hypertension in the athletic population · proper measurement many factors can influence bp...
TRANSCRIPT
Hypertension in the Hypertension in the Athletic PopulationAthletic Population
Matthew Lewullis, DOMatthew Lewullis, DOMercy Sports MedicineMercy Sports Medicine
Norristown, PANorristown, PA
ObjectivesObjectives
Overview of hypertensionOverview of hypertensionProper blood pressure Proper blood pressure measurementmeasurementGuidelines for athletic Guidelines for athletic participationparticipation
AdultsAdultsChildren and AdolescentsChildren and Adolescents
MedicationsMedicationsBP measurement on the BP measurement on the sidelinesideline
PrevalencePrevalence
HTN affects approx. 60 HTN affects approx. 60 million Americansmillion AmericansMost common medical Most common medical issue in athletesissue in athletesReduce CAD, CVA, Reduce CAD, CVA, CHF, etc.CHF, etc.Improved detection, Improved detection, treatment, and control of treatment, and control of HTN in adults over the HTN in adults over the last 3 decadeslast 3 decades

Risk FactorsRisk Factors
Coronary artery diseaseCoronary artery diseaseCerebral vascular Cerebral vascular accidentaccidentCongestive heart failureCongestive heart failureAtrial fibrillationAtrial fibrillationLeft ventricular Left ventricular hypertrophyhypertrophyRetinal diseaseRetinal diseaseKidney diseaseKidney disease
Proper MeasurementProper Measurement
Many factors can influence BP measurementMany factors can influence BP measurementbladder distension, room temperature, recent exercise, bladder distension, room temperature, recent exercise, alcohol or nicotine, arm position, muscle tension, talking, alcohol or nicotine, arm position, muscle tension, talking, background noise, decongestants, caffeine, etc.background noise, decongestants, caffeine, etc.
Ideal to sit for 5 minutes prior to testingIdeal to sit for 5 minutes prior to testingRemove clothing, donRemove clothing, don’’t roll up the patientt roll up the patient’’s shirts shirtPatient comfortable in a chair with back and arm Patient comfortable in a chair with back and arm supportedsupportedMiddle of cuff at level of right atriumMiddle of cuff at level of right atrium
Middle of sternumMiddle of sternum
Proper MeasurementProper Measurement
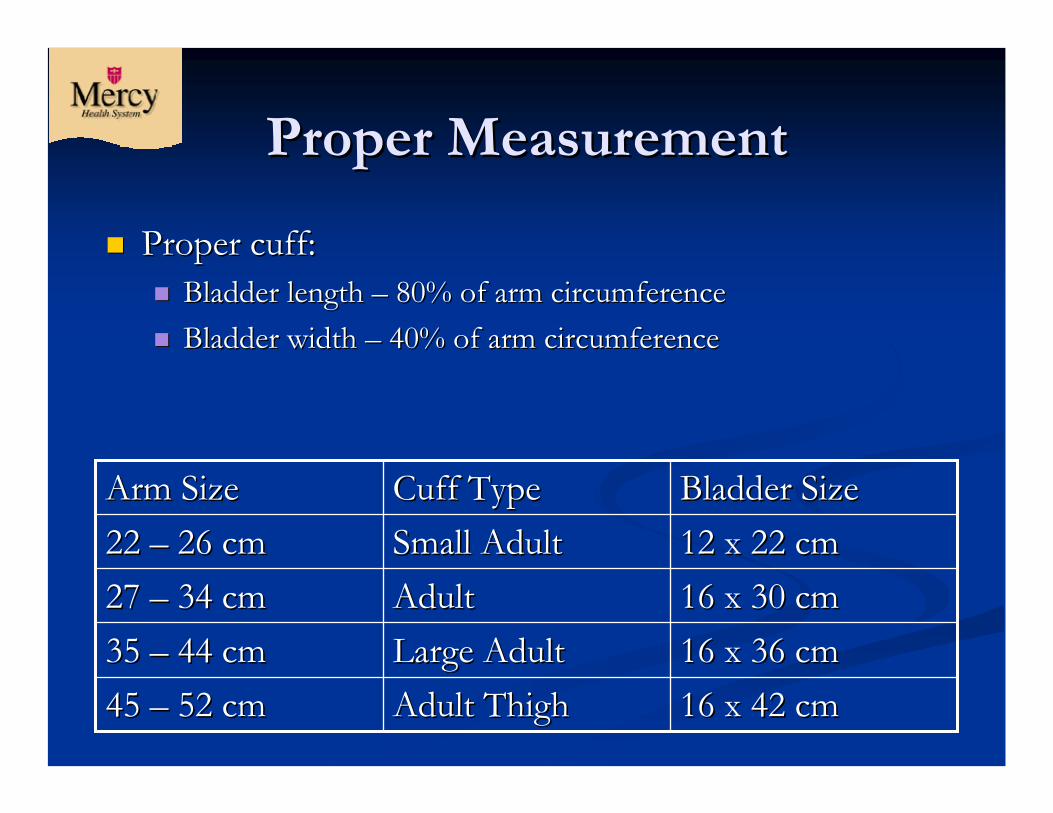
Proper cuff:Proper cuff:Bladder length Bladder length –– 80% of arm circumference80% of arm circumferenceBladder width Bladder width –– 40% of arm circumference40% of arm circumference
