home-based patient care during an influenza pandemic ...€¦ · • health care, especially in...
TRANSCRIPT

Home-based patient care during
an influenza pandemic.
Field test of Key Messages.Sierra Leone Nov – Dec 2009 & March 2010
Dr Tim HealingDip.Clin.Micro, DMCC, CBIOL, FZS, FRSB
,, Course Director,
Course in Conflict and Catastrophe Medicine
Worshipful Society of Apothecaries of London
Faculty of Conflict and Catastrophe Medicine

The Project• People living in resource poor countries are likely to be
severely affected by events such as an influenza pandemic
• Health care, especially in remote areas, is likely to be very limited
• Very high levels of poverty mean that few can afford health care or drugs
To help address these problems WHO produced guidance on home-based patient care during a pandemic.
– This contained a number of Key Messages
– These had to be appropriate for the countries where they would be used.
– WHO undertook field trials of the Key Messages in various parts of the world including Sierra Leone.

The key messages
Understanding the disease1. What is influenza A (H1N1)?
Preventing infection2) Cover your mouth and nose when you cough or
sneeze with a sleeve/scarf (respiratory etiquette)
3) Hand hygiene
4) Separate the sick from others
5) Ventilate the area where the patient is nursed
6) One care giver for each sick person
Nursing the sick7) Hydrate the patient
8) Antibiotic treatment for pneumonia
9) Assess if the patient needs to seek health care

The Sierra Leone programme team & MoHS and other
agencies working with the team
WHO Global Influenza Programme, Geneva
• Dr Tim Healing (Field Test Project Manager)
• Dr Julienne Ngoundoung Anoko (Social Anthropologist)
• Ms Anna Bowman (WHO Technical Officer)
• Mr Guilhem Alandry (Videographer)
WHO Office, Freetown
• Mrs Aminata Kobie (Health Promotion Information Adviser)
• Mrs Mary Massaquoi (Translator/Local adviser)
• Mr Lawrence Babawo (Translator/Local adviser)
MoHS National level
• Health and education team
• Disease prevention and control team
MoHS District level
• Health and education departments
• District medical authorities
• Lassa Fever outreach team (Kenema)

Sierra Leone
Slightly larger than the Republic of
Ireland, slightly smaller than
Austria
At the time of this study:
• Emerging from 11 years of
civil war
• Trying to reintegrate returning
refugees, relocated IDPs,
former combatants &
amputees

Sierra Leone –
some basic
factsSL UK
• Population 5,485,998 61,708,895
• UNDP HDI position 180/182 21/182
• Annual income per capita $340 $28,350
• Annual health expenditure per capita $43 $3,399
• Annual health expenditure as % of GDP 3.5% 8.4%
• Popn below poverty line (<$1.25/day) 53% 0
• Life expectancy at birth (m/f - years) 39/42 75/82
• Healthy life expectancy (m/f - years) 27/30 69/72
• Maternal mortality/100,000 live births 970 13.95
• Infant mortality/1,000 live births 155 4.93
• Under 5y mortality 26.9% 0.6%

Test Sites

Test sites
Two test sites were used
• George Brook (DwarzakFarm), a deprived community on the southern side of Freetown
• Blama town, the main town of the Small Bo Chiefdom, about 12 miles west of Kenematown

George Brook (Dwarzak
Farm) Community,
Freetown
• Urban site, edge of Freetown
• Population ca. 32,000
• Extends up a valley into the hills around the city
• Many houses hard to reach
• Home to 16 ethnic groups

Official medical care
in George Brook
• Government health centre– Community Health Officer (CHO)
with 25 staff.
– Basic services
• ante- and post-natal care,
• family planning
• treatment for infections including malaria and TB
• minor trauma.
– Tests for HIV/AIDS (+ve cases referred to Freetown hospitals)
– 15 inpatient beds (mainly maternity)
– Labour room for deliveries
– Charge on cost recovery basis (some exemptions).

Other health care in George Brook
• Private clinics
• Self styled “doctors”
• Advice from pharmacies & unofficial drug
outlets
• Traditional Healers
(Many are cheaper than the government
clinic & therefore used more).

