hormonoterapia y nuevas terapias biológicas en cáncer de...
TRANSCRIPT

Hormonoterapia y Nuevas Terapias Biológicas en Cáncer de Mama
Avanzado: Una realidad
Diego Soto de Prado Otero
Hospital Clínico Universitario de Valladolid

Esquema de la presentación
1. Introducción. Mecanismo de acción.
2. Inhibidores de CDK 4/6
3. Inhibidores de m-TOR y PI3K
4. Conclusiones


MECANISMO DE ACCIÓN DE LA HORMONOTERAPIA

MECANISMO DE ACCIÓN DE LA HORMONOTERAPIA

SuprarrenalSuprarrenal
AndrostendionaAndrostendiona TestosteronaTestosterona
AromatasaAromatasa
EstronaEstrona EstradiolEstradiol
x Inhibidores de la Aromatasa
MECANISMO DE ACCIÓN DE LA HORMONOTERAPIA

x Ooforectomía
Irradiación ovárica
x Análogos LHRH
MECANISMO DE ACCIÓN DE LA HORMONOTERAPIA

x SERM’s
Tamoxifeno, Toremifeno
Fulvestrant
MECANISMO DE ACCIÓN DE LA HORMONOTERAPIA

TERAPIAS DIRIGIDAS EN TUMORES LUMINALES
Año Hormonoterapia Mecanismo de acción
1977 SERMs
Tamoxifeno
Toremifeno
Antagonistas del RE en el tejido
mamario
1990 IA
Anastrozol
Exemestano
Letrozol
Inhiben la síntesis de estrógenos en
mujeres postmenopáusicas.
2000 SERDs
Fulvestrant
Se une al RE, impide su
dimerización y acelera su
degradación.
Análogos de la LHRH Goserelina

Klijn JG, et al. J Natl Cancer Inst. 2000;92:903-911.
Overall Survival
EORTC Premenopausal: Survival Benefit for Ovarian Suppression and TAM

AI, aromatase inhibitor; TAM, tamoxifen.
Mouridsen, et al. Oncologist 2004;4:489–496; Bonneterre, et al. Cancer 2001;92:2247–2258;
Paridaens, et al. J Clin Oncol 2008;26:4883.
First-Line Therapy: Aromatase Inhibitors Showed Consistent Superiority over Tamoxifen (Postmenop)
Pro
po
rtio
n w
ith
ou
t p
rog
ressio
n
Time (months)
0
0.6
1.0
0 36
0.4
0.8
0.2
TAM
30 24 12 6 18
TTP (months) P
Letrozole Tamoxifen
9.4 6.0
<0.0001
Anastrozole Tamoxifen
10.7 6.4
0.022
Exemestane Tamoxifen
10.5 5.5
0.028
AI

• Phase III SWOG S0226 study
Mehta RS, et al. N Engl J Med. 2012;367:435-444.
FULVESTRAN
Bergh J, et al. J Clin Oncol. 2012;30:1919-1925.
FACT Study

Di Leo A, et al. J Natl Cancer Inst. 2014;106(1):djt337.
Second Line (AI Resistant): CONFIRM Long-term Benefits in OS (ITT)
Di Leo A, et al. J Clin Oncol. 2010;28:4594-4600.
Erratum in: J Clin Oncol. 2011;29:2293.

FIRST (Fase IIB)


PI3K
AKT ER
GRB2
P
P
P P
ER
CoA
ER CoA
AP-1
P
CoA
TFs
EREs AP-1/SP-1 TFs-REs
P ER
S6KI
mTOR inhibitors
SOS Shc
Rb
E2F E2F
Gene transcription
Cyclin D
CDK4/6
P P P
P P
Cyclin D
CDK4/6
CDK4/6 inhibitors
P P
mTOR
Estrogen receptor downregulator
Growth factor receptor (eg, EGFR)
Ras
Raf
MAPK
Src
PI3K inhibitors
Aromatase inhibitors
MEK p21
p16
G1
S G2
M
p53
Cell cycle
Tyrosine kinase inhibitors