16 x 42 cm16 x 42 cmAdult ThighAdult Thigh45 45 –– 52 cm52 cm16 x 36 cm16 x 36 cmLarge AdultLarge Adult35 35 –– 44 cm44 cm16 x 30 cm16 x 30 cmAdultAdult27 27 –– 34 cm34 cm12 x 22 cm12 x 22 cmSmall AdultSmall Adult22 22 –– 26 cm26 cmBladder SizeBladder SizeCuff TypeCuff TypeArm SizeArm Size
Proper MeasurementProper Measurement
Inflate about 30 mmHg beyond disappearance Inflate about 30 mmHg beyond disappearance of the radial pulseof the radial pulseDeflate slowly at about 2Deflate slowly at about 2--3 mmHg3 mmHgAppearance of sound is systolicAppearance of sound is systolicDisappearance of sound is diastolicDisappearance of sound is diastolicPrecise BP is usually an average of multiple Precise BP is usually an average of multiple measurements over weeks or monthsmeasurements over weeks or months
GuidelinesGuidelines
The Seventh Report of the Joint National Committee The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC VII), August 2004.of High Blood Pressure (JNC VII), August 2004.The Fourth Report on the Diagnosis, Evaluation, and The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Treatment of High Blood Pressure in Children and Adolescents, September 1996, revised May 2005.Adolescents, September 1996, revised May 2005.36th Bethesda Conference: Recommendations for 36th Bethesda Conference: Recommendations for Determining Eligibility for Competition in Athletes Determining Eligibility for Competition in Athletes with Cardiovascular Abnormalities: Task Force 5: with Cardiovascular Abnormalities: Task Force 5: Systemic Hypertension, 2005.Systemic Hypertension, 2005.

JNC VIIJNC VII
Guidelines for adultsGuidelines for adultsNo specific indications or recommendations for No specific indications or recommendations for athletesathletes
≥≥100100≥≥160 or160 orHTN, Stage IIHTN, Stage II9090--9999140140--159 or159 orHTN, Stage IHTN, Stage I8080--8989120120--139 or139 orPrePre--hypertensionhypertension<80<80<120 and<120 andNormalNormalDiastolic BPDiastolic BPSystolic BPSystolic BPCategoryCategory
JNC VIIJNC VII
PrePre--hypertension, Stage I, II hypertension, Stage I, II –– lifestyle modificationslifestyle modificationsWeight reduction (BMI 18.5Weight reduction (BMI 18.5--24.9)24.9)DASH dietDASH dietSodium restriction (2.4g sodium)Sodium restriction (2.4g sodium)Aerobic physical activity (>30min/day, most days)Aerobic physical activity (>30min/day, most days)Moderation of alcohol consumptionModeration of alcohol consumption
Men (Men (≤≤2 drinks/day), Women (2 drinks/day), Women (≤≤1 drink/day)1 drink/day)
Stage I Stage I –– at least one medication, rec. thiazide type at least one medication, rec. thiazide type diuretics for most patients (HCTZ, Zaroxolyn, etc.)diuretics for most patients (HCTZ, Zaroxolyn, etc.)
