hx-osce-2
DESCRIPTION
OSCETRANSCRIPT
7/18/2019 hx-osce-2
http://slidepdf.com/reader/full/hx-osce-2 1/6
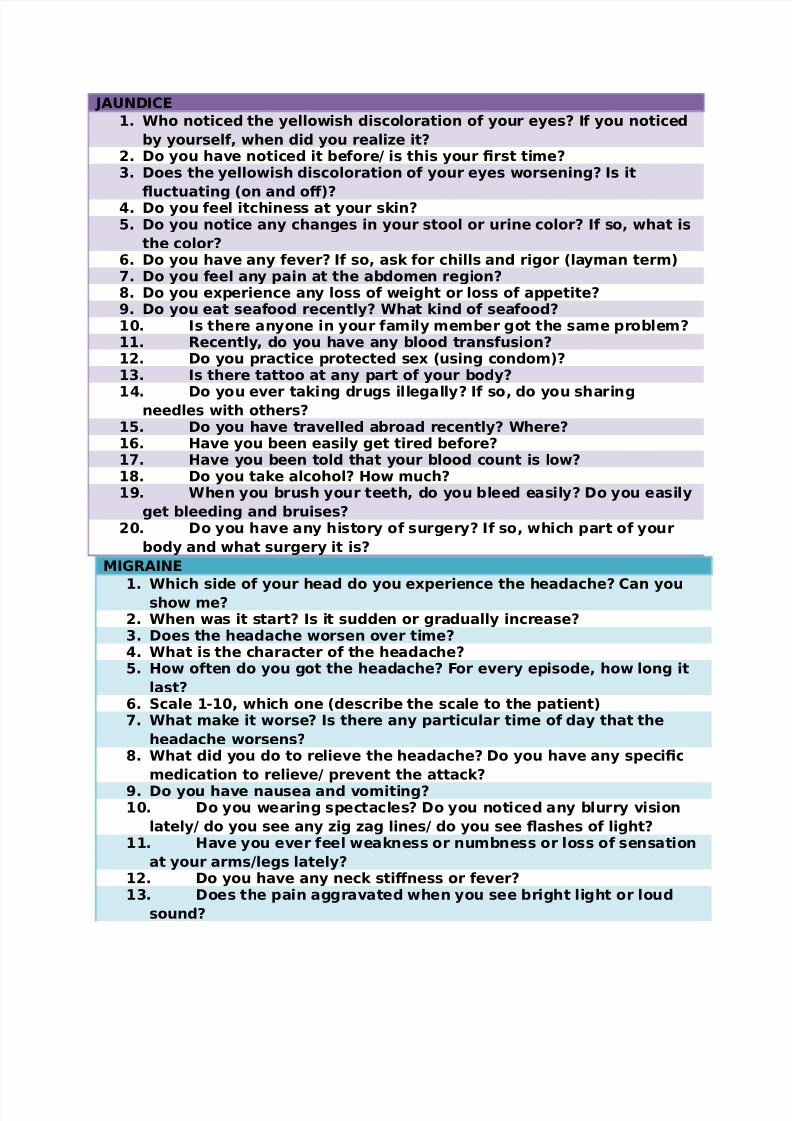
JAUNDICE
1. Who noticed the yellowish discoloration of your eyes? If you noticed
by yourself, when did you realie it?!. Do you ha"e noticed it before# is this your $rst ti%e?&. Does the yellowish discoloration of your eyes worsenin'? Is it
(uctuatin' )on and o*+?. Do you feel itchiness at your s-in?. Do you notice any chan'es in your stool or urine color? If so, what is
the color?/. Do you ha"e any fe"er? If so, as- for chills and ri'or )lay%an ter%+0. Do you feel any ain at the abdo%en re'ion?2. Do you e3erience any loss of wei'ht or loss of aetite?4. Do you eat seafood recently? What -ind of seafood?15. Is there anyone in your fa%ily %e%ber 'ot the sa%e roble%?11. 6ecently, do you ha"e any blood transfusion?1!. Do you ractice rotected se3 )usin' condo%+?1&. Is there tattoo at any art of your body?
1. Do you e"er ta-in' dru's ille'ally? If so, do you sharin'needles with others?
1. Do you ha"e tra"elled abroad recently? Where?1/. 7a"e you been easily 'et tired before?10. 7a"e you been told that your blood count is low?12. Do you ta-e alcohol? 7ow %uch?14. When you brush your teeth, do you bleed easily? Do you easily
'et bleedin' and bruises?!5. Do you ha"e any history of sur'ery? If so, which art of your
body and what sur'ery it is?
8I96AINE
1. Which side of your head do you e3erience the headache? Can youshow %e?!. When was it start? Is it sudden or 'radually increase?&. Does the headache worsen o"er ti%e?. What is the character of the headache?. 7ow often do you 'ot the headache? :or e"ery eisode, how lon' it
last?/. ;cale 1<15, which one )describe the scale to the atient+0. What %a-e it worse? Is there any articular ti%e of day that the
headache worsens?2. What did you do to relie"e the headache? Do you ha"e any seci$c
%edication to relie"e# re"ent the attac-?
4. Do you ha"e nausea and "o%itin'?15. Do you wearin' sectacles? Do you noticed any blurry "ision
lately# do you see any i' a' lines# do you see (ashes of li'ht?11. 7a"e you e"er feel wea-ness or nu%bness or loss of sensation
at your ar%s#le's lately?1!. Do you ha"e any nec- sti*ness or fe"er?1&. Does the ain a''ra"ated when you see bri'ht li'ht or loud
sound?

