hypertension 2017: the times and guidelines are...
TRANSCRIPT

Emerging Challenges in Primary Care:
2017
Hypertension 2017: The Times and
Guidelines Are Changing
1

Faculty
§ Jan Basile, MDProfessor of MedicineSeinsheimer Cardiovascular Health ProgramDivision of General Internal MedicineMedical University of South CarolinaRalph H. Johnson VA Medical CenterCharleston, SC
2

§ Jan Basile, MD serves on the speakers bureau for Amgen, Arbor, and Janssen. Dr. Basile also serves as a consultant for Novartis, Medtronic, and Up-to-date.
3
Disclosures
3

Learning Objectives:§ Recognize the evolving epidemiology and
improvements in control rates of hypertension.§ Review proper blood pressure (BP)
measurement technique and the role of office, home, and 24-hr Ambulatory BP measurement in the diagnosis and treatment of hypertension.
§ Recognize current recommendations for first- line agents in the treatment of hypertension.
§ Discuss the impact of recent trials and recommendations on evolving BP treatment goals for individualized therapy.

PRE-TEST QUESTIONS
55

Recent BP Control Rates (< 140/90 mm Hg) in a the Kaiser Permanente Health Care System Has Been As High As:
Pre-test ARS Question 1
1. 95%2. 80%3. 70%4. 50%5. I am unsure

The BP Measurement that correlates least with Clinical Outcome is the:
Pre-test ARS Question 2
1. Nighttime BP2. Daytime BP3. 24-hour BP4. Office BP5. None of the above
Recently recommended systolic BP targets in different populations at risk include all of the following except:
1. <150 mmHg2. <140 mmHg3. <130 mmHg4. <120 mmHg5. <110 mm Hg
Pre-test ARS Question 3

The thiazide/thiazide-like diuretic with the shortest half life is:
1. Hydrochlorthiazide2. Indapamide3. Chlorothalidone4. Metolazone5. They all have the same half-life
Pre-test ARS Question 4
Choose the Best Answer:According to JNC 8, which of the following antihypertensive drug classes is not appropriate for initial use in an uncomplicated hypertensive patient?
1. Calcium Channel Blocker2. Thiazide-type diuretic3. Beta-blocker4. ACE Inhibitor or ARB5. None of the above
Pre-test ARS Question 5

Educational Objective #1
Recognize the evolving epidemiology and improving control rates of hypertension.

The Impact of Hypertension
Mozzafarian D et al. Circulation 2015; 131: e29-322. Roger VL, et al. Circulation. 2012;125:e2–e220. Rapsomaniki, E et al. Lancet. 2014;/383:1899-1911. May 31, 2014
- Approximately 69% of people who have a first heart attack, 77% of those who have a first stroke, and 74% of those who have HF have a BP >140/90 mm Hg - HTN contributes to 360,000 deaths each year in the US - Poor Medication Adherence is a major barrier to effective BP control as only about 57% remain adherent to their BP medication at 2 years follow-up
- 1 in 3 US adults > 20 years of age have hypertension
- HTN is associated with shorter overall life expectancy cutting about 5 years of life compared to normotensive adult men and women

Awareness, Treatment, and Control of HBP by Race/Ethnicity NHANES: 2007–2012
Mozzafarian D et al. Circulation 2016; 131: e38-360.
White Black
Hisp

Kaiser Permanente Hypertension Control Rates 2001-2009
KPNC=Kaiser Permanente Northern California HEDIS=Healthcare Effectiveness Data and Infomation Set JAMA. 2013 Aug 21; 310(7): 699–705

Management of Adult Hypertension1
1.
If ACEI intolerant or pregnancy potential
Calcium Channel Blocker
Add amlodipine 5 mg X ½ daily à 5 mg X 1 daily à 10 mg daily
Beta-Blocker OR Spironolactone
Add atenolol 25 mg daily à 50 mg daily (Keep heart rate > 55) OR
IF on thiazide AND eGFR ≥ 60 ml/min AND K < 4.5 Add spironolactone 12.5 mg daily à 25 mg daily
If not in control
If not in control
If not in control
Thiazide Diuretic
Chlorthalidone 12.5 mg à 25 mg
OR HCTZ 25 mg à 50 mg
If not in control
ACE-Inhibitor2 / Thiazide Diuretic
Lisinopril / HCTZ
(Advance as needed) 20 / 25 mg X ½ daily 20 / 25 mg X 1 daily 20 / 25 mg X 2 daily
Pregnancy Potential: Avoid ACE-Inhibitors2
Kaiser Permanente Hypertension Algorithm
Go,AS et al J Am Coll Cardiol. 2013
BP Goal < 140/90 mm Hg

Aspects of a Capitated Health Care System and Improved BP Control Rates
1. Access 2. Formulary Availability 3. More Frequent Follow-up with In-House
Laboratory 4. Best Electronic Health Record with Evidence-
Based Metrics 5. Pay for Performance 6. Nurse and Pharmacist-Managed Clinics

Educational Objective #2
Review proper blood pressure (BP) measurement technique and the role of office, home, and 24-hr Ambulatory BP measurement in the diagnosis and treatment of hypertension.

