how much vector control is needed to achieve malaria elimination?
TRANSCRIPT

Opinion
How much vector control is needed toachieve malaria elimination?Jill N. Ulrich1, Diana P. Naranjo2, Temitope O. Alimi1, Gunter C. Muller3, andJohn C. Beier1,4
1 Leonard and Jayne Abess Center for Ecosystem Science and Policy, University of Miami, Coral Gables, FL, 33146, USA2 MAIA Program, College of Arts and Sciences, University of Miami, Coral Gables, FL, 33146, USA3 Department of Parasitology, Kuvin Center for the Study of Tropical and Infectious Diseases, Hadassah Medical School,
Hebrew University, Jerusalem, 91120, Israel4 Department of Epidemiology and Public Health, University of Miami Miller School of Medicine, Miami, FL, 33136, USA
Roll Back Malaria’s ambitious goals for global malariareduction by 2015 represent a dilemma for NationalMalaria Control Programs (NMCPs) that are still far frommalaria elimination. Current vector control efforts byNMCPs generally fall short of their potential, leavingmany NMCPs wondering how much vector control itwill take to achieve malaria elimination. We believe theanswer is detailed in the relationships between theentomological inoculation rate (EIR) and four epidemio-logical measures of malaria in humans. To achieve ade-quate vector control, NMCPs must evaluate EIRs toidentify problematic foci of transmission and reduceannual EIRs to less than one infectious bite per person.
New goals for malaria eliminationDuring the first decade of Roll Back Malaria (2000–2010),many NMCPs quickly scaled up malaria control interven-tions and successfully curtailed transmission. According tocase reports, the estimated global incidence of malaria fellby 17% between 2000 and 2010 [1]. These accomplish-ments were made possible by considerable public interest,leadership of international agencies, and major fundingorganizations [2,3], as well as by impressive dedication ofNMCPs. Also in the past decade, 42 malaria-endemiccountries increased their per capita spending by US$1000, thereby increasing the availability of domesticfunds for mosquito control. The WHO estimates that ifjust 1% of total domestic spending were allocated to ma-laria control, 75 of the 99 countries with ongoing malariatransmission could provide an insecticide-treated net(ITN) to each at-risk person. In 2010, 27 countries in theAfrican Region and 42 in other WHO regions made thecommitment to do so [1].
Inspired by a decade of achievements and renewedcommitments by malaria-endemic nations, Roll BackMalaria’s 2011 Global Malaria Action Plan includes ambi-tious new targets. By the end of 2015, we hope to have: (i)reduced global malaria deaths to near zero; (ii) reducedglobalmalaria cases by 75%; and (iii) eliminatedmalaria inat least eight to ten new countries [4]. Elimination remainsa distant goal for many nations, including India, Pakistan,Brazil, Colombia, Papua New Guinea, and most of Africa
Corresponding author: Ulrich, J.N. ([email protected]).
104 1471-4922/$ – see front matter � 2013 Elsevier Ltd. All rights reserved. htt
[1]. In these settings, new vector control tools and strate-gies are needed for malaria elimination [5,6], but scale-upsare unlikely given the funding outlook for the next fewyears [1]. Instead of implementing expensive nation-widescale-ups, NMCPs can rely on ‘lessons learned’ in vectorcontrol to consider how to adapt and improve strategies forelimination.
Reliance on vector control has been at the heart of suc-cessful reductions of malaria achieved on a global scale [7].In areas of high transmission, long-lasting insecticide-trea-tednets (LLINs) can reducemalaria incidenceby50%and inareas of low transmission, by 62% [8]. Indoor residualspraying (IRS) has been equally effective, reducing inci-dence by 57% in children under five in an area of hightransmission in Tanzania [9] and by 90–95% in an area oflow transmission in Pakistan [10]. A recent meta-analysisshows that IRS is capable of reducing prevalence by 62%[11]. Although there is limited evidence on the combinedimpact of LLINs and IRS, it is thought that there areadditive effects [12]. The tools of LLINs and IRS alonecan drivemalaria rates down to the point where concurrentefforts can be taken to eliminatemalaria parasite reservoirsof infection [3]. However, increasing insecticide resistancealong with environmental and health concerns demand thedevelopment and adoption of viable alternative methods.Integrated Vector Management (IVM) therefore promotesthe synergistic application of different interventions as wellas effective collaboration within the health sector and withother public sectors in order to best reduce transmission[13]. An IVM-based approach promises struggling NMCPscost effectiveness, monitoring of impact on vector popula-tions and pathogen transmission, sustainability and com-patibility with local health systems but demands moreeffective planning and decision making at the lowest possi-ble administrative levels [14]. This article highlights, sim-plifies, and provides practical guidance for NMCPsaddressing the important issue of how much vector controlis needed to achieve malaria elimination.