JNC VIIJNC VII
Stage II Stage II –– 2 medications for most patients2 medications for most patientsCAD and CVA risk doubles for every 20/10 CAD and CVA risk doubles for every 20/10 increase in BP, starting at 115/75increase in BP, starting at 115/75Most patients require 2 or more medications to Most patients require 2 or more medications to reach goalreach goalEvaluation of HTN patient should at least Evaluation of HTN patient should at least include physical exam, electrocardiography, include physical exam, electrocardiography, urinalysis, kidney function, electrolytes, urinalysis, kidney function, electrolytes, cholesterol to assess for target organ damagecholesterol to assess for target organ damage
GuidelinesGuidelines
The Seventh Report of the Joint National Committee The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC VII), August 2004.of High Blood Pressure (JNC VII), August 2004.The Fourth Report on the Diagnosis, Evaluation, and The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Treatment of High Blood Pressure in Children and Adolescents, September 1996, revised May 2005.Adolescents, September 1996, revised May 2005.36th Bethesda Conference: Recommendations for 36th Bethesda Conference: Recommendations for Determining Eligibility for Competition in Athletes Determining Eligibility for Competition in Athletes with Cardiovascular Abnormalities: Task Force 5: with Cardiovascular Abnormalities: Task Force 5: Systemic Hypertension, 2005.Systemic Hypertension, 2005.
Children and AdolescentsChildren and Adolescents
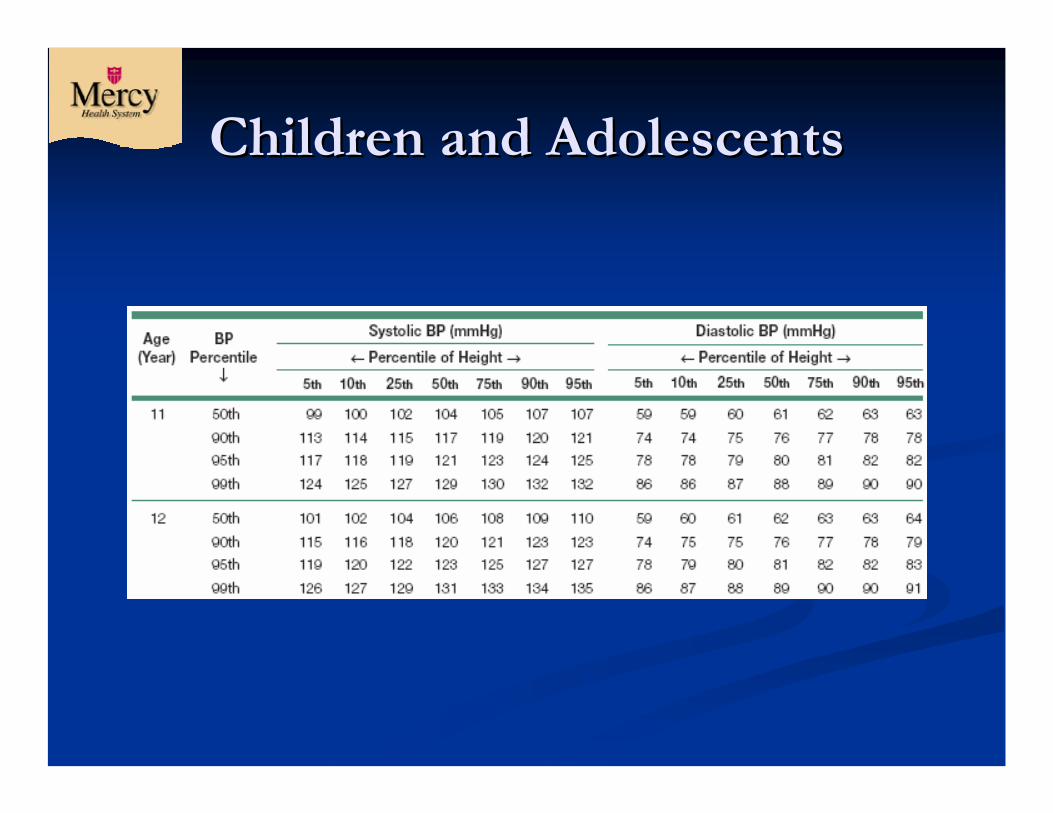
Classification stages Classification stages same as JNC VIIsame as JNC VIIBased on age, sex, and Based on age, sex, and percentile of heightpercentile of heightMore emphasis on More emphasis on detecting target organ detecting target organ damagedamage3 separate measurements 3 separate measurements to diagnose HTNto diagnose HTN
Children and AdolescentsChildren and Adolescents

Children and AdolescentsChildren and Adolescents
>99%+5 (SBP or DBP)>99%+5 (SBP or DBP)HTN, Stage IIHTN, Stage II
95%95%--99%+5 (SBP or DBP)99%+5 (SBP or DBP)HTN, Stage IHTN, Stage I
90%90%--95% (SBP or DBP)95% (SBP or DBP)PrePre--hypertensionhypertension
<90% (SBP and DBP)<90% (SBP and DBP)NormalNormal
BP percentileBP percentileCategoryCategory
Children and AdolescentsChildren and Adolescents
