human gingival fibroblast functions are stimulated by oxidized nano-structured titanium surfaces
TRANSCRIPT

Human gingival fibroblast functions are stimulatedby oxidized nano-structured titanium surfaces
Luigi Guida a, Adriana Oliva b, Maria Assunta Basile b, Michele Giordano c,Livia Nastri a, Marco Annunziata a,*aMultidisciplinary Department of Medical–Surgical and Dental Specialties, Second University of Naples, Via L. De
Crecchio, 6, 80138 Naples, ItalybDepartment of Biochemistry and Biophysics ‘‘F. Cedrangolo’’, Second University of Naples, Via L. De Crecchio, 7,
80138 Naples, Italyc Institute for Composite and Biomedical Materials, National Research Council (IMCB-CNR), Piazzale Enrico Fermi 1,
80055 Portici, Italy
j o u r n a l o f d e n t i s t r y 4 1 ( 2 0 1 3 ) 9 0 0 – 9 0 7
a r t i c l e i n f o
Article history:
Received 27 March 2013
Received in revised form
12 July 2013
Accepted 18 July 2013
Keywords:
Dental implant
Human gingival fibroblasts
Surface topography
Cell adhesion
Cell proliferation
Collagen synthesis
a b s t r a c t
Objectives: The aim of this study was to analyze the features of an oxidized titanium implant
surface and to evaluate its effects on the response of human gingival fibroblasts.
Methods: 10 mm � 10 mm � 1 mm turned (control) and oxidized (test) titanium samples
(P.H.I. s.r.l., Italy) were examined by scanning electron microscopy and atomic force
microscopy and characterized by height, spatial and hybrid roughness parameters. Primary
cultures of human gingival fibroblasts were seeded on titanium samples, and cell morphol-
ogy, adhesion, proliferation and extracellular matrix deposition, in terms of type I collagen
synthesis, were evaluated.
Results: Control and test surfaces appeared considerably different at the microscopic
analyses: turned samples were grooved, whereas oxidized surfaces showed a more complex
micro- and nano-scaled texture, as evidenced by roughness parameters. Cell adhesion and
proliferation rate, as well as collagen synthesis, were greater on oxidized vs turned surfaces.
Conclusions: Although both control and test samples were in the range of average roughness
proper of smooth surfaces, they exhibited significantly different topographic properties in
terms of height and, mostly, hybrid parameters. Furthermore, oxidized surfaces enhanced
human gingival fibroblast adhesion, proliferation and extracellular matrix deposition, and
this could be due to the different structure at micro- and nano-scale levels.
Clinical significance: Oxidized nanostructured titanium surfaces could have a significant
clinical utilization in virtue of their affinity for soft tissue attachment at the implant neck
and/or at the transmucosal portion of the prosthetic abutment.
# 2013 Elsevier Ltd. All rights reserved.
Available online at www.sciencedirect.com
journal homepage: www.intl.elsevierhealth.com/journals/jden
1. Introduction
The use of implant-supported dental prostheses represents
today one of the most proposed rehabilitative option for the
treatment of edentulism worldwide, thanks to the positive
* Corresponding author. Tel.: +39 0815665515; fax: +39 0815665515.E-mail address: [email protected] (M. Annunziata).
0300-5712/$ – see front matter # 2013 Elsevier Ltd. All rights reservehttp://dx.doi.org/10.1016/j.jdent.2013.07.009
impact of such rehabilitations on oral function, and conse-
quently on systemic health, and to their high survival and
success rates over extended follow-up periods.1–6
The main cause of implant failure is represented by the
perimplantitis infection, as a consequence of the penetration
d.

j o u r n a l o f d e n t i s t r y 4 1 ( 2 0 1 3 ) 9 0 0 – 9 0 7 901
of bacterial plaque into the peri-implant sulcus,7,8 so that the
game of implant success is mainly played at level of the peri-
implant soft-tissue attachment. The interface between the
transmucosal portion of implant surface and the surrounding
soft tissue is characterized by a fibroblast-rich barrier tissue,
which represents the main obstacle to bacterial invasion of
deep peri-implant tissues, being of pivotal importance for the
long-term stability and maintenance of the implant itself.9–12
Topographic and physicochemical properties of implant
surfaces have been demonstrated to affect both hard and soft
peri-implant tissue responses. For instance, different surface
treatments are routinely used to increase implant roughness
and promote osseointegration.13 Conversely, the transmuco-
sal portion of implant rehabilitations is conventionally made
of a smooth turned titanium surface in order to minimize
bacterial colonization. However, there is a growing evidence
that implant surface characteristics may play a role in the
attachment of peri-implant soft tissues.12,14–16
One of the most recent frontiers in dental implant research
includes the modification of the surface topography at nano-
scale level. Nano-structured surfaces have been speculated to
influence cell behaviour in a different way compared to
conventionally sized surfaces. Nanoscaled features may
create biomimetic relationship between alloplastic surfaces
and bone tissue through the recapitulation of natural cellular
environments at the nanoscale level13,17,18 whereas little is
known about their effect on soft peri-implant tissues.
