how i manage gut symptoms in patients with diabetes
TRANSCRIPT

How I manage gut symptoms in patients with diabetes
Dr John S LeedsConsultant Gastroenterologist & Associate Senior
Lecturer
Freeman Hospital & University of Newcastle Upon Tyne

Outline
GI symptoms in diabetes
Investigations in diabetes
Management in diabetes

Introduction
Intensive glycaemic control is the cornerstone of management1
Reduced morbidity and mortality1,2
Other medical conditions can contribute3
1 The DCCT research group. NEJM 1993;329(14):977-986.2 Tesfaye S et al. EURODIAB IDDM Complications Study. Diabetologia 1996;39:1377-84.3 Tesfaye S et al. EURODIAB Prospective Complications Study. NEJM 2005;352:341-50.

IntroductionDiabetes and the GI tract associated in 19361
More common in male, type 1 patients of increasing duration
“Diabetic diarrhoea”
No large prevalence studies in patients with Type 1 diabetes mellitus.2
1 Bargen JA. Mayo Clinic Proc 1936;2:737.2 Bytzer P. Arch Intern Med 2001;161:1989–1996.

IssuesMechanisms uncertain
Helicobacter pylori infectionPsychological factorsImpaired sensory functionDisordered motor function resulting from autonomic neuropathyAbnormal blood glucose levels
Acute changes in blood glucose concentrations (independent of neuropathy) can effect motor function and modulate perception of sensations from the GI tract
Diabetes and GI associationsCoeliac diseaseSmall bowel bacterial overgrowthExocrine pancreatic insufficiencyThyroid dysfunctionAutonomic neuropathy?IBDMedications
What is the size of this problem...?
Previous study
1 study of gastrointestinal symptoms in people with Type 1 diabetes:Postal survey of 15,000 people.60% response rate.Only 27 subjects having Type 1 diabetes.Symptoms/glycaemic control self reported.No investigations performed
Bytzer P et al. Prevalence of gastrointestinal symptoms associated with diabetes mellitus:a population-based survey of 15,000 adults. Arch Intern Med 2001;161:1989–1996.

Sheffield studyPatients recruited from Sheffield Diabetes Centre (≈2000 Type 1 DM)
Type 1 if presented at early age, with DKA or progressed to insulin in <1 year
>95% Type 1 DM managed by secondary care
Recruited when attending for annual review, foot clinic or DAFNE clinic
MethodsRoutine bloods (including lipids and LFT’s)Endomyseal antibody (IgA)Anti-tissue transglutaminase antibody (IgA)Total IgA levelGastrointestinal symptom questionnaireShort Form-36v2 quality of life assessment toolHbA1c
Urinary ACRPositive antibody or IgA deficiency offered duodenal biopsy
GI symptoms
440/706 (62.3%, CI 58.6 - 65.9) T1DM had GI symptoms
284/604 (47.0%, CI 42.9 - 51.1) controls had GI symptoms
OR 1.9 (1.5–2.3, p<0.0001)
Leeds JS, Hadjivassiliou M, Tesfaye S, Sanders DS. Lower gastrointestinal symptoms are associated with worse glycemic control and quality of life in type 1 diabetes mellitus. BMJ Open Diabetes Res Care. 2018 May 29;6(1):e000514
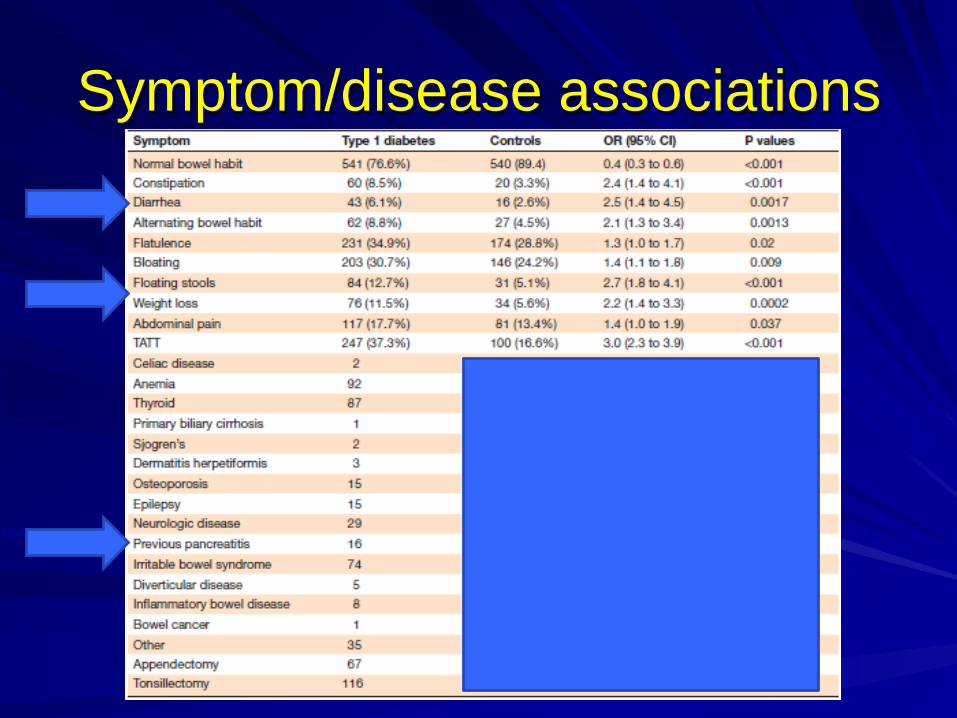
Symptom/disease associations

