human resources for health plan 2015 draft - who.int · strategy 4.1 appropriate hr policies in...
TRANSCRIPT

January 2012
Human Resources for Health
Strategic Plan 2011 2015
Draft


i
TABLE OF CONTENTS
List of Tables v
Acronyms vi
Foreword ix
Acknowledgements x
Section 1 Introduction 1Background 1Development of the Plan 1
Section 2 The Health Sector 5Introduction 5National and Health policy frameworks 5
The Interim Constitution of Nepal 2007 5The National Health Policy 1991 520 year Second Long Term Health Plan (SLTHP) 1997 2017 6Free Health Care Policy 6Three Year Plan 6The Nepal Health Sector Programme (NHSP) 6The Health Services Act (1997) 7
Health financing 7Decentralisation 8Health goals and outcomes 9Health status 10Service delivery structures and mechanisms 12Referral system 13Public private partnership 13Health service providers 14
Government health providers 14Private/for profit health service providers 14NGO/non profit health providers 15
Future service delivery plans and priorities 15
Section 3 HRH Situation Analysis 17Introduction 17Guiding policies, plans and strategies 17
The Health Services Act 1994 18The 2003 2017 Strategic Plan for Human Resources for Health 18NHSP 2004 2010 18NHSP 2 2010 2015 19
Staffing levels 21Vacancies/shortages in public sector facilities 26Workforce Characteristics 28

ii
Recruitment and attraction 28Distribution 29Health workforce attrition and retention 32Health worker performance 33Productivity 36Absenteeism 37
Performance management systems 38Basic and pre service training 39Post basic and in service training 42HR functions, systems and capacity 44
HR information systems 46Projecting HRH requirements and workforce planning 48
Preliminary Projections 52
Section 4 Aim, Outputs, Strategies & Activities 56Aim Of The HRH Strategic Plan 56
Output 1: Appropriate Supply Of Health Workers For Labour Market Needs 57Strategy 1.1 Improve HR Planning For The Health Sector 57
Rationale 57Activities 58
Strategy 1.2 Improve Recruitment And Deployment Processes And Ensure They AreEffective And Timely 58
Rationale 58Activities 60
Strategy 1.3 Improve Attractiveness Of Jobs For Increased Recruitment And Retention60
Rationale 60Activities 61
Strategy 1.4 Ensure Basic And Pre Service Education And Training Is In Line WithRequirements For The Health Sector 61
Rationale 61Activities 62
Output 2 Equitable Distribution Of Health Workers 63Strategy 2.1 Review Current Distribution Trends And Processes And EnsureDeployment Systems Result In Equitable Distribution Of Health Workers 63
Rationale 63Activities 63
Strategy 2.2 Make Jobs/Postings In Rural And Remote Areas More Attractive To RetainHealth Workers 64
Rationale 64Activities 65
Strategy 2.3 Prepare And Support Staff Better For Working And Living In Remote Areas65
Rationale 65Activities 66

iii
Strategy 2.4 Improve Workers�’ Living And Social Conditions In Remote Locations 66Rationale 66
Activities 66Strategy 2.5 Compulsory Service To Improve Rural Service Provision 67
Rationale 67Activities 67
Strategy 2.6 Continue And Identify New Areas For Task Shifting And Alternative StaffingIn Clinical Areas (E.G. Anaesthesia, Ultrasound Etc.) 67
Rationale 67Activities 68
Strategy 2.7 Use NGOs And Private Health Providers For Service Delivery In MostDifficult Areas 68
Rationale 68Activities 68
Output 3: Improved Performance Of Health Workers 68Strategy 3.1 Provide Staff With Leadership And Clear Direction 68
Rationale 68Activities 70
Strategy 3.2 Strengthen Skills/Capacity Of Health Workers To Do Their Jobs 70Rationale 70
Activities 71Strategy 3.3 Ensure Effective Reward And Sanction Systems In Place 72
Rationale 72Activities 72
Strategy 3.4 Reduce Staff Absence From Assigned Posts 72Rationale 72
Activities 73Strategy 3.5 Ensure Staff At All Levels Have An Enabling Work Environment 73
Rationale 73Activities 73
Strategy 3.6 Strengthen Teamwork Approaches 73Rationale 73
Activities 73Output 4 Effective And Coordinated HR Management And Development Across The HealthSector 73
Strategy 4.1 Appropriate HR Policies In Place 73Rationale 74
Activities 74Strategy 4.2 Appropriate Organisational Structures, Systems And Capacity DevelopedTo Support The HR Functions 74
Rationale 74Activities 75
Strategy 4.3 Effective Coordination Mechanisms In Place At All Levels Within TheHealth System 75

iv
Rationale 75Activities 76
Section 5 Implementation of the Plan 77Introduction 77Risks and assumptions 77Implementation arrangements 78
Annual Implementation plans 79Monitoring and Evaluation of the Plan 79Costing and financing the HRH Strategic Plan and health Workforce Plan 79
Annex 1 Technical Working Groups (TWG) Membership 81
Annex 2 Strategies, Activities and sub activities 83
Annex 3 Stakeholders that received and/or reviewed the draft HRH Plan 99
Annex 4 Budget 101
Annex 5: Existing Ayurvedic Workforce 2011 102
v
List of Tables
Table 1 Health Indicators........................................................................................................................10
Table 2 Main causes of morbidity and mortality....................................................................................11
Table 3 Public and prIvate health facilities and institutions...................................................................12
Table 4 Number of health facilities in the public sector 1991 2011 ......................................................13
Table 5 NHSP 2 Proposed HRH interventions ........................................................................................20
Table 6 Registered medical doctors December 2010.............................................................................21
Table 7 Medical Specialists registered with Nepal Medical Council.......................................................22
Table 8 Registered Nurses July 2011 ......................................................................................................22
Table 9 Registered Health Professionals July 2011 ................................................................................23
Table 10 Health Professionals with permanent registration July 2011..................................................23
Table 11 Doctors in the public and private sectors 2011 .......................................................................24
Table 12 Human resources for health in the public and private sector 2011 ........................................25
Table 13 Ratio of doctors and nursing/midwifery staff to population ..................................................26
Table 14: MoHP sanctioned and filled posts 2007/08............................................................................27
Table 15 Distribution of government health facilities by development region......................................30
Table 16 Distribution of health facilities in the public sector by geographic region 2008 .....................30
Table 17 Public sector staff in sanctioned posts, appointments and resignations ................................33
Table 18 Causes of absenteeism among public health workers 2008....................................................38
Table 19 Medical Colleges 2011 .............................................................................................................40
Table 20 Annual intakes to Nursing Training Programmes 2007/8........................................................41
Table 21: Units of the MoHP involved in HRH........................................................................................45
Table 22: Posting and transfer authority by level of institution.............................................................45
Table 23 Proposed HRH requirements ...................................................................................................51
Table 24 Preliminary projections 2011...................................................................................................54
Table 25 Example of assumptions associated with the strategies .........................................................78

vi
Acronyms
AA Anaesthesia AssistantAHP Allied Health ProfessionalAHW Auxiliary Health WorkerAIDS Acquired Immune Deficiency SyndromeANC Ante Natal ClinicANM Auxiliary Nurse MidwifeASRH Adolescent Sexual and Reproductive HealthAWPB Annual Work Plan and BudgetBCC Behaviour Change CommunicationBME Bio Medical Equipment TrainingBOR Bed Occupancy RateBPKIHS B.P. Koirala Institute of Health SciencesCCF Country Coordination and FacilitationCEOC Comprehensive Emergency Obstetric CareCME Continuing Medical EducationCPD Continuing Professional DevelopmentCPR Contraceptive Prevalence RateCSO Community Service OrganisationsCTEVT Council of Technical Education and Vocational TrainingDHO District Health OfficerDPHO District Public Health OfficeDoCPR Department of Civil Personnel RecordsDoHS Department of Health ServicesEDP External Development PartnerEHCS Essential Health Care ServicesEPI Expanded Programme on ImmunisationFCHV Female Community Health VolunteersFP Family PlanningFY Fiscal YearGESI Gender Equality and Social InclusionGoN Government of NepalHA Health AssistantHDI Human Development IndexHFMC Health Facility Management CommitteeHIV Human Immunodeficiency VirusHMIS Health Management Information SystemsHP Health PostsHR Human ResourcesHRH Human Resources for HealthHRP/M/D HRH Planning, Management and DevelopmentHRM Human Resource ManagementHuRIS Human Resource Information SystemINGO International Non Governmental OrganisationIST In Service TrainingIT Information TechnologyLATH Liverpool Associates in Tropical HealthM&E Monitoring and Evaluation

vii
MBBS Bachelor of Medicine Bachelor of SurgeryMCH Maternal Child HealthMCHW Maternal and Child Health WorkerMD Medical DoctorMDG Millennium Development GoalMDGP Medical Doctors General PracticeMISP Minimum Initial Service PackageMMR Maternal Mortality RateMNCH Maternal Neonatal Child HealthMoGA Ministry of General AdministrationMoHP Ministry of Health and PopulationMoLD Ministry of Local DevelopmentMoU Memorandum of UnderstandingNCDs Non communicable DiseasesNDHS National Demographic and Health SurveyNGO Non Governmental OrganisationNHSP Nepal Health Sector ProgrammeNHSP IP Nepal Health Sector Programme Implementation PlanNHTC National Health Training CentreNRs Nepali RupeesNSI Nick Simons InstituteO&M Operations and ManagementOPD Out Patient DepartmentORC Outreach ClinicsOT Operation TheatreOTTM Operation Theatre and Technical ManagementPIS Personnel Information SystemPHC Primary Health CarePHCC Primary Health Care CentrePSC Public Service CommissionPST Pre Service TrainingPPP Public Private PartnershipRHTC Regional Health Training CentreSAS Safe Abortion ServiceSBA Skilled Birth AttendantsSLTHP Second Long Term Health PlanSHPs Sub Health PostsSTS Service Tracking SurveySWAP Sector Wide ApproachTB TuberculosisTC Technical CommitteeTIS Training Information SystemToR Terms of ReferenceTU IOM Tribhuvan University Institute of MedicineTWG Technical Working GroupsUN United NationsUNDP United Nations Development ProgrammeUSD US DollarsVDC Village Development Committee

viii
VHW Village Health WorkerWHO World Health Organisation
Exchange Rate December 2011
Rs 100 = USD 1.2

ix
Foreword

x
Acknowledgements

1
Section 1 Introduction
BACKGROUND
There is a diverse range of factors that influence the Human Resources for Health (HRH)situation in Nepal. On the demand side factors influencing the demand for human resourcesinclude evolving health service requirements; new and emerging diseases; infrastructuraldevelopment; population and changes in the distribution of population; and newtechnologies. Supply side factors that influence the availability of health workers include thenumber and type of health workers produced through the education and training system;labour market dynamics; private and Non Governmental Organisation (NGO) participation inservice delivery; and the flow and movement of health workers.
Global initiatives are influencing HRH policies and plans, such as the MillenniumDevelopment Goals (MDGs), the World Health Organisation (WHO) Global Code of Practiceon the International Recruitment of Health Personnel1 and Global Policy Recommendationson 'Increasing access to health workers in remote and rural areas through improvedretention'.2 Key national policies, plans and legislation that impact on HRH include NationalHealth Policy 1991, Civil Service Act 1993, Health Services Act 1997, the 20 year SecondLong Term Health Plan (SLTHP) for FY 1997 2017, Local Self Governance Act 1998, the 20032017 Strategic Plan for Human Resources for Health, the Nepal Health Sector Programme(NHSP) 2004 �– 2010, Good Governance Act 2007, Interim Constitution, 2007, the Three YearPlan (2010/11 �– 2012/13)3 and the NHSP 2 2010 �– 2015.4 In addition the evolvingdecentralisation and federalism process will have implications for future HRM policies andsystems.
In developing the HRH Strategic Plan these developments, opportunities and challengeshave been taken into consideration. The Plan provides an analysis of the current HRHsituation in Nepal and presents strategies and activities for addressing current and futureHRH issues and challenges.
DEVELOPMENT OF THE PLAN
The NHSP 2 identifies a number of HRH challenges and constraints that are affecting thedelivery of health services and the achievement of health outcomes. It proposes a range ofstrategies and issues to address these challenges in the 5 year plan period. It recommends
1 http://www.who.int/hrh/migration/code/practice/en/2 WHO (2010). Global Policy Recommendations Increasing access to health workers in remote and rural areas throughimproved retention. WHO, Geneva.3 Government of Nepal National Planning Commission (2010). Three Year Plan Approach Paper (2010/11 2012/13)4 Ministry of Health and Population Government of Nepal (2010). Nepal Health Sector Programme Implementation Plan II(NHSP IP 2) 2010 �– 2015 Final Draft 18 March 20

2
that the staffing projections made in the 2003 Strategic Plan for HRH5 be reassessed in lightof the evolving political, policy and health environment.
In 2010 the Ministry of Health and Population (MoHP) established a Country Coordinationand Facilitation (CCF) mechanism and began developing a new and updated HRH StrategicPlan (2011 2015) to address some of the long standing HRH problems. The MoHP adoptedthe 2009 Global Health Workforce Alliance�’s CCF principles and process to guide thedevelopment process.6
At the start up workshop with key MoHP officials and other stakeholders in November 2010five key HRH problem areas and issues were identified:
Shortages of HRH as a result of imbalances between supply and demand Maldistribution of staff, especially in remote and rural areas Poor staff performance, including productivity, quality, and availability Fragmented approaches to human resource planning, management and
development HRH Financing
Workshop participants agreed that these would be the priority areas to be addressedthrough the new HRH Strategic Plan. A Technical Committee (TC) and five Technical WorkingGroups (TWGs) (see Annex 1 for membership) were formed to coordinate inputs anddevelop the HRH Strategic Plan. Participants agreed that a longer term Health WorkforcePlan and HRH projections would be developed once more comprehensive information onthe health workforce were available. The Workforce Plan will be developed during Year I ofthe implementation of the HRH Strategic Plan.
Participants agreed on a road map to guide the Plan development process. This includedfurther data collection and analysis by the five TWGs and consultations with the TechnicalCommittee and the wider CCF membership.
In March 2011 the TWGs reported on progress to a meeting of the TC, chaired by theSecretary, Dr Mishra.7 The process of developing the Plan was endorsed and the followingfeedback provided:8
The Plan will be for four years, from mid 2011 to mid 2015, to coincide with the endof the Nepal Health Sector Programme (NHSP 2)
Both public and private sectors should be included in the Plan, but it should be clearwhich strategies relate to which sectors9
5 Ministry of Health (2003). NEPAL Strategic Plan for Human Resources for Health 2003 2017.6 Country Coordination and Facilitation (CCF) Principles and Process on human resources for health (HRH) for an integratedhealth workforce response7Bista, B. G. (2011). Human Resources for Health: the process of developing HRH strategic plan status reporting (4 March2011), NHSSP.8Ministry of Health and Population (2011). Milestone 7: Periodic Review on the development of the HR Plan (Draft) Martineau,T. and Bista, B.G.

3
There will be a mixed set of planning assumptions, not based only on population10
While the problem analysis may have led to a different structure of strategies, theseshould be clearly related to the common HR areas of recruitment, retention,training, etc.
The HRH plan should be fully aligned with NHSP 2, which already includes a numberof HR strategies and other service delivery related strategies that need to besupported by the HRH Strategic Plan.
Following the meeting of the TC, the TWGs undertook further work to consolidate, prioritiseand cost the strategies and activities in the Plan.11
The draft Plan was disseminated to stakeholders for review and was revised several times toincorporate stakeholder�’s comments and feedback. It was disseminated internally within theMoHP and then to other government ministries and agencies, External DevelopmentPartners (EDPs) and CCF members (Annex 3 provides a list of stakeholders consulted). Finallyin January 2012 the draft Plan was presented and reviewed at a meeting of CCF membersand the final draft submitted to the MoHP to undergo the approval process.
The multi stakeholder consultative and collaborative processes adopted by the MoHP tosupport the development of the Plan will be maintained throughout the implementationand review phases of the Plan.12
As set out in the CCF principles, the HRH situation analysis contained in this HRH StrategicPlan is based on an analysis of information that was available, mainly on the public healthworkforce and an examination of trends within the political, socio economic, legal andorganisational context. Information on the private and NGO sectors was not available at thetime of developing the Plan but data will be collected and these data, and the findings of the2011 Service Tracking Survey and other surveys will help to produce a more comprehensiveoverview and profile of the entire heath workforce. This new information will also informthe development of the HRH component of the Annual Work Plan and Budget (AWPB) for2013 and onwards.
A more comprehensive HRH profile, including gender and social inclusion data, will becritical to enable the MoHP determine its future HRH requirements and to develop a longterm Health Workforce Plan. The HRH Information System (HuRIS) will be strengthened tosupport the workforce planning process and become a more reliable repository for HRinformation.
10These might include population growth (this has increased 35% between 1991 and 2008, while the number of health workershas increased only by 3.4%.); facility plans (upgrading of health and sub health posts and PHCCs to community hospitals),changes in service delivery (e.g. the introduction of 24/7 services in some facilities), creation or absorption of new types ofposts (e.g. anaesthetist assistants); and the absorption of contract staff to permanent positions.11 HRH Workshop Report June 25/26 201112Country Coordination and Facilitation for Human Resources for Health. Institution Capacity Building. 12th 15th July 2010,Cairo, Egypt

4
The MoHP will translate and prioritise the strategies and activities contained in the HRHStrategic Plan into costed time bound interventions that will be included in the Annual WorkPlan and Budget (AWPB).
A Monitoring and Evaluation (M&E) Plan aligned with the targets and indicators contained inthe NHSP 2 and other review and monitoring mechanisms will be developed. Indicators willbe disaggregated; gender sensitive and inclusive, and M&E information will be used tomodify strategies and activities and to inform the design of subsequent plans andinterventions.
This Section 1 discusses the context and process of developing the HRH plan. Section 2describes the current health status and contextual factors in the health environment. Ithighlights key health polices and plans that are influencing the management anddevelopment of HRH. The HRH situation analysis in Section 3 identifies and examines key HRissues, functions and challenges, including recruitment, deployment, attrition, and training.
Section 4 presents the outputs, strategies and activities that will be implemented to addressidentified HRH issues and challenges, to achieve agreed outputs and to support theimplementation of the NHSP 2. The Plan adopts a 4 year timeframe, from mid 2011 to 2015,in order to align it to the NHSP 2 timeframe; however the outputs and strategies are nottime bound and they could continue to guide HRH plans and investments beyond this initialfour year period.
Finally, Section 5 presents issues related to the implementation of the Plan such as riskanalysis, implementation arrangements, M&E systems, and budgeting and resourcemobilisation strategies.

5
Section 2 The Health Sector
INTRODUCTION
According to the preliminary results of the Population Census of 2011, the population ofNepal is 26.6 million with an annual growth rate of 1.40%.13 In 2001, 84.1% of the populationlived in rural areas and 14.2% in urban areas, but the rate of urbanisation has beenincreasing rapidly in recent years. Nepal�’s Human Development Index is 0.428 with a rank of138 out of 177 countries14 and in 2010/11 Nepal has a gross national income of US $ 261 percapita15. Twenty percent of the population live below the national poverty line.
Nepal is broadly divided into three horizontal ecological belts, namely, Mountain, Hill, andTerai. Vertically it is divided into five development regions and administratively into 75districts, which are further divided into smaller administrative units known as VillageDevelopment Committees (VDCs) and municipalities. The VDCs and municipalities arefurther divided into wards.16 At the district level, departmental or ministry offices overseeplans and programmes for that sector. The District Health Officer is responsible for all healthactivities of the district including the organisation and management of district hospital,PHCs, HPs and SHPs.
NATIONAL AND HEALTH POLICY FRAMEWORKS
Nepal has a fairly comprehensive framework of health policies, strategies and plans in place.The main components of the framework are: the National Health Policy 1991; Second LongTerm Health Plan (1997 2017); Ninth Five Year Plan (1997 2002); Medium Term ExpenditureFramework; Nepal Health Sector Programme, Tenth Plan (Poverty Reduction Strategy Paper)2002 2007; and Health Sector Strategy �– an Agenda for Reform 2004.
The Interim Constitution of Nepal 2007
Nepal has made a political commitment for the health of the people at the highest level bydeclaring �‘Basic health a fundamental right of its people�’ in the Interim Constitution of Nepal2007. The right to health is stated in 9 out of 31 proposed fundamental rights in theconstitution.
The National Health Policy 1991
The National Health Policy (1991) provides a framework to guide health sectordevelopment. It aims to extend the primary health care system to the rural population so
13 WHO Country Office for Nepal (2007) Health System in Nepal: Challenges and Strategic Options14 National Planning Commission/UNDP (2011) Millennium Development Goal Needs Assessment for Nepal 201015 Economic Survey, 2010/11 published by Ministry of Finance16 Population Division, Ministry of Health and Population (2011) Nepal Demographic and Health Survey 2011 PreliminaryReport

6
that they can benefit from modern medical facilities and services from trained health careproviders.17
20 year Second Long Term Health Plan (SLTHP) 1997 2017
The Ministry of Health and Population�’s (MoHP) 20 year Second Long Term Health Plan(SLTHP) for FY 1997 2017 guides health sector development for the overall improvement ofthe health of the population. It is based on Primary Health Care principles and aims toimprove the health status of the most vulnerable groups.18 It defines a cost effectivepackage of Essential Health Care Services (EHCS) to address the most essential health needsof the population. It aims to provide technically competent and socially responsible healthpersonnel in appropriate numbers for quality healthcare throughout the country,particularly in under served areas.19
Free Health Care Policy
As guided by the Interim Constitution, the Government is providing essential health careservices (emergency and inpatient services) free of charge to poor, destitute, disabled,senior citizens and FCHVs in 25 bedded district hospitals and Primary Health Care Centre(PHCCs), and to all citizens at Sub Health Post (SHP)/ Health Post (HP) and PHC level. In orderto implement the Free Health Care Policy effectively, the MoHP has introduced operationalguidelines based on the new budget policy.
Three Year Plan
The Three Year Plan (2010/2011 2012/2013) seeks to establish the right of the citizen to freebasic health care services. Public health issues preventive, promotional and curative healthservices will be implemented as per the principles of primary health services.20
The Nepal Health Sector Programme (NHSP)
The MoHP�’s �‘Health Sector Reform Strategy; an agenda for reform 2004�’ is beingimplemented through the Nepal Health Sector Programme. The NHSP is a sector wideprogramme focused on performance results and health policy reforms implemented under aSector Wide Approach (SWAP), with an agreed set of performance indicators and policyreform milestones for the programme duration. The policy reform milestones are outlined inthe Nepal Health Sector Programme (NHSP) document.
There are eight outputs in the National Health Sector Programme. Three are related tostrengthening health service delivery and five are designed to improve institutional capacityand management, including human resource management. 21 The MoHP is currentlyimplementing the second Plan, the NHSP 2 (2010 2015).
17 Ministry of Health and Population (2011) Department of Health Services Annual Report 2009 201018 WHO Country Office for Nepal (2007) Policy Papers on Health, Nepal19 Ministry of Health and Population (2011) Department of Health Services Annual Report 2009 2010 p.1320 Government of Nepal National Planning Commission (2010) Three Year Interim Plan (2010/11 2012/13)21 Ministry of Health and Population (2011) Department of Health Services Annual Report 2009 2010 p. 19

7
The Health Services Act (1997)
The Health Services Act (1997) makes provisions for the management of health workersemployed by the MoHP and provides guidance on the recruitment, deployment, promotion,and discipline of health workers. Since its enactment, the Act has had a number ofamendments and appears to have a degree of flexibility that makes it responsive to adynamic and evolving health system and to a diverse and multicultural health workforce.The Act is currently in the process of amendment.
HEALTH FINANCING
The Government consistently increased the health sector�’s budget during the periodcovered by NHSP IP1, from NRs. 6.5bn in 2004 5 to NRs. 17.8bn in 2009 10. Governmentspending on health is high compared to other SEARO countries and as a result fiscal spacefor further budget expansion is very limited.
In 2009/10 the health sector share of the overall government budget was 6.24% (Rs.17.84bn), rising to 7.24% in 2011. There has been an increasing shift of funds to the 75districts and a corresponding reduction in funding to the centre. In 2009 districts receivedabout half of the total health budget directly or indirectly from central funds.
Of the total health sector budget, Rs. 13.42bn (75.20%) was allocated for the execution ofprogrammes under the Department of Health Services, of which Rs. 12.9bn (96.52%) wasallocated to the recurrent budget, and 3.48% allocated to the capital budget. The ExternalDevelopment Partners�’ contributions comprised 50.53% of the total budget underDepartment of Health Services (DoHS).
Over the past three years, the allocation of the health development budget for child andmaternal health has increased significantly and Nepal is on track to achieve MillenniumDevelopment Goals (MDG) 4, 5 and 6.22 However the substantial gains achieved in reducingchild and maternal mortality will be difficult to sustain without continued external support.
Despite the considerable improvements in the provision of health services and increasedfunding allocations to districts, public expenditure on health continues to be mainly basedon central Government financing and delivery of services. The MoHP has had littleopportunity to achieve the vision outlined in the NHSP IP 2004 2010 of a more efficient andeffective decentralised health sector, with greater utilisation of private providers to deliverservices. NHSP 2 includes plans to achieve improved governance and accountability tosustain Government and External Development Partner (EDP) support, and make the bestuse of limited resources.23
22 Ministry of Health and Population Government of Nepal (2010) Nepal Health Sector Programme Implementation Plan II(NHSP IP 2) 2010 �– 2015 Final Draft 18 March 2010 p. 2223 Ministry of Health and Population Government of Nepal (2010) Nepal Health Sector Programme Implementation Plan II(NHSP IP 2) 2010 �– 2015 Final Draft 18 March 2010