PrePre--hypertensionhypertensionWeight and diet management, introduce physical activityWeight and diet management, introduce physical activityMedicate if target organ damageMedicate if target organ damageReRe--check 6 monthscheck 6 months
Stage IStage IMedicate if symptomatic, target organ damage, 2Medicate if symptomatic, target organ damage, 2oo HTN, HTN, diabetes, or if fail abovediabetes, or if fail aboveReRe--check every 1check every 1--2 weeks2 weeks
Stage IIStage IIInitiate medical therapyInitiate medical therapy
Children and AdolescentsChildren and Adolescents
EvaluationEvaluationHistory, physical, BUN, creatinine, electrolytes, History, physical, BUN, creatinine, electrolytes, urinalysis, CBC, and urine cultureurinalysis, CBC, and urine cultureRenal ultrasoundRenal ultrasoundEchocardiogramEchocardiogramRetinal examRetinal examAmbulatory BP monitoring if suspected Ambulatory BP monitoring if suspected ““whitewhite--coat coat HTNHTN””
Children and AdolescentsChildren and Adolescents
ClearanceClearanceCompetitive sports participation should be restricted Competitive sports participation should be restricted only in the presence of uncontrolled Stage 2 HTN or only in the presence of uncontrolled Stage 2 HTN or target organ damage, until BP is normalized.target organ damage, until BP is normalized.
Recommend regular aerobic physical activity (30Recommend regular aerobic physical activity (30––60 60 minutes of moderate physical activity on most days) minutes of moderate physical activity on most days) and limitation of sedentary activities to less than 2 and limitation of sedentary activities to less than 2 hours per dayhours per dayWith the exception of power lifting, resistance training With the exception of power lifting, resistance training is beneficial.is beneficial.
GuidelinesGuidelines
The Seventh Report of the Joint National Committee The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC VII), August 2004.of High Blood Pressure (JNC VII), August 2004.The Fourth Report on the Diagnosis, Evaluation, and The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Treatment of High Blood Pressure in Children and Adolescents, September 1996, revised May 2005.Adolescents, September 1996, revised May 2005.36th Bethesda Conference: Recommendations for 36th Bethesda Conference: Recommendations for Determining Eligibility for Competition in Athletes Determining Eligibility for Competition in Athletes with Cardiovascular Abnormalities: Task Force 5: with Cardiovascular Abnormalities: Task Force 5: Systemic Hypertension, 2005.Systemic Hypertension, 2005.
