high-dose oral ambroxol for early treatment of pulmonary...
TRANSCRIPT
High-dose Oral Ambroxol for Early Treatmentof Pulmonary Acute Respiratory DistressSyndrome an Exploratory Randomized
Controlled Pilot Trialby Arun K Baranwal1 Aparna S Murthy2 and Sunit C Singhi2
1All India Institute of Medical Sciences Patna-801507 India2Postgraduate Institute of Medical Education and Research Chandigarh-160012 India
Correspondence Arun K Baranwal Additional Professor amp Head Department of Pediatrics All India Institute of Medical Sciences Patna801507 India Tel thorn91-7766908325 E-mail ltbaranwal1970gmailcomgt
A B S T R A C T
Objective To evaluate efficacy of high-dose oral ambroxol in acute respiratory distress syndrome(ARDS) with respect to ventilator-free days (VFD)
Design Prospective randomized placebo-controlled blinded pilot trialPatients Sixty-six mechanically ventilated patients (1 month to 12 years) with ARDS who were
hand-ventilated for lt24 hr before pediatric intensive care unit admissionInterventions Patients randomized to oral ambroxol (40 mgkgday in four divided doses)
(nfrac14 32) or placebo (nfrac14 34) until 10 days extubation or death whichever is earlierMeasurements and Main Results Majority (91) had pneumonia and bronchiolitis Two study
groups were similar in baseline characteristics Mean partial pressure of arterial oxygenfraction ofinspired oxygen and oxygenation index were gt175 and lt10 respectively with no difference in thetwo study groups VFD were similar in the two study groups Overall mortality was 26 No adverseevents were noted with ambroxol
Conclusions Among ventilated pulmonary ARDS patients with oxygenation index of lt10mortality was 26 Ambroxol did not improve VFD Study with higher and more frequently admin-istered doses of ambroxol in larger sample is suggested after having generated relevant pharmacoki-netic data among critically ill children
K E Y W O R D S ambroxol acute respiratory distress syndrome children ventilator-free days in 14days
I N T R O D U C T I O NAcute respiratory distress syndrome (ARDS) in chil-dren is usually caused by ldquodirectrdquo pulmonary causes[1] more so in resource-poor economies [2 3]Release of cytokines and oxidants proteasendashantipro-tease imbalance surfactant deficiency and alveolarbiofluid overproduction are final common pathways
irrespective of cause Despite pathologic understand-ing of ARDS its management continues to be chal-lenging Though lung-protective ventilatory strategyimproved outcome [4] search for an effective drugcontinues [5] Majority of pharmacotherapeuticinterventions eg steroid [6] anti-oxidants [7 8]surfactant replacement [9] and b-agonists [10 11]
VC The Author [2015] Published by Oxford University Press All rights reserved For Permissions please email journalspermissionsoupcom
339
Journal of Tropical Pediatrics 2015 61 339ndash350doi 101093tropejfmv033Advance Access Publication Date 30 June 2015Original Paper
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
have targeted a single pathway of otherwise complexprocess and failed Drug acting on multiple patho-genetic pathways may succeed clinically [8]
Ambroxol has mucoactive [12] anti-inflamma-tory anti-oxidant and surfactant-promoting proper-ties [13] Moreover it gets concentrated selectivelyin lungs [14] Though clinical data are scanty[14ndash18] ambroxolmdasha safe and economical drugmdashmay be considered for treatment of ARDS for itspotential to improve gas exchange [19ndash21] Ifclinical efficacy could be established ambroxol wouldbe an attractive therapeutic option for its low costand toxicity Current exploratory randomizedblinded controlled pilot trial was designed to evalu-ate efficacy of high-dose oral ambroxol in children(age 1 month to 12 years) requiring ventilation forpulmonary ARDS (pARDS) with specific referenceto ventilator-free days in 14 days (VFD14) in re-source-constraint setting Improvement in ventila-tory and oxygenation parameters were secondaryobjectives
M A T E R I A L S A N D M E T H O D S
PatientsAll intubated ventilated patients in 12-bed pediatricintensive care unit (PICU) were screened for studyeligibility each day over 14-month period (August2007ndashSeptember 2008) Entry criteria included allconsecutive children (age 1 month to 12 years) withrespiratory failure owing to diffuse bilateral pulmon-ary infiltrates partial pressure of arterial oxygen(PaO2)fraction of inspired oxygen (FiO2) 300positive end expiratory pressure (PEEP) 5 cmH2O and ventilated for 12 hr [22] Patients withpersistent hypotension (defined as systolic bloodpressure lt5th centile [70 mmHg thorn2 age in years])despite resuscitation for initial 12 hr were excludedto avoid indirect lung injury and to concentrate onpARDS only considering higher biological plausibil-ity of ambroxol in the later Patients hand-ventilatedfor gt24 hr before mechanical ventilation wasexcluded to limit risk of significant barotraumaPatients with active bleeding requiring bloodfluidvolume replacement chronicrestrictive lung diseasereactiveupper airway disease neuromuscular re-spiratory failure raised intracranial pressure
congenital valvular or myocardial heart disease car-diogenic pulmonary edema andor post-operativepatients were excluded to limit confounders Patientswith acute renal failure were excluded as ambroxol isexcreted mainly from kidneys
Study drugOral ambroxol is used for treatment of pulmonarydiseases and reported to be safe [23] Higher intra-venous doses in adults (1000 mgday) [14 16] andpreterm newborns (30 mgkgday 7 days) [15 24]were also safe Orally administered ambroxol gets ab-sorbed rapidly with 73 bioavailability with time topeak plasma concentration being 2 hr in an adultstudy [25] Elimination t12 is biphasicmdashwith an at12 of 13 hr and b t12 of 88 hr [25] Thus 40mgkgday (in four divided doses) may be con-sidered to be an acceptable maximal safe oral dosefor children Though intestinal absorption in critic-ally ill patients is different from healthy person thisdose was considered as starting point for the pilotstudy
Study protocolTrial was designed and analyzed according toConsolidated Standards of Reporting Trials recom-mendations and checklist (Fig 1) [26] After in-formed consent from fatherlegal guardian eligiblepatients were randomized to intervention or placebousing computer-generated random number tablewithin 24 hr of PICU admission Study assignmentswere serially numbered in opaque and sealed enve-lopes Intervention group received oral ambroxol(40 mgkgday) in four divided doses for 10 days oruntil extubation whichever was earlier Identical-looking tablets of ambroxol (of 50 mg) and placebowere prepared and packs containing dosage for 20kg body-weight patient were dispensed Tablets werecrushed suspended in water and administeredthrough nasogastric tube Investigators doctorsnurses and data manger were blinded to treatmentassignment Institutional ethics committee approvedthe study protocol
At enrollment patientsrsquo demographics baselineassessment and Pediatric Risk of Mortality III(PRISM-III) were recorded Vitals oxygen saturationon pulse oximeter (SpO2) and central venous
340 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
pressure (if required) were monitored continuouslyand recorded 2 hourly Ventilator settings bloodgases end-tidal CO2 and chest radiograph data werecollected for initial 28 days or until extubationwhichever was earlier In addition pulmonary statusand respiratory support extubation readiness fluidbalance caloric and protein intake and pediatric
logistic organ dysfunction (PeLOD) score [27] re-corded Investigations were recorded if available andreflected the values obtained closest to 0800 am
Patients in both groups were managed accordingto prevalent unit protocol for ventilation sedationhemodynamics nutrition extubation readiness andgeneral nursing care Lung-protective ventilation was
Paents fulfilled inclusion criteria (n=89)
Randomized (n=67)
Allocated to Placebo (n=34)
Received allocated intervenon (n=34)
Did not receive allocated intervenon (n=0)
Allocated to Ambroxol (n=33)
Received allocated intervenon (n=32)
Did not receive allocated intervenon (n=0)
Lost to follow up (n=0)
Disconnued intervenon (n=0)
Lost to follow up (n=0)
Disconnued intervenon (n=1)
( for acute renal failure within 2 days)
Included in Analysis (n=34)
Excluded from Analysis (n=0)
Included in Analysis (n=32)
Excluded from Analysis (n=1)
22 Excluded 2 Parents refused to parcipate 4 Missed enrollment window 2 Chronic Lung Disease 2 Neuromuscular Weakness 3 Raised Intracranial Pressure 2 Postoperave Paents 3 Acute Renal Failure 4 Refractory Shock
Fig 1 Patient flowchart through clinical trial
High-dose Oral Ambroxol for pulmonary ARDS 341
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
employed and included pressure-control ventilationwith peak inflating pressure lt30 cm H2O PEEP5ndash10 cm H2O tidal volume 5ndash6 mlkg FiO2 lt06and permissive hypercapnea (PaCO2 gt80torr whilepH gt725) if required Aim was to achieve optimaloxygenation (PaO2 60ndash80 mmHg SpO2 88ndash92)while limiting barotrauma Sedation protocolinvolved continuous diazepam (midazolam in some)and morphine infusions to achieve and maintainRamsay Score of 3ndash4 [28] with morning sedationinterruption Intravenous fluid was initiated as 23maintenance and feed was introduced at the earliestOnce patients were on full feed volume was relaxedto full maintenance After achievement of spontan-eous breathing oxygenation index (OI) lt6 decreaseandor plateau in ventilator support over 12 hourspatients were tested for extubation readiness Patientstatus was verified at discharge from PICU If diedprimary and secondary causes of death were re-corded Adverse events were monitored and reportedto Institutional Ethics Committee
Study outcomesConsidering difficulty in achieving mortality benefitin current critical care scenario [29] and unclear con-tribution of ARDS to mortality [30] composite out-come measure like ventilator-free days (VFD)incorporating both mortality and ventilation dur-ation are being considered [31] Primary outcomewas VFD14 which is defined as number of daysfrom point of successful weaning to day 14 (D14) ofenrollment Death during first 14 days is consideredto be equivalent to unresolved respiratory failureand thus is equated to zero VFD14 Secondary out-come measures included all-cause mortality ventila-tor days among survivors number of patients aliveand ventilator-free on D14 time-to-recovery fromARDS (ie when patients met extubation readinesscriteria after randomization) changes in ventilationand oxygenation parameters
Statistical analysisSimple unrestricted randomization was used to allo-cate patients in two groups Nonparametric MannndashWhitney U test and X2 test (or Fisherrsquos exact test ifrequired) were used to compare groups with quanti-tative outcomes Survival analysis using KaplanMeier curves was performed for time-to-event data
eg ventilation duration time-to-recovery and PICUstay Repeated measures analysis of variancewas planned to assess trend in ventilation and oxy-genation parameters SPSS version 16 was used forstatistical analysis A plt 005 was consideredsignificant
R E S U L T SOut of 67 eligible patients 33 were randomized toambroxol while 34 to placebo (Fig 1) Per-protocolanalysis was performed after excluding one patient inambroxol group who developed acute renal failureon day 2 leading to discontinuation of drugManagement included unmonitored hand-ventilationwith self-inflating bag for initial few hours (usuallyupto 24 h) in emergency room (ER) or pediatricwards (PWs) before PICU admission as more oftenthan not ventilator was not available for immediateapplication Of 66 patients 42(64) had moderateto severe ARDS (PaO2FiO2 200) [22] at ran-domization Thirteen of the remaining 24 patientswho had mild ARDS (PaO2FiO2 201ndash300) at en-rollment progressed in severity subsequently Twogroups were comparable for demographic profile nu-tritional status severity of illness at randomizationdiagnoses metabolic profile cause of lung injury aswell as in baseline respiratory characteristics (Tables1 and 2) Bronchopneumonia and bronchiolitis werethe commonest (91) causes of pARDS Three pa-tients (45) had chemotherapy-induced febrile neu-tropenia Eight (12) (four in each group) patientshad positive blood culture at PICU admissionmdashStaphylococcus aureus (3) Burkholderia cepacia (2)Acinetobacter (1) E coli (1) and Candida (1)
VFD14 was similar in two groups (pfrac14 056) sowas time-to-recovery from ARDS and other clinicaloutcomes (Table 3 and Fig 2) PaO2FiO2 OIneed for PEEP tidal volume and PaCO2 were alsosimilar during first 14 days (Figs 3 and 4) Healthcare associated infections (HCAIs) were seen in25(38) patients more in placebo group (1634 vs932 pfrac14 011) Out of these 19(76) were culturepositive gram-negative bacilli (14) being the com-monest (Candia 4 Staphylococcus 3) Blood-stream infections (14) were commonest followed byurinary tract infections (11) All-cause mortality was258 (1766) with similar distribution of early
342 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
(lt3 days) or late (gt3 days) deaths in the twogroups ARDS was considered as primary cause ofdeath in 53 (917) patients three of them wereimmunocompromised Forty-one percent (717)
of deaths were ascribed to HCAIs while onesuccumbed to hyperkalemia-induced arrhythmiaAmong survivors median (interquartile range) venti-lation duration was 7 (6) and 8 (45) days inambroxol and placebo groups respectively Diarrheawas noted in 6 (19) patients receiving ambroxolOne patient developed renal failure on D2 ofambroxol Serial blood pressure and cardiac compo-nent of PeLOD score were comparable in the twogroups during first 14 days contrasting the experi-mental data [33]
Table 1 Baseline patientsrsquo characteristics atenrollment
Characteristics Placebo(nfrac14 34)
Ambroxol(nfrac14 32)