7/18/2019 hx-osce-2
http://slidepdf.com/reader/full/hx-osce-2 2/6
1. If you ha"in' your %enstruation, does the ain worsenin'?1. Is there any articular food )intense (a"or food such as dar-
choc and cheese+ that worsenin' the ain? Do you drin- red wine? Is
the headache beco%e se"ere when you drin- it?1/. Do you feel stress lately?10. Is there anyone in your fa%ily %e%ber 'ot the sa%e roble%?12. Do you ta-e oral contraceti"e ills?
IN=E68I==EN= C>AUDICA=IN
1. Where is the ain? Can you oint the side?!. When does the ain co%e )e3ertion+? Does the ain relie"e when
you are restin'?&. 7ow far can you wal- before you feel the ain? What is the
di*erence for the last ti%e )before you 'ot the ain+ and now?. Do you feel any ain when you are at rest or in the ni'ht?. Is there any swellin' at your le's?/. 7ow lon' does the ain last?0. Do you feel the ain at buttoc-@s area? Is it relie"ed at rest?
2. Do you ha"e erectile dysfunction# decrease in libido?4. Are you a chronic s%o-er? 7ow %any ci'arettes er day? Do you
sto? When?15. Do you ha"e D8#7=#7C>? Is it "ery hi'h? Are you on
treat%ent? Well control?11. 7a"e you been in hosital for this roble%? Any in"esti'ation
done on you that calls doler?1!. Do you ta-e any dru's for this roble%? Any blood thinner
such as asirin# cloido'rel?1&. Do you ta-e oral contraceti"e ills?1. Do you ha"e ain at the chest when you wal- and relie"e at
rest? Do you ha"e stro-e before? Do you ha"e wea-ness at yourhand#le'? Any discoloration of you toes?
1. What is your occuation?
B6NC7IA> A;=78A
1. When it all started?!. 7ow often you 'ot it?&. 7ow lon' does it last for e"ery eisode?. Does it ro'ressi"ely worsenin'?
. 7a"e you been dia'nose with asth%a before?/. What did you do to relie"e the ain? Did you use any inhaler?0. Now, are you usin' the inhaler freuently? 7ow %any ti%es in a day#
wee-?2. Do you ha"e the attac- when you e3ercise#doin' sorts acti"ity?
What did you do when you 'et it?4. Does the cold weather worsenin' your condition?15. When you stress, do you 'et it?

7/18/2019 hx-osce-2
http://slidepdf.com/reader/full/hx-osce-2 3/6
11. Do you ha"e cats?1!. Do you ha"e carets at your house?1&. Are there any soft toys such as teddy bear at your house?1. Are you aller'ic towards dust? Do you ha"e runny nose?1. Do you 'et ain )at the facial area+ and sense of hea"iness
early in the %ornin'? )sinusitis+1/. Do you ha"e food aller'y?10. Do you ha"e itchiness at any art of your body and it co%es at
the sa%e lace? )ece%a+12. Do you ha"e any dru' aller'y that will cause itchiness, face
swellin' or shortness of breath?14. Do you e"er bein' hositalied because of this roble%?
entilated?!5. Any of your fa%ily %e%bers who 'ot the sa%e roble%?!1. Do you s%o-in'? 7ow %any ci'arettes er day?!!. E"er e3erienced any dry cou'h?!&. What is your occuation?
C7E;= AIN1. Where do you feel the ain? Can you lease oint out where the ain
felt?!. Is the ain co%e suddenly or 'radually?&. Can you describe the character of the ain? Is it shar# cra%in'#
etc.. :or how lon' do you feel the ain?. ;cale 1<15, which one? Does the ain 'et worse within !5 %inutes?
Does the ain awa-en you fro% slee?/. Does the ain radiate to your nec-# aw or left ar%# anywhere else?0. Do you e3erience any rofuse sweatin'# nausea and "o%itin'#
an3iety and alitation?2. What %a-e the ain worse? What did you do to relie"e the ain at
that ti%e?4. Is this your $rst eisode?15. If noF so, do you -now about the dru' called as 9=N that was
ut under your ton'ue? Do you ut 9=N under your ton'ue while
ha"in' the attac-?11. Do you ha"e 7=# D8# 7C>? Are you on treat%ent and is it well
control?1!. Are you s%o-er? When did you start s%o-in'? 7ow %any
ci'ars you s%o-e er day? Do you still s%o-in'? When do you sto
and why?1&. What is your occuation? Is it a stressful ob? Do you lo"e your
ob?1. Is there anyone in your $rst de'ree relati"es# fa%ily %e%ber
who died G for %ale and G/ for fe%ale because of heart disease?1. Any ast history of stro-e? Do you su*er any transient
wea-ness at any art of your body? Do you feel sudden wea-ness at
your li%bs and suddenly dissol"e# 'o away?