Anodic oxidation is one of the most diffused technology
able to create structures of nano-scale dimension on the
implant surface. Recently we have demonstrated that nano-
structured surfaces obtained by anodic oxidation can affect
bone cell behaviour.19 The aim of the present study was to
characterize the micro- and nano-texture of an oxidized
titanium implant surface in comparison with a conventional
turned one, and to evaluate the ability of such surface to affect
the response of human gingival fibroblasts (HGF) in terms of
adhesion, proliferation and collagenic matrix synthesis.
2. Materials and methods
2.1. Products and reagents
All cell culture biologicals were purchased from Gibco BRL
(Grand Island, NY, USA), and all chemicals were from Sigma
Chemical Co. (St. Louis, MO, USA) when not otherwise specified.
2.2. Specimen preparation
Two different titanium implant surfaces were analyzed:
turned titanium surfaces (control) and oxidized titanium
surfaces (test). All specimens were provided by a commercial
firm (P.H.I. s.r.l., San Vittore Olona, Milano, Italy) in form of
10 mm � 10 mm � 1 mm samples of commercially pure tita-
nium. Test samples were produced by a process of anodic
oxidation carried out for 24 h in an aqueous solution of 1 M
sulphuric acid and 0.15% hydrofluoric acid at a cell voltage of
20 V at room temperature. After anodization, the samples
were thoroughly rinsed in distilled water and subsequently in
acetone, and finally dried with nitrogen stream.
For cell culture assays the samples were sterilized by
autoclaving and put on the bottom of 24-well plates.
2.3. Surface topography characterization
Qualitative and quantitative measurements of titanium
surfaces were made by atomic force microscopy (AFM). In
parallel, implant samples were also imaged by scanning
electron microscopy (SEM) to visualize their topographic
features on a larger spatial range.
AFM technique is based on a tip of atomic level, which is
brought close to the sample. The interaction forces between
the tip and the sample are recorded by the deflection of a laser
beam reflecting on the cantilever attached to the tip, in order
to produce an accurate three-dimensional map of outer
surface.
The images were obtained with an AFM-SNOM system: the
Multiview 1000 (by Nanonics Imaging Ltd), scanning probe
microscope operating in AFM tapping mode. The measuring
range available with this system was 75 mm in x, y and z
direction. Super-thin probes (cantilevered optical fibre probes,
nominal spring constant �5 N/m, resonance frequency in the
range 50–100 kHz, by Nanonics Imaging Ltd) with a tip radius
of curvature 5 nm were used in order to minimize convolution
effects.
Images were acquired at a 50 mm � 50 mm dimensional
range. Six images were collected on different points, randomly
distributed upon the surface, belonging both to the centre, and
to the edge of the samples.
A 25 mm � 25 mm Gaussian filter was applied to separate
roughness from errors of form and waviness, as recom-
mended by Wennerberg and Albrektsson.20 The evaluation
and the images were obtained using SPIPTM (Scanning Probe
Image Processor, Image Metrology, Denmark) software. The
following surface parameters were considered:
Sa (mm) = average roughness; average height deviation
from a mean plane within the measuring area, Sds
(mm�2) = summit density; the number of summits per unit
area, Sdr (%) = developed interfacial area ratio; additional
surface area contributed by the roughness compared to a
totally flat plane.
2.4. Preparation of human gingival fibroblasts
Samples of gingival tissue were harvested from healthy
donors undergone periodontal surgery.
Informed consent and research protocol were institution-
ally approved, according to the Declaration of Helsinki.
Collected tissues were washed two times with phosphate
buffered saline (PBS; 150 mM NaCl, 20 mM sodium phosphate
pH 7.2) supplemented with antibiotics (100 U/ml penicillin,
100 mg/ml streptomycin) and cut into small pieces with a
sterile surgical blade. Tissue fragments were digested in 1 ml
of Dulbecco’s modified Eagle’s medium-F12 (DMEM-F12)
containing antibiotics and 1 mg/ml type IV collagenase
(Worthington Biochemical, Freehold, NJ, USA) at 37 8C for
3 h. Released cells were harvested, plated in complete DMEM-
F12 containing antibiotics and 10% foetal bovine serum, and
incubated at 37 8C in a 5% CO2 humidified atmosphere. First
cell islets were visible after 3–4 days and confluence was

Fig. 1 – 50 mm T 50 mm atomic force microscopy (AFM) 3D
images of oxidized and turned implant surfaces.
j o u r n a l o f d e n t i s t r y 4 1 ( 2 0 1 3 ) 9 0 0 – 9 0 7902
reached in about 2–3 weeks. During this period, fresh medium
was added two times per week, never removing the entire
conditioned medium. After the confluence was reached, cells
were trypsinized and cultures expanded. For this study, HGF
obtained from two volunteers, one woman and one man, aged
35 and 56 years, respectively, were used. The cells harvested
from each donor were kept separately and not pooled.