Age (year) median (IQR) 115 (322) 137 (342)Age Number ()lt 1 year 16 (47) 13 (40)1ndash5 years 11 (32) 14 (44)gt5 years 7 (21) 5 (16)
Sex ratio (MF) 2311 2210Nutritional status (reference NCHS median)a
Normal (gt80) 18 (56) 17 (50)PEM grade 1 (71ndash80) 5 (16) 4 (12)PEM grade 2 (61ndash70) 5 (16) 8 (24)PEM grade 3 (51ndash60) 3 (9) 5 (15)PEM grade 4 (50) 1 (3) 0 (0)Serum albumin at
admission median(IQR) gmdl
229 (088) 260 (100)
Number ofpatients withhypoalbuminemia()b
24 (706) 23 (719)
PRISM III scoremedian (IQR)
500 (700) 600 (775)
PeLOD scoremedian (IQR)c
550 (1000) 1000 (1000)
Cause of pARDSPneumonia 29 (85) 27 (84)Bronchiolitis 5 (15) 1 (3)Kerosene poisoning 0 (0) 2 (6)Aspiration pneumonia 0 (0) 1 (3)Pulmonary hemorrhage 0 (0) 1 (3)
Blood culture positive 4 (12) 4 (13)Febrile Neutropenia 2 (6) 1 (3)
IQRfrac14 interquartile range PEMfrac14 protein energy malnutritionpARDSfrac14 Pulmonary Acute Respiratory DistressaMalnutrition was graded based on the criteria defined by IndianAcademy of PediatricsbHypoalbuminemia was defined as an albumin level of lt34 gdl for pa-tients gt7 months and lt25 gdl for patients lt7 months [32]cPeLOD Pediatric Logistic Organ Dysfunction (non-pulmonary) Score
Table 2 Baseline respiratory characteristics atenrollment
Respiratory characteristics Placebo(nfrac14 34)
Ambroxol(nfrac14 32)
PaO2FiO2 ratioa
mean (SD)1771 (707) 1906 (816)
Severity of ARDSnumber ()Mild ARDS
(PF ratio 201ndash300)10 (29) 14 (44)
Moderate ARDS(PF ratio 101ndash200)
20 (59) 14 (44)
Severe ARDS(PF ratio 100)
4 (12) 4 (12)
PEEP mean (SD) 65 (25) 62 (16)Quantitative pulmonary involvement
(as per chest radiograph)1 quadrant 0 (0) 0 (0)2 quadrant 2 (6) 2 (6)3 quadrant 7 (21) 6 (19)4 quadrant 25 (73) 24 (75)MAP mean (SD) 123 (51) 117 (42)OI mean (SD) 95 (108) 76 (46)VT (mlkg) mean (SD) 57 (17) 54 (13)PIP mean (SD) 194 (69) 186 (42)
Murrayrsquos lung injury scoreMild to moderate
(01ndash25)26 (76) 22 (69)
Severe (gt25) 8 (24) 10 (31)
IQRfrac14 interquartile range SDfrac14 standard deviation PaO2frac14 partial pres-sure of arterial oxygen FiO2frac14 fraction of inspired oxygenPEEPfrac14 positive end expiratory pressure PIPfrac14 peak inflating pressureMAPfrac14mean airway pressure OIfrac14 oxygenation Index VTfrac14 tidalvolumeaArterial blood gases in both groups were assessed at 0800 hours daily
High-dose Oral Ambroxol for pulmonary ARDS 343
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
D I S C U S S I O NCurrent study add to scarcely available data on clin-ical characteristics and outcomes of ventilated pediat-ric ARDS patients from developing economies [2 334] Ours being a tertiary care hospital without refer-ral and transport system we usually receive patientsvery late Thus patients are likely to be the severestof lot Pneumonia and bronchiolitis were commonest(90) causes of ARDS making it a syndrome ofrelatively homogeneous etiology in our setting as
against 40ndash65 reported from industrialized econo-mies (Table 4) PRISM-III score calculated fromdata collected during first 24 h of PICU admissionwere comparable with that in other pediatric ARDSstudies [35 37] However as all of our patients wereresuscitated and received post-resuscitation support-ive care (including hand-ventilation) for significantperiod in ERPWs before being shifted to PICUmany vital signs might have improved by the timethey reached PICU Thus actual PRISM-III scoresat beginning of hand-ventilation in ERPWs is likelyto be higher than ones calculated at PICU admissionmaking them sicker than what got reflected inPRISM-III scores All-cause mortality (of 26) is sig-nificantly higher compared with industrializedeconomies (Table 4) after factoring in higher meanPaO2FiO2 (gt175) lower mean OI (lt10) andlesser number of patients with immunocompromisedstatus Poor referral advanced stage of illness at ad-mission and suboptimal post-resuscitation care inERPWs may be one set of possible causative fac-tors While in PICU suboptimal patientsndashnurseratio poorly trained critical care nurses and poor in-fection control practices may be another These arethe issues of concern and indicate potentials of im-provement in critical care in the study settings
Early treatment was planned to have potentialbeneficial effects of ambroxol early during acute phase
Table 3 Primary and secondary outcome variables
Outcome Placebo (nfrac14 34) Ambroxol (nfrac14 32) pa
Primary outcome variableVentilator-free days at D14 (VFD14)b 50 (70) 50 (97) 056Ventilator-free days at D14 (VFD14) (mean 6 SD) 44 (36) 50 (45) ndash
Secondary outcome variablesAlive and ventilator-free at D14c 24 (71) 21 (66) 045Ventilator days among survivorsb 80 (45)(nfrac14 25) 70 (60) (nfrac14 24) 055Number of days to recover from ARDSd among survivorsb 100 (50)(nfrac14 25) 85 (70)(nfrac14 24) 054PICU stay among survivors (day)b 1200 (500) 1150 (775) 042All-cause mortalityc 9 (26) 8 (25) 089Early deaths (3 days)c 3 (38) 4 (44) 077Late deaths (gt3 days)c 5 (62) 5 (56)
ap-values are based on MannndashWhitney U test for number of VFD14 ventilator days among survivors time-to-recovery from ARDS duration of PICUstay v2 test (or Fisher Exact Test) for number of patients alive and ventilator-free at day 14 all-cause mortalitybData expressed as median (interquartile range)cData expressed as number (percentage)dAmong survivors number of days from randomization to meeting extubation readiness criteria for 24 consecutive hours through day 14
Time to recovery (Days)6050403020100
Cum
ulat
ive
a
t giv
en ti
me
10
08
06
04
02
00
placebo-censoreddrug-censoredplacebodrug
Study Groups
Fig 2 KaplanndashMeier curves comparing time-to-recoveryfrom ARDS in the two groups (censored for in-PICUmortality Log-Rank test pfrac14 094)
344 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
(a)
(b)
(c)
0
10
20
30
40
50
60
70
0 2 4 6 8 10 12 14 16
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
OI
0
100
200
300
400
500
600
700
0 5 10 15
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
PF
0
2
4
6
8
10
12
14
16
18
0 5 10 15
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
PEEP
Fig 3 Dot plot showing trend of mean PaO2FiO2 ratio oxygenation Index and PEEP during first 14 days
High-dose Oral Ambroxol for pulmonary ARDS 345
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
of illness We demonstrated safety tolerance and roleof high-dose oral ambroxol (40 mgkgday in fourdivided doses) in ventilated pARDS patients for thefirst time Ambroxol failed to improve oxygenationventilation VFD time-to-recovery mortality and thusto suggest therapeutic potential in pARDS in thestudy setting owing to small sample size Two-thirdsof patients had hypoalbuminemia and thus gut edema
possibly affecting ambroxolrsquos bioavailability Dosagechosen was maximal safe dose based on availableclinical data Therapeutic efficacy and safety of fur-ther higher dose may be subject of future scrutinyHigher doses may also be helpful in eradicating patho-gens adhered to bronchiolaralveolar epithelium [39]Ambroxol selectively gets concentrated in lungswithin 3 min of intravenous administration but it falls
(a)
(a)
0
50
100
150
200
250
0 2 4 6 8 10 12 14 16
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
PaCO
2
0
2
4
6
8
10
12
14
0 2 4 6 8 10 12 14 16
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
TV
FIG 4 Dot plot showing trend of mean tidal volume and PaCO2 during first 14 days
346 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
Tab
le4
Com
pari
son
ofcl
inic
alch
arac
teri
stic
san
dou
tcom
eof
pedi
atri
cA
RD
Sin
vari
ous
stud
ies
Clin
ical
Pro
file
Dah
lem
etal
[35
]C
urle
yet
al[
36]
Flor
iet
al[
37]
Wils
onet
al[
9]A
NZ
ICS
[38]
Hu et
al[
3]Z
hu etal
[2]
Che
tan
etal
[34
]In
dex
stud
y
nfrac14
443
nfrac14
102
nfrac14
328
nfrac14
152
nfrac14
117
nfrac14
306
nfrac14
401
nfrac14
17nfrac14
66
Stud
ype
riod
1998
ndash200
020
01ndash2
004
1996
ndash200
020
00ndash2
003
2004
ndash200
520
06ndash2
007
2009
2003
ndash200
620
07ndash2
008
Cou
ntry
ofst
udy
Net
herl
ands
USA
USA
USA
Aus
tral
iaan
dN
ewZ
eala
ndC
hina
Chi
naIn
dia
Indi
a
Pne
umon
ia11
4
56
35
34
46
75
63
18
82
Bro
nchi
oliti
s15
9
14
ndash7
12
ndashndash
ndash9
Asp
irat
ion
ndash11
15
8
8ndash
ndash6
5Se
psis
341
15
13
36
17
15
34
30
3
Nea
rdr
owni
ngndash
ndash9
53
ndash2
6ndash
Car
diac
dise
ase
ndashndash
7ndash
ndashndash
9ndash
ndashP
aO2
FiO
2ra
tio21
15a
147
and
153a
b
128
and
126a
b
17
71
and
190
6ab
Oxy
gena
tion
Inde
xN
A15
0an
d18
0a
b
200
and
205
ab
95
and
76a
b
Imm
uno-
com
prom
ised
Stat
us9
1N
A
34
45
Oth
ers
91
421
11
9
ndash1
540
2
Mor
talit
y27
8
22
28
35
45
30
70
26
NAfrac14
Info
rmat
ion
not
avai
labl
efrac14
info
rmat
ion
coul
dno
tbe
retr
ieve
ddu
eto
non-
acce
ssib
ility
offu
llm
anus
crip
ts
a Mea
nbIn
the
two
arm
sof
the
stud
yco
hort
High-dose Oral Ambroxol for pulmonary ARDS 347
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
dramatically at 2 h [33] Thus for sustained clinicaleffect more frequent administration (4 hourly or even2 hourly) may be required As pARDS was mostlycaused by pneumonia and bronchiolitis and majority(92) of survivors required ventilation for 14 daysD14 may be an optimal reference for measure of VFDin the study setting This pilot trial is relied on a con-venience sample results (Table 3) from which indi-cates need of sample size of 388 patients in each armwith one-sided significance level (a error) of 005 and80 power to detect 20 improvement in theobserved median VFD14 of 5 days (ie reduction of1 day in VFD14) [40]
Strengths include randomized design and care-fully planned protocols to define ventilator manage-ment sedation and extubation readiness to minimizevariations in daily management of patients Thereare many limitations as well major one being the un-regulated unmonitored hand-ventilation beforePICU admission which may have caused baro-trauma Lack of specific information on its durationmay be a potential confounder Study cohort was re-stricted to pARDS only These issues are unavoid-able and need to be tolerated to develop clinicallyefficacious interventions in the prevalent settingsHowever these would affect generalizability of re-sults Study was underpowered to demonstrate dif-ference in VFD14 There is lack of data onpharmacokinetics of enterally administered ambroxolin critically ill children It needs to be addressed be-fore conducting similar study in future Further in-flammatory oxidative and anti-protease markersshould also be evaluated to assess its pharmacologicefficacy Stratification according to severity of ARDSmay identify a subgroup of responders
C O N C L U S I O N SStudy provides useful information on prevalent situ-ation in the resource-constraint economies informsabout limitations in conducting trials in these set-tings and questionable generalizability of their re-sults Pediatric pARDS is mostly caused bypneumonia and bronchiolitis After factoring inhigher PaO2FiO2 lower OI and lesser patientswith immunocompromised states mortality is highcompared with industrialized peers High-dose oralambroxol failed to improve VFD14 In the current
cost-conscious health care environment its potentialas adjuvant therapy should be explored after havingaddressed the aforementioned issues Large pro-spective study of appropriate power with higherdoses of oral ambroxol administered more frequentlyis desirable VFD14 as composite outcome measuresis suggested for ventilated pediatric pARDS patientshowever it needs further validation
A C K N O W L E D G E M E N T SThe drug (ambroxol hydrochloride) was provided by MsAristo Pharmaceuticals Pvt Ltd Mumbai (India) The tabletsof drug (ambroxol) and placebo (lactose) was prepared atUniversity Institute of Pharmaceutical Sciences PunjabUniversity Chandigarh (India)
Work done at Emergency and Critical Care DivisionAdvanced Pediatrics Center Postgraduate Institute ofMedical Education and Research Chandigarh-160012 India
Presented at the 20th ESPNIC Medical amp NursingAnnual Congress at Verona Italy June 15ndash17 2009rdquo
R E F E R E N C E S1 Ventre KM Arnold JH Acute lung injury and acute re-
spiratory didtress syndrome In Nichols DG (ed) RogerrsquosTextbook of Pediatric Intensive Care 4th ednPhiladelphia PA Lippincott Williams amp Wilkins 2008731ndash66
2 Zhu YF Xu F Lu XL et al Chinese Collaborative StudyGroup for Pediatric Hypoxemic Respiratory FailureMortality and morbidity of acute hypoxemic respiratoryfailure and acute respiratory distress syndrome in infantsand young children Chin Med J 20121252265ndash71
3 Hu X Qian S Xu F et al Chinese Collaborative StudyGroup for Pediatric Respiratory Failure Incidence man-agement and mortality of acute hypoxemic respiratory fail-ure and acute respiratory distress syndrome from aprospective study of Chinese paediatric intensive care net-work Acta Paediatr 201099715ndash21
4 Hanson JH Flori H Application of the acute respiratorydistress syndrome network low-tidal volume strategy topediatric acute lung injury Respir Care Clin N Am 200612349ndash57
5 De Luca D Piastra M Tosi F et al Pharmacological thera-pies for pediatric and neonatal ALIARDS an evidence-based review Curr Drug Targets 201213906ndash16
6 Brun-Buisson C Richard JC Mercat A et al REVA-SRLFAH1N1v 2009 Registry Group Early corticosteroids insevere influenza AH1N1 pneumonia and acute respiratorydistress syndrome Am J Respir Crit Care Med 20111831200ndash6
348 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
7 Singer P Shapiro H Enteral omega-3 in acute respiratorydistress syndrome Curr Opin Clin Nutr Metab Care200912123ndash8
8 Pacht ER DeMichele SJ Nelson JL et al Enteral nutri-tion with eicosapentaenoic acid gamma-linolenic acidand antioxidants reduces alveolar inflammatory mediatorsand protein influx in patients with acute respiratory dis-tress syndrome Crit Care Med 200331491ndash500
9 Wilson DF Thomas NJ Markowitz BP et al Effect ofexogenous surfactant (calfactant) in pediatric acutelung injury a randomized controlled trial JAMA 2005293470ndash6