Vector control strategies must be targeted andevidence basedMalaria is highly related to environmental characteristicsthat delineate foci of transmission. Therefore, identification
p://dx.doi.org/10.1016/j.pt.2013.01.002 Trends in Parasitology, March 2013, Vol. 29, No. 3

Opinion Trends in Parasitology March 2013, Vol. 29, No. 3
of high transmission areas, use of geographical informationsystems, and statistical analysis tied in with entomologicalsurveillance [15] can scale the type and intensity of inter-ventions and cost effectively reduce the burden of the dis-ease. Using transmission as a measure of malaria risk,NMCPs can see that current vector control tools can de-crease pathogen transmission in low to moderate transmis-sion settings; however, additional strategies are needed toreduce malaria prevalence in high transmission areas [16].Such targeted strategies are cost effective and can curtailmalaria effectively on a national scale.
The recent success of Turkey is an example of effectivelytargeted vector control strategies. Several studies wereconducted in Turkey to target malaria control efforts,revealing that: (i) Plasmodium vivax is the only speciesfrom autochthonous cases; (ii) Anopheles sachavori is themost prominent vector; (iii) larvae of this vector are mostabundant in June; (iv) the vector is 95% zoophilic and bitesmostly at night; (v) September is the month of highestmalaria transmission; and (vi) most transmission is con-centrated in the Southeastern Anatolia Region. Interven-tions for vector control in Turkey are planned using thesestudies along with regular assessments in high-risk pro-vinces and are grounded in the principles of IVM. Allavailable and effective measures, including indoor residualspraying, larval control activities, and spray spacing, areintegrated and applied to areas of high transmission. Focalspraying is carried out whenever a new malaria case isdetected during the period of active malaria transmission.At the same time, environmental management includingdrainage, filling, intermittent irrigation of fields, andplanting eucalyptus trees for drying land with a high watertable, etc., is applied in selected regions. Turkey’s MalariaControl Program, which began in 1983, brought the num-ber of malaria cases down from 66 681 in 1983 to just 84 in2006. The programwas so successful that it led to Turkey’stransition to the elimination phase in 2010 [17].
Robustmonitoring and evaluation systems are essentialto targeted vector control strategies and thus to malariaelimination. Standard monitoring of progress in vectorcontrol is usually measured in terms of household coverageof LLINs and/or IRS and by health system indicators ofhow many cases of malaria and how many deaths due tomalaria. However, for countries transitioning from controlto elimination efforts, measures of impact should shift infocus from coverage and health system indicators to infec-tion and transmission. As transmission intensity drops tonear-elimination levels, standard monitoring and evalua-tion programs should expand to include surveillance activ-ities, marked by active case detection, parasitologicalexamination, antimalarial drug treatment, epidemiologi-cal investigation, entomological investigation, eliminationof foci, and case and community follow-up [18].
Accurate metrics of transmission are the evidence baseof effectively targeted vector control. Annual case incidenceand prevalence are two commonly used metrics, but theyare problematic for several reasons. To measure incidenceaccurately, all cases in the population must be identifiedthrough both passive and active detection, as passivedetection alone results in estimates that are too low.Individuals with asymptomatic infections are often not
accounted for in incidence measures; however, they con-tinue to be reservoirs for transmission. Prevalence relieson probability sampling of the population, which is prob-lematic because often transmission occurs in nonrandomfoci of cases. Unless extremely large sample sizes are used,prevalence provides imprecise measures at low levels oftransmission [18]. These vague metrics often lead to con-flicting evidence. For example, in Zambia a study showedthat following diagnosed clinical cases back to their home-stead lead to clusters of asymptomatic cases during the lowtransmission season. Simultaneously in a randommalariasurvey, such clustering was not seen [19]. NMCPs shouldbe cautious when using incidence and prevalence alone fortargeted vector control efforts, given that their focus is noton the vectors themselves.