Regulation of the G1/S Checkpoint in Breast Cancer
Pl3K/Akt
STATs MAPKs
ER/PR/AR Wnt/β-catenin
NF-κB
p16
p21
p53
CDK4/6 Cyclin D
RB
RB
Gene transcription
G2 S
M
G1
G0
P P P
P
Inactive
Active tumor suppressor
E2F
E2F
R
D-type cyclins regulated in response to mitogenic stimuli, including activation of RTKs and steroid hormone receptors1
• Cyclin D1 is amplified in 15–20% of breast cancers

INHIBIDORES DE CDK 4/6
1. PALBOCICLIB (PFIZER)
2. RIBOCICLIB (NOVARTIS)
3. ABEMACICLIB (LILLY)

Palbociclib Inhibidor selectivo de CDK4/6. Previene la P-pRB, induciendo una “arresto” de la célula en G1. Toxicidad más frecuente: NEUTROPENIA y TROMBOPENIA
N = 66
1:1
Part 1: All Comers
ER+, HER2– BC
R A N D O M I Z A T I O N
PD 0332991 125 mg QDa +
Letrozole 2.5 mg QD
Letrozole
2.5 mg QD
Part 2: Biomarker-Positive
N = 99
1:1 ER+, HER2–
BC with CCND1 amp
and/or loss of p16
R A N D O M I Z A T I O N
PD 0332991 125 mg QDa +
Letrozole 2.5 mg QD
Letrozole
2.5 mg QD
PALOMA-1 :Phase 2 Trial

TERAPIAS DIRIGIDAS EN TUMORES LUMINALES
FINN Lan Oncol 2015
Median PFS LET-PALBO 20.2 m (95%CI 13.8-27.5)
LET 10.2 m (95%CI 5.7-12.6)

TERAPIAS DIRIGIDAS EN TUMORES LUMINALES
FINN Lan Oncol 2015
Median PFS
LET 5.7 m (95%CI 2.6-10.5)
LET-PALBO 26.1 m (95%CI 11.2-NE)
Median PFS
LET 11.1 m (95%7.1-16.4)
LET-PALBO 18.1 m (95%CI 13.1-27.5)


PALOMA-2

PALOMA3 Study Design
Placebo (3 wks on/ 1wk off)
+ Fulvestrant†
(500 mg IM q4w)
Palbociclib (125 mg QD;
3 wks on/1 wk off) +
Fulvestrant† (500 mg IM q4w)
†administered on Days 1 and 15 of Cycle 1.
● Visceral metastases
● Sensitivity to prior
hormonal therapy
● Pre-/peri- vs Post-
menopausal
Clinicaltrials.gov NCT01942135
2:1 Randomization
N=521
Stratification:
• Post-menopausal patients must have progressed on prior aromatase inhibitor therapy.
n=347
n=174
• HR+, HER2– ABC
• Pre-/peri-* or post-menopausal
• Progressed on prior endocrine therapy:
– On or within 12 mo adjuvant
– On therapy for ABC
• ≤1 prior chemotherapy regimen for advanced cancer
*All received goserelin.

Cristofanilli M. SABCS 2015
ESTUDIO PALOMA-3
2ª Línea Hormonoresistentes.
Pre/ postmenopausicas.
PFS: 9,5 m vs 4,6 m
HR: 0,46


● MONALEESA-1: Letrozol Ribociclib (Neoadjuvant)
● MONALEESA-2: Letrozol Ribociclib (mBC, 1L)
● MONALEESA-3: Fulvestrant Ribociclib (mBC, 1L)
● MONALEESA-7: TAM/NSAI + goserelin Ribociclib (premenop, mBC)
Inhibidor selectivo de CDK4/6. Previene P-pRb
Sinergico con inhibidores de PI3K/Akt/mTOR (Everolimus y Buparlisib)
Tóxicidad: GI (35%) y Neutropenia (40%)
RIBOCICLIB

