hutt valley district health board · hutt valley district health board. ... and encourages maori...
TRANSCRIPT
2001
Report for the six months ended 30 June
Hutt Valley District Health Board

Hu
tt Valley D
istrict Health
Bo
ardC
on
tents
1Directory
Statement of Purpose
Hutt Valley DHB Profile
Hutt Valley DHB Development
Board Members’ Report
Chairman’s Report
Chief Executive’s Report
Service Highlights
Financial Statements
Statement of Accounting Policies
Statement of Financial Performance
Statement of Movements in Equity
Statement of Financial Position
Statement of Cashflows
Notes to the Financial Statements
Statement of Objectives and Service Performance
Governance, Funding and Planning Services
Provider Services
Statement of Responsibility
Report of the Audit Office
2
3
4
5
8
10
12
15
25
26
28
29
30
31
33
40
41
48
51
52
Contents
Head OfficePilmuir HousePilmuir StreetLower Hutt
Postal AddressPrivate Bag 31-907Lower Hutt
BankersBank of New Zealand
SolicitorsImpact Legal
AuditorAudit New ZealandWellingtonOn behalf of the Controller and Auditor-General
Hutt Valley DHB PeopleBoard MembersThe Board consists of tenmembers, including a chairmanand a deputy chair, appointedby the Minister of Health.
Warren YoungChairmanBComm, FCA, CMA, FCIS,FNZIM, FinstD
Hon Margaret ShieldsDeputy ChairQSO, BA
Dr Chris CunninghamBSc(Hons), PhD
Peter GlensorBA
Barbara GrieveMBA, BA(Hons)
Dr Ate MoalaMB ChB
Marian RedwoodBA, Dip Tchg, ATCL
Shaan StevensBCA, LLB, CA
Brenda TahiBSocSci, MBA
Vern Winitana
Chief ExecutiveStephen McKernan
Hutt Valley DHB PeopleCommittee MembersThe membership of thecommittees is as follows.
Hospital Advisory CommitteeBarbara Grieve (Chairperson)Dr Chris CunninghamWarren Young
Community and Public HealthAdvisory CommitteePeter Glensor (Chairperson)Dr Ate MoalaMargaret ShieldsVern Winitana
Disability Support AdvisoryCommitteeMarian Redwood (Chairperson)Margaret ShieldsVern Winitana
Finance and Audit CommitteeShaan Stevens (Chairperson)Brenda TahiWarren Young
2
Hu
tt V
alle
y D
istr
ict
Hea
lth
Bo
ard
Dir
ecto
ry
Directory
Hu
tt Valley D
istrict Health
Bo
ardStatem
ent o
f Purp
ose
3Vision, Mission and ValuesThe Board has established the following vision,mission and values for Hutt Valley DHB.
VisionTo be New Zealand’s foremost District Health Boardin optimising the health and wellbeing of our community.
MissionTo excel in the way we consult, communicate, planand provide health services to our community.
ValuesWorking together: with our providers, communitygroups and other agencies;
Leadership: within our community and throughsetting a positive example;
Respect: for each other and the rights ofindividuals;
Communicating effectively: with our community,with our staff and our clients;
Caring: for our community and for each other; and
Excellence: in all that we do.
Statement of Purpose

The Hutt Valley DHB is responsible for planning,prioritising, funding and providing government-funded health care and disability support servicesfor the 135,000 people that live in the Hutt Valley.The Hutt Valley DHB as an organisation employs1,700 people, most of whom work for Hutt Hospitaland our community and regional health services.This is the part of the Hutt Valley DHB that weoften now refer to as the ‘provider arm’.
A Board, which has a membership of up to 11 people, has strategic oversight or governance the Hutt Valley DHB. The Board has responsibilityfor delivering on local and national healthobjectives within a current annual budget ofapproximately $160 million.
The Hutt Valley DHB has been in existence since1 January 2001. By the middle of 2002 it willhave the capability to meet the goals specifiedin the New Zealand Public Health and DisabilityAct, amongst which are to:
• Improve, promote and protect the health of communities within the Hutt Valley
• Better coordinate health services in the Hutt Valley;for example, GP and hospital-based services
• Ensure effective care or support of those in needof personal health services or disability support
• Promote the inclusion and participation in society of people with disabilities
• Reduce health disparities by improving health outcomes for Maori and other population groups
• Encourage community participation in health improvement, and in planning for the provisionof health services and any significant changesto the provision of health services.
This will involve buying services from a wide rangeof health and disability service providers, includingGPs, mental health providers, rest homes,pharmacies, private laboratories and hospitals.
With the additional responsibilities of buying,managing and providing a much wider range ofservices to meet the needs of our community, thereis the requirement for a strong funding and planningmanagement capability within Hutt Valley DHB.
4
Hu
tt V
alle
y D
istr
ict
Hea
lth
Bo
ard
Hu
tt V
alle
y D
HB
Pro
file
Hutt Valley DHB Profile
5With the implementation of the NZ Public Healthand Disability Act 2000, the Hutt Valley DHB wasformed. This meant a move from health provisionto include funding and planning functions. Thefirst six months of operation for the Planningand Funding team were largely focused on buildingcapacity.
Financial management systems, processes andresources to accommodate the new fundingfunction have been established and are in place.A financial analyst, portfolio managers andcontract administrator have joined the Fundingand Planning team from the Health FundingAuthority/Ministry of Health.
Sound relationships with Maori are in place, andconsultation with both Maori and Pacific peopleis ongoing. Mechanisms have been put in placeto enable Maori representation on all serviceplanning groups to provide input in the healthservice planning for the Hutt community. Similardialogue was commenced with Pacific peoples’groups in the Hutt Valley to enable the DHB tobetter understand their health needs and encouragetheir participation in the work of the DHB.
A key development for district health boards isthe need to produce a 5-year strategic plan. Thestrategic plan for the Hutt Valley DHB will outlinehealth care provision for the Hutt communityfor the next 5-10 years, and will form the initialfocus for prioritisation activity. The first phasesin the development of this plan have beencompleted. Service planning groups have beenestablished to develop plans focused on the New Zealand Health Strategy population healthobjectives. The planning groups are working toterms of reference, a defined project scope anda planned timetable. The service plans will beconsolidated into a draft strategic plan, whichwill go out for public consultation in early 2002.
Community consultation is an integral part ofthe plan and this is occurring in several ways:
• By involvement of community providers, GPs, consumers, Pacific, Maori and inter-sectorial stakeholders in service planning groups tohelp the DHB develop draft plans
• By meetings with providers and keystakeholders on key planning issues
• Once the plan has been approved by the Boardas a draft for consultation, a program of meetingsand focus groups will be set up and all affectedparties, including Hutt residents, will have the opportunity to make formal submissions.
Health needs analysis is in the early stages of development and is being carried out in conjunction
with the development of the strategic plan. A number of factsheets including profiles of theHutt Valley District have been developed. The Hutt Valley District Profiles were presentedat several Hutt Valley DHB public meetings. A provider forum explained the proposedtransition process for contract devolution fromMoH to the DHB and provided an opportunity forquestions from the floor.
A shared support agency has been establishedfor the six central DHB’s. The Central RegionTechnical Advisory Service Ltd (TAS) is expectedto provide the DHB’s with applied analysis, serviceplanning and external audit services in order toinform local funding and planning decisions.
Decision-making PrinciplesHutt Valley DHB has adopted the following interim decision-making principles. They will bediscussed during the consultation of the strategicplan in 2002.
Maori HealthIn making funding decisions, the DHBacknowledges the special relationship betweenMaori and the Crown under the Treaty of Waitangiand encourages Maori participation in providingand using services. Maori health issues will beconsidered when applying all of the otherdecision-making principles, by adopting theDHB-wide approach to the partnership i.e.,
• Seeking partnership, participation andprotection of Maori and their values and culture
• Seeking to reduce Maori health inequities• Seeking to increase Maori development in health• Ensuring Maori workforce, retention, recruitment
and training is reflective of the Maori community.
EffectivenessEffectiveness will include the extent to whichhealth and disability services produce desiredhealth outcomes, such as reductions in pain, themaintenance of daily living activities andextending life. Effectiveness will be quantifiedwhere possible.
CostThe DHB will consider the total economic costs ofservices, including flow-on effects in both the healthand other social sectors, to ensure availablefunding is used to achieve the maximum possiblegain in health and independence status.
Hu
tt Valley D
istrict Health
Bo
ardH
utt V
alley DH
B D
evelop
men
t
Hutt Valley DHB Development