The EIR, which estimates an individual’s level of expo-sure toPlasmodium falciparum-infectedmosquitoes, is themost useful measure for estimating malaria transmissionintensity. It can be used to indicate the proportion ofhumans infected at any given time and to predict thespread of malaria to uninfected individuals, elements thatare crucial to modelingmalaria transmission [20]. The EIRis the product of the human biting rate (the number of bitesper person per day by vector mosquitoes) and the sporozo-ite rate, the fraction of vector mosquitoes that are infec-tious [21]. There are no underlying assumptions for eitherof these two empirical components. The lack of uniformityin EIR measurement methods [22] – human bait collec-tions (HBCs), pyrethrum spray catches (PSCs), light traps,and window exit traps to determine the human biting rate;dissection of mosquito salivary glands, enzyme-linked im-munosorbent assays (ELISAs) and PCR-based methods todetermine the sporozoite rate – has often been cited as aweakness of the metric [23]. However, the variety of meth-odological approaches to the EIR offers flexibility, especial-ly for countries with limited human and financial resourcesto conduct the surveys. For example, the HBC and sporo-zoite dissection techniques are labor intensive and areoften replaced with quicker and simpler combinations ofPSCs, light traps, ELISA, and PCR [23]. All NMCPs mustdetermine which methods best suit their logistic situa-tions, the important point being that the collection meth-ods be standardized within each nation.
The relationships between the EIR and other epidemio-logical metrics show why the EIR is the most usefulmeasure for focusing vector interventions on the areas ofhighest transmission (Figure 1). First, there is a nearlinear relationship between EIRs and malaria incidence(Figure 1a) [24–26]. Whereas malaria incidence only takesinto account detected or reported cases, the EIR measurestransmission regardless of clinical outcomes, thereby mak-ing it a slightly better predictor of infection. Not surpris-ingly, if vector control efforts focus on reducing EIRs, theincidence will also decrease. Second, even with annualEIRs <5 per person, prevalence rates can range anywherefrom 1% to 60% (Figure 1b) [25,27–29]. If annual EIRs arenot decreased to less than one, prevalence will generallyremain unaffected even with extensive progress in vectorcontrol. Third, annual EIRs of only a few infective bites canbe associated with high annual incidence rates of severedisease (Figure 1c) [8,30–34]. As a result, incidence of
105

[(Figure_1)TD$FIG]
The more infec�ve bites, the more people contract malariaeach year.
Seasonal high exposure to many infec�ve bitesincreases parasite numbers in the blood.
Even with just a few infec�ve bites, many people s�llcontract severe malaria.
Even with just a few infec�ve bites, most people s�llhave malaria.
(a)
<35 days>35 daysKey:
Number of infec�ve bite exposures
Geom
etric
mea
n pa
rasit
emia
Annual EIR
(b)
(c) (d)
EIR
A�ac
k ra
te in
chi
ldre
n (In
cide
nce)
Sites
Annual infec�ve bites /person
EIR
Incidence of severe malaria
Rates per 1000 children
Mal
aria
pre
vale
nce
%
MU
<60
200400600800
1000120014001600
6 – 11 12 – 23 24 – 47 >48
0
10
20
30
40
50
010203040506070
0.000.0 0.5 1.0 1.5 2.0
0.02
0.04
0.06
0.08
0.10
FB KB ZW KW MK UF KY MT
00 150 300 600 750
20
40
60
80
100
450
TRENDS in Parasitology
Figure 1. Epidemiological–entomological relationships. (a) The relationship between the entomological inoculation rate (EIR) and Plasmodium falciparum malaria
incidence as calculated in children in Saradidi, Kenya, during 39 two-week periods when EIRs were <1.7 [24]. (b) The relationship between annual EIR and prevalence of P.
falciparum malaria based on data obtained from 31 sites throughout Africa [27]. (c) The relationship between annual EIR and the incidence of severe malaria infections in
children at nine sites in Kilifi District, Kenya: Mukombe, Fumbini, Kiberani, Zowerani, Kambi ya Wari, Mikingirini, Ufuoni, Kaoyeni, and Mtondia [32]. (d) Dose- and time-
dependent relations between EIR and P. falciparum parasitemia among children of three different ages from the same village (Got Onyango) of western Kenya [35].