8
The MoHP is currently developing a Health Financing Strategy and the budget emphasis is onimproving accessibility to health services, especially by remote and vulnerable groups andon the health of children and pregnant mothers.24 According to the DoHS 2011 AnnualReport,25 more funds will be provided to the social welfare sectors, including health and thepresent health budget will be increased. However, further budget expansion to financehealth workforce expansion plans will very much depend on the fiscal space available.
DECENTRALISATION
Nepal is currently transitioning from a unitary system of governance to a federal system andplanning is underway for transferring power from the centre to the sub nationalgovernment. The political and constitutional imperative of provincial autonomy in Nepal'sproposed federalist system will support the devolution of responsibility for health serviceprovision.
The broad objective underlying decentralisation is to bring government closer to the peopleand to make service delivery more effective, efficient and equitable. Decentralised healthmanagement will help to improve health service delivery with increased level of downwardaccountability, community ownership and wider coverage giving better access to localpeople, especially the poor and excluded groups.
In 2011 the MoHP submitted preliminary ideas for the future organisation of the healthsector under a federal state. Issues such as the provision and location of services and therole of the central MoHP in a federal state were explored. Further conceptualisation andconsultations on these issues will continue in 2012. There has been some progress with thedecentralisation and devolution of authority from the centre to the sub national levels.During 2004/2005 the Ministry handed over 1,433 health and sub health posts and PHCCs in29 districts to local health management committees. Semi autonomous status has beengranted to 52 of the 88 public hospitals although the extent of their autonomy varies. In FY2009/2010 about 58% of the MoHP budget was allocated directly to district programmes.
A �‘Strengthening of Local Health Governance Programme�’ designed and developed by MoHPis being piloted in 7 districts. It includes provisions for providing formula based health grantsto district and below, an increased role for local government units and other innovativeapproaches. This programme is being implemented in collaboration with MoLD, concernedDistrict Development Committees and some EDPs. Based on experiences and lessonslearned pilot districts will be further expanded in the plan period.
According to the DoHS Annual Report 2009/2010 (2066 2067), decentralisation andregionalisation will continue to be strengthened and peripheral units will be made more
24 WHO Country Office for Nepal (2007) Health System in Nepal: Challenges and Strategic Options25 Ministry of Health and Population (2011) Department of Health Services Annual Report 2009 2010

9
autonomous.26 District Health Offices (DHOs) will be given more responsibility for theplanning and management of health services from district to village levels. Increased localautonomy will be accompanied by changes in the financing, management and governance ofhealth sector institutions.27 Management structures and system will continue to evolve, asthe political process of federalisation is being agreed and adopted.
HEALTH GOALS AND OUTCOMES
The goal of the NHSP 2 is to improve the health and nutritional status of the Nepalipopulation, especially for the poor and excluded. The three objectives set out in the NHSP 2results framework are:
1. To increase access to and utilisation of quality essential health care services;2. To reduce cultural and economic barriers to accessing health care services and
harmful cultural practices in partnership with non state actors; and3. To improve the health system to achieve universal coverage of essential health
services.
Table 1 below shows the main health indicators such as life expectancy by sex, mortality bysex, by age (infant, maternal, under five), HIV/AIDS prevalence rate and safe drinking wateraccess.
26 Ministry of Health and Population (2011) Department of Health Services Annual Report 2009 201027 Ministry of Health and Population Government of Nepal (2010) Nepal Health Sector Programme Implementation Plan II(NHSP IP 2) 2010 �– 2015 Final Draft 18 March 2010

10
Table 1 Health Indicators
MDG/Impact Indicator Achievement Target1991 1996 2001 2006 2009 2010 2015
Life expectancy at birth 62 66 67.3Infant mortality (per 1,000 livebirths)
106 78.5 64 48 41 4132
Under 5 mortality rate (per 1,000live births)
158 118.3 91 61 50 5038
Maternal mortality rate (per 1,000live births)
539 539 415 281 229 229134
Immunisation coverage 81 82 90HIV prevalence among pregnantwomen aged 15 24 years
NA NA NA NA NA 0.490.35
Malaria annual parasite incidence(per 1,000)
NA 0.54 0.40 0.28 NA 0.15 Halt andreversetrend
Prevalence rate associated with TB(per 100,000 population)
N/A N/A N/A N/A N/A 244210
% with access to safe drinking water N/A N/A N/A N/A N/A 80.4 73% with access to sanitation N/A N/A N/A N/A N/A 43.0 53.0% Births attended by skilled healthworkers (MDG indicator)
N/A N/A N/A 19% 33% 3660.0
% Births in a Health Facility N/A N/A N/A 18 N/A 28 N/A% PW receiving at least 1 ANC visit N/A N/A N/A N/A N/A 87.4 N/ASource: NHSP II; DoHS Annual Report, 2009 2010; Nepal Demographic and Health Survey 2006 & 2011 and MDG NeedAssessment, 2010.
HEALTH STATUS
In spite of the transitional situation, political instability and other challenges, Nepal is likelyto achieve six of the eight MDGs by 2015. There has been steady improvement in healthoutcomes and impact and in equality of access during the first NHSP (2004 10). Nepal met orexceeded nearly all of the outcome and service output targets that were set for 2004 10,and is on track to meet the child and maternal mortality MDGs.28 In 2010 Nepal received anaward from the UN for progress towards MDG 5 and a GAVI award for progress in childsurvival (MDG 4).
Essential Health Care Services (EHCS), available and provided by the HPs, SHPs and PHCCsare free to all. At district hospitals, outpatient, inpatient and emergency services, includingmedicines, are free of charge to poor, vulnerable, and marginalised groups, and 40 essentialmedicines are free of charge to all. Institutional deliveries in government hospital andfacilities are free of charge to all women.
There was a 35% increase in new outpatient contacts in 2007 8, and increased utilisation bypoor and disadvantaged groups following the introduction of free services at PHCCs, healthand sub health posts, and targeted free services at district hospitals. During NHSP 2, several
28 Ministry of Health and Population Government of Nepal (2010) Nepal Health Sector Programme Implementation Plan II(NHSP IP 2) 2010 �– 2015 Final Draft 18 March 2010
11
services will be added to the existing EHCS package to further address reproductive andchild health problems, communicable and non communicable diseases, and improve thehealth status of Nepal�’s citizens, especially the poor and excluded.
Increasing skilled attendance at delivery is an intervention for reducing maternal mortality.Increasing percentage of deliveries attended by health workers at the national and theregional levels is a positive sign of the effectiveness of programme interventions through thedemand and supply side financing. This increase in the percentage of deliveries by healthpersonnel could also be explained by the revision of the target population.29
The proportion of births attended by a skilled provider over the last five years has nearlydoubled, from 19% in 2006 to 36%, while the proportion of babies delivered in a healthfacility has increased from 18% in 2006 to 28% in 2010.30
However there are a number of health issues that continue to cause concern, such as theprevalence of hunger and stunting and the large number of poor and deprived people inNepal.31 The delivery of quality health services in remote areas remains a challenge32 andthe health of excluded and very poor populations has not improved as expected. Mortalityand morbidity rates, especially among women and children, are high. Nepal still has asignificant challenge to meet the MDG target of 60% births attended by a skilled provider.
Many of the health problems are exacerbated by under utilisation of resources; shortages ofadequately trained personnel; underdeveloped infrastructure; poor public sectormanagement; and weak intra and inter sectoral co ordination.33
Table 2 below shows the main causes of morbidity and mortality in Nepal.
Table 2 Main causes of morbidity and mortality
Main causes of morbidity Main causes of mortalityAcute Respiratory Infection Neonatal DeathsGastritis CancerEnteric Fever SuicideChronic Bronchitis TuberculosisCancer DiabetesAccidents and InjurySource: MoHP 2011
However, the NHSP 2 will continue to build on the successes of the first NHSP and willaddress the remaining constraints, including HRH constraints, to increasing access andutilisation of essential health care services. There will be a particular focus on tackling
29 Ministry of Health and Population (2011) Department of Health Services Annual Report 2066/67 (2009 2010) p. 11330 Population Division, Ministry of Health and Population (2011) Nepal Demographic and Health Survey 2011 Preliminary Report31 Government of Nepal National Planning Commission (2010) Three Year Plan Approach Paper (2010/11 2012/13)32 Government of Nepal National Planning Commission (2010) Three Year Plan Approach Paper (2010/11 2012/13)33 http://www.mohp.gov.np Country Profile 2009

12
disparities between the wealthier population and the poor, vulnerable and marginalisedpopulations.34
SERVICE DELIVERY STRUCTURES AND MECHANISMS
The government health service operates at national, regional, zonal, district levels andbelow (e.g. PHCCs, health posts, sub health posts), as well as at community level. Ayurvedaservices are provided at all levels of the health system.
Table 3 below shows the number and location of public and private hospitals, PHCCs/HealthCentres, HPs and SHPs providing health services. There are approximately 50,000 FemaleCommunity Health Volunteers (FHCVs) supporting the delivery of services. Table 4 shows theincrease in the number and type of government facilities since 1991.
Table 3 Public and private health facilities and institutions
SN FacilityNumber Available
bedsRural Urban
1 Public Hospitals 16 79 7637
2 Public PHC 214 0 642
3 Public HP/SHP 3816 0 0
3 Private for profit Hospitals 12 93 4621
4 Medical Colleges 0 20 10576
5 Mission Hospitals 6 2 612Total 4064 194 24088
Source: MoHP 2010
34 Ministry of Health and Population Government of Nepal (2010) Nepal Health Sector Programme Implementation Plan II(NHSP IP 2) 2010 �– 2015 Final Draft 18 March 2010

13
Table 4 Number of health facilities in the public sector 1991 2011
Health Institutions 1991 2001 2004 2009 2010 2011Regional TB Centre 1 1 1 1 1 1Centres (e.g. HIV/AIDS, NHTC) n/a 4 5 5 5 5Specialty /Tertiary/Central Hospitals 7 8 13 13 13 13Ayurvedic, Homeo and UnaniHospitals 4 4 4 4 4 4Regional and Zonal Hospitals n/a 3 10 11 13 15Ayurvedic Clinics 82 275 275 288 288 288District Hospitals 65 67 65 65 65 65Rural Hospitals n/a n/a 1 2 2 3Primary Health Centres 33 193 205 213 214 214Health Posts 351 701 679 679 682 1204Sub Health Posts n/a 3129 3129 3158 3158 2636Out Reach Clinics n/a 30780 30780 30071 30071 30071Total 543 35161 35162 34505 34511 34514Source: MOHP 2011 and DOHS Annual Report 2001 02, 2008/09
REFERRAL SYSTEM
The health referral system was designed to ensure that the majority of the populationreceive public health and minor treatment in places accessible to them and at a price theycan afford. The SHP and HP are the first contact points for basic health services, as well asthe point for community based activities, such as (Primary Health Care) PHC Outreach clinicsand Expanded Programme on Immunisation (EPI) clinics. Referrals are made to each levelabove the SHP and HP to the PHCC, to district, zonal and regional hospitals, and to specialtytertiary care centres in Kathmandu. Logistical, financial, supervisory, and technical support isprovided from the centre to the periphery.35
During the timeframe of the NHSP 2, the referral system will be strengthened to ensure therural population is referred to well equipped and appropriately staffed institutions. SomeHPs will be upgraded and converted to PHCCs. Improvements will be made in theorganisation and management of health facilities at the central, regional and district levels.The referral system will be strengthened through the improved partnership with andutilisation of private sector hospitals (particularly medical colleges) for referral.
PUBLIC PRIVATE PARTNERSHIP
There are a number of successful public private partnerships operating in the health sector,especially in the areas of service delivery, and the production and training of healthprofessionals. Partnerships between public/government entities, private/commercialentities and civil society have a contribution to make in improving the health of the poor by
35 Ministry of Health and Population (2011) Department of Health Services Annual Report 2009 2010

14
combining the different skills and resources of various organisations in innovative ways.Public agencies can benefit from working in collaboration with the private sector, especiallyin areas where the sector lacks expertise and experience 36
In Nepal there is as yet no formal mechanism for public private partnerships in the healthsector, but a white paper on Public Private Partnership (PPP) has been drafted andcirculated. The Government is committed (e.g. NHSP 2 and the Three Year Plan ApproachPaper 2010/11 2012/13) to developing and strengthening policies and mechanisms topromote and regulate the participation of private, governmental, non governmental,community and co operative organisations in the provision of health services. The privatesector and NGOs will continue to be encouraged to produce and train health professionalsthat meet health sector needs and to provide health services in rural and remote areas.
HEALTH SERVICE PROVIDERS
The principal agency for the management of health care delivery and provision of healthservices is the MoHP, through the Department of Health Services DoHS, headed by theDirector General. The MoHP administers services through Regional Health Directorates andDistrict Health Offices. There are over 1,300 health management boards/committeesresponsible for the management of hospitals and other health facilities.
The private for profit and not for profit sectors health provide health services through 17NGO run hospitals, 17 eye hospitals, 87 private hospitals and nursing homes, 39pharmaceutical industries of Nepali origin and 240 foreign based pharmaceuticalcompanies, 40 diagnostic laboratories and research centres, and two radiotherapyfacilities.37
Government health providers
Government facilities provided curative services to 60% of the population in 2007 8. Over85% of clients received services from health posts, sub health posts and outreach clinics,about 10% from PHCCs, and the remaining 5% from hospitals. In 2007/08 a total of 706,128people received treatment through 291 government Ayurvedic Centres at national, regionaland district levels.
Private/for profit health service providers
The private sector has expanded over the years and includes private pharmacies, privatehospitals, nursing homes, private practitioners, and private training institutions. In 2010 itwas estimated that the sector employed around 20,000 health workers in its facilities.38
36 WHO public private partnerships for health http://www.who.int/trade/glossary/story077/en/37 Ministry of Health and Population Government of Nepal (2010) Nepal Health Sector Programme Implementation Plan II(NHSP IP 2) 2010 �– 2015 Final Draft 18 March 201038 Ministry of Health and Population Government of Nepal (2010) Nepal Health Sector Programme Implementation Plan II(NHSP IP 2) 2010 �– 2015 Final Draft 18 March 2010
15
Private hospitals are mainly located in urban areas and are used predominantly by therichest. Private sector pharmacies are widespread, providing examinations as well astreatment, and are major recipients of out of pocket spending by all income groups.Roughly 50% of the acute illness patents go to private practitioners for their treatment.However, the sector remains underutilised; the NHSP 2 suggests the government couldmake better use of private health facilities for the production and training of healthprofessionals and as practicum sites for medical students.39
There are 18 privately run medical colleges, and the private sector produces almost 90% ofall the medical doctors (MBBS) in the country, and a similar share of staff nurses.40 Duringthe timeframe of the NHSP 2, the Government is planning to improve the regulation of theprivate health training institutions in order to ensure that production meets requirements.
NGO/non profit health providers
The not for profit sector includes mission hospitals, I/NGOs, community organisations,cooperatives, and trust and philanthropic organisations. This sector is more broadly involvedin partnering with the Government of Nepal (GoN) in delivering EHCS and public healthservices. Although the contracting out of service provision and the management of facilitieshas progressed slowly, there are partnerships with NGOs in many areas, including themanagement of government hospitals, and the provision of family planning, safemotherhood, TB, and HIV/AIDS services.41 No definitive information is currently available onthe numbers of health staff employed by NGOs and other non profit health providers.
FUTURE SERVICE DELIVERY PLANS AND PRIORITIES
The government recognises that the health problems and health needs of the population inthe future will differ from those faced under the first NHSP IP. The MoHP is alreadyexploiting many of the most cost effective interventions for reducing mortality andmorbidity. Further reductions in neo natal, child and maternal deaths will require afunctioning health system able to respond to emergencies 24/7 and the ability to reachcurrently underserved populations. Tackling the problem of malnutrition will require a multisectoral approach. In this regard, a committee formed by National Planning Commission isexpected to mitigate this problem.
The burden of disease is changing, and the population will increasingly demand qualitycurative services for non communicable diseases. The percentage of aged population isincreasing and consequently there is an increasing demand for service delivery. This is anarea where public private partnerships and alternative financing mechanisms may havemore of a role to play. At the same time, technology will continue to change, and
39 Ministry of Health and Population Government of Nepal (2010) Nepal Health Sector Programme Implementation Plan II(NHSP IP 2) 2010 �– 2015 Final Draft 18 March 201040 Ministry of Health and Population Government of Nepal (2010) Nepal Health Sector Programme Implementation Plan II(NHSP IP 2) 2010 �– 2015 Final Draft 18 March 2010 p. v41 Ministry of Health and Population Government of Nepal (2010) Nepal Health Sector Programme Implementation Plan II(NHSP IP 2) 2010 �– 2015 Final Draft 18 March 2010

16
developments that have made it possible for FCHVs to treat problems that were previouslythe province of physicians will continue to be made.
During NHSP 2 EHCS will be scaled up, and maintaining and further strengthening coverageis a priority. Further increases are planned in the coverage of several programmes such asexpanded population and family planning, safe motherhood and child health, and motherand child nutrition. The Skilled Birth Attendants (SBA) training strategy will be implemented;training 5,000 by 2012, and reaching full coverage (7,000) by 2015. The existingcommunicable disease programmes will be maintained and the response to NonCommunicable Diseases (NCDs) and injuries will be expanded. Emergency capacity will bestrengthened in facilities near to major highways. Mental health services will be added tothe EHCS package and will address amongst other issues, the increasing number of suicidesamong women of reproductive age.
The government will also consider various options to improve physical access to facilities,including new investment in health and sub health posts where justified, more frequentoutreach clinics, options for relocating existing facilities, and contracting the private sectorto provide services. During NHSP 2 all sub health posts will be upgraded to health posts thatwill have birthing units. An additional Health Assistant (HA) will be posted to the HPs and theexisting Maternal and Child Health Worker (MCHW) position will be upgraded to AuxiliaryNurse Midwife (ANM).

17
Section 3 HRH Situation Analysis
INTRODUCTION
The Human Resources for Health (HRH) Strategic Plan 2011 2015 has been produced withthe best information that was available on the HRH situation at the time (from November2010 to December 2011). The Situation Analysis that follows is based on a review andanalysis of the documentary evidence, on the outputs of the TWGs and other stakeholderconsultations. Information from the MoHP Human Resource Information System (HuRIS)and from the government�’s Personnel Information System (PIS) was also reviewed.
At the time this Plan was being developed (up to December 2011) the information availableon government health workers was not up to date or complete. Only limited informationwas available on health workers employed by the private and NGO sectors. As a result muchof the analysis and commentary contained in this Plan covers only government/public healthsector facilities, providers and employees. However more comprehensive information maysoon be available through the Service Tracking Survey (STS) undertaken by the MoHP in late2011 and more recent MoHP led data collection initiatives.
The analysis of the public sector health workforce is based on different primary andsecondary data sources and datasets; as a result there are gaps and in some casesconsiderable inconsistencies in the findings. The use of different classifications andcategorisations also make it difficult to compare staffing levels and trends over time. ThisPlan contains specific strategies and activities to address some of these issues and improveHRH information systems and processes in the MoHP, in the professional councils, traininginstitutions and other private sector organisations. The findings of current and future HRHstudies will be used to help enrich and strengthen the HRH evidence base and will providemore reliable information for HRH decision making.
GUIDING POLICIES, PLANS AND STRATEGIES
The MoHP recognises that a competent and motivated workforce is required to providequality health services, achieve health goals and outcomes and the objectives of the NHSP 2(i.e. increase access to and utilisation of quality essential health care services). In 2003 theMoHP developed the Strategic Plan for Human Resources for Health (2003 2017) and incollaboration with its partners has undertaken a number of interventions to improve theplanning, management and development of HRH.
However the Government, the MoHP and the EDPs recognise that there are still a number ofHRH challenges that need to be overcome. The NHSP�–2 recommends a more scientific androbust assessment of HRH requirements be undertaken to inform workforce planning and in2008 WHO proposed that �‘to move forward there is an immediate need to review the policy& the strategic plan & update it�’.

18
As described in Sections 1 and 2 there are various policies, plans and programmes that affectthe HRH situation. Some of these are discussed below:
The Health Services Act 1994
The major policy document governing the employment of health sector staff is the HealthServices Act 1994.42 This was created to provide more flexibility in the employment of healthstaff (�“in order to make the health service more competent, vigorous, service oriented andresponsible�”) than the Civil Service Act 1992, which covers most government employeesincluding those on secondment to MoHP from other ministries (e.g. Ministry of GeneralAdministration, Ministry of Finance). Five amendments have been made to this Act, themost recent being in January 2010. Amongst many other things the Health Services Actprovides the rules on transfer, deputation and promotion. The Act allowed for a changefrom a rank system of posts to a grade system.
Another important policy decision outside the Health Service Act was to allow localcontracting, partly to deal with staffing shortages and partly aligned with thedecentralisation of HR management to facility level.
The 2003 2017 Strategic Plan for Human Resources for Health
The 2003 2017 Strategic Plan was intended to (a) specify the direction and growth of humanresource growth, (b) outline human resource objectives for the medium term, and (c)identify short term policy actions for the MoHP. It includes future human resourcerequirements and supply and examines their implications for training and traininginstitutions. The Plan, which was formally adopted, projects a 71% increase in the publicsector workforce by 2017.43
NHSP 2004 2010
During NHSP 2004 2010 a range of interventions were implemented to address HRHchallenges. These included:
A two year compulsory service scheme for physicians who studied under thegovernment�’s scholarship scheme. To date 280 medical doctors in the scheme havejoined the DoHS to work in peripheral health facilities.
2,100 maternal and child health workers working in sub health posts were enrolledin an 18 month ANM course
Vacant posts of Maternal Child Health (MCH) workers and ANMs were filled bycontract staff in many districts.
Incentive packages to retain doctors, nurses and technicians were developed andintroduced.
42 Nepal Law Commission (2010) Nepal Health Service Act, 2053 (1997) with updates. Available at:http://www.lawcommission.gov.np/index.php/ne/acts english/doc/654/raw43 Ministry of Health and Population/RTI (2009) Human Resource Strategy Option for Safe Delivery. Riitta Liisa KolehmainenAitken and Ishwar Bahadur Shrestha

19
A one year biomedical equipment technician course was developed to improve thebiomedical equipment maintenance system and 90 technicians graduated.
A Policy on SBA and a long term plan were formulated and in service training ofSBAs started.44
Training of all health personnel including FCHVs in integrated management ofchildhood illness (IMCI).
NHSP 2 2010 2015
The NHSP 2 notes that �‘a competent, motivated health workforce forms the core of a highquality, effective and efficient health system�’.45 It acknowledges that there was someimprovement in the HRH situation during the NHSP 2004 2009, but recognises that there arestill HRH challenges to overcome. These include:
Health worker shortages, e.g. only two thirds of positions for doctors and nurses arefilled and there are skills shortages in specialised areas.
Deployment and retention of essential health workers, especially in rural andremote areas.
Fragmented HR management and incomplete HR information. Improving the skills of the health workforce. Poor staff attendance and motivation affecting productivity and the quality of
services. Low participation of Dalits and other highly excluded groups in the health workforce.
The NHSP 2 recommends that HRH requirements to support the delivery of EHCS and otherhealth programmes are reassessed in the context of an evolving health, social, economic,and political environment. It proposes specific interventions to overcome the challenges andthese have been grouped around key HRH areas and are summarised and presented in Table5 below.
44 Ministry of Health and Population/RTI (2009) Human Resource Strategy Option for Safe Delivery. Riitta Liisa KolehmainenAitken and Ishwar Bahadur Shrestha45 Ministry of Health and Population Government of Nepal (2010) Nepal Health Sector Programme Implementation Plan II(NHSP IP 2) 2010 �– 2015 Final Draft 18 March 2010

20
Table 5 NHSP 2 Proposed HRH interventions
HRH Area InterventionRecruitment Procedures in place to contract obstetricians,
anaesthesiologists, paediatricians, gynaecologists, MDGPs,medical officers, physiotherapists, nurses, ANMs andother diagnostic support staff
Staff recruited from marginalised groups and allocated tounderserved areas
Deployment of 5,000 additional FCHVs and replacementof 2,000 who will retire/leave
Training and capacitydevelopment
Pre service and in service training strengthened Refresher training for all providers at district hospitals and
below Production of multi skilled workforce to provide more
integrated services Expansion of SBA training Training of 5,000 additional FCHVs New training curricula and courses Provision of career development opportunities Re evaluation of the role of the National Health Training
Centre Analytical capacity at the MoHP strengthened
Productivity andperformance
Performance incentives piloted and evaluated Continued payment of provider incentives for safe
delivery Replacement of village health worker cadre with AHWs Teams posted to district hospitals Legal framework for anaesthesia assistants established
Public private partnership Use of private sector to provide specialised services torural areas.
Partnership developed with the Ministry of LocalDevelopment and with municipalities
Source: NHSP 2010
A rapid assessment of HR planning, management and development capacity, conducted in2010 found the characteristics of HRH to be as follows:46
Supply of most cadres increasing (e.g. institutions for training staff nurses haveincreased from 6 in 1991 to 103 in 2010), and 2003 staffing projections no longer valid.
46Nepal Health Sector Support Programme (2010). Draft Capacity Assessment for Health Systems Strengthening. An assessmentof capacity building for health systems strengthening and the delivery of the NHSP 2 results framework. Martineau, T (LATH)and Subedi H. N.
21
Inequity in access to health workers is worsening, despite the increase in supply, due tothe difficulty in attracting and retaining staff in remote areas, even though innovationssuch as local contracting are showing promise.
Expansion of training, much of which is now provided by the private sector, has notbeen accompanied by maintenance and development of standards. This has implicationsfor the quality of service delivery.
There is a lack of accurate data on staffing, especially for non government employers.
STAFFING LEVELSGovernment data sources estimate that of the current 78,000 civil servants employed by thegovernment, approximately 31,500 (40%) are employed in the MoHP.
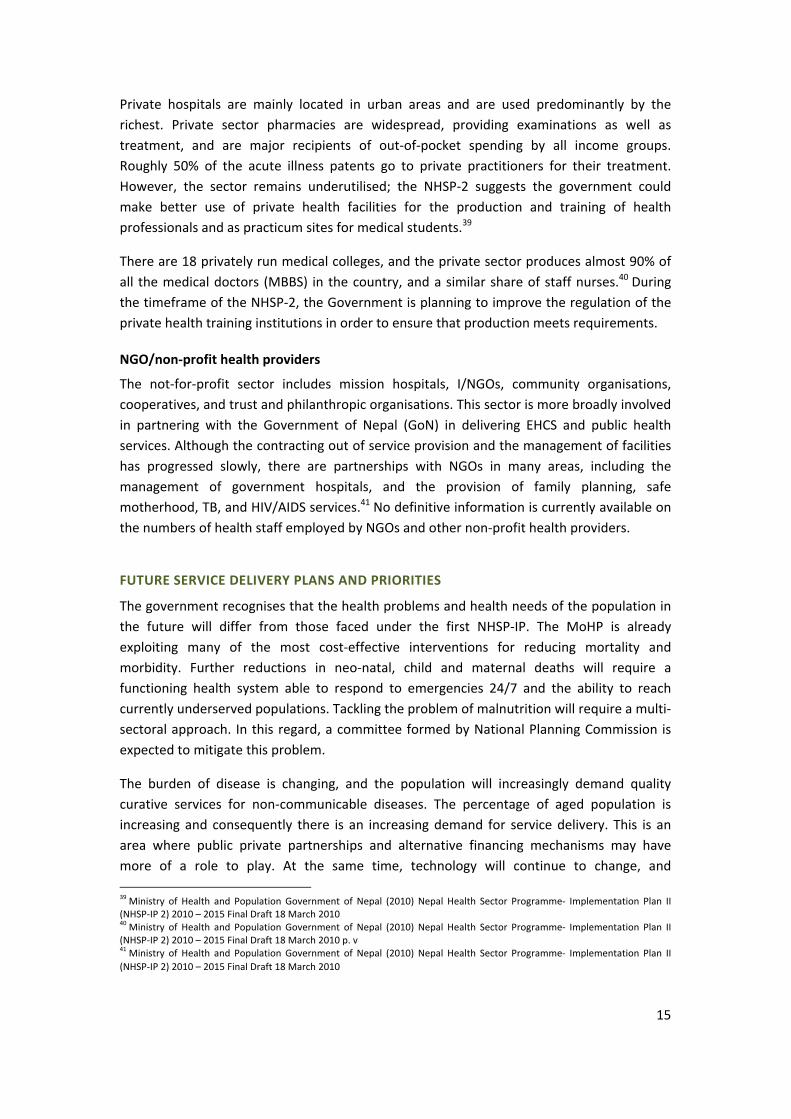
Data from the Medical Council for 2010 indicate that there were 12,194 Nepali medicaldoctors and 4,752 non Nepali medical doctors registered in Nepal (see Table 6 below). Ofthe 12,194 Nepali doctors registered, 2,000 were consultants and specialists. Table 7 showsthe number, sex and type of specialists registered. The greatest number of specialists is inthe areas of obstetrics and gynaecology (237), followed by general surgery (232), internalmedicine (195), and paediatrics (182). One third of all the specialists registered are female,and most are working in the areas of obstetrics and gynaecology and paediatrics.
Table 6 Registered medical doctors December 2010
Category Registration(National)
Registration(foreign)
Total
MBBS 10194 n/a 10194Consultant 2000 n/a 2000Not identified n/a 4752 4752Total 12194 4752 16946Source: Nepal Medical Council 2010