10 Matthay MA Abraham E Beta-adrenergic agonist therapyas a potential treatment for acute lung injury Am J RespirCrit Care Med 2006173254ndash5
11 Perkins GD McAuley DF Thickett DR et al The szlig-Agonist Lung Injury Trial (BALTI) a randomizedplacebo-controlled clinical trial Am J Respir Crit CareMed 2006173281ndash7
12 Wunderer H Morgenroth K Weis G The cleaningsystem of the airways physiology pathophysiologyand effects of ambroxol Med Monatsschr Pharm20093242ndash7
13 Malerba M Ragnoli B Ambroxol in the 21st centurypharmacological and clinical update Expert Opin DrugMetab Toxicol 200841119ndash29
14 Li Q Yao G Zhu X High-dose ambroxol reduces pul-monary complications in patients with acute cervical spi-nal cord injury after surgery Neurocrit Care 201216267ndash72
15 Wauer RR Schmalisch G Bohme B et al Randomizeddouble blind trial of Ambroxol for the treatment of respira-tory distress syndrome Eur J Pediatr 1992151357ndash63
16 Refai M Brunelli A Xiume F et al Short-term periopera-tive treatment with ambroxol reduces pulmonarycomplications and hospital costs after pulmonary lobec-tomy a randomized trial Eur J Cardiothorac Surg 200935469ndash73
17 Xia DH Xi L Xv C et al The protective effects ofambroxol on radiation lung injury and influence on pro-duction of transforming growth factor beta(1) and tumornecrosis factor alpha Med Oncol 201027697ndash701
18 Ulas MM Hizarci M Kunt A et al Protective effect ofambroxol on pulmonary function after cardiopulmonarybypass J Cardiovasc Pharmacol 200852518ndash23
19 Wang Y Wang FY Pan Z et al Effects of ambroxolcombined with low-dose heparin on TNF-alpha andIL-1beta in rabbits with acute lung injury [Article inChinese] Zhongguo Ying Yong Sheng Li Xue Za Zhi201127231ndash5
20 Su X Wang L Song Y et al Inhibition of inflammatoryresponses by ambroxol a mucolytic agent in a murinemodel of acute lung injury induced by lipopolysaccharideIntensive Care Med 200430133ndash140
21 Ma YT Tian YP Shi HW et al Effects of high doseambroxol on lung injury induced by paraquat in ratsZhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi200725523ndash6
22 ARDS Definition Task Force Ranieri VM RubenfeldGD Thompson BT et al Acute respiratory distress syn-drome the Berlin Definition JAMA 20123072526ndash33
23 Schulz M Hammrlein A Hinkel U Safety and usage pat-tern of an over-the-counter ambroxol cough syrup a com-munity pharmacy based cohort study Int J ClinPharmacol Ther 200644409ndash21
24 Schmalisch G Wauer RR Bohme B Effect of earlyambroxol treatment on lung functions in mechanically ven-tilated preterm newborns who subsequently developed abronchopulmonary dysplasia Respir Med 200094378ndash84
25 Couet W Girault J Reigner BG Steady-state bioavailabil-ity and pharmacokinetics of ambroxol and clenbuterol ad-ministered alone and combined in a new oral formulationInt J Clin Pharmacol Ther Toxicol 198927467ndash72
26 Schulz KF Altman DG Moher D CONSORT GroupCONSORT 2010 Statement updated guidelines for re-porting parallel group randomised trials BMC Med 2010818
27 Leteurtre S Martinot A Duhamel A et al Validation ofthe paediatric logistic organ dysfunction (PeLOD) scoreprospective observational multicentre study Lancet2003362192ndash7
28 Ramsay MAE How to use the Ramsay Score to assess thelevel of ICU Sedation http5jsnaccuminacjpHow20to20use20the20Ramsay20Score20too20assess20the20level20of20ICU20Sedationhtm (1August 2014 date last accessed)
29 Rubenfeld GD Caldwell E Peabody E et al Incidenceand outcomes of acute lung injury N Engl J Med 20053531685ndash93
30 Demling RH Adult respiratory distress syndrome cur-rent concepts New Horiz 19931388ndash401
31 Schoenfeld DA Bernard GR Network ARDS Statisticalevaluation of ventilator-free days as an efficacy measure inclinical trials of treatments for acute respiratory distresssyndrome Crit Care Med 2002301772ndash7
32 Horowitz IN Tai K Hypoalbuminemia in critically ill chil-dren Arch Pediatr Adolesc Med 20071611048ndash1052
33 Wauer RR Schmalisch G Ambroxol for prevention andtreatment of Hyaline membrane disease Eur Resp J 1989257sndash65s
34 Chetan G Rathisharmila R Narayanan P et al Acute re-spiratory distress syndrome in pediatric intensive careunit Indian J Pediatr 2009761013ndash16
35 Dahlem P van Aalderen W Hamaker M et al Incidenceand short-term outcome of acute lung injury in mechanic-ally ventilated children Eur Respir J 200322980ndash5
36 Curley MAQ Hibberd PL Fineman LD et al Effect ofprone positioning on clinical outcomes in children with
High-dose Oral Ambroxol for pulmonary ARDS 349
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
acute lung injury a randomized controlled trial JAMA2005294229ndash37
37 Flori HR Glidden DV Rutherford GW et al Pediatricacute lung injury prospective evaluation of risk factorsassociated with mortality Am J Respir Crit Care Med2005171995ndash1001
38 Erickson S Schibler A Numa A et al Paediatric StudyGroup Australian and New Zealand Intensive Care Society(ANZICS) Acute lung injury in pediatric intensive care in
Australia and New Zealand a prospective multicentre ob-servational study Pediatr Crit Care Med 20078317ndash23
39 Capsoni F Ongari AM Minonzio F Effect of ambroxolon human phagocytic cell function Boll Ist Sieroter Milan198564236ndash9
40 Sample Size Calculator Two Parallel Sample MeansHypothesis One-Sided Non-InferioritySuperiorityhttpwwwcctcuhkeduhkstatmeantsmp_suphtm(24 March 2015 date last accessed)
350 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
- fmv033-TF1
- fmv033-TF2
- fmv033-TF3
- fmv033-TF4
- fmv033-TF6
- fmv033-TF7
- fmv033-TF8
- fmv033-TF9
- fmv033-TF10
- fmv033-TF11
- fmv033-TF12
- fmv033-TF13
- fmv033-TF15
-

have targeted a single pathway of otherwise complexprocess and failed Drug acting on multiple patho-genetic pathways may succeed clinically [8]
Ambroxol has mucoactive [12] anti-inflamma-tory anti-oxidant and surfactant-promoting proper-ties [13] Moreover it gets concentrated selectivelyin lungs [14] Though clinical data are scanty[14ndash18] ambroxolmdasha safe and economical drugmdashmay be considered for treatment of ARDS for itspotential to improve gas exchange [19ndash21] Ifclinical efficacy could be established ambroxol wouldbe an attractive therapeutic option for its low costand toxicity Current exploratory randomizedblinded controlled pilot trial was designed to evalu-ate efficacy of high-dose oral ambroxol in children(age 1 month to 12 years) requiring ventilation forpulmonary ARDS (pARDS) with specific referenceto ventilator-free days in 14 days (VFD14) in re-source-constraint setting Improvement in ventila-tory and oxygenation parameters were secondaryobjectives
M A T E R I A L S A N D M E T H O D S
PatientsAll intubated ventilated patients in 12-bed pediatricintensive care unit (PICU) were screened for studyeligibility each day over 14-month period (August2007ndashSeptember 2008) Entry criteria included allconsecutive children (age 1 month to 12 years) withrespiratory failure owing to diffuse bilateral pulmon-ary infiltrates partial pressure of arterial oxygen(PaO2)fraction of inspired oxygen (FiO2) 300positive end expiratory pressure (PEEP) 5 cmH2O and ventilated for 12 hr [22] Patients withpersistent hypotension (defined as systolic bloodpressure lt5th centile [70 mmHg thorn2 age in years])despite resuscitation for initial 12 hr were excludedto avoid indirect lung injury and to concentrate onpARDS only considering higher biological plausibil-ity of ambroxol in the later Patients hand-ventilatedfor gt24 hr before mechanical ventilation wasexcluded to limit risk of significant barotraumaPatients with active bleeding requiring bloodfluidvolume replacement chronicrestrictive lung diseasereactiveupper airway disease neuromuscular re-spiratory failure raised intracranial pressure
congenital valvular or myocardial heart disease car-diogenic pulmonary edema andor post-operativepatients were excluded to limit confounders Patientswith acute renal failure were excluded as ambroxol isexcreted mainly from kidneys
Study drugOral ambroxol is used for treatment of pulmonarydiseases and reported to be safe [23] Higher intra-venous doses in adults (1000 mgday) [14 16] andpreterm newborns (30 mgkgday 7 days) [15 24]were also safe Orally administered ambroxol gets ab-sorbed rapidly with 73 bioavailability with time topeak plasma concentration being 2 hr in an adultstudy [25] Elimination t12 is biphasicmdashwith an at12 of 13 hr and b t12 of 88 hr [25] Thus 40mgkgday (in four divided doses) may be con-sidered to be an acceptable maximal safe oral dosefor children Though intestinal absorption in critic-ally ill patients is different from healthy person thisdose was considered as starting point for the pilotstudy
Study protocolTrial was designed and analyzed according toConsolidated Standards of Reporting Trials recom-mendations and checklist (Fig 1) [26] After in-formed consent from fatherlegal guardian eligiblepatients were randomized to intervention or placebousing computer-generated random number tablewithin 24 hr of PICU admission Study assignmentswere serially numbered in opaque and sealed enve-lopes Intervention group received oral ambroxol(40 mgkgday) in four divided doses for 10 days oruntil extubation whichever was earlier Identical-looking tablets of ambroxol (of 50 mg) and placebowere prepared and packs containing dosage for 20kg body-weight patient were dispensed Tablets werecrushed suspended in water and administeredthrough nasogastric tube Investigators doctorsnurses and data manger were blinded to treatmentassignment Institutional ethics committee approvedthe study protocol
At enrollment patientsrsquo demographics baselineassessment and Pediatric Risk of Mortality III(PRISM-III) were recorded Vitals oxygen saturationon pulse oximeter (SpO2) and central venous
340 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
pressure (if required) were monitored continuouslyand recorded 2 hourly Ventilator settings bloodgases end-tidal CO2 and chest radiograph data werecollected for initial 28 days or until extubationwhichever was earlier In addition pulmonary statusand respiratory support extubation readiness fluidbalance caloric and protein intake and pediatric
logistic organ dysfunction (PeLOD) score [27] re-corded Investigations were recorded if available andreflected the values obtained closest to 0800 am
Patients in both groups were managed accordingto prevalent unit protocol for ventilation sedationhemodynamics nutrition extubation readiness andgeneral nursing care Lung-protective ventilation was
Paents fulfilled inclusion criteria (n=89)
Randomized (n=67)
Allocated to Placebo (n=34)
Received allocated intervenon (n=34)
Did not receive allocated intervenon (n=0)
Allocated to Ambroxol (n=33)
Received allocated intervenon (n=32)
Did not receive allocated intervenon (n=0)
Lost to follow up (n=0)
Disconnued intervenon (n=0)
Lost to follow up (n=0)
Disconnued intervenon (n=1)
( for acute renal failure within 2 days)
Included in Analysis (n=34)
Excluded from Analysis (n=0)
Included in Analysis (n=32)
Excluded from Analysis (n=1)
22 Excluded 2 Parents refused to parcipate 4 Missed enrollment window 2 Chronic Lung Disease 2 Neuromuscular Weakness 3 Raised Intracranial Pressure 2 Postoperave Paents 3 Acute Renal Failure 4 Refractory Shock
Fig 1 Patient flowchart through clinical trial
High-dose Oral Ambroxol for pulmonary ARDS 341
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
employed and included pressure-control ventilationwith peak inflating pressure lt30 cm H2O PEEP5ndash10 cm H2O tidal volume 5ndash6 mlkg FiO2 lt06and permissive hypercapnea (PaCO2 gt80torr whilepH gt725) if required Aim was to achieve optimaloxygenation (PaO2 60ndash80 mmHg SpO2 88ndash92)while limiting barotrauma Sedation protocolinvolved continuous diazepam (midazolam in some)and morphine infusions to achieve and maintainRamsay Score of 3ndash4 [28] with morning sedationinterruption Intravenous fluid was initiated as 23maintenance and feed was introduced at the earliestOnce patients were on full feed volume was relaxedto full maintenance After achievement of spontan-eous breathing oxygenation index (OI) lt6 decreaseandor plateau in ventilator support over 12 hourspatients were tested for extubation readiness Patientstatus was verified at discharge from PICU If diedprimary and secondary causes of death were re-corded Adverse events were monitored and reportedto Institutional Ethics Committee
Study outcomesConsidering difficulty in achieving mortality benefitin current critical care scenario [29] and unclear con-tribution of ARDS to mortality [30] composite out-come measure like ventilator-free days (VFD)incorporating both mortality and ventilation dur-ation are being considered [31] Primary outcomewas VFD14 which is defined as number of daysfrom point of successful weaning to day 14 (D14) ofenrollment Death during first 14 days is consideredto be equivalent to unresolved respiratory failureand thus is equated to zero VFD14 Secondary out-come measures included all-cause mortality ventila-tor days among survivors number of patients aliveand ventilator-free on D14 time-to-recovery fromARDS (ie when patients met extubation readinesscriteria after randomization) changes in ventilationand oxygenation parameters
Statistical analysisSimple unrestricted randomization was used to allo-cate patients in two groups Nonparametric MannndashWhitney U test and X2 test (or Fisherrsquos exact test ifrequired) were used to compare groups with quanti-tative outcomes Survival analysis using KaplanMeier curves was performed for time-to-event data
eg ventilation duration time-to-recovery and PICUstay Repeated measures analysis of variancewas planned to assess trend in ventilation and oxy-genation parameters SPSS version 16 was used forstatistical analysis A plt 005 was consideredsignificant