7/18/2019 hx-osce-2
http://slidepdf.com/reader/full/hx-osce-2 4/6
1/. 7a"e you been ad%itted to the hosital? =o the coronary care
unit )CCU+ or nor%al ward? 7ow lon' you ha"e been ad%itted? Is
there any co%lication arise after the ad%ission?10. Is there any secial rocedure li-e an'io'ra% done to you?

7/18/2019 hx-osce-2
http://slidepdf.com/reader/full/hx-osce-2 5/6
=7H6ID ):CU; 7I;=6H : =76ID :UNC=IN AND 9I=6E+ if the
uestion as- you about focus history of =7H6ID :UNC=IN only, don@t
as- the atient anythin' about the swellin', wastin' your ti%e
1. Do you notice any chan'es in your aetite )increase or decrease+
and your wei'ht )'ain or loss+?
!. Which one do you refer, war% en"iron%ent or cold en"iron%ent orboth?
&. Do you ha"e rofuse sweatin'?. Any chan'es in your bowel habit recently? )such as diarrhea or
constiation +. Do you ha"e any increase in heart beatin'?/. 7ow about your %ood? Do you feel unusually ner"ous# irritable?0. About your %enstruation, is it re'ular? Also as- about the (ow.2. If u wal-s for a distance or cli%bin' stair, do you notice that you
easily 'ot ;B# lethar'ic?4. Do you 'et %uscle wea-ness?15. Do you notice any tre%or at your hand?
11. Do you ha"e any roble% with your eye? Any double "ision?
Notice bul'in' of the eye? Any swellin' around the eyes?1!. Do you feel that your s-in is dry and rou'h?1&. Do you notice any lu% at your nec-? As- co%lete history of
lu%F
• :irst noticed
• ro'ression
• Any associated sy%to%sF dysha'ia, ;B, ainful,
hoarseness of "oice
• E"er disaear?
• Notice any other lu%?1. Do you ha"e any fa%ily %e%bers who 'ot thyroid roble%?1. Do you ta-e any %edication?

7/18/2019 hx-osce-2
http://slidepdf.com/reader/full/hx-osce-2 6/6
B6EA;= >U8
1. Which side of your breast do you feel the lu%?!. When it was $rst noticed?&. Who noticed the lu%, you or your husband, etc.? r you notice the
lu% because there is ain?. Does the lu% ainful? )ta-e further history of the ain<not %uch<+. Does the lu% a*ect your resiration# swallowin'?/. Do you feel disco%fort because of the lu%?0. chan'e associated with %enstrual cycle )don@t -now how to
interret it into uestion+2. Does the lu% 'ettin' bi''er? Earlier what sie, and now what sie?
As- for the chan'es in the nature of the lu% )fro% ainless to
ainful or "ice "ersa+4. Does the lu% e"er disaear )esecially when you lyin' down#
doin' e3ercise+.
15. Do you notice any other lu%, esecially at the a3illa?11. What do you thin- cause the lu% )any history of trau%a+?1!. Is there any dischar'e fro% your nile? What is the a%ount?
Is it continuous or on and o*? What is the color of the dischar'e? Is
there any bloodstained aear?1&. What is your a'e when you ha"in' your $rst %enstruation?
8enoause?1. What is your a'e when you ha"in' your $rst re'nancy? 7ow
%any ti%es do you 'et re'nant? )Before that, as- whether she@s
%arried and ha"in' children or not.+1. Do you breast feed your children?
1/. Do you ta-e oral contraceti"e ills# hor%onal relace%enttheray?
10. Is there anyone in your fa%ily# $rst de'ree relati"es who
ha"in' breast cancer# o"arian cancer?