22
Table 7 Medical Specialists registered with Nepal Medical Council
S.N Subject Male Female Total1 General Practice 80 26 1062 E.N.T 51 13 643 Psychiatry 38 5 434 Anaesthesiology 89 31 1205 Radiology and Imaging 84 12 966 Paediatrics 133 49 1827 Nephrology 5 3 88 Master in Dental Surgery (MDS) 52 39 919 T.B. and Respiratory 7 1 810 Community Medicine Public Health 33 10 4311 Pharmacology 13 1 1412 Obs & Gyn 71 166 23713 M.S (General Surgery) 222 10 23214 Orthopaedics 160 1 16115 Cardiology 69 5 7416 Ophthalmology 61 45 10617 Internal Medicine 177 18 19518 Clinical Pathology 38 38 7619 Dermatology + Venereology 39 23 6220 Neurology 14 3 1721 Gastroenterology 14 2 1622 Urology 14 0 1423 Surgical Oncology 14 0 1424 Forensic Medicine 6 0 625 Microbiology 7 4 1126 Nuclear Medicine 4 0 4
Total 1495 505 2000Source: Nepal Medical Council 2010
Table 8 shows that there were 33,733 Nepali and 684 non Nepali nurses with permanentregistration in 2011, yet there were only 6,553 employed in the public health sector in thatyear. Over half (51%) of the total number of nurses registered were ANMs.
Table 8 Registered Nurses July 2011
Category Nurse ANM Total Foreignnursing
Grandtotal
Permanent registration 16299 17424 33733 684 34417Total 16299 17424 33733 684 34417Source: Nepal Nursing Council 2011
The Nepal Ayurveda Medical Council estimates that in 2012 there are 785 Ayurvedic healthproviders consisting of specialists, doctors and Health Assistants (See Annex 5 for a detailedbreakdown of the Ayurvedic workforce). In 2012 the Nepal Pharmacy Council had registereda total of 2,949 personnel, of which 2,069 had a Diploma in Pharmacy and 880 had aBachelor�’s Degree in Pharmacy. Table 9 below shows that there were 47,987 HealthProfessionals registered in Nepal in 2011, 5,514 of which had temporary registration. The

23
Table also shows the level of the qualification they have attained, with the majority havingattained a Level 3 qualification. Table 10 provides more information on the types of healthprofessionals that have permanent registration.
Table 9 Registered Health Professionals July 2011
Category Level 1(Bachelor)
Level 2(PCL)
Level 3(TSLC)
Total
Permanent registration 1619 4232 36622 42473Temporary registration 611 1003 3900 5514Total 2230 5235 40522 47987Source: Nepal Health Professional Council 2011
Table 10 Health Professionals with permanent registration July 2011
No. Discipline
LevelLevel 1
Bachelor &above
Level 2PCL
Level 3TSLC
1. Public Health 654 �– �–2. Health Education 45 9 �–3. Medicine �– 2780 293014. Medical Microbiology 20 �– �–5. Diag. Health Lab 544 536 58286. Diag. Radiography 98 164 437. Diag. Radiotherapy 4 9 �–8. Diag. Cytology 2 �– �–9. Diag. Haematology 7 �– �–10. Diag. Biochemistry 20 �– �–11. Ayurved 6 191 104612. Homeopathy 44 10 �–13. Unani 12 �– �–14. Acupuncture 12 1 1115. Physiotherapy 86 74 3516. Community Based Rehabilitation 1 �– �–17. Prosthetic & Arthritic 2 1 �–18. Dental Assistant �– 37 35619. Naturopathy 7 �– 120. Yoga 8 �– 121. Ophthalmology 40 390 �–22. Operation Theatre and Allied
Health Sciences �– 30 �–23. Clinical Psychology 2 �– �–24. Speech and Hearing 5 �– �–Sub Total 1619 4232 36622Total 42473Source: Nepal Health Professional Council 2011

24
The data presented above indicate that the production and stock of most cadres of healthworkers is adequate to meet the service delivery needs of the country. The data presentedin the previous Section 2 indicate that the MoHP provides a wide coverage in its primary andsecondary health care services. However there is a general problem of understaffing ingovernment facilities, especially in remote and rural government facilities, with the MoHPunable to attract and retain sufficient number of skilled health workers. According to the2003 Strategic Plan for Human Resources for Health 2003 to 2017, 47 this has been a longstanding problem, especially for more highly trained staff cadres.
There are acute shortages of doctors, specialists and nurses, especially staff nurses,48 indistrict hospitals and PHCCs. Recent data presented in Table 11 below indicate that of the12,194 Nepali medical doctors registered (see Table 6 above) in Nepal in 2011, there are8,335 working in the country, 1,447 of these in the public sector and 6,888 in the privatesector.
Table 11 Doctors in the public and private sectors in 2011
Cadre Public sector Private forprofit sector
Total
Scholarship Sanctioned andfilled posts
Doctors 335 1112 6888 8335Source: HuRIS 2010 and DoHS 2010
A significant number of health workers are employed in the private and NGO sectors;estimated to be 20,000 in 2010, while others are working outside the sector and thecountry.
Table 12 below shows that in 2011 the MoHP has 27,770 employees, including scholarshipdoctors, of whom 20,663 are technical and 7,137 (26%) are administrative and support staff.In 2012 there are 785 Ayurvedic service providers. In addition there are also approximately50,000 FCHVs supporting the delivery of health services. The MoHP has been successful inrecent years in raising the skills levels of the health workforce and its efficiency.
47 MoHP (2003) Strategic Plan for Human Resources for Health 2003 to 201748 2011 MoHP Service Tracking Study Preliminary findings

25
Table 12 Human resources for health in the public and private sector 2011
CadrePublicsector
Private forprofit sector Total
SanctionedDoctors, (including 335Scholarship doctors) 1, 447 6888 8335
Nurses 6553 n/a 6553
Paramedics 7559 n/a 7559
Public health workers 4289 n/a 4289Alternative medicine(Ayurvedic) 785 n/a 785Admin & Support 7137 n/a 7137Total 27770 6888 34,658Source: HuRIC 2010, DOHS 2010, and Nepal Ayurveda Medical Council 2012;
There could be approximately 3,500 permanent and contract staff in addition to thisnumber, that have not yet been incorporated onto the HuRIS. According to the DoHS2009/10 Annual Report, a total of 1,348 additional Paramedics/Allied Health Professional(AHP) posts were created and filled during 2008/09 and a similar number were added during2009/10 in order to upgrade sub health posts to health posts. In addition there were 586ANMs and 40 staff nurses recruited on local contracts to support 24 hour delivery services inPHCCs and HPs in 2009/10.49 These staff numbers are not reflected in the 2011 figurespresented in Table 12 above.
Staffing has not kept pace with population growth, which grew at a rate of 45% between1991 and 2011, compared to an increase in staffing of only 3.4% in the same period (about10% of the population growth rate). The sanctioned post system is used by the governmentsector to manage and control staffing levels in the sector. In some cases there are notenough sanctioned posts available to recruit all the health workers that are produced andrequired. This system is not sufficiently flexible and/or responsive to allow the sector toperiodically realign and readjust staffing levels in line with population growth; health serviceneeds, training output and a changing disease burden.50 There is also inadequate numbersof sanctioned posts for staff that have upgraded their skills and qualifications e.g. those whohave trained as SBAs.
Table 13 below shows that Nepal currently has 0.042 doctors per 1,000/population ratio and0.25 nurses per 1,000/population ratio. These ratios are based on an estimated 2011population of 26.6 million and use the 2011 staffing data that were available for the public
49 Ministry of Health and Population (2011) Department of Health Services Annual Report 2009 2010 p.9650 WHO Country Office for Nepal (2007) Policy Papers on Health, Nepal

26
sector doctor (1,112) and nursing (6,553) cadres. This represents a total ratio of 0.29 healthworkers per 1,000/population, which is significantly less than the WHO recommendation of2.3 per 1,000/population and low compared to selected countries in the region
Table 13 Ratio of doctors and nursing/midwifery staff to population
Country Doctor Date Nursing & Midwifery Date
Bhutan 0.24 2011 1.09 2011Bangladesh 0.26 2004 0.14 2004Nepal 0.04 2011 0.23 2011India 0.06 2005 0.80 2004Sources: WHO Global Health Atlas 2011, WHO 2006 and MoHP HuRIS and PIS
However the picture for doctors changes dramatically when the number of doctors in theprivate sector is included in these calculations. For example if the number of doctorsemployed in the country (see Table 11) 8,335 is used, the ratio would be almost 0.31doctors per 1,000/population, which is higher than that of Bangladesh, but is still muchlower than the WHO recommendation.
As is evident from the data presented in the Tables above, the availability of adequatenumbers of skilled health workers in the public sector is one of the most critical bottlenecksin scaling up needed health interventions in the health sector. These problems are rooted inthe weaknesses inherent in the structures, systems and capacity used to plan, manage anddevelop the health workforce, as well as labour market dynamics.
The situation is expected to become more serious as new and expanded health programmescome on stream during the NHSP 2, and as the population grows and the demand andutilisation of services increases. The MoHP TWG formed to examine and analyse theimbalances between supply and demand identified several reasons for the shortages andnon availability of some cadres of staff51. These include the lack of up to date HRHinformation; unregulated training institutions that are not producing sufficient numbers ofthe types of health workers needed to meet service delivery demands; weak HR planningsystems and capacity; obsolete staffing norms and standards; ill informed deploymentdecisions; lack of performance incentives; as well as health worker migration.
The 2011 MDG Assessment Report found that frequent transfers, study leave, deputation,training workshops and high patient load, including unfilled sanctioned posts, are key factorsaffecting the availability of staff.52
VACANCIES/SHORTAGES IN PUBLIC SECTOR FACILITIES
According to the NHSP 2, two thirds of the public sector�’s sanctioned positions for doctorsand nurses are filled and 82% of posts are filled at PHCCs and district hospitals.53 Vacancy
51 Ministry of Health and Population (2011) Milestone 7: Periodic Review on the development of the HR Plan (Draft) Martineau,T. & Bista, B. Nepal Health Sector Support Programme52 National Planning Commission/UNDP (2011) Millennium Development Goal Needs Assessment for Nepal 2010

27
rates are particularly high for skills that are most needed, and are most acute in remote andrural areas.
In 2008 WHO highlighted the shortage of qualified doctors and midwives and indicated thata third of PHCCs had no doctors.54 It suggested that doctors �‘prefer to join private services inurban settings or migrate to developed countries�’.
Table 14 shows shortages across the different cadres in 2007/08 and indicates that therewere shortages across the board, but these were most acute for doctors.
Table 14: MoHP sanctioned and filled posts in 2007/08
Position Sanctioned Filled Vacant % of filledpositions
% Share
Medical doctor 1,062 816 246 76.84 4.34Nursing staff including ANMs 5,935 5,307 628 89.42 24.25Paramedics 10,642 9,212 1,430 86.56 43.48Other 6,838 6,394 444 93.51 27.94Total 24,477 21,729 2,748 88.77 100.00Source: Annual Report, DoHS, 2007/08, cited in NHSP 2
The NHSP 2 highlights shortages in other areas. There are only 1,000 trained SBAs availableand another 6,000 are needed; 90 Medical Doctors General Practice (MDGPs) are neededbut only 34 are available. There is also a chronic shortage of anaesthetists, psychiatrists,radiologists, radiographers, and anaesthesia assistants. In addition, more health systemsmanagement personnel are needed, such as procurement specialists, health legislationexperts, epidemiologists, health economists, health information specialists, HR managers,hospital managers, and health governance experts.
A study conducted in 2009/10 by the MoHP on Obstetric Morbidity and Related CareSeeking Behaviour, focusing on maternal health and family planning services, found that lessthan 80% of the sanctioned posts were filled in the surveyed health facilities.55 Of the postsfilled about 10% of the staff were not available during the time of survey. Essentialequipment and drugs were also lacking in most of the health facilities.56
The 2011 MDG Assessment found shortages of SBAs and specialised TB staff. It recommendsthat vacant posts, particularly at the district level, be filled immediately and priority given tocandidates from local communities.57
In 2008/09 the fund for Comprehensive Emergency Obstetric and Neonatal Care (CEONC)services, was used to support the recruitment of staff and the purchase of equipment, drugsand supplies. It is also used to hire on short term contracts private sector health workers toprovide Caesarean Section (CS) services. The CS team includes an MDGP or
53 Ministry of Health and Population Government of Nepal (2010) Nepal Health Sector Programme Implementation Plan II(NHSP IP 2) 2010 �– 2015 Final Draft 18 March 2010 p. vi54 WHO HRH NEPAL http://www.nep.searo.who.int/en/Section10.htm 200855 Ministry of Health and Population (2011) Department of Health Services Annual Report 2066/67 (2009 2010) pp. 127 13056 Ministry of Health and Population (2011) Department of Health Services Annual Report 2066/67 (2009 2010) pp. 127 13057 National Planning Commission/UNDP (2011) Millennium Development Goal Needs Assessment for Nepal 2010

28
Obstetrician/Gynaecologist (OBS/GYN), an anaesthetist or Anaesthesia Assistant (AA) and anOperation Theatre (OT) trained nurse.
In order to fill critical posts the MoHP has also been employing a number of obstetricians,gynaecologists, MDGPs, medical officers, nurses and ANMs on short term contracts.58
Preliminary findings from the 2011 Service Tracking Study indicate that in the 16 regional,zonal and district hospitals surveyed, administrative staff make up the greatest number ofcontracted staff, followed by ANMs. In the PHCCs, HPs and SHPs survey, it is administrativestaff, AHWs and ANMs who are on contract.
WORKFORCE CHARACTERISTICS
Recruitment and attraction
Despite the measures adopted by the MoHP (e.g. short term contracting, CEOC funds,incentives, etc.), attracting sufficient numbers of skilled staff into the public health sectorremains a challenge. The lack of sanctioned posts for some cadres and facilities also limitsthe numbers that can be recruited. Anecdotal evidence suggests that there is a pool ofunemployed graduates; e.g. one estimate is that there are between two and three hundredtrained ANMs available in the labour market.
The TWG working on this area identified a number of reasons for the problems related toattraction and recruitment. These included a lack of information on vacancies and shortages;lengthy and unwieldy recruitment systems; insufficient sanctioned posts; financialconstraints to creating new posts; unwillingness of graduates to consider public sector jobs;and more attractive employment conditions offered by private and NGO employers.
The MoHP has conducted a number of Operations and Management (O&M) surveys andidentified the new positions that are required to deliver services. For example the FamilyHealth Division in the MoHP has identified that 28 MDGP, 12 Gynaecologist and 40Anaesthesia Assistant (AA) posts will need to be created to improve the provision of CEOCservices. These posts have not yet been approved. The MoHP is also seeking approval tocreate 330 new specialist positions.59 Any new posts need to be sanctioned and fundedbefore the MoHP can recruit and deploy the staff to fill them.
It is increasingly being recognised that MDGPs are the most appropriate doctor cadre forrural areas,60 and increasing the numbers recruited and deployed to rural areas is a priority.The creation of positions for hospital managers and recruitment of managers is also criticalto ensure that HRH and other resources are effectively managed in the delivery of services.
Local recruitment allows the MoHP to by pass and avoid the often lengthy procedures forcreating new posts and for recruiting staff. However, this has resulted in an unknown �– but
58 Ministry of Health and Population (2011) Department of Health Services Annual Report 2009 2010 p.9659 Reported by the Personnel Administration Division60 The Nick Simons Institute has developed a scholarship system for MDGP doctors, and according to the NSI Report on FiveYears of Progress 2006 11 the MOHP recently asked the NSI to �‘rapidly and widely scale up�’ the Rural Staff Support Programme.

29
reportedly quite large �– number of employed staffs that are not on the formal payroll orentered onto the HuRIS.
The short term nature of the contracts and the high turnover of contract staff are causingconsiderable disruption of services. A current constraint is that contracts can only be givenfor a 12 month period and it can take up to 5 months to negotiate a follow on contract. Inaddition those hired on 12 month contracts often work for as little as 6 months, because ofdelays with the contracting and budget approval processes. Reportedly some contract postsare filled by staff who are on leave from their full time government jobs and their availabilitydepends on the amount of leave they can take.
The 2008 Nepal Safe Delivery Survey examined the willingness of private medical andnursing students to work for government.61 None of the students surveyed intended to jointhe public health service; the majority was planning to continue their studies abroad. Morethan half of the nursing students (57%) wanted to work for the private or NGO sector aftergraduation. The reason they gave for their unwillingness to join the public sector includedthe following: poor physical facilities, lack of equipment/supplies, poor workingenvironment, lack of opportunities for upgrading knowledge, and lack of security (personalsafety) and non availability of staff quarters.
The MoHP is planning to initiate multi year contracting to address some of these issues andthe NHSP recommends that greater continuity of services multi year contracts be providedfor obstetric, gynaecological, paediatric, physiotherapy, and other diagnostic supportservices.62 This Plan supports this initiative and contains a range of short (e.g. expansion ofmulti year contracting to other critical and scarce cadres) and long term strategies (e.g.more attractive career pathways for MDGPs, 63 districts given more responsibility for therecruitment of staff, etc.) aimed at attracting sufficient numbers of appropriately skilledhealth workers into government facilities (see Output 2 in Section 4 of this Plan). It alsocontains strategies and activities to strengthen the Health Facility Management Committees(HFMCs), as they are also responsible for the recruitment and management of contract staff.
Distribution
The evidence indicates that sufficient stocks of most categories of health workers are beingproduced and the greatest challenge to the availability of health workers in governmentfacilities is the way in which staff are deployed and distributed. For example, out of anational stock of 8,335 medical doctors, only 1,112 are in government facilities. Two thirdsof these are working in the Kathmandu valley or in other cities.64 The 2008 Nepal SafeDelivery Field Survey reported that key Maternal Neonatal Child Health (MNCH) staff such as
61 Ministry of Health and Population/ RTI (2009) Human Resource Strategy Option for Safe Delivery Riitta Liisa KolehmainenAitken, MD, and DrPH Prof. Ishwar Bahadur Shrestha62 Ministry of Health and Population Government of Nepal (2010) Nepal Health Sector Programme Implementation Plan II(NHSP IP 2) 2010 �– 2015 Final Draft 18 March 2010 p.6563 MoHP (2011) Readiness of Comprehensive Emergency Obstetric and Neonatal Care in Nepal64 Ministry of Health and Population Government of Nepal (2010) Nepal Health Sector Programme Implementation Plan II(NHSP IP 2) 2010 �– 2015 Final Draft 18 March 2010

30
specialist doctors (e.g. obstetrician/gynaecologists, anaesthesiologists and MDGPs), andstaff nurses were not equitably distributed.
Table 15 and 16 below present the 2008 information on government health facilities bydevelopment region and geographic terrain.
Table 15 Distribution of government health facilities by development region
DevelopmentRegion
RegionalHospital
ZonalHospital
DistrictHospital
PHCC Healthpost
Total
Eastern 0 3 14 50 142 209Central 1 3 12 67 170 253Western 1 1 16 42 144 204Mid Western 1 1 13 29 133 177Far Western 0 2 7 20 89 118Total 3 10 62 208 678 961Source: Ministry of Health and Population (2009)
Table 16 below shows that the hill region has the highest number of health facilities overall.The mountain region has no zonal or regional hospital.
Table 16 Distribution of health facilities in the public sector by geographic region 2008
Geographicregion
Regionalhospital
Zonalhospital
DistrictHospital
PHCC Healthpost
Total
Mountain 0 0 16 20 149 185Hill 2 1 32 101 364 500Terai 1 9 14 87 165 276Total 3 10 62 208 678 961Source: Ministry of Health and Population (2009)
Maldistribution has been a longstanding concern in the health sector and the deployment ofhealth personnel to the rural and remote areas of the country remains a challenge. Theseareas are generally under staffed and absenteeism is a growing problem. A significantnumber of sanctioned posts, especially for skilled and specialist staff, are vacant in theseareas. A 2009 review of the skills mix in the health workforce revealed that only 4.2% weredoctors; 12% were nurses, excluding ANMs; nearly half (47%) were paramedics; and almostone third (28%) were support staff.65 Transfer practices are also causing distortions in thedistribution of health workers.66
Private sector health facilities tend to be located in the urban areas resulting in greaternumbers of health workers in these areas. Although there are more private health careproviders in urban areas, these are less accessible to poor urban populations who have aspoor, or worse, health status than rural populations. Public health facilities in urban areasare few, of low quality and poorly staffed. An urban health policy and strategy is being
65 HuRIC, 200866 HRH Workshop Report June 25/26 2011

31
developed, which will help to address the gap in health services for the rapidly growingurban population.
The MoHP TWG that was formed to work on this issue identified several reasons formaldistribution. These included lack of informed and transparent deployment and transferdecisions, lack of standardised procedures for placement and transfer, poor workingenvironment, insufficient incentives to attract and retain staff in remote and rural areas andother personal, professional and economic reasons.67
Better enforcement of and compliance with the deployment procedures will ensure thatstaff with appropriate skills are posted to the facilities where they are needed and wherethey can use their skills. The 2008 Nepal Safe Delivery Field Survey found that a largenumber of MDGPs and staff nurses were posted to facilities where their qualifications andskills were not required.68 For example MDGPs or Medical Doctors who have specialist skillswere posted as medical officers, and staff nurses with anaesthesia training were working inthe general wards.69 In 2011 as part of its follow up of AAs in the field, the Nick SimonsInstitute (NSI) collected data on the status of Comprehensive Emergency Obstetric Care(CEOC) services and HRH availability at government district hospitals. They made contactwith 79 of the 91 AAs trained. Of those contacted, only 49 were still working and using theirskills. One of the main reasons given not using their skills was that there was no doctor inthe facility to conduct operations.70 This finding is corroborated by another study in 2010,which concluded the �‘primary bottleneck�’ in the provision of CEOC services was a lack of�‘specialists with surgery skills. 71
There are various initiatives in place to promote more equitable distribution of the healthworkforce. For example the Health Services Act encourages staff to serve in rural areas byproviding career development opportunities and incentive packages to those who take up arural posting. 72 The 2011 DoHS Annual Plan indicates that career development andopportunities for higher education will be made available for doctors and health workerswho are willing to work in villages and rural areas.73
The Female Community Health Volunteers (FCHVs) deployed in the mountain regions andremote districts, partly compensate for the shortage of professional health workers, and it isexpected that during the NHSP 2 that this number will increase by 5,000.74
67 Ministry of Health and Population (2011) Milestone 7: Periodic Review on the development of the HR Plan (Draft)Martineau, T. & Bista, B. (2011). Nepal Health Sector Support Programme68 Ministry of Health and Population/ RTI (2009) Human Resource Strategy Option for Safe Delivery Riitta Liisa KolehmainenAitken and Ishwar Bahadur Shrestha69Ministry of Health and Population/RTI (2009). Human Resource Strategy Option for Safe Delivery Riitta Liisa KolehmainenAitken and Ishwar Bahadur Shrestha70 NSI (2011) Nepal MoHP CEOC Service vs Human Resource Provision71 MoHP (2011) Readiness of Comprehensive Emergency Obstetric and Neonatal Care in Nepal72 Interview with MoHP official73 Ministry of Health and Population (2011). Department of Health Services Annual Report 2009 201074 Ministry of Health and Population Government of Nepal (2010) Nepal Health Sector Programme Implementation Plan II(NHSP IP 2) 2010 �– 2015 Final Draft 18 March 2010

32
Health workforce attrition and retention
The availability of skilled and motivated health workers in sufficient numbers in the rightplace and at the right time is critical to deliver effective health services and achieve healthoutcomes. The shortage of qualified health workers in remote and rural areas impedesaccess to health care services for a significant percentage of the population; it slowsprogress towards attaining the MDGs and challenges the aspirations of achieving health forall.
As described above one of the main reasons for the current shortage of staff is the inabilityof the government to attract and retain certain health worker cadres. There are a number ofreasons for this, including supply, attrition and distribution factors.
The NHSP 2 suggests that doctors are migrating to the private and NGO health sectorswithin the country, while others are leaving the country altogether. Professional councils arebeing approached for letters of good standing by staff wanting to work abroad,75 but it is notclear how many of these actually leave. As shown earlier there are significant numbers ofspecialists in obstetrics, gynaecology and paediatrics registered with the Medical Council,yet many of these posts are vacant in the government health facilities.
Table 17 below shows the data that are available on the main causes of attrition amongpublic health workers. In 2009 and 2010 the leading cause was �‘voluntary�’ followed by �‘age�’.
Ministry of Health and Population (2011) Human Resource Information System Assessment. Blair G., LATH

33
Table 17 Public sector staff flows
Demographics 2006 2007 2008 2009 2010 2011Number of Staff at the start of theyear 24,539 24,774 24,906 24,945 25,189 25,313New Appointments 235 132 39 244 124 13Retirement at the start of the year 44 57 87 165 314 472Other losses:Voluntary 9 12 40 85 61 9Forced With Facility 2 1 1 2 0 0By Age 1 16 30 58 80 31By Service Period 1 0 0 0 0 0Deceased 0 0 7 4 17 4Pending Transfer Employees 0 0 0 0 0 21Forced Without Facility 0 1 0 0 0 0Pending Retired Employees 0 0 0 0 0 12Total Exit 13 30 78 149 158 77Actual Staff at the end of theyear/till date 24,717 24,819 24,780 24,875 24,841 24,777Source: HuRIS, MoHP 2011
A number of studies have been conducted to determine the most effective retentionstrategies in Nepal. In a 2008 survey to ascertain the expectations of medical graduates ofthe government health system, the key priorities were academic support for post graduatetraining, followed by financial incentives, career advancement support, allowances, betterdiagnostic facilities, and security.76 This Plan contains strategies and activities to explore thisarea further and to support the retention of health workers.
Health worker performance
A motivated health workforce is essential to a well functioning health system and motivatedemployees are likely to be more productive. There is evidence that there is a range ofmonetary and non monetary incentives (e.g. recognition, appreciation, opportunities forcareer advancement, etc.) that can be used to improve performance and influence heathworkers�’ behaviours. The fairness of the rewards offered will also affect the manner inwhich individuals view their jobs and the organisation, and the amount of effort they expendin accomplishing tasks.
The skill mix that exists currently in many government health facilities, where doctors andnurses are in the minority, does not allow for the delivery of quality health care. The NHSP 2
76 Health Sector Reform Support Programme (2008) Costing Study on Incentives Packages for Nepal�’s Health Care Professionals

34
recommends that the skills of existing health workers must be further developed and vacantpositions of unskilled staff be upgraded to semi skilled.77
Motivation and performance are closely linked. A study of motivation among health workersin Nepal identified the following factors: opportunities for training and further study, salaryand incentives, personal factors (such as safety, communication), leadership andmanagement, staff quarters, supportive community, recruitment conditions and careerdevelopment opportunities, good working environment, team work and supportive staff,appreciation and recognition of work and supportive supervision.78 The findings also indicatethat poor career prospects and a lack of sanctioned posts were key demotivators for MDGPsin district hospitals.
Various incentive schemes are being used to motivate health workers and improveperformance and productivity. The funds for the free delivery policy or the Aamaprogramme was reported to have improved morale and helped the number of staff workingon delivery care to remain stable or increase in some facilities. In one facility the attendanceof staff improved because the facility had introduced a rule that any staff member on leavefor more than 2 weeks did not get a share of the incentive. The Aama programme was alsoreported to have contributed to more active HFMCs in some cases. 79
Poor staff motivation and performance negatively affects the delivery and take up of healthservices, and the achievement of MDGs and the National Health Indicators. While the rootcauses and the true extent of poor performance need to be further substantiated throughin depth analysis, the TWG working on this area identified the following causes:
Skills related factors
Poor quality basic education Weak in service training systems, approaches and programmes Lack of investment or prioritisation by the sector in skills development
Environmental factors
Lack of HRH policies and strategy Weak Human Resource Management (HRM) and performance management systems
and non compliance with procedures and regulations Lack of career pathways Ineffective procedures for deployment and transfer Inadequate physical working environment, including infrastructure, equipment and
supplies and transport
77 Ministry of Health and Population Government of Nepal (2010) Nepal Health Sector Programme Implementation Plan II(NHSP IP 2) 2010 �– 2015 Final Draft 18 March 2010 p.8478 Ministry of Health and Population/RTI (2009) Human Resource Strategy Option for Safe Delivery Riitta Liisa KolehmainenAitken and Ishwar Bahadur Shrestha79 Witter, S., Khadka, S., Hom Nath, and Tiwari S. (2011) The national free delivery policy in Nepal: early evidence of its effectson health facilities Health Policy Plan.