Kenema

Small Bo chiefdom
• One of 16 chiefdoms
in the Kenema
District
• Population ca 34,550
• Ruled by a
Paramount Chief

Blama town, Small Bo Chiefdom
• Blama – country town, far from Freetown
• Ca. 9000 inhabitants
• 4 ethnic groups (Mende – largest)
• Formerly prosperous (rail centre)
• Rural economy with weekly market in central market place

Government and other health facilities
in Blama
• Community Health Centre – CHO, 5 staff + some volunteers.
– Facilities include
• Ante- and post- natal clinics
• labour ward,
• TB, malaria and HIV/AIDS diagnosis
• minor trauma
• complicated cases referred to Kenemahospital
• Other health care similar to George Brook– Private clinics
– Self styled “doctors”
– Advice from pharmacies & unofficial drug outlets
– Traditional Healers
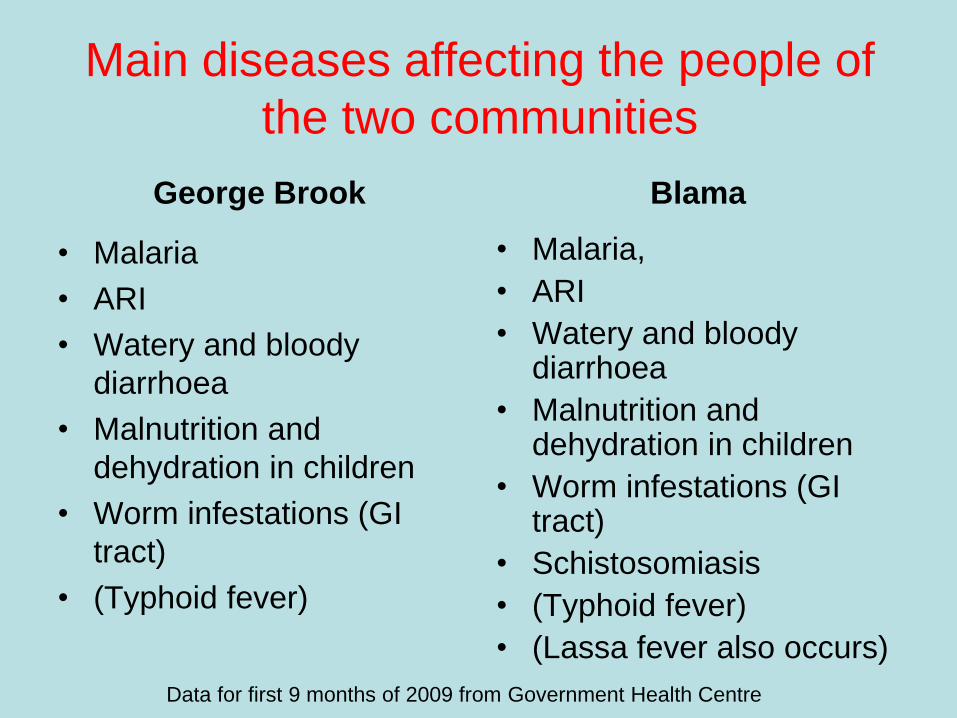
Main diseases affecting the people of
the two communities
George Brook
• Malaria
• ARI
• Watery and bloody
diarrhoea
• Malnutrition and
dehydration in children
• Worm infestations (GI
tract)
• (Typhoid fever)
Blama
• Malaria,
• ARI
• Watery and bloody diarrhoea
• Malnutrition and dehydration in children
• Worm infestations (GI tract)
• Schistosomiasis
• (Typhoid fever)
• (Lassa fever also occurs)
Data for first 9 months of 2009 from Government Health Centre

The programme

Working with the communities
• Developed partnerships with the two communities
• Project aims presented to community leaders
• Anthropologist built relationship with the community
• This allowed the community to – take ownership of the
programme
– select & develop the messages
– develop ways to deliver the messages

Gathering socio cultural information
• Qualitative
anthropological surveys
• As many community
groups as possible
interviewed
• Observation of day to
day life behaviours