R E S U L T SOut of 67 eligible patients 33 were randomized toambroxol while 34 to placebo (Fig 1) Per-protocolanalysis was performed after excluding one patient inambroxol group who developed acute renal failureon day 2 leading to discontinuation of drugManagement included unmonitored hand-ventilationwith self-inflating bag for initial few hours (usuallyupto 24 h) in emergency room (ER) or pediatricwards (PWs) before PICU admission as more oftenthan not ventilator was not available for immediateapplication Of 66 patients 42(64) had moderateto severe ARDS (PaO2FiO2 200) [22] at ran-domization Thirteen of the remaining 24 patientswho had mild ARDS (PaO2FiO2 201ndash300) at en-rollment progressed in severity subsequently Twogroups were comparable for demographic profile nu-tritional status severity of illness at randomizationdiagnoses metabolic profile cause of lung injury aswell as in baseline respiratory characteristics (Tables1 and 2) Bronchopneumonia and bronchiolitis werethe commonest (91) causes of pARDS Three pa-tients (45) had chemotherapy-induced febrile neu-tropenia Eight (12) (four in each group) patientshad positive blood culture at PICU admissionmdashStaphylococcus aureus (3) Burkholderia cepacia (2)Acinetobacter (1) E coli (1) and Candida (1)
VFD14 was similar in two groups (pfrac14 056) sowas time-to-recovery from ARDS and other clinicaloutcomes (Table 3 and Fig 2) PaO2FiO2 OIneed for PEEP tidal volume and PaCO2 were alsosimilar during first 14 days (Figs 3 and 4) Healthcare associated infections (HCAIs) were seen in25(38) patients more in placebo group (1634 vs932 pfrac14 011) Out of these 19(76) were culturepositive gram-negative bacilli (14) being the com-monest (Candia 4 Staphylococcus 3) Blood-stream infections (14) were commonest followed byurinary tract infections (11) All-cause mortality was258 (1766) with similar distribution of early
342 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
(lt3 days) or late (gt3 days) deaths in the twogroups ARDS was considered as primary cause ofdeath in 53 (917) patients three of them wereimmunocompromised Forty-one percent (717)
of deaths were ascribed to HCAIs while onesuccumbed to hyperkalemia-induced arrhythmiaAmong survivors median (interquartile range) venti-lation duration was 7 (6) and 8 (45) days inambroxol and placebo groups respectively Diarrheawas noted in 6 (19) patients receiving ambroxolOne patient developed renal failure on D2 ofambroxol Serial blood pressure and cardiac compo-nent of PeLOD score were comparable in the twogroups during first 14 days contrasting the experi-mental data [33]
Table 1 Baseline patientsrsquo characteristics atenrollment
Characteristics Placebo(nfrac14 34)
Ambroxol(nfrac14 32)
Age (year) median (IQR) 115 (322) 137 (342)Age Number ()lt 1 year 16 (47) 13 (40)1ndash5 years 11 (32) 14 (44)gt5 years 7 (21) 5 (16)
Sex ratio (MF) 2311 2210Nutritional status (reference NCHS median)a
Normal (gt80) 18 (56) 17 (50)PEM grade 1 (71ndash80) 5 (16) 4 (12)PEM grade 2 (61ndash70) 5 (16) 8 (24)PEM grade 3 (51ndash60) 3 (9) 5 (15)PEM grade 4 (50) 1 (3) 0 (0)Serum albumin at
admission median(IQR) gmdl
229 (088) 260 (100)
Number ofpatients withhypoalbuminemia()b
24 (706) 23 (719)
PRISM III scoremedian (IQR)
500 (700) 600 (775)
PeLOD scoremedian (IQR)c
550 (1000) 1000 (1000)
Cause of pARDSPneumonia 29 (85) 27 (84)Bronchiolitis 5 (15) 1 (3)Kerosene poisoning 0 (0) 2 (6)Aspiration pneumonia 0 (0) 1 (3)Pulmonary hemorrhage 0 (0) 1 (3)
Blood culture positive 4 (12) 4 (13)Febrile Neutropenia 2 (6) 1 (3)
IQRfrac14 interquartile range PEMfrac14 protein energy malnutritionpARDSfrac14 Pulmonary Acute Respiratory DistressaMalnutrition was graded based on the criteria defined by IndianAcademy of PediatricsbHypoalbuminemia was defined as an albumin level of lt34 gdl for pa-tients gt7 months and lt25 gdl for patients lt7 months [32]cPeLOD Pediatric Logistic Organ Dysfunction (non-pulmonary) Score
Table 2 Baseline respiratory characteristics atenrollment
Respiratory characteristics Placebo(nfrac14 34)
Ambroxol(nfrac14 32)
PaO2FiO2 ratioa
mean (SD)1771 (707) 1906 (816)
Severity of ARDSnumber ()Mild ARDS
(PF ratio 201ndash300)10 (29) 14 (44)
Moderate ARDS(PF ratio 101ndash200)
20 (59) 14 (44)
Severe ARDS(PF ratio 100)
4 (12) 4 (12)
PEEP mean (SD) 65 (25) 62 (16)Quantitative pulmonary involvement
(as per chest radiograph)1 quadrant 0 (0) 0 (0)2 quadrant 2 (6) 2 (6)3 quadrant 7 (21) 6 (19)4 quadrant 25 (73) 24 (75)MAP mean (SD) 123 (51) 117 (42)OI mean (SD) 95 (108) 76 (46)VT (mlkg) mean (SD) 57 (17) 54 (13)PIP mean (SD) 194 (69) 186 (42)
Murrayrsquos lung injury scoreMild to moderate
(01ndash25)26 (76) 22 (69)
Severe (gt25) 8 (24) 10 (31)
IQRfrac14 interquartile range SDfrac14 standard deviation PaO2frac14 partial pres-sure of arterial oxygen FiO2frac14 fraction of inspired oxygenPEEPfrac14 positive end expiratory pressure PIPfrac14 peak inflating pressureMAPfrac14mean airway pressure OIfrac14 oxygenation Index VTfrac14 tidalvolumeaArterial blood gases in both groups were assessed at 0800 hours daily
High-dose Oral Ambroxol for pulmonary ARDS 343
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
D I S C U S S I O NCurrent study add to scarcely available data on clin-ical characteristics and outcomes of ventilated pediat-ric ARDS patients from developing economies [2 334] Ours being a tertiary care hospital without refer-ral and transport system we usually receive patientsvery late Thus patients are likely to be the severestof lot Pneumonia and bronchiolitis were commonest(90) causes of ARDS making it a syndrome ofrelatively homogeneous etiology in our setting as
against 40ndash65 reported from industrialized econo-mies (Table 4) PRISM-III score calculated fromdata collected during first 24 h of PICU admissionwere comparable with that in other pediatric ARDSstudies [35 37] However as all of our patients wereresuscitated and received post-resuscitation support-ive care (including hand-ventilation) for significantperiod in ERPWs before being shifted to PICUmany vital signs might have improved by the timethey reached PICU Thus actual PRISM-III scoresat beginning of hand-ventilation in ERPWs is likelyto be higher than ones calculated at PICU admissionmaking them sicker than what got reflected inPRISM-III scores All-cause mortality (of 26) is sig-nificantly higher compared with industrializedeconomies (Table 4) after factoring in higher meanPaO2FiO2 (gt175) lower mean OI (lt10) andlesser number of patients with immunocompromisedstatus Poor referral advanced stage of illness at ad-mission and suboptimal post-resuscitation care inERPWs may be one set of possible causative fac-tors While in PICU suboptimal patientsndashnurseratio poorly trained critical care nurses and poor in-fection control practices may be another These arethe issues of concern and indicate potentials of im-provement in critical care in the study settings
Early treatment was planned to have potentialbeneficial effects of ambroxol early during acute phase
Table 3 Primary and secondary outcome variables
Outcome Placebo (nfrac14 34) Ambroxol (nfrac14 32) pa
Primary outcome variableVentilator-free days at D14 (VFD14)b 50 (70) 50 (97) 056Ventilator-free days at D14 (VFD14) (mean 6 SD) 44 (36) 50 (45) ndash
Secondary outcome variablesAlive and ventilator-free at D14c 24 (71) 21 (66) 045Ventilator days among survivorsb 80 (45)(nfrac14 25) 70 (60) (nfrac14 24) 055Number of days to recover from ARDSd among survivorsb 100 (50)(nfrac14 25) 85 (70)(nfrac14 24) 054PICU stay among survivors (day)b 1200 (500) 1150 (775) 042All-cause mortalityc 9 (26) 8 (25) 089Early deaths (3 days)c 3 (38) 4 (44) 077Late deaths (gt3 days)c 5 (62) 5 (56)
ap-values are based on MannndashWhitney U test for number of VFD14 ventilator days among survivors time-to-recovery from ARDS duration of PICUstay v2 test (or Fisher Exact Test) for number of patients alive and ventilator-free at day 14 all-cause mortalitybData expressed as median (interquartile range)cData expressed as number (percentage)dAmong survivors number of days from randomization to meeting extubation readiness criteria for 24 consecutive hours through day 14
Time to recovery (Days)6050403020100
Cum
ulat
ive
a
t giv
en ti
me
10
08
06
04
02
00
placebo-censoreddrug-censoredplacebodrug
Study Groups
Fig 2 KaplanndashMeier curves comparing time-to-recoveryfrom ARDS in the two groups (censored for in-PICUmortality Log-Rank test pfrac14 094)
344 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
(a)
(b)
(c)
0
10
20
30
40
50
60
70
0 2 4 6 8 10 12 14 16
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
OI
0
100
200
300
400
500
600
700
0 5 10 15
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
PF
0
2
4
6
8
10
12
14
16
18
0 5 10 15
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
PEEP
Fig 3 Dot plot showing trend of mean PaO2FiO2 ratio oxygenation Index and PEEP during first 14 days
High-dose Oral Ambroxol for pulmonary ARDS 345
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
of illness We demonstrated safety tolerance and roleof high-dose oral ambroxol (40 mgkgday in fourdivided doses) in ventilated pARDS patients for thefirst time Ambroxol failed to improve oxygenationventilation VFD time-to-recovery mortality and thusto suggest therapeutic potential in pARDS in thestudy setting owing to small sample size Two-thirdsof patients had hypoalbuminemia and thus gut edema
possibly affecting ambroxolrsquos bioavailability Dosagechosen was maximal safe dose based on availableclinical data Therapeutic efficacy and safety of fur-ther higher dose may be subject of future scrutinyHigher doses may also be helpful in eradicating patho-gens adhered to bronchiolaralveolar epithelium [39]Ambroxol selectively gets concentrated in lungswithin 3 min of intravenous administration but it falls
(a)
(a)
0
50
100
150
200
250
0 2 4 6 8 10 12 14 16
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
PaCO
2
0
2
4
6
8
10
12
14
0 2 4 6 8 10 12 14 16
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
TV
FIG 4 Dot plot showing trend of mean tidal volume and PaCO2 during first 14 days
346 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
Tab
le4
Com
pari
son
ofcl
inic
alch
arac
teri
stic
san
dou
tcom
eof
pedi
atri
cA
RD
Sin
vari
ous
stud
ies
Clin
ical
Pro
file
Dah
lem
etal
[35
]C
urle
yet
al[
36]
Flor
iet
al[
37]
Wils
onet
al[
9]A
NZ
ICS
[38]
Hu et
al[
3]Z
hu etal
[2]
Che
tan
etal
[34
]In
dex
stud
y
nfrac14
443
nfrac14
102
nfrac14
328
nfrac14
152
nfrac14
117
nfrac14
306
nfrac14
401
nfrac14
17nfrac14
66
Stud
ype
riod
1998
ndash200
020
01ndash2
004
1996
ndash200
020
00ndash2
003
2004
ndash200
520
06ndash2
007
2009
2003
ndash200
620
07ndash2
008
Cou
ntry
ofst
udy
Net
herl
ands
USA
USA
USA
Aus
tral
iaan
dN
ewZ
eala
ndC
hina
Chi
naIn
dia
Indi
a
Pne
umon
ia11
4
56
35
34
46
75
63
18
82
Bro
nchi
oliti
s15
9
14
ndash7
12
ndashndash
ndash9
Asp
irat
ion
ndash11
15
8
8ndash
ndash6
5Se
psis
341
15
13
36
17
15
34
30
3
Nea
rdr
owni
ngndash
ndash9
53
ndash2
6ndash
Car
diac
dise
ase
ndashndash
7ndash
ndashndash
9ndash
ndashP
aO2
FiO
2ra
tio21
15a
147
and
153a
b
128
and
126a
b
17
71
and
190
6ab
Oxy
gena
tion
Inde
xN
A15
0an
d18
0a
b
200
and
205
ab
95
and
76a
b
Imm
uno-
com
prom
ised
Stat
us9
1N
A
34
45
Oth
ers
91
421
11
9
ndash1
540
2
Mor
talit
y27
8
22
28
35
45
30
70
26
NAfrac14
Info
rmat
ion
not
avai
labl
efrac14
info
rmat
ion
coul
dno
tbe
retr
ieve
ddu
eto
non-
acce
ssib
ility
offu
llm
anus
crip
ts
a Mea
nbIn
the
two
arm
sof
the
stud
yco
hort
High-dose Oral Ambroxol for pulmonary ARDS 347
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
dramatically at 2 h [33] Thus for sustained clinicaleffect more frequent administration (4 hourly or even2 hourly) may be required As pARDS was mostlycaused by pneumonia and bronchiolitis and majority(92) of survivors required ventilation for 14 daysD14 may be an optimal reference for measure of VFDin the study setting This pilot trial is relied on a con-venience sample results (Table 3) from which indi-cates need of sample size of 388 patients in each armwith one-sided significance level (a error) of 005 and80 power to detect 20 improvement in theobserved median VFD14 of 5 days (ie reduction of1 day in VFD14) [40]
Strengths include randomized design and care-fully planned protocols to define ventilator manage-ment sedation and extubation readiness to minimizevariations in daily management of patients Thereare many limitations as well major one being the un-regulated unmonitored hand-ventilation beforePICU admission which may have caused baro-trauma Lack of specific information on its durationmay be a potential confounder Study cohort was re-stricted to pARDS only These issues are unavoid-able and need to be tolerated to develop clinicallyefficacious interventions in the prevalent settingsHowever these would affect generalizability of re-sults Study was underpowered to demonstrate dif-ference in VFD14 There is lack of data onpharmacokinetics of enterally administered ambroxolin critically ill children It needs to be addressed be-fore conducting similar study in future Further in-flammatory oxidative and anti-protease markersshould also be evaluated to assess its pharmacologicefficacy Stratification according to severity of ARDSmay identify a subgroup of responders
C O N C L U S I O N SStudy provides useful information on prevalent situ-ation in the resource-constraint economies informsabout limitations in conducting trials in these set-tings and questionable generalizability of their re-sults Pediatric pARDS is mostly caused bypneumonia and bronchiolitis After factoring inhigher PaO2FiO2 lower OI and lesser patientswith immunocompromised states mortality is highcompared with industrialized peers High-dose oralambroxol failed to improve VFD14 In the current
cost-conscious health care environment its potentialas adjuvant therapy should be explored after havingaddressed the aforementioned issues Large pro-spective study of appropriate power with higherdoses of oral ambroxol administered more frequentlyis desirable VFD14 as composite outcome measuresis suggested for ventilated pediatric pARDS patientshowever it needs further validation