35
Bureaucratic decision making practices Health worker focus on private practice Lack of recognition of social values, gender issues, social inclusion Economic and political instability Political and social pressure to misuse power Ineffective communication /coordination between HRH related stakeholders
Financial/motivational issues
Low remuneration for levels of skills and expertise Limited allowances Lack of performance based monetary incentives No reward or recognition for good performance
Factors such as low levels of skills and knowledge also affect performance and productivity.In 2008 the Nepal Safe Delivery Field Survey reported that there was a lack of SBA skillsamong all relevant cadres. Despite a concerted effort to train ANMs as SBAs, the NHSP 2 hasidentified that another 6,000 SBAs are needed. More recent studies indicate that clients arenot satisfied with health worker attitudes and behaviours, e.g. the Rapid Assessment ofAama Programme, Social Audit of Aama Programme. 80
A 2011 study looking at the readiness of CEONC services found that despite the provision ofthe CEOC fund, there were a low proportion of CS services available. One of the reasonscited was the challenges that the hospitals faced in hiring and managing a private CEONCteam, including a lack of applicants, friction between the lesser paid government staff andthe members of the private team and weak management and leadership capacity.81
The MoHP has been working in collaboration with the National Health Training Centre(NHTC) and other stakeholders to improve in service training and the skills of providers toenhance the quality of care provided. Reviews have already been conducted for maternalhealth and safe motherhood services and training courses have been strengthened toaddress the gaps identified.
With support from the NSI, the MoHP and NHTC have conducted training needsassessments, leading to the creation and adoption of new training courses (e.g. Mid LevelPracticum, AA, SBA and Biomedical Technician training) for mid level workers and SBAs, andthe introduction of a distance Continuing Medical Education (CME) course for doctors 82
However, the impact of these initiatives has yet to be evaluated. Preliminary findings fromthe 2011 Service Tracking Study indicate that ANMs and AHWs received the most training ofall the cadres that were in the facilities surveyed.83
80 Family Health Division, DoHS, (2010) Assessment of Aama Surakshya Programme81 MoHP (2011) Readiness of Comprehensive Emergency Obstetric and Neonatal Care in Nepal82 NSI (2011) Five Years of Progress 2006 201183 Service Tracking Study 2011 Preliminary findings

36
The MoHP plans to identify other essential health workers and conduct further trainingneeds assessment to determine how the gaps can be addressed. Over the time frame of theNHSP 1,000 MCHWs will be upgraded to ANMs and over 1,200 Village Health Worker (VHW)positions will be upgraded to AHWs. Skills of care providers and support staff at health andsub health posts, PHCCs and district hospitals will be updated through in service refreshingtraining, coaching and onsite support.84
Productivity
Low productivity is identified as another key HRH challenge in the NHSP 2. For example,2006/07 data from Health Management Information Systems (HMIS) indicates thatparamedics�’ clinical consultations per day were as low as 6 at HPs and SHPs. Daily output perphysician varied between regions. On average, a physician located in a district hospital in theTerai Region saw 18 outpatients and 3 inpatients per day, nearly twice as many as physicianslocated in the mountain districts. A doctor in a referral hospital saw on average only 10outpatients and 3 inpatients daily.85 It was recognised that factors beyond the control of thestaff, such as the availability of drugs, affect patient demand and productivity. However, thefindings provide evidence of low productivity and demonstrate that there were sufficientnumbers of staff available at that time to increase utilisation and coverage.
Staff need equipment and supplies to do their work. The 2008 Nepal Safe Delivery Survey86
found that all ten of the district hospitals visited by the survey team lacked the equipmentcritical for safe delivery, but there were some instances where equipment was not beingfully utilised.87 The 2011 study that examined the Readiness of Comprehensive EmergencyObstetric and Neonatal Care in Nepal found that the availability of drugs and suppliespurchased through the CEOC Fund made it easier for health workers to treat people quicklyand equally, which led to improved staff morale.88
As mentioned above some staff have limited opportunities to use their skills, and there is aninappropriate skills mix in some facilities. These factors also affect productivity, the standardof care and type and range of services provided. During the NHSP 2, one strategy that will beadopted involves upgrading and training vertical programme supervisors (Family Planning[FP], EPI, TB/Leprosy, disease control, etc.) to function as public health supervisors.
Uncoordinated and ill informed transfers affect the productivity of teams when key teammembers are moved, particularly for the management of delivery complications. Forexample when one member of a CEONC team (e.g. the AA, MDGP, OBS/GYN, and OperationTheatre (OT) nurse) is transferred, Caesarean Section services cannot be provided.
84 Ministry of Health and Population Government of Nepal (2010) Nepal Health Sector Programme Implementation Plan II(NHSP IP 2) 2010 �– 2015 Final Draft 18 March 2010 p. 8385 Ministry of Health and Population Government of Nepal (2010) Nepal Health Sector Programme Implementation Plan II(NHSP IP 2) 2010 �– 2015 Final Draft 18 March 201086 Ministry of Health and Population/RTI (2009) Human Resource Strategy Option for Safe Delivery Riitta Liisa KolehmainenAitken and Ishwar Bahadur Shrestha87 Ministry of Health and Population/RTI (2009) Human Resource Strategy Option for Safe Delivery Riitta Liisa KolehmainenAitken and Ishwar Bahadur Shrestha88 MoHP (2011) Readiness of Comprehensive Emergency Obstetric and Neonatal Care in Nepal

37
Effective management systems and capacity will support staff performance and productivity.In 2007, WHO proposed that the roles of health system managers needed to be redefined,with more emphasis given to developing managers�’ competencies and skills for intersectoral coordination and partnership building.89
In 2011, NSI, in conjunction with NHTC, conducted a study to assess the management andleadership training needs of hospital managers. Its preliminary findings suggest that a cadreof managers needs to be created; they can be equipped with appropriate competenciesthrough pre and in service training and CPD, and supported through an enabling workingenvironment to improve the management of hospitals and the delivery of services. Thestudy proposes that a pilot programme of in service management and leadershipdevelopment be conducted with selected hospital management teams.90 Management andleadership capacity will also be critical as the federalisation process continues and asauthority for HRM and health facility performance is further decentralised and devolved tothe sub national levels.
Absenteeism
Absenteeism is another problem that affects health worker productivity. The 2008 NepalSafe Delivery Field Survey91 found that that a significant number of doctors, nurses andparamedics were not present in their workplace at the time of the survey. The situation wasworse in the most remote districts. The 2009/10 MoHP study on Obstetric Morbidity andRelated Care Seeking Behaviour found that 10% of the staff deployed were not availableduring the time of the survey.92
Authorised absence, such as deputation, leave, study leave and training were cited as themain causes of absenteeism among doctors and staff nurses. Preliminary findings from the2011 Service Tracking Survey indicate that deputation is greatest among VHWs and Lab Staffin the hospitals, among HAs and VHWs in PHCCs and among AHWs, HAs, and VHWs in HPs.
Table 18 below provides information on causes of authorised and unauthorised(�‘disobedience�’) absenteeism in 2008. The negative figures for MDGPs and ANMs may bedue to the fact that staffing is greater than the number of sanctioned posts.
89 WHO Country Office for Nepal (2007) Health System in Nepal: Challenges and Strategic Options90 NSI (2011) Hospital Management Training A Summary Report91 Ministry of Health and Population/RTI (2009) Human Resource Strategy Option for Safe Delivery Riitta Liisa KolehmainenAitken and Ishwar Bahadur Shrestha92 Ministry of Health and Population (2011) Department of Health Services Annual Report 2066/67 (2009 2010) pp. 127 130

38
Table 18 Causes of absenteeism among public health workers 2008
Staff category Filledposts
Presentlyworking
No.absent
%absent
Cause of absenteeismLeave Study/
trainingDeputation Disobedience
Regional/Zonal HospitalAnaesthesiologist 8 6 2 25 50 0 50 0Obs/Gyne 11 6 5 45 20 0 60 20Paediatrician 13 13 0MGDP 4 5 1Medical Officer 102 98 4 4 25 50 25 0Staff Nurse 328 284 44 13 7 39 32 23ANM
57 69 12 21 0 0 100 0Total 523 481 42 87 102 89 267 43
District HospitalPaediatrician 1 0 1 1 0 0 100 0Medical Officer 11 10 1 10 0 0 100 0Staff Nurse 44 36 8 18 12 50 25 13ANM 23 23 0 0Total 84 74 10 12 10 40 40 10
Primary Health Care CentreMedical Officer 6 4 2 33 0 100 0 0Staff Nurse 10 7 3 30 0 67 0 33ANM 41 39 2 5 0 0 100 0Total 57 50 7 12 0 57 29 14
Health PostANM 14 14 0
Source: MoHP 2009
PERFORMANCE MANAGEMENT SYSTEMS
There is a performance management system in operation in the civil service and somesectors and ministries such as Ministry of Finance (MoF) and MoGA are implementing it. It isthe responsibility of each sector to implement and adapt the system to its own needs. Arecent report suggests that the system of performance based incentives in place in MoGA ishaving very positive results on performance, particularly with staff working on the PIS,evidenced through improved and updated information systems.93
One of the strategies proposed in the National Planning Commission�’s Three year Plan(2010/11 2012/13) is to make �‘the implementation of the performance based employeereward and punishment policy effective�’, and employee's performance evaluation lesssubjective.94
A performance management system has not yet been implemented within the MoHP. Butthe NHSP 2 indicates that performance based and retention based payment systems will beintroduced during the plan period. Incentive packages for health works will be developed
93Ministry of Health and Population (2011). Human Resource Information System Assessment. Blair G., LATH94 Government of Nepal National Planning Commission (2010). Three Year Plan Approach Paper (2010/11 2012/13)

39
and piloted and operations research will be used to observe the impact on performance andretention.
Regular monitoring, supervision, facilitation, onsite support and technical backup and thedevolution and delegation of authority for case and resource management to the lowerlevels, will help to increase productivity and performance. A focus on the deployment ofteams of health workers as opposed to posting individual health workers will also help toensure the optimum skills mix to deliver quality services.
BASIC AND PRE SERVICE TRAINING
Nepal has numerous government and private sector pre service health training institutions.The professional councils oversee the training of health workers and the Council forTechnical Education and Vocational Training (CTEVT) oversees much of the lower leveltraining.95
In 2011 there are 16 medical colleges offering the MBBS programme, 2 offering the MBBSand BDS programmes and a further three offering only the BDS programme. These collegesare listed in Table 19.
95 See http://www.ctevt.org.np/about_ctevt.asp

40
Table 19 Medical Colleges 2011
No. Programme College1. MBBS TU Institute of Medicine, Maharajgunj2. Manipal College of Medical Science, Pokhara3. Bharatpur Medical College, Chitwan4. Nepal Medical College, Jorpati5. Kathmandu Medical College, Sinamangal6. Nepalgunj Medical College, Nepalgunj7. KU School of Medicine Science, Kavre8. National Medical College, Birgunj9. Janaki Medical College, Janakpur10. Nobel Medical College, Biratnagar11. KIST Medical College, Gwarko12. Lumbini Medical College and Research Centre, Palpa13. Chitwan Medical College, Chitwan14. Patan Medical Science Academy, Lalitpur15. Gandaki Medical College, Pokhara16. National Academy of Medical Science, Bir Hospital (conducting a
Post Graduate Program).17 MBBS and BDS BP Koirala Institute of Health Sciences, Dharan18 Universal College of Medical Science, Bhairahawa19 BDS People's Dental College, Naya Bazaar20 MB Kedia Dental College, Birgunj21 Kantipur Dental College, BasundharaSource: MoHP 2011
In 2008/09 there was an annual intake of 1,240 students into the Medical Colleges and 241students receiving scholarships. After graduation, scholarship holders are required to workfor two to five years in a government health facility. However as discussed few graduatesare willing to remain in government health service, with many preferring to work in theprivate health sector or abroad.
According to the MoHP, in 2011 there were 83 nursing schools accredited by the NepalNursing Council, providing all levels of education (e.g. ANM, PCL, Bachelor of Nursing,Bachelor of Science, Masters of Nursing, etc.). As shown in Table 20 the annual intake tonursing schools is about 1,300. Many of the teaching hospitals do not have a nursing school,which makes it difficult to retain nursing graduates in the government facilities. In 2009 theCouncil of Technical Education and Vocational Training (CTEVT) of the Ministry of Education(MoE) and its affiliated campuses was training approximately 1,000 ANMs annually everyyear.

41
Table 20 Annual intakes to Nursing Training Programmes 2007/8
Name of the Institution Annual IntakeTU �– IOM and its affiliated campuses 270BPKIHS 40Kathmandu University 40Council of Technical Education and VocationalTraining (CTEVT) 960Total 1,310Source: MoHP 2009
Because many of the nurses produced seek employment in the private sector and outsidethe country,96 the annual nursing output is insufficient to meet requirements for safedelivery in government health facilities at the lower levels.
The Nepal Health Professional Council 2010 data indicate that there are 78 institutes andcolleges offering Technical SLC, 63 institutions offering Proficiency Certificate Level, while 29offer Bachelor Degrees & higher qualifications abroad.97 Training opportunities in disciplinesthat are critical for service delivery, such as general medicine (MDGPs), anaesthesiology,(Anaesthesiology Assistants) and radiology are available, but not all of the places availableare filled.
Anecdotal evidence suggests that the quality of basic and pre service training, particularly inprivate sector training institutions, needs to be improved. Some of the health workersproduced by these institutions do not have the level of skills required to provide qualityservices. They often have to be retrained and/or receive intensive in service training toenable them to provide the services to the standards required. The 2008/09 MaternalMortality and Morbidity Study, found that some service providers, especially those inremote districts, reported lacking confidence in carrying out some procedures because theyhad not received training on new developments and there were no senior or appropriatelyskilled staff to support them in managing complicated cases.98
The TWG working on this area recommended the following interventions to improve thesituation: regulation of training by the MoHP in collaboration with the professional councilsand the MoE; revision and development of curricula; skills development for teaching staffand improved quality of instructional approaches. The MoHP plans to work with the Ministryof Education, universities, teaching institutions and the professional councils to regulatetraining to ensure that the staff it requires are being produced, and to improve the overallquality of training.
96 Ministry of Health and Population/ RTI (2009) Human Resource Strategy Option for Safe Delivery Riitta Liisa KolehmainenAitken and Ishwar Bahadur Shrestha97 Ministry of Health and Population (2011). Department of Health Services Annual Report 2009 201098 MoHP 2009 Maternal Mortality and Morbidity Study 2008/09

42
POST BASIC AND IN SERVICE TRAINING
The National Health Training Centre (NHTC) is responsible for developing and providing inservice training, upgrading and specialised training for public health workers, for thedevelopment of curricula and the training of trainers. The NHTC liaises with the PlanningDivision of the MoHP to identify the training needs of the different health programmes andprovides training programmes in line with the 2004 National Health Training Strategy and asdirected by periodic plans.
NHTC has provided basic training for ANMs, upgrading training for AHWs and ANMs, andreproductive health training. It also provides clinical and non clinical training. The NHTCoversees 5 Regional Training Centres and training is provided through a network of thecentral NHTC, 6 regional training centres, one sub regional training centre, 30 districttraining facilities, and 14 training health posts. There are also 18 clinical training sitesattached to regional and zonal hospitals for clinical competency based training. The trainingteams provide technical as well as managerial inputs for national, regional, district andcommunity level training programmes.99
During the NHSP 2, training will be decentralised to the district level to enable districts toplan and implement training relevant to their needs and to minimise the training burden atthe central level. Existing training and capacity building packages will be reviewed, revised,and used to support the Ministry�’s pilot initiative �‘Strengthening Local Health GovernanceProgramme�’.
The SBA In Service Training Strategy (2006 2012) aims to provide competency based inservice training in SBA to all eligible current and newly recruited ANMs, staff nurses, anddoctors who work in government facilities, and to increase the number of SBA training sites.It estimates that over 5,000 SBAs will need to be trained by 2012 to reach the target of 60%SBA assisted births by 2015.100 The Strategy proposes the establishment of additional SBAtraining sites and the incorporation of SBA skills training into pre service training curriculafor medical officers and nurses. By 2010, 2,535 SBAs had been trained.
Training will be provided to continue to improve SBA and MNCH skills of health workers.Training will be provided to MCHWs to enable them to upgrade to ANMs and toapproximately 1,200 Village Health Worker (VHW) who will upgrade to AHWs. The NHTC isalso planning to provide management and leadership development training programmes.
The NHTC has a Training Information System (TIS) that is an Oracle based system. It is notfully utilised currently due to capacity constraints and a paper based system is being usedinstead. NHTC plans to add additional fields to the database and is currently working with apilot district to help them capture the training it provides. It also intends to link the TIS andthe HuRIS.101 Strengthening the TIS will help with the monitoring of training interventions
99 Ministry of Health and Population (2011) Department of Health Services Annual Report 2009 2010 pp. 225 226100 Ministry of Health and Population/ RTI (2009) Human Resource Strategy Option for Safe Delivery Riitta Liisa KolehmainenAitken and Ishwar Bahadur Shrestha101 Ministry of Health and Population (2011) Human Resource Information System Assessment. Blair G., LATH

43
and reduce the need for individual training databases for different projects andprogrammes.102 It was reported that health workers sometimes attend the same coursetwice and that the investment in training is being lost because trained staff are being postedto facilities and posts where they cannot use the skills they have acquired through thetraining. With a link between TIS and a personnel database (either HuRIS or PIS), thisproblem may be avoided.
The NHSP 2 proposes that the role of the NHTC be re evaluated. It also recommends thatthere should be more integrated approaches to the delivery and monitoring of training toenhance quality and minimize cost. It proposes the formation of a National Health TrainingCoordination Committee to promote intersectoral training coordination and cooperation.
There are few districts with training facilities, and many are conducting training without thenecessary training infrastructure. Uncoordinated training is also contributing to absenteeismand affecting the availability of essential health workers. The 2011 MDG Assessment Reportindicates that staff in remote districts has not received adequate training on newdevelopments related to maternal health and were not competent to manage complicatedmaternal cases.103
An assessment of in service training and CPD capacity in the health sector in Nepal wasconducted in mid 2011.104 Findings indicate that the government is committed to trainingand has allocated financial and human resources for training interventions. Private sectorproviders are contracted to provide training and there are a number of �‘best practices�’training approaches being adopted in Nepal, e.g. workplace based training.
However the assessment also highlighted a number of improvement areas. Much of thetraining was found to be is �‘supply driven�’ and not based on individual and/or organisationalneeds and requirements. Training in topics such as management, human resources, datamanagement, finance, etc. is not provided. Many of the training approaches used areclassroom based and practical elements are weak. Training providers are not regulated andthe quality of some providers is poor. Overall a more systematic and coordinated approachwas recommended. This Assessment recommended ways in which the in service trainingand CPD system could be strengthened, and identified a number of priority areas foraction.105 These include:
Establishing a systematic and coordinated approach to in service training and CPDthrough the development of structures, strategies and plans aligned with the HRHStrategic Plan and in collaboration with stakeholders.
Ensuring continuous improvements in training approaches through scaling up goodpractices and revision of training materials in line with GESI principles.
102Ministry of Health and Population (2011) Human Resource Information System Assessment. Blair G., LATH103 National Planning Commission/UNDP (2011). Millennium Development Goal Needs Assessment for Nepal 2010104Ministry of Health and Population (2011). Training Capacity Assessment and Strategy Development. Elliot, L., LATH105 Ministry of Health and Population (2011). Training Capacity Assessment and Strategy Development, Elliot L, LATH

44
Strengthening institutions�’ ability to provide training and CPD, and strengthencontracting mechanisms and guidelines.
Improving current regulation mechanisms by promoting national and internationalpartnerships and making CPD a requirement for re registration with professionalcouncils
HR FUNCTIONS, SYSTEMS AND CAPACITY
The functions related to the HRP/M/D in the public sector are carried out by multiple actorsin a number of government organisations and agencies, including the MoE, Public ServiceCommission (PSC), Ministry of Finance, MoGA, the professional councils and in manydifferent units within the MoHP and DoHS. While there is logic to the allocation of thesefunctions, making the overall system work requires very effective coordination andcommunication.
Within the MoHP no single department has overall responsibility for HRH, responsibility isspread across three divisions (see Table 21). These include the Personnel AdministrationDivision, responsible for recruitment, posting and promotion of health workers; the HumanResource and Financial Management Division, concerned with human resource planning andHR development; and the Policy, Planning and International Cooperation Division,responsible for fellowship and scholarship programmes. Another three units under theMoHP namely the DoHS, Department of Ayurveda and Department of Drug Administrationalso perform a number of HR functions.
Both Joint Secretaries have HR in their remit and since they are of the same rank, which isalso equal to that of the Director of NHTC, neither is in a position to set the agenda forNHTC. In addition, both Joint Secretaries are employed by the Ministry of GeneralAdministration (under the Civil Service Act) and are subject to frequent transfers betweenministries.106
106 Nepal Health Sector Support Programme (2010) Draft Capacity Assessment for Health System Strengthening. Anassessment of capacity building for health systems strengthening and the delivery of the NHSP 2 results framework. Martineau,T (LATH)and Subedi H. N.