Outcomes of the surveys

Local knowledge & explanations of
Influenza A (H1N1)
• “Doesn’t exist. The government is just
creating panic. Where are the sick people?”
• “Is a manipulation by the political authorities”
• “A disease created by the United States
since the terrorist attacks of 9/11”
• Some remembered that it affects Asian
countries and kills a lot of chickens
• A lot of pigs were killed in Egypt
• Not a Sierra Leonean concern

Why did radio messages about
H1N1 fail to reach the people?
• Broadcast at wrong times
• Market traders may have radios on but do
not listen carefully
• Radio batteries are expensive

Are colds and “flu-like illness” (“fresh
cold”) diseases?Thinking about this is confused
• In general “Fresh Cold” not considered to be an infectious disease and not considered to be dangerous
• Colds and flu-like illness result of unpleasant external conditions (e.g. the Harmattan)
• All are likely to get it so no attempts are made to avoid it “Better all have it at the same time than one after the other”
Therefore communities might not recognise H1N1 infection as a disease, or attempt to prevent its spread, at least initially, without extensive sensitisation
H1N1 became known locally as “New Fresh Cold”

Normal treatment for “fresh cold”
• Normally treated at home with:
– Hot pepper soup
– [But:
• No fluids (provokes vomiting)
• No hot drinks (due to sore throat)]
– Hot baths
– Wearing warm clothes
– Mentholated rub
– Rest, paracetamol
– Nursed outside (sheltered part of veranda) during
day, go inside at night to sleep

Attitudes to behaviours that can affect
transmission, prevention and mitigation
of the disease
• Washing hands
• Coughing and
sneezing
• Blowing the nose
• Spitting

Washing hands before eating
Don’t need to wash the hands before
eating because use a spoon to eat
But in fact
– handle meat, chicken or fish in their food
with their hands.
– handle the dishes

Washing hands after cleaning the
baby’s bottom
• Mothers don’t wash hands properly after cleaning
baby’s bottom
• “Children’s shit is not infectious, not dangerous”

Coughing and sneezing.
People tend to:
• Cover mouth and nose with both hands
• Rub the droplets into their hands and
clean their hands on their clothes.
• Some use handkerchiefs which may be
kept in the pocket up to a week before
being washed
• Same handkerchief used on children

Blowing the nose
• Often blow the nose with fingers, throw the
mucus on the ground & clean their hands on
their clothes
• Children’s noses are cleaned with their
mother’s clothes/hands or the children’s
clothes
• Some mothers suck their child’s nose with
their mouth to extract the mucus and then
spit it out.

Spitting
• Most people spit on the ground/floor in
the same place where they are seated
or are standing.

Understanding the disease
1. What is influenza A (H1N1)?
Preventing infection
2. Cover your mouth and nose when you cough or sneeze with a sleeve/scarf (respiratory etiquette)
3. Hand hygiene
4. Separate the sick from others
5. Ventilate the area where the patient is nursed
6. One care giver for each sick person
Nursing the sick
7. Hydrate the patient
8. Antibiotic treatment for pneumonia
9. Assess if the patient needs to seek health care
Understanding the disease
1. What is influenza A (H1N1)?
Preventing infection
2. Cover your mouth and nose when you cough or sneeze with a sleeve/scarf (respiratory etiquette)
3. Hand hygiene
4. Separate the sick from others
5. Use outside spaces
6. Eat from separate dishes and with separate utensils
Nursing the sick
7. Hydrate the patient
8. Antibiotic treatment for pneumonia
9. Assess if the patient needs to seek health care
The original Key Messages Messages assessed as
important at both sites