Hu
tt V
alle
y D
istr
ict
Hea
lth
Bo
ard
Hu
tt V
alle
y D
HB
Dev
elo
pm
ent
EquityThe DHB will seek equity of outcome to reduceremediable disparities in health status for groupswith lower levels of health, including (but notlimited to) the Maori population, the Pacificpopulation and groups of high health need.
Consistency with the New Zealand Health StrategyThe DHB will give priority to initiatives that areconsistent with the NZHS health gain and servicepriority areas.
AcceptabilityThe expectations and values of Hutt Valleyresidents will be taken into account in the DHB’sdecision-making process. The implication of thisprinciple is that some services where theevidence for effectiveness is weak, but which arehighly valued by the community, may continueto be funded. As per the Maori Health principle,the values of the Maori community would needto be given particular consideration.
Administration of funding agreements with providersHutt Valley DHB will put in place new policiesrelating to the administration and funding of contracts.
Operational ManagementFunding Agreements will be administered byFunding and Planning staff. A key relationship(portfolio) manager will be assigned to eachprovider.
Authority to Approve ContractsAn internal DHB mechanism, the FundingManagement Group (FMG), will be developed tooversee and give structure to management ofdelegated authority relating to renewing andchanging service agreements.
Provider performance management, reporting andmonitoring Hutt Valley DHB performance management willinclude the following key components:
• Minimum quality and corporate capability standards• Pre-agreement audit• Service specifications• Business rules • Volume and price schedule • Provider reporting and monitoring • Provider feedback • Scheduled compliance audits • Issue-based audits • Outcomes review.
With the development of these new policies,procedures and resources, Hutt Valley DHB is in agood position to take advantage of the opportunitiesin the new health sector environment.
Human ResourcesOur Human Resource goal is to be an ‘Employerof Choice’, meaning that employees choose towork for Hutt Valley DHB when presented withother choices of employment.
During the year a number of projects wereimplemented to address key staffing issues.These were:
• Recruitment and retention project to develop recruitment and retention strategies that will ensure people who are employed match theskills requirements of Hutt Valley DHB. It alsoseeks to address the reasons why people leavethe organisation
• Training and development project to build capability by developing the critical skillsrequired in staff
• Performance management project that links individual and team performance to Hutt ValleyDHB’s strategic goals.
These issues are not unique to Hutt Valley DHB;they affect all DHB’s. We have establishedproject groups involving staff, union delegatesand managers to bring about improvedorganisational performance. The project groupshave been meeting since March 2001 withsignificant progress being made.
Employment RelationsOur approach to employee relations is to continueto work co-operatively with staff and unions ina dynamic and open way, acknowledging each
other’s needs within organisational constraints.To this end we will continue to hold monthlyservice meetings and quarterly Chief Executivemeetings with the PSA and NZNO.
Health & SafetyOn 19-20 April Hutt Valley DHB underwent anACC Workplace Safety Management Practicesaudit. The audit was a comprehensive overviewof the organisation, seeking evidence of a strongsafety culture among managers and staff. As aresult Hutt Valley DHB has received the secondhighest level of accreditation and an ACCworkplace cover premium discount of 15%.
6
EstablishmentIn accordance with the provisions of the NewZealand Public Health and Disability Act 2000,Hutt Valley Health Corporation Limited wasdisestablished on 31 December 2000, and theHutt Valley DHB was created on the same date.This statutory report is therefore the first reportof Hutt Valley DHB and covers the 6-monthperiod ending 30 June 2001.
Principal ActivitiesThe activities of the Hutt Valley DHB areconsiderably expanded on those undertaken byits predecessor. With effect from 1 July 2001systems, processes and resources are in place to enable the new entity to assume responsibilityfor the funding of all local personal health,mental health, Maori health and Pacific peopleshealth services. Whilst funding these healthservices is an important component for the Hutt Valley DHB, other key activities include acomprehensive needs analysis, the prioritisationof services, broad-based consultation withstakeholders, the development of protocols fordecision making, and contract monitoring.
The Hutt Valley DHB continues to own and operatethe Hutt hospital. The services provided includethe specialities of medicine, surgery, mentalhealth, child health, maternity and public health.Within that general description are specialistservices in burns, plastic and maxillo-facial surgery,rheumatology, coronary care, intensive care,radiology and rehabilitation, a hospital dentalservice and associated child oral health service.
Hutt Valley DHB also has public health servicesthat operate from sites in Porirua, Wellingtonand the Hutt Valley, community mental healthservices that have sites situated in the Hutt Valley,and certain physiotherapy services that areprovided from an Upper Hutt base.
Financial ResultsThe financial results presented in this reportrepresent the financial results for the Hutt ValleyDHB and are in respect of the 6-month periodending 30 June 2001.
The organisation achieved a net surplus aftercapital charge of $598,000. This comparesfavourably with the budgeted surplus of $596,000.During a period of transition and considerablechange, the Board Members are comfortable withthis result.
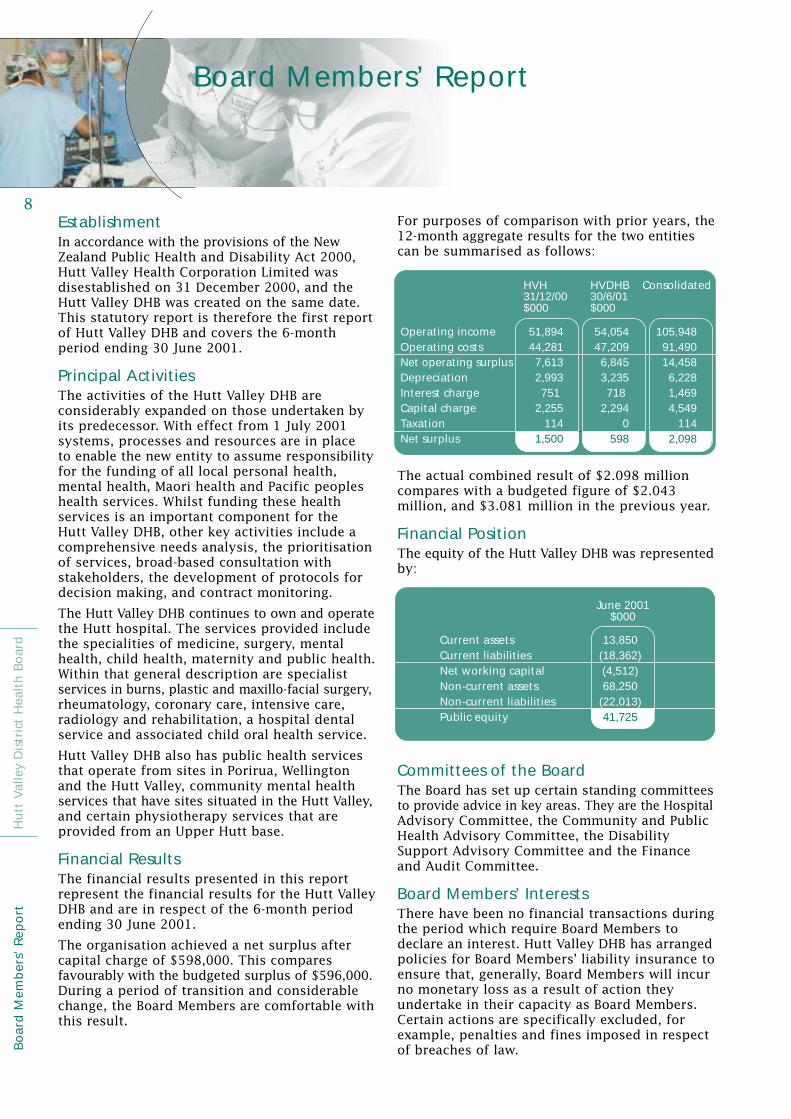
For purposes of comparison with prior years, the12-month aggregate results for the two entitiescan be summarised as follows:
The actual combined result of $2.098 millioncompares with a budgeted figure of $2.043million, and $3.081 million in the previous year.
Financial PositionThe equity of the Hutt Valley DHB was representedby:
Committees of the BoardThe Board has set up certain standing committeesto provide advice in key areas. They are the HospitalAdvisory Committee, the Community and PublicHealth Advisory Committee, the Disability Support Advisory Committee and the Financeand Audit Committee.
Board Members’ InterestsThere have been no financial transactions duringthe period which require Board Members todeclare an interest. Hutt Valley DHB has arrangedpolicies for Board Members’ liability insurance toensure that, generally, Board Members will incurno monetary loss as a result of action theyundertake in their capacity as Board Members.Certain actions are specifically excluded, forexample, penalties and fines imposed in respectof breaches of law.
8
Hu
tt V
alle
y D
istr
ict
Hea
lth
Bo
ard
Bo
ard
Mem
ber
s’ R
epo
rt
Operating incomeOperating costsNet operating surplusDepreciationInterest chargeCapital chargeTaxationNet surplus
HVH31/12/00$000
HVDHB30/6/01$000
Consolidated
51,89444,2817,6132,993751
2,255114
1,500
105,94891,49014,4586,2281,4694,549
1142,098
54,05447,2096,8453,235718
2,2940
598
Current assetsCurrent liabilitiesNet working capitalNon-current assetsNon-current liabilitiesPublic equity
June 2001$000
13,850(18,362)(4,512)68,250
(22,013)41,725
Board Members’ Report
9Board Members’ RemunerationDuring the period the following remuneration waspaid to the Board Members of Hutt Valley DHB.
Remuneration of EmployeesThe number of employees (excluding BoardMembers) whose annual income was within thespecified bands is as follows:
The information in the above tablehas been derived from remunerationpaid for the year 1 July 2000 to 30 June 2001.
The Chief Executive’s current remuneration bracketis $260,000 – $269,000. Of the 53 employeesshown above, 48 are medical or dental employees.
If the remuneration of part-time employees weregrossed up to an FTE basis, the total numberwith salaries of $100,000 or more would be 91,compared with the actual number of 53.
AuditorThe Controller and Auditor-General is appointedunder section 43 of the New Zealand Public Healthand Disability Act 2000. Audit New Zealand hasbeen contracted to provide these services.
For and on behalf of the Board
Warren C YoungChairman2 October 2001
Hu
tt Valley D
istrict Health
Bo
ardB
oard
Mem
bers’ R
epo
rt
W Young (Chairman)M Shields (Deputy Chair)B GrieveM RedwoodS StevensC CunninghamP GlensorA MoalaB TahiV Winitana*Total
Board Members’ Fees(incl Committee Fees)
$000
19.511.810.29.6
10.29.89.99.89.88.5
109.1* V Winitana was appointed to the Board in February 2001
$000100-109110-119120-129130-139140-149150-159160-169170-179180-189190-199200-209210-219Total
1997631121112
53
“The activities of the Hutt Valley DHB areconsiderably expanded on those undertakenby its predecessor.’
Hutt Valley District Health Board Members(from left to right): Marian Redwood, Peter Glensor,Chris Cunningham, Margaret Shields (Deputy Chair),Barbara Grieve, Warren Young (Chairman), Stephen McKernan (Chief Executive), Brenda Tahi,Vern Winitana, Shaan Stevens, David Williment(Board Secretary) and Ate Moala.