45
Table 21: Units of the MoHP involved in HRH
Joint Secretary HumanResources and Finance
Division
Joint Secretary PersonnelAdministration Division
Policy, Planning and InternationalCooperation Division
Human ResourceDevelopment Section(includes HuRIC)
Personnel AdministrationSection
International Support,Scholarships, InternationalCooperation Coordination Section
Promotions SectionActs, Regulations &Consultation Section
Source: MoHP 2010
The Administration of the DOHS and the Regional and District Offices deal with posting andthe transfer of staff according to grades as shown in Table 22 below.
Table 22: Posting and transfer authority by level of institution
Institutional level GradesDOHS 6 7Regional office 4 5District office 1 4Source: MoHP 2010
The PSC is responsible for recruitment and promotion of approximately 80,000 governmentstaff, including those employed by the MoHP. It manages a quota system for recruitment aspart of positive discrimination policy to improve social inclusion. Its Regional and Zonaloffices have delegated authority.107 As part of a 3 year reform programme the PSC isstreamlining its procedures with support from the ADB supported e governance project.
The role of MoGA is to regulate and manage the civil service as prescribed by thegovernment�’s rules and regulations and management of pension entitlements. 108 Itoversees the structures and staffing (establishment) of government departments and keepsrecords of civil servants. MoGA seconds administrative staff to other ministries.
Professional councils, namely the Medical Council, the Nursing Council and the PharmacyCouncil, are responsible for registration, licensing and accreditation of training institutions.They register new graduates, oversee the training curriculum and approve new traininginstitutions.
Because there are multiple actors, with sometimes opposing interests, involved in the HRfunctions, approaches to HR planning, management and development can be fragmented
107 See http://www.psc.gov.np/engintroduction.php108 See http://www.moga.gov.np/beta/index.php#

46
and poorly coordinated. Many of the staff responsible for HR are employed by MoGA andcan be transferred at any time, leading to a high turnover of staff.109
However there have been some recent improvements in the planning, management anddevelopment of HRH, and some effective systems and practices are in place, as evidenced bythe award Nepal received from the UN for progress towards MDG 5. Other initiatives andinterventions have been undertaken, including the establishment of structures anddevelopment of plans which provide strategic oversight and directions for HRH, e.g. theestablishment of the Country Coordination Facilitation (CCF) mechanism provides directionfor HRH interventions and the NHSP 2 has made provisions for strengthening HRH planning,management and development. Systems and procedures are being strengthened to addressstaffing shortages and performance issues; e.g. contracting arrangements have beenestablished for doctors after completion of scholarships, arrangements have beendeveloped for staff to cover for those on study and leave, and a proposal for a performancebased incentive scheme for doctors has been submitted to the MoF for approval.
An assessment of the capacity for HR planning, management and development wasconducted in 2010.110 It noted that the CCF would provide a forum for improved stakeholdercollaboration and communication, and that the new HRH Strategic Plan would provide amore strategic direction for HRH interventions. However, it also confirmed that HRHstructures and systems in the MoHP and across government were fragmented andincomplete. There was a low skill base in strategic HR planning and management, and therewere no structures in place for coordinating HRH across the health sector and for aligningstaffing requirements with the rapidly expanding supply from training.
HR information systems
Two major HR databases exist with data on the health workforce employed by thegovernment The HuRIS is the MoHP�’s information system, which maintains information onstaff employed in the health sector only. The MoGA has a hard copy file database for allgovernment employed staff that was recently overhauled and updated for healthemployees. It also manages the PIS, which is housed within the Department of CivilPersonnel Records (DoCPR). The PIS is the repository for HR information for the whole of thepublic service and is used for managing pensions. The DoCPR keeps records and informationof the 87,000 government employees (with the exception of teachers, police, paramilitaryand armed forces).
It was originally planned that the HuRIS would include other government sectors (e.g. police,army) and the private sector, but this has not yet happened. The HuRIS contains detailed jobrelated information on each individual, including job history, training and personal detailsbut is slow and offers limited information because it is dependent on largely voluntary self
109 Information based on interview with MoHP110 Nepal Health Sector Support Programme (2010) Draft Capacity Assessment for Health System Strengthening. An assessmentof capacity building for health systems strengthening and the delivery of the NHSP 2 results framework. Martineau, T(LATH)and Subedi H. N.

47
declared information inputs. Though HuRIS is capable of forecasting the retirement andreplacement of staff, the data are incomplete and could not be used as a reliable planningand management system. The major problems appear to be with regular updating of thesystem at district level, due to poor internet connectivity in some locations and highturnover of trained operators, especially at district and institutional levels. Professionalcouncils also hold data on key professionals for which they are responsible. However, thevalidity of these data is also uncertain and the systems do not monitor, for example, trainingand education for all members.
There are limited data available in the MoHP to provide evidence of the main HRH problemsand challenges, and to identify which cadres are the most affected. There is a lack ofaccurate and comprehensive routine workforce information at the national level and thereare no readily available and up to date figures showing flows and trends in the main staffgroups, such as doctors and nurses, over the last decade. Many of the reports cited aboveare using data on staffing that is three years old or older.111
A survey in 2008 demonstrated the lack of consistency in staffing data collected in the fieldand the Human Resource Information Centre (now referred to as HuRIS). It raised concernsabout the quality of the information for human resource planning, training, andmanagement.112 This was echoed a year later in the NHSP 2 when it was noted that �‘thepresent human resource information system HuRIS is not up to date and is believed tocontain only three fourths of the total personnel�’.113 This Plan contains strategies andactivities to strengthen HuRIS so that it can generate and provide up to date and reliableinformation for managing human resources. The MoHP is adapting WHO instruments andtemplates and will soon begin collecting, compiling and maintaining data on both theprivate for profit and private not for profit/NGO sectors. 114
In 2011 an assessment of the Human Resource Information System was conducted.115 Its keyfindings and recommendations are presented and discussed below.116
National statistics on staff numbers are not being collected and reported on a routine basis,making it difficult to monitor and track staff movements. Job classifications are inconsistent,which makes identifying trends in staffing difficult, due to classification of staff categories.The MoHP tends to get national workforce data from regions rather than use HuRIS,because of its unreliability. Because the HuRIS information on new entries and resignationsis incomplete, it cannot be used to monitor staff flows, particularly staff losses/attrition.
111 Ministry of Health and Population (2011). Human Resource Information System Assessment. Blair G., LATH112 Ministry of Health and Population/ RTI (2009). Human Resource Strategy Option for Safe Delivery Riitta Liisa KolehmainenAitken and Ishwar Bahadur Shrestha113Ministry of Health and Population Government of Nepal (2010) Nepal Health Sector Programme Implementation Plan II(NHSP IP 2) 2010 �– 2015 Final Draft 18 March 2010114 Ministry of Health and Population (2011) Milestone 7: Periodic Review on the development of the HR Plan (Draft)Martineau, T. & Bista, B. (2011). Nepal Health Sector Support Programme115 Ministry of Health and Population (2011) Human Resource Information System Assessment. Blair G., LATH116 Ministry of Health and Population (2011) Human Resource Information System Assessment. Blair G., LATH

48
The PIS is currently being upgraded and the database is being validated to develop it into afully functioning HuRIS and paperless process for HR administration. If the PIS can produceaccurate workforce reports and meet the needs of the MoHP given the current investmentin its upgrading, a decision may need to be made as to whether efforts should continue tobe made to strengthen and improve the HuRIS. However, HuRIS may still be needed as theMoHP role in HR planning is envisioned to increase significantly, with the production of alarge number of reports on a routine basis. This includes an annual report of HR information,which should also be published on the MoHP website.117
Regions, Districts and Hospitals produce workforce reports on sanctioned and filled postsand vacancies, which are used to plan and monitor recruitment. Staff in 73 out of 75 districtshave been trained in entering data into HuRIS, but some of those trained have beentransferred and their replacements are untrained and therefore do not use the system.118
Workforce information that is available at region and district levels should be submitted tothe MoHP on a regular basis to enable the MoHP compile annual workforce reports,including reports on sanctioned and filled posts and vacancies for the main staff groups.Additional staff should be trained in the analysis of workforce information and the use ofExcel�’s spreadsheet and graphics functions.
Systems and procedures are needed to ensure that routine workforce information iscollected on a regular basis. Workforce information should be updated each year and a timeseries produced to show changes year by year. In order to monitor initiatives aimed atimproving the retention of essential staff in rural areas, recruitment and vacancy figuresshould be monitored on a regular basis. Data on staff losses (e.g. resignations, retirement,etc.) and age profiles should be collected by staff group, on an annual basis and publishedfor MoHP planning and budgeting cycle purposes. An annual report on all HR Informationshould be produced. The training information system is currently being strengthened andexpanded, and once it is fully functional data on the number of newly qualified staffgraduating for each profession should be collected annually.
PROJECTING HRH REQUIREMENTS AND WORKFORCE PLANNING
A Health Workforce Plan will be developed in Year 1 to support improved workforceplanning and will provide short, medium and long term HRH projections. A more completeand comprehensive HRH profile will be required for the Workforce Plan, which will highlightthe shortages and skills gaps and forecast the numbers and cadres required to close the gapsbetween the future demands and the current workforce. Capacity will be developed forworkforce planning and planning processes and systems institutionalised within the MoHPso that the Plan can be monitored, reviewed and adjusted on an annual basis.
The first step in developing the Health Workforce Plan will be to update and validate currentHRH data and the MoHP has already begun collating and analysing data in order to develop
117 Ministry of Health and Population (2011) Human Resource Information System Assessment. Blair G., LATH118 Ministry of Health and Population (2011) Human Resource Information System Assessment. Blair G., LATH

49
a more comprehensive profile of the workforce in the public and private sectors. The MoHPwill also continue to strengthen the collection, analysis and capturing of routine workforceinformation and to improve systems and capacity to maintain and monitor these data. Thiswill ensure that reliable data are available in a timely manner for policy makers, decisionmakers and managers to inform HR decision making and will provide a solid foundation andevidence base for workforce planning.
The MoHP will ensure that the current and future service delivery requirements are keyconsiderations in developing the projections. Other factors, such as free health services;utilisation; infrastructural development; GESI; the provisions of Health Services Act,119
financial resources, decentralisation and greater involvement of the private sector will alsobe considered.
Routine monitoring information and survey data (e.g. MoHP HuRIS and HMIS, MoGA PIS,Demographic and Health Surveys, etc.) will be used to develop and review the projectionsand make the necessary adjustments.
The MoHP will review various options for developing the projections and select the mostappropriate. Options that could be used to determine the HRH projections could be:
based on the number of vacant sanctioned posts
based on the catchment population
based on changes in patterns of disease and to meet health needs, including thenumbers and kinds of services required to respond to these outcomes. This couldentail collecting and analysing a range of demographic, sociocultural andepidemiological data
based on service demands and the utilization rates for different population groups,and applying these to the future population profile to determine the scope andnature of expected demands for services
based on service targets e.g. specifies targets for the production (and presumedutilization) of various types of health services and the institutions providing thembased on a set of assumptions, and determines how they must evolve in number,size and staffing in accordance with productivity norms.
Currently the recruitment and deployment of HRH are controlled by a sanctioned postsystem, and workforce planning is based on facility based staffing standards in which thereare fixed numbers of sanctioned posts for each category of staff per level of health facility.Stakeholder consultations and participation in the workforce planning will be facilitated toensure that a balance is struck between the professional ideal and what is economically
119 A recent amendment proposed to the Health Service Act states that �‘45% of the posts to be filled by open competition shallbe set aside and be filled up by having separate competition between women, Adiwasi/Janjati (ethnicity), Madhesi, Dalit,disabled and backward groups�’. It also states that the employees may form trade unions under the provision of this Act.
50
affordable.120 The workforce planning process could be undertaken incrementally, forexample as a pilot in a particular region or district.
Workforce demand is sometimes based on activity ratios that link the number of staff to thevolume of work e.g. �‘nurses per occupied bed�’. However, the ratios need to be agreed,usually using international comparisons as a starting point, suitably adjusted for degree ofcomplexity and other contextual factors. For example, surgeon numbers are oftendetermined by the number of operations undertaken, the acuity of patients and thecomplexity of the procedures. Demand exercises will be undertaken with inputs frommembers of the health professions who are actively engaged in clinical work.121
Recent plans and various new health initiatives and programmes call for the recruitment anddeployment of additional staff for the MOHP as shown in the Table 23 below.
120Ministry of Health and Population (2011). Human Resource Information System Assessment. Blair G., LATH121Ministry of Health and Population (2011). Human Resource Information System Assessment. Blair G., LATH

51
Table 23 Proposed HRH requirements
Source Cadre Quantity Additional Information
NHSP 2 SBA 6000 1000 SBAs available34 MDGPs availableChronic shortage ofanaesthetists, psychiatrists,radiologists, radiographers,anaesthesia assistants).
All cadres to be provided overthe 5 years of the NHSP 2
MDGPs 90Anaesthetists 44Radiologists 55Physiotherapists, 20PhysiotherapyAssistants 70Psychiatrists 56Radiographers 100AAs 62ANMs
1000
An additional 1,000 ANMs(200 per year) will be recruitedfrom the Dalit and otherexcluded groups
Doctors, 3 nurses,and support staff
Not specified
The number of communityhospitals is expected toincrease and one additionaldoctor, 3 nurses, and supportstaff will be required to runthese community hospitals ona 24/7 basis.
HAs
3,100
3,100 SHPs will be upgraded toHPs during NHSP 2. Each newHP will require an additionalHA
Mobile Teams
Not specified
Mobile teams will beorganised to provide specialistservices to remote areas.
NHSP 2 Health systemrelated staff
7 procurementspecialists3 health legislationexperts7 epidemiologists7 health economists3 health governanceexpertsUnspecified numberof healthinformationspecialists, HRmanagers, hospitalmanagers
There is a shortage of humanresources related to healthsystems managementprocurement specialists,health legislation experts,epidemiologists, healtheconomists and healthgovernance experts
The NationalSBA Policy(2006)
Identifies maternal healthstaffing requirements forhealth posts and sub healthposts

52
Source Cadre Quantity Additional Information
2008 NepalSafe DeliveryField Survey
Staff to provideMaternal and ChildHealth Services
Required mainly at districtand community levels
DoHS AnnualReport2066/67(2009/2010)
ANMs
Vaccinators
Insufficient number of SBAscreate ANM posts for healthfacilities in remote hill andmountain districtsIncrease number of SBAtraining sitesAlternative provision ofvacant post of vaccinators (Fillvacant post or contract outlocally)Reallocate existingImmunisation staff atdifferent levels
FHD/MOHPO&M SurveyReport 2011
MDGPs,Gynaecologists &AnaesthesiaAssistants for CEOCservices
28 MDGPS12 Gynaecologists40 AnaesthesiaAssistants
O&M survey conducted byFHD/MOHP for 40 districts forthe creation of posts forMDGP/Gynaecologist andAnaesthesia Assistant forCEOC service
MoHP O & MSurvey
Specialists330
2011 MDGAssessmentReport
Staff to provideMaternal and ChildHealth, Malariaand TB services
Additional staff required toprovide maternal and childhealth services and to supportthe delivery of malaria and TBservices.
2011 ReadinessofComprehensiveEmergencyObstetric andNeonatal care
At least oneMDGP/OBGYN & ½Advanced SkilledBirth Attendants(ASBAs) plus asupport team (2AAs, OT Nurse,supported by asenior CS doctor ineach CEONC district
Preliminary Projections
In December 2011 the MoHP developed preliminary projections for key cadres as shown inTable 24. It estimated that approximately 14,210 doctors, nurses and paramedic staff wouldbe needed over the four years of the Plan. The Nepal Ayurveda Medical Council estimatesthat it would need an additional 2,642 Ayurvedic health providers over the next 5 years. In2012 the Nepal Pharmacy Council indicated that it would need a total of 4,292 staff by 2025to staff all the retail and wholesale pharmacy units in the country.

53
Projections for other cadres such as pharmacy and traditional medicine will be developedduring the proposed workforce planning process in Year 1. There are notes that provide anexplanation of how the projections were calculated given below Table 24.

54
Table 24 Preliminary projections 2011
No. Cadres Posts ExistingNo.
AdditionalNo.
RequiredRemarks
1. Medical Doctors 1.1 Specialists: 9th,10th and 11th level
330
1.2 8th Level MBBSDoctors1.2.1 Physiotherapists1.2.2 Pathologists1.2.3Ophthalmologists
479
151315
1.3 BDS Doctors 802. Staff
Nurses/Nurses (a) For 1204 HPswith Birthing Centres(BCs)(b) For 2636upgraded HPs(c) For 240 PHCs(d) For Districtlevel and above
1203 8690
2408
5272240770
Including forproposedbirthingcentres
3. Health Assistants(HA)
1244 3536
4. Auxiliary HealthWorkers (AHW)
AHWVHW
49233958
n/a VHWsupgraded toAHWs
5. ANMS ANMMCHW
17813307
n/a MCHWupgraded toANMStaff nursesare proposedinstead ofANMs
6. Paramedics 7648
6.1 Lab Technicians (LT) 435
6.2 Radiographers 3556.3 Anaesthesia Assistants 1416.4 Physiotherapy
Assistants28
6.5 Ophthalmic Assistants 656.6 Psychiatrists 28
Total 14210

55
Notes:1.1 This number is based on the negotiation between MoHP & National Medical Association(NMA) in 2010 about increasing the number of sanctioned posts of specialist doctors
1.2 The 479 posts of MBBS Doctor are proposed for Central level hospitals (3 for 13 centralhospitals; 2 for 15 regional/zonal hospitals; 2 for 65 District Hospitals; 2 for 20 Ruralhospitals; and 1 for 240 PHCs1.2.1 This post is proposed for regional/zonal hospitals1.2.2 This post is proposed for central level hospitals1.2.3 This post is proposed for regional/zonal hospitals
1.3 One BDS Doctor post is proposed for 15 regional/zonal hospitals and 65 district levelhospitals
2. The 8690 nurses posts are proposed on the basis of 2 for 1204 HPs (with BC); 2 for 2,636upgraded SHPs; 1 for 240 PHCs; 3 for 20 Rural hospitals; 4 for 65 District Hospitals; 10 for 11zonal hospitals; 20 for 4 regional hospitals; and 20 for 13 central hospitals
3. One each for the upgraded SHPs, and one third of AHWS
4. This post has not been proposed. Only HAs are proposed
5. Staff Nurse posts are proposed instead of ANMs
6.1 435 Lab Technician (LT) posts are proposed as follows: 1 for 240 PHCs; 1 for 20 RuralHospitals; 2 for 65 District Hospitals; and 3 for 15 regional/zonal hospitals6.2. 355 Radiographer posts are proposed as follows: 1 for 240 PHCs; 1 for 20 RuralHospitals; 1 for 65 District Hospitals; 2 for 15 regional/zonal hospitals6.3. 141 Anesthetist Assistant posts are proposed as follows: 1 for 20 Rural Hospitals; 1 for65 District Hospitals, 2 for 15 regional/zonal hospitals and 2 for 13 central hospitals6.4. 28 Physiotherapy Assistant posts are proposed as follows: 1 for regional/zonal hospitals,1 for central level hospitals6.5 65 Ophthalmic Assistant posts are proposed for all District hospitals6.6 28 Psychiatrists posts are proposed as follows: 1 for central level hospitals and 1 forregional/zonal hospitals

56
Section 4 Aim, Outputs, Strategies & Activities
Aim Of The HRH Strategic Plan
The overall aim of the HRH Strategic Plan is: �‘to ensure the equitable distribution ofappropriately skilled human resources for health (HRH) to support the achievement ofhealth outcomes in Nepal and in particular the implementation of NHSP 2�’.
In order to contribute to this aim, the main focus of the specific strategies and activities willbe to support the achievement of the following four outputs:
1. Appropriate supply of health workers for labour market needs2. Equitable distribution of health workers3. Improved health worker performance4. Effective and coordinated HR planning, management and development
across the health sector
The HRH Strategic Plan is a four year plan, aligned to the remaining timeframe of the NHSP2, covering the period from 2011 to 2015. The strategies and activities contained in the Planhave been designed to build on the achievements of the first NHSP (2004 2010) and tosupport the implementation of the HRH strategies contained in the NHSP 2. It responds tothe HRH situation analysis conducted by the TWGs that were formed to support thedevelopment of the Plan. It responds to the issues, challenges and findings contained inassessments and surveys such as the 2008 Nepal Safe Delivery Field Survey, the 2010assessment of HR planning, management and development capacity, the 2011 MDGAssessment Report, and the 2011 assessments of the MoHP HR information systems and inservice training capacity. It aims to support the health sector in its efforts to develop a�‘comprehensive and balanced package of measures �….to support improvements in healthsystem performance�’.
This section presents the outputs, strategies and activities to be undertaken and achievedover the timeframe of the HRH Strategic Plan. A broad mix of strategies and approaches isrequired to improve the current situation and address the challenges that exist. Many of thestrategies and activities in this section focus on HRH challenges in the government sectorbecause limited information was available on the private and NGO sectors when this Planwas being developed. However, there are studies currently being conducted and othersplanned that will provide information on these other sectors and help with the productionof a more comprehensive profile of the overall health workforce.
The HRH Strategic Plan includes strategies and activities to strengthen HR functions,capacity, structures and systems to manage and develop HRH and to improve stakeholdercollaboration and coordination of HRH across the sector. There are strategies and activitiesto strengthen the attraction, recruitment, deployment and retention of essential cadres, andto strengthen pre service and in service training to improve health worker skills andperformance. Strategies and practices adopt a gender and social inclusion perspective.Marginalised groups will be trained and retained in the health sector to provide services

57
across the sector, but especially to underserved populations. Strategies to strengthenpublic private partnerships and to improve the involvement and participation of the privateand NGO sectors in the provision of services are also included in the Plan.
Some of the strategies and activities contained in the Plan relate to the whole sector; butmost focus on the MoHP and government health workers. Activities that have beenprioritised for inclusion in a costed Year 1 Implementation Plan are indicated and these willbe further developed into sub activities. Annex 2 presents more detailed activities and subactivities for each of the strategies.
Output 1: Appropriate Supply Of Health Workers For Labour Market Needs
Strategy 1.1 Improve HR Planning For The Health Sector
HR information systems (HuRIS) and leadership and HR planning capacity will bestrengthened to ensure that relevant, reliable and up to date information on HRH across thesector is available for HR Planning and the development of a Workforce Plan.
The MoHP will focus on updating and validating current HRH data and ensuring that routineworkforce information is collected and analysed on a regular basis for the governmentsector in the first instance. Systems and capacity will be strengthened to maintain andmonitor HRH trends and initiatives (e.g. monitoring and managing entries and exits from theMoHP) and mechanisms put in place to make this information available to policy makers,decision makers and managers. A gender and social inclusion perspective will be adopted inthe design of data collection tools and the analysis of data.
Once the government system is functioning in the MoHP and data available on governmentsector employees, the MoHP will begin collecting and analysing information on the privateand NGO sectors. There are a number of ongoing initiatives and others planned that willcontribute to the information gathering and analysis processes and support thedevelopment of a more comprehensive profile of HRH across the sector. An annual ServiceTracking Survey, which collected data on HRH from a sample of facilities, was conducted in2011. The MoHP has also begun compiling a national HRH profile. Other organisations, suchas NGOs, private health providers, and the professional councils will also be supported tostrengthen their information systems.
All of these initiatives will contribute to establishing an improved evidence base for HRH inthe country. The information generated will also support the MoHP to undertake a morecomprehensive workforce planning exercise across the whole health sector (including theprivate and NGO sectors). Workforce monitoring information will be available to helpmanagers and decision makers to plan and review the impact of HR policies andinterventions. Monitoring historic trend information will show how staff numbers havechanged over a period of time and how this compares with utilisation levels, case loads andtotal population. The availability of information on recruitment, distribution, age profiles,staff losses (e.g. resignations, retirement, etc.) will help to inform planning and management

58
decisions, including retention and performance issues. The HuRIS will be strengthened tomanage and maintain these HR data and to generate reports that will support HR planningand management processes. Linkages and networking between the HuRIS and othergovernment information systems, such as the PIS and the TIS will also be strengthened.
Strengthen leadership and capacity in HR planning, including the HR Division in MoHP,Department of Health Services, and staff at regional and district levels
Strengthen HR information systems and capacity within the MoHP to generate reliableand up to date information on HRH, firstly in the public sector and thereafter in theprivate and NGO sectors, for routine and strategic HR planning and management (Year 1and ongoing)
Improve availability and use of disaggregated HRH and training information (e.g. gender,caste, ethnicity, cadre, facility, geographical area) for HR planning and management(Year 1 and ongoing)
Collect and analyse information on service needs across the health sector (Year 1) Produce Health Workforce Plan (by June 2012) that will determine HRH requirements
(numbers, skills, gender, etc.) and supply to meet service delivery needs across thesector over the short, medium and long term (Year 1)
Develop capacity and establish and institutionalise planning mechanisms Put HURIS online and provide training to relevant field staff
Strategy 1.2 Improve Recruitment And Deployment Processes And Ensure They AreEffective And Timely
The timely recruitment and deployment of essential health workers is a challenge in thepublic health sector. There are various factors that affect the effective functioning of therecruitment and deployment systems, including: a lack of information on vacant positionsand shortages, weak systems to implement and enforce recruitment and deploymentpolicies and processes, and financial constraints and lengthy procedures to establish andsanction additional government posts for critical and scarce staff.
The MoHP will work more closely with the PSC, which is responsible for the selection ofpermanent staff, to ensure more effective and timely recruitment procedures. Procedureswill be streamlined, and GESI principles adopted to ensure that all the trained healthprofessionals available in the labour force are attracted into the health sector and are moreequitably distributed. The findings and recommendations of the O&M surveys that havebeen conducted will be reviewed and progress and/or bottlenecks in having the postsapproved and created will be assessed. Information will be collected on the numbers andtypes of unemployed health workers available and plans developed to fast track their entryinto the public health sector. Information and communication systems will be improved toensure that recruitment information on the jobs available in the public health sector is morewidely disseminated and targets graduates.
Frequent transfers are impacting on staff utilisation and productivity, especially onteamwork when one of the team is moved. The implementation of the transfer policy will be

59
reviewed to assess the extent to which political influence is impacting on the effectivetransfer of staff and how exiting procedures are impacting on staff shortages,maldistribution, underutilisation, and/or team working and productivity. The policy will alsobe reviewed for its gender implications.
More focused efforts will be made to increase the numbers of MDGPs recruited anddeployed to rural areas, as this cadre is increasingly recognised as the most appropriatemedical doctor cadre for rural areas.122 Increased numbers of midwives, nutrition personnelas well as hospital and health facility managers are required. People with these skills andqualifications are available in the labour force, and efforts will be made to attract anddeploy them to the facilities where they are needed.
Female Community Health Volunteers (FCHVs) support and promote the utilisation of healthservices. A FCHV Fund has been established to support the activities of the volunteers. Anelectronic database has been developed and is used at the central as well as district levelsfor the planning and implementation of the FCHV programme.123 Further studies will beconducted to assess their impact on service delivery and health outcomes.
The NHSP 2 indicates that multi year contracts will be provided for obstetric, gynaecological,paediatric, physiotherapy, and other diagnostic support services.124 To ensure that thesehealth workers and the others that are required are recruited as efficiently as possible,contracting procedures will be streamlined and strengthened and multi year contractingexpanded.
The reasons for short term contracting and local contacting need to be better understood,and studies could be conducted to examine factors such as: insufficient sanctioned posts,lengthy centralised recruitment processes, difficulties attracting and retaining staff, or lackof people with these skills in the labour market. The proposed review of localrecruitment/contracting procedures and practice will also examine these factors, assess theextent to which procedures are transparent and equitable, and determine whetherappropriately skilled staff are being appointed and deployed. The overall cost of short termcontracting will be examined and compared with the cost of creating sanctioned posts todetermine where efficiencies could be made.
Where local contracting is taking place, priority will be given to the recruitment of local staffand candidates from marginalised communities who have the required skills. Staff on localcontracts will also be given the same in service training opportunities as other healthworkers, so that they too can update and refresh their skills.
Mechanisms to monitor and manage the quality and performance of contract staff will alsobe strengthened. Other employment arrangements and contracting options will be
122 The Nick Simons Institute has developed a scholarship system for MDGP doctors; according to the NSI Report on Five Yearsof Progress 2006 11 the MOHP recently asked the NSI to �‘rapidly and widely scale up�’ the Rural Staff Support Programme.123 Ministry of Health and Population (2011). Department of Health Services Annual Report 2066/67 (2009 2010) pp. 119 120124 Ministry of Health and Population Government of Nepal (2010). Nepal Health Sector Programme Implementation Plan II(NHSP IP 2) 2010 �– 2015 Final Draft 18 March 2010 p.65

60
explored. For example the contracting function could be outsourced to another agency suchas an NGO or a private organisation, which could also be given responsibility for managingthe performance of the contract staff. Other options could include the creation of a HealthService Commission, giving the districts more responsibility and authority for recruitment,etc. The role of the Health Facility Management Committee (HFMCs) in the recruitmentprocess and the management of contract staff will also be reviewed.
Existing recruitment and deployment systems and practices will be reviewed throughsystems audits to identify a) whether the practices are complying with policies andprocedures, including GESI principles, and b) where the bottlenecks are.
Assess current recruitment and deployment processes and systems, identify problemsand bottlenecks, including GESI related issues and use findings to streamline andstrengthen systems
Review and strengthen contracting systems and practices (including expansion of multiyear contracting)
Review O&M studies and identify and advocate for priority vacancies/positions to befilled (informed by health workforce plan and workforce projections to be developed inYr 1)
Create management and other health systems posts to improve the management ofhospitals and other health facilities and overall health systems, e.g. HR planning,management and development, health economics, procurement, logistics, etc.
Use Health Workforce Plan and HRH projections to guide recruitment and posting ofstaff according to job requirements (Year 1 and ongoing)
Determine number of trained unemployed health workers available for work andimplement procedures to attract, recruit and deploy (Year 1)
Review and assess experience with local recruitment/contracting to ensure that systemsand processes are transparent and equitable, and that appropriately skilled staff arebeing hired before expanding its use
Explore and practice alternative recruitment and employment arrangements (e.g. multiyear contracting, creation of a Health Service Commission, etc.)
Review and document the role and contribution of FCHVs to delivery of health services
Strategy 1.3 Improve Attractiveness Of Jobs For Increased Recruitment AndRetention
All employers need to ensure that they have robust systems and procedures in place toattract, recruit and retain adequate numbers of staff with the appropriate skills to fill vacantand new posts in facilities at all levels. Strategy 2.2 below provides more details on issuesand activities related to retention and making jobs and postings in the rural areas moreattractive. Employers need information on the labour market and need to understand healthworker job preferences and job seeking behaviour. Employers can use this information toimprove the attractiveness of jobs in the health sector, especially in the government healthsector, which may include reviewing the conditions of service, remuneration and otherincentives (e.g. recognition and rewards, career development training opportunities, etc.).

