hypnosis, placebo an, d suggestion in the treatment of … reported failures to replicate this side...
TRANSCRIPT

Hypnosis, Placebo, and Suggestion in theTreatment of Warts
NICHOLAS P. SPANOS, PHD, ROBERT J. STENSTROM, MA,AND JOSEPH C. JOHNSTON, MA
Two experiments assessed the effects of psychological variables on wart regression. In Exper-iment 1, subjects given hypnotic suggestion exhibited more wart regression than those giveneither a placebo treatment or no treatment. In Experiment 2, hypnotic and nonhypnotic subjectsgiven the same suggestions were equally likely to exhibit wart regression and more likely toshow this effect than no treatment controls. In both experiments, treated subjects who lostwarts reported more vivid suggested imagery than treated subjects who did not lose warts.However, hypnotizability and attribute measures of imagery propensity were unrelated to wartloss. Subjects given the suggestion that they would lose warts on only one side of the body didnot show evidence of a side-specific treatment effect.
INTRODUCTION
Warts are benign tumors of the skin, andmembers of the papillomaviruses genus areresponsible for the various types of infec-tious warts, i.e., Verruca vuJgarus, Ver-ruca pJantaris, Verruca pJana juveniJis,Condylom accuminatum (1). Interest-ingly, a good deal of anecdotal evidence,along with a number of clinical studies,implicate psychological factors in the re-mission of warts (e.g., 2-4). The most com-monly employed psychological treat-ments for warts are hypnotic suggestionand various placebo interventions (e.g., sa-line injections defined as potent wart cures).Most investigators have interpreted the re-sults of uncontrolled clinical studies asdemonstrating that both hypnotic and pla-
From the Department of Psychology, Faculty ofSocial Sciences, Carleton University, Ottawa, Can-ada.
Address reprint requests to: Nicholas P. Spanos,Ph.D., Department of Psychology, Faculty of SocialSciences, Carleton University, Loes Building, OttawaKlS 5B6, Canada.
Received for publication September 3, 1987; re-vision received January 14, 1988.
Psychosomatic Medicine 50:245-260 (1988)Copyright © 19B8 by the American Psychosomatic Society, IncPublished by Elsevicr Science Publishing Co , Inc52 Vanderbilt Avenue, New York, NY 10017
cebo interventions induce wart regression(see 5, 6 for reviews). This contention has,however, been challenged, and several in-vestigators (7-9) have argued that the find-ings of these studies can be adequately ex-plained in terms of spontaneous remission.
The available data concerning sponta-neous remission rates for warts are not en-tirely consistent (10, 11). Moreover, mostclinical studies provide no data concern-ing pretreatment duration of warts beyondthe patients' unsubstantiated estimates.Unfortunately, the accuracy of these esti-mates is simply unknown. For these rea-sons, it is hazardous to draw conclusionsabout treatment efficacy in wart studiesthat lack an untreated control group.
Only two studies in this area have in-cluded untreated control subjects. Mem-mesheimer and Eisenlohr (12) applied aninnocuous dye that was described as a warttreatment to the warts of 70 subjects, while70 controls received no treatment. After 1V2 months, and again after 3 months, sub-jects in the placebo group had lost morewarts than controls. By 6 months, how-ever, there were no differences betweenthe groups in wart remission. Surman et
245
0033-3174/88/S3.50

N. SPANOS et al.
al. (13) gave hypnotic suggestions for wartremission to 17 subjects and no treatmentto seven others. At the end of 3 months,53% of the hypnotic subjects, but none ofthe controls, had lost at least some of theirwarts. The findings of these two controlledstudies certainly suggest the operation ofa psychological treatment effect. Never-theless, given the somewhat counterintui-tive nature of the findings, the wide be-tween-subject variability found in rates ofspontaneous remission for warts (e.g., 11),and the small number of control subjectstested by Surman et al (13), replication ofthese findings is called for. The presentstudy includes two controlled experi-ments aimed at replicating and extendingprevious findings concerning the role ofpsychological factors in wart remission.
HYPNOSIS, IMAGERY,AND PLACEBOS
One potentially important differencebetween hypnotic and placebo treatmentsconcerns the psychological orientations thatsubjects develop toward these procedures.Both procedures attempt to instill expec-tations of treatment success. However,hypnotic subjects are encouraged to seethemselves as engaged in cognitive activ-ity that will bring about their own recov-ery. For example, suggestions for wartregression encourage subjects to becomeinvolved in vividly imagining their wartsas tingling, shrinking, disappearing, andso on. Placebo procedures, on the otherhand, tacitly define subjects as the passiverecipients of a therapeutic procedure. Sub-jects given a placebo are not asked to imag-ine anything or to view themselves as ac-tively involved in bringing about their ownrecovery. Instead, they are instructed to
simply wait for therapeutic effects to oc-cur, or to look for indications that sucheffects are in progress (e.g., to notice anytingling around the wart). One purpose ofour first experiment was to compare wartregression in subjects assigned to a hyp-notic, placebo, or no treatment controlcondition.
Several investigators (14, 15) have ar-gued that the important therapeutic com-ponent in hypnotic treatments is the im-agery encouraged by the suggestions forwart regression. According to this hypoth-esis, subjects who generate the most vividsuggested imagery are the most likely toexhibit wart regression. In order to ex-amine this hypothesis, we assessed thevividness that our hypnotic subjects at-tributed to their suggested imagery. We alsoexamined relationships between the re-porting of suggested sensations and treat-ment efficacy in both the hypnotic and pla-cebo treatments.
Hypnotizability and Wart Remission
Subjects vary substantially in their levelof responsiveness to hypnotic suggestions(i.e., hypnotizability), and a number ofstandardized scales for the assessment ofhypnotizability are available (e.g., 16).Three studies (6,17,18) reported that highlyhypnotizable subjects given a hypnotictreatment were more likely to lose wartsthan low hypnotizables. On the other hand,one study (9) reported that none of 20 highlyhypnotizable subjects treated with hyp-nosis exhibited wart regression, and an-other study (13) found no relationship be-tween hypnotizability and wart loss inhypnotically treated subjects.