In accordance with the provisions of the PublicHealth and Disability Act 2000, the Hutt Valley DHBwas established on 31 December 2000. As part of its expanded business, the new Crown entityacquired on that date all the assets and undertakingof Hutt Valley Health Corporation Limited. Whilstthe following comments address the statutoryreporting requirements of the Hutt Valley DHB forthe 6 months ended 30 June 2001, where relevantand appropriate, reference is also made to theaggregate results of the two entities for the fullyear to 30 June 2001. This gives a betterunderstanding of the operational performanceover the full 12-month period, and facilitates a better comparison with the historical results ofthe provider arm of the Hutt Valley DHB, i.e. whenthe primary function was the ownership andoperation of the Hutt hospital.
Over the past 12 months much has been written andsaid about the structural and philosophical changesmade in the funding and delivery of health servicesto our respective communities. At the Hutt ValleyDHB we see our objectives very clearly. Put simply,we intend to improve the health status of theresidents in our region by better integrating primaryand secondary care services, and by working moreco-operatively with all stakeholders to achieve this.
In the governance of the Hutt Valley DHB there arethree statutory sub-committees which have beenformed by the DHB Board Members. One isresponsible for the affairs and performance ofthe hospital. The second deals with issues facedby those in the community with disability orphysical handicap. The third advises on the healthneeds of our catchment population, and the mixand range of services required to improve theoverall health status of our people. Although notrequired under statute, a finance and auditcommittee has also been established to monitorthe fiscal results of the entity. Whilst these sub-committees are advisory in nature, their terms of reference are both prescriptive and objective,and will ensure that the policy and statutoryintentions of Government are satisfied. Whereverpractical, the statutory sub-committees includemembers co-opted from the public in addition tothe appointed Board Members.
It has been satisfying to note the extent to whichthe community has engaged with the Hutt ValleyDHB in the process and programme of governancein recent months. From the outset we have soughtto make information readily available to the public,and convened most of our meetings in public.Minimal reliance has been placed on our ability tohold meetings in closed session. The Board andsub-committee meetings have been well attended
by outside visitors, and the wide variety of publicmeetings facilitated by Board Members have beenwell patronised. This desire to conduct our affairsin an open and transparent way is not only consistentwith our statutory duties. It also evidences our desireto have the community actively engaged in thedecision-making process of the Hutt Valley DHB.
It is important to recognise that the structure ofthe Hutt Valley DHB has a hospital provider armwhich is quite separate and distinct from thecommunity oriented funding and planningresponsibilities. This ensures a complete separationof these activities. For instance, there is no scopefor hospital management to in any way ‘capture’ orotherwise influence the nature or funding ofservices being contracted with community providers.
The implementation of the Government’s healthpolicy resides with the members of the districthealth boards. The composition of the Hutt ValleyDHB Board was significantly altered in Augustlast year preparatory to the advent of the HuttValley DHB, and will change further following thelocal body elections later this year. This is likelyto bring the members on the Hutt Valley DHB toeleven in number, at least two of whom will beMaori. Of this number, seven are elected positionsand four are intended to be appointed by theMinister of Health. This ratio recognises thestrong community input and accountability thatarises with the advent of district health boards.
The challenge for the new board will be to balancepublic expectation and demand for more andbetter health services with the ever-present fundinglimitations. The revised structures in themselvesdo not create more health dollars. The Hutt ValleyDHB must therefore pursue a range of options forproducing cost economies and efficiencies whichcan in turn be applied to further enhancing healthdelivery and service outcomes. The Hutt Valley DHBcontinues to work closely with the Ministry ofHealth and other district health boards to identifyways for achieving savings and avoiding anyunnecessary duplication of resources, both humanand financial. Most significant in this context hasbeen the joint establishment with the six otherdistrict health boards in the Central Region of ashared support agency. This entity will provideapplied analysis to better inform the planning andfunding decisions of the individual DHB members.
It is worth commenting that the predecessororganisation to the Hutt Valley DHB was mostnotable in the hospital sector in terms of its abilityto secure worthwhile gains and continually improveits operating performance. Over a 6-year period it turned an $18 million loss into a current year $2 million surplus, a $20 million turnaround.
10
Hu
tt V
alle
y D
istr
ict
Hea
lth
Bo
ard
Ch
airm
an’s
Rep
ort
Chairman’s Report