61
The MoHP will improve its understanding of the reasons health workers leave not just thecadres (e.g. nurses), but also the different health workers within those cadres (e.g. staffnurses) in order to target and differentiate attraction and retention strategies. Attritionrates and trends will be monitored and the information used to develop the mostappropriate strategies differentiated according to health worker cadre, gender specificneeds, the job and the service needs of the location and/or facilities.
Information (disaggregated) collected and reviewed on job preference and job seekingbehaviour
Labour market information reviewed regularly (Year 1 and ongoing) Develop/improve GESI sensitive policies to manage retention
Strategy 1.4 Ensure Basic And Pre Service Education And Training Is In Line WithRequirements For The Health Sector
The MoHP, particularly the Department of Health Services (DoHS), will work closely with theMoE and the training institutions, to ensure that the training and education systems forhealth professionals are aligned with and informed by MoHP programmes and healthpriorities. They will work in collaboration with the Professional Councils to regulate andsupport training institutions/providers to enable them to produce adequate numbers ofhealth workers with the relevant and appropriate skills and knowledge to deliver healthservices to the standards required. They will explore innovative ways to improve the qualityand relevance of health training systems such as the models and approaches discussed at arecent workshop for health training stakeholders facilitated by the MoHP e.g. the �‘adopt adistrict�’ model.
Producing for requirements will also reduce over production and will help to refocustraining investments on less qualified staff and on producing staff with the skills that areneeded at the district level and below. Highly qualified staff often do not have skills that arerelevant and appropriate for the lower levels of the health system. Greater synergy will befostered between basic and pre service training systems and in service training and CPDsystems so that the investment in health training and development produces health workerswith appropriate and relevant skills and knowledge.
Mechanisms and processes to regulate and assure the quality of training institutions andproviders will be reviewed and strengthened. Memoranda of Understanding (MoUs) and/orformal service agreements will be signed with private training institutions, training curriculaand programmes will be reviewed and standardised, and systems put in place to assure thequality of their outputs. The MoHP will support and strengthen the Health ProfessionalCouncils to enable them play a greater role in the accreditation, review and regulation ofhealth training institutions.
The TIS is currently being strengthened and expanded and when it is fully functional, it willproduce data on the numbers of newly qualified staff graduating for each profession

62
annually. Aligned with information on service delivery needs, this will help to inform trainingplans and programmes. The TIS is currently being strengthened; once it is fully functionaldata on the number of graduates for each profession should be collected annually.Information on Pre Service Training (PST), In Service Training (IST) and ContinuingProfessional Development (CPD), such as information on numbers and types of trainingprogrammes provided by government and private institutions and providers, curricula andprogramme content, number and capacity of facilities, numbers and types of teaching staff,current and projected intakes and outputs will be required to strengthen the planning andcoordination of human resource development systems.
The MoHP will continue to invest significant resources in pre service and in service trainingprogrammes over the timeframe of the NHSP 2 and this Plan to produce a health workforceequipped with the skills to deliver quality services and achieve health outcomes. Based onthe findings of various studies and reviews of HRH for maternal health and stakeholderconsultations, it has been agreed that the recently drafted post basic Bachelor MidwiferyProgramme will be piloted with existing PCL nurses. When these nurse midwives graduatethey will not only serve as service providers with international midwifery educationalstandards, but will also have acquired skills in management, teaching (i.e. SBA trainers),supervision, monitoring and evaluation. The MoHP will develop supportive policies andguidelines that will define their roles and responsibilities, as well as outline regulation,recruitment, deployment, and retention arrangements.
Supportive supervision and post training follow up will be improved to support healthworkers to use and apply their skills and to assess the relevance and appropriateness of theskills and knowledge acquired. The training will be evaluated to assess the impact onperformance and service provision and the findings used to improve the design and contentof further training programmes.
Collect data on current projected production and assess potential for increase/decreaseof specific cadres (Year 1 and ongoing)
Strengthen mechanisms for communication and collaboration between MoHP and MoEand establish inter ministerial fora (to include MoHP, MoE, National PlanningCommission, MoF, PSC, etc.) to coordinate and address production and regulatory issues
Work with the MoE to expand/reduce training, informed by service delivery needs e.g.produce MDGPs, Hospital Managers; establish more rural based trainingsites/institutions, etc.
Improve accreditation and regulation of pre service training institutions to ensure anadequate supply of appropriately skilled and knowledgeable health workers and assurethe quality of the training provided
Strengthen mechanisms to follow up and support health workers after training and toevaluate the impact of the training on performance.

63
Output 2 Equitable Distribution Of Health Workers
Strategy 2.1 Review Current Distribution Trends And Processes And EnsureDeployment Systems Result In Equitable Distribution Of Health Workers
There are various types of workforce distribution problems, and while the focus in this Planis on rural versus urban distribution, the needs of urban populations and the quality ofurban health services will also need attention in the coming years. These will be addressedin part by the upcoming urban health strategy. A good starting point for improvingworkforce deployment systems and practices would be a review of WHO's recent guidelineson staffing remote areas to identify interventions that may be replicable in the Nepal healthcontext.125
The equitable distribution of staff depends on the availability of good data to determinewhere the vacancies and greatest HRH needs are. More comprehensive and up to date dataon the distribution of health workers, both in terms of numbers and skills, across thedifferent sectors and geographical regions of the country will be available through thestrengthened HR information systems.
A better understanding of the skills mix required at the different levels of the health systemwill ensure that the staff available are posted to facilities where their skills are needed andthey can be fully utilised. For MDGPs will be posted to CEOC districts and facilities to enabletrained Advanced Skilled Birth Attendants and Skilled Birth Attendants practice and use theirskills. More reliable information will also be available to ensure that scholarships doctors aremore equitably distributed.
The remote area policies and systems that are in place in the health sector will be reviewedand deployment processes mapped out to get a better understanding of what shouldhappen, what does happen in practice and what is the effect on staff distribution.
Criteria for placement and transfer will be developed and utilised, and the predictability ofrotations established to ensure transparent implementation. Training institutions willencourage applications from students from remote areas and marginalised groups; andestablishing quota systems may help with this.
Review regulation and enforcement of remote area policies and systems and identifybarriers
Collect, analyse and update distribution data of sanctioned and filled postsdisaggregated by location, cadre, gender, caste, and ethnicity (Year 1)
Introduce corrective action to address barriers and strengthen policies and systems
125 World Health Organization (2010). Increasing access to health workers in remote and rural areas through improvedretention. Global policy recommendations

64
Strategy 2.2 Make Jobs/Postings In Rural And Remote Areas More Attractive ToRetain Health Workers
This strategy builds on Strategy 1.3, but with a particular focus on jobs in rural areas. TheMoHP has implemented and adopted a number of strategies to improve the distribution andretention of health workers. For example, the bonding of scholarship doctors and thewithholding of licenses until they have served out the bonding period have been effective inincreasing the number of junior doctors deployed and retained in the rural and remoteareas.
Various studies have been conducted to examine the reasons for shortages in rural andremote areas. These need to be better understood and this could include furtherexamination of the numbers and types of health workers being produced; the proportion ofthose produced that are entering the public health service and the length of time they stay;alternative employment opportunities; and migration trends. The reasons formaldistribution could also be better understood to determine the underlying cause of theproblem; is it due to a lack of information on where the vacancies and needs are; due toineffective transfer and deployment systems; or unwillingness of staff to go to where theyare posted. Further analysis will ensure that appropriate strategies are developed to addressthe problem.
Some studies have examined the impact of job satisfaction, motivation and incentives onretention. The findings of these studies and other international research126 in this areasuggest that implementing a bundle of contextually relevant interventions can help toimprove retention. 127
Piloting different bundles of interventions with different health worker cadres and teamswill help to determine the most effective bundle to use to attract and retain the staffrequired. Interventions could include career development and advancement opportunities,creating an enabling work working environment, recruitment of local people; provision ofadequate supplies and equipment, and other factors such as good leadership and HRmanagement, team work and clear job roles and plans.
The impact of interventions and bundles already in operation will be studied and theevidence and findings generated better utilised to inform new strategies andinterventions.128 More information may be needed on the incentive structure that influencesan individual's choice of job and location, e.g. studies and/or research on the �‘push�’ and�‘pull�’ factors that affect different categories of staff.
126 WHO (2010) Increasing access to health workers in remote and rural areas through improved retention. Global policyrecommendations127 See findings of the 2008 Nepal Safe Delivery Field Survey; the MoHP/NSI 2010 Mid term Assessment of the Rural StaffSupport Programme; the (2008) Health Sector Reform Support Programme Costing Study on Incentives Packages for Nepal�’sHealth Care Professionals; and various MoHP O&M Surveys.128 MoHP/Nick Simmons Institute (2010) Mid term Assessment of the Rural Staff Support Programme

65
Studies to determine migratory patterns and trends among the different health workercadres and the push and pull factors that influence external and internal migration will alsobe conducted. The findings will inform the design of interventions to reduce internalmigration and movement between the government, private, and NGO sectors and helpachieve a better public private mix. Female health workers face also constraints to workingin remote areas because of gender related issues (e.g. family responsibilities, etc.) and theseconstraints will be addressed through supportive interventions.
The availability of more comprehensive information, disaggregated by sex, cadre, age, casteand ethnicity through the HuRIS and other information systems, will enable employers todevelop more targeted and differentiated retention packages (monetary and non monetaryincentives) to make postings more attractive and help to retain staff in underserved areas.
Any future expansion and/or scale up of these initiatives must be well managed andcoordinated, to ensure that they do not distort distribution imbalances even further. Anyincentives and allowances to be provided will be linked to absence management and will beperformance based.
The functioning of the HFMCs will be strengthened so that they can support initiatives toimprove the working environment and to address some of the factors identified as being keyto retaining staff such as security.
Review, revise, implement and monitor career benefits related to rural posting andtransfers (linked to 1.1 and 1.3)
Identify push and pull factors, disaggregating these for women, people from differentsocial groups, income status and locations
Review existing retention schemes across the sector, including in the private and NGOsectors, and identify the most appropriate and effective schemes and incentives
Use findings of review to develop retention policy and schemes Conduct research on critical HRH areas focusing on remote areas and link to planning
processes Improve working environment in collaboration with HFMCs to attract and retain staff
Strategy 2.3 Prepare And Support Staff Better For Working And Living In RemoteAreas
Students in basic and pre service training will be exposed to more practical training inremote areas so that they are better prepared for working in these areas. All newemployees, contract staff and those being transferred to remote areas will receive adequateorientation before they are posted, including information on the location and facility theywill be posted to. This will build on and add to the information provided during their preservice training.
66
Safety and security for female staff are issues that will also be considered. In the moreremote facilities, new staff will be linked up with senior staff members who can support andmentor them. Local district health office and the HFMCs will also support health workersdeployed to their areas. Pre service training curricula will be reviewed and revised to includethis type of information to better prepare health workers for living and working in ruralareas.
Provide job and posting orientation after recruitment for different cadres Strengthen mechanisms to ensure that health workers posted to remote areas
receive regular supportive supervision and mentoring support
Strategy 2.4 Improve Workers�’ Living And Social Conditions In Remote Locations
Health workers are likely to be more willing to go and remain in remote areas that haveadequate living and social conditions. Studies conducted in Nepal indicate that factors suchas housing, schooling for dependents, transport, security, etc. are important to attract andretain health workers.
The NSI Rural Staff Support Programme is focusing on many of these issues with varyingdegrees of success. Recent programme assessments indicate that improvingcommunications and providing opportunities for health workers in rural areas to networkwith each other have been very effective in retaining MDGPs. The findings also suggest thatworking closely with the local government and the community has addressed many of thesecurity issues. It will also be important that infrastructural development and constructionand renovation plans for health facilities include improvements for staff housing.
Some of the factors required to improve living and working conditions in remote areas arenot within the control or remit of the MoHP, e.g. schooling and security, and will requireliaison with other government agencies at central and local levels. Further federalisation anddecentralisation may lead to improved transport and schooling, and districts may havegreater control over the allocation of resources to address some of these issues.
Review policy and practice related to the following areas:o Improved securityo Access to schoolso Improved housingo Communications (including internet)o Transporto Subsidised health services
Strengthen functioning of health facility/hospital management committees (e.g.local level resource mobilisation for improving living and social conditions for healthworkers)

67
Strategy 2.5 Compulsory Service To Improve Rural Service Provision
As proposed in Strategy 2.3 above, staff will need to be better prepared and supported forworking and living in remote areas. There are increasing numbers of young doctors workingout their scholarship bonds in rural and remote government facilities. The effectivedeployment and utilisation of these doctors will be critical for their performance andretention within the public health sector. The MoHP will work in collaboration with the MoEto strengthen mechanisms that will adequately support and mentor these scholarshipdoctors. New graduates and junior staff posted to remote areas will also be linked up withsenior and more experienced health workers.
The scholarship doctors will also have job descriptions that clearly outline theirresponsibilities. Communications and opportunities for networking with other junior doctorswill be improved. Strategies such as posting newly recruited doctors to larger facilities in lessremote areas for a short period of time before they begin their rural posting will beexplored. This would allow them to gain more practical experience and work under thementorship and supervision of more experienced staff.
When policies and procedures are in place for compulsory service, the MoHP, incollaboration with the professional councils will ensure compliance through withholdingregistration and/or further postgraduate training opportunities until the agreed period hasbeen served.
Review compulsory service experiences and assess impact on deployment and retentionof junior doctors (e.g. scholarship and new entrants), specialists and other senior staff inperipheral health facilities
Use findings of review to develop and pilot the introduction of incentive packages (e.g.career development, post graduate training, etc.) to attract, motivate and retainscholarship doctors.
Strategy 2.6 Continue And Identify New Areas For Task Shifting And AlternativeStaffing In Clinical Areas (E.G. Anaesthesia, Ultrasound Etc.)
Decisions for task shifting should be based on the following:
an analysis of key shortages
what can feasibly and safely be done by cadres to whom it is proposed that tasks beshifted
whether the decision is a short term or long term solution to the shortage

68
The analysis and review to be undertaken will also examine cases where specialist staff havebeen posted to generalist positions and are not fully utilising their skills.
Review and conduct analysis of key shortages and scarce skills (Year 1 and ongoing) Conduct workload and job analysis for all health professional jobs/posts
Strategy 2.7 Use NGOs And Private Health Providers For Service Delivery In MostDifficult Areas
The feasibility of this strategy needs to be further explored in the context of PPP, and willrequire consultations with the NGO and private health sectors. There has some progress todate with PPP, and this is an area that requires further analysis and refinement. Greaterparticipation and investment by the private sector in the public health sector will beencouraged. For example, private training institutions using government health facilities aspracticum sites for their students will be encouraged to ensure that posts are filled and toinvest in infrastructure and other areas.
Gaps in service delivery in difficult areas will be identified, services that NGOs and privateproviders could provide identified, and the most appropriate type of partnership agreed andformalised.
More information will be obtained on the strategies used by the NGO and private sectors toattract and retain staff in difficult areas. The HFOMCs, local health training institutions andother organisations such as women�’s groups, representative organisations and youth clubswill also be better utilised to provide services.
Prepare modalities for PPPs and expand PPPs for the management of district hospitals Ensure Community Service Organisations (CSO) and HFOMCs participation in social
auditing process
Output 3: Improved Performance Of Health Workers
Strategy 3.1 Provide Staff With Leadership And Clear Direction
The MoHP has also identified that the leadership and management capacity of hospitalsmanagers and management teams needs to be improved and strengthened. The EDPs areplanning to use performance based contracts with selected hospitals, and the management

69
of these contracts and the achievement of the agreed performance standards and targetswill require a certain level of management expertise.
The preliminary findings of the 2011 study 129 to assess the management and leadershiptraining needs of hospital managers, recommends the creation of a cadre of managers, toimprove the management of hospitals and the delivery of services.
While the attrition and retention of staff is often the key focus of plans and interventions,the MoHP will ensure that equal attention is given to managing the performance of theavailable staff. Facility managers and those responsible for the management of HRH will beequipped with the skills and tools to do this effectively. The MoHP will introduceperformance based and retention based payment systems. Incentive packages for healthworkers will be developed and piloted, and operations research will be used to observe theimpact on performance. Findings will inform the scale up of these schemes to othergeographical areas.
An assessment of how work plans are used at institutional and facility levels will help todetermine the extent to which they are guiding the work of individuals and teams. Thefindings of the review will be used to establish procedures and mechanisms to support thedevelopment of work plans linked to performance management and appraisal systems.Managers and staff will be supported and trained on how to develop, implement, monitorand evaluate work plans. Work plans will be reviewed on a regular basis and mechanismsput in place to facilitate stakeholder meetings at all levels (HFMC, VDC, Municipality, District,Region and National) to review performance.
Recent experiences of developing and/or updating job descriptions e.g. for MDGPs, SBAs,etc. will also be reviewed. The results of the review will be used to revise, update or developjob descriptions for key posts at the different levels. Performance based indicators forindividuals and health facility will be developed and introduced and these will be linked toincentives where there is critical shortage of staff, and to career development and capacityimprovement.
The review and development of job descriptions, job plans and performance basedindicators will enhance the functioning of the performance management system. An openappraisal system will be implemented to support measure and monitor staff performanceand development. The functioning and impact of the system on performance andproductivity will be regularly reviewed and evaluated.
Greater involvement of HFMCs in performance management processes will be encouragedand facilitated. They will also play a role reducing absenteeism, generating extra resourcesfor facilities and staff, and enhancing the quality of services provided by improving relationsbetween providers and the community.
129 NSI (2011). Hospital Management Training. A Summary Report

70
Design and develop an in service leadership and management programme and pilot inYear 1 in selected health facilities
Annual work plans for institution and individuals developed, implemented andmonitored
Review/develop job descriptions for staff at all levels in collaboration with facilitymanagers.
Update/develop and introduce performance appraisal/management system forindividuals and health facilities in line with service delivery programmes (link withperformance based incentives where there is critical shortage of HRH)
Strengthen the implementation of performance appraisal/management systems tomake them more objective
Strategy 3.2 Strengthen Skills/Capacity Of Health Workers To Do Their Jobs
An assessment of the overall training and CPD capacity in the health sector was undertakenin August 2011.130 It identifies a number of good practices and approaches already in placethat could be scaled up. It recommends that the capacity of regulatory bodies be improvedand more systematic approaches to the regulation, management and provision of in servicetraining and CPD be adopted. It also proposes that CPD and/or skills testing be made arequirement for registration with the professional councils
The NHSP 2 indicates that there will be a substantial number of health workers trainedthroughout the plan period. The MoHP plans to upgrade and update the skills of providersto enhance the quality of care. Over 1,000 MCHWs will be upgraded to ANMs, and there areover 1,200 vacant positions for VHWs that will be upgraded to AHWs. Skills of care providersand support staff at health and sub health posts, PHCCs and district hospitals will beupdated through in service refreshing training, coaching and onsite support.131
The MoHP and NHTC have been working to improve in service training and ensure thathealth workers have the skills and capacity to do their jobs well. Reviews have already beenconducted for maternal health and safe motherhood services, and training courses havebeen strengthened to address the gaps identified. Initial findings from the ongoing (2012)study on human resources for maternal health, focusing on midwifery, identified the needfor an evaluation to review the national SBA policy and programme. The results of theevaluation will guide the revision of the National In service Training Strategy (2006 2012),enhance the impact of the SBA workforce and lead to improved maternal and newbornhealth services in Nepal. The Family Health Division (FHD) of the DoHS, in collaboration with
130 Ministry of Health and Population (2011) Training Capacity Assessment and Strategy Development. Elliot, L., LATH131 Ministry of Health and Population Government of Nepal (2010) Nepal Health Sector Programme Implementation Plan II(NHSP IP 2) 2010 �– 2015 Final Draft 18 March 2010 p. 83

71
NHTC and UNFPA will undertake this evaluation in 2012, (as documented in the recentReproductive Health Review organized by FHD)
Training needs assessments have led to the creation and adoption of new training courses(e.g. Mid Level Practicum, AA, SBA and Biomedical Technician training) for critical healthworkers, such as mid level workers and SBAs, and the introduction of a distance CME coursefor doctors to address the skills gaps identified. 132 Other essential health workers will beidentified and further training needs assessment conducted to determine how gaps can beaddressed.
A more strategic long term perspective on human resource development in the healthsector will be adopted to ensure that health workers at all levels have the necessarytechnical, clinical, management and supervisory skills and knowledge to deliver qualityservices. The introduction of the post basic Bachelor Midwifery Programme, describedabove in Strategy 1.4, is an example of the MoHPs efforts to strengthen service providerskills and standards. The development of the Health Workforce Plan (as described inStrategy 1.1) will help to identify the types of health workers and level of skills that will berequired, which will in turn inform the design and content of training programmes andcurricula.
As described in Strategy 1.4, pre service training will be strengthened to ensure that healthworkers have a strong knowledge base to begin with and that basic training supports goodperformance. Providers of in service training and CPD, including NHTC, will be assessed andstrengthened to ensure that the training they provide produces appropriately skilled andknowledgeable health workers. A priority activity will be the assessment of the NHTCcapacity and the development of a revised Strategic Plan for the institution.
Training curricula will be reviewed and revised based on systematic reviews of the desiredskills set for different cadres. Revisions will also be in line with GESI principles so that healthworkers can recognise and respond to issues of women, the poor and the excluded.Regulation and contracting mechanisms and guidelines will be strengthened. Training siteswill be assessed and monitored and additional sites created to ensure that all health workershave equal access to professional development and skills enhancement opportunities. Thenumber and quality of teaching staff and teaching approaches and methodology will also bereviewed and strengthened. These initiatives will be linked to and support the interventionsproposed in Strategy 3.1 above.
As much as possible IST and CPD initiatives will utilise approaches such as on the jobtraining, mentoring, coaching and distance learning to ensure that training does not lead toincreased absenteeism and disruption of services. Distance learning approaches and optionswill be considered for staff development, to avoid taking essential health workers away fromalready understaffed facilities.
132 NSI (2011) Five Years of Progress 2006 2011

72
Review, assess and strengthen institutional pre service and in service training capacityto provide education, training and CPD that supports service delivery and qualityperformance (Year 1 and ongoing)
Provide relevant in service training courses and CPD to upgrade and update skills ofproviders and enhance the quality of care (especially of specialist, doctor and seniornursing cadres)
Review the working/opening hours for public health facilities at district level and below Strengthen contracting and accreditation mechanisms and capacity of Professional
Councils to enforce and monitor compliance Establish mechanisms and develop criteria and tools to measure, monitor and evaluate
training outcomes, training quality and impact and transfer of learning and skills to joband performance
Conduct an evaluation and review of the national SBA policy and programme and revisethe National In service Training Strategy (2006 2012) accordingly
Strategy 3.3 Ensure Effective Reward And Sanction Systems In Place
The implementation of this strategy will involve a policy and systems review and is inked toactivities outlined in Strategy 3.1. The performance appraisal form (Ka SA MU form) will bereviewed and updated. A transparent and open performance evaluation system, alignedwith public sector developments and reforms, will be established and appraisals conductedon an ongoing and regular basis (e.g. every 6 or 12 months). Health workers will be involvedin the design of reward and sanction systems; unless these systems are perceived as beingfair, they will not have the desired motivational effect on behaviour. Performance criteriawill also be GESI sensitive. Performance based incentives are being used in other ministriesand could be adapted and tailored for the health sector
Link rewards and sanctions, especially promotion within grades, to performance Mechanisms in place for health workers to provide feedback on the perceived fairness
of reward and punishment systems. Pilot performance based incentive system and evaluate impact Ensure Regional Directorates are providing supportive supervision and monitoring the
health workforce at all levels in their regions.
Strategy 3.4 Reduce Staff Absence From Assigned Posts
A review will be conducted of the systems currently in place to manage absence. Aqualitative study involving staff and managers will provide more understanding of how thecurrent system is working. A monitoring system for both transfers and deputation will also
73
be developed and this may help to reduce political influences on transfers. Strengtheningthe planning and coordination of training will help to reduce absence as a result of training.
Improve planning and management of transfers and deputations (kaaj) Strengthen absence management mechanisms Implement alternative arrangements for staff that are on leave or on deputation for
long periods.
Strategy 3.5 Ensure Staff At All Levels Have An Enabling Work Environment
Staff are more likely to perform well when there is an enabling work environment, includinghaving the necessary equipment and tools (e.g. medical diagnostic and InformationTechnology (IT) equipment, infrastructure, furnishings, etc.) to do their jobs. If this increasesjob satisfaction, an added benefit might be improved retention (linked to activities inStrategy on retention)
Identify which factors in the work environment affect staff performance most Liaise with relevant departments and agencies (e.g. logistics and supplies departments)
to provide an enabling environment
Strategy 3.6 Strengthen Teamwork Approaches
Effective teamwork improves the quality and coverage of health services and is an effectivemechanism where there is understaffing and a high workload. A review of current teamworkpractices will be conducted, including an examination of the impact of transfers onteamwork. Producing case studies of good and effective teamwork practices would be auseful first step in addressing this issue. Teamwork will also ensure that there is anappropriate skills mix to deliver a specific package of services in the facilities e.g. CEOC sitesand Birthing Centres
Review successful teamwork practices and document Disseminate good practice case studies to facility managers and support scale up
Output 4 Effective And Coordinated HR Management And Development Across The HealthSector
Strategy 4.1 Appropriate HR Policies In Place

74
Some of the current HR and related policies might no longer be relevant or appropriate forthe management of the current health workforce. They will be reviewed to determine whichare still valid and/or which are not being effectively implemented. The international andnational policy and regulatory environment will be scanned regularly and HR policies andsystems reviewed and modified accordingly. Various amendments have been made to theHealth Service Act and the National Health Policy is currently being revised and updated. HRpolicies will be aligned with other policy frameworks, e.g. Health Service Act, NationalHealth Policy, GESI strategy and other new and evolving international and national healthpolicies, legislation and regulations.
The ability of HR decision makers and managers to implement and resource the strategies inthe Plan and to achieve the agreed outputs will require a supportive policy and regulatoryenvironment. Implementation plans will be aligned with and supported by national andhealth policy frameworks, e.g. the authority to increase recruitment, improve distribution,increase production will need to be resourced, mandated and sanctioned.
Review existing national, health and HR policies, identify gaps and revise or develop newpolicies as necessary
Identify and promote organisational culture needed to support implementation ofrevised policies and systems through leadership of senior management
Introduce licensing examinations for all health professionals. Create mechanisms for re licensing
Strategy 4.2 Appropriate Organisational Structures, Systems And CapacityDeveloped To Support The HR Functions
A rapid assessment of HR related departments found that there was a fragmented structureand a lack of capacity to effectively perform the functions, including the management of HRinformation.133 Organisational structures at all levels will be strengthened and will haveappropriately skilled staff with the tools necessary to coordinate, manage and perform HRfunctions. The structure and capacity of the professional councils will be also bestrengthened to conduct licensing and accreditation and maintain and monitor professionalstandards. These structures and competencies will be critical as health care services are
133 Nepal Health Sector Support Programme (2010). Draft Capacity Assessment for Health System Strengthening. Anassessment of capacity building for health systems strengthening and the delivery of the NHSP 2 results framework. Martineau,T (LATH) and Subedi H. N.

