Stillbirth> Fetal distress> Isoimmunization> Twins, Triplets, etc.> PROM> Abnormal placental (shape,
size, two vessels, etc)

Placental Pathology – What we do.
Photographic documentation> Maternal and fetal surfaces
photographed on all placentas with anyabnormality.
Medicolegal issues> Documentation> “Why wasn’t the placenta
submitted for Pathological examination.” Maternal surface showing adherent blood clot
in a patient who underwent emergent C-section due to clinical abruption.

Placental Pathology – What we do.
Systematic gross and microscopic examination.> Standard tissue sections:
> Umbilical cord> Membranes> Disk (x2)> Abnormalities.
Anatomical approach.> Umbilical Cord
> Length, insertion, twist, knots, number of vessels, inflammation > Membranes - amnion, chorion, decidua.
> Color, chorioamnionitis, amniotic epithelium abnormalities, meconium, maternal vessels.
> Placental Disk - fetal and maternal structures. > Size, hemorrhage, maturity, infarct, nucleated RBCs, maternal
space, villi.

Placental Pathology – Normal v. Abnormal.
Fetal surface showing showing essentially normal umbilical cord, membranes and disk .
Maternal surface showing showing essentially normal decidua and placental tissue.

Placental Pathology – Normal v. Abnormal.
Normal decidua including blood vessels is maternal tissue.
Immature (first trimester) villi (fetal tissue). The intervillus space is maternal.

Placental Pathology – Common umbilical cord abnormalities.
Velamentous insertion of umbilical cord (a/w hemorrhage, or fetal death)
Two vessel umbilical cord (single umbilical artery)(a/w fetal
gentourinary abnormalities)
True knot (left; a/w fetal death) and “false” knot (right)

Placental Pathology – Fetal inflammatory response: umbilical cord abnormalities.
Stage 2: Arteritis Stage 3: Necrotizing funisitis
Stage 1: Phlebitis
“Placenta potpourri: thepernicious, picayune and pervasive” (Phyllis C Huettner, MD Washington
University. 2010 USCAP)

APSSSP Companion Meeting: “Placenta potpourri: thepernicious, picayune and pervasive” (Phyllis C Huettner, MD Washington University)
Fetal inflammatory response (FIP) Syndrome> Pathogenesis complex: cytokine mediated.
Fetal complications> Neonatal sepsis> Pneumonia> Bronchopulmonary dysplasia> Intraventricular hemorrhage> Cerebral palsy> Necrotizing enterocolitis

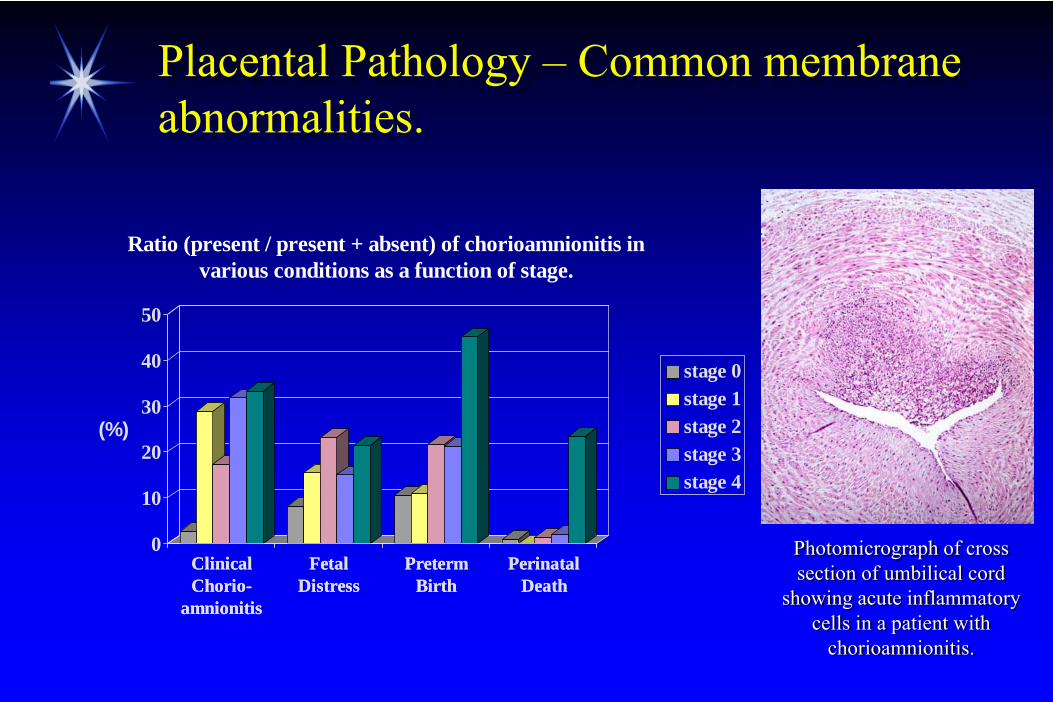
Placental Pathology – Common membrane abnormalities.
Fused, diamniotic twin placental.
Dichorionic dividing membrane (Zygosity: 87% DZ, 13% MZ)
Monochorionic dividing membrane (Zygosity: 100% MZ)