Symptom burden
Type 1 DM increased prevalence of >2 GI symptoms

Glycaemic control
Symptom Symptomatic T1DM HbA1c T1DM control HbA1c p
Diarrhoea 8.2% (66 mmol/mol) 7.3% (56mmol/mol) <0.001
Constipation 8.2% (66 mmol/mol) 7.9% (62 mmol/mol) 0.45
Alternating 8.5% (69 mmol/mol) 7.9% (62 mmol.mol) <0.001
Abdo pain 8.25% (67 mmol/mol) 7.7% (61 mmol/mol) 0.0021

Quality of life
Diarrhoea patients investigated
102 individuals with diarrhoea offered94 agreed to investigationsCoeliac screen, IgAFaecal elastase-1IleocolonoscopyGlucose hydrogen breath testAutonomic testing
What should we look for?
Coeliac diseaseIBSPancreatic exocrine insufficiencyIBDAutonomic neuropathy/SBBOCancer

T1DM and coeliac diseaseAuthor Country N Antibody panel Known CD (n) New CD (n) Prevalence (95%
CI)
Collin, (1989) Finland 195 AGA, ARA 0 8 4.1 (2.1 – 8.6)
Page, (1994) UK 767 AGA 0 14 1.8 (1.0 – 3.0)
Sategna-Guidetti, (1994) Italy 383 EMA 0 10 2.6 (1.3 – 4.8)
Rensch, (1996) USA 47 EMA 0 3 6.4 (1.3 – 17.5)
De Vitis, (1996) Italy 1114 AGA, EMA 0 63 5.7 (4.4 – 7.2)
Cronin, (1997) Ireland 101 EMA 0 5 4.9 (1.6 – 11.2)
Talal, (1997) USA 185 EMA 0 4 2.2 (0.6 – 5.4)
Sjöberg, (1998) Sweden 848 AGA, EMA 8 14 2.6 (1.6 – 3.9)
Guvenc, (2002) Turkey 100 EMA 0 6 6.0 (2.2 – 12.6)
Mahmud, (2005) USA 158 EMA, tTG 0 11 6.9 (3.5 – 12.1)
Doolan, (2005) Australia 131 EMA, tTG 0 11 8.4 (4.3 – 14.5)
Picarelli, (2005) Italy 94 EMA 0 6 6.4 (2.4 – 13.4)
Aygun, (2005) Turkey 122 EMA 0 3 2.5 (0.5 – 7.0)
Buysschaert, (2005) Belgium 400 EMA, tTG 0 10 2.5 (1.2 – 4.6)
Walter, (2007) Canada 124 tTG 3 7 8.1 (3.9 – 14.3)
Remes-Troche (2008) Mexico 84 tTG 0 5 5.9 (1.9 – 13.3)
TOTAL 4853 11 180 3.7 (3.2 – 4.3)
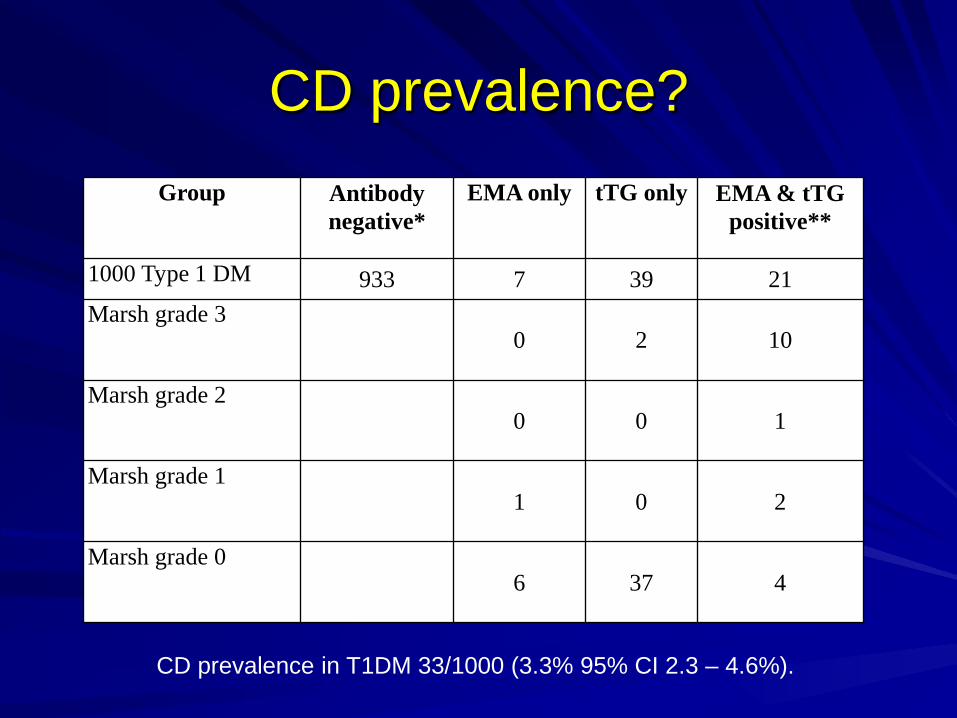
CD prevalence?Group Antibody
negative*EMA only tTG only EMA & tTG
positive**
1000 Type 1 DM 933 7 39 21Marsh grade 3
0 2 10
Marsh grade 20 0 1
Marsh grade 11 0 2
Marsh grade 06 37 4
CD prevalence in T1DM 33/1000 (3.3% 95% CI 2.3 – 4.6%).