Cultures between the second and fourth passage were used
in the present experiments.
2.5. Cell adhesion and proliferation evaluation by MTT
Control and test samples were put on the bottom of 24-well
plates. HGF were seeded on implant surfaces at a density of
30,000 cells/cm2 in complete culture medium. Cell adhesion to
implant surfaces at 6 h and cell proliferation at 48 h and 7 days
from plating were assessed by MTT vitality assay.21 The key
component of this assay is 3-(4,5-dimethylthiazol-2-yl)-2,5-
diphenyltetrazolium bromide (MTT). Mitochondrial dehydro-
genases of living cells reduce the tetrazolium ring, yielding a
blue formazan product that can be measured spectrophoto-
metrically. Cells were washed with PBS and incubated with
0.5 mg/ml MTT solution for 4 h at 37 8C. At the end of this time,
the liquid was aspirated and the insoluble formazan produced
was dissolved in isopropanol–HCl 0.1 M. The optical density
was measured at 570 nm, subtracting background absorbance
determined at 690 nm.
2.6. Cell adhesion and morphology evaluation by SEM andCLSM
Cell adhesion and morphology were also evaluated by
scanning electron microscopy (SEM) and confocal laser
scanning microscopy (CLSM). For SEM analysis cells were
plated on titanium surfaces as above mentioned. After 6 h the
cells were rinsed three times with PBS and fixed for 30 min
with 2.5% glutaraldehyde. The fixed cell layers were washed in
PBS, dehydrated by graded ethanol solutions (from 60% to
100%) and subjected to critical point drying. Samples were
mounted on stubs, coated with Au/Pd alloy and examined by
SEM (Philips SEM XL20).
Actin-based cytoskeleton was evidenced by immunofluo-
rescent staining using CLSM (C1-si, Nikon, Tokyo, Japan) after
24 h from cell seeding. The samples were prepared as follows:
titanium disks with layered cells were washed twice in PBS to
remove non attached cells. After rinsing, the cells were fixed in
4% paraformaldehyde in PBS for 10 min at 37 8C and
permeabilized with 0.2% Triton X-100 in PBS for 5 min at
37 8C. Permeabilized cells were treated with 0.5 ml/ml rhoda-
mine-phalloidin (Invitrogen, Paisley, UK) for 30 min and rinsed
in PBS.
2.7. Type I collagen synthesis
Conditioned medium of HGF cultured for 6 h, 48 h and 7 days
was collected and the amount of type I collagen released was
detected and quantified using a commercially available
enzyme-linked immunosorbent assay (ELISA) kit (Cosmo Bio
Co. Ltd, Tokyo, Japan). Assay buffer, sample and the
biotinylated anti-collagen antibody were added simultaneously
to the wells of microtiter-plate on which purified collagen was
immobilized. After washing, peroxidase labelled avidin, that
reacted with the biotinylated antibody on the microtiter-plate,
was added. Following further washing steps, tetramethylben-
zidine, a peroxidase substrate, was added. The level of type I
collagen in the sample was calculated on the basis of the optical
density determined at 450 nm and normalized to cell number.
In proportion to increase the collagen concentration of samples,
the colour density decreased since the amount of biotinylated
antibody and peroxidase labelled avidin decreased.
2.8. Statistical analysis
All the experiments were performed two times in quadrupli-
cate on two different cell preparations. No intra-group
difference was detected in any of the investigated parameters.
Differences between the experimental groups were analyzed
by non-parametric statistics (Wilcoxon Rank-Sum Test), with
the value of significance set at p < 0.05.22 Statistical analysis
was carried out using the NCSS software (NCSS for Windows,
Kaysville, Utah, USA).
3. Results
Three-dimensional AFM images of oxidized and turned
titanium samples are shown in Fig. 1. Fig. 2 shows SEM
images of the two surfaces at low and high magnification. It
is clearly observable in both SEM and AFM images that
grooves appeared on the turned samples, whereas the
oxidized ones showed a more complex topography. The
grooves present on the turned samples exhibited a prefer-
ential direction, whereas in the oxidized samples a uni-
formly rough surface, with grain-like particles of mean
diameter of 1.89 � 0.47 mm, seemed to be superimposed on a
previously grooved surface. A higher magnification SEM
image revealed the effective nanostructure of the oxidized
surface which was covered by tightly packed nano-tubules
with an external and internal mean diameter of 119 � 22 nm
and 50 � 11 nm, respectively.
