howard fink, md, mph minneapolis va medicine research conference january 22, 2009 parkinson’s...
TRANSCRIPT

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
Parkinson’s Disease Parkinson’s Disease and Skeletal Healthand Skeletal HealthMinneapolis VA Medicine Research Minneapolis VA Medicine Research
ConferenceConference
January 22, 2009January 22, 2009
Howard Fink, MD, MPHHoward Fink, MD, MPH

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
SummarySummary
• There is accumulating evidence that PD is an important osteoporosis risk factor.

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
SummarySummary
• There is accumulating evidence that PD is an important osteoporosis risk factor.
1. What is that evidence?
2. By what mechanism(s) may PD be associated with osteoporosis?
3. What should be done about this?
Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
SummarySummary
• There is accumulating evidence that PD is an important osteoporosis risk factor.
1. What is that evidence?
2. By what mechanism(s) may PD be associated with osteoporosis?
3. What should be done about this?

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
SummarySummary
• There is accumulating evidence that PD is an important osteoporosis risk factor.
1. What is that evidence?
2. By what mechanism(s) may PD be associated with osteoporosis?
3. What should be done about this?

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
Parkinson’s DiseaseParkinson’s Disease

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
Parkinson’s DiseaseParkinson’s Disease
• Clinical presentation: – Tremor, rigidity, bradykinesia– Postural instability & gait disorder– Dementia may occur at late stages
• Course: – Usually mid- to late-life onset
• First symptoms occur at >55 yrs in 70% of patients
• Prevalence rises to ~3% at >80 yrs– Slowly progressive

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
OsteoporosisOsteoporosis

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
OsteoporosisOsteoporosis
• Definition:– Skeletal disorder w/ reduced bone strength &
increased fracture risk

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
OsteoporosisOsteoporosis• Bone strength reflects dynamic bone
remodeling– Bone breakdown is coupled to subsequent bone
formation– Skeleton repairs & adapts to changes in its strain
exposure
• Bone strength is function of:– Bone mineral density (BMD)– Bone geometry– Bone quality (i.e. architecture, turnover, damage)

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
OsteoporosisOsteoporosis• Epidemiology:
– There is no existing clinical measure of bone strength
– Defined by BMD criteria (strong predictor of fracture risk)
– FRAX calculator of absolute fracture risk to help define treatment thresholds: http://www.shef.ac.uk/FRAX/
– Most who might be considered for treatment based on BMD or FRAX are undiagnosed
• Consequences: – ~1.5 million “osteoporotic” fractures/yr in U.S., most
commonly spine, hip and wrist

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
What is the evidence What is the evidence for Parkinson’s Disease for Parkinson’s Disease
as a risk factor for as a risk factor for Osteoporosis?Osteoporosis?

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
Association of PD with Association of PD with OsteoporosisOsteoporosis
• Multiple case-control or retrospective studies published 1987-2002 reported PD associated with lower BMD– None reported consistent findings at >1
skeletal site– Half examined BMD measures not in wide
clinical use– No studies examined whether factors other
than age & sex could have accounted for observed findings

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
Association of PD with Association of PD with OsteoporosisOsteoporosis
• In prospective data from the Study of Osteoporotic Fractures (SOF)1:
– PD associated with ~2-fold increased hip fracture risk partially attenuated by adjustment for age & baseline BMD
• Association between PD & fractures assumed attributable in part to increased falls risk
1Taylor BC, JAGS 2004

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
Association Between Parkinson’s Disease Association Between Parkinson’s Disease and Low Bone Density and Falls in Older and Low Bone Density and Falls in Older
Men: Men: The Osteoporotic Fractures in Men The Osteoporotic Fractures in Men
(MrOS) Study.(MrOS) Study.
Fink HA, Kuskowski MA, Orwoll ES, Cauley JA, Ensrud KE.
J Am Geriatr Soc 53:1559–1564, 2005

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
MrOS Study DesignMrOS Study Design
• Ongoing multi-site, prospective cohort study of predictors of osteoporosis and fractures in older men
• Enrolled 5995 men aged >65, primarily from population-based sources

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
Baseline Data Baseline Data CollectionCollection
• Ascertainment of PD:
– Subject self-report to questionnaire: “Has a doctor or other healthcare provider ever told you that you had or have Parkinson’s disease?”
• N=52 with PD
• N=5943 with no PD
• Measurement of BMD– DXA: Areal BMD (g/cm2) of lumbar spine, total hip &
hip subregions