75
decentralised and authority for HR recruitment, deployment and other managementdecisions further devolved to district levels and below.
HR systems, processes and practices for recruitment and deployment, promotion, managingstaff absence, contracting and transfers and other HR functions will be reviewed. The gapsidentified through these reviews will provide the entry points for support interventions. GESIresponsibilities of HR staff also need to be identified, and capacity and skills developed toensure that GESI principles are observed and adopted. Strategies and activities to supportthe strengthening of the HuRIS for workforce planning are included under Strategy 1.1above.
A standard HR framework will be adapted to review the HR functions, including the HuRIS.Previous capacity assessment exercises conducted in the MoHP and their findings will bereviewed and built on. As the form of federalisation becomes known, the organisationalstructures performing the HR functions and the capacity of HR and management staff atcentral and sub national levels will need to be reviewed and modified and/or strengthened.
Review existing structures, systems and capacity at all levels in the MoHP and across thehealth sector, using HR functions framework to identify gaps and overlaps, includingfrom a GESI perspective
Develop proposals and plans for strengthening structures, systems and capacity Strengthen leadership capacity and governance structures and promote greater
engagement and involvement of policy makers and senior management in HR planning,management and development (linked to various capacity strengthening initiativesincluded in Outputs 1 3)
Prepare for restructuring required as part of federalisation
Strategy 4.3 Effective Coordination Mechanisms In Place At All Levels Within TheHealth System
HR functions are the responsibility of a diverse set of stakeholders and actors withsometimes opposing interests and this often makes it difficult to achieve an agreed andcoordinated approach. There is a multiplicity of government and private sector agencies,institutions and stakeholders involved, which results in fragmentation and weakcoordination and inefficient HR practices that reduces the sector�’s ability to maintain astrategic perspective.
However there have been some achievements made towards improving coordinationthroughout the development of this HRH Strategic Plan, evidenced through increasing MoHPownership and commitment, the establishment and effective functioning of the CCF (thehigh level multi stakeholder committee established in November 2010 to oversee thedevelopment of the HRH Strategic Plan) and the high levels of stakeholder participation and

76
interest. These achievements will be safeguarded and maintained to support theimplementation of the Plan.
The CCF will become a more formal structure, aligned with existing coordination structuresand mechanisms within the MoHP. It will be composed of representatives from the keystakeholder groups and will promote partnership, communication, collaboration, andcoordination between all the actors and agencies (including the private and NGO sectors,MoHP departments and programmes, other government agencies, donors, consumers, etc.)and strengthen formal and informal linkages across the sector, at both strategic andtechnical levels.
The CCF will continue to play a coordinating role and oversee the implementation,monitoring, evaluation and revision/updating of the Plan. It will support the development ofannual HRH implementation plans at all levels and their incorporation into the MoHP�’sAWPB process. It will also support the mobilisation and allocation of adequate funding fromgovernment, donors, and other agencies to successfully implement the Plan.
Various multisectoral technical working groups and committees that have an HRH focusalready exist within the MoHP/DoHS, e.g. the TWG established under the FHD to focus onHRH for maternal health. The outputs of such groups and committees will be monitored toensure that proposed initiatives are aligned with the aims and outputs of the Plan. Other subcommittees and/or technical working groups may be established to coordinate and/ormonitor specific HRH strategies and interventions, such as workforce planning, training,HRIS, HRM (e.g. recruitment, distribution, retention, and performance management),monitoring and evaluation, etc.
Obtain more clarity on underlying causes of fragmentation and weak coordination Formalise and strengthen the CCF to function as a high level HRH Coordinating
Committee at national level (Year 1 and ongoing) Mechanisms reviewed and in place between MoHP and other health stakeholders
providers to supplement the delivery of health service
77
Section 5 Implementation of the Plan
INTRODUCTION
It will be extremely challenging to address all of the HRH issues and challenges highlighted inthis Plan. The effort needs to be well coordinated and carried out by people withappropriate skills and experience. Strengthening HRM systems and capacity in the MoHPand other organisations and agencies responsible for HR functions will be particularlyimportant for the effective management of the current workforce and to ensureinvestments in scaling up the numbers of staff achieve the desired outcomes.
The MoHP will ensure that there are robust human resource policies, capacity, structures,and systems to manage and develop human resources and to enhance productivity acrossthe health sector. The MoHP is also fully committed to ensuring that other measures such asimplementation arrangements and mechanisms, risk management, monitoring andevaluation, and budgeting and resource mobilisation strategies are in place to give the Planthe best chance of success.
The implementation of the Plan will be coordinated, supported and regularly monitored,reviewed and evaluated in order to assess progress, modify and adjust strategies andactivities, and develop subsequent plans and interventions. Finally, the 4 Year HRH StrategicPlan, Annual Implementation Plans and the proposed Health Workforce Plan will be costedand resources mobilised. These are discussed in greater detail below.
RISKS AND ASSUMPTIONS
HRH cannot be considered in isolation from the socioeconomic, political, legal, and healthcontext, and there are factors in the external environment that may adversely affect theHRH situation and the overall performance of the health sector during the plan period.
The following are some of the assumptions for the successful accomplishment of this plan:
Partners and collaborators are willing to fund and support the HRH Strategic Plan. MoHP and senior management in other government departments are willing to
participate in the development, approval and review of policies, systems andpractices to facilitate the implementation of the HRH Strategic Plan.
Health sector partners responses and actions to address HRH issues are coordinatedand strategic.
Private sector involvement leads to improved coverage and access to healthservices.
MoHP staff and senior management from other key government Ministries supportthe implementation and monitoring and evaluation of the Plan. This support willtranslate into required resource allocation.

78
However well designed the strategies might be, there are factors beyond the control of theMoHP and other stakeholders, which may hinder the achievement of the Plan�’s aims andoutputs. As part of coordinating and managing the implementation of the Plan, the MoHPwill monitor and manage the risks to mitigate their impact and regularly check whetherassumptions remain true.
If the assumptions are found not to hold true, some redesign of the strategies may berequired. Table 25 below provides a sample table that will be populated in Year 1 as part ofthe planning and development process for this HRH Strategic Plan. In it the risks are restatedas assumptions, which supports the link between the strategies and their respectiveoutputs.
Table 25 Example of assumptions associated with the strategies
Output/Strategy Assumptions/Risks StrategyAppropriatesupply of healthworkers for labourmarket needs
All key stakeholders are andcontinue to be included in theplanning processRegular review meetings,monitoring and evaluation informdecisions and action takenHR information systems arestrengthened and enhance flows ofdata between the centre and theregions/districts
Improve HR Planning for HealthSectorImprove MoHP recruitment anddeployment processes, andensure they are effective andtimelyImprove attractiveness of jobsfor increased recruitment andretention
IMPLEMENTATION ARRANGEMENTS
There is a common danger that the plan remains simply that �– a Plan. It is thereforeimportant that the strategies and activities are reviewed and revised on a regular basis toensure the greatest chance of implementation. Strategies and long term plans must be setout with clear priorities. Stakeholders who participated in the January 2012 CCF meetingsuggested that the strategic plan and annual Implementation Plans should be linked to theNHSP 2 Three Year Implementation Plan and HRH related budgets and costs be included inthe Medium Term Expenditure Framework (MTEF). They also recommended that acommunication strategy should be developed to support the effective implementation ofthe Plan.
The implementation of the Strategic Plan will take place at various levels of the health caredelivery system. The participation of officers and managers at regional, district and facilitylevels and staff from the training institutions in the implementation will also be critical.
Political commitment will be a critical factor in the effective implementation of the Plan.Stakeholders also recommended that the CCF be formalised and become the steering bodyto oversee the implementation of the Plan. The MoHP and CCF will provide strategicguidance to interpret the strategies and activities into annual costed action plans that will beincluded in the AWPB; they ensure that implementation and progress is reviewed and

79
emerging HRH issues and challenges highlighted and discussed during the Joint AnnualReview (JAR), and that JAR recommendations are implemented in subsequent years.
Annual Implementation plans
The MoHP, the CCF and other stakeholders will translate and prioritise the strategies andactivities contained in the HRH Strategic Plan into more detailed annual implementationplans. The activities and indicative sub activities for each of the strategies are presented inAnnex 2. These have been costed and a draft budget (excluding the wage bill for the currentand future health workforce) for the implementation of the Plan over the 4 years has beendeveloped. The MoHP will further refine priority activities and these will be captured in the2012 AWPB.
MONITORING AND EVALUATION OF THE PLAN
The implementation of the Plan will be monitored, reviewed and evaluated on an annualbasis as part of the Joint Annual Review process. This will provide opportunities forreflecting on the purpose, strategies, and outputs of the Plan and for reviewing the qualityof the outcomes. Strategies and activities will be modified and adjusted and new plansdeveloped.
The implementation and monitoring of the strategies in the Plan will require furtherinformation gathering and analysis, particularly for the proposed Health Workforce Plan (seeStrategy 1.1) to be developed in Year 1. This will need to be supported by relevant andreliable HRH information systems. Basic and post basic training plans will also be linked tothese projections.
A Monitoring and Evaluation Plan and HR indicators aligned with NHSP 2 indicators will bedeveloped. Monitoring the implementation of the HRH Strategic Plan will be done at threelevels: the national, regional and district levels. At the national level, the CCF will coordinatethe development of Annual Implementation Plans and oversee the monitoring of theimplementation of the Plan. The approved HRH Strategic Plan and the AnnualImplementation Plans will be disseminated widely and posted on the MoHP website.
M&E data will be collected and analysed regularly and used to prepare quarterly and annualreports on HRH. These reports will be disseminated to senior management and M&Einformation shared with policy makers and managers. At the regional and district levels themonitoring of the Implementation Plan will be integrated into the existing routine healthplanning and monitoring systems.
COSTING AND FINANCING THE HRH STRATEGIC PLAN AND HEALTH WORKFORCE PLAN
The HRH Strategic Plan includes a budget that provides a breakdown of the costs forimplementing each of the HRH strategies (See Annex 4), excluding salaries and allowances.The Health Workforce Plan will include a budget for maintaining the existing workforce and

80
the cost of increasing the numbers of staff produced, recruited and upgraded over the 4years of the Plan and the longer term.
Financing to train and employ the additional staff required will need to be mobilised. Thereare a number of human resource programmes already supported by external developmentpartners. A strategy for marketing the plan and attracting additional funds will bedeveloped. The fact that there is a comprehensive and integrated strategy for humanresources will make this area more attractive to funders.

81
ANNEX 1 TECHNICAL WORKING GROUPS (TWG) MEMBERSHIP
TWG I: Shortage of HRH Staff Imbalance between supply and demand and proposedmember of technical working group are:
Mr. Krishna Karki Under Secretary, MoHP (Member Secretary) Mrs. Ishwori Devi Shrestha, Nursing In charge, MoHP Dr. Mukanda Panthi �– registrar Dr. T.P. Thapa �– Kist Medical College (private sector) Dhan Prasad Paudel, Ragistar �– public Health council Mr. Parsuram Shrestha �– Sr. Public Health MoE Representative (Higher & technical Education) Dr. Maureen Dariang NHSSP
Note: Mr. Karki has been serving as the care taker Member Secretary due to the transfer ofMr. Prem Raj Giri who was named as the Member Secretary at the beginning.
TWG II: Mal distribution of staff especially in remote and rural areas and proposedmember of technical working group are:
Mr Krishna Karki , Under Secretary, MoHP (Member Secretary) Dr. Angel Magar Dr. Ganga Shakya NHSSP Dr. Mark Zimmerman, Nick Simons Institute Ms. Anita Lama �– Medical Council Representative from Ministry of General Administration
TWG III: Poor staff performance (productivity, quality, and availability) and proposedmember of technical working group are:
Mr. Kabi Raj Khanal Under Secretary, MoHP (Member Secretary) Ms. Pramila Dewan �– Nursing association Mr. BinodThapa CTEVT Dr. Senendra Upreti �– Director, Curative Division Mr. Hom Nath Subedi NHSSP Dr. Choplal Bhusal �– Nepal Research Council ,Bhwaniprasad Shrestha MoGA Representative from Merlin

82
TWG IV: Fragmented approach to human resource planning, management anddevelopment, and proposed member of technical working group are:
• Mr. Ram Chandra Khanal �– Sr. Public Health Administrator, MoHP (MemberSecretary)
• Dr B R Marasini �– Senior Health Administrator• Ms. Janaki K.C. �– Nursing association• Dr. Kedar Baral PAHC• Lila Paudel �– section officer• Tulsi Shrestha _ under secretary• Dr. Shyam Mani• Dr. Anjani Kumar Jha• Pan Bdr. Chettri• Dr R. K. Tuladhar (PHS)• Mr. Krishna Sharma, NHSSP
TWG V: HRH Financing and proposed member of technical working group are:
• Mr Shiva Simkhada Under Secretary (Account Section), MoHP (MemberSecretary)
• Suresh Tiwari NHSSP
• Devi Prasain NHSSP
• Representation from EDP
• Dr. Badri Raj Pandey
• Mr. Mohan Thapa �– Account Officer
• Dr. Devendra Gyewali
• Nirmal HariAdhikari (MoF)

83
ANNEX 2 STRATEGIES, ACTIVITIES AND SUB ACTIVITIES
Outputs:
1. Appropriate supply of health workers for labour market needs2. Equitable distribution of health workers3. Improved health worker performance4. Effective and coordinated HR planning, management and development across thehealth sector
Activities Sub activities
Output 1: Appropriate supply of health workers for labour market needs
Strategy 1.1 Improve HR Planning for Health Sector
Strengthen leadership and capacity in HR planningincluding the HR division in MoHP, Department ofHealth Services, and staff at regional and district levels
Assess HR planning capacity and use findings todevelop a Capacity Improvement Plan
Implement capacity improvement plan e.g.coaching, mentoring, TA support, on/off the jobtraining, external training courses, etc.
Strengthen HR information systems and capacity withinthe MoHP to generate reliable and up to dateinformation on current HRH, firstly in the public sectorsand thereafter the private and NGO sectors for routineand strategic HR planning and management (Year 1)
Review and strengthen MoHP HR informationsystem (HuRIS) at all levels and update database(may include provision of IT equipment, software,capacity development interventions, etc.)
Agree recommendations of 2011 HRIS assessmentto be implemented
Coordinate efforts of other stakeholders (e.g. Savethe Children, WHO) to generate information onthe private and NGO sectors and provide a morecomprehensive profile of HRH across the sector
Assess training information management systems(TIMS)
Strengthen training information managementsystems (TIMS)
Network and link HuRIS to other informationsystems e.g. HMIS, PIS, professional councils,MoHP departments, District and regional facilitiesand offices, and private/NGO service providers

84
Improve availability and use of disaggregated HRH andtraining information (e.g. gender, caste, ethnicity, cadre,facility, geographical area) for HR planning andmanagement (Year 1 and ongoing)
Collect, analyse, and maintain disaggregated HRinformation for the whole health sector on aregular basis.
Orientation for policy makers anddepartment/programme heads and HR managersto access and use HRH information for advocacy,policy formulation and decision making
Collect and analyse information on service deliveryneeds across the health sector (Year 1)
Use service delivery data (HMIS) to support thedevelopment of a medium to long term HealthWorkforce Plan and to accurately determine HRHrequirements
Produce Health Workforce Plan (by June 2012) that willdetermine HRH requirements (numbers, skills, gender,etc.) and supply to meet service delivery needs acrossthe sector over the short, medium and long term (Year1)
Develop sector wide HR profile with disaggregateddata on sex, age, caste/ethnicity, regional identity,cadre/post, workplace, training, etc.
Identify MoHP and other employers' plans forservice change/expansion.
Conduct Labour Market study drawing on mostrecent census data
Conduct workload and job analysis for existing andnew health professional jobs/posts and defineoptimum staffing norms for service delivery needs
Review and explore other factors that willinfluence HRH requirements e.g. decentralisation,infrastructural development /expansion,provisions of the Health Services Act, specificservice needs to address barriers of women, poorand excluded, GESI, free health services, otherhealth/national policies and regulations, etc.
Establish drafting team and build capacity ofmembers to determine HRH requirements basedon analysis of needs and other factors anddevelop, monitor and update long term HealthWorkforce Plan.
Establish HRH requirements for the health sectorfor the short, medium and long term
Develop mechanisms to cost new HRHrequirements.

85
Identify finances potentially available (fiscal space)and mobilise any additional funds required.
Prepare budgets for expanded health workforcee.g. salaries with justification and evidence
Service needs to address barriers of women, poorand excluded to access health services identified
Facilitate stakeholder consultations to getagreement on Workforce Plan and HRHprojections and requirements
Develop capacity and establish and institutionaliseplanning mechanisms
Update and maintain database so that it cangenerate up to date and reliable disaggregateddata and reports
Provide mentoring and coaching support to HuRISstaff
HuRIS and TIMS used to update HRH profile on anannual basis and to adjust HRH requirements andprojections
Put HuRIS online and provide training to relevant filedstaffStrategy 1.2 Improve MoHP recruitment and deployment processes and ensure they are effective andtimelyAssess current recruitment and deployment processesand systems, identify problems and bottlenecks,including GESI related issues and use findings tostreamline and strengthen systems
Conduct assessment/systems audit of currentincluding checking that recruitment systems anddeployment processes accommodate need forgender equality and social inclusion
Use findings to develop systems strengtheninginterventions (may include equipment, capacitydevelopment interventions, advocacy, etc.)
Amend Health Service Act, if necessary tofacilitate provision of posts and the production,recruitment and promotion of public health sectorworkers
Use HuRIS generated information to identifysanctioned filled and vacant positions andnew/additional posts and recruit and deploy/poststaff accordingly
Make informed, transparent and timely requeststo the Public Service Commission to recruit to fillvacant positionsAdvertise and/or make information available on

86
vacancies and jobs through Public ServiceCommission (PSC) at least once a year.Ensure PSC recruitment criteria includes technical,human and conceptual GESI sensitive skills (linkedto job descriptions)Provide induction/ orientation/training linked tojob responsibilities for all categories.Promote team working and deploy teams toensure appropriate skills mix in facilities
Review and strengthen contracting systems andpractices (including expansion of multi year contracting)
Conduct study of contracting procedures andpractices (study to examine what type/age/sex/ ofhealth workers is on contract, location of post,duration of contract, administration/managementof contracts, etc)
Expand multi year contracting for essential andscarce cadres (Year 1 and ongoing)
Improve procedures for the management ofcontracted staff and administration of contracts(Year 1 and ongoing)
Review O&M studies and identify and advocate forpriority vacancies to be filled (informed by HealthWorkforce Plan and workforce projections to bedeveloped in Year 1)
Review recommendations and advocate forpriority vacancies/positions to be filled
Management and other health systems posts created toimprove the management of hospitals and other healthfacilities and overall health systems e.g. HR planning,management and development, health economics,procurement, logistics, etc.Use Health Workforce Plan to guide recruitment andposting of staff according to job requirements (Year 1and ongoing)
Use job descriptions, service deliveryrequirements and information on local context toguide advertising, selection, recruitment anddeployment of health workers
Review and update the existing assessmentsystems for selection and appointment of staff
Use distribution data to determine location ofvacant posts and skills mix required and useinformation to make deployment decisions
Determine number of trained unemployed healthworkers available for work and implement proceduresto attract, recruit and deploy (Year 1)
Conduct study (including review of training supplydata and employment figures) and disseminatefindings.
Target unemployed health workers throughspecial advertisements and provide freerefresher/reorientation training
Review and assess experience with localrecruitment/contracting to ensure systems and
Assess role and responsibility of HFOMCs andother groups (e.g. women�’s group, youth clubs

87
processes are transparent and equitable andappropriately skilled staff are being hired beforeexpanding its use
etc.) in local recruitment
Conduct review and use findings for scale up or fordesign of more appropriate strategies
Explore and practice alternative recruitment andemployment arrangements (e.g. multi year contracting,creation of a health Service Commission, etc.)
Conduct review and use findings to pilotoutsourcing of recruitment function forcontracting and management of specific cadres toprivate or NGO agencies
Review and document role and contribution of FCHVsfor potential expansion or use with other cadres
Conduct study to examine role and impact ofFCHVs
Strategy 1.3 Improve attractiveness of jobs for increased recruitment and retentionCollect and review information (disaggregated) on jobpreference and job seeking behaviour
Conduct study for health workers in public, privateand NGO sectors and use findings to inform thedesign of attraction and retention strategies
Review labour market information regularly (Year 1) Collect and analyse labour market data andupdate database, HuRIS and HRH profile
Develop/improve GESI sensitive policies to manageretention
Collect and analyse data to inform GESI policies tosupport attraction and retention strategies forthese groups
Strategy 1.4 Ensure pre service training is in line with requirements for the health sectorCollect data on projected production and assesspotential for increase/decrease of specific cadres (Year1)
Collect and analyse data on production frompublic, private and NGO training institutions andproviders
Establish and maintain TIMSStrengthen mechanisms for communication andcollaboration between MoHP and MoE and establishinter ministerial for a (to include MoHP, MoE, NPC,MoF, PSC, etc.) to coordinate and address trainingproduction and regulatory issuesWork with MoE to expand/reduce pre service training,informed by service delivery needs e.g. training ofMDGPs, Hospital Managers, assessment/establishmentof more rural based training sites/institutions, etc.
Develop National Health Pre service TrainingStrategy and annual implementation plans linkedto and informed by Health Workforce Plan Year 1
Improve accreditation and regulation of pre servicetraining institutions to ensure an adequate supply ofskilled and knowledgeable health workers and assurethe quality of the training provided
Map stakeholders (e.g. professional council andassociations) and determine their roles andresponsibilities for the accreditation, regulationand monitoring of health training institutions
Strengthen capacity of Professional Councils toregulate and monitor training institutions
Review and strengthen accreditation andregulation procedures and guidelines inconsultation with relevant bodies
Monitor enforcement of guidelines andregulations of pre service training
Strengthen mechanisms to follow up and support healthworkers after training and to evaluate the impact of the
Review current mechanisms

88
training on performance. Strengthen or develop post training follow up andimpact evaluation instruments/tools
Output 2 Equitable distribution of health workers
Strategy 2.1 Review current situation and experiences and ensure deployment systems result in equitabledistribution of health workers
Review regulation and enforcement of remote areapolicies and systems and identify barriers
Conduct policy and systems audit to identifybottlenecks
Collect, analyse and update distribution data ofsanctioned and filled posts disaggregated by location,cadre, gender, caste, and ethnicity (Year 1)
Identify underserved and remote populations andareas (e.g. caste, ethnicity, gender)
Collect and analyse data and update profile andHRH database and use to make deploymentdecisions
Deployment based on defined needs (population,geography, disease burden, etc.)
Monitor distribution trendsUse findings to strengthen systems Take corrective action to address barriers and
strengthen policies and systemsStrategy 2.2 Make jobs/postings in rural areas more attractiveReview, revise, implement and monitor career benefitsrelated to rural posting and transfer (linked to Strategies1.1 and 1.3)
Identify career benefits and use information forthe development of attraction, training andretention strategies
Identify push and pull factors, disaggregating these forwomen, people from different social groups, incomestatus and locations
Collect and analyse data on push and pull factors
Gender specific issues identified and addressedReview existing retention schemes across the sector,including in the private and NGO sectors and identifythe most appropriate and effective schemes andincentives
Conduct study and use findings to designretention strategies
Develop policies and procedures to attract andretain scarce staff e.g. career developmentopportunities for MDGPs posted to underservedand remote areas
Explore possibilities of staff rotation to fill gaps
Monitor impact on retentionUse findings of review to develop retention policy andschemes
Identify and provide targeted retentionmeasures for remote areas
Identify and provide retention measures forselected cadres/ posts
Research on critical HRH gaps focusing on remote areasand link to planning process
Conduct evaluation and use findings to determineappropriate package of allowances
Monitor impact on retentionImprove working environment to attract and retain staffin collaboration with HFMCs
Study to identify factors that improve workingenvironment