Developing the messages
• WHO team & MoHS
adapted key
messages to local
socio-cultural context
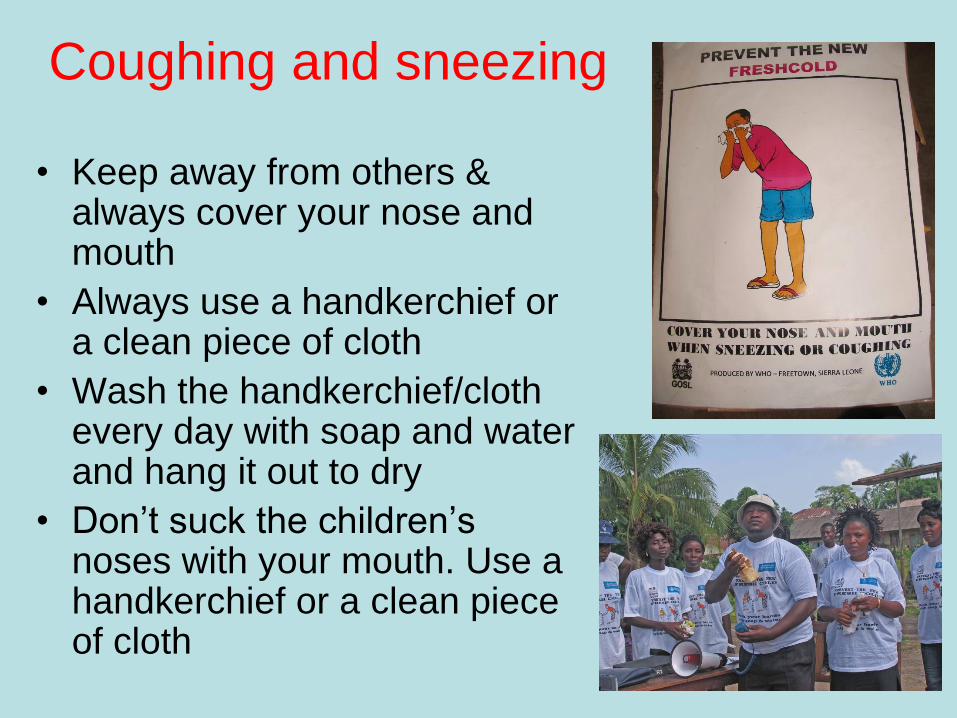
Coughing and sneezing
• Keep away from others & always cover your nose and mouth
• Always use a handkerchief or a clean piece of cloth
• Wash the handkerchief/cloth every day with soap and water and hang it out to dry
• Don’t suck the children’s noses with your mouth. Use a handkerchief or a clean piece of cloth

Wash your hands frequently with
water and soap
After coughing & sneezing
and
– When arriving at home
– Before eating
– Before touching or preparing
food
– Before feeding your baby
– After using the latrines
– After cleaning the baby’s
bottom

Reinforcing the hand
washing message
• Soap kills germs (washing
with water only doesn’t)
• Ask another person to
handle the kettle used for
washing
• (Use ash for mechanical
cleansing when soap/water
is short – ideally followed by
water rinse)

Hydration
• Drink a lot of fluids
(water/juice/lemon
grass/pepper soup)
• Eat fruit to help keep
the body strong and
prevent dehydration
• Continue breastfeeding
the baby

Use outside areas
• Reduces contact with infectious droplets
• Helps reduce infectious droplets inside.
Difficult to
1) Separate patient from others indoors due to large numbers of people in houses
2) Ventilate house at night –windows closed/covered to keep out mosquitoes