Limitations of Office Blood Pressure Measurement
• Insufficient number of readings plus an inherent variability of blood pressure in the office
• Poor technique (e.g., operator use and equipment status)
• White coat effect
• Masked effect
CHALLENGES TO ACCURATE OFFICE BLOOD PRESSURE MEASUREMENTS
Pickering TG, White W. J Clin Hypertens. 2008;10:850–855.
Chobanian AV et al. Hypertension. 2003;42:1206–1252; Izzo JL, Sica DA, Black HR, eds. Hypertension Primer: The Essentials of High Blood Pressure. 4th ed. Philadelphia: 2008:335–338.
Poor BP Measurement Technique May Be Associated with Elevated BP in the Office

Devices
BPTru, Omron HEM-907, Welch Allyn PRO BP 2400 Myers MG. et al. Hypertension 2010;55:195-200.
Automated Oscillometric
BP Device
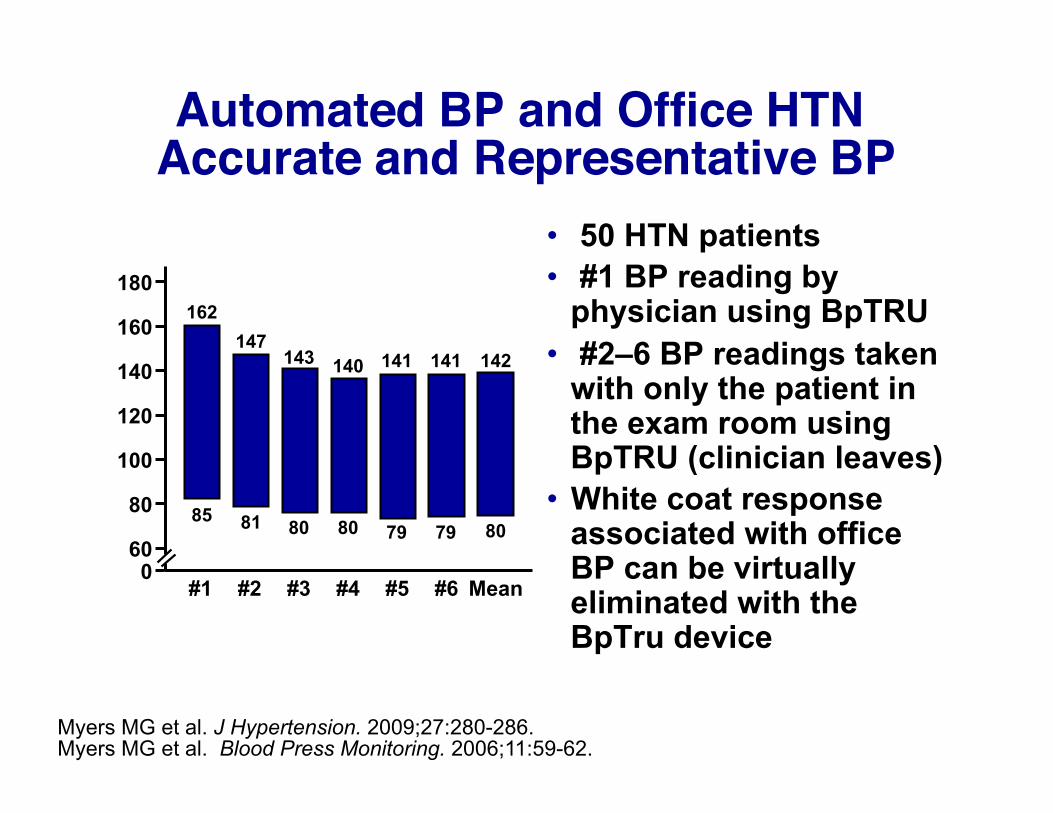
Automated BP and Office HTN Accurate and Representative BP
• 50 HTN patients • #1 BP reading by
physician using BpTRU • #2–6 BP readings taken
with only the patient in the exam room using BpTRU (clinician leaves)
• White coat response associated with office BP can be virtually eliminated with the BpTru device
Myers MG et al. J Hypertension. 2009;27:280-286. Myers MG et al. Blood Press Monitoring. 2006;11:59-62.
180
160
140
120
100
80
60 0
#1 #2 #3 #4 #5 #6 Mean Automated (BpTRU) Readings
Blo
od P
ress
ure
(mm
Hg)
85
162
81
147
80
143
80
140
79
141
79
141
80
142

BP Measurement in the Office in Established Patient
1. Preferably taken before the patient ever sees the clinician caring for the patient
2. - 5 minutes of rest-(built into the device to wait 5 min) - no conversation - seated comfortably with feet on the floor - arm at heart level - no tobacco or caffeine for 30 minutes before BP - have the examiner leave the room
3. Two to Three seated readings taken 1 minute apart (averaged) using an automated oscillometric BP device (AOBP)
4. An upright reading (after 1 minute of quiet standing)

The Concept of White-Coat and Masked Hypertension
Office
135 True
Normotensive
True Hypertensive
White Coat HTN
Home or Day<m
e AB
PM
SBP
mmHg
135
140
140
Derived from Pickering et al. Hypertension 2002:40:795-796
Office Measurement SBP mmHg
Home or Day<m
e ABPM
Masked Hypertension

Office, 24-hr, Daytime and Night-time SBP as Predictors of Cardiovascular Endpoints – Syst-Eur
Systolic blood pressure (mm Hg)
2-yr
inci
denc
e of
ca
rdio
vasc
ular
end
poin
ts 0.20
0.16
0.12
0.08
0.04
0.00
90 110 130 150 170 190 210 230
Nighttime 24-hr Daytime Conventional (office)
Staessen JA et al. JAMA. 1999;282:539-46.
Conclusion:Non-Office
SBP: A Better
Predictor of CV Events
than Office BP