Topographical parameters for both surfaces estimated by
AFM are reported in Table 1. When no filtering procedure was
applied, oxidized samples showed Sa values comparable to
turned ones, whereas using a 25 mm � 25 mm Gaussian filter
the situation reversed, with a significantly higher Sa mean
value for the oxidized surface. Such filter-dependence of the

Fig. 2 – Low and high magnification scanning electron microscopy (SEM) images of oxidized and turned titanium surfaces.
j o u r n a l o f d e n t i s t r y 4 1 ( 2 0 1 3 ) 9 0 0 – 9 0 7 903
roughness values was not evidenced for the other parameters
measured. The developed surface area of oxidized surface
showed the most evident difference between samples, being
the Sdr of the oxidized surface about one order of magnitude
higher than that of the turned one. On the contrary, no
significant difference of Sds between the two surfaces could be
assessed.
The following step in the characterization of titanium
surfaces was the biological evaluation of their interaction with
HGF in terms of cell adhesion, proliferation and extracellular
matrix deposition. At the SEM analysis, cells appeared
intimately spread on implant surfaces (Fig. 3). In particular
many cellular processes, such as philopodia and lamellipodia,
were evident on the oxidized surface, with a veil-like
appearance, in close contact with the underlying titanium
surface. Furthermore, the intimate interaction of cell process-
es with the nano-tubular structures became evident at higher
magnification.
Table 1 – Surface parameters of oxidized and turned titanium sGaussian filtering. Data are expressed as medians with minim
Parameter Sa (mm) Sd
Filter size None 25 mm � 25 mm None
Oxidized 0.227 (0.130–0.276) 0.076 (0.061–0.097) 1.105 (0.968–1.60
Turned 0.297 (0.193–0.343) 0.036 (0.020–0.69) 0.582 (0.405–1.70
Signif. p < 0.01
N = 6/group; signif. = statistically significant difference between oxidized
Immunofluorescence images (Fig. 4) showed a different
behaviour of the actin cytoskeleton of HGF grown for 6 h on
turned vs oxidized samples. In particular, cells appeared
fusiform and stretched out along the parallel grooves of the
turned surface, whereas a more evident spreading, without a
preferential direction, could be observed on the oxidized
sample.
When at 6-h MTT viability test was performed, markedly
greater values, as expression of higher numbers of adherent
cells, were evidenced on oxidized surfaces with respect to
turned ones (Fig. 5). Furthermore, at longer times, the
fibroblasts plated on the oxidized sample proliferated at a
substantially higher rate than cells attached on the turned
surface, reaching the maximum difference at 7 days.
In a parallel manner, when type I collagen production was
evaluated over time, HGF plated on the oxidized titanium
showed to synthesize a significantly higher protein amount,
normalized to cell number, compared with cells grown on the
urfaces (50 mm T 50 mm analysis range), with and withoutum and maximum values reported in parentheses.
s (mm�2) Sdr (%)
25 mm � 25 mm None 25 mm � 25 mm
0) 1.225 (1.090–1.700) 11.150 (7.860–24800) 10.500 (7.390–24.200)
0) 0.982 (0.769–1.910) 1.175 (0.552–3.050) 0.799 (0.212–2.480)
p < 0.01 p < 0.01
and turned.