A C K N O W L E D G E M E N T SThe drug (ambroxol hydrochloride) was provided by MsAristo Pharmaceuticals Pvt Ltd Mumbai (India) The tabletsof drug (ambroxol) and placebo (lactose) was prepared atUniversity Institute of Pharmaceutical Sciences PunjabUniversity Chandigarh (India)
Work done at Emergency and Critical Care DivisionAdvanced Pediatrics Center Postgraduate Institute ofMedical Education and Research Chandigarh-160012 India
Presented at the 20th ESPNIC Medical amp NursingAnnual Congress at Verona Italy June 15ndash17 2009rdquo
R E F E R E N C E S1 Ventre KM Arnold JH Acute lung injury and acute re-
spiratory didtress syndrome In Nichols DG (ed) RogerrsquosTextbook of Pediatric Intensive Care 4th ednPhiladelphia PA Lippincott Williams amp Wilkins 2008731ndash66
2 Zhu YF Xu F Lu XL et al Chinese Collaborative StudyGroup for Pediatric Hypoxemic Respiratory FailureMortality and morbidity of acute hypoxemic respiratoryfailure and acute respiratory distress syndrome in infantsand young children Chin Med J 20121252265ndash71
3 Hu X Qian S Xu F et al Chinese Collaborative StudyGroup for Pediatric Respiratory Failure Incidence man-agement and mortality of acute hypoxemic respiratory fail-ure and acute respiratory distress syndrome from aprospective study of Chinese paediatric intensive care net-work Acta Paediatr 201099715ndash21
4 Hanson JH Flori H Application of the acute respiratorydistress syndrome network low-tidal volume strategy topediatric acute lung injury Respir Care Clin N Am 200612349ndash57
5 De Luca D Piastra M Tosi F et al Pharmacological thera-pies for pediatric and neonatal ALIARDS an evidence-based review Curr Drug Targets 201213906ndash16
6 Brun-Buisson C Richard JC Mercat A et al REVA-SRLFAH1N1v 2009 Registry Group Early corticosteroids insevere influenza AH1N1 pneumonia and acute respiratorydistress syndrome Am J Respir Crit Care Med 20111831200ndash6
348 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
7 Singer P Shapiro H Enteral omega-3 in acute respiratorydistress syndrome Curr Opin Clin Nutr Metab Care200912123ndash8
8 Pacht ER DeMichele SJ Nelson JL et al Enteral nutri-tion with eicosapentaenoic acid gamma-linolenic acidand antioxidants reduces alveolar inflammatory mediatorsand protein influx in patients with acute respiratory dis-tress syndrome Crit Care Med 200331491ndash500
9 Wilson DF Thomas NJ Markowitz BP et al Effect ofexogenous surfactant (calfactant) in pediatric acutelung injury a randomized controlled trial JAMA 2005293470ndash6
10 Matthay MA Abraham E Beta-adrenergic agonist therapyas a potential treatment for acute lung injury Am J RespirCrit Care Med 2006173254ndash5
11 Perkins GD McAuley DF Thickett DR et al The szlig-Agonist Lung Injury Trial (BALTI) a randomizedplacebo-controlled clinical trial Am J Respir Crit CareMed 2006173281ndash7
12 Wunderer H Morgenroth K Weis G The cleaningsystem of the airways physiology pathophysiologyand effects of ambroxol Med Monatsschr Pharm20093242ndash7
13 Malerba M Ragnoli B Ambroxol in the 21st centurypharmacological and clinical update Expert Opin DrugMetab Toxicol 200841119ndash29
14 Li Q Yao G Zhu X High-dose ambroxol reduces pul-monary complications in patients with acute cervical spi-nal cord injury after surgery Neurocrit Care 201216267ndash72
15 Wauer RR Schmalisch G Bohme B et al Randomizeddouble blind trial of Ambroxol for the treatment of respira-tory distress syndrome Eur J Pediatr 1992151357ndash63
16 Refai M Brunelli A Xiume F et al Short-term periopera-tive treatment with ambroxol reduces pulmonarycomplications and hospital costs after pulmonary lobec-tomy a randomized trial Eur J Cardiothorac Surg 200935469ndash73
17 Xia DH Xi L Xv C et al The protective effects ofambroxol on radiation lung injury and influence on pro-duction of transforming growth factor beta(1) and tumornecrosis factor alpha Med Oncol 201027697ndash701
18 Ulas MM Hizarci M Kunt A et al Protective effect ofambroxol on pulmonary function after cardiopulmonarybypass J Cardiovasc Pharmacol 200852518ndash23
19 Wang Y Wang FY Pan Z et al Effects of ambroxolcombined with low-dose heparin on TNF-alpha andIL-1beta in rabbits with acute lung injury [Article inChinese] Zhongguo Ying Yong Sheng Li Xue Za Zhi201127231ndash5
20 Su X Wang L Song Y et al Inhibition of inflammatoryresponses by ambroxol a mucolytic agent in a murinemodel of acute lung injury induced by lipopolysaccharideIntensive Care Med 200430133ndash140
21 Ma YT Tian YP Shi HW et al Effects of high doseambroxol on lung injury induced by paraquat in ratsZhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi200725523ndash6
22 ARDS Definition Task Force Ranieri VM RubenfeldGD Thompson BT et al Acute respiratory distress syn-drome the Berlin Definition JAMA 20123072526ndash33
23 Schulz M Hammrlein A Hinkel U Safety and usage pat-tern of an over-the-counter ambroxol cough syrup a com-munity pharmacy based cohort study Int J ClinPharmacol Ther 200644409ndash21
24 Schmalisch G Wauer RR Bohme B Effect of earlyambroxol treatment on lung functions in mechanically ven-tilated preterm newborns who subsequently developed abronchopulmonary dysplasia Respir Med 200094378ndash84
25 Couet W Girault J Reigner BG Steady-state bioavailabil-ity and pharmacokinetics of ambroxol and clenbuterol ad-ministered alone and combined in a new oral formulationInt J Clin Pharmacol Ther Toxicol 198927467ndash72
26 Schulz KF Altman DG Moher D CONSORT GroupCONSORT 2010 Statement updated guidelines for re-porting parallel group randomised trials BMC Med 2010818
27 Leteurtre S Martinot A Duhamel A et al Validation ofthe paediatric logistic organ dysfunction (PeLOD) scoreprospective observational multicentre study Lancet2003362192ndash7
28 Ramsay MAE How to use the Ramsay Score to assess thelevel of ICU Sedation http5jsnaccuminacjpHow20to20use20the20Ramsay20Score20too20assess20the20level20of20ICU20Sedationhtm (1August 2014 date last accessed)
29 Rubenfeld GD Caldwell E Peabody E et al Incidenceand outcomes of acute lung injury N Engl J Med 20053531685ndash93
30 Demling RH Adult respiratory distress syndrome cur-rent concepts New Horiz 19931388ndash401
31 Schoenfeld DA Bernard GR Network ARDS Statisticalevaluation of ventilator-free days as an efficacy measure inclinical trials of treatments for acute respiratory distresssyndrome Crit Care Med 2002301772ndash7
32 Horowitz IN Tai K Hypoalbuminemia in critically ill chil-dren Arch Pediatr Adolesc Med 20071611048ndash1052
33 Wauer RR Schmalisch G Ambroxol for prevention andtreatment of Hyaline membrane disease Eur Resp J 1989257sndash65s
34 Chetan G Rathisharmila R Narayanan P et al Acute re-spiratory distress syndrome in pediatric intensive careunit Indian J Pediatr 2009761013ndash16
35 Dahlem P van Aalderen W Hamaker M et al Incidenceand short-term outcome of acute lung injury in mechanic-ally ventilated children Eur Respir J 200322980ndash5
36 Curley MAQ Hibberd PL Fineman LD et al Effect ofprone positioning on clinical outcomes in children with
High-dose Oral Ambroxol for pulmonary ARDS 349
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
acute lung injury a randomized controlled trial JAMA2005294229ndash37
37 Flori HR Glidden DV Rutherford GW et al Pediatricacute lung injury prospective evaluation of risk factorsassociated with mortality Am J Respir Crit Care Med2005171995ndash1001
38 Erickson S Schibler A Numa A et al Paediatric StudyGroup Australian and New Zealand Intensive Care Society(ANZICS) Acute lung injury in pediatric intensive care in
Australia and New Zealand a prospective multicentre ob-servational study Pediatr Crit Care Med 20078317ndash23
39 Capsoni F Ongari AM Minonzio F Effect of ambroxolon human phagocytic cell function Boll Ist Sieroter Milan198564236ndash9
40 Sample Size Calculator Two Parallel Sample MeansHypothesis One-Sided Non-InferioritySuperiorityhttpwwwcctcuhkeduhkstatmeantsmp_suphtm(24 March 2015 date last accessed)
350 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
- fmv033-TF1
- fmv033-TF2
- fmv033-TF3
- fmv033-TF4
- fmv033-TF6
- fmv033-TF7
- fmv033-TF8
- fmv033-TF9
- fmv033-TF10
- fmv033-TF11
- fmv033-TF12
- fmv033-TF13
- fmv033-TF15
-

pressure (if required) were monitored continuouslyand recorded 2 hourly Ventilator settings bloodgases end-tidal CO2 and chest radiograph data werecollected for initial 28 days or until extubationwhichever was earlier In addition pulmonary statusand respiratory support extubation readiness fluidbalance caloric and protein intake and pediatric
logistic organ dysfunction (PeLOD) score [27] re-corded Investigations were recorded if available andreflected the values obtained closest to 0800 am
Patients in both groups were managed accordingto prevalent unit protocol for ventilation sedationhemodynamics nutrition extubation readiness andgeneral nursing care Lung-protective ventilation was
Paents fulfilled inclusion criteria (n=89)
Randomized (n=67)
Allocated to Placebo (n=34)
Received allocated intervenon (n=34)
Did not receive allocated intervenon (n=0)
Allocated to Ambroxol (n=33)
Received allocated intervenon (n=32)
Did not receive allocated intervenon (n=0)
Lost to follow up (n=0)
Disconnued intervenon (n=0)
Lost to follow up (n=0)
Disconnued intervenon (n=1)
( for acute renal failure within 2 days)
Included in Analysis (n=34)
Excluded from Analysis (n=0)
Included in Analysis (n=32)
Excluded from Analysis (n=1)
22 Excluded 2 Parents refused to parcipate 4 Missed enrollment window 2 Chronic Lung Disease 2 Neuromuscular Weakness 3 Raised Intracranial Pressure 2 Postoperave Paents 3 Acute Renal Failure 4 Refractory Shock
Fig 1 Patient flowchart through clinical trial
High-dose Oral Ambroxol for pulmonary ARDS 341
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
employed and included pressure-control ventilationwith peak inflating pressure lt30 cm H2O PEEP5ndash10 cm H2O tidal volume 5ndash6 mlkg FiO2 lt06and permissive hypercapnea (PaCO2 gt80torr whilepH gt725) if required Aim was to achieve optimaloxygenation (PaO2 60ndash80 mmHg SpO2 88ndash92)while limiting barotrauma Sedation protocolinvolved continuous diazepam (midazolam in some)and morphine infusions to achieve and maintainRamsay Score of 3ndash4 [28] with morning sedationinterruption Intravenous fluid was initiated as 23maintenance and feed was introduced at the earliestOnce patients were on full feed volume was relaxedto full maintenance After achievement of spontan-eous breathing oxygenation index (OI) lt6 decreaseandor plateau in ventilator support over 12 hourspatients were tested for extubation readiness Patientstatus was verified at discharge from PICU If diedprimary and secondary causes of death were re-corded Adverse events were monitored and reportedto Institutional Ethics Committee
Study outcomesConsidering difficulty in achieving mortality benefitin current critical care scenario [29] and unclear con-tribution of ARDS to mortality [30] composite out-come measure like ventilator-free days (VFD)incorporating both mortality and ventilation dur-ation are being considered [31] Primary outcomewas VFD14 which is defined as number of daysfrom point of successful weaning to day 14 (D14) ofenrollment Death during first 14 days is consideredto be equivalent to unresolved respiratory failureand thus is equated to zero VFD14 Secondary out-come measures included all-cause mortality ventila-tor days among survivors number of patients aliveand ventilator-free on D14 time-to-recovery fromARDS (ie when patients met extubation readinesscriteria after randomization) changes in ventilationand oxygenation parameters
Statistical analysisSimple unrestricted randomization was used to allo-cate patients in two groups Nonparametric MannndashWhitney U test and X2 test (or Fisherrsquos exact test ifrequired) were used to compare groups with quanti-tative outcomes Survival analysis using KaplanMeier curves was performed for time-to-event data
eg ventilation duration time-to-recovery and PICUstay Repeated measures analysis of variancewas planned to assess trend in ventilation and oxy-genation parameters SPSS version 16 was used forstatistical analysis A plt 005 was consideredsignificant
R E S U L T SOut of 67 eligible patients 33 were randomized toambroxol while 34 to placebo (Fig 1) Per-protocolanalysis was performed after excluding one patient inambroxol group who developed acute renal failureon day 2 leading to discontinuation of drugManagement included unmonitored hand-ventilationwith self-inflating bag for initial few hours (usuallyupto 24 h) in emergency room (ER) or pediatricwards (PWs) before PICU admission as more oftenthan not ventilator was not available for immediateapplication Of 66 patients 42(64) had moderateto severe ARDS (PaO2FiO2 200) [22] at ran-domization Thirteen of the remaining 24 patientswho had mild ARDS (PaO2FiO2 201ndash300) at en-rollment progressed in severity subsequently Twogroups were comparable for demographic profile nu-tritional status severity of illness at randomizationdiagnoses metabolic profile cause of lung injury aswell as in baseline respiratory characteristics (Tables1 and 2) Bronchopneumonia and bronchiolitis werethe commonest (91) causes of pARDS Three pa-tients (45) had chemotherapy-induced febrile neu-tropenia Eight (12) (four in each group) patientshad positive blood culture at PICU admissionmdashStaphylococcus aureus (3) Burkholderia cepacia (2)Acinetobacter (1) E coli (1) and Candida (1)
VFD14 was similar in two groups (pfrac14 056) sowas time-to-recovery from ARDS and other clinicaloutcomes (Table 3 and Fig 2) PaO2FiO2 OIneed for PEEP tidal volume and PaCO2 were alsosimilar during first 14 days (Figs 3 and 4) Healthcare associated infections (HCAIs) were seen in25(38) patients more in placebo group (1634 vs932 pfrac14 011) Out of these 19(76) were culturepositive gram-negative bacilli (14) being the com-monest (Candia 4 Staphylococcus 3) Blood-stream infections (14) were commonest followed byurinary tract infections (11) All-cause mortality was258 (1766) with similar distribution of early
