hiv and cardiovascular disease - .: regency :. · r e c a d r i s k i n h i v ? yes ... hiv and...
TRANSCRIPT
HIV and
Cardiovascular Disease
Joseph Cofrancesco Jr. MD, MPH, FACPAssociate Professor of Medicine
Director, Institute for Excellence in Education
Johns Hopkins University School of Medicine
Objectives
• Detail the CV risk of HIV+ patients:
– HIV
– ARV Treatment
• ARV that may be associated with � CV risk
– Traditional Risk Factors

Case

George Bush• 48 year old male new to your practice
• HIV+ 8 years and “feels great”
• PMH: “Sometimes my blood pressure is high”
• FH: “I’m adopted”
• SH: Heterosexual, monogamous (“1 slip”), works
as government official
– Exercises 3x week
– Alcohol: None in >5 years (History of alcohol abuse)
– Smokes : 1+ ppd x 22 years
– No illicit drug use

GB• Medication: ABC/3TC and LVP/r
• PE: Well appearing BMI 28, 148/94, pulse 62,
afebrile (pain score 0)
– Normal exam
• Labs
– CD4= 538 cells/mm3
– VL<20 copies
– Lipids: 210 mg/dL, HDL 38 mg/dL
– Glucose (fasting): 107 mg/dL
– Hep B Immune, Hep C negative
– Reminder: WNL

Q1: Is George at risk for CVD?
1. Yes, equal to HIV negative, matched, peers
2. Yes, higher than HIV negative, matched, peers
• Because of HIV infection
3. Yes, higher than HIV negative, matched, peers
• Because of HAART
4. No, HIV is protective

#1: Is th
ere�CAD ris
k
in HIV?
Yes
But,
by how much
is debatable.

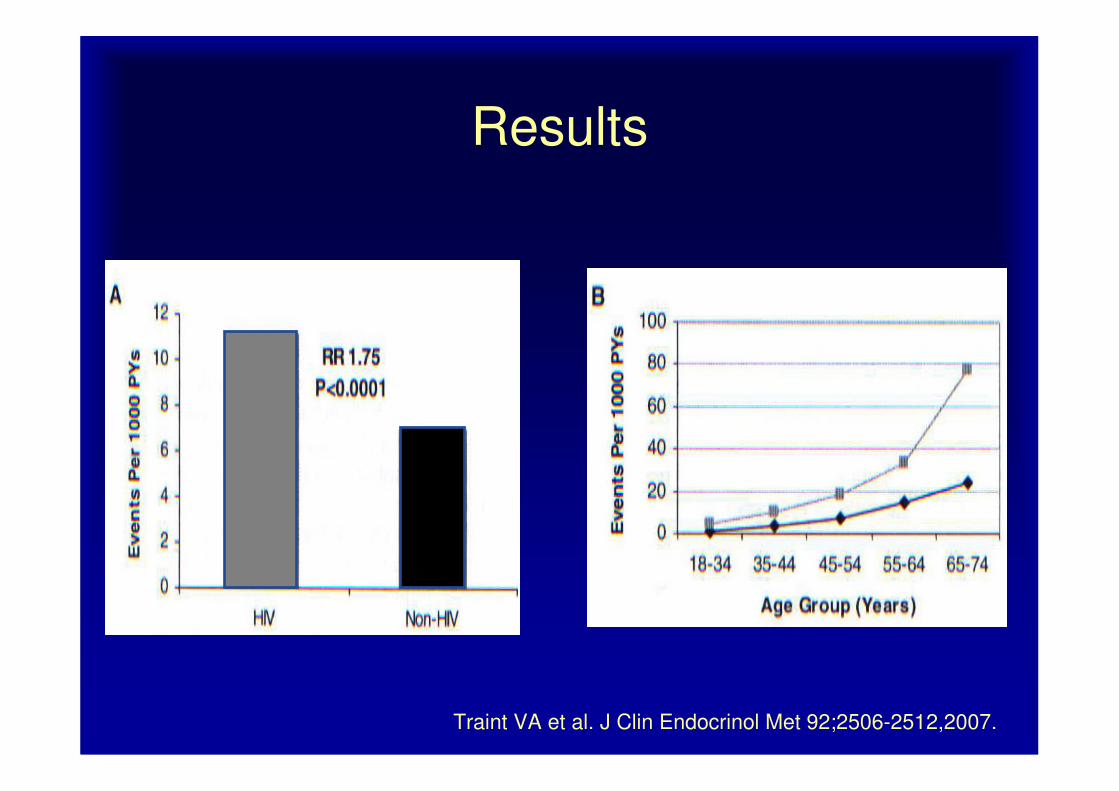
• Health system wide cohort
• HIV+ = 3,851 HIV - = 1,044,589
• October 1, 1996 – June 20, 2004
• MI: 189 HIV+, 26, 142 HIV-
• (Incomplete data on smoking)
Traint VA et al. J Clin Endocrinol Met 92;2506-2512,2007.
Traint VA et al. J Clin Endocrinol Met 92;2506-2512,2007.
Results