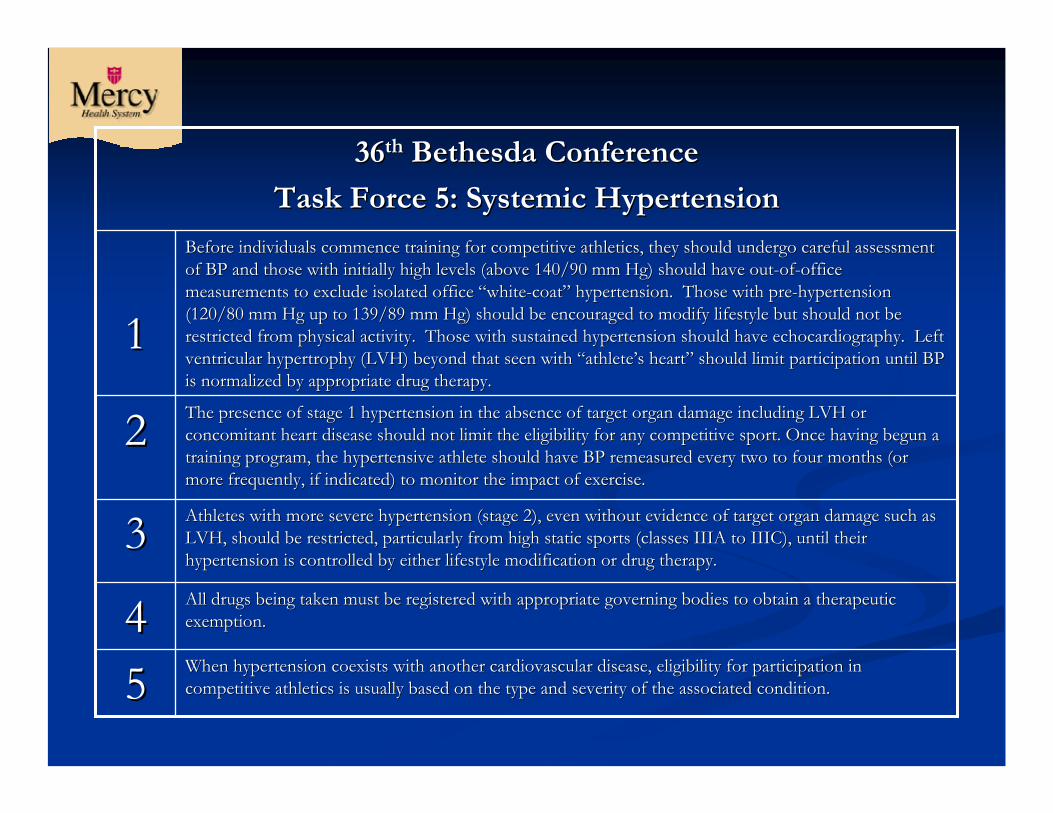
When hypertension coexists with another cardiovascular disease, When hypertension coexists with another cardiovascular disease, eligibility for participation in eligibility for participation in competitive athletics is usually based on the type and severity competitive athletics is usually based on the type and severity of the associated condition.of the associated condition.55
All drugs being taken must be registered with appropriate governAll drugs being taken must be registered with appropriate governing bodies to obtain a therapeutic ing bodies to obtain a therapeutic exemption.exemption.44
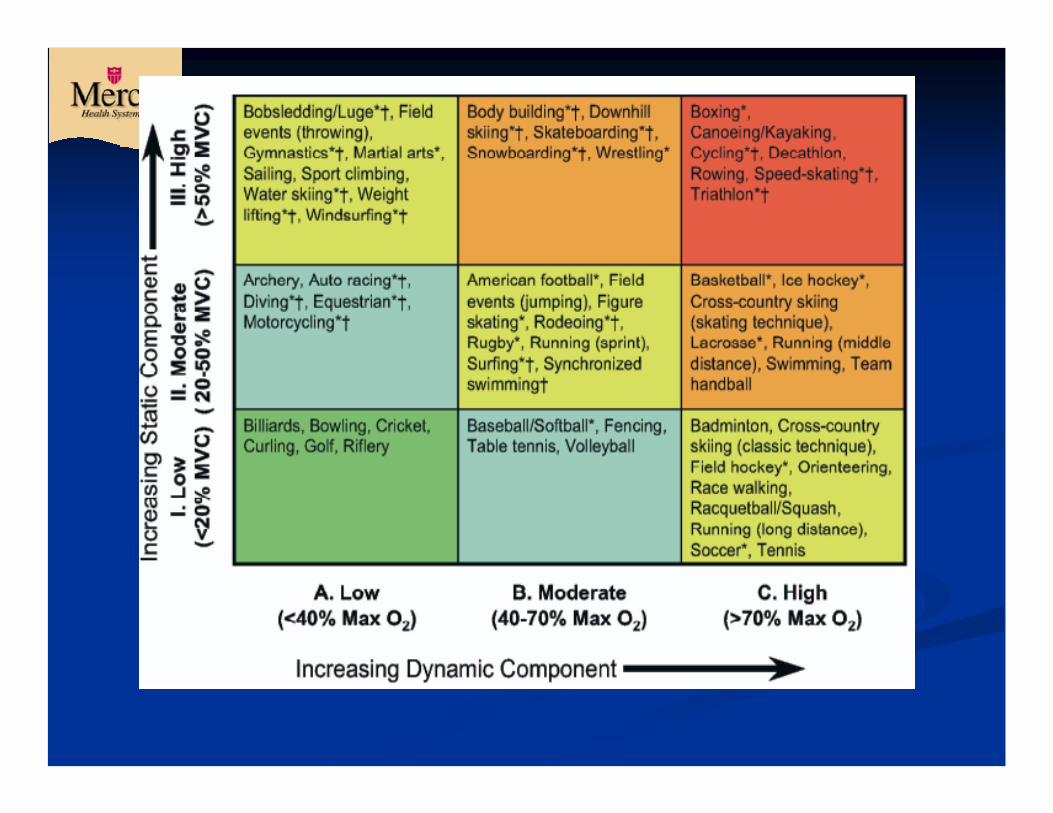
Athletes with more severe hypertension (stage 2), even without eAthletes with more severe hypertension (stage 2), even without evidence of target organ damage such as vidence of target organ damage such as LVH, should be restricted, particularly from high static sports LVH, should be restricted, particularly from high static sports (classes IIIA to IIIC), until their (classes IIIA to IIIC), until their hypertension is controlled by either lifestyle modification or dhypertension is controlled by either lifestyle modification or drug therapy.rug therapy.
33
The presence of stage 1 hypertension in the absence of target orThe presence of stage 1 hypertension in the absence of target organ damage including LVH or gan damage including LVH or concomitant heart disease should not limit the eligibility for aconcomitant heart disease should not limit the eligibility for any competitive sport. Once having begun a ny competitive sport. Once having begun a training program, the hypertensive athlete should have BP remeastraining program, the hypertensive athlete should have BP remeasured every two to four months (or ured every two to four months (or more frequently, if indicated) to monitor the impact of exercisemore frequently, if indicated) to monitor the impact of exercise. .