342 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
(lt3 days) or late (gt3 days) deaths in the twogroups ARDS was considered as primary cause ofdeath in 53 (917) patients three of them wereimmunocompromised Forty-one percent (717)
of deaths were ascribed to HCAIs while onesuccumbed to hyperkalemia-induced arrhythmiaAmong survivors median (interquartile range) venti-lation duration was 7 (6) and 8 (45) days inambroxol and placebo groups respectively Diarrheawas noted in 6 (19) patients receiving ambroxolOne patient developed renal failure on D2 ofambroxol Serial blood pressure and cardiac compo-nent of PeLOD score were comparable in the twogroups during first 14 days contrasting the experi-mental data [33]
Table 1 Baseline patientsrsquo characteristics atenrollment
Characteristics Placebo(nfrac14 34)
Ambroxol(nfrac14 32)
Age (year) median (IQR) 115 (322) 137 (342)Age Number ()lt 1 year 16 (47) 13 (40)1ndash5 years 11 (32) 14 (44)gt5 years 7 (21) 5 (16)
Sex ratio (MF) 2311 2210Nutritional status (reference NCHS median)a
Normal (gt80) 18 (56) 17 (50)PEM grade 1 (71ndash80) 5 (16) 4 (12)PEM grade 2 (61ndash70) 5 (16) 8 (24)PEM grade 3 (51ndash60) 3 (9) 5 (15)PEM grade 4 (50) 1 (3) 0 (0)Serum albumin at
admission median(IQR) gmdl
229 (088) 260 (100)
Number ofpatients withhypoalbuminemia()b
24 (706) 23 (719)
PRISM III scoremedian (IQR)
500 (700) 600 (775)
PeLOD scoremedian (IQR)c
550 (1000) 1000 (1000)
Cause of pARDSPneumonia 29 (85) 27 (84)Bronchiolitis 5 (15) 1 (3)Kerosene poisoning 0 (0) 2 (6)Aspiration pneumonia 0 (0) 1 (3)Pulmonary hemorrhage 0 (0) 1 (3)
Blood culture positive 4 (12) 4 (13)Febrile Neutropenia 2 (6) 1 (3)
IQRfrac14 interquartile range PEMfrac14 protein energy malnutritionpARDSfrac14 Pulmonary Acute Respiratory DistressaMalnutrition was graded based on the criteria defined by IndianAcademy of PediatricsbHypoalbuminemia was defined as an albumin level of lt34 gdl for pa-tients gt7 months and lt25 gdl for patients lt7 months [32]cPeLOD Pediatric Logistic Organ Dysfunction (non-pulmonary) Score
Table 2 Baseline respiratory characteristics atenrollment
Respiratory characteristics Placebo(nfrac14 34)
Ambroxol(nfrac14 32)
PaO2FiO2 ratioa
mean (SD)1771 (707) 1906 (816)
Severity of ARDSnumber ()Mild ARDS
(PF ratio 201ndash300)10 (29) 14 (44)
Moderate ARDS(PF ratio 101ndash200)
20 (59) 14 (44)
Severe ARDS(PF ratio 100)
4 (12) 4 (12)
PEEP mean (SD) 65 (25) 62 (16)Quantitative pulmonary involvement
(as per chest radiograph)1 quadrant 0 (0) 0 (0)2 quadrant 2 (6) 2 (6)3 quadrant 7 (21) 6 (19)4 quadrant 25 (73) 24 (75)MAP mean (SD) 123 (51) 117 (42)OI mean (SD) 95 (108) 76 (46)VT (mlkg) mean (SD) 57 (17) 54 (13)PIP mean (SD) 194 (69) 186 (42)
Murrayrsquos lung injury scoreMild to moderate
(01ndash25)26 (76) 22 (69)
Severe (gt25) 8 (24) 10 (31)
IQRfrac14 interquartile range SDfrac14 standard deviation PaO2frac14 partial pres-sure of arterial oxygen FiO2frac14 fraction of inspired oxygenPEEPfrac14 positive end expiratory pressure PIPfrac14 peak inflating pressureMAPfrac14mean airway pressure OIfrac14 oxygenation Index VTfrac14 tidalvolumeaArterial blood gases in both groups were assessed at 0800 hours daily
High-dose Oral Ambroxol for pulmonary ARDS 343
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
D I S C U S S I O NCurrent study add to scarcely available data on clin-ical characteristics and outcomes of ventilated pediat-ric ARDS patients from developing economies [2 334] Ours being a tertiary care hospital without refer-ral and transport system we usually receive patientsvery late Thus patients are likely to be the severestof lot Pneumonia and bronchiolitis were commonest(90) causes of ARDS making it a syndrome ofrelatively homogeneous etiology in our setting as
against 40ndash65 reported from industrialized econo-mies (Table 4) PRISM-III score calculated fromdata collected during first 24 h of PICU admissionwere comparable with that in other pediatric ARDSstudies [35 37] However as all of our patients wereresuscitated and received post-resuscitation support-ive care (including hand-ventilation) for significantperiod in ERPWs before being shifted to PICUmany vital signs might have improved by the timethey reached PICU Thus actual PRISM-III scoresat beginning of hand-ventilation in ERPWs is likelyto be higher than ones calculated at PICU admissionmaking them sicker than what got reflected inPRISM-III scores All-cause mortality (of 26) is sig-nificantly higher compared with industrializedeconomies (Table 4) after factoring in higher meanPaO2FiO2 (gt175) lower mean OI (lt10) andlesser number of patients with immunocompromisedstatus Poor referral advanced stage of illness at ad-mission and suboptimal post-resuscitation care inERPWs may be one set of possible causative fac-tors While in PICU suboptimal patientsndashnurseratio poorly trained critical care nurses and poor in-fection control practices may be another These arethe issues of concern and indicate potentials of im-provement in critical care in the study settings
Early treatment was planned to have potentialbeneficial effects of ambroxol early during acute phase
Table 3 Primary and secondary outcome variables
Outcome Placebo (nfrac14 34) Ambroxol (nfrac14 32) pa
Primary outcome variableVentilator-free days at D14 (VFD14)b 50 (70) 50 (97) 056Ventilator-free days at D14 (VFD14) (mean 6 SD) 44 (36) 50 (45) ndash
Secondary outcome variablesAlive and ventilator-free at D14c 24 (71) 21 (66) 045Ventilator days among survivorsb 80 (45)(nfrac14 25) 70 (60) (nfrac14 24) 055Number of days to recover from ARDSd among survivorsb 100 (50)(nfrac14 25) 85 (70)(nfrac14 24) 054PICU stay among survivors (day)b 1200 (500) 1150 (775) 042All-cause mortalityc 9 (26) 8 (25) 089Early deaths (3 days)c 3 (38) 4 (44) 077Late deaths (gt3 days)c 5 (62) 5 (56)
ap-values are based on MannndashWhitney U test for number of VFD14 ventilator days among survivors time-to-recovery from ARDS duration of PICUstay v2 test (or Fisher Exact Test) for number of patients alive and ventilator-free at day 14 all-cause mortalitybData expressed as median (interquartile range)cData expressed as number (percentage)dAmong survivors number of days from randomization to meeting extubation readiness criteria for 24 consecutive hours through day 14
Time to recovery (Days)6050403020100
Cum
ulat
ive
a
t giv
en ti
me
10
08
06
04
02
00
placebo-censoreddrug-censoredplacebodrug
Study Groups
Fig 2 KaplanndashMeier curves comparing time-to-recoveryfrom ARDS in the two groups (censored for in-PICUmortality Log-Rank test pfrac14 094)
344 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
(a)
(b)
(c)
0
10
20
30
40
50
60
70
0 2 4 6 8 10 12 14 16
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
OI
0
100
200
300
400
500
600
700
0 5 10 15
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
PF
0
2
4
6
8
10
12
14
16
18
0 5 10 15
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
PEEP
Fig 3 Dot plot showing trend of mean PaO2FiO2 ratio oxygenation Index and PEEP during first 14 days
High-dose Oral Ambroxol for pulmonary ARDS 345
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
of illness We demonstrated safety tolerance and roleof high-dose oral ambroxol (40 mgkgday in fourdivided doses) in ventilated pARDS patients for thefirst time Ambroxol failed to improve oxygenationventilation VFD time-to-recovery mortality and thusto suggest therapeutic potential in pARDS in thestudy setting owing to small sample size Two-thirdsof patients had hypoalbuminemia and thus gut edema
possibly affecting ambroxolrsquos bioavailability Dosagechosen was maximal safe dose based on availableclinical data Therapeutic efficacy and safety of fur-ther higher dose may be subject of future scrutinyHigher doses may also be helpful in eradicating patho-gens adhered to bronchiolaralveolar epithelium [39]Ambroxol selectively gets concentrated in lungswithin 3 min of intravenous administration but it falls
(a)
(a)
0
50
100
150
200
250
0 2 4 6 8 10 12 14 16
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
PaCO
2
0
2
4
6
8
10
12
14
0 2 4 6 8 10 12 14 16
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
TV
FIG 4 Dot plot showing trend of mean tidal volume and PaCO2 during first 14 days
346 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
Tab
le4
Com
pari
son
ofcl
inic
alch
arac
teri
stic
san
dou
tcom
eof
pedi
atri
cA
RD
Sin
vari
ous
stud
ies
Clin
ical
Pro
file
Dah
lem
etal
[35
]C
urle
yet
al[
36]
Flor
iet
al[
37]
Wils
onet
al[
9]A
NZ
ICS
[38]
Hu et
al[
3]Z
hu etal
[2]
Che
tan
etal
[34
]In
dex
stud
y
nfrac14
443
nfrac14
102
nfrac14
328
nfrac14
152
nfrac14
117
nfrac14
306
nfrac14
401
nfrac14
17nfrac14
66
Stud
ype
riod
1998
ndash200
020
01ndash2
004
1996
ndash200
020
00ndash2
003
2004
ndash200
520
06ndash2
007
2009
2003
ndash200
620
07ndash2
008
Cou
ntry
ofst
udy
Net
herl
ands
USA
USA
USA
Aus
tral
iaan
dN
ewZ
eala
ndC
hina
Chi
naIn
dia
Indi
a
Pne
umon
ia11
4
56
35
34
46
75
63
18
82
Bro
nchi
oliti
s15
9
14
ndash7
12
ndashndash
ndash9
Asp
irat
ion
ndash11
15
8
8ndash
ndash6
5Se
psis
341
15
13
36
17
15
34
30
3
Nea
rdr
owni
ngndash
ndash9
53
ndash2
6ndash
Car
diac
dise
ase
ndashndash
7ndash
ndashndash
9ndash
ndashP
aO2
FiO
2ra
tio21
15a
147
and
153a
b
128
and
126a
b
17
71
and
190
6ab
Oxy
gena
tion
Inde
xN
A15
0an
d18
0a
b
200
and
205
ab
95
and
76a
b
Imm
uno-
com
prom
ised
Stat
us9
1N
A
34
45
Oth
ers
91
421
11
9
ndash1
540
2
Mor
talit
y27
8
22
28
35
45
30
70
26
NAfrac14
Info
rmat
ion
not
avai
labl
efrac14
info
rmat
ion
coul
dno
tbe
retr
ieve
ddu
eto
non-
acce
ssib
ility
offu
llm
anus
crip
ts
a Mea
nbIn
the
two
arm
sof
the
stud
yco
hort
High-dose Oral Ambroxol for pulmonary ARDS 347
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
dramatically at 2 h [33] Thus for sustained clinicaleffect more frequent administration (4 hourly or even2 hourly) may be required As pARDS was mostlycaused by pneumonia and bronchiolitis and majority(92) of survivors required ventilation for 14 daysD14 may be an optimal reference for measure of VFDin the study setting This pilot trial is relied on a con-venience sample results (Table 3) from which indi-cates need of sample size of 388 patients in each armwith one-sided significance level (a error) of 005 and80 power to detect 20 improvement in theobserved median VFD14 of 5 days (ie reduction of1 day in VFD14) [40]
Strengths include randomized design and care-fully planned protocols to define ventilator manage-ment sedation and extubation readiness to minimizevariations in daily management of patients Thereare many limitations as well major one being the un-regulated unmonitored hand-ventilation beforePICU admission which may have caused baro-trauma Lack of specific information on its durationmay be a potential confounder Study cohort was re-stricted to pARDS only These issues are unavoid-able and need to be tolerated to develop clinicallyefficacious interventions in the prevalent settingsHowever these would affect generalizability of re-sults Study was underpowered to demonstrate dif-ference in VFD14 There is lack of data onpharmacokinetics of enterally administered ambroxolin critically ill children It needs to be addressed be-fore conducting similar study in future Further in-flammatory oxidative and anti-protease markersshould also be evaluated to assess its pharmacologicefficacy Stratification according to severity of ARDSmay identify a subgroup of responders
C O N C L U S I O N SStudy provides useful information on prevalent situ-ation in the resource-constraint economies informsabout limitations in conducting trials in these set-tings and questionable generalizability of their re-sults Pediatric pARDS is mostly caused bypneumonia and bronchiolitis After factoring inhigher PaO2FiO2 lower OI and lesser patientswith immunocompromised states mortality is highcompared with industrialized peers High-dose oralambroxol failed to improve VFD14 In the current
cost-conscious health care environment its potentialas adjuvant therapy should be explored after havingaddressed the aforementioned issues Large pro-spective study of appropriate power with higherdoses of oral ambroxol administered more frequentlyis desirable VFD14 as composite outcome measuresis suggested for ventilated pediatric pARDS patientshowever it needs further validation
A C K N O W L E D G E M E N T SThe drug (ambroxol hydrochloride) was provided by MsAristo Pharmaceuticals Pvt Ltd Mumbai (India) The tabletsof drug (ambroxol) and placebo (lactose) was prepared atUniversity Institute of Pharmaceutical Sciences PunjabUniversity Chandigarh (India)
Work done at Emergency and Critical Care DivisionAdvanced Pediatrics Center Postgraduate Institute ofMedical Education and Research Chandigarh-160012 India
Presented at the 20th ESPNIC Medical amp NursingAnnual Congress at Verona Italy June 15ndash17 2009rdquo
R E F E R E N C E S1 Ventre KM Arnold JH Acute lung injury and acute re-
spiratory didtress syndrome In Nichols DG (ed) RogerrsquosTextbook of Pediatric Intensive Care 4th ednPhiladelphia PA Lippincott Williams amp Wilkins 2008731ndash66
2 Zhu YF Xu F Lu XL et al Chinese Collaborative StudyGroup for Pediatric Hypoxemic Respiratory FailureMortality and morbidity of acute hypoxemic respiratoryfailure and acute respiratory distress syndrome in infantsand young children Chin Med J 20121252265ndash71
3 Hu X Qian S Xu F et al Chinese Collaborative StudyGroup for Pediatric Respiratory Failure Incidence man-agement and mortality of acute hypoxemic respiratory fail-ure and acute respiratory distress syndrome from aprospective study of Chinese paediatric intensive care net-work Acta Paediatr 201099715ndash21