Eat from separate dishes, use
separate utensils
Helps prevent
transmission from
one person to
another
(Can be difficult to
follow due to
traditional food
sharing behaviours)
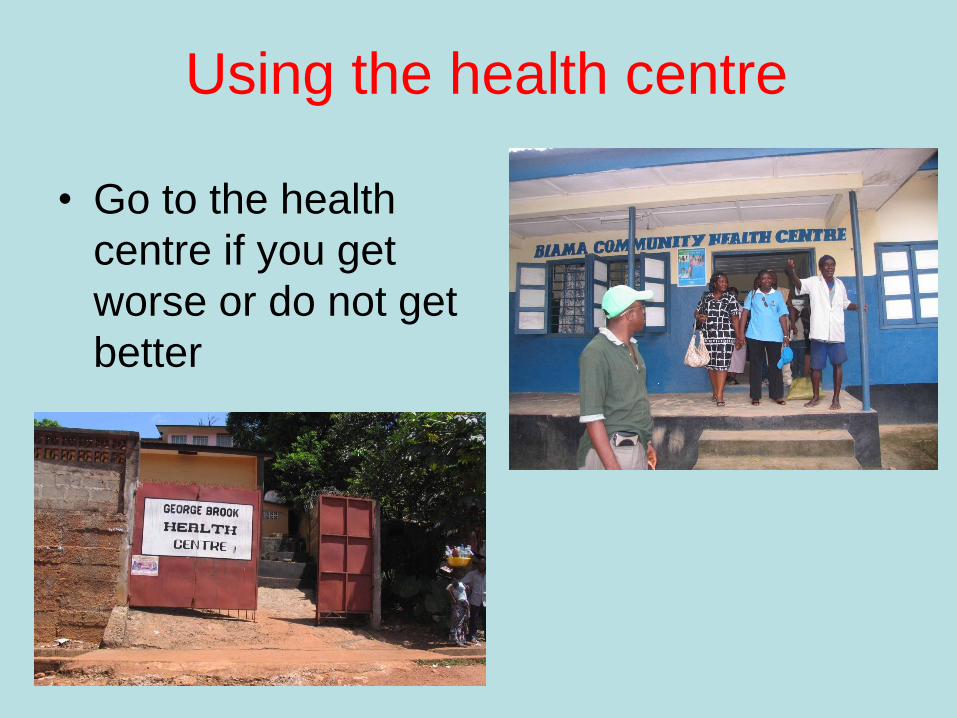
Using the health centre
• Go to the health
centre if you get
worse or do not get
better