Antibody performanceAntibody Sensitivity (%) Specificity (%) PPV NPV
IgG AGA 33.3 98.7 0.46 0.98
IgA AGA 50 95.34 0.27 0.98
EMA 83.3 98.2 0.61 0.99
tTG 100 95.2 0.41 1.0
EMA & tTG 83.3 99.1 0.76 0.99

Does CD affect T1DM?
Leeds JS, Hopper AD, Hadjivassiliou M, Tesfaye S, Sanders DS. High prevalence of microvascular complications in adults with type 1diabetes and newly diagnosed celiac disease. Diabetes Care. 2011 Oct;34(10):2158-63.

Potential CD and diabetes
CD is associated with neurological issuesCombination of CD and T1DM adds risk
Is enteropathy needed?Is there immunological pathophysiology?
Potential CD and T1DM
4 groups recruited:
DM potential CDCDDMT1DM onlyCD only

Potential CD and T1DM
Leeds JS, Hopper AD, Hadjivassiliou M, Tesfaye S, Sanders DS. Potential coeliac disease in Type 1 diabetes mellitus: does a positive antibody lead to increased complications? Nutr Metab Cardiovasc Dis. 2014 Apr;24(4):378-83.

IBS
15% in general population
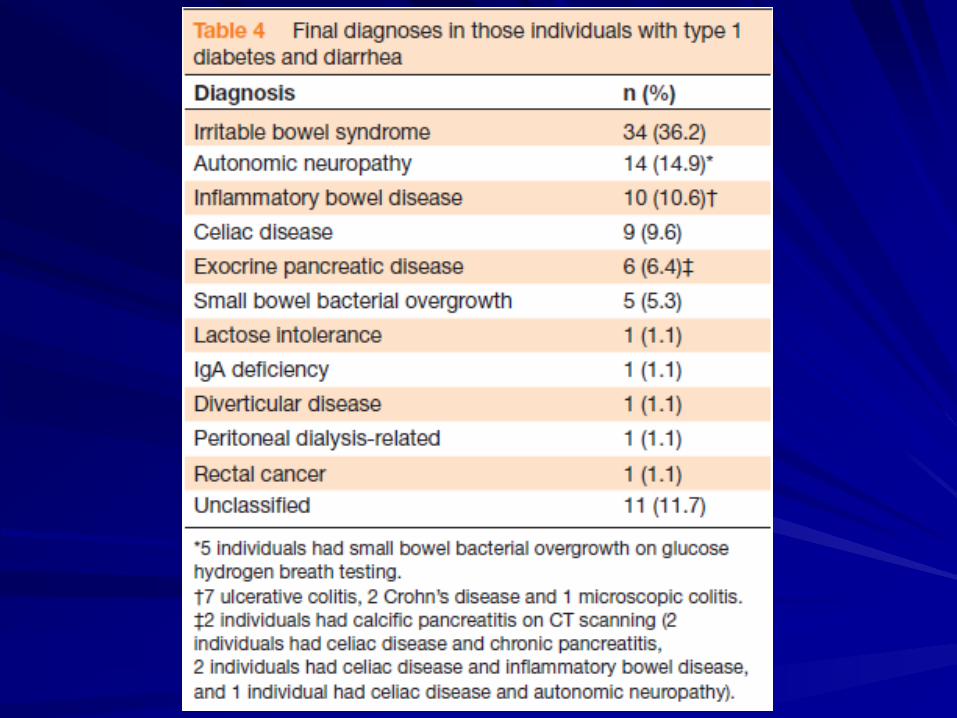
36.2% in our study
Altered somatic perceptionDegrees of intestinal dysmotility and neuropathy?No other studies of prevalence...
Leeds JS, Hadjivassiliou M, Tesfaye S, Sanders DS. Lower gastrointestinal symptoms are associated with worse glycemic control and quality of life in type 1 diabetes mellitus. BMJ Open Diabetes Res Care. 2018 May 29;6(1):e000514

T1DM and IBD
T1DM (n= 662)IBD (n= 622)Non diabetic controls (n= 602)IBD 12/662 (1.5%) in T1DM and 2/602 (0.3%) in controls (OR 5.5, 1.2-24.9; p=0.03)T1DM 4/662 (0.6%) in IBD and 0.4% (OR 1.5, 0.38-6.07; p=0.56) in controls.

Effects of both diseases