4 Hanson JH Flori H Application of the acute respiratorydistress syndrome network low-tidal volume strategy topediatric acute lung injury Respir Care Clin N Am 200612349ndash57
5 De Luca D Piastra M Tosi F et al Pharmacological thera-pies for pediatric and neonatal ALIARDS an evidence-based review Curr Drug Targets 201213906ndash16
6 Brun-Buisson C Richard JC Mercat A et al REVA-SRLFAH1N1v 2009 Registry Group Early corticosteroids insevere influenza AH1N1 pneumonia and acute respiratorydistress syndrome Am J Respir Crit Care Med 20111831200ndash6
348 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
7 Singer P Shapiro H Enteral omega-3 in acute respiratorydistress syndrome Curr Opin Clin Nutr Metab Care200912123ndash8
8 Pacht ER DeMichele SJ Nelson JL et al Enteral nutri-tion with eicosapentaenoic acid gamma-linolenic acidand antioxidants reduces alveolar inflammatory mediatorsand protein influx in patients with acute respiratory dis-tress syndrome Crit Care Med 200331491ndash500
9 Wilson DF Thomas NJ Markowitz BP et al Effect ofexogenous surfactant (calfactant) in pediatric acutelung injury a randomized controlled trial JAMA 2005293470ndash6
10 Matthay MA Abraham E Beta-adrenergic agonist therapyas a potential treatment for acute lung injury Am J RespirCrit Care Med 2006173254ndash5
11 Perkins GD McAuley DF Thickett DR et al The szlig-Agonist Lung Injury Trial (BALTI) a randomizedplacebo-controlled clinical trial Am J Respir Crit CareMed 2006173281ndash7
12 Wunderer H Morgenroth K Weis G The cleaningsystem of the airways physiology pathophysiologyand effects of ambroxol Med Monatsschr Pharm20093242ndash7
13 Malerba M Ragnoli B Ambroxol in the 21st centurypharmacological and clinical update Expert Opin DrugMetab Toxicol 200841119ndash29
14 Li Q Yao G Zhu X High-dose ambroxol reduces pul-monary complications in patients with acute cervical spi-nal cord injury after surgery Neurocrit Care 201216267ndash72
15 Wauer RR Schmalisch G Bohme B et al Randomizeddouble blind trial of Ambroxol for the treatment of respira-tory distress syndrome Eur J Pediatr 1992151357ndash63
16 Refai M Brunelli A Xiume F et al Short-term periopera-tive treatment with ambroxol reduces pulmonarycomplications and hospital costs after pulmonary lobec-tomy a randomized trial Eur J Cardiothorac Surg 200935469ndash73
17 Xia DH Xi L Xv C et al The protective effects ofambroxol on radiation lung injury and influence on pro-duction of transforming growth factor beta(1) and tumornecrosis factor alpha Med Oncol 201027697ndash701
18 Ulas MM Hizarci M Kunt A et al Protective effect ofambroxol on pulmonary function after cardiopulmonarybypass J Cardiovasc Pharmacol 200852518ndash23
19 Wang Y Wang FY Pan Z et al Effects of ambroxolcombined with low-dose heparin on TNF-alpha andIL-1beta in rabbits with acute lung injury [Article inChinese] Zhongguo Ying Yong Sheng Li Xue Za Zhi201127231ndash5
20 Su X Wang L Song Y et al Inhibition of inflammatoryresponses by ambroxol a mucolytic agent in a murinemodel of acute lung injury induced by lipopolysaccharideIntensive Care Med 200430133ndash140
21 Ma YT Tian YP Shi HW et al Effects of high doseambroxol on lung injury induced by paraquat in ratsZhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi200725523ndash6
22 ARDS Definition Task Force Ranieri VM RubenfeldGD Thompson BT et al Acute respiratory distress syn-drome the Berlin Definition JAMA 20123072526ndash33
23 Schulz M Hammrlein A Hinkel U Safety and usage pat-tern of an over-the-counter ambroxol cough syrup a com-munity pharmacy based cohort study Int J ClinPharmacol Ther 200644409ndash21
24 Schmalisch G Wauer RR Bohme B Effect of earlyambroxol treatment on lung functions in mechanically ven-tilated preterm newborns who subsequently developed abronchopulmonary dysplasia Respir Med 200094378ndash84
25 Couet W Girault J Reigner BG Steady-state bioavailabil-ity and pharmacokinetics of ambroxol and clenbuterol ad-ministered alone and combined in a new oral formulationInt J Clin Pharmacol Ther Toxicol 198927467ndash72
26 Schulz KF Altman DG Moher D CONSORT GroupCONSORT 2010 Statement updated guidelines for re-porting parallel group randomised trials BMC Med 2010818
27 Leteurtre S Martinot A Duhamel A et al Validation ofthe paediatric logistic organ dysfunction (PeLOD) scoreprospective observational multicentre study Lancet2003362192ndash7
28 Ramsay MAE How to use the Ramsay Score to assess thelevel of ICU Sedation http5jsnaccuminacjpHow20to20use20the20Ramsay20Score20too20assess20the20level20of20ICU20Sedationhtm (1August 2014 date last accessed)
29 Rubenfeld GD Caldwell E Peabody E et al Incidenceand outcomes of acute lung injury N Engl J Med 20053531685ndash93
30 Demling RH Adult respiratory distress syndrome cur-rent concepts New Horiz 19931388ndash401
31 Schoenfeld DA Bernard GR Network ARDS Statisticalevaluation of ventilator-free days as an efficacy measure inclinical trials of treatments for acute respiratory distresssyndrome Crit Care Med 2002301772ndash7
32 Horowitz IN Tai K Hypoalbuminemia in critically ill chil-dren Arch Pediatr Adolesc Med 20071611048ndash1052
33 Wauer RR Schmalisch G Ambroxol for prevention andtreatment of Hyaline membrane disease Eur Resp J 1989257sndash65s
34 Chetan G Rathisharmila R Narayanan P et al Acute re-spiratory distress syndrome in pediatric intensive careunit Indian J Pediatr 2009761013ndash16
35 Dahlem P van Aalderen W Hamaker M et al Incidenceand short-term outcome of acute lung injury in mechanic-ally ventilated children Eur Respir J 200322980ndash5
36 Curley MAQ Hibberd PL Fineman LD et al Effect ofprone positioning on clinical outcomes in children with
High-dose Oral Ambroxol for pulmonary ARDS 349
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
acute lung injury a randomized controlled trial JAMA2005294229ndash37
37 Flori HR Glidden DV Rutherford GW et al Pediatricacute lung injury prospective evaluation of risk factorsassociated with mortality Am J Respir Crit Care Med2005171995ndash1001
38 Erickson S Schibler A Numa A et al Paediatric StudyGroup Australian and New Zealand Intensive Care Society(ANZICS) Acute lung injury in pediatric intensive care in
Australia and New Zealand a prospective multicentre ob-servational study Pediatr Crit Care Med 20078317ndash23
39 Capsoni F Ongari AM Minonzio F Effect of ambroxolon human phagocytic cell function Boll Ist Sieroter Milan198564236ndash9
40 Sample Size Calculator Two Parallel Sample MeansHypothesis One-Sided Non-InferioritySuperiorityhttpwwwcctcuhkeduhkstatmeantsmp_suphtm(24 March 2015 date last accessed)
350 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
- fmv033-TF1
- fmv033-TF2
- fmv033-TF3
- fmv033-TF4
- fmv033-TF6
- fmv033-TF7
- fmv033-TF8
- fmv033-TF9
- fmv033-TF10
- fmv033-TF11
- fmv033-TF12
- fmv033-TF13
- fmv033-TF15
-

employed and included pressure-control ventilationwith peak inflating pressure lt30 cm H2O PEEP5ndash10 cm H2O tidal volume 5ndash6 mlkg FiO2 lt06and permissive hypercapnea (PaCO2 gt80torr whilepH gt725) if required Aim was to achieve optimaloxygenation (PaO2 60ndash80 mmHg SpO2 88ndash92)while limiting barotrauma Sedation protocolinvolved continuous diazepam (midazolam in some)and morphine infusions to achieve and maintainRamsay Score of 3ndash4 [28] with morning sedationinterruption Intravenous fluid was initiated as 23maintenance and feed was introduced at the earliestOnce patients were on full feed volume was relaxedto full maintenance After achievement of spontan-eous breathing oxygenation index (OI) lt6 decreaseandor plateau in ventilator support over 12 hourspatients were tested for extubation readiness Patientstatus was verified at discharge from PICU If diedprimary and secondary causes of death were re-corded Adverse events were monitored and reportedto Institutional Ethics Committee
Study outcomesConsidering difficulty in achieving mortality benefitin current critical care scenario [29] and unclear con-tribution of ARDS to mortality [30] composite out-come measure like ventilator-free days (VFD)incorporating both mortality and ventilation dur-ation are being considered [31] Primary outcomewas VFD14 which is defined as number of daysfrom point of successful weaning to day 14 (D14) ofenrollment Death during first 14 days is consideredto be equivalent to unresolved respiratory failureand thus is equated to zero VFD14 Secondary out-come measures included all-cause mortality ventila-tor days among survivors number of patients aliveand ventilator-free on D14 time-to-recovery fromARDS (ie when patients met extubation readinesscriteria after randomization) changes in ventilationand oxygenation parameters
Statistical analysisSimple unrestricted randomization was used to allo-cate patients in two groups Nonparametric MannndashWhitney U test and X2 test (or Fisherrsquos exact test ifrequired) were used to compare groups with quanti-tative outcomes Survival analysis using KaplanMeier curves was performed for time-to-event data
eg ventilation duration time-to-recovery and PICUstay Repeated measures analysis of variancewas planned to assess trend in ventilation and oxy-genation parameters SPSS version 16 was used forstatistical analysis A plt 005 was consideredsignificant
R E S U L T SOut of 67 eligible patients 33 were randomized toambroxol while 34 to placebo (Fig 1) Per-protocolanalysis was performed after excluding one patient inambroxol group who developed acute renal failureon day 2 leading to discontinuation of drugManagement included unmonitored hand-ventilationwith self-inflating bag for initial few hours (usuallyupto 24 h) in emergency room (ER) or pediatricwards (PWs) before PICU admission as more oftenthan not ventilator was not available for immediateapplication Of 66 patients 42(64) had moderateto severe ARDS (PaO2FiO2 200) [22] at ran-domization Thirteen of the remaining 24 patientswho had mild ARDS (PaO2FiO2 201ndash300) at en-rollment progressed in severity subsequently Twogroups were comparable for demographic profile nu-tritional status severity of illness at randomizationdiagnoses metabolic profile cause of lung injury aswell as in baseline respiratory characteristics (Tables1 and 2) Bronchopneumonia and bronchiolitis werethe commonest (91) causes of pARDS Three pa-tients (45) had chemotherapy-induced febrile neu-tropenia Eight (12) (four in each group) patientshad positive blood culture at PICU admissionmdashStaphylococcus aureus (3) Burkholderia cepacia (2)Acinetobacter (1) E coli (1) and Candida (1)
VFD14 was similar in two groups (pfrac14 056) sowas time-to-recovery from ARDS and other clinicaloutcomes (Table 3 and Fig 2) PaO2FiO2 OIneed for PEEP tidal volume and PaCO2 were alsosimilar during first 14 days (Figs 3 and 4) Healthcare associated infections (HCAIs) were seen in25(38) patients more in placebo group (1634 vs932 pfrac14 011) Out of these 19(76) were culturepositive gram-negative bacilli (14) being the com-monest (Candia 4 Staphylococcus 3) Blood-stream infections (14) were commonest followed byurinary tract infections (11) All-cause mortality was258 (1766) with similar distribution of early
342 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
(lt3 days) or late (gt3 days) deaths in the twogroups ARDS was considered as primary cause ofdeath in 53 (917) patients three of them wereimmunocompromised Forty-one percent (717)
of deaths were ascribed to HCAIs while onesuccumbed to hyperkalemia-induced arrhythmiaAmong survivors median (interquartile range) venti-lation duration was 7 (6) and 8 (45) days inambroxol and placebo groups respectively Diarrheawas noted in 6 (19) patients receiving ambroxolOne patient developed renal failure on D2 ofambroxol Serial blood pressure and cardiac compo-nent of PeLOD score were comparable in the twogroups during first 14 days contrasting the experi-mental data [33]
Table 1 Baseline patientsrsquo characteristics atenrollment
Characteristics Placebo(nfrac14 34)
Ambroxol(nfrac14 32)
Age (year) median (IQR) 115 (322) 137 (342)Age Number ()lt 1 year 16 (47) 13 (40)1ndash5 years 11 (32) 14 (44)gt5 years 7 (21) 5 (16)
Sex ratio (MF) 2311 2210Nutritional status (reference NCHS median)a
Normal (gt80) 18 (56) 17 (50)PEM grade 1 (71ndash80) 5 (16) 4 (12)PEM grade 2 (61ndash70) 5 (16) 8 (24)PEM grade 3 (51ndash60) 3 (9) 5 (15)PEM grade 4 (50) 1 (3) 0 (0)Serum albumin at
admission median(IQR) gmdl
229 (088) 260 (100)
Number ofpatients withhypoalbuminemia()b
24 (706) 23 (719)
PRISM III scoremedian (IQR)
500 (700) 600 (775)
PeLOD scoremedian (IQR)c
550 (1000) 1000 (1000)
Cause of pARDSPneumonia 29 (85) 27 (84)Bronchiolitis 5 (15) 1 (3)Kerosene poisoning 0 (0) 2 (6)Aspiration pneumonia 0 (0) 1 (3)Pulmonary hemorrhage 0 (0) 1 (3)
Blood culture positive 4 (12) 4 (13)Febrile Neutropenia 2 (6) 1 (3)
IQRfrac14 interquartile range PEMfrac14 protein energy malnutritionpARDSfrac14 Pulmonary Acute Respiratory DistressaMalnutrition was graded based on the criteria defined by IndianAcademy of PediatricsbHypoalbuminemia was defined as an albumin level of lt34 gdl for pa-tients gt7 months and lt25 gdl for patients lt7 months [32]cPeLOD Pediatric Logistic Organ Dysfunction (non-pulmonary) Score
Table 2 Baseline respiratory characteristics atenrollment
Respiratory characteristics Placebo(nfrac14 34)
Ambroxol(nfrac14 32)
PaO2FiO2 ratioa
mean (SD)1771 (707) 1906 (816)
Severity of ARDSnumber ()Mild ARDS
(PF ratio 201ndash300)10 (29) 14 (44)
Moderate ARDS(PF ratio 101ndash200)
20 (59) 14 (44)
Severe ARDS(PF ratio 100)
4 (12) 4 (12)
PEEP mean (SD) 65 (25) 62 (16)Quantitative pulmonary involvement
(as per chest radiograph)1 quadrant 0 (0) 0 (0)2 quadrant 2 (6) 2 (6)3 quadrant 7 (21) 6 (19)4 quadrant 25 (73) 24 (75)MAP mean (SD) 123 (51) 117 (42)OI mean (SD) 95 (108) 76 (46)VT (mlkg) mean (SD) 57 (17) 54 (13)PIP mean (SD) 194 (69) 186 (42)
Murrayrsquos lung injury scoreMild to moderate
(01ndash25)26 (76) 22 (69)
Severe (gt25) 8 (24) 10 (31)