Unfortunately, most studies in this areadid not use standardized scales to assesshypnotizability, and the psychometric
246 Psychosomatic Medicine 50:245-260 (1988)

HYPNOSIS IN WART TREATMENT
properties of the assessment proceduresthat were used are unknown. Further-more, in these studies hypnotizability wasassessed before the hypnotic wart treat-ment. Consequently, subjects' knowledgethat they were hypnotizable or unhypno-tizable may have influenced the mannerin which they responded to subsequentsuggestions for wart regression. For ex-ample, some evidence (19, 20) indicatesthat hypnotizability correlates with sug-gested analgesia when hypnotizability isassessed before analgesia testing and whensubjects conceptually link their hypnotiz-ability with the analgesia test situation.However, when hypnotiability is assessedafter analgesia testing,or if low hypnotiz-ables are assured that they can exhibit sug-gested analgesia despite their low hyp-notizability, then the significant correlationbetween hypnotizability and suggestedanalgesia often disappears. In other words,hypnotizability testing can create potentexpectations concerning how subjects arelikely to respond to forthcoming sugges-tions. For example, as a consequence ofhaving previously tested low in hypnotiz-ability, some subjects may come to believethat they are unable to generate the im-agery called for by the suggestion for wartremission. Therefore these subjects maymake no attempt, or only a half-heartedattempt, to generate such imagery. In thepresent experiments we eliminated poten-tial interpretive problems of this kind byassessing hypnotizability at the end of the6-week assessment period that followedtreatment administration.
Some investigators (21) have suggestedthat hypnotizability should predict wartregression following psychological inter-vention regardless of whether the psycho-logical treatment involves administrationof an hypnotic induction procedure. To
test this possibility we assessed subjectsin all treatments for hypnotizability at theend of their follow-up period.
Specificity Effects
Perhaps the most dramatic finding inthis research area concerns the idea thatsuggestions can exert a selective effect onwart regression. In one study (18), highlyhypnotizable subjects, all of whom hadwarts on both sides of their body, weregiven the hypnotic suggestion that theywould lose only the warts on one side. Thesuggestion was always aimed toward theside of the body with the largest numberof warts. Nine out of the ten highly hyp-notizable subjects lost warts only on thetreated side, while the remaining subjectlost warts bilaterally.
Five subsequent studies (7-9, 13, 22)have reported failures to replicate this sidespecific treatment effect. However, most ofthese replication failures have had meth-odological difficulties. For instance, in twoof these studies (9, 22), so few subjects lostwarts on either side that no conclusionsabout a side-specific effect were possible.Two other studies (7, 8) failed to find aside-specific effect when using a placeboas the treatment. Unfortunately, neitherstudy employed hypnotic suggestion.
Surman et al. (13) unambiguously failedto replicate the side-specific treatment ef-fect. In that study, ten subjects with bilat-eral warts lost warts following a hypnoticsuggestion directed at one side of the body.In nine out of the ten cases, however, wartloss was bilateral rather than treatment-side specific.
In order to further explore the side-spe-cific effect, subjects in both of our exper-iments with bilateral warts were given atreatment directed to only one side of their
Psychosomatic Medicine 50:245-260 (1988) 247

N. SPANOSetal.
body. To test for the specificity effect, thedata from the two experiments were com-bined. Consequently, these findings arediscussed at the end of Experiment 2.
METHOD (EXPERIMENT 1)
SubjectsSixty-four individuals with warts on one or both
hands (29 males, 35 females, ages 10-74 years) weresolicited for participation in a study of warts throughadvertisements placed on posters around the Carle-ton University campus, in local newspapers, and onthe radio. Subjects were informed that several treat-ments for warts were being compared and that somesubjects would be assigned to a placebo treatment.Subjects were asked to abstain from any other warttreatment for the duration of the study. All were paid$15 for their participation.
ProcedureSubjects were randomly assigned to a hypnotic
suggestion (N = 22), cold laser placebo (N = 24), orno treatment control condition (N = 17). All subjectswere seen individually by a research assistant, whocounted the warts on each of their hands and re-corded their age and their estimates of the durationof their warts (in months). Subjects were then es-corted to the treatment room and introduced to themale therapist, who conducted both the hypnoticand placebo treatments. Hypnotic and placebo sub-jects were administered their respective treatmentsand scheduled to return in six weeks for follow-upevaluation. Control subjects were informed that theywere on a waiting list and were asked to return in 6weeks to receive treatment. At the 6 weeks follow-up session, subjects again had their warts countedby a research assistant and were then tested for hyp-notizability using the Carleton University Respon-siveness to Suggestion Scale (CURSS; 13). This scaleyields an objective (CURSS: 0) score that reflects thenumber of suggestions to which subjects made theappropriate behavioral response, and a subjective score(CURSS: S) that reflects the intensity of their subjec-tive responses to the suggestions. At this time, sub-jects were also assessed on a modification of the Bettsvividness of imagery questionnaire (23). The researchassistant who counted subjects' warts in the baselineand follow-up sessions was blind to subjects' treat-ment assignment.
Hypnotic Treatment.Eleven of the 22 subjects in this group had warts
on both hands. In these 11 cases, one hand was cho-sen at random as the target hand, and all treatmentsuggestions were referred exclusively to the targethand. After being comfortably seated and asked toclose their eyes, subjects were orally administered a5-min hypnotic induction procedure (modified from24). Following the induction procedure, and withouta break in continuity, subjects were administered asuggestion for wart elimination that was 2 min induration. The suggestion asked subjects to attend tothe sensations in their target hand and informed themrepeatedly that the skin around their warts was be-ginning to tingle and grow warm. The suggestion alsoinformed subjects that their warts would shrink andfall off and asked them to vividly imagine their wartsshrinking in size and dissolving away. Following thesuggestion, subjects opened their eyes and rated thevividness with which they had imagined their wartsshrinking and disappearing on a 7-point scale withalternatives that ranged from "No image present"(scored 0) to "Extremely vivid; as vivid as though itwas actually happening" (scored 6). Next, subjectsrated the intensity with which they experienced sixsensations around their warts (tingling, warmth,throbbing, numbness, shrinking, prickling). Eachsensation was rated on a 7-point scale that rangedfrom "not at all" (scored 0) to "strongly" (scored 6).The six items were totaled to yield a single sensationscore for each subject.
Following their sensation ratings, subjects wereasked to again close their eyes and were readmin-istered the same 2-min suggestion. Finally, subjectswere "awakened," instructed to count their warts everyday, and after each counting to close their eyes andspend 3 to 4 min imagining the warts on their targethand disappearing.
Placebo TreatmentThese subjects were informed that they would be
treated with a relatively new technique known as a"cold laser." They were given a few minutes to readan article from Life Magazine (May 1982) on the med-ical use of lasers, and afterwards they read a briefbut technical account of laser action. This technicalaccount included an explanation in terms of "differ-ential tissue density" of how the cold laser wouldkill their warts without effecting surrounding healthytissue. Subjects with bilateral warts (N = 12) wereinformed that only one hand would be treated at that
248 Psychosomatic Medicine 50:245-260 (1988)

HYPNOSIS IN WART TREATMENT
time and that the other hand would be treated in 6weeks. The target hand was chosen randomly.