• Cross sectional
• Outpatient
• n=220 HIV +
• Belo Horizonte,
Brazil
Moreira Guimaraes MM et al. Int J Clin Pract, May 2010, 64,6:739-745

Moreira Guimaraes MM et al. Int J Clin Pract, May 2010, 64,6:739-745
Results

• Prospective, recruited
cohort– 78 HIV +,
– 32 HIV – (similar
recruitment)
• Recruitment– 4 community centers in
Boston, and newspaper
advertisements
• 64-slice CT
(Sensations64)
AIDS. 2010 Jan 16;24(2):243-53.

Relative Risk CVD: HIV+ vs. HIV-
Islam FM, et. al. Relative risk of Cardiovascular …, HIV Medicine. 2012

• HIV-infected participants:
– Diversity, 16 HIV/ ID clinics or cohorts
– geographic representative of US patients with HIV
• Control participants
– 2 centers, Coronary Artery Risk Development in
Young Adults (CARDIA) study
• Birmingham, Alabama
• Oakland, California
Grunfeld C et al. AIDS 2009, 23:1841-1849
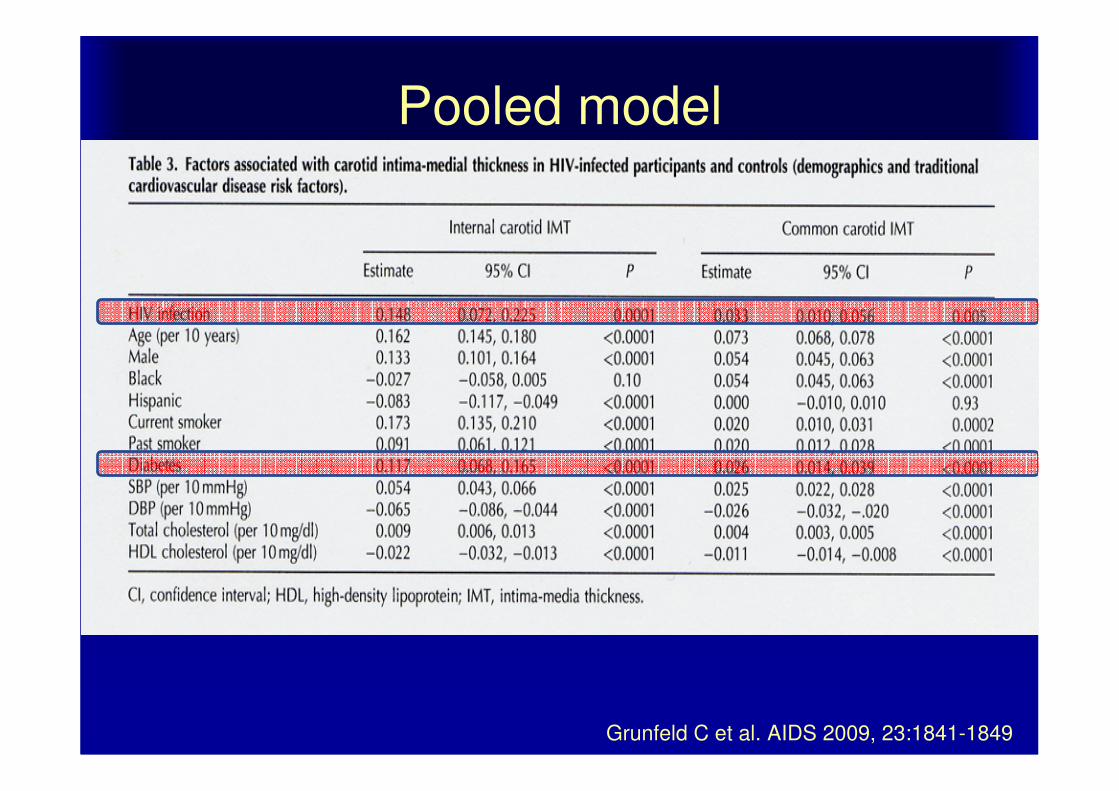
Pooled model
Grunfeld C et al. AIDS 2009, 23:1841-1849

But . . .
• Can you really fully “adjust”?
– Tobacco use in HIV 2-3 x higher
• Are we “over adjusting”
– Synergy of Risk Factors?
• Can you find true HIV negative comparators?
• Usual issues with Cohort studies, Retrospective
studies
– MI still relatively rare event
• Is Hep B, C considered?

#2: Does contro
lling H
IV
eliminate th
e excess
risk?
No, not all of it
Why not?