11By any yardstick this is a most commendableeffort, and particularly so in the health industrywhich is hallmarked by funding shortfalls. The keytargets contained in the Statement of Intent andBusiness Plan approved by Shareholding Ministersin respect of the 2001 year were all met.
As the Board Members’ Report reveals, the financialresults of the provider and funding divisions forthe 6 months to 30 June 2001 were very much inline with budget. This is notwithstanding a numberof one-off costs associated with the formation ofthe Hutt Valley DHB, and developing the capabilityof the new entity to assume the planning andfunding obligations devolved from the HealthFunding Authority and Ministry of Health. It isequally pleasing to note that during a year oftransition and some uncertainty, the Hutt ValleyDHB and its predecessor organisation achieved anaggregate surplus of $2.098 million for the full12-month period to 30 June 2001. This compareswith a combined budget surplus of $2.043 million,which was always viewed by the Board Membersas a ‘stretch target’. The fact is that no otherdistrict health board achieved a comparable surplusfor the full period to 30 June 2001, and mostconcluded the year with a substantial overall loss.
The Hutt Valley DHB inherited a strong balancesheet from its predecessor. The debt ratio, whichmeasures the extent to which the organisation isreliant upon borrowed monies to sustain itsbusiness, presently stands at a very respectable49%. This compares with the sector average onthe same basis of calculation of 65%. The cost of servicing debt is over nine times covered bythe level of surplus reported in the latest year.However, whilst still well within the borrowingcovenants, the losses anticipated over the next 3-year planning cycle would suggest that theseratios will be placed under considerable pressure.
We are now in the final stages of reconfiguringand upgrading the hospital campus. Of our originalbudget of $22.4 million, $11.1 million relates toprojects completed in prior years, $7.1 millionwas expended in the 2001 year, and there remainsa further $4.2 million to conclude the programme.Overall completion is scheduled to be no later thanJune 2002. This whole exercise has been at theheart of the strategic plan developed some 5 yearsago. It has produced major enhancements in theefficient delivery of services, has enabled theprogressive sale of redundant assets, has createdsavings substantially in excess of $1.0 million peryear, and has avoided core maintenance workdeferred from prior years. It is to be hoped thatthese hard won benefits are not lost in thecurrent round of health sector restructuring.
In purely operationalterms, the Hutt ValleyDHB has achievedvirtually all the target thresholds set by the BoardMembers at the beginning of the year. On theprovider side, inpatient and day-case activitycomfortably exceeded contracted levels, bedoccupancy and average length of stay weresuccessfully held at the anticipated rates, waitinglists continue to drop, and the quality of operatingtheatre management remained high. All theseindicators point to an efficiently run hospital. It is also pleasing to note that patient satisfactionwith the services provided by the hospital remainsat a high level. As far as the more embryonicfunding and planning activities of the Hutt ValleyDHB are concerned, resources, systems andprocesses are now in place to enable theorganisation to contract provider services in aninformed and responsible manner.
Whilst there still remain issues around the adequacyof our funding, the Hutt Valley DHB has not allowedany fiscal limitations to hinder its drive for qualityimprovement. During the year the organisationwas recognised with three nationally measuredawards for quality excellence, namely, full DHB-wideaccreditation by Quality Health New Zealand, thefirst such recognition of any district health board,a strong endorsement from the AccidentCompensation Commission in connection withworkplace safety management practices, andaccreditation of our diagnostic radiology servicesunder the International Accreditation New Zealandstandards, one of only four district health boardsto achieve this distinction.
Finally, and on behalf of the board, I would liketo thank all staff for their contribution during aperiod of considerable change, and perhaps somefrustration. That the year concluded on such apositive note is in no small way attributable to thecommitment of our people. I believe that the extentof support and understanding from our workforcemore than any other factor distinguishes ourorganisation from the rest of the sector. The HuttValley DHB is now poised to carry the successesof its recent past into the future and, in its widerrole, this augurs well for the health and wellbeingof the population we serve.
Warren C YoungChairman
Hu
tt Valley D
istrict Health
Bo
ardC
hairm
an’s R
epo
rt
“At the Hutt Valley DHB we see our objectives very clearly. Put simply, we intend to improve the health status of the residents in our region...”