Penny HA, Leeds JS, Kurien M, Averginos A, Hopper AD, Hadjivassiliou M, Tesfaye S, Sanders DS. The relationship betweeninflammatory bowel disease and type 1 diabetes mellitus: a study of relative prevalence in comparison with population controls.J Gastrointestin Liver Dis. 2015 Mar;24(1):125-6Jh;kj

Autonomic dysfunction/SIBO
Increasing duration of diabetes
Autonomic neuropathy leads to altered motility
Bacterial overgrowth leads to further damage

SIBO and diabetesAuthor N Cohort Controls Prevalence
Virally-Monod 35 All types No 15/35 (42.8%)Zeitz 50 All types No 17/50 (34%)Urita 82 All types No 28/82 (34.1%)Ojetti 50 Type 1 No 13/50 (26%)Rana 84 Type 2 Yes (45) 13/84 (15.5%)Cesario 30 Type 1 No 8/30 (26.7%)
Adamska 148 Type 1 Yes (41) 56/148(37.8%)
Rana 175 Type 2 Yes (175) 26/175(14.8%)
Malik 75 Type 1 Yes (75) 17/75 (22.7%)

Management
SIBOProbiotics
Antibiotics – Rifaximin, coamox, cipro, tetracyc
Dietetics – elemental, low FODMAP
Autonomic neuropathyTreat SIBO
Improve glycaemic control
Anti-diarrhoeals
Clonidine?

There’s more than 2 types??Type 1 diabetes (insulin deficiency)A. Immune mediatedB. Idiopathic
Type 2 diabetes (Insulin resistance)
Type 4 Gestational diabetes mellitus (GDM)
Type 3 diabetesA. Genetic defects of ᵝ-cell functionB. Genetic defects in insulin action
C. Diseases of the exocrine pancreas1. Pancreatitis2. Trauma/pancreatectomy3. Neoplasia4. Cystic fibrosis5. Hemochromatosis6. Fibrocalculous pancreatopathy7. Others
D. EndocrinopathiesE. Drug- or chemical-inducedF. InfectionsG. Uncommon forms of immune-mediated diabetesH. Other genetic syndromes sometimes associated with diabetes