Relative Risk CVD
HIV+
vs. HIV -
HIV+ and
ART
vs.
HIV -
Islam FM, et. al. Relative risk of Cardiovascular …, HIV Medicine. 2012
CAD and Inflammation
• HIV+ without known CAD (n=27), well-controlled
disease – CD4 592±294 cells/mm3
– HIV RNA <48 copies/mL.
– On ART (duration 12±4 years)
• HIV neg (n = 27)
– matched for age, gender, and Framingham Score (FRS) no known CAD
• HIV neg, known CAD (n = 27)
Subramanian et al. CROI 2012 #121

CAD and Inflammation
• Arterial wall inflammation
– 18FDG-PET
– traditional and non-traditional risk markers
• including coronary calcium (CAC)
– marker of macrophage activation, sCD163.
• Arterial inflammation prospectively determined
– ratio of FDG uptake in the arterial wall of the ascending aorta/blood background [target to
background ratio (TBR)].
Subramanian et al. CROI 2012 #121

Results
Similar results subset (n = 22)
undetectable virus
(p = 0.0007)
Subramanian et al. CROI 2012 #121
In addition
• Aortic TBR remained significantly higher
restricted to
– Zero calcium, FRS <10, LDL <100 mg/dL (p ≤0.01).
• Aortic TBR was associated
– sCD163 (r = 0.53, p = 0.03)
– Not with C-reactive protein (CRP) or D-dimer (p>0.05).
Subramanian et al. CROI 2012 #121

HIV and Cardiovascular Disease:
Recommendations for Evaluation
• Part of initial patient visit
• Obtain baseline fasting lipid profile
– LDL-C, total cholesterol, HDL-
C, triglycerides
• Assess risk factors
– Family history, smoking,
diabetes, hypertension, obesity,
exercise
• Identify comorbidities and/or pre-existing conditions
– Pancreatitis, CAD, etc
• Change modifiable risk factors
• Promote lifestyle changes
• Offer treatment options
• Follow-up as needed
Initial Subsequent

#3: How much does
specific ARV
contribute?
Lots of debate
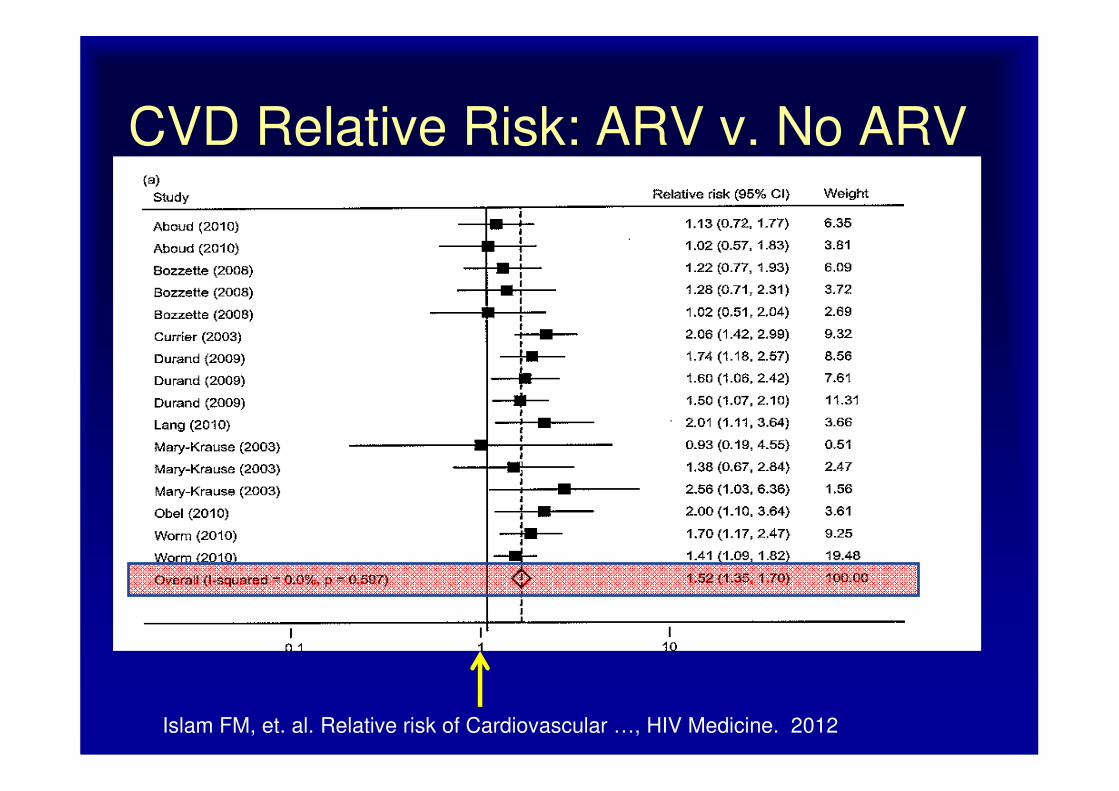
CVD Relative Risk: ARV v. No ARV
Islam FM, et. al. Relative risk of Cardiovascular …, HIV Medicine. 2012