Placental Pathology – Common membrane abnormalities.
Fetal surface (cord removed) showing marked meconium staining. High-power microscopic (below) showing
pigment-laden histiocytes (a/w fetal distress)
Fetal surface showing amnion nodosum (a/w oligohydramnios)
Acute atherosis of maternal decidual vessels (a/w HTN, PIH, pre-eclampsia, eclampsia)

Placental Pathology – Common membrane abnormalities.
Fetal membranes grossly unremarkable showed pigment-laden histiocytes
Iron histochemical stain confirms the pigment is hemosiderin. Clue to the true nature of the
pigment is the presence of pigment in the decidua.

Placental Pathology – Common membrane abnormalities.
Stages of Chorioamnionitis. (van Hoeven, et al. Ped Pathol and Lab Med 1996;16:731-744)
> stage 1: Five neutrophils/hpf in five nonadjacent fields - no involvement of amnion.
> stage 2: Neutrophils in amnion but not to the amniotic epithelium.
> stage 3: Neutrophils in all layers of amnion; only focal necrosis.
> stage 4: Necrosis w/ loss of architecture in the amnion.
Acute chorioamnionitis affecting only one twin (top; a/w preterm delivery, etc).
Placental Pathology – Common membrane abnormalities.
ClinicalChorio-
amnionitis
FetalDistress
PretermBirth
PerinatalDeath
0
10
20
30
40
50
(%)
ClinicalChorio-
amnionitis
FetalDistress
PretermBirth
PerinatalDeath
Ratio (present / present + absent) of chorioamnionitis in various conditions as a function of stage.
stage 0stage 1stage 2stage 3stage 4
Photomicrograph of cross section of umbilical cord
showing acute inflammatory cells in a patient with
chorioamnionitis.
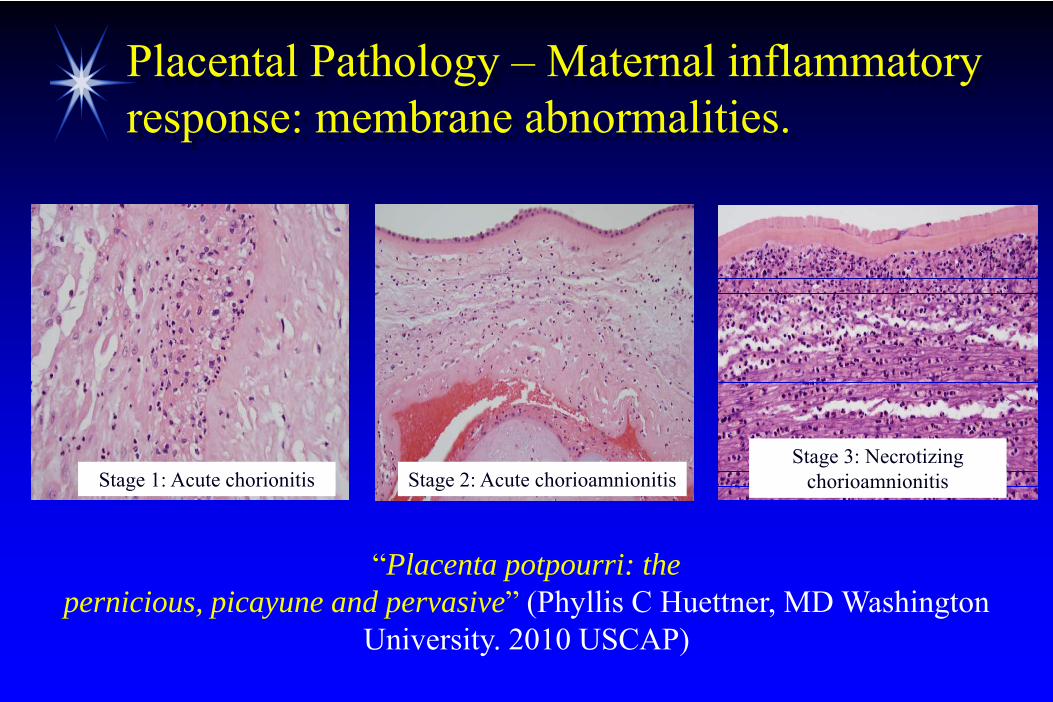
Placental Pathology – Maternal inflammatory response: membrane abnormalities.
“Placenta potpourri: thepernicious, picayune and pervasive” (Phyllis C Huettner, MD Washington
University. 2010 USCAP)
Stage 1: Acute chorionitis Stage 2: Acute chorioamnionitisStage 3: Necrotizing
chorioamnionitis