89
Use findings to improve working environment
Monitor impact on attraction and retentionStrategy 2.3 Prepare and support staff better for working and living in remote areasProvide job and posting orientation after recruitmentfor different cadres
Design orientation programmes to include trainingin relevant skills areas for specific cadres e.g. newentrants and scholarship doctors, health systemsmanagement training, clinical training in SBA, CAC,ER Management, etc. and to provide informationon workplace (link to Output 3 on performance)
Include information and training on working inrural areas in pre service training curriculum
Strengthen mechanisms to ensure that health workersposted to remote areas receive regular supportivesupervision and mentoring support
Review and strengthen support supervision andmentoring systems and practice in collaborationwith service delivery programmes (link toperformance management and in servicetraining/CPD)
Identify and provide gender specific supportStrategy 2.4 Improve workers living and social conditions in remote locationsReview policy and practice related to the followingareas:Improved securityAccess to schoolsImproved housingCommunications (including internet)TransportSubsidised health services
Review polices and advocate with relevantdepartments, agencies and local governancegroups to improve these areas
Strengthen functioning of health facility/hospitalmanagement committee (e.g. local level resourcemobilization) to support living and social conditions forhealth workers)
Identify roles and responsibilities and strengthenfunctioning (e.g. may include capacitydevelopment interventions, supplies, equipment,financial support to hold meetings, etc.)
Collaborate with local government, VDCs,community groups, etc. to initiate improvements
Strategy 2.5 Compulsory service to improve rural service provisionReview compulsory service experiences and assessimpact on deployment and retention of junior doctors(e.g. scholarship and new entrants) and specialists andother senior staff in peripheral health facilities
Conduct review and impact assessment
Use findings to inform attraction and retentionstudies (linked to Strategies 2.1 to 2.4)
Use findings to inform decisions about expandingthe scheme or adopting other approaches (Year 1and ongoing)
Use findings of the review to develop and pilot theintroduction of incentive packages (e.g. careerdevelopment, post graduate training, etc.) to attract,motivate and retain scholarship doctors

90
Strategy 2.6 Continue and identify new areas for task shifting and alternative staffing in clinical areas (e.g.anaesthesia, ultrasound etc.)Review and conduct analysis of key shortages andscarce skills (Year 1 and ongoing)
Review conducted and data analysed and findingsused to update HRH profile and inform andupdate health workforce planning
Conduct ongoing workload and job analysis for existingand new health professional jobs/posts
Data collected and analysed on an annual basisand used to update Health Workforce Plan and HRprojections
Review and update job descriptions/ToRs for newjobs and responsibilities
Pilot introduction of job descriptions for specificcadres/jobs
Strategy 2.7 Use NGOs and private health providers for service delivery in most difficult areasPrepare modalities for PPP and expand PPPs for themanagement of district hospitals
Conduct review of existing PPP initiatives
Use findings to expand and scale up
Identify additional providers to provide services inremote locations
Identify appropriate package of incentives toencourage private providers to provide services inunderserved and remote areas
MoHP develop and implement robust monitoringand supervision systems
Ensure CSO and HFMCs participation in social auditingprocess
Social audits conducted in collaboration with CSO& HFOMCs
Output 3: Improved performance of health workersStrategy 3.1 Provide staff with leadership and clear directionDesign and develop an in service leadership andmanagement programme and pilot in Year 1 in selectedhealth facilities
Design and develop materials for programme andpilot in district hospitals
Follow up, evaluate and scale upAnnual work plans for institutions/facilities andindividuals developed, implemented and monitored.
Assess resource (HR, infrastructure and skills)requirements to deliver mandated quality healthservices (including identifying existing strengthand gaps)
Provide training to facility managers to develop,resource implement, monitor and evaluate workplans and individual capacity development plans(linked to performance management andappraisal).
Develop career development pathways�–linked tocapacity development plans

91
Incorporate gender and inclusion aspects in theworkplan
Implement planned activities and monitorregularly
Review/develop job descriptions for staff at all levels incollaboration with facility managers.
Review existing job descriptions and identify gaps
Revise/update and /develop and endorse jobdescriptions.
Provide health workers with facility work planduring induction process and orient healthworkers on the job descriptions.
Update/develop performance appraisal/managementsystem in line with service delivery programmes andpublic sector systems (link with performance basedincentives where there is critical shortage of HRH)
Review existing public sector performancemanagement systems annually.
Adapt/develop tools and systems
Provide feedback to heath workers onperformance through supervision and appraisalsystems
Pilot the implementation of performanceappraisal/management systems.
Design Operations Research Study and identifyfacilities/staff to conduct study to monitor andevaluate impact of performance managementsystems
Conduct study and examine all aspects ofperformance management system includingdevelopment and use of job descriptions andworkplans, implementation of annual appraisals,capacity improvement plans, feedbackmechanisms, use of social audit/client satisfactionmeasurement tools, etc. and disseminate findings
Strategy 3.2 Strengthen skills/capacity of health workers to do their jobsReview, assess and strengthen institutional trainingcapacity to provide pre service and in service education,training and CPD that supports service delivery andquality performance (Year 1 and ongoing)
Develop tool for assessment of TrainingInstitutions (Year 1)Conduct capacity assessment of NHTC (Year 1) tocover the following areas:Infrastructure teaching facilities and staff andstudent accommodation;Staffing levels number and skills of

92
tutors/teaching staffTraining curricula and materialsNumber and quality of practicum sites,Instructional approaches (theory/practical,classroom/practicum sites, etc)Student population (including information onentry requirements, student selection, intakes,attrition, nationality/ethnicity of students,numbers and types of graduates produced,destination of graduates post training)Training information systemsHR systems and practices (recruitment, retentionand professional development of teaching staff),Financial resources
Stakeholder consultations to review findings andidentify short, medium and long terminterventions.
Revise and update the 2004 NHTC strategy anddevelop Capacity Improvement Plan (Year 1) anddevelop Training Implementation Plans on anannual basis
Map and assess capacity of other existing preservice and in service training institutions anddevelop Institutional Capacity Improvement Plans(to include training standards, protocols andguidelines) and Implementation Plans on anannual basis
Develop a National In Service Training (IST) & CPDStrategy and prepare in service training and CPDplans on an annual basis (Linked to National Preservice Training Strategy)
Review and strengthen contracting mechanismsfor training providers and institutions
Establish and maintain a training informationmanagement system (TIMS) to maintain andmonitor numbers, names of trainees, trainingprogramme undertaken, training provider, makingit mandatory for all staff to report training taken(e.g. information documented during performanceappraisal process) )

93
Provide relevant in service training courses and CPDsessions to upgrade and update skills of providers andenhance the quality of care
Identify critical cadres on an annual basis (basedon HRH profile and Workforce Plan included andcosted in Strategy 1.1) and conduct TrainingNeeds Assessment as per proposed NationalIST/CPD Strategy and Annual Implementation Plan
Design and deliver in service training programmesand CPD for selected cadres informed by findingsof TNA and National IST/CPD Strategy
Review training approaches and design andintroduce new and innovative approaches for thedelivery and content of on the job training andmentoring (e.g. distance and tele medicineprogrammes/work based learning)
Strengthen competencies and skills of healthworkers to respond to GESI related issues
Develop mechanisms and implementinduction/orientation/training for all healthworkers
Conduct TNA and provide in service training tolocally recruited health workers based on needand job responsibilities
Review the working/opening hours for public healthfacilities at district level and below
Strengthen contracting and accreditation mechanismsand capacity of Professional Councils to enforce andmonitor compliance
Review, revise/develop quality assurance,regulation and accreditation procedures andguidelines for training institutions and monitorcompliance
Strengthen capacity of professional councils(included in Strategy 1.4)
Improve current regulation mechanisms bymaking CPD a requirement for re registration
Establish mechanisms and develop criteria and tools tomeasure, monitor and evaluate training outcomes,training quality and impact and transfer of learning andskills to job and performance
Develop tools and mechanisms to conductmonitoring and evaluation of trainers and traininginstitutions
Promote continuous improvements in trainingapproaches
Evaluate and review the national SBA policy andprogramme and revise the National In service TrainingStrategy (2006 12) accordingly (Year 1)Strategy 3.3 Ensure effective reward and sanction systems in placeLink reward and sanctions, especially promotion within Review and update existing performance appraisal

94
grades, to performance form (Ka SA MU form) based on portfolio basedevaluation
Review/revise/develop promotion criteria that issensitive to gender and inclusion issues
Department heads and managers conduct annualperformance appraisals and appraisal informationis documented and used for promotion decisions
Sanction discriminatory behaviour towardswomen, poor and the excluded
Mechanisms in place for health workers to providefeedback on the perceived fairness of reward andpunishment systems.
Develop tools and mechanisms for health workersto provide feedback on reward and punishmentsystem
Establish a process of feedback from HFOMCregarding behaviour of health workers
Pilot performance based incentive system Identify and agree performance indicators andtargets/outcomes
Identify and select pilot facilities (e.g. 5 facilitiesper region per annum)
Determine and cost incentives to be provided
Monitor and evaluate impact on performanceEnsure Regional Directorates are providing supportivesupervision and monitoring the health workforce at alllevels in their regionsStrategy 3.4 Reduce staff absence from their assigned postsImprove planning and management of transfers anddeputations (kaaj)
Review current practice of staff transfers anddeputation and identify the gaps
Ensure managers enforce and comply with rulesand regulations for deputation and transfer
Establish policy provisions to improve planningand management of transfers and deputationsincluding the following provisions:�• targeted training and recruitment of healthworkers from remote rural districts�• compulsory service with provision ofappropriate support and incentives for selectedhealth workers (e.g. new graduates MBBS, Nurses,and paramedics and other key cadres) inunderserved and remote areas to avoid frequenttransfer and deputation�• attractive financial incentives (e.g. hardshipallowance, non practice allowance, housing

95
allowance, family transport support and annualleave) to reduce absence�• devolve authority to regional health offices torecruit, deploy and manage health workers�• priority given to health workers willing totransfer to post in home town and/or district andsame location postings for spouses�• Reward and sanction for violating HRmanagement rules and regulations on stafftransfer and deputation.
Identify gender specific constraints and adoptinnovative ways to address them so that womenemployees can work comfortably
Develop and implement monitoring systems toensure managers enforce and comply with rulesand regulations for deputation and transfer e.g.develop, maintain and implement a roster fortransfer of staff before/or at the time ofrecruitment.
Monitor and document impact of transfers onteam working (Year 1 and ongoing).
Strengthen absence management mechanisms Review current levels of staff absenteeism,identify gaps and develop and agree mechanismsto minimise.
Establish systems and procedures for themanagement of absence for meetings, workshops& training e.g. document staff movement andscheduling for meetings, workshops, etc.
Introduce distance and tele medicineprogrammes/work based learning for staffworking in underserved and remote areas
Implement mechanisms and procedures toimprove participation of political, social andunion/associations pressure/influence in HRM(especially in areas of transfer, deputation, studyleave, etc.)
Implement alternative arrangements for staff that areon leave or deputation for long periods
Strategy 3.5 Ensure staff at all levels have an enabling work environmentIdentify which factors in the work environment affectstaff performance most
Identify factors through consultations with healthworkers, facility managers and other stakeholders
Liaison with relevant departments and agencies (e.g.logistics and supplies departments) to provide an
Conduct political and social mobilisation to createenabling environment (e.g. social security, better

96
enabling environment accommodation, incentives for family and careeropportunities and/or posting in accessible facility)at the health facility to reduce absence andmaximise retention of health workers
Strategy 3.6 Strengthen team working approachesReview successful team working practices anddocument
Conduct review in selected facilities
Disseminate good practice case studies to facilitymanagers and support scale up
Produce case study and disseminate
Output 4 Effective and coordinated HR management and development across the health sectorStrategy 4.1 Appropriate HR policies in placeReview existing national, health and HR policies, identifygaps and revise or develop new policies as necessary
Map and synthesize key policies
Review policies on recruitment, transfer,promotion, leave, and working environment,considering the following: GESI related issues,maternity leave, paternity leave, child care, breastfeeding, flexible working, etc.
Amend/revise policies as required ensuring GESIaspects are considered and gender specificresponsibilities of women recognised
Identify and promote organisational culture needed tosupport implementation of revised policies and systemsthrough leadership of senior management
Assess organisational culture strengths and gaps
Identify issues experienced by women staff andstaff of excluded communities
Conduct sessions/dialogue to discuss workingenvironment aspects within teams
Establish process for regular discussions for apositive working environment
Introduce licensing examinations for all healthprofessionalsCreate mechanisms for re licensingStrategy 4.2 Appropriate organisational structures, systems and capacity developed to support the HRfunctionsReview existing structures, systems and capacity at alllevels in the MoHP and across the health sector, using HRfunctions framework to identify gaps and overlaps,including from a GESI perspective
Review impact of existing organisationalstructures and staffing on HR functions andidentify the gaps
Conduct a GESI audit of the organisationalstructures, systems and staff
Carry out audit of selected systems and processesin central MoHP (linked to Outputs 1, 2 and 3)
Conduct capacity assessment of HR staff incentral MOHP to carry out HR functions

97
Explore the option of establishing a HRHManagement Division at MoHP that willincorporate all existing HR related functions inthe MoHP
Develop proposals and plans for strengtheningstructures, systems and capacity
Use findings to determine key HR functions andappropriate structures/staffing
Review staffing needs of new/revised structuresand recruit new staff if necessary, with dueconsideration given to sex, caste/ethnicity anddiversity
Develop capacity improvement plan andinterventions e.g. coaching, mentoring, on/offthe job training programmes for existing staff
Identify HR systems strengthening initiatives e.g.information systems (Linked to Strategies inOutput 1)
Identify tools required for staff to perform HRfunctions
Strengthen leadership and governance structures andpromote greater engagement and involvement of policymakers and senior management in HR planning,management and development (linked to variouscapacity strengthening initiatives included in Outputs 13)
Map and assess capacity and role of governancestructures in HRH
Strengthen the leadership capacity of policymakers and senior managers in the MoHP andhealth facilities
Strengthen HR systems and processes are ensurethat are transparent and efficient
Prepare for restructuring required as part offederalisation
Review and assess devolution/decentralisation ofauthority to regions, districts and health facilitycommittees and boards for HR planning,management and development
Use findings to develop Capacity ImprovementPlans for all levels
Strategy 4.3 Effective coordination mechanisms in place at all levels within the health systemObtain more clarity on underlying causes offragmentation and weak coordination
Map and consult HRH stakeholders to assesscauses of fragmentation and coordination
Formalise and strengthen the CCF to function as a highlevel HRH Coordinating Committee at national level (Year1)
Support and facilitate regular /monthly meetingsof CCF
Review and revise ToR for CCF
Review composition for CCF
Orient CCF on GESI issues
98
Identify specific responsibilities of CCF on GESI
CCF establishes sub committees at central,regional and lower levels for implementation andmonitoring of HRH Strategic Plan (Year 1)
Mechanisms reviewed and in place between MoHP andother health providers to supplement the delivery ofhealth services
Mechanisms agreed and in place for thecoordination of stakeholders HRH inputs andinvestments, including donors, the private sectorand other government sectors and agencies
Mechanisms in place to mobilize communitysupport for HRH

99
ANNEX 3 STAKEHOLDERS THAT RECEIVED AND/OR REVIEWED THE DRAFT HRH PLAN
Name Title Ministry/Organisation/AgencyDr Praveen Mistra Population Secretary MoHPMr Pratap Kumar Pathak Secretary Ministry of General
Administration (MoGA)Mr. Tilak Ram Sharma Joint Secretary Human
Resource and FinancialManagement Division & Chairof HRH Technical Committee
MoHP
Mr. Surya Prasad Acharya Joint Secretary PersonnelAdministration Division
MoHP
Dr Lava Deo Aawasthi Joint Secretary Ministry of EducationMr Atma Ram Pandey Joint Secretary National Planning
CommissionDr Bal Krishna Suvedi Chief, Policy Planning and
International CooperationDivision
MoHP
Mr Parshu Ram Shrestha Director General, DoHSMr. Kabiraj Khanal Under Secretary, Human
Resource Development SectionMoHP
Mr. Shiva PrasadShimkhada
Under Secretary FinanceDivision, & Core Team Member
MoHP
Mr. Tulsi Bdr. Shrestha Under Secretary Department Of Health ServiceMr Radha KrishnaPradhan
Under Secretary National PlanningCommission
Dr.Senendra Raj Upreti Chief Curative Division, MoHPDr Babu Ram Marasani MoHPMr Santosh Dahal MoHPProfessor Ghanim Alsheikh
HRH Consultant GHWA
Dr Tirtha Rana Public Health and NutritionSpecialist
Consultant
Dr MuhammadMahmood Afzal
Technical Officer Head ofCountry Facilitation Team
Global Health WorkforceAlliance, WHO
Health Services Academy Health Services Academy PakistanMerlin MerlinLatika Maskey Pradhan Program Manager AUSAid, Australian EmbassyDr Sharad Onta Institute of Medicine.Mr. Ram Chandra Khanal Senior Public Health
AdministratorMoHP
Mr. Parshu Ram Shrestha Senior Public HealthAdministrator
Department Of Health Service
Mr. Khagendra PrasadRijal
Section Officer HuRIC Unit, MoHP
Mr. Arjun Prasad Poudel Account Officer MoHPMr. Shovakar Neupane Section Officer MoEMs. Anita Lama Pra.a Nepal Medical CouncilProf. Trilok Pati Thapa Principal KIST Medical College

100
Mr. Arjun Bhadur Singh Director National Health TrainingCenter
Dr. Muknda Raj Panthi Registrar NAMSMr. Dhan Prasad Poudel Registrar NHPCMr. Sabin Kumar sharma Computer Programmer HuRIC Unit, MoHPMr. Gauri Bhadur Thapa Dietician Supervisor NPHFMr. Sharad BantaMr. Tirtha Rana ConsultantMs. Ishwori Devi Shrestha MoHPDr. Amit Bhandari Health Advisor DFID NepalDr Bert Voetberg Lead Health Specialist World BankDr Frank Paulin WRO WHO NepalDr Mark Zimmerman Executive Director Nick Simons InstituteMs. Takma K.C Nepal Nursing CouncilMs. Daya Laxmi JoshiBaidhya
President Nepal Nursing Council
Ms. Pramila Dewan President Nepal Nursing AssociationMr. Laxman PrasadGhimire
MoHP
Dr. Giridhari SharmaPaudel
Planning, Monitoring andSystem StrengtheningSpecialist
Western Regional HealthDirectorate, Pokhara
Dr. Bisho Raj Khanal Regional Director MoHP, PokharaDr. Buddhi B. Thapa Medical Superintendent Western Regional Hospital
PokharaMr. Ramesh Adhikari District Health Officer MoHP, Kaski, PokharaDr Nancy Gerein International Lead NHSSPMr Greg Whiteside QA Advisor NHSSPMr. Tomass Lievens Health Economist OPMDr Suresh Tawari Health Financing Advisor NHSSPMs. Chaya Jha GESI Advisor NHSSPMr Ramchandra ManSingh
Health Systems GovernanceAdvisor
NHSSP
Mr Sitaram Prasai GESI Advisor NHSSPMr Ajit Pradhan M&E Research Advisor NHSSPDr Maureen Dariang EHCS Advisor NHSSPDr Ganga Shakya MNH Advisor NHSSPMr Hom Nath Subedi Equity and Access Advisor &
Core Team MemberNHSSP
Mr Krishna Sharma Head of Admin and Finance NHSSPDr Devi Prasad Prasai Consultant, Demand side
FinancingNHSSP
Mr Bal Govinda Bista National HR Consultant LATH/NHSSP
Dr Shiva Adhikari Associate Professor ofEconomics (Health),
TribhuvanUniversity/LATH/NHSSPCosting Consultant
Dr Angel Magar Consultant/Core TeamMember
WHO
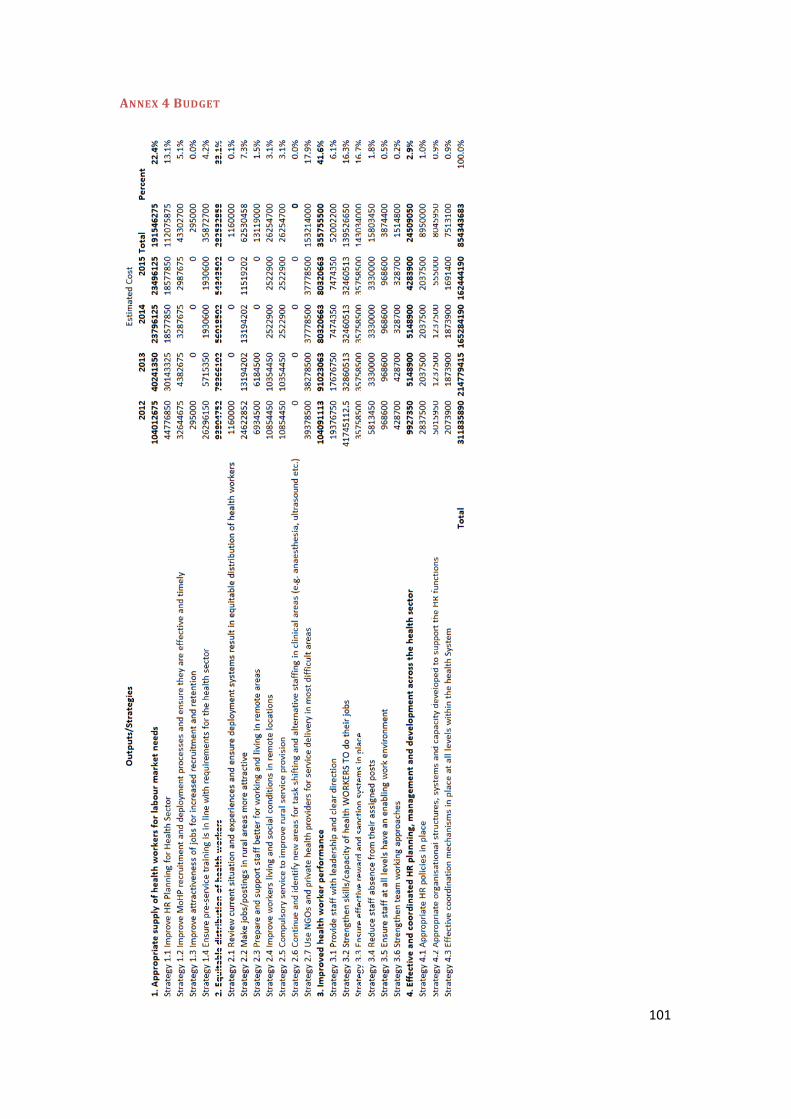
101
ANNEX 4 BUDGET
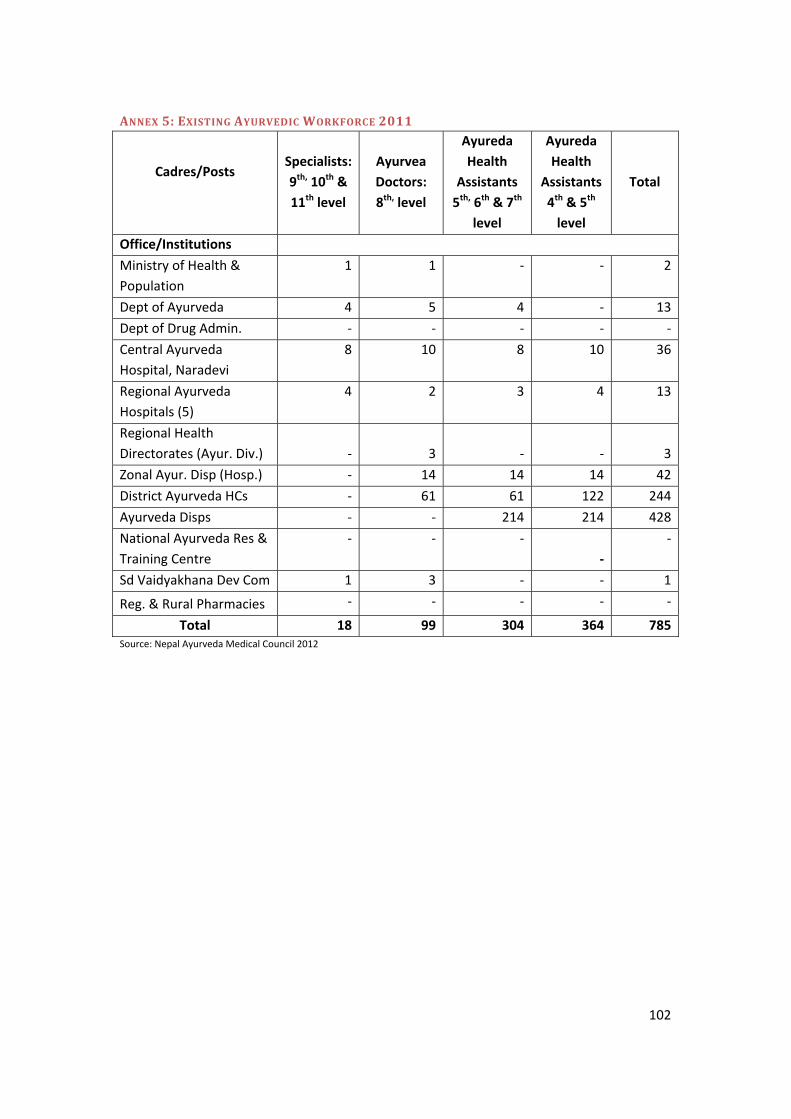
102
ANNEX 5: EXISTING AYURVEDIC WORKFORCE 2011
Cadres/PostsSpecialists:9th, 10th &11th level
AyurveaDoctors:8th, level
AyuredaHealth
Assistants5th, 6th & 7th
level
AyuredaHealth
Assistants4th & 5th
level
Total
Office/InstitutionsMinistry of Health &Population
1 1 2
Dept of Ayurveda 4 5 4 13Dept of Drug Admin.Central AyurvedaHospital, Naradevi
8 10 8 10 36
Regional AyurvedaHospitals (5)
4 2 3 4 13
Regional HealthDirectorates (Ayur. Div.) 3 3Zonal Ayur. Disp (Hosp.) 14 14 14 42District Ayurveda HCs 61 61 122 244Ayurveda Disps 214 214 428National Ayurveda Res &Training CentreSd Vaidyakhana Dev Com 1 3 1
Reg. & Rural PharmaciesTotal 18 99 304 364 785
Source: Nepal Ayurveda Medical Council 2012

103