ARV : � CAD Risk
• Indirectly, by � Traditional Risk Factors
– Lipids
– Glucose
– Body shape/fat
– ?Other inflammatory markers
• Directly
– Inflammation
– Arterial wall damage
– Coagulation factors
– Other
ARV : � CAD Risk
• Indirectly, by � Traditional Risk Factors
– Lipids
– Glucose
– Body shape/fat
– ?Other inflammatory markers
• Directly
– Inflammation
– Arterial wall damage
– Coagulation factors
– Other

0
10
20
30
40
50
60
70
Fontas E, et al. J Infect Dis. 2004;189:1056-1074.
ART-naïveNRTI + NNRTINRTI + PINRTI + dual PI
Pati
en
ts (
%)
TotalCholesterol(>240 mg/dL)
LDL-C(>130 mg/dL)
HDL-C(<35 mg/dL)
Triglycerides(>200 mg/dL)
Prevalence of Abnormal Lipids2

Total Cholesterol HDL LDL Triglycerides
Protease Inhibitors
Atazanavir (unboosted) ↔ ↔/↑ ↔ ↔
Atazanavir/ritonavir ↔ ↑ ↑ ↑
Darunavir/ritonavir ↔ ↔ ↑ ↑
Fosamprenavir/ritonavir ↑↑ ↑ ↑↑ ↑↑
Lopinavir/ritonavir ↑↑ ↔ ↑↑ ↑↑
Nelfinavir ↑↑ ↔ ↑↑ ↑
Saquinavir/ritonavir ↑ ↑ ↑↑ ↑↑
Tipranavir/ritonavir ↑↑ ↔ ↑↑ ↑↑
Malvestutto CD, Aberg JA. Coronary heart disease in people infected with HIV. Cleve Clin J Med 2010; 77(8):547-556.Hill A, Sawyer W, Gazzard B. Effects of first-line use of nucleoside analogues, efavirenz, and ritonavir-boosted protease inhibitors on lipid levels. HIV Clin Trials 2009; 10(1):1-12. Fontas E, van LF, Sabin CA, Friis-Moller N, Rickenbach M, d'Arminio MA, et al. Lipid profiles in HIV-infected patients receiving combination antiretroviral therapy: are different antiretroviral drugs associated with different lipid profiles? J Infect Dis 2004; 189(6):1056-1074.
PIs

Total Cholesterol HDL LDL Triglycerides
Non-nucleoside Reverse Transcriptase InhibitorEfavirenz ↑ ↑ ↑ ↑, ↑↑
Nevirapine ↑ ↑↑ ↑ ↑
Etravirine ↔ ↔ ↔ ↔
nNRTI
Malvestutto CD, Aberg JA. Coronary heart disease in people infected with HIV. Cleve Clin J Med 2010; 77(8):547-556.Hill A, Sawyer W, Gazzard B. Effects of first-line use of nucleoside analogues, efavirenz, and ritonavir-boosted protease inhibitors on lipid levels. HIV Clin Trials 2009; 10(1):1-12. Fontas E, van LF, Sabin CA, Friis-Moller N, Rickenbach M, d'Arminio MA, et al. Lipid profiles in HIV-infected patients receiving combination antiretroviral therapy: are different antiretroviral drugs associated with different lipid profiles? J Infect Dis 2004; 189(6):1056-1074.

NRTIsTotal
Cholesterol HDL LDL TG
Nucleoside reverse transcriptase inhibitorsAbacavir ↑ ↑ ↔, ↑ ↔, ↑
Lamivudine ( & FTC) ↔ ↔ ↔ ↔
Tenofovir DF ↔ ↔ ↔ ↔
Stavudine ↑ ↔ ↑ ↑↑
Zidovudine ↑ ↔ ↔ ↔
Malvestutto CD, Aberg JA. Coronary heart disease in people infected with HIV. Cleve Clin J Med 2010; 77(8):547-556.Hill A, Sawyer W, Gazzard B. Effects of first-line use of nucleoside analogues, efavirenz, and ritonavir-boosted protease inhibitors on lipid levels. HIV Clin Trials 2009; 10(1):1-12. Fontas E, van LF, Sabin CA, Friis-Moller N, Rickenbach M, d'Arminio MA, et al. Lipid profiles in HIV-infected patients receiving combination antiretroviral therapy: are different antiretroviral drugs associated with different lipid profiles? J Infect Dis 2004; 189(6):1056-1074.