There’s more than 2 types??Type 1 diabetes (insulin deficiency)A. Immune mediatedB. Idiopathic
Type 2 diabetes (Insulin resistance)
Type 4 Gestational diabetes mellitus (GDM)
Type 3 diabetesA. Genetic defects of ᵝ-cell functionB. Genetic defects in insulin action
C. Diseases of the exocrine pancreas1. Pancreatitis2. Trauma/pancreatectomy3. Neoplasia4. Cystic fibrosis5. Hemochromatosis6. Fibrocalculous pancreatopathy7. Others
D. EndocrinopathiesE. Drug- or chemical-inducedF. InfectionsG. Uncommon forms of immune-mediated diabetesH. Other genetic syndromes sometimes associated with diabetes

Diabetes cohorts
Some patients with CP develop endocrine failure.
Some patients with diabetes have exocrine dysfunction.
Prevalence of pancreatic diabetes (3c) is likely to be underestimated.1,2
1. Angelopoulos N et al. Pancreatology 2005;5 :122 – 131.2. Hardt PD et al. Diabetes care 2008; 31 :Suppl 2:S165 – S169.

Prevalence of Type 3C diabetesRecords of 1,922 patients retrospectively examined.157 (8%) reclassified diabetes type 3c:
Chronic pancreatitis (76%)Pancreatic cancer (9%)Haemochromatosis (8%)Cystic fibrosis (4%)Previous pancreatic surgery (3%)
MechanismsRelationship between endocrine & exocrine function →smaller pancreas in DM subjects.
Exocrine destruction → endocrine disease.
Insulin deficiency → pancreatic atrophy.
Autonomic neuropathy → impaired enzyme release.
Associated GI disease affecting exocrine tissue e.g. coeliac disease.
Reduced pancreatic blood flow.
Islet cell antibodies cross react with acinar cells.

Previous studies
Overall prevalence of Fel-1 <100:
Type 1 DM 26 – 44%Type 2 DM 12 – 20%

DM and exocrine insufficiency
101 DM patients with Fel-1 <100 → fat excretion testing
41 had normal fat excretion (<7g/day)20 had fat excretion 7 – 10g/day40 had fat excretion >10g/day(12 were >15g/day)
Hardt PD et al. High prevalence of steatorrhoea in 101 diabetic patients likely to suffer from exocrine pancreaticinsufficiency according to low fecal elastase 1 concentrations. Dig Dis Sci 2003;48(9):1688-1692.

DM and ERCP changes
Hardt PD et al. Pancreas 2002;25(1) :e6-e9.

TreatmentNo change in:
Glycaemic control
GI symptoms
Fat soluble vitamin levels.
16 week double blind randomized placebo controlled trial in 80 DM patients (Fel-1<100)
Ewald N et al. Diabetes Metab Res Rev 2007; 23: 386–391.

Type 3c matters?
Treating malabsorption – GI and DM
Addressing relevant risk factors
Assessing micronutrient deficiencies
Bone mineral density

Diabetes and cancer
Diabetes associated with increased risk of cancer
Earlier?Symptoms ascribed to DM complications?
Increased complications with treatment
Larsson SC et al. Diabetes mellitus and risk of colorectal cancer: a meta-analysis. J Natl Cancer Inst. 2005;97(22):1679–1687.Stein KB et al. Colorectal Cancer Outcomes, Recurrence, and Complications in Persons With and Without Diabetes Mellitus: A Systematic Review and Meta-Analysis. Dig Dis Sci. 2010;55(7):1839-51.

Diabetes and BAM
Interestingly, NO prevalence studies
Personal experience
Metformin can cause lack of reabsorptionof TI bile acids
Scarpello JH et al. Effect of metformin on bile salt circulation and intestinal motility in type 2 diabetes mellitus. Diabet Med. 1998 Aug;15(8):651-6.

Medications and GI symptoms
MetforminAcarboseAmylinGliptins (pancreatitis)GLP-1 agonistsGlinidesStatins

Summary
GI symptoms are common in diabetes
Increased prevalence of GI diseases
Associated with poorer Qol and HbA1c
Often under-investigated

Summary continued
Rome criteria – IBS managementCheck medications – alter if you canCoeliac serology – GFDFaecal calprotectin/colonoscopy – IBD RxFaecal elastase-1 – Investigate furtherGHBT – rifaximinSeHCAT scan – bile acid sequestrants

Acknowledgements
Prof D S SandersProf S Tesfaye
Bardhan Research and Education TrustSolvay