Disseminating the messages
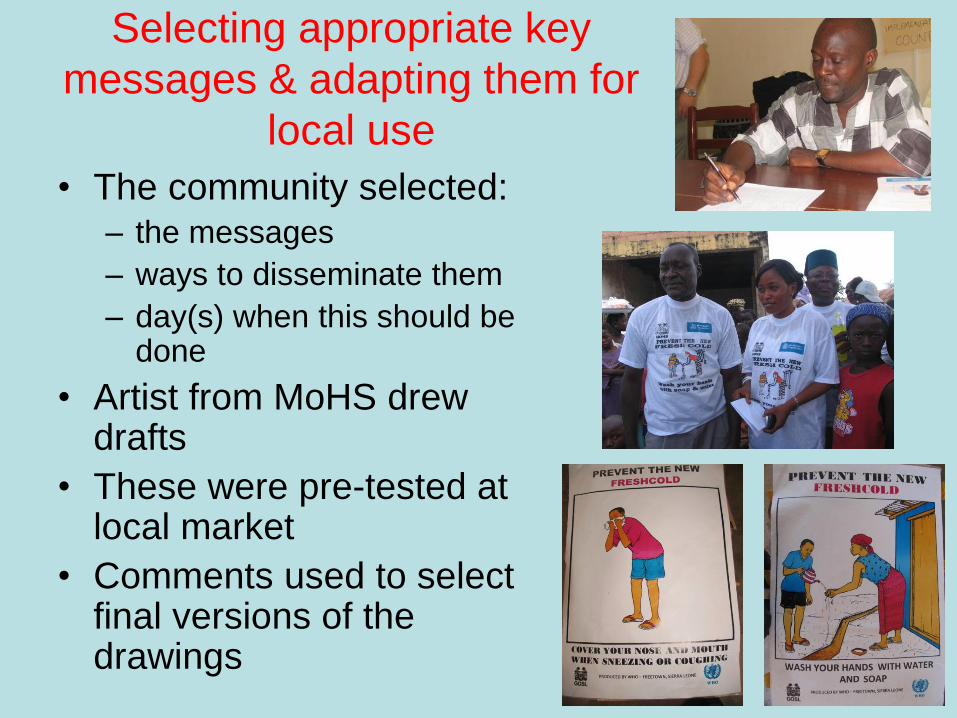
Selecting appropriate key
messages & adapting them for
local use
• The community selected:– the messages
– ways to disseminate them
– day(s) when this should be done
• Artist from MoHS drew drafts
• These were pre-tested at local market
• Comments used to select final versions of the drawings
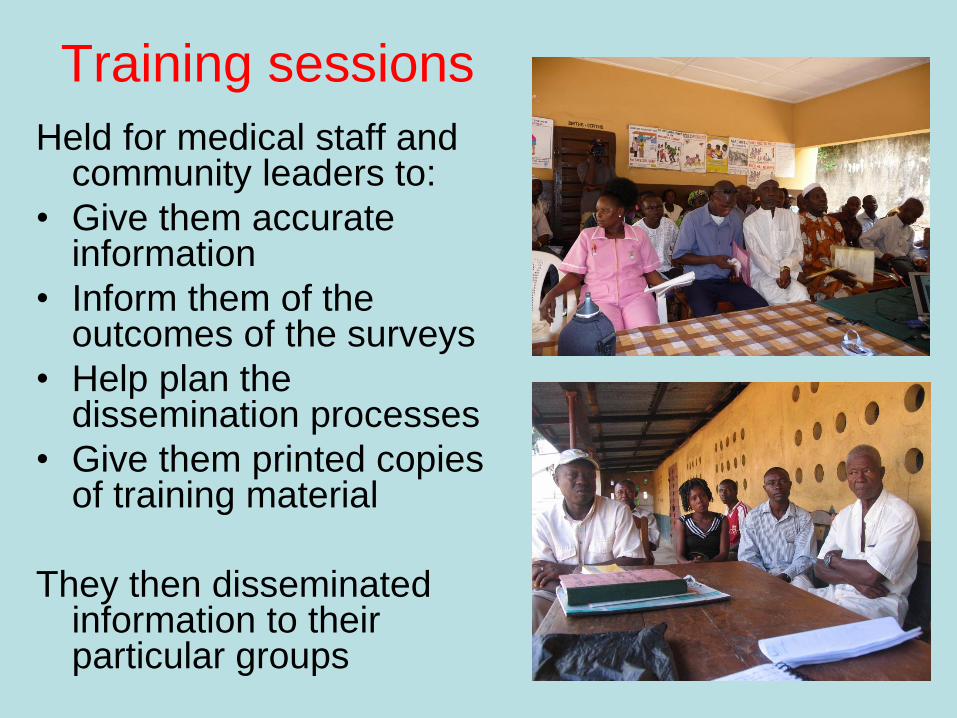
Training sessions
Held for medical staff and community leaders to:
• Give them accurate information
• Inform them of the outcomes of the surveys
• Help plan the dissemination processes
• Give them printed copies of training material
They then disseminated information to their particular groups

Importance of women
• Women:
– are the homecare givers
– as primary carers for the sick, are the key to effective care of H1N1 patients in the community
– Women’s associations are more active than the men’s
• At the request of the communities women were especially represented in the actions and training sessions
The Actions
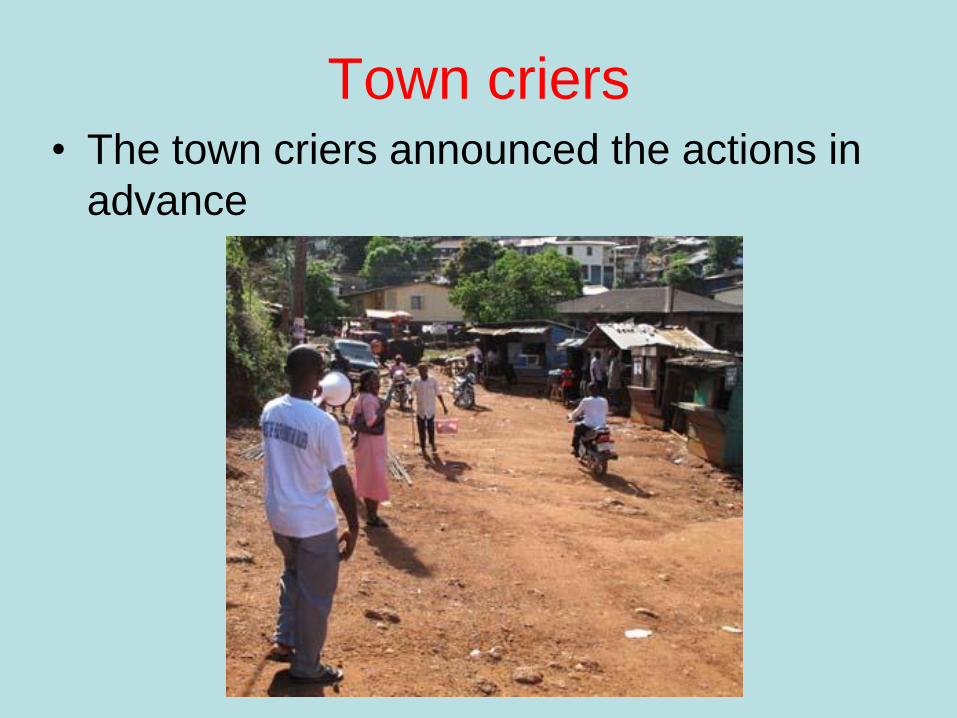
Town criers• The town criers announced the actions in
advance