OthersTotal
Cholesterol HDL LDL Triglyceride
sIntegrase strand transfer inhibitors
Raltegravir ↔ ↔ ↔ ↔
Entry Blockers
Maraviroc ↔ ↑, ↔ ↔ ↔
Enfuvirtide ↔ ↔ ↔ ↔
DeJesus E, et al 15th CROI, 2008; Boston # 929
ARV : � CAD Risk
• Indirectly, by � Traditional Risk Factors
– Lipids
– Glucose
– Body shape/fat
– ?Other inflammatory markers
• Directly
– Inflammation
– Arterial wall damage
– Coagulation factors
– Other

D:A:D Study Group. N Engl J Med. 2007;356:1723-1735.

Worm SW et al. JID 2010:201

CVD Relative Risk: PI v. non PI
Islam FM, et. al. Relative risk of Cardiovascular …, HIV Medicine. 2012
Similar
plots NRTI
or
NNRTI:
NO signal

AbacavirAbc causes heart
attacks, Never use
it!
Abc is
totally safe,
Always use it!

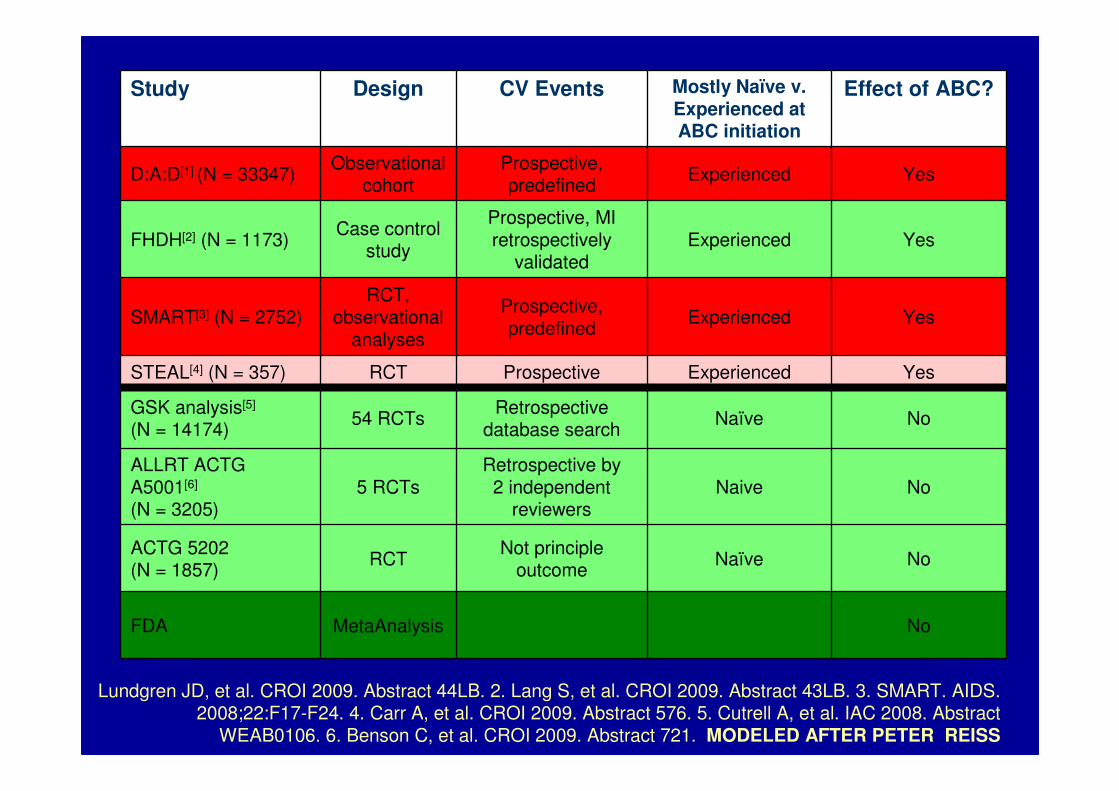
Study Design CV Events Mostly Naïve v. Experienced at ABC initiation
Effect of ABC?
D:A:D[1] (N = 33347)Observational
cohortProspective, predefined
Experienced Yes
FHDH[2] (N = 1173)Case control
study
Prospective, MI retrospectively
validatedExperienced Yes
SMART[3] (N = 2752)RCT,
observational analyses
Prospective, predefined
Experienced Yes
STEAL[4] (N = 357) RCT Prospective Experienced Yes
GSK analysis[5]
(N = 14174)54 RCTs
Retrospective database search
Naïve No
ALLRT ACTG A5001[6]
(N = 3205)5 RCTs
Retrospective by 2 independent
reviewersNaive No
ACTG 5202(N = 1857)
RCTNot principle
outcomeNaïve No
FDA MetaAnalysis No
Lundgren JD, et al. CROI 2009. Abstract 44LB. 2. Lang S, et al. CROI 2009. Abstract 43LB. 3. SMART. AIDS. 2008;22:F17-F24. 4. Carr A, et al. CROI 2009. Abstract 576. 5. Cutrell A, et al. IAC 2008. Abstract
WEAB0106. 6. Benson C, et al. CROI 2009. Abstract 721. MODELED AFTER PETER REISS
FHDH[2] (N = 1173)Case control
study
Prospective, MI retrospectively
validatedExperienced Yes -> NO
Study Design CV Events Mostly Naïve v. Experienced at ABC initiation
Effect of ABC?
D:A:D[1] (N = 33347)Observational
cohortProspective, predefined
Experienced Yes
FHDH[2] (N = 1173)Case control
study
Prospective, MI retrospectively
validatedExperienced Yes
SMART[3] (N = 2752)RCT,
observational analyses
Prospective, predefined
Experienced Yes
STEAL[4] (N = 357) RCT Prospective Experienced Yes
GSK analysis[5]
(N = 14174)54 RCTs
Retrospective database search
Naïve No
ALLRT ACTG A5001[6]
(N = 3205)5 RCTs
Retrospective by 2 independent
reviewersNaive No
ACTG 5202(N = 1857)
RCTNot principle
outcomeNaïve No
FDA MetaAnalysis No
Lundgren JD, et al. CROI 2009. Abstract 44LB. 2. Lang S, et al. CROI 2009. Abstract 43LB. 3. SMART. AIDS. 2008;22:F17-F24. 4. Carr A, et al. CROI 2009. Abstract 576. 5. Cutrell A, et al. IAC 2008. Abstract
WEAB0106. 6. Benson C, et al. CROI 2009. Abstract 721. MODELED AFTER PETER REISS