Opinion Trends in Parasitology March 2013, Vol. 29, No. 3
severe disease and thus the malaria mortality rate willremain high even after extensive vector control, and so itmay appear as if the vector control is fruitless if EIRs arenot measured. Fourth, above a certain EIR thresholdinfected individuals are at greater risk of a high parasitedensity in the blood (Figure 1d) [35,36], which indicates ahigh degree of active malaria infection. Consequently, byconcentrating on reducing annual EIRs, NMCPs will see adrop in parasitemia levels and fewer individuals withactive infections. The EIR is the only metric sensitiveenough to detect the differences in transmission in thefinal steps towards malaria elimination.
106
There is an important lesson in the relationships be-tween the EIR and other epidemiological measures: localmalaria elimination can only be achieved if strategies formalaria elimination at the country level aim to reduceannual EIRs to levels below one infective bite per person.Because transmission is very efficient even at low levels,decreases in EIRs through vector control may not affect theincidence of severe disease or malaria prevalence unlessEIRs are reduced to levels below one infective bite perperson per year. Hence, NMCPs hoping to close the gapbetween control and elimination should shift their focus ofmonitoring to measuring the EIR. Unfortunately, most
Opinion Trends in Parasitology March 2013, Vol. 29, No. 3
NMCPs have yet to embrace this useful metric. In mostLatin American countries, transmission is considered toolow for NMCPs to invest in monitoring EIRs [37]. Even inAfrica, where there are clusters of alarmingly high trans-mission, the EIR is rarely recorded [38]. Although the
[(Figure_2)TD$FIG]
Establish a structure for
Invest in capac
Iden�fy foci of hig
Conduct entomol
Incorporate EIR measurement into m
Strengthen tools for integrated vector mless than
Con�nue surveillance
Malaria task force forpolicy oversight
Technical sub-commi�eesguided by experts
EIR methods and ac�vecase detec�on for
community workers
Inves�ga�on and mappingof passively and ac�vely
detected casesEIR studies at posts
throughout the country
Vector species and theirdistribu�ons
Popula�on gene�cs,seasonal densi�es, and
vectorial capaci�es
Frequent na�onal EIRstudies
If EIR> 1, weekly caserepor�ng and monthly EIR
studies
Technical commi�ee onvector control
Regional entomologyteams for planning ofregional interven�ons
Con�nued financialsupport for elimina�on
ac�vi�esRigorous ac�ve case
detec�on
Accurate diagnosis andcase confirma�on for
doctors
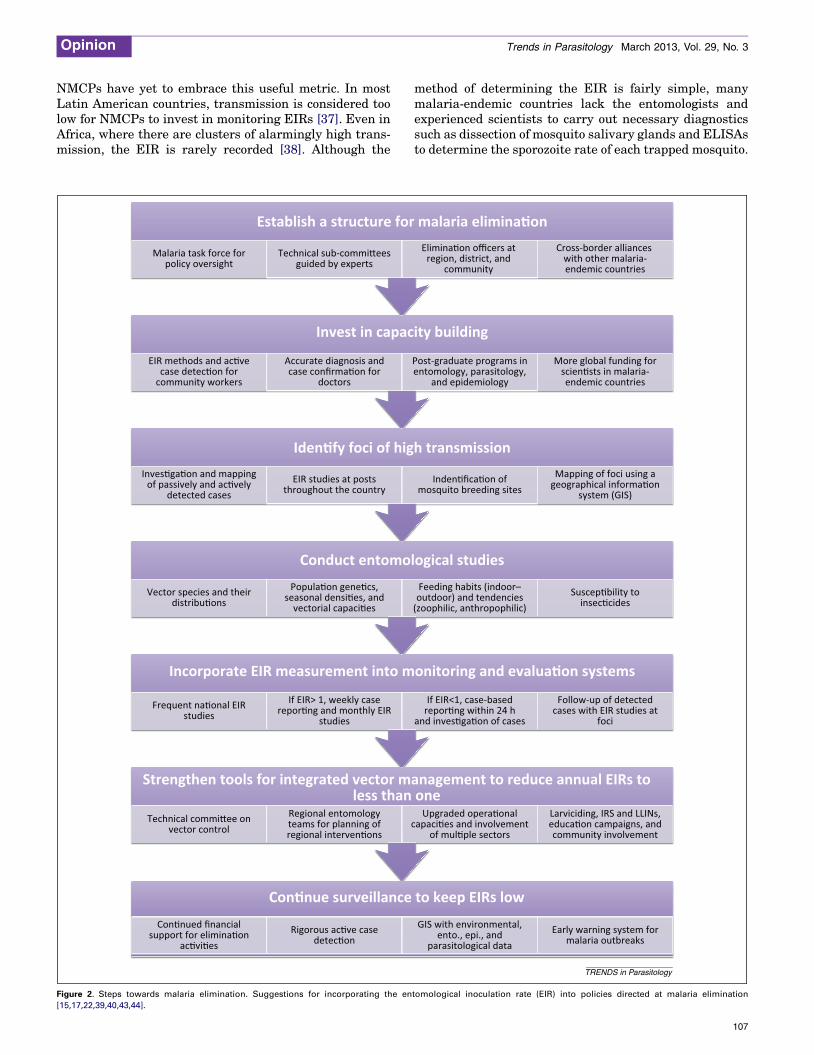
Figure 2. Steps towards malaria elimination. Suggestions for incorporating the en
[15,17,22,39,40,43,44].
method of determining the EIR is fairly simple, manymalaria-endemic countries lack the entomologists andexperienced scientists to carry out necessary diagnosticssuch as dissection of mosquito salivary glands and ELISAsto determine the sporozoite rate of each trapped mosquito.