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
Other Baseline Other Baseline MeasurementsMeasurements
• Age, height, weight
• PMH/comorbidities (e.g. DM, stroke, CHF, fractures, falls)
• Medications
• Habits (e.g. activity, diet, smoking, alcohol)
• Self-reported function (e.g. QOL, IADLs)
• Physical/mental performance (e.g. leg power, walking speed, balance)
• Cognition, vision

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
AnalysesAnalyses
• ANCOVA to estimate cross-sectional association between PD and BMD measures
• Results expressed as mean percentage (95%CI) BMD differences between men with and without PD
• Multivariate model construction:– Considered factors associated both with PD and the
specific BMD measure (p<0.10)
– Variables also examined for clinical comprehensibility, correlation with other associated variables, and degree of missing data
– Step-wise selection (p<0.05 for retention)

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
Association Between PD Association Between PD & Areal BMD (DXA)& Areal BMD (DXA)

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
Fall RiskFall Risk
• After adjusting for age & past falls, those w/PD had 2.3-fold increased risk of multiple future falls

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
The association of Parkinson’s The association of Parkinson’s disease with bone mineral density disease with bone mineral density
and fracture in older women and fracture in older women
Schneider JL, Fink HA, Ewing SK, Ensrud KE, Cummings SR, for the Study of Osteoporotic
Fractures (SOF) Research Group
Osteoporos Int 2008;19:1093-97

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
SOF Study DesignSOF Study Design
• Ongoing multi-site, prospective cohort studying predictors of osteoporosis and fractures in older women
• Enrolled 9704 women aged >65, primarily from population-based sources
• 8105 attended study visit 4 and had known PD status

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
SOF Visit 4 Data SOF Visit 4 Data CollectionCollection
• Ascertainment of PD:
– Self-report questionnaire: “Has a doctor or other healthcare provider ever told you that you had or have Parkinson’s disease?”
• N=73 with PD
• N=8032 with no PD
• Measurement of BMD– Areal BMD (g/cm2) of lumbar spine, total hip & hip
subregions with DXA

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
Other SOF Other SOF MeasurementsMeasurements
Measured at visit 4• Age, height, weight
• PMH/comorbidities (e.g. DM, stroke, CHF, fractures, falls)
• Medications
• Habits (e.g. activity, diet, smoking, alcohol)
• Self-reported health status (e.g. QOL, IADLs)
• Cognition
Measured at visit 2• Neuromuscular function (e.g. leg power, walking speed,
balance)

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
AnalysesAnalyses
• Linear regression to estimate cross-sectional association between PD and hip BMD– Results for mean age-adjusted BMD in men with and
without PD were compared with t-tests
• Cox proportional hazards to estimate risk of incident hip, and nonspine nonhip fractures
Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
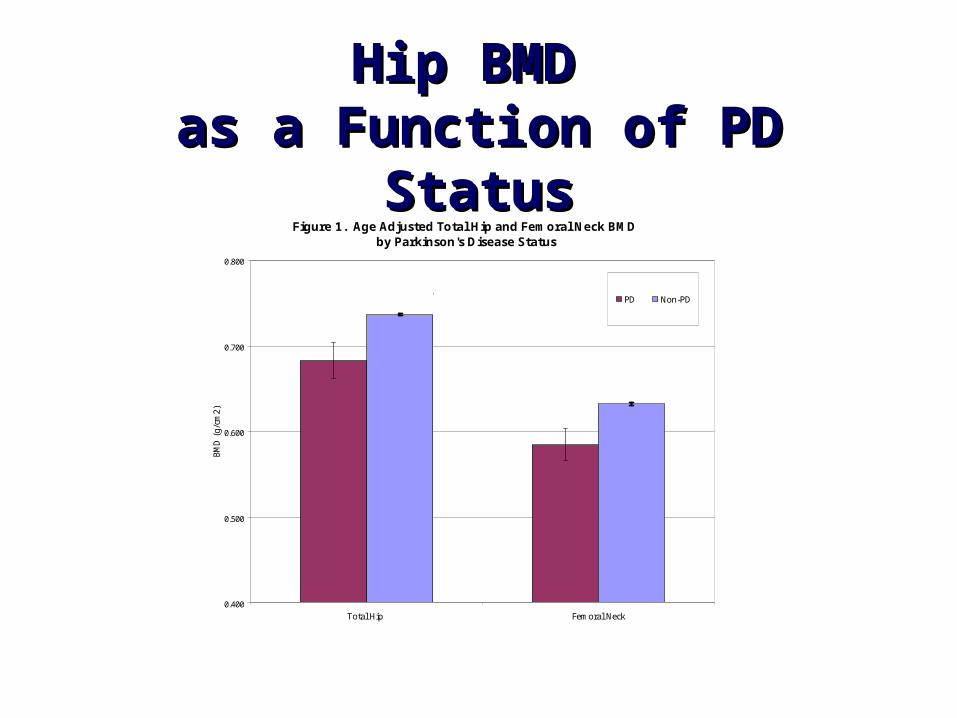
Hip BMD Hip BMD as a Function of PD Statusas a Function of PD Status
Figure 1. Age Adjusted Total Hip and Femoral Neck BMD by Parkinson's Disease Status
0.400
0.500
0.600
0.700
0.800
Total Hip Femoral Neck
BMD
(g/
cm2)
PD Non-PD
0.68 (0.64, 0.72)
0.74(0.73, 0.74)
0.59 (0.55, 0.62)
0.63 (0.63, 0.64)