CVD Relative Risk: ABC
Islam FM, et. al. Relative risk of Cardiovascular …, HIV Medicine. 2012
Q2: If you could address only 1 issue, which has greatest impact on reducing CVD risk?
1. Change LVP/r � EFV
2. Change ABC/3TC � AZT/3TC
3. Have him quit smoking
4. Lower his total cholesterol to 170 mg/dL
5. Change his gender

#4: Traditio
nal Risk
Factors
Relative Risk
vs
Absolute Risk
Traditional Risk
Factors
ARV

CAD Risk Factors
Modifiable/Controllable
• Cigarette smoking
• HTN
• Dyslipidemia
• Diabetes mellitus
Not modifiable
• Gender
– M. more MIs, at older ages, F more likely to die from MI
• Advancing age
– Males >55
– Females >65
• FH premature CHD
– <55 years in men
– <65 years in women
• Obesity
• Physical inactivity
• (Psychosocial)• CKD
• Microabluminuria
• GFR <60 mL/Min

George Bush• 48 year old
• Male
• HIV+
• Smokes : 1 ppd x 12 years
• BP = 148/94
• TC: 210 mg/dL, HDL 38 mg/dL

Framingham Risk: Baseline
Does NOT take into account:- DM (= CVD risk equivalent)- FH- HIV
And, he’s only 48years old, I’m
concerned about the next 50 years!

Framingham Risk: Female
Baseline Risk = 17%

Framingham Risk: BP Controlled
Baseline Risk = 17%

JNC 7 (JNC 8 expected Spring 2012)
JNC 7: U . S . Department of Health and Human Services , National Institutes
of Health National Heart, Lung, and Blood Institute
‡ Treat patients with CKD or DM to BP goal of <130/80 mmHg.

Treatment
Lifestyle
• Low sodium diet
• Weight loss if obese
• Aerobic exercise
• EtOH:
> 2/day, 1.5 to 2-fold �incidence (v. nondrinkers), esp at > 5/day
Moderate alcohol intake �CAD
ABCDs of Pharmacology
• ACE Inhibitor, ARB
• B. blocker
• Calcium channel blocker,
• Diuretic (Thiazide)
• Patients with BP > 20/10 above goal will need
combination therapy

Framingham Risk: Lipids Controlled
Baseline Risk = 17%

NCEP
http://circ.ahajournals.org/cgi/content/full/106/25/3143
http://www.nhlbi.nih.gov/guidelines/cholesterol/atp3full.pdf

NCEP ATP III LDL Targets
mg/dL
CHD + CHD risk equivalent <100 (<70)
Multiple (2+) RF <130
-if 10 year risk > 20% <100
0-1 RF <160
Should HIV count as an additional RF?