malaria elimina�on
ity building
h transmission
ogical studies
onitoring and evalua�on systems
anagement to reduce annual EIRs to one
to keep EIRs low
Elimina�on officers at region, district, and
community
Cross-border alliances with other malaria-endemic countries
Inden�fica�on ofmosquito breeding sites
Mapping of foci using ageographical informa�on
system (GIS)
Feeding habits (indoor–outdoor) and tendencies
(zoophilic, anthropophilic)Suscep�bility to
insec�cides
If EIR<1, case-basedrepor�ng within 24 h
and inves�ga�on of cases
Follow-up of detectedcases with EIR studies at
foci
Upgraded opera�onalcapaci�es and involvement
of mul�ple sectors
Larviciding, IRS and LLINs,educa�on campaigns, andcommunity involvement
GIS with environmental,ento., epi., and
parasitological dataEarly warning system for
malaria outbreaks
Post-graduate programs inentomology, parasitology,
and epidemiology
More global funding forscien�sts in malaria-endemic countries
TRENDS in Parasitology
tomological inoculation rate (EIR) into policies directed at malaria elimination
107

Opinion Trends in Parasitology March 2013, Vol. 29, No. 3
The need to train African scientists in malaria research isrecognized [39]. If progress is to be made towards RollBack Malaria’s goals for 2015, we must address the chal-lenges facing the scientific community inmalaria-endemiccountries [40].
Guiding malaria elimination with the EIRThe targets set forth in Roll Back Malaria’s 2011 GlobalMalaria Action Plan are achievable, but only if NMCPs actnow to target vector control strategies by effectively mea-suring transmission. A successful tool for malaria elimina-tion in the past has been vector control, but now manyNMCPs are finding that even ‘tried-and-true’ vector controlstrategies that have been so effective in other countries donot achieve the results they desire locally. It is important toremember that all global policies on vector control must beadapted to local conditions and available resources. Incontrast to some of the generic vector policy recommenda-tions of the past, IVM recognizes this need: ‘Becausealmost every situation is distinct and complex, it is impos-sible to prescribe standard actions and strategies’ [13].Analysis of the problems and constraints in a local vectorcontrol system is imperative to its success [41]. Local andregional vector control programs can benefit from surveil-lance that produces epidemiological stratification of site-specific situations in order to better address local needs[42]. Instead of prescribing ‘blanket’ approaches that arebound to be ineffective or attempting to predict regionaland local needs, IVM emphasizes capacity building so thatNMCPs can use their own surveillance, analysis, andadaptive management to make the appropriate decisionsfor local circumstances.