Processions• Processions were held at both sites, moving
through the communities and the markets
drawing attention to the key messages
• Those in the processions wore T-shirts with the
messages and carried posters

Proceedings filmed and
photographed

Music, song and dance
• A brass band was
used at George
Brook to attract
attention to the
action
• The Sierra Leonean
singer Amie Kallon
composed a song
and a dance for use
at the action in
Blama

Drama groups
• Local drama groups produced short plays
and songs to highlight the different
messages

Reinforcing the
messagesLocal religious and
civic leaders
gave talks to
highlight the
importance of the
messages and
exhort their
people to take
note and follow
the messages

Children were
very much
involved

Evaluation of the results19th – 29th March 2010
Objectives of the evaluationPrimary objectives
1. Evaluate whether the actions were implemented as planned
Have outputs being delivered as planned (time and place?)
2. Evaluate the process
Has the message/activity reached the people for whom it was designed?
3. Assess the behavioural impact of the information package
As result of the communication activities, what are people
doing now?
Secondary objectives
• Assess the community’s perception of the home-based care project
• Assess the local authorities (Ministry of Health, WHO country office) perception of the home-based care project
• Assess if there were any other consequences due to the project

Methods
Qualitative and quantitative evaluation methods used.
• Focus group discussions (FGD)
• Structured interviews (questionnaires)
• Unstructured observation/Behavioural observation
Results – Primary objectives1. Have outputs being delivered as
planned (time and place?)
2. Has message/activity reached the people for whom it was designed?
3. As result of the communication activities, what are people doing now?
1. Yes
2. An increased understanding of:– influenza AH1N1
– the importance of washing hands with water and soap
– the importance of covering their nose and mouth to avoid the spread of the virus
Increases in overall knowledge about the disease in both communities. But this varied substantially between the rural and the urban sites.
3. Some schools are promoting hand washing and the use of handkerchiefs
But
Most people are not putting home care information into practice
Results – secondary objectives
1. A great acceptance of this project’s
approach both by the communities and by
the national authorities (Ministry of Health
and WHO)
2. An increased enthusiasm and a high level
of interest by the communities in health
issues

Overall conclusions #1Difference between implementation and uptake of the messages
between the urban (GB) and rural (Blama) sites with the former having a grater implementation and uptake.
• Possibly – because people of GB receive more health information than those of
Blama via the media.
– higher level of involvement by the community leaders in GB (the urban site) than in Blama (the rural site).
Community leaders are very important stakeholders when implementing and following up on community level activities.

Overall conclusions #2The most efficient means of conveying
the messages:
• Via community channels at the grass roots level (more effective than mass media such as radio and TV)
• In GB, town crier and drama group performances enhanced interest and kept people informed
• In Blama, Amie Kallon’s original song on influenza was selected as the best information channel
• The impact of posters was very low

Any Questions?