Comparing Statins
• Retrospective Cohort, 2 clinics (n=700)
• Results: (compared to Pravastatin (N=280):
– Atorvastatin (N=303) and Rosuvastatin (N =95)
• Greater � LDL and non HDL cholesterol
• Higher likelihood of reaching NCEP LDL targets
– Rosuvastatin also higher likelihood of reaching non HDL target
• Toxicities: similar
Singh S et al. CID 2011: 52
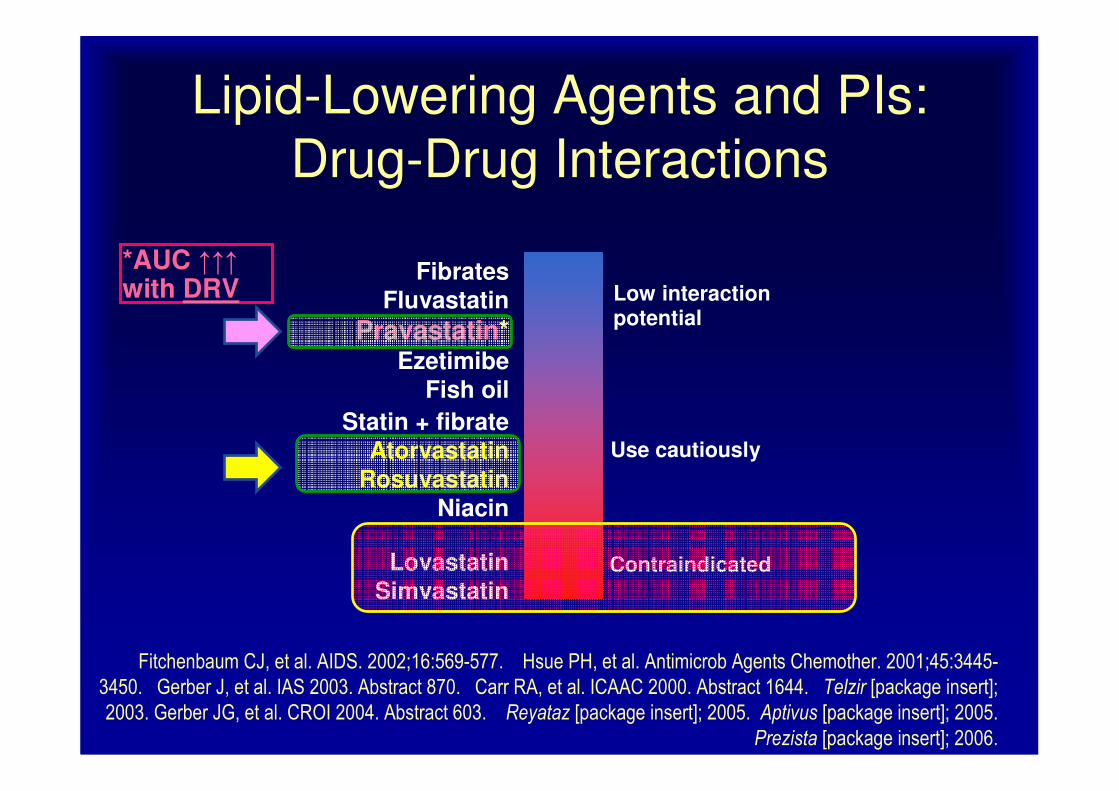
Lipid-Lowering Agents and PIs:
Drug-Drug Interactions
*AUC ↑↑↑with DRV
FibratesFluvastatin
Pravastatin*Ezetimibe
Fish oil
Use cautiously
Statin + fibrateAtorvastatin
Rosuvastatin
Niacin
LovastatinSimvastatin
Contraindicated
Low interactionpotential
Fitchenbaum CJ, et al. AIDS. 2002;16:569-577. Hsue PH, et al. Antimicrob Agents Chemother. 2001;45:3445-
3450. Gerber J, et al. IAS 2003. Abstract 870. Carr RA, et al. ICAAC 2000. Abstract 1644. Telzir [package insert];
2003. Gerber JG, et al. CROI 2004. Abstract 603. Reyataz [package insert]; 2005. Aptivus [package insert]; 2005.
Prezista [package insert]; 2006.

Framingham Risk: BP and Lipids
Controlled
Baseline Risk = 17%


Q3: What do you think the 10 year
risk will be if he was a nonsmoker?
1. 20% (Stress of smoking cessation �s risk)
2. 16% (akin to BP control)
3. 11% (akin to lipid control)
4. 6% (akin to gender effect)
5. 4%
Baseline Risk =
17%