Beyond cultivating local decision making to tailor ge-neric policies, vector control can be improved throughbetter assessments of pathogen transmission. This entailsthat EIRs be estimated for both areas of low and hightransmission and that control efforts be targeted based onthese estimates. It also requires an overhaul of the evalu-ating and monitoring systems to ensure that NMCPs keeptrack of their progress and make strategic plans to tackleproblem areas and to train native scientists in malaria-endemic areas. In order forNMCPs to determine howmuchvector control is needed to eliminate malaria in theircountries and to make progress towards elimination, wesuggest that they take the steps summarized in Figure 2.The incorporation of these initiatives into malaria elimi-nation policies of NMCPs can bring Rollback Malaria’sgoals within closer reach.
AcknowledgmentThis research was supported by grant R01 GM093345 from the NationalInstitutes of Health.
References1 World Health Organization (2011) World Malaria Report 2011, World
Health Organization2 Feachem, R. et al. (2010) Shrinking the malaria map: progress and
prospects. Lancet 376, 1566–15783 Campbell, C. and Steketee, R. (2011) Malaria in Africa can be
eliminated. Am. J. Trop. Med. Hyg. 85, 584–5854 Roll Back Malaria Partnership (2011) A Decade of Partnerships and
Results, World Health Organization
108
5 The malERA Consultative Group on Vector Control (2011) Aresearch agenda for malaria eradication: vector control. PLoS Med.8, e1000401
6 Greenwood, B. (2010) Anti-malarial drugs and the prevention ofmalaria in the population of malaria endemic areas. Malaria J. 9, S2
7 Barat, L. (2006) Four malaria success stories: how malaria burden wassuccessfully reduced in Brazil, Eritrea, India, and Vietnam. Am. J.Trop. Med. Hyg. 74, 12–16
8 Lengeler, C. (2004) Insecticide-treated bed nets and curtains forpreventing malaria. Cochrane Database Syst. Rev. 2, CD000363
9 Curtis, C. (1999) Malaria control: bednets or spraying? Backgroundtrial in Tanzania. Trans. R. Soc. Trop. Med. Hyg. 93, 453–454
10 Rowland, M. et al. (2000) Indoor residual spraying withalphacypermethrin controls malaria in Pakistan: a community-randomized trial. Trop. Med. Int. Health 5, 472–481
11 Kim, D. et al. (2012) Reduction ofmalaria prevalence by indoor residualspraying: a meta-regression analysis. Am. J. Trop. Med. Hyg. 87,117–124
12 Pluess, B. et al. (2010) Indoor residual spraying for preventingmalaria.Cochrane Database Syst. Rev. 4, CD006657
13 World Health Organization (2012) Handbook for Integrated VectorManagement, World Health Organization
14 World Health Organization (2004) Global Strategic Framework forIntegrated Vector Management, World Health Organization
15 Moonen, B. et al. (2010) Operational strategies to achieve andmaintainmalaria elimination. Lancet 376, 6–12
16 Griffin, J. et al. (2010) Reducing Plasmodium falciparum malariatransmission in Africa: a model-based evaluation of interventionstrategies. PLoS Med. 7, 8
17 Ozbilgin, A. et al. (2012) Malaria in Turkey: successful control andstrategies for achieving elimination. Acta Trop. 120, 15–23
18 The malERA Consultative Group on Monitoring, Evaluation, andSurveillance (2011) A research agenda for malaria eradication:monitoring, evaluation, and surveillance. PLoS Med. 8, e1000400
19 Shiff, C. et al. (2011) Designing a sustainable strategy for malariacontrol? Malaria J. 10, 220
20 MacDonald, G. (1957) The Epidemiology and Control of Malaria,Oxford University Press
21 Birley, M. and Charlewood, J. (1987) Sporozoite rate and malariaprevalence. Parasitol. Today 3, 231–232
22 Hay, S. et al. (2000) Annual Plasmodium falciparum entomologicalinoculation rates (EIR) across Africa: literature survey, internet accessand review. Trans. R. Soc. Trop. Med. Hyg. 94, 113–127