I am delighted to present this, the first AnnualReport for the Hutt Valley DHB. In statutory termsthe report covers the 6-month period of 1 January– 30 June 2001. The content, however, for purposesof context and comparison, is presented in a 12-month timeframe, the period when theorganisation operated as Hutt Valley HealthCorporation as well as its present form of HuttValley DHB.
The year has been one of significant change,exciting development and continuing, excellentperformance. Despite time and resource constraints,Hutt Valley DHB met all significant establishmentfunding and capability milestones outlined in theTransitional Crown Funding Agreement with theMinister of Health. Furthermore the organisationmanaged to achieve a year-end financial surplusof $2.098 million which was the largest operatingsurplus within the sector. Given the cost pressureswithin the sector during this period, the result is indeed an excellent achievement.
These pleasing results have been accomplishedagainst a background of other organisationalimprovements, particularly in the area of quality.Hutt Valley DHB is the first district health boardto be awarded full accreditation of the servicesit funds, plans and provides by Quality HealthNew Zealand. The accreditation survey teamnoted that “outstanding leadership has resultedin the development of an organisational culturecharacterised by openness, empowerment ofstaff, clinical and managerial co-operation,customer focus and learning”.
For the services provided by the Hutt Valley DHB,it was pleasing to achieve and, in many areas,exceed our service targets. Once again there hasbeen an increase in inpatient hospital treatmentsand discharges over the past year by 4.0%. There has also been a further increase in daycasedischarges of 12.6%, inpatient operations of 3.4%,laboratory tests of 5.9% and outpatient attendances
of 1.6%. At the Hospital’s Emergency Department,32,000 people were given care, 7% more than theDHB was contracted to treat. This past year morehealth services have been delivered by theorganisation than ever before. This has beenimportant and has ensured that waiting lists arekept at acceptable levels and within nationalguidelines.
The transition to a District Health Board has beena most exciting development, which has broughtnew responsibilities and challenges as we prepareto better meet the health needs of our community.This has required a change in the way we manageour activities; it has required us to refocus ourpriorities. The past 6 months have largely beena period of building capability with the putting inplace of the additional staff, systems and functionsrequired to take on the new responsibilities. It hasincluded the appointment of staff to the Fundingand Planning team of the DHB. This team willprovide the necessary advice to ensure the Boardcan undertake the important functions of needsanalysis, service planning, contract monitoringand health service prioritisation. The DHB hasalso increased its ability to consult and tocommunicate with our community in a genuineand meaningful way. During the 6-month perioda number of provider forums and communitymeetings were undertaken to better inform ourcommunity of these key changes.
With regard to those services the Hutt ValleyDHB provides, we have also better defined theresponsibilities of our two major group operations.Hospital and Secondary Services will focus onthe acute services of the provider arm of theDHB, while Public Health, Primary, Communityand Mental Health services will be managed as afurther grouping which have the objective ofimproving peoples’ health and avoiding the needfor in-patient hospital stay.
12
Hu
tt V
alle
y D
istr
ict
Hea
lth
Bo
ard
Ch
ief
Exec
uti
ve’s
Rep
ort
Total Discharges
2000/011999/200001998/991997/981996/97
30,000
25,000
20,000
15,000
10,000
5,000
0
Waiting List
2000/011999/200001998/991997/981996/97
2500
2000
1500
1000
500
0
Chief Executive’s Report

I would also like toacknowledge, in thisYear of the Volunteer,the very significant contribution that volunteersmake to the provision of care within ourcommunity. Their ongoing support has beenfantastic and is always greatly appreciated bythe patients and staff alike.
Finally, on a personal note, I was delighted to beappointed earlier this year as the Chief Executiveof the Hutt Valley DHB. I strongly believe thatthe DHB environment offers new opportunitiesfor improvement, integration, understandingand co-operation that have not existed previously.I look forward to working with all the providerswithin the Hutt Valley, with our staff andimportantly with our community to collectivelystrive and meet our vision of “being New Zealand’sforemost District Health Board in optimising thehealth and wellbeing of our community”.
Stephen McKernanChief Executive
13A key priority and an area that we need to improveon is the area of human resources and in particularstaff retention and development. Our HumanResources team has implemented a number of projects that are designed to enhance careerdevelopment opportunities, recruitment andretention initiatives and leadership development.These issues affect the health sector as a wholeand addressing them is a key priority for HuttValley DHB. It is pleasing to note the positiveimprovements already being realised by theseprojects.
This year also saw a strengthening of ourpartnership with Maori health providers.Relationships between the DHB and Maoricommunities are strong. We have supported anumber of Maori provider developmentprogrammes, such as the Tamati Whaangaiprogramme, Tu Tangata and Maori Health ProviderCapacity Building initiatives, and will encouragefurther development of Maori Community healthservice initiatives. These programmes help meetthe Board’s priorities of effectively engaging withMaori, ensuring access to services by Maori, and addressing disparities in health outcomes in a meaningful and enduring way.
While the year has been exciting, it has also beenchallenging and I wish to acknowledge thecontribution that the staff have made. Despitethe pressures inevitably associated with change,the staff at the DHB have loyally, diligently andprofessionally carried out their responsibilitiesand provided a very high standard of service toour community. I want to thank them for theirsupport and tireless effort. Their contributionhas made this year’s excellent result possible.
Hu
tt Valley D
istrict Health
Bo
ardC
hief Execu
tive’s Rep
ort
“The year has been one of significant change, exciting development andcontinuing, excellent performance.”
Executive Management Team (back row, left to right): Rob Eaddy (GM Communications), Martin Hefford (GM Funding and Planning),Justin Te Rangiita (HR Manager), Warrick Frater(GM Hospital and Secondary Services), David Williment (Board Secretary), Sam Bartrum(GM Public, Primary, Community and MentalHealth), Trevor Coad (Chief Financial Officer).Front row, left to right: Kuini Puketapu (Maori Health Advisor), Stephen McKernan (Chief Executive), Pam Doole (Director of Nursing),Dr Robert Logan (Director of Medicine).