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
Incident Hip Fracture RiskIncident Hip Fracture Risk

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
Fall RiskFall Risk
• Among community-dwelling older women, after adjusting for age & weight, those w/PD had 3.7-fold increased risk of multiple future falls

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
Association of Parkinson’s disease with accelerated bone loss, fractures
and mortality in older men: the Osteoporotic Fractures in Men
(MrOS) study
Fink HA, Kuskowski MA, Taylor BC, Schousboe JT, Orwoll ES, Ensrud KE,
for the Osteoporotic Fractures in Men (MrOS) Study Group
Osteoporos Int 2008;19:1277-82

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
MrOS Data CollectionMrOS Data Collection
• PD status ascertained at visits 1 & 2 (mean 4.6y interval):
– Subject self-report to questionnaire: “Has a doctor or other healthcare provider ever told you that you had or have Parkinson’s disease
• Visits 1 & 2 measurement of BMD– Areal BMD (g/cm2) of lumbar spine, total hip & hip
subregions with DXA

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
MrOS Visit 1 & 2 MrOS Visit 1 & 2 MeasuresMeasures
• Age, height, weight (weight change from baseline calculated)
• Comorbidities (including recent falls)
• Medications
• Habits (e.g. activity, diet, smoking, alcohol)
• Self-reported function (e.g. QOL, IADLs)
• Physical/mental performance (e.g. leg power, walking speed, balance)
• Cognition

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
AnalysesAnalyses
• Definition of PD: Men reported ‘PD’ at baseline, did not report ‘no PD’ at follow-up (n=46)
• Definition of No PD: Men reported ‘no PD’ at baseline, did not report ‘PD’ at follow-up (n=5891)
• Change in hip BMD estimable in 19 (41.3%) men with PD and 4356 (73.9%) of men without PD.

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
AnalysesAnalyses
• Hip BMD change could not be determined in 27 PD men: – 16 (34.8%) died prior to visit 2
– 1 terminated prior to visit 2
– 2 refused to attend visit 2 due to health problems
– 7 completed visit 2 questionnaire but no BMD measurement
– 1 whose contralateral hip was measured at visit 2

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
AnalysesAnalyses
• Age-adjusted annualized % bone loss in men with & without PD assessed using ANCOVA.
• Variables associated with PD status (p<0.10) examined as covariates in separate age-adjusted models
• Multivariate modeling not performed as only a small number of PD subjects had both baseline & follow-up BMD measures

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
Impact of patient population on results
Volunteer cohort+ Prospective studies allow collection
of extensive pre-fx measures
– Results may not be representative for all men with fx• Participants likely healthier, community-
dwelling, more well-educated, etc

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
Why might PD be Why might PD be associated with associated with osteoporosis?osteoporosis?
Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
Postulated Mechanisms Postulated Mechanisms for PD-Osteoporosis for PD-Osteoporosis
AssociationAssociation• Reduced mobility or
neuromuscular function
• Vitamin D deficiency
• Altered estrogen level
• Low weight / weight loss
• Parkinson’s disease medications
Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
Postulated Mechanisms Postulated Mechanisms for PD-Osteoporosis for PD-Osteoporosis
AssociationAssociation• Reduced activity or neuromuscular
function– PD→reduced activity and
neuromuscular function→increased bone resorption