Out-of-Office Blood Pressure Measurement
Use and Advantages: • Helps identify WCH and masked hypertension • Multiple readings throughout the day may reveal patterns in
blood pressure and periods when control is inadequate • Improves patient adherence • Reduces costs • Take readings 1 week per month, 2 readings in the am and pm,
throw out the first day and get 24 values for a week q month
Pickering TG, White W. J Clin Hypertens. 2008;10:850–855; Izzo JL, Sica DA, Black HR, eds, and the Council for High Blood Pressure Research (American Heart Association). Hypertension Primer: The Essentials of High Blood Pressure. 4th ed. Philadelphia: Lippincott Williams & Wilkins; 2008:339–342.
• Provides a better risk prediction than office-based monitoring
• Correlates better with the cardiac (LVH) and renal (albuminuria) consequences of hypertension than office readings
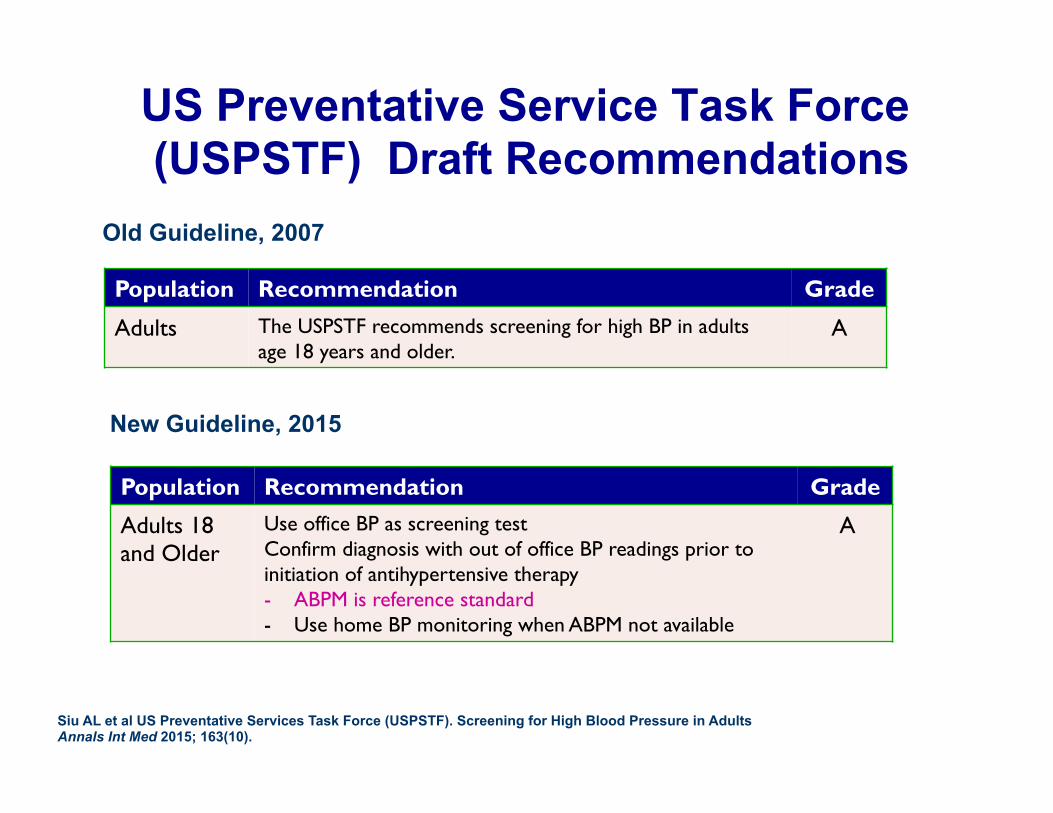
US Preventative Service Task Force (USPSTF) Draft Recommendations
Population Recommendation Grade
Adults The USPSTF recommends screening for high BP in adults age 18 years and older.
A
Population Recommendation Grade
Adults 18 and Older
Use office BP as screening test Confirm diagnosis with out of office BP readings prior to initiation of antihypertensive therapy - ABPM is reference standard - Use home BP monitoring when ABPM not available
A
Old Guideline, 2007
New Guideline, 2015
Siu AL et al US Preventative Services Task Force (USPSTF). Screening for High Blood Pressure in Adults Annals Int Med 2015; 163(10).

Why Is It That We Continue To Deny Our Patients Ambulatory Blood Pressure Monitoring
ABPM recommended to confirm the diagnosis of hypertension by:
1. USPSTF (2015) 2. Canadian Hypertension Education Program
2016 (CHEP) 3. NICE British 2011 4. European Society of Hypertension Position
Paper on ABPM-2013
O’Brien Eon. Hypertension. 2016;67:00-00. DOI: 10.1161/HYPERTENSIONAHA.115.06777.)

Ambulatory BP monitoring
• Multiple readings over the course of 24 hours
• Superior to office BP in predicting outcomes
• Considered to be the noninvasive gold standard

Educational Objective #3
Recognize Current First-Line Antihypertensive Agents in the
Treatment of hypertension.

Development of HTN Guidelines: The JNCs and Initial Drug Therapy
43 drugs Low-dose diuretics, β-blockers
added
JNC III
1972
NHBPEP starts
Earliest guidelines
28 drugs DBP ≥105 diuretics
JNC I JNC II
34 drugs diuretics
JNC IV
50 drugs ACEI, CAs
added
JNC VI
84 drugs 7 options
68 drugs diuretics/ β-blockers
JNC V JNC 7
>125 drugs diuretics
(ALLHAT)
8th report
December 18, 2013
1976
1980
1984
1988
1993
1997 2003 2013 1973

Initial Medications For The Management of Hypertension
Thiazide
Thiazide-Type
Diuretics
ACE inhibitors or
ARBs Calcium
antagonists
Lifestyle Modification—Especially Diet and Exercise
2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report From the Panel Members Appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014; 311(5): 507-520. Feb 5, 2014

Years to CHD Event 0 1 2 3 4 5 6 7
Cum
ulat
ive
CH
D E
vent
Rat
e
0
0.04
0.08
0.12
0.16
0.20 RR (95% CI) p value
A/C 0.98 (0.90–1.07) 0.65
L/C 0.99 (0.91–1.08) 0.81
Chlorthalidone Amlodipine Lisinopril
Cumulative Event Rates for the Primary Outcome (Fatal CHD or Non-fatal MI) by ALLHAT Treatment
Group
ALLHAT Collaborative Research Group. JAMA. 2002;288:2981–2997.

ADA 2017: Hypertension (HTN) Managment
§ Previously ACE Inhibitors or ARBs were 1st-line recommendations for HTN management
§ Expansion of recommended anti-hypertensives w/o clinical proteinuria to include thiazide diuretics or DHP-CCBs as 1st-line agents
§ The BP goal in Diabetes is < 140/90 mm Hg § Consideration of empagliflozin or liraglutide for
certain high-risk individuals ADA Standards of Medical Care in Diabetes. Diabetes Care 2017; 40 (Suppl.1):S75-S87.