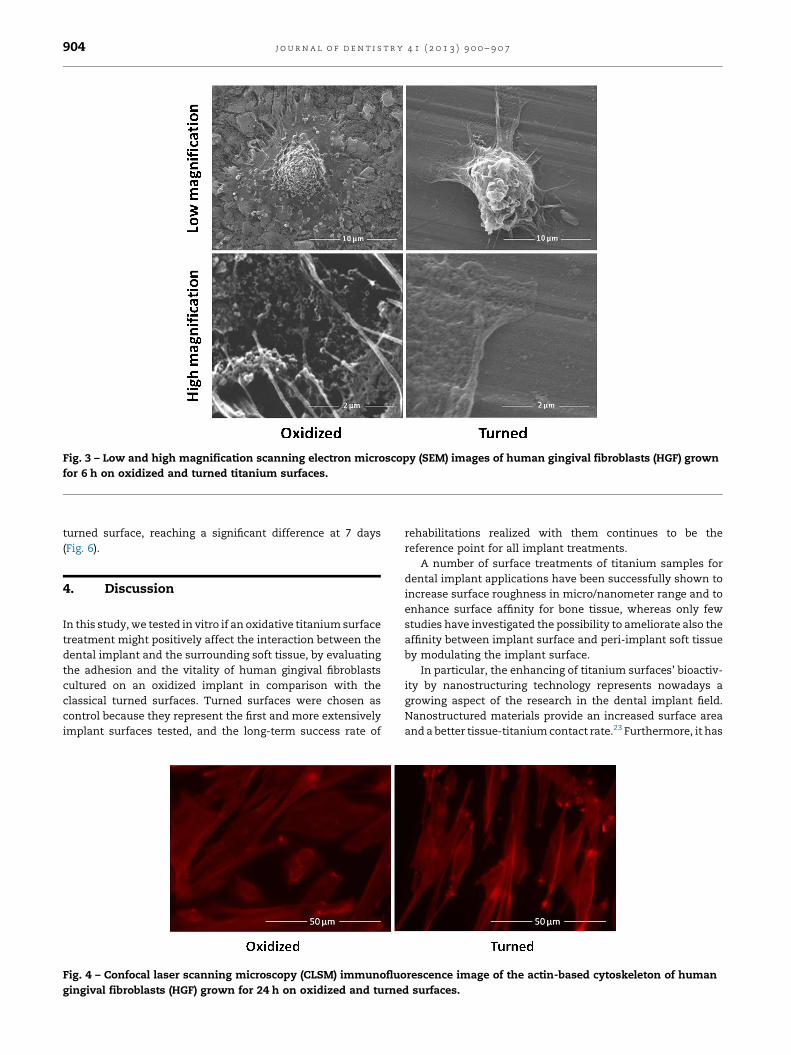
Fig. 3 – Low and high magnification scanning electron microscopy (SEM) images of human gingival fibroblasts (HGF) grown
for 6 h on oxidized and turned titanium surfaces.
j o u r n a l o f d e n t i s t r y 4 1 ( 2 0 1 3 ) 9 0 0 – 9 0 7904
turned surface, reaching a significant difference at 7 days
(Fig. 6).
4. Discussion
In this study, we tested in vitro if an oxidative titanium surface
treatment might positively affect the interaction between the
dental implant and the surrounding soft tissue, by evaluating
the adhesion and the vitality of human gingival fibroblasts
cultured on an oxidized implant in comparison with the
classical turned surfaces. Turned surfaces were chosen as
control because they represent the first and more extensively
implant surfaces tested, and the long-term success rate of
Fig. 4 – Confocal laser scanning microscopy (CLSM) immunofluo
gingival fibroblasts (HGF) grown for 24 h on oxidized and turne
rehabilitations realized with them continues to be the
reference point for all implant treatments.
A number of surface treatments of titanium samples for
dental implant applications have been successfully shown to
increase surface roughness in micro/nanometer range and to
enhance surface affinity for bone tissue, whereas only few
studies have investigated the possibility to ameliorate also the
affinity between implant surface and peri-implant soft tissue
by modulating the implant surface.
In particular, the enhancing of titanium surfaces’ bioactiv-
ity by nanostructuring technology represents nowadays a
growing aspect of the research in the dental implant field.
Nanostructured materials provide an increased surface area
and a better tissue-titanium contact rate.23 Furthermore, it has
rescence image of the actin-based cytoskeleton of human
d surfaces.

Fig. 5 – Human gingival fibroblast (HGF) adhesion and
proliferation on oxidized and turned titanium surfaces
assessed by MTT test. Data are expressed as medians with
lower/upper quartiles and minimum/maximum values.
N = 8/group; *p < 0.001.
j o u r n a l o f d e n t i s t r y 4 1 ( 2 0 1 3 ) 9 0 0 – 9 0 7 905
been speculated that they directly affect bone cell behaviour in
a different way from conventional rough surfaces, that is
creating a biomimetic relationship with host tissues through
the recapitulation of natural cellular environments at the
nanoscale level.13,17,24
When we talk of surface features in the nanometer scale,
we refer to topographical characteristics with dimensions less
than 100 mm. The oxidized surface we tested showed both a
micro- and a nanoscale topography. In particular, we
evidenced grain-like particles of microscale dimension super-
imposed on a previously grooved surface covered by tightly
packed tubular structures of nanoscale dimension.
Several approaches are currently available for manipulat-
ing experimental surfaces at the nanoscale level, including
self-assembly of molecules monolayers, physical approaches,
chemical approaches, nanoparticle deposition or optical
methods.13 All these technologies differ from one to another
for cost, time, reproducibility, complexity of the procedure and
for shape, size and chemistry of the nanostructures. The
anodic oxidation method is able to form nanostructured
features by creating a new oxide layer upon the surface of the
titanium implants used as an anode in a galvanic cell with a
suitable electrolyte.25,26 The characteristic of such oxide layer
can be modulated depending on the parameters used for
oxidation. The oxidized surfaces tested in our experiments
exhibited nanostructures of controlled and reproducible
dimension, with an extremely uniform and isotropic distribu-
tion over the surface.