Abemaciclib
La principal toxicidad es Gastrointestinal (52% diarrea; 30% nauseas) y Neutropenia (16%). Atraviesa la BHE.
Datos de actividad sinérgica con Gemcitabina.
Dos estudios con datos para el 2017 :
MONARCH-1 : Fase II de Abemaciclib en 2ª línea en pacientes postmenopaúsicas RE+ HER2- pretratadas con QT. Objetivo 1º: T. Resp.
MONARCH-2: Fase III de Abemaciclib +/- FULV en 1ª ó 2ª línea en pacientes postmenopaúsicas RE+ HER2- en progresión a HT. Objetivo 1º: PFS

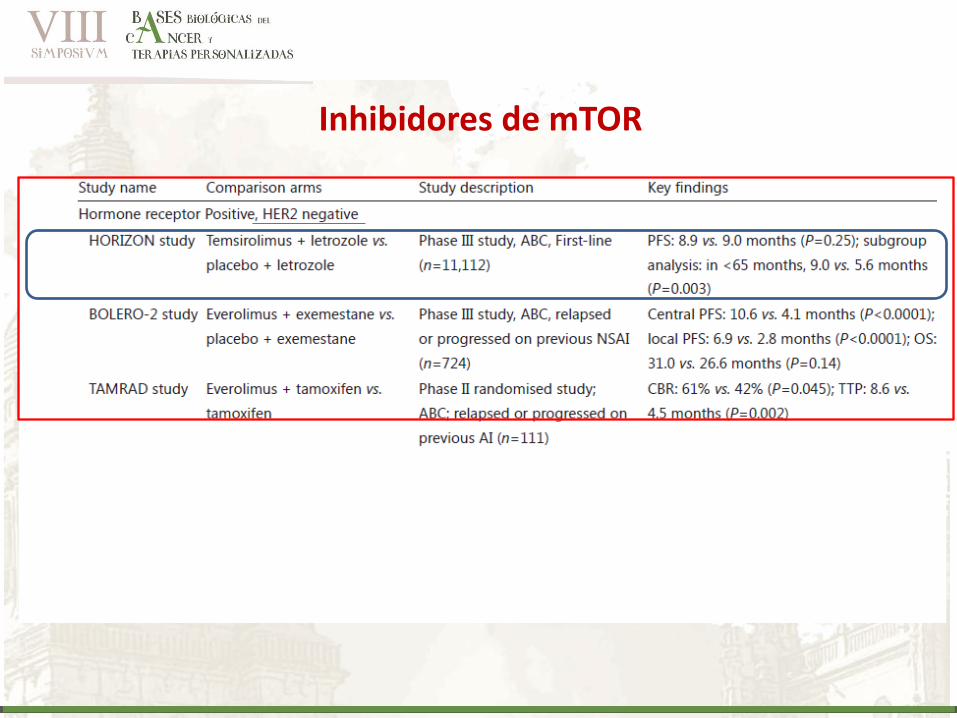
Inhibidores de mTOR
Inhibidores de mTOR

CBR
P = 0.045 (exploratory analysis)
TTP
• TAM: 4.5 months
• TAM + EVE: 8.6 months
• HR (95% CI) = 0.54 (0.36-0.81)
• P = 0.0021 (exploratory analysis)
Abbreviations: CI, confidence interval; EVE, everolimus;
HR, hazard ratio; TAM, tamoxifen.
Bachelot T, et al. J Clin Oncol. 2012;22(30):2718-2724.
TAM TAM + EVE
42.1
% (29-56)
61.1% (47-74)
0
10
20
30
40
50
60
70
CB
R, %
of
Pa
tien
ts (
95
% C
I)
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Months
0.0 0.1 0.2 0.3 0.4 0.5
0.6 0.7 0.8 0.9 1.0
TT
P P
rob
ab
ilit
y
TAM
At risk
57
54 45 39 34 28 26 25 20 19 17 14 10 3 3 2 1
44 30 24 22 16 13 11 7 6 4 2 2 1 0 0
TAM + EVE
TAMRAD: Phase II randomised study; ABC; relapsed or progressed on
previous AI (n=111)