§ The available evidence does not support the use of beta-blockers as first-line drugs in the treatment of hypertension.
Cochrane Review:Beta-blockers should not be first line for
hypertension
Cochrane Database of Systematic Reviews. Published by John Wiley & Sons, Ltd. January 24, 2007.

ASCOT-BPLA ELSA INVEST LIFE MRC Old UKPDS Total events
0.5 0.7 1 1.5 2
Atenolol Other drug RR RR (n/N) (n/N) (95% Cl) (95% Cl)
422/9618 14/1157
201/11309 309/4588
56/1102 17/358
1019/28132
327/9639 9/1177
176/11267 232/4605
45/1081 21/400
810/28169
1.29 (1.12–1.49) 1.58 (0.69–3.64) 1.14 (0.93–1.39) 1.34 (1.13–1.58) 1.22 (0.83–1.79) 0.90 (0.48–1.69) 1.26 (1.15–1.38)
Favors atenolol
Favors other drug
β-Blocker Meta-analysis Stroke: Atenolol vs Other Antihypertensive Agents
ASCOT-BPLA, Anglo-Scandinavian Cardiac Outcomes Trial–Blood Pressure Lowering Arm; CI, confidence interval; ELSA, European Lacidipine Study on Atherosclerosis; INVEST, International Verapamil-Trandolapril Study; LIFE, Losartan Intervention For Endpoint reduction; MRC, Medical Research Council; RR, relative risk; UKPDS, United Kingdom Prospective Diabetes Study.
Lindholm LH et al. Lancet. 2005;366(9496):1545-1553.

Educational Objective #4
Discuss the impact of recent trials and recommendations on evolving BP treatment goals for individualized therapy.
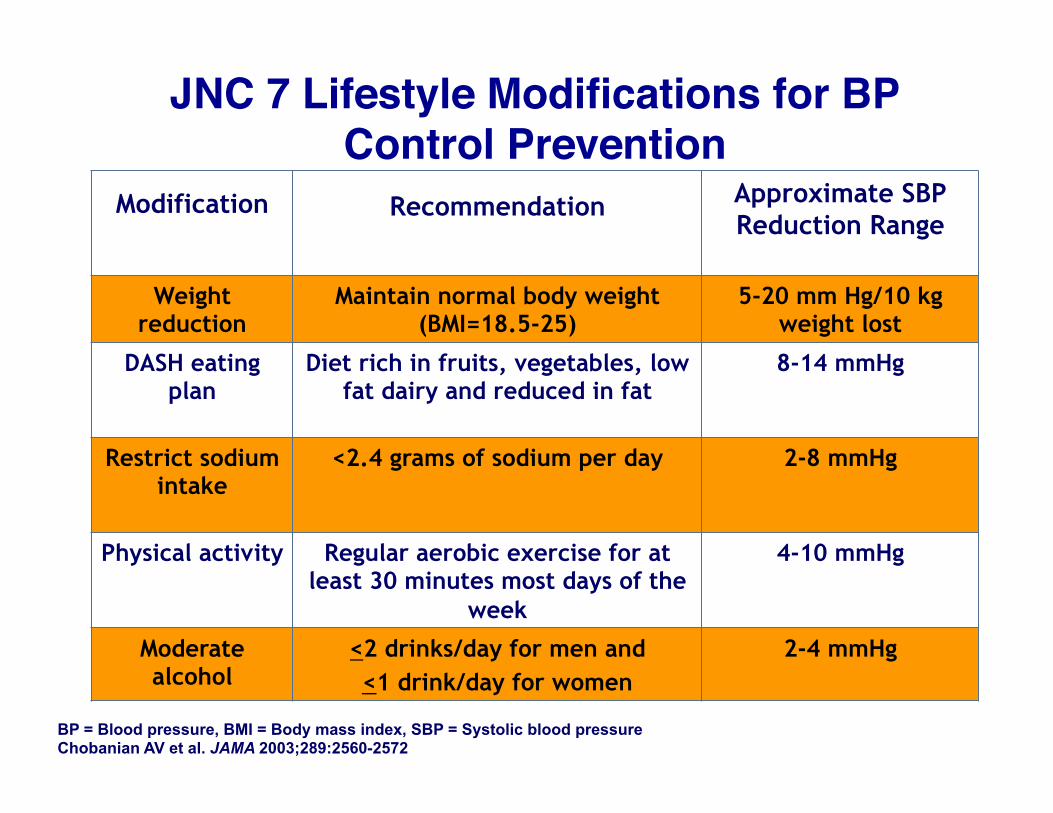
JNC 7 Lifestyle Modifications for BP Control Prevention
Modification Recommendation Approximate SBP Reduction Range
Weight reduction
Maintain normal body weight (BMI=18.5-25)
5-20 mm Hg/10 kg weight lost
DASH eating plan
Diet rich in fruits, vegetables, low fat dairy and reduced in fat
8-14 mmHg
Restrict sodium intake
<2.4 grams of sodium per day 2-8 mmHg
Physical activity Regular aerobic exercise for at least 30 minutes most days of the
week
4-10 mmHg
Moderate alcohol
<2 drinks/day for men and <1 drink/day for women
2-4 mmHg
BP = Blood pressure, BMI = Body mass index, SBP = Systolic blood pressure Chobanian AV et al. JAMA 2003;289:2560-2572