The "laser" was housed in a sound-attenuatedchamber. It was a metal devise with numerous dialsand buttons and an opening in which subjects placedtheir target hand. When the "laser" was switched on,it made a whirring sound, and a sweeping pink lightcould be seen in the opening. Subjects donned "pro-tective goggles" and placed their hand in the openingfor the first of two 4-min "laser doses." They weretold that they might experience some tingling, pric-kling, and warmth in their hand during the treatmentbut not to be alarmed at these sensations. Followingthat first "laser dose," subjects completed the samesensation questionnaire given to the hypnotic sub-jects, and then placed their hand back in the "laser"for their second dose. Following the placebo treat-ment, subjects were instructed to count their wartsevery day and at these times to notice whether theyexperienced any sensations in their warts.
No Treatment ControlsAfter their warts were counted, these subjects were
informed that they were on a waiting list and wouldbe administered a treatment for their warts in 6 week'stime.
RESULTS
Table 1 shows the number of warts atbaseline for subjects in the three condi-tions. A one way analysis of variance {AN-OVA) indicated no significant differencesamong conditions in number of baselinewarts, F(2,61) < 1. Separate ANOVAs also
indicated no significant differences be-tween conditions in subjects' ages or intheir estimates of wart duration.
Unfortunately, there is no ideal way toquantify wart loss. In the present study thenumber of warts possessed by subjects atbaseline ranged from one to 60. Almost athird of the subjects (N = 20) had onlyone wart at baseline, and slightly more thanhalf the subjects (N = 33) had three or fewerwarts at baseline. Subjects with a smallnumber of baseline warts could show onlysmall decreases in absolute number ofwarts, even when they lost all of their warts.On the other hand, a measure of percent-age loss also has difficulties. For example,a subject who loses her only wart gets ahigher percentage loss score (100%) thana subject who loses 25 of his 50 warts (50%).We dealt with the measurement issue byusing both a continuous and a dichoto-mous index of wart loss. The continuousindex was percentage of wart loss frombaseline, and the dichotomous index waswhether or not a subject lost any (one ormore) warts.
Treatment Effects
Table 1 shows that subjects in the threeconditions differed significantly in per-centage of warts lost (F (2,61) = 7.17,p < 0.01). Post hoc analyses indicated that
TABLE 1. Means for Number of Warts at Baseline, Percent Wart Loss, Age and Estimated Duration ofWarts in Hypnotic, Placebo, and No Treatment Control Conditions
BaselinePercent lossAgeDuration
M
7.32"33.68a
29.45a
77.83a
Hypnosis
SD
14.9241.4811.1397.31
Placebo
M
7.21a
9.086
28.33a
64.04a
SD
10.7622.2513.4043.70
Control
M
5.35a
2.06b
29.06a
78.00a
SD
6.116.39
14.0452.95
Within rows, means sharing the same letter superscript fail to differ significantly at a = .05.Estimated duration is in months.
Psychosomatic Medicine 50:245-260 (1988) 249
N. SPANOS et al.
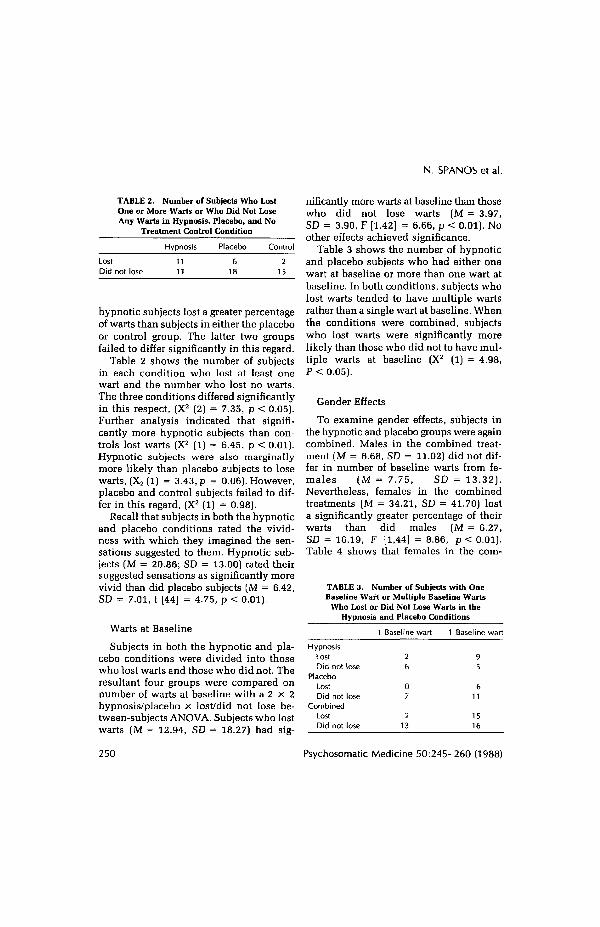
TABLE 2. Number of Subjects Who LostOne or More Warts or Who Did Not LoseAny Warts in Hypnosis, Placebo, and No
Treatment Control Condition
Hypnosis Placebo Control
LostDid not lose
hypnotic subjects lost a greater percentageof warts than subjects in either the placeboor control group. The latter two groupsfailed to differ significantly in this regard.
Table 2 shows the number of subjectsin each condition who lost at least onewart and the number who lost no warts.The three conditions differed significantlyin this respect, (X2 (2) = 7.35, p < 0.05).Further analysis indicated that signifi-cantly more hypnotic subjects than con-trols lost warts (X2 (lj = 6.45, p < 0.01).Hypnotic subjects were also marginallymore likely than placebo subjects to losewarts, (X2(l) = 3.43, p = 0.06). However,placebo and control subjects failed to dif-fer in this regard, (X2 (1) = 0.98).
Recall that subjects in both the hypnoticand placebo conditions rated the vivid-ness with which they imagined the sen-sations suggested to them. Hypnotic sub-jects [M = 20.86; SD = 13.00) rated theirsuggested sensations as significantly morevivid than did placebo subjects (M = 6.42,SD = 7.01, t [44] = 4.75, p < 0.01).
Warts at Baseline
Subjects in both the hypnotic and pla-cebo conditions were divided into thosewho lost warts and those who did not. Theresultant four groups were compared onnumber of warts at baseline with a 2 x 2hypnosis/placebo x lost/did not lose be-tween-subjects ANOVA. Subjects who lostwarts (M = 12.94, SD = 18.27) had sig-
nificantly more warts at baseline than thosewho did not lose warts [M = 3.97,SD = 3.90, F [1.42] = 6.66, p < 0.01). Noother effects achieved significance.