Fig. 6 – Type I collagen synthesis by human gingival
fibroblasts (HGF) grown on turned and oxidized surfaces.
Data are expressed as medians with lower/upper quartiles
and minimum/maximum values. N = 8/group; *p < 0.001.
Although both tested oxidized and turned surfaces must be
included in the ‘‘smooth’’ category (following Albrektsson and
Wennerberg classification of 2004)27 basing on their Sa value at
a wide range, however they showed considerably different
characteristics at micro- and nanoscale level that could not be
detected by conventional roughness analysis. In fact, only
when a proper filter was applied to exclude errors of form and
waviness, and adjunctive three-dimensional surface param-
eters were considered, it was possible to find out the
significantly more complex texture of the oxidized surface
and its nanoscale features. This finding confirms what was
described by Wennerberg and Albrektsson20 that an exhaus-
tive characterization of a surface can be obtained only using
multiple roughness parameters and proper filtering proce-
dures. Each surface parameter, indeed, evaluates specific
topographical aspects and is expression of specific surface
features. For this reason, two distinct surfaces may appear
comparable in terms of a given surface parameter, but
significantly different measuring other ones or applying
specific filtering procedures. Also in our case, the surface
analysis of turned and oxidized surfaces led to considerably
different results in terms of Sa, for instance, with vs without
Gaussian filtering, or in terms of Sds vs Sdr. In particular, the
significantly higher Sdr values measured for the oxidized
surface with respect to turned one indicates a higher
developed area and is expression of the complex texture,
especially at nanoscale level, of such surface. At the same time,
however, both surfaces resulted comparable in terms of Sds,
which measures the density of summits over the surface. Such
finding on one side is expression of a similar pattern of summits
distribution over both surfaces and, on the other side, is also
affected by the specific thresholds existing for summits to be
properly detected, so that the oxidized surface could be
underestimated in terms of Sds. In fact, to be detectable and
measured as Sds, summits are constrained to be separated by at
least 1% of the minimum ‘‘X’’ or ‘‘Y’’ dimension comprising the
three-dimensional measurement area. Additionally, summits
are only found above a threshold that is 5% of the ten-point
mean roughness (Sz) above the mean plane.
The higher percentage of additional area contributed by the
complex nano-roughened oxidized surface could have some
implications from a biological standpoint at either tissue level,
providing larger and more intimate interlocking between
implant surface and peri-implant soft tissue, or cellular level,
as it will be discussed in succession.
In order to evaluate the biological features of these
surfaces, we choose, as cellular model, primary cultures of
human gingival fibroblasts, which are the main resident cell
population inside the peri-implant connective attachment.
We found that fibroblasts very intimately adhered on the
oxidized surface, taking contact with the complex micro and
nano topography of such surface by numerous philopodia-
like cellular extensions. Differently, HGF exhibited a less
intimate spreading on smooth turned surfaces, as evidenced
by comparing the respective SEM and immunofluorescence
microscopy images. Both direct cell–surface interactions
and indirect protein–surface interactions may explain this
finding,28 which is of pivotal importance, representing the
first step of every following event at the soft tissue-implant
interface.

j o u r n a l o f d e n t i s t r y 4 1 ( 2 0 1 3 ) 9 0 0 – 9 0 7906
We also found that the adhesion and the proliferation rate
of fibroblasts was significantly increased on the oxidized
nano-structured surface with respect to the turned one, in a
time dependent manner.
Interestingly, and in support of our data, a recent study
demonstrated that fibroblast functions were stimulated by
oxidized nanostructured titanium surfaces,29 although in that
case cells of animal origin (NIH/3T3 murine fibroblasts) were
used.
Another finding of this study was that HGF cultured on
oxidized surfaces showed higher levels of type I collagen
synthesis. Type I collagen is the major component of the
extracellular matrix of connective tissues and plays a central
role in the architecture of the peri-implant tissue which is
formed by both epithelial and connective structures. In
particular, the connective attachment underlying the junc-
tional epithelium is constituted by a scar-tissue-like tissue
with high density of high turn-over fibroblasts (about one third
in volume) and collagen fibres (about two third in volume)
disposed in close contact with the titanium surface of the
implant neck.10
The more complex surface topography of anodic oxidized
samples at both the micro and the nano-scale level can
explain, at least in part, the different cellular functions put in
evidence in our study.