Placental Pathology – Common disk abnormalities.
Twin gestation with accessory (succenturiate) lobe (a/w hemorrhage
during delivery)
Small (a/w IUGR, pre-eclampsia, trisomy) circumvallate (membranes
double back; a/w fetal demise) placenta. A large placenta is a/w
DM, syphilis, fetal anemia / hydrops, Beckwith-Wiedemann syndrome)
Villi (left) intimately (no intervening decidua) associated with myometrium (right) c/w placental accreta. Placenta increta invades more deeply and percreta invades through.

Placental Pathology – Common disk abnormalities.
Fetal surface showing well developed (palpable) thrombi
Fetal surface with focal (palpable) vascular calcification consistent with
prior thrombosis
“Defense Attorneys get excited when the Pathologist sees thromboses in the chorionic plate vessels”

Placental Pathology – Common disk abnormalities.
Cross section of disk showing typically well-circumscribed infarct. Very common incidental finding, particularly post-dates placentas. High percentage (below) infarcts may be
associated with IUFD
Cross section of disk showing maternal floor infarct (MFI) with
extensive fibrin deposition extending from the basalis. MFI and the
related massive perivillous fibrinoid may be a/w IUGR and fetal death and
may recur with subsequest pregnancies.

Placental Pathology – Common disk abnormalities.
Photomicrograph showing acute supperative, necrotizing villitis. Causative organisms include Candida, campylobacter, CMV,
coccidiodes, Group B strep, HSV, Listeria [this case], syphilis, others.
Photomicrograph showing histiocytic infiltrate in the intervillous space (chronic intervillositis).
Subtle, rare lesion a/w recurrent pregnancy loss

Placental Pathology – Common disk abnormalities.
Photomicrograph showing lymphocytes (maternal, CD8+) within villi (villitis of unknown etiology; VUE). Common, subtle, often focal, non-specific lesion a/w
IUGR, recurrent pregnancy loss, cerebral palsey and encephalopathy when multifocal. May recur with subsequent pregnancies. (Redline RW. Human Pathol
2007;38:1439-1446)
“VUE with villous fibrosis
(loss of maternal
vessels) more severe than
VUE without.”

Placental Pathology – Common disk abnormalities.
Chorionic plate vasculitiswith thrombosis - considered part of the fetal inflammatory
response.“Placenta potpourri: thepernicious, picayune and
pervasive” (Phyllis C Huettner, MD Washington University. 2010
USCAP)

Placental Pathology - Issues
Indications for Placental examination> ACOG and CAP> Patient Safety Initiative (Donald W. Aaronson, MD,
JD, MPH, Medical Director Patient Safety, Advocate Health Care)
What we do – documentation> Photographic> Standardized grosses
Processes: Idiopathic