Table 3 shows the number of hypnoticand placebo subjects who had either onewart at baseline or more than one wart atbaseline. In both conditions, subjects wholost warts tended to have multiple wartsrather than a single wart at baseline. Whenthe conditions were combined, subjectswho lost warts were significantly morelikely than those who did not to have mul-tiple warts at baseline (X2 (1) = 4.98,P < 0.05).
Gender Effects
To examine gender effects, subjects inthe hypnotic and placebo groups were againcombined. Males in the combined treat-ment (M = 6.68, SD = 11.02) did not dif-fer in number of baseline warts from fe-males (M = 7.75, SD = 13.32).Nevertheless, females in the combinedtreatments (M = 34.21, SD = 41.70) losta significantly greater percentage of theirwarts than did males (M = 6.27,SD = 16.19, F [1,44] = 8.86, p < 0.01).Table 4 shows that females in the com-
TABLC 3. Number of Subjects with OneBaseline Wart or Multiple Baseline Warts
Who Lost or Did Not Lose Warts in theHypnosis and Placebo Conditions
HypnosisLostDid not lose
PlaceboLostDid not lose
CombinedLostDid not lose
1 Baseline wart
26
07
213
1 Baseline wart
95
611
1516
250 Psychosomatic Medicine 50:245-260 (1988)

HYPNOSIS IN WART TREATMENT
TABLE 4. Number of Males and Females Losingand Not Losing Warts in the Hypnosis and
Placebo Conditions Combined
Males Females
LostDid not lose
bined treatments more frequently lost atleast one wart than did males, X2 (1) = 6.88,p < 0 1 .
Questionnaires and Hypnotizability
Table 5 shows the mean questionnaireand hypnotizability scores for subjects wholost and did not lose warts in both thehypnosis and placebo conditions. In thehypnotic condition, subjects who lost wartsreported significantly more vivid sug-gested imagery than those who did not lose(F [1,20] = 5.30, p O < .05). In this con-dition, those who lost warts also tendedto report higher levels of suggested sen-sations than did those who did not losewarts (F [1,20] = 3.59, p < 0.07). Hyp-notic subjects in the "lost" and "did notlose" groups failed to differ significantlyon any of the questionnaire or hypnotiz-ability variables. In the placebo group, noneof the questionnaire or hypnotizability
variables differentiated significantly be-tween those who lost and did not lose warts.
Pearson correlation coefficients werecomputed between each questionnairevariable and percentage of wart loss in boththe hypnosis condition and the placebocondition. In the hypnosis condition, per-centage of wart loss correlated signifi-cantly with vividness of suggested im-agery (r [20] = .58, p < 0.01) and vividnessof suggested sensations (r [20] = .54,p < 0.05), but failed to correlate signifi-cantly with any of the other questionnairevariables. In the placebo condition, per-centage of wart loss failed to correlate sig-nificantly with any of the questionnairevariables.
DISCUSSION
Hypnotic subjects lost significantly morewarts than controls, and relatedly, morehypnotic subjects than controls lost one ormore of their warts. These findings repli-cate those of Surman et al. (13) and makeit highly unlikely that the effects of hyp-notic suggestions on wart regression canbe "explained away" in terms of sponta-neous remission.
Subjects given the "cold laser" placebo
TABLE 5. Means on Questionnaire and Hypnotizability Variable for Subjects Who Lost and Did NotLose Warts in the Hypnotic and Placebo Conditions
Imagery vividnessImagined sensationsCURSS:OCURSS:SBetts imageryEstimated duration
M
4.1125.822.457.18
66.6486.64
Hypnosis
Lost
SD
1.0515.83
1.134.07
15.27135.97
Did not lose
M
2.7115.911.915.91
72.3663.55
SD
1.387.111.053.02
11.2852.66
M
—6.671.835.83
70.8352.83
Placebo
Lost
SD
7.911.471.60
10.0729.33
Did not lose
M
6.332.335.27
67.9466.68
SD
6,951.243.29
11.0248.63
Psychosomatic Medicine 50:245-260 (1988) 251

N. SPANOSetal.
lost fewer warts than hypnotic subjects andalso reported less intense experiencing ofsuggested sensations than did hypnoticsubjects. These findings may indicate thathypnotic subjects were more subjectivelyinvolved in their treatment than were pla-cebo subjects and that subjective involve-ment in the treatment process is helpfulin bringing about wart regression. Thefinding that placebo group subjects failedto differ significantly from controls in wartloss was somewhat surprising given thesignificant placebo effect reported byMemmesheimer and Eisenlohr (12). Per-haps our rather complicated "cold laser"placebo was simply less convincing thansuch relatively simple procedures as hav-ing medical personnel (instead of psy-chologists) paint the warts or inject sub-jects with innocuous substances definedas powerful wart medications. Futurestudies that employ a range of differentplacebo procedures, and that indepen-dently assess each procedure for believa-bility, might provide useful information.
In hypnotic subjects, wart regressioncorrelated significantly with the reportedvividness of suggested imagery and sug-gested sensations. Interestingly, in thesesame subjects wart regression failed to cor-relate significantly with either an attributemeasure of the propensity to imagine viv-idly (The Betts Questionnaire) or withhypnotizability dimension. These find-ings indicate that in the case of wartregression, situation specific indicators ofsubjects' cognitive involvements and mo-tivations may be better outcome predictorsthan global indexes of fantasy pronenessand suggestibility. The global indicatorsmay simply be too far removed from theparticular constellation of context specificmotivations, imaginings, and beliefs thatdetermine subjects' responses to the treat-ment suggestions. On the other hand, these
findings may simply point to limitationsin the particular indexes of imagery andhypnotizability employed in our study. Toexamine this possibility, our second ex-periment employed a second standardizedtest of hypnotizability and two differentattribute measures of imaginal activity.
Our finding that treatment effects werelarger for females than for males was sur-prising, because five previous studies (6,12, 13, 17, 22) found no sex differences inwart regression in subjects treated witheither hypnotic suggestion or placebo.Thus, our findings with respect to sex dif-ferences should be considered highly ten-tative until replicated.
Our finding that subjects with manywarts showed a better treatment responsethan those with only a few is consistentwith the results of at least two earlier stud-ies (12, 22). In one study (22), for example,30% of the 10 subjects with four or morewarts showed wart regression followinghypnotic treatment, while none of the 12subjects with three or fewer warts showedany treatment effect.