Stage 1 Hypertension (SBP 140–159 or DBP 90–99 mmHg)
Thiazide-type diuretics for most May consider ACEI, ARB,
β-blocker, CCB, or combination
In Patients With Hypertension
INITIAL DRUG CHOICES
LIFESTYLE MODIFICATIONS
Not at Goal Blood Pressure (<140/90 mmHg) (<130/80 mmHg for those with diabetes or CKD)
Optimize dosages or add additional drugs until goal blood pressure is achieved Consider consultation with hypertension specialist
Drug(s) for the compelling indications Other antihypertensive drugs
(diuretics, ACEI, ARB, β-blocker, CCB) as needed
Not at Goal Blood Pressure
In Patients With Compelling Indications Related to Hypertension
Stage 2 Hypertension (SBP >160 or DBP >100 mmHg)
2-drug combination for most (usually thiazide-type diuretic and ACEI or ARB or β-blocker or CCB)
Management of Blood Pressure-JNC 7
Adapted from Chobanian AV et al. Hypertension. 2003;42:1206–1252.
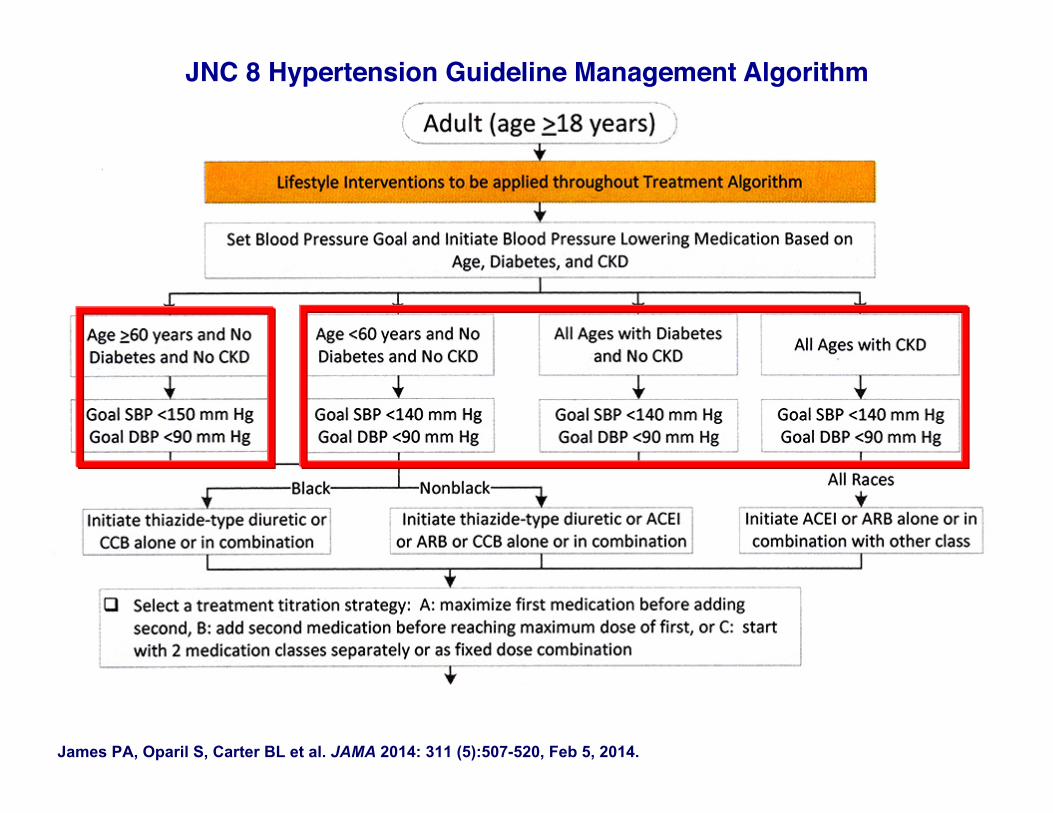
James PA, Oparil S, Carter BL et al. JAMA 2014: 311 (5):507-520, Feb 5, 2014.
JNC 8 Hypertension Guideline Management Algorithm

40
Qaseem A et al. ACP/AAFP Drug Rx of HTN in Adults 60 and Over: A clinical practice guideline from the ACP and AAFP. Ann Intern Med. 2017 Jan 17. [Epub ahead of print]
ACP/AAFP Hypertension Pharmacologic Guideline in Adults > 60 Years of Age
1.Start treatment for persistent SBP >150 mm Hg and achieve < 150 mm Hg to reduce risk for stroke, cardiac events, and death.-Strong recommendation, High-Quality Evidence 2. In patients with a hx of stroke or TIA achieve a goal of < 140 mm Hg to reduce recurrent stroke-Weak recommendation, Moderate, Quality Evidence 3. In high CV risk (diabetes, vascular disease, metabolic syndrome, CKD, for example) achieve a SBP of < 140 mm Hg-Weak recommendation, low-quality evidence

2016 Canadian Hypertension BP Guidelines
• AOBP* has replaced auscultatory BP measurement – Provider leaves the room eliminating white-coat effect – Eliminates conversation with provider or nurse – Multiple measurements taken with mean value calculated – Provides greater visit-to-visit consistency – Avoids digit preference and rounding
Leung AA et al.Can J Card . 2016;32:569-588.
** Referring to the 4 SPRINT categories of patients-clinical or subclinical CVD, CKD, aged > 75 years of age, 10-yr CVD risk > 15%
• In adults > 50 years of age, using AOBP, with SBP > 130 mm Hg, in “selected high-risk patients”**, intensive management to achieve a target SBP < 120 mm Hg is recommended
.AOBP=Automated Office Blood Pressure

N Engl J Med 2015;373:2103-‐16.
Intensive Group < 120 mm Hg; Standard Group < 140 mm Hg.

Major Inclusion Criteria
• At least 50 years old (30% AA, 10% Hispanic, 58% White) with no upper age exclusion
• Systolic blood pressure – SBP: 130 – 180 mm Hg on 0 or 1 medication – SBP: 130 – 170 mm Hg on up to 2 medications – SBP: 130 – 160 mm Hg on up to 3 medications – SBP: 130 – 150 mm Hg on up to 4 medications
• Risk (one or more of the following 4 high-risk groups) – Presence of clinical or subclinical CVD (not stroke)-20% – Chronic Kidney Disease (CKD), defined as eGFR 20–59
ml/min/1.73m2 -28% – Framingham Risk Score for 10-year CVD risk ≥ 15%
– Not needed if eligible based on preexisting CVD or CKD – Age ≥ 75 years-28%
SPRINT Research Group, NEJM 2015; 373:2103-2116.