TAM
TAM + EVE
0,0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0,8
0,9
1,0
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40
Pro
bab
ilit
y o
f S
urv
ival
Months
TAMRAD
Primary resistance
• N (%) of events
• TAM: 15 (54%)
• TAM + EVE: 12 (46%)
• HR = 0.73; 95% CI, 0.34-1.55
• P = 0.41 (exploratory analysis)
Secondary resistance
• N (%) of events
• TAM: 16 (55%)
• TAM + EVE: 4 (15%)
• HR = 0.21; 95% CI, 0.07-0.63
• P = 0.002 (exploratory analysis)
TAMRAD: Phase II randomised study; ABC; relapsed or progressed on
previous AI (n=111)
TAM
TAM + EVE

ESTUDIO BOLERO-2
Baselga J et al, New Engl J Med 2012

1.0
0.8
0.6
Pro
bab
ilit
y o
f
Pro
gre
ss
ion
-Fre
e S
urv
ival
0.4
0.2
0
28 26 24 22 20 18 16 14
Time (months)
12 10 8 6 4 2 0
0 0
1 0
4 0
10 1
13 1
23 2
42 6
57 9
99 17
147 27
194 42
236 61
318 103
394 146
485 239
EVE+EXE PBO+EXE
No. at risk
HR = 0.45 (95% CI, 0.38-0.54) Log-rank P < .0001
Kaplan-Meier medians EVE+EXE: 7.8 months PBO+EXE: 3.2 months
Censoring times EVE+EXE (n/N = 310/485) PBO+EXE (n/N = 200/239)
BOLERO: Phase III study, ABC, relapsed or progressed on previous NSAI (n=724) PFS Based on Local Assessment
Abbreviations: CI, confidence interval; EVE, everolimus; EXE, exemestane; HR, hazard ratio; PBO, placebo; PFS, progression-free survival.
Yardley DA, et al. Adv Ther. 2013;30:870-884. 15
03
0340
34
PFS based on local assessment at 18-mo follow-up

BOLERO-2 (39-mo f/up): Overall Survival
Abbreviations: CI, confidence interval; EVE, everolimus; EXE, exemestane; HR, hazard ratio; PBO, placebo.
Piccart M, et al. EBCC 2014. Abstract 1LBA.
232
109
248
113
266
120
279
130
292
145
311
153
330
162
347
170
373
182
399
194
414
201
429
211
448
220
471
232
485
239
EVE+EXE
PBO+EXE
No. at risk
HR = 0.89 (95% CI, 0.73-1.10) Log-rank P = .1426
Kaplan-Meier medians EVE+EXE: 30.98 months PBO+EXE: 26.55 months
Censoring times
11
5
23
8
39
18
58
28
91
41
118
56
154
77
196
98
216
102
0
0
1
1
15
03
0340
34

Various PI3K/AKT/mTOR Pathway Alterations Have Been Detected in HR+ Breast Cancer
RTKs can be
overexpressed
or overactivated
in cancer
PTEN
AKT
PIP2
PIP3
Tumor growth and progression
Resistance to anticancer therapy
PIK3CA mutation is the
most frequent genetic
alteration
mTORC1 PRAS40 p27 GSK3 FOXO Casp9 BAD AS160 MDM2 eNOS
mTORC2
PI3K
AKT
INHIBIDORES DE PI3k

Pan-PI3K class I inhibitors
• Inhibit all four isoforms of class I PI3K (α, β, γ, δ) and provide the broadest inhibition of PI3K3,6
• May be better suited to combination therapy and in tumour types lacking PIK3CA mutations4
First-generation
Dual PI3K/mTOR inhibitors
• Target homologous regions in the catalytic sites of PI3K and downstream components mTORC1 and mTORC23,6
• Targeting two levels of the pathway may provide the potential advantage of stronger inhibition3,6
Isoform specific inhibitors
• Characterised by greater and PI3K isoform-specific activity3
• Provide the potential to completely block a specific target while limiting toxicities associated with a broader inhibition5
PI3K inhibitors in development
• Three generations of PI3K inhibitors have now been developed
Second-generation Third-generation