EXPERIMENT 2
A good deal of experimental work in-dicates that hypnotic and motivated non-hypnotic subjects respond equivalentlywhen given the same suggestions. Equiv-alent levels of responding in these twogroups have been found for suggestionsthat call for such varied responses as an-algesia, age-regression, hallucination, mo-toric and sensory alterations, and allergicreactions (for reviews, see 25, 26). Onlyone study (22) compared hypnotic andnonhypnotic subjects given the same sug-gestion for wart regression. Unfortunately,the number of subjects per treatment wassmall, a no-treatment control condition was
252 Psychosomatic Medicine 50:245-260 (1988)

HYPNOSIS IN WART TREATMENT
not employed, and very few subjects ineither treatment lost warts. Consequently,the results were ambiguous.
The major components in hypnotictreatments for wart regression usually in-clude the definition of the situation ashypnosis, the administration of an induc-tion procedure that emphasises relaxation,and suggestions to imagine the warts dis-appearing. In order to determine whetherdefining the situation as hypnosis or re-laxation facilitated any wart regression ef-fects produced by the suggestion alone, wecompared the following four conditions;a) hypnotic induction plus suggestion, b)the same suggestion preceeded by non-hypnotic relaxation instructions, c) thesuggestion alone, and d) a no-treatmentcontrol condition. Each subject was ad-ministered their treatment twice separatedby a 1-week interval. Following each treat-ment session, subjects rated the vividnesswith which they imagined the sensationssuggested to them their degree of relaxa-tion, and the extent to which they expe-rienced generalized alterations in con-sciousness (e.g., "I felt dazed," "time stoodstill"). A number of investigators (e.g., 27)have emphasized the importance of sub-jects' expectations of treatment success inbringing about wart regression. In fact, ithas been argued (27) that expectation isthe only important psychological media-tor of wart regression. Supposedly, otherpsychological variables (such as engagingin the suggested imagery) are importantonly to the extent that they bolster sub-jects' expectations of treatment success.Alternatively, other investigators havesuggested that subjects' expectations arelargely unrelated to treatment outcome andhave reported successful treatment inhighly skeptical subjects (e.g., 28, 29). Un-fortunately, no studies have systemati-cally assessed the relationship between
expectations and treatment outcome. Inorder to examine this issue, subjects in eachof our treatments estimated how effectivethey believed their treatment would be atremoving their warts.
At the end of the 6-week follow-up pe-riod, all subjects were tested on two dif-ferent hypnotizability scales and were ad-ministered Tellegen and Atkinson's (30)questionnaire measure of absorption inimaginative activities, as well as the ver-sion of the Betts' imagery questionnaireused in Experiment 1 (23).
METHODSubjects
Forty-five males and 31 females (ages 15-66 years)with warts on one or both hands were recruited forparticipation in a study on the psychological treat-ment of warts in the same manner as in Experiment1.
ProcedureSubjects were randomly assigned to four condi-
tions with 19 subjects in each condition. The fourconditions were a) the same hypnotic induction pro-cedure plus wart remission suggestion used in Ex-periment 1, b) the wart remission suggestion pre-ceeded by relaxation instructions in place of thehypnotic induction, c) the suggestion alone withoutpreliminary hypnotic or relaxation instructions, andd) no treatment control.
The relaxation instructions were modelled afterthe hypnotic instructions used in Experiment 1. Theywere the same length as the hypnotic instructions.However, they defined the situation as relaxationrather than hypnosis, and all references to drowsi-ness, sleep, and hypnosis were replaced with refer-ences to relaxation and comfort.
Subjects in the three treatment groups were ad-ministered their respective treatment procedurestwice, with a week separating the two administra-tions. Within each treatment, 11 subjects were ad-ministered the procedures by a male experimenter,and eight were administered them by a female ex-perimenter. Subjects in all conditions returned forfollow-up evaluation 6 weeks after their initial ses-
Psychosomatic Medicine 50:245-260 (1988) 253

N. SPANOS et al.
sion. In the first session, and again at the 6-weekfollow-up, subjects' warts were counted by a tech-nician who was blind to subjects' treatment assign-ment.
questionnaire assesses subjects' propensities for in-volvement in everyday fantasy (e.g., reading novels).
In-session QuestionnairesImmediately after each treatment procedure, sub-
jects were administered the following question-naires.
Intensity of Imagined Sensations. Subjects ratedthe extent to which they experienced each of the foursensations (i.e., tingling, warmth, shrinking, prick-ling) described in the suggestion. Each sensation wasrated on a 7-point scale, and the four sensation itemswere totaled to yield a single suggested vividnessscore.
Expectation of Treatment Success. Subjects re-sponded to the following item: "How effective do youthink this treatment will be at removing your warts?"Alternatives ranged from "not at all effective" (scored0) through "moderately effective" (scored 5) to "ex-tremely effective" (scored 10).
Altered Experience. Field (31) constructed a scaleto assess alterations in experience frequently asso-ciated with hypnotic induction (e.g., "I felt dazed").We modified the scale by eliminating all items thatmade explicit reference to sleep or hypnosis. Thirty-three items remained that tapped a range of altera-tions in body image, relaxation, and sensory expe-riences. All items were scored dichotomously andtotaled to yield a single altered experience score.
Relaxation. Subjects rated their degree of relaxa-tion on a six-item scale that was anchored with thedescriptors "very tense" (scored 1) at one end to "veryrelaxed" (scored 6) at the other end.
Measures Taken at Follow-upAfter their warts had been counted at the 6-week
follow-up, subjects were assessed for hypnotizabilityboth on the CURSS and on a 10-item version of theStanford Hypnotic Susceptibility Scale, Form C(SHSS : C) (32). This version of the SHSS :C has beenmodified in our laboratory to yield both an objectivemeasure (SHSS : C/O) and a subjective measure(SHSS : C/S) of hypnotizability (33). The CURSS andSHSS : C were administered at least 1 day apart incounterbalanced order. Before CURSS administra-tion subjects completed the version of the Betts im-agery scale used in Experiment 1. Before SHSS : Cadministration they completed Tellegen and Atkin-son's (30) questionnaire measure of absorption. This
RESULTS
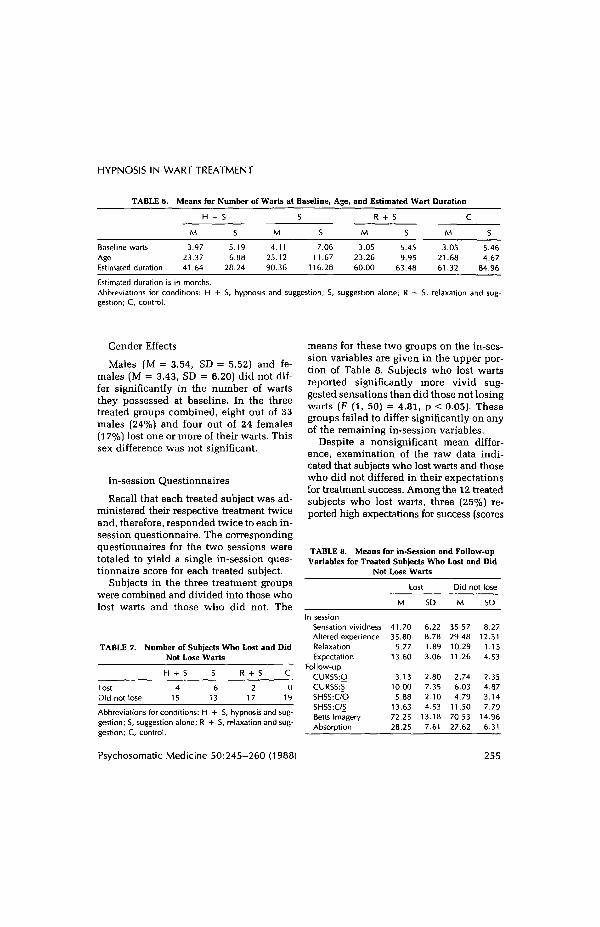
There were no significant treatmentdifferences in number of warts at base-line, F (3, 68) < 1. There were also nosignificant treatment differences in sub-jects' ages or in the estimated duration oftheir warts. The means involved in theseanalyses are given in Table 6.