Major Exclusion Criteria
• Stroke (SPS3) • Diabetes (ACCORD) • Congestive heart failure (symptoms or EF < 35%) • Proteinuria >1g/d • CKD with eGFR < 20 mL/min/1.73m2 (MDRD) • Polycystic Kidney Disease • Adherence issues in the past • Non-ambulatory • Living in a Nursing home
SPRINT Research Group, NEJM 2015; 373:2103-2116.
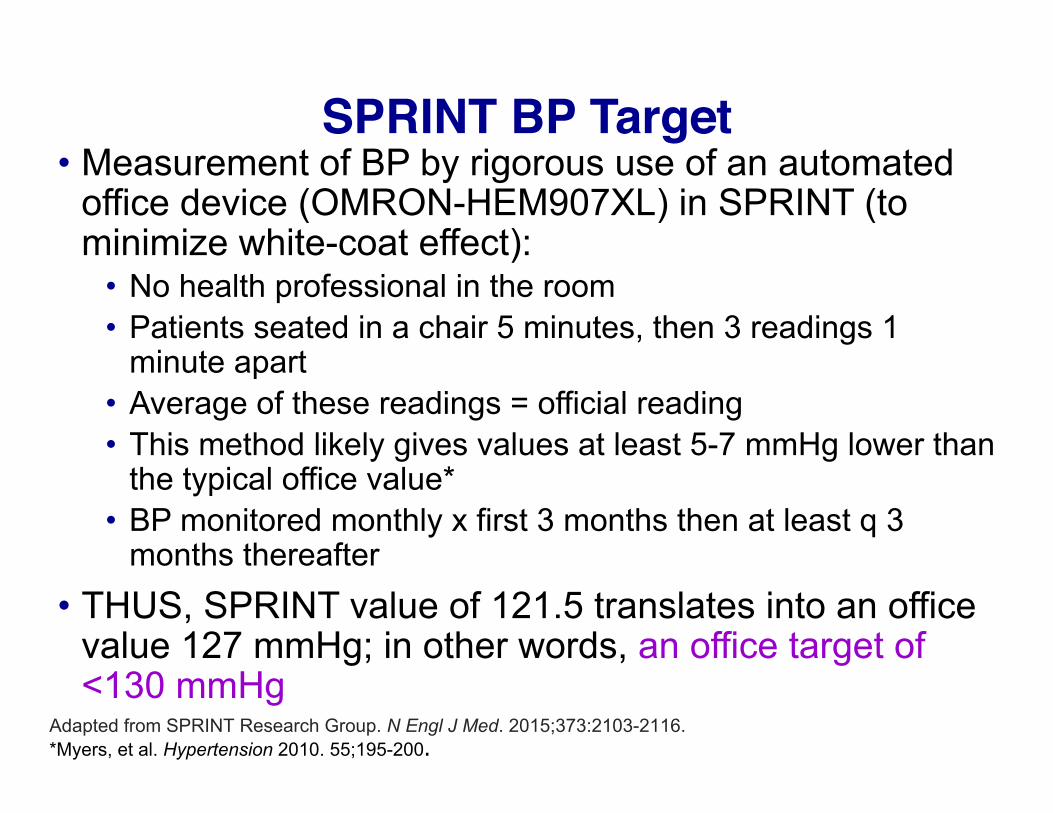
SPRINT BP Target• Measurement of BP by rigorous use of an automated
office device (OMRON-HEM907XL) in SPRINT (to minimize white-coat effect):
• No health professional in the room • Patients seated in a chair 5 minutes, then 3 readings 1
minute apart • Average of these readings = official reading • This method likely gives values at least 5-7 mmHg lower than
the typical office value* • BP monitored monthly x first 3 months then at least q 3
months thereafter • THUS, SPRINT value of 121.5 translates into an office
value 127 mmHg; in other words, an office target of <130 mmHg
Adapted from SPRINT Research Group. N Engl J Med. 2015;373:2103-2116. *Myers, et al. Hypertension 2010. 55;195-200.

46
BP Treatment
• Agents from all major antihypertensive drug classes available free of charge – Classes with best CVD outcomes in
trials given priority • Chlorthalidone encouraged as
thiazide-type diuretic • Amlodipine encouraged as CCB
SPRINT Research Group, NEJM 2015; 373:2103-2116.

Chlorthalidone: The Preferred Thiazide-Type Diuretic for HTN
• Greater potency • 24-hour duration of action • Much greater evidence base for CV outcome improvement at the current doses recommended (12-25 mg)

Diuretics Used to Treat HypertensionBA (%) T½ (hours) DOA (hours)
Thiazide and Thiazide-like Diuretics
Hydrochlorothiazide 65 – 75 3.0 – 10.0 6 – 12 Chlorothiazide 30 – 50 15.0 – 25.0 6 – 12 Chlorthalidone 65 24.0 – 55.0 24 – 72 Bendroflumethiazide 90 2.5 – 5.0 18 – 24 Indapamide 90 6.0 – 15.0 24 – 36 Metolazone 65 14 12 – 24
Loop Diuretics Bumetanide 80 – 90 0.3 – 1.5 4-6 Furosemide 10 – 100 0.3 – 3.4 6-8 Torsemide 80 – 100 3.0 – 4.0 6-8
Potassium-Sparing Diuretics
Amiloride 15-20 17.0 – 26.0 24 Triamterene 83 (55)* 3.0 (3.0)* 7-9 Spironolactone >90 1.5 – 15.0† 48-72 Eplerenone 69 2.2 – 9.4 NA
*Parentheses denote active metabolite. †The half-life of one active metabolite, potassium canrenoate, is 15 h. BA = bioavailability; T½ = half-life; DOA = duration of action: NA = unknown. Reprinted from Brater DC. In: Principles of Pharmacology: Based Concepts and Clinical Applications. 1995:657-672, with permission from Springer Science and Business Media; Delyani JA, et al. Cardiovasc Drug Rev. 2001;19:185-200; Rosenberg J, et al. Cardiovasc Drug Ther. 2005;19:301-306; Sica DA. Congest Heart Fail. 2003;9:100-105.