Different studies suggested that surface properties (topog-
raphy, physics, chemistry) of the transmucosal portion of
dental implants can affect the architecture of the peri-implant
mucosal barrier.12,15,16,30 It has been suggested that a certain
surface roughness may be needed for optimal soft tissue
sealing, enhancing the interaction between the surface
texture and soft tissue cell attachment and proliferation.30
In particular, minor epithelial downgrowth and longer
connective tissue seal have been histologically demonstrated
in humans for rough titanium implants (oxidized and acid-
etched) compared to smooth ones (turned).15
Surface roughness and chemical composition of the
implant surface, however, have been suggested to have a
significant impact on bacterial adhesion and plaque forma-
tion.31–33 It has been suggested by in vitro observations that a
surface roughness value (Ra) of about 0.2 mm can be consid-
ered as a threshold value below which no further significant
changes in the total amount of adhering bacteria can be
observed.34 However, the clinical relevance of such limit is
questionable, and the few and heterogeneous studies avail-
able do not allow to find a strong correlation between surface
characteristics and the initiation of peri-implantitis.7,35 Both
oxidized and turned surfaces tested in this study, although
characterized by not-filtered Sa values slightly higher than
0.2 mm, remain largely below the upper limit of smooth
surfaces (i.e. 0.5 mm), which are currently applied at the
transmucosal portion of fixtures and abutments. In this sense,
it is particularly interesting the possibility that nano-struc-
tured surfaces, may on one side enhance the attaching and
sealing of peri-implant soft tissues, being, on the other side, as
low-attractive for oral bacteria as conventional turned
surfaces.
In conclusion, the present in vitro study demonstrated that
a nanostructured titanium implant surface obtained by anodic
oxidation clearly stimulated gingival fibroblast functions over
time, including adhesion, proliferation and extracellular
matrix synthesis, compared to traditional smooth turned
surfaces. Such biological effects can be related to the different
texture between the two titanium surfaces at the micro- and
mainly at the nano-scale level, which could be properly
characterized only using a multi-parameter analytical ap-
proach.
The possibility to affect cell behaviour and, by this, increase
the stability of the peri-implant mucosal barrier, simply acting
on surface modifications is particularly fascinating. Further
studies, however, are needed to investigate the in vivo and
clinical implications of such encouraging preliminary results.
Acknowledgement
The authors want to thank P.H.I. (San Vittore Olona, Milano,
Italy) for kindly providing the titanium samples used in the
present study.
r e f e r e n c e s
1. Ferrigno N, Laureti M, Fanali S, Grippaudo G. A long-termfollow-up study of non-submerged ITI implants in thetreatment of totally edentulous jaws Part I: Ten-year lifetable analysis of a prospective multicenter study with 1286implants. Clinical Oral Implants Research 2002;13:260–73.
2. Ekelund JA, Lindquist LW, Carlsson GE, Jemt T. Implanttreatment in the edentulous mandible: a prospective studyon Branemark system implants over more than 20 years.International Journal of Prosthodontics 2003;16:602–8.
3. Rasmusson L, Roos J, Bystedt H. A 10-year follow-up study oftitanium dioxide-blasted implants. Clinical Implant Dentistryand Related Research 2005;7:36–42.
4. Smith B, Baysan A, Fenlon M. Association between oral healthimpact profile and general health scores for patients seekingdental implants. Journal of Dentistry 2009;37:357–9. May.
5. Thomason JM, Kelly SA, Bendkowski A, Ellis JS. Two implantretained overdentures – a review of the literature supportingthe McGill and York consensus statements. Journal ofDentistry 2012;40:22–34.
6. Moynihan PJ, Elfeky A, Ellis JS, Seal CJ, Hyland RM,Thomason JM. Do implant-supported dentures facilitateefficacy of eating more healthily? Journal of Dentistry2012;40:843–50.
7. Heitz-Mayfield LJ. Peri-implant diseases: diagnosis and riskindicators. Journal of Clinical Periodontology 2008;35:292–304.
8. Al-Radha AS, Pal A, Pettemerides AP, Jenkinson HF.Molecular analysis of microbiota associated with peri-implant diseases. Journal of Dentistry 2012;40:989–98.
9. Berglundh T, Lindhe J, Ericsson I, Marinello CP, Liljenberg B,Thomsen P. The soft tissue barrier at implants and teeth.Clinical Oral Implants Research 1991;2:81–90.
10. Moon IS, Berglund T, Abrahamsson I, Linder E, Lindhe J. Thebarrier between the keratinized mucosa and the dentalimplant. An experimental study in the dog. Journal of ClinicalPeriodontology 1999;26:658–63.
11. Klinge B, Meyle J. Working group 2 soft-tissue integration ofimplants consensus report of working group 2. Clinical OralImplants Research 2006;17:93–6.
12. Schupbach P, Glauser R. The defense architecture of thehuman periimplant mucosa: a histological study. Journal ofProsthetic Dentistry 2007;97:S15–25.

j o u r n a l o f d e n t i s t r y 4 1 ( 2 0 1 3 ) 9 0 0 – 9 0 7 907
13. Mendonca G, Mendonca DB, Aragao FJ, Cooper LF.Advancing dental implant surface technology – frommicron- to nanotopography. Biomaterials 2008;29:3822–35.