Slightly more than half the subjects inthis experiment had only one wart at base-line (N = 39, 51.3%), and the large ma-jority had three or fewer warts at baseline(N = 64, 84.2%). Because the number ofwarts at baseline was so severely skewedtoward the low end, we measured wartloss exclusively in terms of our dichoto-mous lost one or more/lost none index.
Treatment Effects
Table 7 shows the number of subjectsin each condition who lost and who didnot lose warts. The four conditions dif-fered significantly in this regard (X2
(3) = 7.92, p < 0.05). Further analyses in-dicated that the three treated groups failedto differ significantly from one another.Furthermore, subjects in the three treatedgroups combined more frequently lost wartsthan did controls, X2 (1) = 4.75, p < 0.05.Hypnotic subjects taken alone more fre-quently lost warts than did controls, X2
(1) = 4.47, p < 0.05; and suggestion onlysubjects taken alone also more frequentlylost warts than did controls (X2 (1) = 7.12,p < 0.01). However, relaxation-plus-sug-gestion subjects failed to differ signifi-cantly from controls in this respect (X2
(1) = 2.11).
254 Psychosomatic Medicine 50:245-260 (1988)
HYPNOSIS IN WART TREATMENT
TABLE 6.
Baseline wartsAgeEstimated duration
Means for Number of Warts at Baseline,
H -
M
3.9723.3741.64
i/i
i/i
5.196.88
28.24
c
M
4.1125.1290.36
i/i
7.0611.67
116.28
Age, and Estimated Wart Duration
R + S
M
3.0523.2660.00
S
5.459.95
63.48
C
M
3.0521.6861.32
S
5.464.67
84.96
Estimated duration is in months.Abbreviations for conditions: H + S, hypnosis and suggestion; S, suggestion alone; R + S, relaxation and sug-gestion; C, control.
Gender Effects
Males [M = 3.54, SD = 5.52] and fe-males (M = 3.43, SD = 6.20) did not dif-fer significantly in the number of wartsthey possessed at baseline. In the threetreated groups combined, eight out of 33males (24%) and four out of 24 females(17%) lost one or more of their warts. Thissex difference was not significant.
In-session Questionnaires
Recall that each treated subject was ad-ministered their respective treatment twiceand, therefore, responded twice to each in-session questionnaire. The correspondingquestionnaires for the two sessions weretotaled to yield a single in-session ques-tionnaire score for each treated subject.
Subjects in the three treatment groupswere combined and divided into those wholost warts and those who did not. The
TABLE 7.
LostDid not lose
Number of Subjects Who Lost and DidNot Lose Warts
H + S S
4 615 13
R + S
217
C
019
means for these two groups on the in-ses-sion variables are given in the upper por-tion of Table 8. Subjects who lost wartsreported significantly more vivid sug-gested sensations than did those not losingwarts (F (1, 50) = 4.81, p < 0.05). Thesegroups failed to differ significantly on anyof the remaining in-session variables.
Despite a nonsignificant mean differ-ence, examination of the raw data indi-cated that subjects who lost warts and thosewho did not differed in their expectationsfor treatment success. Among the 12 treatedsubjects who lost warts, three (25%) re-ported high expectations for success (scores
TABLE 8. Means for in-Session and Follow-upVariables for Treated Subjects Who Lost and Did
Not Lose Warts
Lost Did not lose
Abbreviations for conditions: H + S, hypnosis and sug-gestion; S, suggestion alone; R + S, relaxation and sug-gestion; C, control.
In sessionSensation vividnessAltered experienceRelaxationExpectation
Follow-upCURSS:OCURSS:SSHSS:C/OSHSS:C/SBetts ImageryAbsorption
M
41.7035.80
9.7713.60
3.1310.005.88
13.6372.2528.25
SD
6.228.781.893.06
2.807.352.104.53
13.187.61
M
35.5729.4810.2911.26
2.746.034.79
11.5070.5327.62
SD
8.2712.31
1.154.53
2.354.873.147.79
14.966.31
Psychosomatic Medicine 50:245-260 (1988) 255

N. SPANOS et al.
of 8 or above) in at least one treatmentsession, and nine (75%) reported moderateexpectations (scores of 4-7). None of thesesubjects reported low expectations of suc-cess in either session (scores below 4). Onthe other hand, among the 45 treated sub-jects who failed to lose warts, the corre-sponding figures were 14 (31%) with highexpectations, 16 (36%) with with moder-ate expectations, and 15 (33%) with lowexpectations. In other words, subjects wholost warts and those who did not lose wartswere about equally likely to hold high ex-pectations for treatment success. How-ever, subjects who held very low expec-tations for treatment success never lost anywarts. This pattern of findings may indi-cate that suggestion-induced wart regres-sion is likely to occur only when subjectshold moderate-to-high expectations fortreatment success. However, positive ex-pectations, in and of themselves, provideno assurance that a treatment effect willoccur.