23 Kelly-Hope, L. and McKenzie, F. (2009) The multiplicity of malariatransmission: a review of entomological inoculation ratemeasurements and methods across sub-Saharan Africa. Malaria J.8, 19
24 Beier, J. et al. (1994) Plasmodium falciparum incidence relative toentomological inoculation rates at a site proposed for testing malariavaccines in western Kenya. Am. J. Trop. Med. Hyg. 49, 529–536
25 Elissa, N. et al. (2003) Relationship between entomological inoculationrate, Plasmodium falciparum prevalence rate, and incidence ofmalaria attack in rural Gabon. Acta Trop. 85, 355–361
26 Maxwell, C. et al. (2003) Variation of malaria transmission andmorbidity with altitude in Tanzania and with introduction ofalphacypermethrin treated nets. Malaria J. 2, 28
27 Beier, J. et al. (1999) Entomological inoculation rates and Plasmodiumfalciparum malaria prevalence in Africa. Am. J. Trop. Med. Hyg. 61,109–113
28 Smith, D. and McKenzie, F. (2004) Statics and dynamics of malariainfection in Anopheles mosquitoes. Malaria J. 3, 13
29 Smith, D. et al. (2005) The entomological inoculation rate andPlasmodium falciparum infection in African children. Nature 438,492–495
30 Trape, J. et al. (1987) Malaria and urbanization in Central Africa: theexample of Brazzaville. Part V: pernicious attacks and mortality.Trans. R. Soc. Trop. Med. Hyg. 81, 34–42
31 Snow, R. et al. (1994) Severe childhood malaria in two areas ofmarkedly different falciparum transmission in East Africa. ActaTrop. 57, 289–300
32 Mbogo, C. et al. (1995) Relationships between Plasmodium falciparumtransmission by vector populations and the incidence of severe diseaseat nine sites on the Kenyan coast. Am. J. Trop. Med. Hyg. 52, 201–206

Opinion Trends in Parasitology March 2013, Vol. 29, No. 3
33 Snow, R. et al. (1997) Relation between severe malaria morbidity inchildren and level of Plasmodium falciparum transmission in Africa.Lancet 349, 1650–1654
34 Okiro, E.A. et al. (2009) Age patterns of severe paediatric malaria andtheir relationship to Plasmodium falciparum intensity.Malaria J. 8, 4
35 McElroy, P. et al. (1997) Dose and time-dependent relationshipsbetween exposure to infective inoculation and Plasmodiumfalciparum infection among children in western Kenya. Am. J.Epidemiol. 145, 945–956
36 Ellman, R. et al. (1998) Malaria and anaemia at different altitudes inthe Muheza district of Tanzania: childhood morbidity in relation tolevel of exposure to infection. Ann. Trop. Med. Parasitol. 92, 741–753
37 Arevalo-Herrera, M. et al. (2012) Malaria in selected non-Amazoniancountries of Latin America. Acta Trop. 121, 303–314
38 Hay, S. et al. (2005) Urbanization, malaria transmission, and diseaseburden in Africa. Nat. Rev. Microbiol. 3, 81–90
39 Greenwood, B. et al. (2012) The Gates Malaria Partnership: aconsortium approach to malaria research and capacity development.Trop. Med. Int. Health 17, 558–563
40 Ntoumi, F. and Priebe, G. (2010) Africanizing scientific knowledge: themultilateral initiative onmalaria as amodel?Malaria J. 9 (Suppl. 3), S7
41 Van denBerg, H. et al. (2012)Guidance on Policy-making for IntegratedVector Management, World Health Organization
42 Impoinvil, D. et al. (2007) Comparison of mosquito control programs inseven urban sites in Africa, the Middle East, and the Americas.HealthPolicy 83, 196–212
43 Namibia Ministry of Health and Social Services (2010) MalariaStrategic Plan (2010–2016), Namibia Ministry of Health and SocialServices
44 The malERA Consultative Group on Integration Strategies (2011) Aresearch agenda for malaria eradication: cross-cutting issues foreradication. PLoS Med. 8, e1000404
109