Representative Outcome Studies Using Chlorthalidone vs HCTZ
Chlorthalidone HCTZ (dose) MRFIT
(50–100 mg) MRFIT
(50–100 mg)
SHEP (12.5–25 mg)
ACCOMPLISH (2.5–25 mg)
ALLHAT (12.5–25 mg)
Medical Research Council trial in the Elderly (MRC-E)
(25–50 mg)
Treatment of Mild Hypertension trial (TOMHS)
(12.5–25 mg)
VA Cooperative Study Group on antihypertensive agents
(50–100 mg)
Hypertension Detection and Follow-up Program (HDFP)
(25–100 mg)
HCTZ=hydrochlorothiazide. Germino F.W. Curr Cardiol Rep. 2012;14:673-677.

−12.4 −11.4
−13.5
−7.4 −8.1 −6.4
-‐16 -‐14 -‐12 -‐10 -‐8 -‐6 -‐4 -‐2 0
CLD 25 mg HCTZ 50 mg
Chlorthalidone 25 mg Has Greater BP-Lowering Efficacy vs HCTZ 50 mg, Especially at night
CLD=chlorthalidone; HCTZ=hydrochlorothiazide.
Red
uctio
n in
Mea
n SB
P B
asel
ine
to W
eek
8, m
m H
g
24-hour Mean SBP Daytime Mean SBP Night-time Mean BP
Daytime was 6:00 AM to 10:00 PM; night-time, 10:00 PM to 6:00 AM.
P=0.009 P=0.054 P=0.230
Ernst ME, et al. Hypertension. 2006;47:352-358.

Medication Classes by Treatment Group
Last Visit Per Participant Prior to 8/20/2015
Supplement to N Engl J Med. 2015;373:2103-16.
Intensive Group < 120 mm Hg; Standard Group < 140 mm Hg.

Systolic BP During Follow-up
Mean SBP 136.2 mm Hg
Mean SBP 121.4 mm Hg
Average SBP (During Follow-‐up) Standard: 134.6 mm
Hg Intensive: 121.5 mm
Hg
Average number of anHhypertensive medicaHons
Number of parHcipants
Standard
Intensive
Year 1
SPRINT Research Group, Figure 2. NEJM 2015; 373:2110.
(N=9361)
Number of ParHcipants
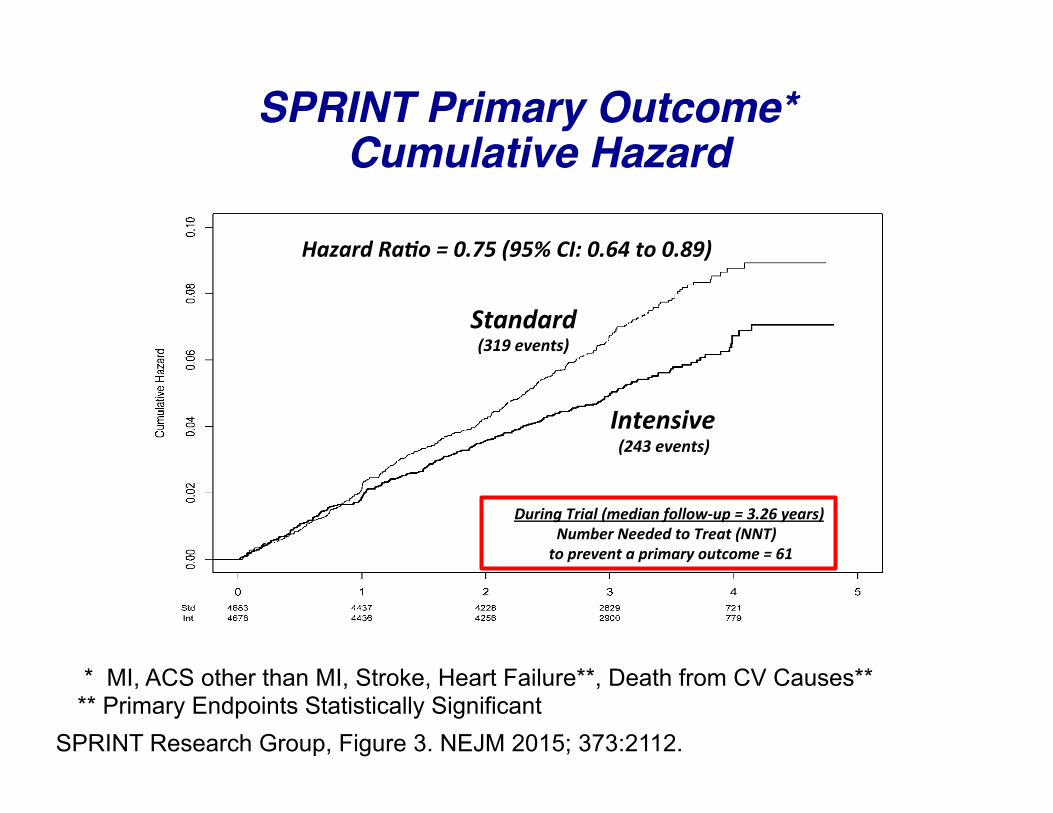
Hazard RaHo = 0.75 (95% CI: 0.64 to 0.89)
Standard
Intensive (243 events)
During Trial (median follow-‐up = 3.26 years) Number Needed to Treat (NNT) to prevent a primary outcome = 61
SPRINT Primary Outcome* Cumulative Hazard
(319 events)
SPRINT Research Group, Figure 3. NEJM 2015; 373:2112.
* MI, ACS other than MI, Stroke, Heart Failure**, Death from CV Causes** ** Primary Endpoints Statistically Significant

*Treatment by subgroup interacLon
Primary Outcome Experience in the 6 Pre-specified Subgroups of Interest
SPRINT Research Group. N Engl J Med. 2015;373:2103-2116.