This pattern of findings is consistent withthe following hypothesis. Cognitive in-volvement in the suggested strategies fa-cilitates physiological processes that leadto wart regression. Subjects with low ex-pectations for treatment success are un-likely to initiate or become involved in thesuggested strategies, and consequently, areunlikely to lose warts. Subjects who de-velop high expectations for treatment suc-cess tend to lose warts if their high ex-pectations lead them to become involvedin the suggested strategies. However, sub-jects who cannot or will not develop suchinvolvements are unlikely to exhibit wartregression even when they hold relativelypositive expectations for treatment suc-cess. In order to test these ideas, we se-lected those subjects who held moderateor high expectations for treatment successbut did not lose warts (N = 30). These
subjects (M = 35.93, SD = 7.71) reportedsignificantly less vivid imagined sensa-tions than did the 12 subjects who lost allwarts (all of whom reported moderate orhigh expectations and whose vividnessscores are given in Table 8 (t (40) = 1.93,p < 0.02 one-tailed). In other words, whensubjects who lost and did not lose wartswere equated for expectations, those wholost warts indicated higher involvement inthe suggestion (reported more vivid sug-gested imagery) than those who did notlose warts.
Post-follow-up Variables
The bottom portion of Table 8 shows themeans on hypnotizability measures, Bettsimagery, and absorption for subjects wholost and did not lose warts. None of thesevariables differed significantly between thelost/did not lose groups.
Side-specific Treatment Effects
Recall that in both experiments, sub-jects with bilateral warts were given atreatment aimed at the warts on only onehand. In order to examine any selectiveeffect of the treatment on the target hand,we combined subjects from the two ex-periments who a) had bilateral warts, b)received a treatment, and c) lost at leastone wart from either hand. Fifteen subjectsmet all of these criteria. Twelve of thesesubjects (seven hypnotic, five placebo) werefrom Experiment 1, and three subjects (twohypnotic, one suggestion only) were fromExperiment 2.
Table 9 shows the number of warts eachof these subjects possessed at baseline onboth their treated and untreated hands, thenumber of warts lost from each hand, andthe percentage of warts lost from each hand.It is clear from this table that subjects tended
256 Psychosomatic Medicine 50:245-260 (1988)

HYPNOSIS IN WART TREATMENT
TABLE 9. Number of Warts and Number ofWarts Lost on Treated and Untreated Hands
Baseline numberof warts
Post-test—number lost(percent lost)
SS Treated Untreated Treated Untreated
112
382
2541
551222351
31
221
1012221252381
4 (36.4)2 (10.0)
10 (26.3)1 (50)
12 (48)7(17)1 (20)2 (40)1 (100)0(—)1 (50)2 (100)1 (33.3)0(—)1 (100)
1 (4.5)
2 (20)
1 (50)0(—)2(100)1 (20)2 (100)2 (66.6)3 (37.5)1 (100)
Ss 1-8 had more baseline warts on the treated hand. Ss9-15 had as many or more baseline warts on the un-treated as on the treated hand.
to have more baseline warts on the treatedthan on the untreated hands. Conse-quently, any tendency for subjects to losemore warts on the treated rather than theuntreated hand might be due to baselinedifferences rather than treatment specific-ity. We addressed this issue by dividingthese 15 subjects into those with morebaseline warts on the treated hand (N = 8)and those with an equal number or fewerbaseline warts on the treated than the un-treated hand (N= 7).
Subjects with more baseline warts onthe treated hand lost a significantly greaterpercentage of warts on the treated hand(M = 42.13, SD = 26.37) than on the un-treated hand (M = 9.25, SD = 17.85, F [1,7] = 8.71, p < 0.05). In fact, five of theseeight subjects (62.5%) lost warts exclu-sively on the treated hand, and none lostwarts exclusively on the untreated side.
Taken in isolation, these findings wouldsuggest a strong side-specific treatment ef-fect. However, in subjects who had at leastas many baseline warts on the untreatedas on the treated side, the "specificity ef-fect" disappeared. For these seven sub-jects, there was no significant differencein the percentage of warts lost from thetreated hand (M = 54.76, SD = 45.86) orfrom the untreated hand (M = 60.71,SD = 41.89, F (1, 6) < 1). Moreover, onlyone of these subjects (14%) lost warts ex-clusively from the treated hand, while twoof them (28%) lost warts exclusively fromthe untreated hand.
DISCUSSION
In Experiment 2 hypnotic subjects andsubjects given the suggestion alone wereequally likely to lose warts, and more likelyto lose warts, than no-treatment controlsubjects. These findings are consistent witha large body of data that indicates that hyp-notic and motivated nonhypnotic subjectsrespond similarly when they are admin-istered the same suggestions (25). Morespecifically, these findings indicate thatneither an hypnotic induction procedurenor instructions for relaxation enhance theefficacy of suggestions at inducing wartregression. From a practical perspective,the equivalent outcomes in the hypnotic-suggestion and suggestion-alone condi-tions indicate that therapists can offer psy-chological treatment for warts without ex-pending the extra time required to employhypnotic procedures, familiarize patientswith such procedures, divest patients offears and negative attitudes toward hyp-nosis, and so on.
Neither hypnotizability nor attributemeasures of imagery propensity predictedwart regression in either experiment. Ex-
Psychosomatic Medicine 50:245-260 (1988) 257

N. SPANOS et al.
periment 2 employed two different scalesto assess behavioral and subjective in-dexes of hypnotizability, and two differentattribute measures of imaginal propensity.Consequently, the failure of these vari-ables to predict treatment outcome cannotbe attributed to properties or deficienciesunique to one particular index of hypno-tizability or propensity for imagery. Morelikely, the failure of these indexes to pre-dict treatment outcome was related to theirlack of relevance to the treatment. Hyp-notizability and imaginal propensity werealways assessed at the end of the study.Consequently, the constellation of situa-tion-specific attitudes, expectations, andmotivations that influenced subjects' lev-els of responding to these postexperimen-tally administered indexes was probablyvery different from the constellation ofmotives and attitudes that determined theirpsychological response to the treatmentsuggestion.
Unlike the attribute indexes, subjects'ratings of suggested imagery vividnesscorrelated significantly with wart regres-sion. Interestingly, ratings of relaxation andof general alterations in experiences failedto predict wart regression. Thus, the extentto which subjects employed their imageryskills in the treatment context, for the spe-cific purpose called for by the suggestion,predicted treatment outcome. On the otherhand, subjects' propensities to imagine incontexts other than the treatment session(indexed by the attribute questionnaires),their propensities to subjectively and be-haviorally enact hypnotic responses in acontext unrelated to the treatment, and theirlikelihood of experiencing psychologicaleffects that were not directly called for bythe suggestion (i.e., relaxation, generalizedalterations in experience), were simply ir-relevant to treatment success. The findingthat degree of suggested imagery predicted
treatment outcome is open to at least twointerpretations. On the one hand, it maybe that imaginal processes are, for somereason, particularly important in initiatingor modulating the chain of physiologicalresponses that leads to wart regression. Al-ternatively, the important psychologicalvariable may not be imagery per se, butinstead subjects' degree of subjective in-volvement in a process that they considerto be therapeutic. In the present study, thesevariables were confounded. It would be ofinterest in a future study to compare animagery-suggestion treatment to some pro-cedure that encourages subjects' involve-ment in a wart-regression treatment thatdoes not involve generating wart-regres-sion imagery.