15
Hu
tt Valley D
istrict Health
Bo
ardService H
igh
ligh
ts
The following service reports cover the full 12-month reporting period which incorporatesthe organisation’s functions both as Hutt ValleyHealth and Hutt Valley DHB.
SurgicalThe Hutt Valley DHB surgical service has continuedto develop in line with contract, waiting listrequirements and quality enhancement.
The redevelopment of the Regional Plastics Serviceafter the sudden death of Mr. Max Lovie has beena challenge to the people working in that specialty.Achievements to date have been remarkable underthe circumstances, and the service developmentsare a credit to the specialists and professionalsworking in that field.
Highlights for the surgical service this past yearinclude:
• The completion of the site optimisation projectfor the orthopaedic, gynaecology and generalsurgical wards
• The commencement of the site optimisationproject for a new facility for the generalsurgical and gynaecological outpatientsdepartment
• The commencement of the site optimisationproject for the plastics ward and a plasticsoutpatient facility
• The change in process management for plasticpatients in the area of cleft lip and palate, andvascular anomalies – laser surgery is at theleading edge of technology and provides a topquality service.
• Achievement of contract volumes which again have increased over previous years.
To enable surgical services to meet core contracttargets and booking system requirements,caseweights in gynaecology and orthopaedicswere contracted out to Boulcott Clinic; the ongoingrelationship and development of new initiativesand responsibilities has provided opportunitiesand challenges to both organisations. The ACCcontract is now a joint venture between BoulcottClinic and Hutt Valley DHB. Following clinicalassessment, patients are admitted to the mostappropriate hospital for surgery.
MedicalOver the last 12 months the two most significantevents for the medical service have been:
• The site optimisation project, with the combiningof two medical wards into one and thealignment of the cardiology and rheumatologyinpatient and outpatient services to theHeretaunga block, and
• The successful accreditation survey.
The combined medical ward utilises a 54-bedspace and has required significant staffreorganisation to make it effective. A changemanagement process was implemented to reviewprevious work arrangements and to meet thechallenges of operating a 54-bed unit.
Quality improvement has continued to be a majorfocus. A senior medical consultant has beenappointed as the quality representativesupervising clinical audit and taking a lead rolein quality initiatives. This includes the review ofclinical documentation requirements for themedical service and other initiatives agreedwithin the service quality committee.
The number of patients admitted has continuedto exceed contracted volumes. The service, inresponse to those demands, introduced two nursespecialist roles focusing on respiratory andcardiac ailments, these being the most commonclinical conditions admitted to the service. Thisinitiative has been very successful in achieving areduction of length of stay and readmission ratefor these conditions as well as improving theservice linkages with the primary care community.
2000/011999/200001998/991997/981996/97
Acutes Total
Operations Acute & Elective
8,000
7,500
7,000
6,500
6,000
5,500
5,000
4,500
4,000
3,500
3,000
2,500
2,000
1,500
1,000
500
0
Electives
Service Highlights

16
Hu
tt V
alle
y D
istr
ict
Hea
lth
Bo
ard
Serv
ice
Hig
hlig
hts
The coronary unit has installed a state of the artcardiac monitoring system complete with mobilewireless telemetry. The service is now able tomonitor patients from the top three floors of theHeretaunga block and directly from theemergency department and the short stay unit.
Emergency DepartmentThe service provided care to 32,000 people overthe financial year, 7% more than contracted. A significant proportion are people who couldhave their care successfully managed by theirprimary caregiver. To that end the service hasestablished a project group to identifyopportunities to reduce presentations to thedepartment. The project group includes generalpractitioners, Pacific and Maori health providers,primary care nurses and managers and keyhospital staff.
The service has re-evaluated the triage and co-ordination nursing roles. This has resulted innew role specific positions with clearaccountabilities being established. The triagenurse is now located where patients first presentat the reception area of the department. Thedepartment continues to review its staff mix andskill to ensure the service has the capability tomeet the increasing demand.
Specialist Rehabilitation During the year, a new permanent geriatricspecialist was appointed, a rehabilitationphysician has returned after a year overseas andthe pyschogeriatrician time has increased inresponse to rehabilitation requirements in thepyschogeriatric age group.
Mental HealthThe Mental Health Service continues to build on the achievements of previous years andconsiderable progress has been made over thepast 12 months in meeting the goals set in the2000/01 service plan. Work is well underway inimplementing National Mental Health Standardsacross all services. The main focus has been theimplementation of the client pathway, single file,consumer participation project, whanau/familyparticipation project and meeting the standardsfor accreditation. Another key development has been the establishment of the Quality Team.This team has been active in developing andimplementing the client pathway and reviewingpolicies.
Maori Mental HealthFollowing the change in strategic directioninitiated last year, the Maori Mental Health teamhave refocused Maori mental health care. Thishas resulted in:
• Appointment of identified clinical and non-clinicalstaff – 80% of staff appointments to alcoholand drug services have been made
• Policies for alcohol and drug service beingdeveloped
• Provision of on-call cultural assessments bythe crisis team
• Community hui organised to gain communityfeedback on acceptability of both mainstreamand Maori mental health services to the Maoricommunity.
MaternityOur family-focused Maternity Unit continues tobe popular with women, their families and staff.A highlight for some staff was the Prime Timedocumentary From Here to Maternity, filmedwithin the Hutt Community and the Maternity Unit.
This year 2,117 live births were provided for, fivemore than the previous year and a 9.8% increaseon 1998/99.
8,000
7,000
6,000
5,000
4,000
3,000
2,000
1,000
0
Inpatients Daypatients Total
Daypatients vs Inpatients
2000/011999/200001998/991997/981996/97

17
Hu
tt Valley D
istrict Health
Bo
ardService H
igh
ligh
ts
Hutt Valley DHB Midwives provided 27% of theintrapartum midwifery care and the domiciliarypostnatal midwife attended 371 women and babies.
The Specialist Obstetrician Assessment andManagement Service to Lead Maternity Carers,providing expert specialist assessment and co-ordination and, if necessary, specialist teammanagement, continues to develop and be wellreceived with 751 women seen on an outpatientbasis antenatally.
Children’s HealthIt has been an exciting and challenging year forthe Children’s Health Service. The servicecontinues to concentrate on managing acutedemand in a child and family-focused manner.The addition of a qualified play therapist to thePaediatric team this year has had an extremelypositive impact on preparing, not only childrenbut also their parents with regard to a child’shospitalisation.
The Children’s Assessment Unit continues toprovide a very positive model of care for childrenand their families. 76% of children seen andassessed have avoided an inpatient admissionand were subsequently cared for in their ownhomes by our skilled team of paediatric nurses,with direct contact back to the consultantpaediatrician, or referral back to their GP.
Other strategies implemented during the yearincluded increasing the nursing resources within
the unit and the scope of the neonatal home careservice, the latter enabling some babies on oxygentherapy and naso-gastric feeding to be dischargedand managed at home earlier than had previouslyoccurred.
Regional Public HealthWith the establishment of Hutt Valley DHB, theRegional Public Health Group has assumed a moreprominent and comprehensive role, not only inthe Hutt Valley but also within the wider regionalboundaries for which it has responsibility forproviding services. The following is a summaryof the many highlights in this group over thepast year.
National Cervical Screening Programme (NCSP) – WellingtonFollowing one of the recommendations of theGisborne Inquiry on Cervical Cancer, a quarterlyauditing of the NCSP by an Independent MonitoringGroup (IMG) was established. Their first reporthas identified that Wellington has the highestenrolment in New Zealand of eligible women agedbetween 20 and 65 on the National CervicalScreening Register.
“Achievements to date have been remarkableunder the circumstances, and the servicedevelopments are a credit to the specialistsand professionals working in that field.”
1996/97
Hospital Discharges
10,000
9,000
8,000
7,000
6,000
5,000
4,000
3,000
2,000
1,000
0
1997/98 1998/99 1999/2000 2000/01
Surgical Medical Children’sHealth Maternity Specialist
RehabilitationMentalHealth