Framingham Risk: No Smoking
Baseline Risk = 17%
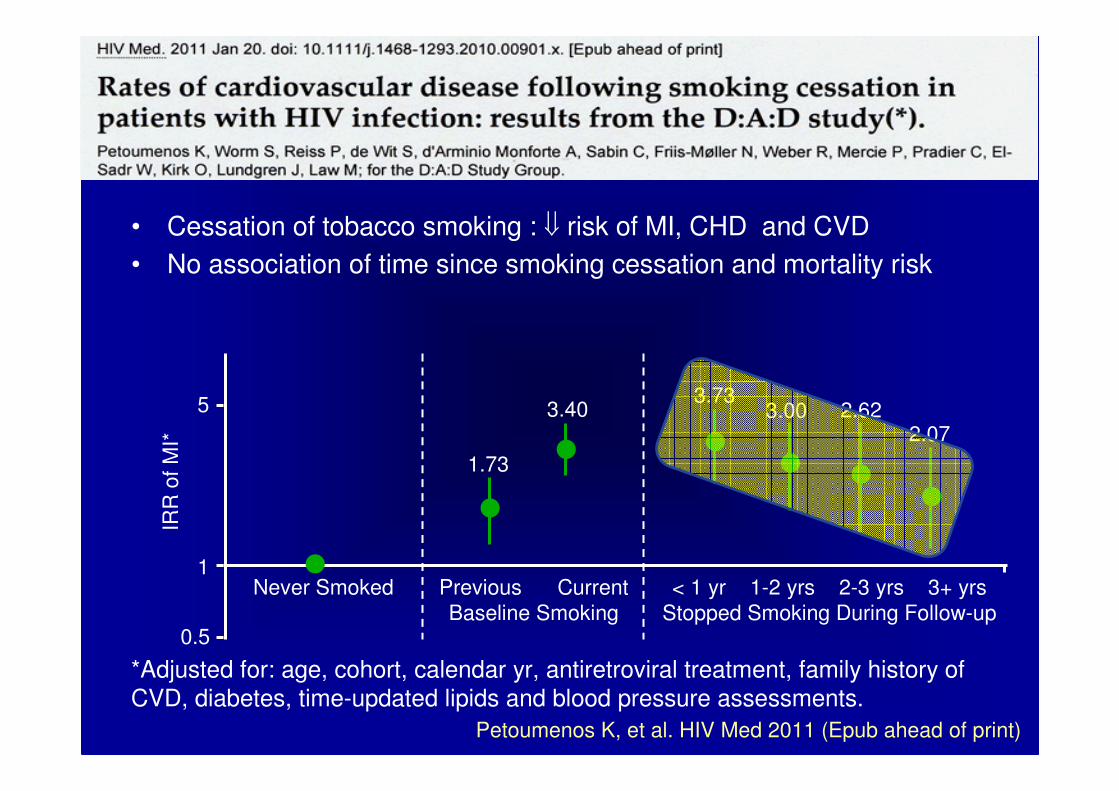
• Cessation of tobacco smoking : ⇓ risk of MI, CHD and CVD
• No association of time since smoking cessation and mortality risk
Petoumenos K, et al. HIV Med 2011 (Epub ahead of print)
*Adjusted for: age, cohort, calendar yr, antiretroviral treatment, family history of
CVD, diabetes, time-updated lipids and blood pressure assessments.
Never Smoked Previous Current
Baseline Smoking
< 1 yr 1-2 yrs 2-3 yrs 3+ yrs
Stopped Smoking During Follow-up
5
IRR
of
MI*
1
0.5
1.73
3.403.73
3.00 2.622.07

Cigarette Cessation
• Offer treatment at each visit
– Most smokers make many attempts
– Specialty clinic or smoking cessation program
• Unwilling to quit: “5 R's" motivational
– Relevance, Risks, Rewards, Roadblocks, and Repetition
• Willing to quit: “5 A's"
– Ask, Advise, Assess, Assist, and Arrange
• Practical counseling:
– Problem solving/skills training; social support
• Person-to-person contact
http://www.uptodate.com/contents/smoking-cessation

Pharmacotherapy + Other
• Nicotene replacement– Transdermal patch
– Gum
– Lozenge
– Inhaer
– Spay
• Medication– Bupropion
– Varenicline
• Hypnosis
• Acupunture
• Most smokers make many attempts
• Specialty clinic or smoking cessation program

Framingham Risk: No Smoking, BP
and Lipid Control
Baseline Risk = 17%

• Men 45-79, when potential benefit � MI > potential
harm of �of GI bleed. (A recommendation)
• Women 55-79, when the potential benefit �
ischemic strokes > potential harm of �of GI bleed.(A recommendation)
Ann Int Med. 2009;150: 396-404
Conclusions

HIV
ARV
Traditional Risk
Factors
CardiovascularDisease
Conclusions
• CVD will be an increasing issue for our patients
– Providers need to be aware
• Controlling HIV � � Risk
– Selecting ARV may be better than others
• Focus on Traditional RF
– Tobacco use
– Lipids, HTN, glucose control
– ASA where appropriate
• High level of suspicion for CAD

No Smoking