The finding in Experiment 2, that ex-pectations for treatment success failed topredict wart regression, contradicts thehypothesis that expectations of treatmentefficacy are the only important psycholog-ical factors in the induction of wart regres-sion (27). On the other hand, our findingthat subjects with low expectations fortreatment success never exhibited wartregression suggests that moderate-to-highexpectations of success may be necessarybut not sufficient for the production ofpsychologically induced wart regression.Psychologically induced wart regressionmay require the occurrence of cognitivefactors that are distinct from expectationsof treatment success, but that are more likelyto occur when subjects hold strong ratherthan weak expectations of success.
The combined findings of our two ex-periments, like most earlier findings, (7-9, 13, 22), provided no evidence for theoccurrence of a side-specific suggestion ef-fect in subjects with bilateral warts. In-stead, our findings suggest that the resultsof the one study (18) that reported such aneffect may have been artifactual. In that
258 Psychosomatic Medicine 50:245-260 (1988)
HYPNOSIS IN WART TREATMENT
study (18), suggestions were always aimed the suggestion was directed. These find-at the side of the body with the most warts, ings are consistent with the hypotheses thatOur subjects lost a significantly greater a) psychological factors induce or facili-percentage of warts on the treated side when tate some set of systemic physiologicalthe treated side had more warts than the processes that lead to wart regression, anduntreated side to begin with. However, b) large clusters of warts are more suscep-when the treated side had the same num- tible to the effects of these systemic pro-ber as or fewer warts than the untreated cesses than is a single or small number ofside, the percentage of warts lost on each warts,side was unrelated to the side toward which
REFERENCES
1. White DO, Fenner F: Medical Virology. New York, Academic Press, 19862. Allington HV: Review of the psychotherapy of warts. Arch Dermatol Syphilol 66:316-326,
19523. Vollmer H: Treatment of warts by suggestion. Psychosom Med 8:138-142, 19464. Zwick KG: Hygiogenisis of warts disappearing without topical medication. Arch Dermatol Syphilol
25:508-521, 19325. Ullman M: On the psyche and warts: I. Suggestion and warts, a review and comment. Psychosom Med
21:473-488, 19596. Ullman M, Dudek S: On the psyche and warts: II. Hypnotic suggestion and warts. Psychosom Med
22:68-76, 19607. Clarke GHV: The charming of warts. J Invest Dermatol 45:15-21, 19658. Stankler L: A critical assessment of the cure of warts by suggestion. Practitioner 198:690-694, 19679. Tenzel JH, Taylor RL: An evaluation of hypnosis and suggestion as treatment for warts. Psychosomatics
10:252-257, 196910. Massing AM, Epstein WL: Natural history of warts. Arch Dermatol 87:306-310, 196311. Rulison RH: Warts, a statistical study of 921 cases. Arch Dermatol Syphilol 46:66-81, 194212. Memmesheimer AM, Eisenlohr E: Untersuchungen uber die suggestive behandlung der warzen. Der-
matol Zeitchr 62:63-68, 193113. Surman OS, Gottlieb SK, Hackett TP, Silverberg EL: Hypnosis in the treatment of warts. Arch Gen
Psychiatry 28:439-441, 197314. Achterberg J: Imagery in healing. Boston, New Science Library, 198515. Barber TX: Changing "unchangeable" bodily processes by (hypnotic) suggestions: A new look at hyp-
nosis, cognitions, imagining, and the mind-body problem. In Sheikh AA (ed), Imagination and Healing.New York, Baywood, 1984
16. Spanos NP, Radtke HL, Hodgins DC, Stam HJ, Bertrand LD: The Carleton University Responsivenessto Suggestion Scale: Normative data and psychometric properties. Psychol Rep 53:523-535, 1983
17. Asher R: Respectable hypnosis. Br Med J 1:309-313, 196518. Sinclair-Gieben AHC, Chalmers D: Evaluation of treatment of warts by hypnosis, Lancet 11:480-482,
195919. Spanos NP, Hodgins DC, Stam HJ, Gwynn MI: Suffering for science: The effects of implicit social
demands on response to experimentally induced pain. J Per Soc Psychol 46:1162-1172, 198420. Spanos NP, Kennedy SK, Gwynn MI: The moderating effect of contextual variables on the relationship
between hypnotic susceptibility and suggested analgesia. J Abnorm Psychol 53:523-535, 198421. Wadden T, Anderton CH: The clinical use of hypnosis. Psychol Bull 91:215-243, 198222. Johnson RFQ, Barber TX: Hypnosis, suggestion and warts: An experimental investigation implicating
the importance of "believed in efficacy." Am J Clin Hypn 20:165-174, 1978
Psychosomatic Medicine 50:245-260 (1988) 259

N. SPANOS et al.
23. Shor RE, Orne MT, O'Connell DB: Psychological correlates of plateau hypnotizability in a specialvolunteer sample. J Person Soc Psychol 3:80-95, 1966
24. Barber TX: Hypnosis: A scientific approach. New York, Van Nostrand, 196925. Barber TX, Spanos NP, Chaves JF: Hypnosis imagination and human potentialities. New York, Perga-
mon, 197426. Spanos NP: A social psychological approach to hypnotic behavior. In Weary G, Mirels HR (eds),
Integrations of Clinical and Social Psychology. New York, Oxford, 198227. Kirsch I: Response expectancy as a determinant of experience and behavior. Am Psychol 40:1189-1202,
198528. Couper L, Davis T: A difficult wart treated by suggestion. Br Med J 2:1398, 195229. Sulzberger MB, Wolf J: The treatment of warts by suggestion. Med Rec 140-:552-557, 193430. Tellegen A, Atkinson G: Openness to absorbing and self-altering experiences ("absorption") a trait
related to hypnotic susceptibility. J Abnorm Psychol 83:268-277, 197431. Field P: An inventory scale of hypnotic depth. Inter J Clin Exper Hypn 13:238-249, 196532. Weitzenhoffer AM, Hilgard ER: The Stanford Hypnotic Susceptibility Scale, Form C. Palo Alto, Calif.
Consulting Psychologists Press, 196233. Spanos NP, Salas J, Menary EP, Brett PJ: A comparison of overt and subjective responses to the Carleton
University Responsiveness to Suggestion Scale and the Stanford Hypnotic Susceptibility Scale underconditions of group administration. Psychol Rep 58:847-856, 1985
260 Psychosomatic Medicine 50:245-260 (1988)