14. Abrahamsson I, Zitzmann NU, Berglundh T, Linder E,Wennerberg A, Lindhe J. The mucosal attachment totitanium implants with different surface characteristics: anexperimental study in dogs. Journal of Clinical Periodontology2002;29:448–55.
15. Glauser R, Schupbach P, Gottlow J, Hammerle CH.Periimplant soft tissue barrier at experimental one-piecemini-implants with different surface topography inhumans: a light-microscopic overview and histometricanalysis. Clinical Implant Dentistry and Related Research2005;7:S44–51.
16. Welander M, Abrahamsson I, Berglundh T. The mucosalbarrier at implant abutments of different materials. ClinicalOral Implants Research 2008;19:635–41.
17. Kubo K, Tsukimura N, Iwasa F, Ueno T, Saruwatari L, Aita H,et al. Cellular behavior on TiO2 nanonodular structures in amicro-to-nanoscale hierarchy model. Biomaterials2009;30:5319–29.
18. Wennerberg A, Albrektsson T. On implant surfaces: areview of current knowledge and opinions International.Journal of Oral and Maxillofacial Implants 2010;25:63–74.
19. Annunziata M, Oliva A, Buosciolo A, Giordano M, Guida A,Guida L. Bone marrow mesenchymal stem cell response tonano-structured oxidized and turned titanium surfaces.Clinical Oral Implants Research 2012;23:733–40.
20. Wennerberg A, Albrektsson T. Suggested guidelines for thetopographic evaluation of implant surfaces. InternationalJournal of Oral and Maxillofacial Implants 2000;15:331–44.
21. Mosmann T. Rapid colorimetric assay for cellular growthand survival: application to proliferation and cytotoxicityassays. Journal of Immunological Methods 1983;65:55–63.
22. Hannigan A, Lynch Christopher D. Statistical methodologyin oral and dental research: pitfalls and recommendations.Journal of Dentistry 2013;41:385–92.
23. Meirelles L, Arvidsson A, Albrektsson T, Wennerberg A.Increased bone formation to unstable nano rough titaniumimplants. Clinical Oral Implants Research 2007;18:326–32.
24. Guida L, Annunziata M, Rocci A, Contaldo M, Rullo R, OlivaA. Biological response of human bone marrow
mesenchymal stem cells to fluoride-modified titaniumsurfaces. Clinical Oral Implants Research 2010;21:1234–41.
25. Le Guehennec L, Soueidan A, Layrolle P, Amouriq Y. Surfacetreatments of titanium dental implants for rapidosseointegration. Dental Materials 2007;23:844–54.
26. Wennerberg A, Albrektsson T. Effects of titanium surfacetopography on bone integration: a systematic review.Clinical Oral Implants Research 2009;20:172–84.
27. Albrektsson T, Wennerberg A. Oral implant surfaces: part 1– review focusing on topographic and chemical properties ofdifferent surfaces and in vivo responses to themInternational. Journal of Prosthodontics 2004;17:536–43.
28. Brunette DM. The effects of implant surface topography onthe behavior of cells. International Journal of Oral andMaxillofacial Implants 1988;3:231–334.
29. Miura S, Takebe J. Biological behavior of fibroblast-like cellscultured on anodized-hydrothermally treated titanium witha nanotopographic surface structure. Journal of ProsthodonticResearch 2012;20. [Epub ahead of print].
30. Quirynen M, De Soete M, van Steenberghe D. Infectious risksfor oral implants: a review of the literature. Clinical OralImplants Research 2002;13:1–19.
31. Teughels W, Van Assche N, Sliepen I, Quirynen M. Effect ofmaterial characteristics and or surface topography onbiofilm development. Clinical Oral Implants Research2006;17:68–81.
32. Al-Radha AS, Dymock D, Younes C, O’Sullivan D. Surfaceproperties of titanium and zirconia dental implantmaterials and their effect on bacterial adhesion. Journal ofDentistry 2012;40:146–53.
33. Annunziata M, Oliva A, Basile MA, Giordano M, Mazzola N,Rizzo A, et al. The effects of titanium nitride-coating on thetopographic and biological features of TPS implant surfaces.Journal of Dentistry 2011;39:720–8.
34. Quirynen M, van der Mei HC, Bollen CM, Schotte A,Marechal M, Doornbusch GI, et al. An in vivo study of theinfluence of the surface roughness of implants on themicrobiology of supra- and subgingival plaque. Journal ofDental Research 1993;72:1304–9.
35. Renvert S, Polyzois I, Claffey N. How do implant surfacecharacteristics influence periimplant disease? Journal ofClinical Periodontology 2011;38:214–22.