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
Postulated Mechanisms Postulated Mechanisms for PD-Osteoporosis for PD-Osteoporosis
AssociationAssociation• Vitamin D deficiency
– PD and osteoporosis both epidemiologically associated with vitamin D deficiency
– Conventional thinking: • PD→decreased sun exposure & dietary vit D
intake→decreased calcium absorption→secondary hyperparathyroidism→increased bone resorption
– Recently theorized:• Vit D deficiency→decreased activation of 1,25-OH vit D
in substantia nigra→disruption of brain cell function (Newmark HL, Mov Disord 2007;22:461-8)
– Vit D receptors and 1-alpha hydroxylase distributed in brain, including most strongly in hypothalamus & substantia nigra (Eyles DW, J Chem Neuroanat 2005;29:21-30)
– Case report of improved PD symptoms with high dose 25-OH vit D (Derex L, Mov Disord 1997;12:612-13)

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
Postulated Mechanisms Postulated Mechanisms for PD-Osteoporosis for PD-Osteoporosis
AssociationAssociation• Altered estrogen level
– Estrogen deficiency known to cause bone loss
– Data suggestive that estrogen deficiency also may contribute to development of PD
• PD more common in M>F, more common in women w/reduced endogenous estrogen exposure
• Aromatase KO mice more vulnerable to parkinsonian neurotoxin MPTP (Morale MC, Brain Res Rev 2008;57:431-43)
• Small trials suggest ERT may improve motor symptoms in PD (Nicolleti A, Clin Neuropharm 2007;30:276-80. Tsang KL, Neurology 2000;54:2292-8)
Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
Postulated Mechanisms Postulated Mechanisms for PD-Osteoporosis for PD-Osteoporosis
AssociationAssociation• Low weight / weight loss
– Weight loss strongly associated with bone loss in prospective studies
– Parkinson’s disease associated with weight loss, both before and after diagnosis
– In older men, adjustment for concurrent weight loss attenuated association between PD and bone loss more than any other variable, but did not eliminate the association1
1 Fink HA, Osteoporos Int 2008;19:1277-82

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
Postulated Mechanisms Postulated Mechanisms for PD-Osteoporosis for PD-Osteoporosis
AssociationAssociation• Parkinson’s disease medications
– From case-control data1 • Inconsistent association between different classes
of PD medications (levodopa, dopamine agonists, COMT inhibitors, MAO-B inhibitors, anticholinergics) and fracture risk
• No evidence that association varied by dose or duration of use
– Interpretation complicated by confounding by indication
1Vestergaard P, Calcif Tissue Int 2007;81:153-61.

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
What, if anything, What, if anything, should be done about should be done about
this?this?

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
What to Do: Clinical?What to Do: Clinical?
• Treat PD patients to reduce bone loss, prevent fractures?– There is some evidence that osteoporosis-
specific treatments reduce bone loss and prevent hip fractures in PD patients.

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
Amelioration of osteoporosis by menatetrenone in elderly female
Parkinson’s Disease patients with vitamin D deficiency.
Sato Y, et al. Bone 2002;31:114.• Double-blind RCT• 120 postmenopausal Japanese PD patients (mean 72y)
– Exclusions: nonvertebral fx, recent or regular use of bone active meds, known cause of osteoporosis
– Mean baseline BMD 2.2 mm Al in both groups (mean T-scores <-2.5)
• 45 mg daily menatrenone (vitamin K2) vs. no treatment x 12m
• Bone loss:– Change in 2nd metacarpal BMD (mm Al, CXD)
• +0.9% menatrenone grp v. -4.3% no treatment grp (p<.0001)
• Fractures:– 1 (1 hip) menatrenone grp vs. 10 (8 hip) no treatment
grp (p=.0082)
Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
Amelioration of osteopenia and hypovitaminosis D by 1-alpha-
hydroxyvitamin D3 in elderly patients with Parkinson’s disease.
Sato Y, et al. J Neurol Neurosurg Psychiatry 1999;66:64.
• Placebo-controlled, double-blind RCT• 86 Japanese PD patients (mean 71y; 51 women)
– Exclusions: nonvertebral fx, recent or regular use of bone active meds, known cause of osteoporosis
– Mean baseline BMD 2.0-2.1 mm Al in both groups (mean T-score <-2.5 vs. normal Japanese ref range)
• 1 mcg vit D vs. placebo daily x 18m• Bone loss:
– Change in 2nd metacarpal BMD (mm Al, computed radiographic densitometry, i.e. CXD)
• -1.2% vit D grp v. -6.7% placebo grp (p<.0001)
• Fractures:– 1 (1 hip) vit D grp vs. 8 (6 hip) placebo grp
(p=.0028)