INHIBIDORES DE PI3k
1. BUPARLISIB (NOVARTIS)
2. ALPELISIB (NOVARTIS)
3. PICTILISIB (ROCHE)
4. TASELISIB (ROCHE)
Regulatory
subunit
Catalytic
subunit p110
p85
PI3K
PI3K
Isoforms
α
β
γ
δ

Buparlisib: Los “Belle”
Paninhibidor PI3k eficaz en líneas PI3k-mut En líneas PI3k-MUT y resistentes a HT o a Everolimus, la combinación con Fulvestran revierte las resistencias

Randomization (1:1) Stratification based on PI3K pathway activation status* and
presence/absence of visceral disease
Main study cohort n≈842
Buparlisib + fulvestrant†
n≈421
Placebo + fulvestrant†
n≈421
PI3K unknown cohort n≈308
Buparlisib + fulvestrant†
n≈154
Placebo + fulvestrant†
n≈154
Postmenopausal patients with HR+/HER2– locally advanced
or metastatic breast cancer refractory to aromatase inhibitor N≈1150
Molecular screening for PI3K pathway activation status*
Study objectives:
Co-primary: PFS (local assessment)‡
Co-key secondary: OS‡
Secondary: Efficacy (ORR,‡§ CBR,‡§ PFS,§ OS§), safetyII, PK¶, patient-reported outcomes‡, ECOG PS‡§

Beneficio en mutaciones con ctDNA PIK3CA mutations

BELLE-2 Safety Profile Was Characterized by Transaminitis, Hyperglycemia, Rash, and Mood Disorders
Buparlisib + Fulvestrant n=573
Placebo + Fulvestrant n=570
Adverse event, % All grades Grade 3 Grade 4 All grades Grade 3 Grade 4
Total 99.5 63.2 14.1 93.0 27.4 4.6
Increased ALT 40.1 18.7 6.8 6.8 1.1 0
Increased AST 37.3 15.0 3.0 9.3 2.8 0
Hyperglycemia 43.1 15.2 0.2 7.7 0.2 0
Rash 32.1 7.7 0.2 6.3 0 0
Anxiety 22.3 5.2 0.2 8.2 0.9 0
Fatigue 31.9 4.9 0 23.9 1.6 0
Depression 26.2 3.7 0.7 8.9 0.4 0
Diarrhea 34.2 3.7 0 14.6 1.1 0
Asthenia 20.1 2.8 0 10.5 1.1 0
Stomatitis 21.6 2.1 0 6.5 0.5 0
Nausea 38.7 1.7 0 23.2 1.4 0
Decreased appetite 29.8 1.6 0 11.1 0.2 0

Phase III randomized study of buparlisib + fulvestrant in patients with HR+/HER2– mBC previously treated with AI and refractory to mTORi1
Randomization (2:1) Stratification based on presence/absence of visceral disease
Postmenopausal patients with HR+/HER2–, locally advanced or mBC, pre-treated with AI
and refractory to endocrine and mTORi combination therapy N≈420
Buparlisib + fulvestrant*
n≈280
Placebo + fulvestrant*
n≈140
Study objectives:
Co-primary: PFS (local assessment)
Co-key secondary: OS
Secondary: Efficacy (ORR, CBR), safety, PK, patient-reported outcomes, time to ECOG PS deterioration

Resistance to everolimus may be linked to feedback activation of the PI3K pathway
Buparlisib + fulvestrant controls tumor growth in everolimus-resistant* xenografts (ZR75-1)1
*Resistance to everolimus acquired by daily treatment with everolimus10 mg for >45 days.
ZR75-1: wild-type PIK3CA, PTEN mutation and loss of function.
1. O’Brien HA, et al. SABCS 2013:PD1−5 (Poster).
Buparlisib
Everolimus
Tu
mo
r vo
lum
e (
mm
3)
Time of treatment (days)
0 42 6 12 18 24 30 36
0
400
200
1000
800
600
Buparlisib + fulvestrant
Everolimus