18
Hu
tt V
alle
y D
istr
ict
Hea
lth
Bo
ard
Serv
ice
Hig
hlig
hts
Within the Maori Cervical screening programme,all Maori Health Provider sub-contract objectivesfor the year were met or exceeded. A Mana WahineStrategic Hui was held in July 2001 at which sixMaori Health Providers from across the regionwere represented. Mana Wahine and RegionalPublic Health facilitated two training workshopsduring the year for new Maori communityeducators in the areas of cervical and breastscreening health promotion.
The alignment of the Pacific Cervical Screeningprogramme with Regional Public Health’s PacificPeoples’ Programme has resulted in co-ordinationthat is strategically and operationally responsiveto national and regional Pacific health goals andobjectives as developed by the Ministry of Healthand Ministry of Pacific Island Affairs.
Communicable DiseaseThe Communicable Disease programme continuesto ensure prompt follow up of notifiable diseasein order to prevent its spread. Of particularpriority for the Wellington Region has been thecontrol and management of tuberculosis andmeningicoccal disease. All cases are immediatelyfollowed up, with contacts screened and whereappropriate supplied with preventative medication.
Further work was undertaken with LocalAuthorities to clarify the respective roles andresponsibilities of Regional Public Health andLocal Authorities in disease follow up. A servicelevel agreement has been developed to supportthis.
Food Safety and QualityEnsuring food safety and quality remains a keyobjective of public health. This past year sawthe toxic algae Gymnodinium catenatum reachthe Wellington coastline. The samplingprogramme revealed levels of the toxin abovethe statutory maximum and the public wereinformed that it was unsafe to collect shellfishfrom these areas.
In January the Ministry of Health implementedan import suspension on beef and beef productsfrom the European Union. This was a precautionaryresponse following the confirmation that BSE hasbeen found in European cattle herds.
Mental Health PromotionTo promote Mental Health Awareness Week andsupport the national anti-discrimination campaignan awards initiative, Awards For Respect, washeld on 12 October 2000 in Wellington. The awardsacknowledged respectful, understanding andsupportive people in the community. Awards ForRespect were presented to nine recipients whowere selected from 42 nominations. The awardswere presented by the Hon Ruth Dyson; Kaumatuapresented awards to Maori recipients.
Health InformationThere are numerous highlights from the past yearin Health Information, from the appointment of a new co-ordinator, to the development of a national resource, and through to the moreproactive focus of the Health Information team.Several resources developed by Regional PublicHealth have, since their production, been addedto the national health information catalogue. In April, the ‘Be Active Everyday’ pamphlet, whichlooks at physical activity, joined the ‘Be ActiveEveryday’ poster, also developed by RegionalPublic Health, as a national resource.
One of Regional Public Health’s more impressiveresource development achievements has beenthe production of the Dental Health and Fluoridepamphlet. The Ministry of Health commentedthat the proposal for this resource was the bestthey had received from a regional provider andrequested that Regional Public Health developthe resource at a national level.
Health Promoting SchoolsThe local Health Promoting Schools programmehas now successfully completed its first year of operation. An initial introduction to HealthPromoting Schools (funded directly by theMinistry of Health) was held in August 2000 forRegional Public Health Public Health Nurses,Health Promoters, and other community healthproviders. Twenty schools have now taken partin implementation workshops facilitated byRegional Public Health with assistance from othereducation and health providers. By 30 June 2001twelve schools had committed to the HealthPromoting Schools process with others planningimplementation in 2002. Programme activityincludes sports injuries, nutrition, mental healthpromotion, sun smart and environmental safety.
19
Hu
tt Valley D
istrict Health
Bo
ardService H
igh
ligh
ts
Pacific Peoples’ HealthOur Children Our Future, the first ever Pacific roadsafety video made by the community for thecommunity, was launched this year to anenthusiastic reception. This was an intersectoralinitiative with the Land Transport Safety Authoritybeing the primary sponsor.
The video features three stories set around aPorirua Pacific family and the dangers childrenface on the roads. It grew out of a need identifiedby caregivers in Porirua for a resource whichwould capture the attention of people caring forPacific children and help stimulate discussion of child road safety issues. It will be used as aresource by the seven community educatorsemployed by Regional Public Health’s PacificPeople’s Health programme, who work throughoutthe Wellington region.
Alcohol and SmokefreeWorld Smokefree Day with its theme ‘Let’s clearthe Air’ was a highly successful promotion of the Alcohol, Tobacco and Other Drugs team thisyear. A wide range of activities was carried outthroughout the region. Supporting communityorganisations such as marae, schools andkohanga reo through the provision of Smokefreesponsorships was another highlight this year. As part of a tripartite relationship betweenRegional Public Health, the Health SponsorshipCouncil and the community the programme wasable to secure $45,000 in sponsorship funding.The sponsorships, which were for Auahi Koreand Smokefree resources, were used in variousways ranging from health days through tosponsoring sports teams and supporting schoolsto become Smokefree.
A further achievement for Regional Public Healththis year was the release in August 2000 of theirCannabis and Youth report. This report was theresult of a study undertaken by Regional PublicHealth to ascertain the usage of cannabis byyoung people in Kapiti and Wairarapa.
Community DentalOver the past year, the Community Dental Service(School Dental Service and Hospital Dental Service)continued to work towards improving the oralhealth of the people of Hutt Valley through thedevelopment and integration of a preventativeapproach to delivering oral health care. This hasbeen facilitated through integrated delivery ofcare on a regional basis across Wellington. The use of mobile dental units, along with anindividualized risk assessment treatment approachto the provision of care, has ensured that theoral health statistics for children in the regionremains the best for the country. The currentand ongoing workforce issues regarding dental
“By 30 June 2001 twelve schools had committed to the Health Promoting Schools process with othersplanning implementation in 2002.”