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
Alendronate and vitamin D2 for prevention of hip fracture in Parkinson’s Disease: a
randomized controlled trial. Sato Y, et al. Movement Disorders 2006;21:924.
• Placebo-controlled, double-blind RCT• 288 Japanese female PD patients aged >65y (mean 72y)
– Exclusions: nonvertebral fx, recent or regular use of bone active meds, known cause of osteoporosis
– Mean baseline BMD 2.1-2.2 mm Al in both groups (mean T-score <-2.5)
– 5 mg alendronate + 1000 IU ergocalciferol vs. placebo + 1000 IU ergocalciferol daily x 24m
• Bone loss:– Change in 2nd metacarpal BMD (mm Al, CXD)
• +3.1% alendronate grp vs. -2.8% placebo grp (p<.001)
• Hip fractures:– 4 alendronate grp vs. 14 placebo grp (RR 0.29,
95%CI=0.10-0.85)

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
Risedronate and ergocalciferol prevent hip fracture in elderly men with Parkinson’s
Disease. Sato Y, et al. Neurology 2007;68:911.
• Placebo-controlled, double-blind RCT• 242 Japanese male PD patients aged >65y (mean 72y)
– Exclusions: nonvertebral fx, recent or regular use of bone active meds, known cause of osteoporosis
– Mean baseline BMD 2.25 mm Al in both groups (mean T-score <-2.5)
– 2.5 mg risedronate + 1000 IU ergocalciferol vs. placebo + 1000 IU ergocalciferol daily x 24m
• Bone loss:– Change in 2nd metacarpal BMD (mm Al, CXD)
• +2.2% risedronate grp v. -2.9% placebo grp (p<.001)
• Hip fractures:– 3 risedronate grp vs. 9 placebo grp (RR 0.33,
95%CI=0.09-1.20)

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
What to Do: Clinical?What to Do: Clinical?
• Treat PD patients to reduce bone loss, prevent fractures?– Trials suggest that supplemental vit D and vit
K2 each reduce bone loss, and that alendronate and risedronate each prevent hip fracture
– All published trials from single investigator in Japanese osteoporotic patients with PD; generalizability to other osteoporotic PD populations unknown
– There is no evidence yet that osteoporosis-specific treatments reduce bone loss and prevent hip fractures in PD patients without osteoporosis.

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
What to Do: Clinical?What to Do: Clinical?
• Screen PD patients for osteoporosis?– Though at increased risk for osteoporosis,
accelerated bone loss, falls, and fractures, patients with PD are infrequently screened for osteoporosis1
– There is no direct evidence on the cost-effectiveness of screening this population for osteoporosis, but demonstrating this will be difficult
– Recommendation: In addition to implementing fall prevention measures, clinicians should consider osteoporosis screening in older patients with PD
1Eng ML, Mov Disord 2006;21:2265-66
Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
What to Do: Research?What to Do: Research?• Examine PD-bone loss association in larger PD
populations, including evaluation of RF for bone loss in PD patients
• RCT to examine whether PD-specific treatment reduces BMD loss, falls & fractures
• RCT to examine whether osteoporosis-specific treatment reduces BMD loss & fractures in nonosteoporotic PD patients
• RCT to examine whether vitamin D and/or estrogen improve PD symptoms
• Consider inclusion of PD as RF in absolute fracture risk models to be utilized for BMD screening, fracture prevention decisions

Howard Fink, MD, MPHMinneapolis VA Medicine Research ConferenceJanuary 22, 2009
Contact Information• For information about this specific presentation
please contact Howard Fink, MD, MPH at [email protected]
• For any questions about the monthly GRECC Audio Conference Series please contact Tim Foley at [email protected] or call (734) 222-4328
• For the link to the evaluation form for this conference that will confer CE credit please go to http://vaww.sites.lrn.va.gov/vacatalog/cu_detail.asp?id=24985 and click the “Handout: Registration and Evaluation” link