Alpelisib • Inhibidor PI3k alfa-selectivo
• MDT: 400 mg/día con FULV o 300 mg/día con IA
• Toxicidad semejante a Buparlisib
PI3
K
RTK
PIP2
PIP3
AK
T
PTE
N
mTORC1
mTORC2
Alpelisib PI3Kα
0
50
100
150
200
250
300
350
400
450
500
0 5 10 15 20 25
Treatment days
Alpelisib significantly decreases tumor volume in the MCF7 (breast)
E545K model
Alpelisib + fulvestrant showed greater
antitumor activity than either agent alone in an
everolimus-resistant, ER-positive breast cancer
model

Combination Neo-adjuvant mBC
Letrozol
Fulvestrant
TAM + goserelin
T-DM1
CBYL719A2201: Letrozole ± BKM120 or
BYL719 (Phase II)
46
CBYL719XUS03T Letrozole + BYL719
(Phase Ib)
CLEE011X2107:
Letrozole + LEE011 ±BYL719 (Phase I/II)
CBYL719X2101 Fulvestrant+ BYL719
(Phase I) CLEE011X2108:
Fulvestrant + LEE011 ±
BKM120 or BYL719 (Phase I/II) SOLAR-1
Fulvestrant ± BYL719 (Phase III) (1/2L)
15
05
0353
78
B-YOND:
TAM + Goserelin with
BKM120 or BYL719 (Phase Ib)
BYL719 + T-DM1 (Phase Ib)

Screening assessments
Randomization (1:1)
PIK3CA-mutant cohort (n≈340) PIK3CA-nonmutant cohort (n≈220)
Randomization (1:1)
Men and postmenopausal women with HR+/HER2– ABC, whose disease progressed on prior AI treatment (N≈560)
A Phase III Randomized Double-blind, Placebo Controlled Study of Alpelisib in Combination With Fulvestrant for Men and Postmenopausal Women With HR+/HER2– Advanced Breast Cancer Which Progressed on or After
Aromatase Inhibitor Treatment
Alpelisib (300 mg QD) + fulvestrant*
(500 mg IM q4w)
Placebo (QD) + fulvestrant*
(500 mg IM q4w)
Alpelisib (300 mg QD) + fulvestrant*
(500 mg IM q4w)
Placebo (QD) + fulvestrant*
(500 mg IM q4w)
Stratification by: • Liver and/or lung
metastases • Prior treatment with any
CDK4/6 inhibitor
Primary endpoint: Progression free survival (PFS; local assessment; PIK3CA-mutant cohort)
Key secondary endpoint: Overall survival (OS; PIK3CA-mutant cohort)
SOLAR-1

PICTILISIB
En neoadyuvancia demostró asociado a ANA un aumento de
la capacidad antiproliferativa de ANA, sobretodo en Luminal B

Phase II FERGI: Combination of fulvestrant and pictilisib in ER+, AI-resistant
advanced BC associated with high rate of toxicity and no significant improvement in
PFS

TASELISIB

Inhibidores PI3K

CONCLUSIONES
1. Dentro de los mecanismos de resistencia al tratamiento hormonal la vía PI3k-
AKT-mTOR y las ciclinas dependientes de kinasas juegan un papel crucial
2. Las líneas de investigación van dirigidas a aumentar la eficacia de los
tratamientos disponibles y recuperar la sensibilidad hormonal:
Fulvestran a “altas” dosis ha demostrado ser superior a IA y probablemente se
instaure en 1ª línea (Estudio FALCON)

CONCLUSIONES
Inhibidores de ciclinas : datos muy positivos en 1ª y 2ª línea.
Inhibidores de m-TOR: papel en las resistencias secundarias (2ª líneas y
sucesivas)
Inhibidores de PI3k: eficacia a costa de una importante toxicidad. Fase III con
beneficio en pacientes PI3k mutadas. Pendientes de resultados con
inhibidores más selectivos.

Muchas gracias…