clinicians, and in particular the national shortageof dental therapists, continue to challenge theability of the service to deliver care in a timelyfashion. Plans are in place to ensure this doesnot negatively impact on patient care.
Clinical SupportThis year has continued with the focus on qualityimprovement with each service establishing keyquality projects and initiatives. Of significanceare the Diagnostic Radiology Services achievingIANZ accreditation status. Our department is oneof only four hospital-based radiology services to have achieved this. The success is a credit tothe investment made by the project team and allstaff to ensure documentation and systems arein place to meet the accreditation standards.
Progress has continued on upgrading andimproving facilities. Pharmacy has been relocatedfrom the ground floor to the first floor of theHeretaunga Block in a newly refurbished area.
The vacant ground floor space is currentlyundergoing refurbishment to extend the GeneralOutpatients Clinics. The new facility will includeeight additional consulting rooms, four of whichwill be dedicated to Women’s Health, along withtwo procedures rooms. The new CommunitiesBuilding is near completion with the third floorset to house both Community Health NursingServices and Social Work. The design has movedaway from the traditional office setting to a moreopen plan approach. The Staff Library is now partof the newly created New Zealand HospitalDatabase Consortium. This includes 12 districthealth boards and the Ministry of Health. The consortium provides access to health sciencedatabases to obtain information for qualitypatient care. Staff can access these services fromthe library, their desktop or a remote locationvia computer link up.
20
Hu
tt V
alle
y D
istr
ict
Hea
lth
Bo
ard
Serv
ice
Hig
hlig
hts

21Maori Health The DHB’s Maori Health Advisory Unit continuesto provide support and advice across theorganisation at all levels. An example of this isthe follow up work undertaken with the FractureClinic to track Maori patients who are notattending outpatient clinics. The wide whanau andDHB network that exists in the Hutt Valley andWairarapa has assisted the Unit to locate patientsand/or whanau and to ensure that attendance at future appointments are maintained. The Unitcontinues to develop and ‘fine tune’ the wardrounds. This entails visiting most inpatients whohave self identified as Maori on admission. A report is generated daily and visits are made.The purpose of the visit is to ensure the whanauare aware that a support Unit is on site and thatthe Whanau House, Te Hauone, is also availablefor accommodation at a reasonable cost. Staff willtake time to talk with whanau and ensure that allservices available to them from within the DHBare accessed.
The Maori Policy Taskforce continues to meet todevelop organisational policy and to critiqueand provide input into service level protocols andpolicy. Input was provided to the Maternal Healthguidelines regarding use of Rongoa (traditionalMaori medicine) and its complementary role toservices provided.
Maori community relationships are strong. HuttValley DHB provides support to the developmentof Maori community schemes such as the TamaitiWhaangai programme, Tu Tangata and MaoriHealth Provider Capacity Building. Initiativessuch as sharing of training opportunities,provision of staff support in management andadvice, sharing of office space and a generalcloser working relationship have assisted inensuring relationships are well managed andsupportive of one another.
Hu
tt Valley D
istrict Health
Bo
ardService H
igh
ligh
ts
“Of significance are the Diagnostic Radiology Servicesachieving IANZ accreditation status. Our department is one of only four hospital-based radiology services to have achieved this.”
22
Hu
tt V
alle
y D
istr
ict
Hea
lth
Bo
ard
Serv
ice
Hig
hlig
hts
Quality and RiskAs noted in the Chairman’s Report, Hutt ValleyDHB was the first district health board to achievefull accreditation for the quality of services itprovides. The 3-year accreditation status, achievedin March, gives assurance to the public that theservices they receive from Hutt Valley DHB meetor exceed the highest quality health and disabilitystandards available in New Zealand. Steadyprogress was also made in meeting Ministry ofHealth guidelines for event reporting. In promotinga culture of safety, mechanisms have beendeveloped to help identify the factors contributingto safety incidents as well as enabling preventativeaction to be taken.
During this period, a risk and performancereporting system has been developed whichprovides Hutt Valley DHB with the ability to linkour identified risks, be they clinical, legal oradministrative, to our key performance indicators.

23
Hu
tt Valley D
istrict Health
Bo
ardService H
igh
ligh
ts
1996/97 1997/98 1998/99 1999/2000 2000/2001 2000/01 2000/01– 1999/00 – 1996/97
Var % Var %
Inpatient discharges 15,339 16,013 16,145 16,968 17,040 0.4 11.1
Daycase discharges 4,163 4,578 5,331 6,948 7,823 12.6 87.9
Total discharges 19,502 20,591 21,476 23,916 24,863 4.0 27.5(incl newborns)
Discharges per day 53.4 56.4 58.8 65.3 67.9 4.0 27.1
Available bed days 108,936 104,399 91,052 85,805 89,718 4.6 -17.6(incl cots)
Occupied bed days 89,670 86,473 75,597 75,614 78,864 4.3 -12.1
Average occupancy 82.3% 82.8% 83.0% 88.1% 87.9% -0.3 6.8
Inpatient operations 3,550 3,865 4,408 4,848 5,015 3.4 41.3
Daypatient operations 1,653 1,754 2,298 2,214 2,444 10.4 47.9
Total operations 5,203 5,619 6,706 7,062 7,459 5.6 43.4(theatre cases)
Elective operations 2,363 2,705 3,391 3,504 3,822 9.1 61.7
Acute operations 2,840 2,914 3,315 3,558 3,637 2.2 28.1
Total operations 5,203 5,619 6,706 7,062 7,459 5.6 43.4
Waiting list total at 30 June 2,176 1,979 1,146 873 868 -0.6 -60.1
Outpatient Attendances
- Surgical 23,909 30,268 29,363 31,163 31,644 1.5 32.4
- Medical 12,761 13,212 15,045 14,901 15,411 3.4 20.8
- Paediatric 3,922 4,045 3,978 4,365 4,207 -3.6 7.3
Emergency Department
- First attendances 27,065 28,154 27,308 28,888 30,259 4.7 11.8
- Total attendances 28,317 29,678 28,735 30,558 31,986 4.7 13.0
Community Contacts
Community contacts – district nursing 41,458 41,356 30,691 34,772 41,063 18.1 -1.0
Births – Hutt Hospital 2,042 1,987 1,928 2,112 2,117 0.2 3.7
School entrant initial 6,182 5,670 6,765 6,187 6,270 1.3 1.4pure tone audiometry
Radiology examinations 43,112 44,531 45,638 47,839 48,202 0.8 11.8
Laboratory tests 692,624 741,647 518,503 563,600 596,983 5.9 -13.8performed
Summary of Service Provision Over Five Years

25
Hu
tt Valley D
istrict Health
Bo
ardFin
ancial Statem
ents
2001
For the six months ended 30 June
Financial Statements
Hu
tt V
alle
y D
istr
ict
Hea
lth
Bo
ard
Rep
ort
fo
r th
e si
x m
on
ths
end
ed 3
0 Ju
ne
20
01