22
Before individuals commence training for competitive athletics, Before individuals commence training for competitive athletics, they should undergo careful assessment they should undergo careful assessment of BP and those with initially high levels (above 140/90 mm Hg) of BP and those with initially high levels (above 140/90 mm Hg) should have outshould have out--ofof--office office measurements to exclude isolated office measurements to exclude isolated office ““whitewhite--coatcoat”” hypertension. Those with prehypertension. Those with pre--hypertension hypertension (120/80 mm Hg up to 139/89 mm Hg) should be encouraged to modify(120/80 mm Hg up to 139/89 mm Hg) should be encouraged to modify lifestyle but should not be lifestyle but should not be restricted from physical activity. Those with sustained hyperterestricted from physical activity. Those with sustained hypertension should have echocardiography. Left nsion should have echocardiography. Left ventricular hypertrophy (LVH) beyond that seen with ventricular hypertrophy (LVH) beyond that seen with ““athleteathlete’’s hearts heart”” should limit participation until BP should limit participation until BP is normalized by appropriate drug therapy.is normalized by appropriate drug therapy.
11
3636thth Bethesda ConferenceBethesda Conference
Task Force 5: Systemic HypertensionTask Force 5: Systemic Hypertension
3636thth Bethesda ConferenceBethesda Conference
Untreated hypertension in athletes may be accompanied by some limitation in exercise performance.Tobacco, excess alcohol, sympathomimetics, cocaine, ephedra, androgens, steroids, growth hormone, NSAIDs, and excessive sodium intake may all increase BP.
PPE Monograph, 3PPE Monograph, 3rdrd EditionEdition
Based on 1996 information for Based on 1996 information for children and adolescentschildren and adolescentsBased on 26Based on 26thth Bethesda ConferenceBethesda ConferenceSums up recommendations for Sums up recommendations for athletes of all age groups at time of athletes of all age groups at time of preparticipation examinationpreparticipation examination
PPE Monograph, 3PPE Monograph, 3rdrd EditionEdition
Restrict from play if:Restrict from play if:Adult with stage IIAdult with stage IIChild with >99%Child with >99%Concern that target organ damage Concern that target organ damage existsexistsSecondary cause of HTN is suspectedSecondary cause of HTN is suspected
Otherwise, may clear to participate Otherwise, may clear to participate while being further evaluatedwhile being further evaluated
MedicationsMedications
Lifestyle modificationsAll antihypertensive drugs may limit exercise capacity.Most patients require at least 2 medications for controlBeta-blockers (metoprolol, atenolol)
Decrease HR and heart contractilityDecrease HR and heart contractilityBanned in shooting, archery, diving, etc.Banned in shooting, archery, diving, etc.
ACE Inhibitors (lisinopril, enalapril)ACE Inhibitors (lisinopril, enalapril)Electrolyte imbalance, coughElectrolyte imbalance, cough
Diuretics (HCTZ, furosemide)Diuretics (HCTZ, furosemide)Electrolyte imbalance, dehydrationElectrolyte imbalance, dehydrationBanned in USOC and NCAABanned in USOC and NCAA
MedicationsMedications
Alpha blockers (terazosin, Alpha blockers (terazosin, clonidine)clonidine)
Orthostatic hypotensionOrthostatic hypotensionARBs (losartan, olmesartan)ARBs (losartan, olmesartan)
Cough, electrolyte imbalanceCough, electrolyte imbalanceNondihydropyridine Nondihydropyridine CalciumCalcium--channel blockerschannel blockers
(diltiazem, verapamil) can (diltiazem, verapamil) can lower HRlower HR
Dihydropyridine CCBs Dihydropyridine CCBs (amlodipine, isradipine )(amlodipine, isradipine )
Swelling, dizzinessSwelling, dizziness
BP on the SidelinesBP on the Sidelines
Orthostatics, Tilt testingOrthostatics, Tilt testingCheck BP and HR supine, then check BP and HR Check BP and HR supine, then check BP and HR standing at 1 minute and 3 minutesstanding at 1 minute and 3 minutesHypovolemia if:Hypovolemia if:
SBP decreases SBP decreases ≥≥20mmHg, DBP decreases 20mmHg, DBP decreases ≥≥10 mmHg, or 10 mmHg, or HR increases HR increases ≥≥10 bpm10 bpm
Useful for syncope, possible internal bleeding, Useful for syncope, possible internal bleeding, dehydration, medication relateddehydration, medication related
Thank youThank you
Websites of InterestWebsites of Interest
http://http://www.nhlbi.nih.gov/health/prof/heart/hwww.nhlbi.nih.gov/health/prof/heart/hbp/hbp_ped.pdfbp/hbp_ped.pdfhttp://www.csmfoundation.org/36th_Bethesdahttp://www.csmfoundation.org/36th_Bethesda_Conference__Conference_--_Eligibility_Recommendations_for_Athletes_wi_Eligibility_Recommendations_for_Athletes_with_Cardiac_Abnormalities.pdfth_Cardiac_Abnormalities.pdfhttp://www.nhlbi.nih.gov/guidelines/hypertenshttp://www.nhlbi.nih.gov/guidelines/hypertension/jnc7full.pdfion/jnc7full.pdf

ReferencesReferences
Chobanian AV, Bakris GL, Black HR et al: The Chobanian AV, Bakris GL, Black HR et al: The seventh report of the Joint National Committee seventh report of the Joint National Committee on prevention, detection, evaluation, and on prevention, detection, evaluation, and treatment of High blood pressure: the JNC 7 treatment of High blood pressure: the JNC 7 report. JAMA 2003;289:2560report. JAMA 2003;289:2560--72.72.National High Blood Pressure Education National High Blood Pressure Education Program Working Group on High Blood Program Working Group on High Blood Pressure in Children and Adolescents. Pediatrics Pressure in Children and Adolescents. Pediatrics 2004; 114 Suppl: 5552004; 114 Suppl: 555--76.76.
ReferencesReferences
Kaplan NM, Gidding SS, Pickering TG, et al: 36th Bethesda Kaplan NM, Gidding SS, Pickering TG, et al: 36th Bethesda Conference: Recommendations for Determining Eligibility for Conference: Recommendations for Determining Eligibility for Competition in Athletes with Cardiovascular Abnormalities: Competition in Athletes with Cardiovascular Abnormalities: Task Force 5: Systemic Hypertension. Journal of the American Task Force 5: Systemic Hypertension. Journal of the American College of Cardiology 2005, 45 (8):1346College of Cardiology 2005, 45 (8):1346--8.8.Pickering TG, Hall JE, Appel LJ, Falkner BE, Graves J, Hill MN, Pickering TG, Hall JE, Appel LJ, Falkner BE, Graves J, Hill MN, Jones DW, Kurtz T, Sheps SG, Roccella EJ. Recommendations Jones DW, Kurtz T, Sheps SG, Roccella EJ. Recommendations for blood pressure measurement in humans and experimental for blood pressure measurement in humans and experimental animals: Part 1: blood pressure measurement in humans: a animals: Part 1: blood pressure measurement in humans: a statement for professionals from the Subcommittee of statement for professionals from the Subcommittee of Professional and Public Education of the AHA Council on HBP. Professional and Public Education of the AHA Council on HBP. CirculationCirculation 2005 Feb 8;111(5):6972005 Feb 8;111(5):697--716. 716.
ReferencesReferences
American Academy of Family Physicians, American American Academy of Family Physicians, American Academy of Pediatrics, American College of Sports Academy of Pediatrics, American College of Sports Medicine, American Medical Society for Sports Medicine, American Medical Society for Sports Medicine, American Osteopathic Academy of Sports Medicine, American Osteopathic Academy of Sports Medicine. Preparticipation Physical Examination. 3rd Medicine. Preparticipation Physical Examination. 3rd ed. Minneapolis, MN: McGraw Hill; 2005.ed. Minneapolis, MN: McGraw Hill; 2005.OO’’Connor MD, F. Hypertension, Athletes and the Connor MD, F. Hypertension, Athletes and the Sports Physician:Sports Physician: Implications of JNC VII, The Fourth Implications of JNC VII, The Fourth Report, and the 36th Bethesda Conference Guidelines. Report, and the 36th Bethesda Conference Guidelines. AMSSM, Albuquerque, NM, 2007.AMSSM, Albuquerque, NM, 2007.