*
*p=0.34, aZer Hommel adjustment for mulHple comparisons
All Cause Mortality Experience in the Six Pre-specified Subgroups of Interest
SPRINT Research Group. N Engl J Med. 2015;373:2103-2116.

SPRINT: Serious Adverse Events* Total SAE Similar
3.8
1.1
0 0.5 1
1.5 2
2.5 3
3.5 4
4.5 5
Hypotension Acute kidney injury or acutre renal failure
≥30% reduc<on in eGFR to <60mL/min/1.73 m2
Intensive Treatment Standard Treatment
HR: 3.49 95% CI: 2.44 -‐ 5.10
P < .001
SPRINT Research Group. N Engl J Med. 2015;373:2103-2116.
Percen
t of p
a<en
ts
Acute Kidney Injury or Acute Renal Failure
≥ 30% Reduc<on in eGFR to < 60mL/min/1.73 m2 in those w/o CKD on entry
2.4
1.4 2.5
4.1
P < .001 P < .001
*Fatal or life threatening event, resulHng in significant or persistent disability, requiring or prolonging hospitalizaHon, or judged important medical event.

Number (%) of ParHcipants Intensive Standard HR (P Value)
Laboratory Measures1 Sodium <130 mmol/L 180 (3.8) 100 (2.1) 1.76 (<0.001) Potassium <3.0 mmol/L 114 (2.4) 74 (1.6) 1.50 (0.006) Potassium >5.5 mmol/l 176 (3.8) 171 (3.7) 1.00 (0.97)
Signs and Symptoms OrthostaHc hypotension2 777 (16.6) 857 (18.3) 0.88 (0.01) OrthostaHc hypotension with dizziness 62 (1.3) 71 (1.5) 0.85 (0.35)
1. Detected on rouHne or PRN labs; rouHne labs drawn quarterly for first year, then q 6 months 2. Drop in SBP ≥20 mmHg or DBP ≥10 mmHg 1 minute aZer standing (measured at 1, 6, and 12 months and yearly thereaZer)
SPRINT Research Group, Adapted from Table 3. NEJM 2015; 373:2114.
Number of Participants with a Monitored Clinical Measure During F/U

Implications of SPRINT for Guidelines and HTN Management
• SPRINT likely will change SBP goal recommenda<ons in the new guidelines coming out Sept 2017
• As big a ques<on is will we change how BP is measured in office prac<ce?
• If SPRINT-‐like pa<ents will have a goal of <130 mm Hg* -‐What about other high-‐risk popula<ons?
• Diabetes mellitus (ACCORD BP)-‐130-‐139 mm Hg* • Post-‐stroke (SPS3)-‐130-‐139 mm Hg*
-‐What about lower risk popula<ons? • Age 50-‐74 yrs, SBP ≥130 mm Hg but lower CVD risk-‐< 140 mm Hg* • Age <50 years with SBP <140 mm Hg-‐already at goal*
ONE SIZE DOES NOT FIT ALL-‐INDIVIDUALIZE
*-Basile opinion.

Hypertension
COR LOE Recommenda.ons Comment/ Ra.onale
Treating Hypertension to Reduce the Incidence of HF
I B-‐R
In paLents at increased risk, stage A HF, the opLmal blood pressure in those with hypertension should be less than 130/80 mm Hg.
NEW: RecommendaLon reflects new RCT data.
CirculaLon. 2017;April 27, DOI: 10.1161/CIR.0000000000000509

Hypertension
COR LOE Recommenda.ons Comment/ Ra.onale
Treating Hypertension in Stage C HFrEF
I C-‐EO
PaLents with HFrEF and hypertension should be prescribed GDMT Ltrated to a\ain systolic blood pressure less than 130 mm Hg.
NEW: RecommendaLon has been adapted from recent clinical trial data but not specifically tested per se in a randomized trial of paLents with HF.
CirculaLon. 2017;April 27, DOI: 10.1161/CIR.0000000000000509

Take Home Messages
• Previous guideline recommendations for SBP targets of < 150 mmHg if aged ≥60 years old as in JNC 8 and recently resurrected by the AAFP/ACP will not be endorsed.
• In most adults—regardless of age and diabetes status—reducing SBP to 130-139 mmHg (< 140)/ 80-89 mm Hg (< 90 mm Hg (if tolerated) appears to offer the best overall organ protection; ie “sweet spot” for the heart, brain, and kidney. How close we get to 130/80 mmHg should be Individualized!

Take Home Messages
• In older and higher-risk hypertensive populations, if a lower BP goal is chosen (< 130 mm Hg), check renal function and electrolytes more regularly.
• How you measure BP is a key determinant to what your target BP should be.
• In patients at increased risk for, or with HFrEF, the optimal BP in those with hypertension should be < 130/80 mm Hg.

“You want the truth? You can’t
handle the truth!”
Jack Nicholson “A Few Good Men” 1992

64
Recent BP Control Rates (< 140/90 mm Hg) in a the Kaiser Permanente Health Care System Has Been As High As:
Post-test ARS Question 1
1. 95%2. 80%3. 70%4. 50%5. I am unsure

65
The BP Measurement that correlates least with Clinical Outcome is the:
Post-test ARS Question 2
1. Nighttime BP2. Daytime BP3. 24-hour BP4. Office BP5. None of the above

66
Recently recommended systolic BP targets in different populations at risk include all of the following except:
1. <150 mmHg2. <140 mmHg3. <130 mmHg4. <120 mmHg5. <110 mm Hg
Post-test ARS Question 3

67
The thiazide/thiazide-like diuretic with the shortest half life is:
1. Hydrochlorthiazide2. Indapamide3. Chlorothalidone4. Metolazone5. They all have the same half-life
Post-test ARS Question 4

68
Choose the Best Answer:According to JNC 8, which of the following antihypertensive drug classes is not appropriate for initial use in an uncomplicated hypertensive patient?
1. Calcium Channel Blocker2. Thiazide-type diuretic3. Beta-blocker4. ACE Inhibitor or ARB5. None of the above
Post-test ARS Question 5

Thank you!Comments or
Questions?