IQRfrac14 interquartile range SDfrac14 standard deviation PaO2frac14 partial pres-sure of arterial oxygen FiO2frac14 fraction of inspired oxygenPEEPfrac14 positive end expiratory pressure PIPfrac14 peak inflating pressureMAPfrac14mean airway pressure OIfrac14 oxygenation Index VTfrac14 tidalvolumeaArterial blood gases in both groups were assessed at 0800 hours daily
High-dose Oral Ambroxol for pulmonary ARDS 343
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
D I S C U S S I O NCurrent study add to scarcely available data on clin-ical characteristics and outcomes of ventilated pediat-ric ARDS patients from developing economies [2 334] Ours being a tertiary care hospital without refer-ral and transport system we usually receive patientsvery late Thus patients are likely to be the severestof lot Pneumonia and bronchiolitis were commonest(90) causes of ARDS making it a syndrome ofrelatively homogeneous etiology in our setting as
against 40ndash65 reported from industrialized econo-mies (Table 4) PRISM-III score calculated fromdata collected during first 24 h of PICU admissionwere comparable with that in other pediatric ARDSstudies [35 37] However as all of our patients wereresuscitated and received post-resuscitation support-ive care (including hand-ventilation) for significantperiod in ERPWs before being shifted to PICUmany vital signs might have improved by the timethey reached PICU Thus actual PRISM-III scoresat beginning of hand-ventilation in ERPWs is likelyto be higher than ones calculated at PICU admissionmaking them sicker than what got reflected inPRISM-III scores All-cause mortality (of 26) is sig-nificantly higher compared with industrializedeconomies (Table 4) after factoring in higher meanPaO2FiO2 (gt175) lower mean OI (lt10) andlesser number of patients with immunocompromisedstatus Poor referral advanced stage of illness at ad-mission and suboptimal post-resuscitation care inERPWs may be one set of possible causative fac-tors While in PICU suboptimal patientsndashnurseratio poorly trained critical care nurses and poor in-fection control practices may be another These arethe issues of concern and indicate potentials of im-provement in critical care in the study settings
Early treatment was planned to have potentialbeneficial effects of ambroxol early during acute phase
Table 3 Primary and secondary outcome variables
Outcome Placebo (nfrac14 34) Ambroxol (nfrac14 32) pa
Primary outcome variableVentilator-free days at D14 (VFD14)b 50 (70) 50 (97) 056Ventilator-free days at D14 (VFD14) (mean 6 SD) 44 (36) 50 (45) ndash
Secondary outcome variablesAlive and ventilator-free at D14c 24 (71) 21 (66) 045Ventilator days among survivorsb 80 (45)(nfrac14 25) 70 (60) (nfrac14 24) 055Number of days to recover from ARDSd among survivorsb 100 (50)(nfrac14 25) 85 (70)(nfrac14 24) 054PICU stay among survivors (day)b 1200 (500) 1150 (775) 042All-cause mortalityc 9 (26) 8 (25) 089Early deaths (3 days)c 3 (38) 4 (44) 077Late deaths (gt3 days)c 5 (62) 5 (56)
ap-values are based on MannndashWhitney U test for number of VFD14 ventilator days among survivors time-to-recovery from ARDS duration of PICUstay v2 test (or Fisher Exact Test) for number of patients alive and ventilator-free at day 14 all-cause mortalitybData expressed as median (interquartile range)cData expressed as number (percentage)dAmong survivors number of days from randomization to meeting extubation readiness criteria for 24 consecutive hours through day 14
Time to recovery (Days)6050403020100
Cum
ulat
ive
a
t giv
en ti
me
10
08
06
04
02
00
placebo-censoreddrug-censoredplacebodrug
Study Groups
Fig 2 KaplanndashMeier curves comparing time-to-recoveryfrom ARDS in the two groups (censored for in-PICUmortality Log-Rank test pfrac14 094)
344 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
(a)
(b)
(c)
0
10
20
30
40
50
60
70
0 2 4 6 8 10 12 14 16
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
OI
0
100
200
300
400
500
600
700
0 5 10 15
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
PF
0
2
4
6
8
10
12
14
16
18
0 5 10 15
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
PEEP
Fig 3 Dot plot showing trend of mean PaO2FiO2 ratio oxygenation Index and PEEP during first 14 days
High-dose Oral Ambroxol for pulmonary ARDS 345
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
of illness We demonstrated safety tolerance and roleof high-dose oral ambroxol (40 mgkgday in fourdivided doses) in ventilated pARDS patients for thefirst time Ambroxol failed to improve oxygenationventilation VFD time-to-recovery mortality and thusto suggest therapeutic potential in pARDS in thestudy setting owing to small sample size Two-thirdsof patients had hypoalbuminemia and thus gut edema
possibly affecting ambroxolrsquos bioavailability Dosagechosen was maximal safe dose based on availableclinical data Therapeutic efficacy and safety of fur-ther higher dose may be subject of future scrutinyHigher doses may also be helpful in eradicating patho-gens adhered to bronchiolaralveolar epithelium [39]Ambroxol selectively gets concentrated in lungswithin 3 min of intravenous administration but it falls
(a)
(a)
0
50
100
150
200
250
0 2 4 6 8 10 12 14 16
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
PaCO
2
0
2
4
6
8
10
12
14
0 2 4 6 8 10 12 14 16
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
TV
FIG 4 Dot plot showing trend of mean tidal volume and PaCO2 during first 14 days
346 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
Tab
le4
Com
pari
son
ofcl
inic
alch
arac
teri
stic
san
dou
tcom
eof
pedi
atri
cA
RD
Sin
vari
ous
stud
ies
Clin
ical
Pro
file
Dah
lem
etal
[35
]C
urle
yet
al[
36]
Flor
iet
al[
37]
Wils
onet
al[
9]A
NZ
ICS
[38]
Hu et
al[
3]Z
hu etal
[2]
Che
tan
etal
[34
]In
dex
stud
y
nfrac14
443
nfrac14
102
nfrac14
328
nfrac14
152
nfrac14
117
nfrac14
306
nfrac14
401
nfrac14
17nfrac14
66
Stud
ype
riod
1998
ndash200
020
01ndash2
004
1996
ndash200
020
00ndash2
003
2004
ndash200
520
06ndash2
007
2009
2003
ndash200
620
07ndash2
008
Cou
ntry
ofst
udy
Net
herl
ands
USA
USA
USA
Aus
tral
iaan
dN
ewZ
eala
ndC
hina
Chi
naIn
dia
Indi
a
Pne
umon
ia11
4
56
35
34
46
75
63
18
82
Bro
nchi
oliti
s15
9
14
ndash7
12
ndashndash
ndash9
Asp
irat
ion
ndash11
15
8
8ndash
ndash6
5Se
psis
341
15
13
36
17
15
34
30
3
Nea
rdr
owni
ngndash
ndash9
53
ndash2
6ndash
Car
diac
dise
ase
ndashndash
7ndash
ndashndash
9ndash
ndashP
aO2
FiO
2ra
tio21
15a
147
and
153a
b
128
and
126a
b
17
71
and
190
6ab
Oxy
gena
tion
Inde
xN
A15
0an
d18
0a
b
200
and
205
ab
95
and
76a
b
Imm
uno-
com
prom
ised
Stat
us9
1N
A
34
45
Oth
ers
91
421
11
9
ndash1
540
2
Mor
talit
y27
8
22
28
35
45
30
70
26
NAfrac14
Info
rmat
ion
not
avai
labl
efrac14
info
rmat
ion
coul
dno
tbe
retr
ieve
ddu
eto
non-
acce
ssib
ility
offu
llm
anus
crip
ts
a Mea
nbIn
the
two
arm
sof
the
stud
yco
hort
High-dose Oral Ambroxol for pulmonary ARDS 347
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
dramatically at 2 h [33] Thus for sustained clinicaleffect more frequent administration (4 hourly or even2 hourly) may be required As pARDS was mostlycaused by pneumonia and bronchiolitis and majority(92) of survivors required ventilation for 14 daysD14 may be an optimal reference for measure of VFDin the study setting This pilot trial is relied on a con-venience sample results (Table 3) from which indi-cates need of sample size of 388 patients in each armwith one-sided significance level (a error) of 005 and80 power to detect 20 improvement in theobserved median VFD14 of 5 days (ie reduction of1 day in VFD14) [40]
Strengths include randomized design and care-fully planned protocols to define ventilator manage-ment sedation and extubation readiness to minimizevariations in daily management of patients Thereare many limitations as well major one being the un-regulated unmonitored hand-ventilation beforePICU admission which may have caused baro-trauma Lack of specific information on its durationmay be a potential confounder Study cohort was re-stricted to pARDS only These issues are unavoid-able and need to be tolerated to develop clinicallyefficacious interventions in the prevalent settingsHowever these would affect generalizability of re-sults Study was underpowered to demonstrate dif-ference in VFD14 There is lack of data onpharmacokinetics of enterally administered ambroxolin critically ill children It needs to be addressed be-fore conducting similar study in future Further in-flammatory oxidative and anti-protease markersshould also be evaluated to assess its pharmacologicefficacy Stratification according to severity of ARDSmay identify a subgroup of responders
C O N C L U S I O N SStudy provides useful information on prevalent situ-ation in the resource-constraint economies informsabout limitations in conducting trials in these set-tings and questionable generalizability of their re-sults Pediatric pARDS is mostly caused bypneumonia and bronchiolitis After factoring inhigher PaO2FiO2 lower OI and lesser patientswith immunocompromised states mortality is highcompared with industrialized peers High-dose oralambroxol failed to improve VFD14 In the current
cost-conscious health care environment its potentialas adjuvant therapy should be explored after havingaddressed the aforementioned issues Large pro-spective study of appropriate power with higherdoses of oral ambroxol administered more frequentlyis desirable VFD14 as composite outcome measuresis suggested for ventilated pediatric pARDS patientshowever it needs further validation
A C K N O W L E D G E M E N T SThe drug (ambroxol hydrochloride) was provided by MsAristo Pharmaceuticals Pvt Ltd Mumbai (India) The tabletsof drug (ambroxol) and placebo (lactose) was prepared atUniversity Institute of Pharmaceutical Sciences PunjabUniversity Chandigarh (India)
Work done at Emergency and Critical Care DivisionAdvanced Pediatrics Center Postgraduate Institute ofMedical Education and Research Chandigarh-160012 India
Presented at the 20th ESPNIC Medical amp NursingAnnual Congress at Verona Italy June 15ndash17 2009rdquo
R E F E R E N C E S1 Ventre KM Arnold JH Acute lung injury and acute re-
spiratory didtress syndrome In Nichols DG (ed) RogerrsquosTextbook of Pediatric Intensive Care 4th ednPhiladelphia PA Lippincott Williams amp Wilkins 2008731ndash66
2 Zhu YF Xu F Lu XL et al Chinese Collaborative StudyGroup for Pediatric Hypoxemic Respiratory FailureMortality and morbidity of acute hypoxemic respiratoryfailure and acute respiratory distress syndrome in infantsand young children Chin Med J 20121252265ndash71
3 Hu X Qian S Xu F et al Chinese Collaborative StudyGroup for Pediatric Respiratory Failure Incidence man-agement and mortality of acute hypoxemic respiratory fail-ure and acute respiratory distress syndrome from aprospective study of Chinese paediatric intensive care net-work Acta Paediatr 201099715ndash21
4 Hanson JH Flori H Application of the acute respiratorydistress syndrome network low-tidal volume strategy topediatric acute lung injury Respir Care Clin N Am 200612349ndash57
5 De Luca D Piastra M Tosi F et al Pharmacological thera-pies for pediatric and neonatal ALIARDS an evidence-based review Curr Drug Targets 201213906ndash16
6 Brun-Buisson C Richard JC Mercat A et al REVA-SRLFAH1N1v 2009 Registry Group Early corticosteroids insevere influenza AH1N1 pneumonia and acute respiratorydistress syndrome Am J Respir Crit Care Med 20111831200ndash6
348 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
7 Singer P Shapiro H Enteral omega-3 in acute respiratorydistress syndrome Curr Opin Clin Nutr Metab Care200912123ndash8
8 Pacht ER DeMichele SJ Nelson JL et al Enteral nutri-tion with eicosapentaenoic acid gamma-linolenic acidand antioxidants reduces alveolar inflammatory mediatorsand protein influx in patients with acute respiratory dis-tress syndrome Crit Care Med 200331491ndash500
9 Wilson DF Thomas NJ Markowitz BP et al Effect ofexogenous surfactant (calfactant) in pediatric acutelung injury a randomized controlled trial JAMA 2005293470ndash6
10 Matthay MA Abraham E Beta-adrenergic agonist therapyas a potential treatment for acute lung injury Am J RespirCrit Care Med 2006173254ndash5
11 Perkins GD McAuley DF Thickett DR et al The szlig-Agonist Lung Injury Trial (BALTI) a randomizedplacebo-controlled clinical trial Am J Respir Crit CareMed 2006173281ndash7
12 Wunderer H Morgenroth K Weis G The cleaningsystem of the airways physiology pathophysiologyand effects of ambroxol Med Monatsschr Pharm20093242ndash7
13 Malerba M Ragnoli B Ambroxol in the 21st centurypharmacological and clinical update Expert Opin DrugMetab Toxicol 200841119ndash29
14 Li Q Yao G Zhu X High-dose ambroxol reduces pul-monary complications in patients with acute cervical spi-nal cord injury after surgery Neurocrit Care 201216267ndash72
15 Wauer RR Schmalisch G Bohme B et al Randomizeddouble blind trial of Ambroxol for the treatment of respira-tory distress syndrome Eur J Pediatr 1992151357ndash63
16 Refai M Brunelli A Xiume F et al Short-term periopera-tive treatment with ambroxol reduces pulmonarycomplications and hospital costs after pulmonary lobec-tomy a randomized trial Eur J Cardiothorac Surg 200935469ndash73
17 Xia DH Xi L Xv C et al The protective effects ofambroxol on radiation lung injury and influence on pro-duction of transforming growth factor beta(1) and tumornecrosis factor alpha Med Oncol 201027697ndash701
18 Ulas MM Hizarci M Kunt A et al Protective effect ofambroxol on pulmonary function after cardiopulmonarybypass J Cardiovasc Pharmacol 200852518ndash23
19 Wang Y Wang FY Pan Z et al Effects of ambroxolcombined with low-dose heparin on TNF-alpha andIL-1beta in rabbits with acute lung injury [Article inChinese] Zhongguo Ying Yong Sheng Li Xue Za Zhi201127231ndash5
20 Su X Wang L Song Y et al Inhibition of inflammatoryresponses by ambroxol a mucolytic agent in a murinemodel of acute lung injury induced by lipopolysaccharideIntensive Care Med 200430133ndash140
21 Ma YT Tian YP Shi HW et al Effects of high doseambroxol on lung injury induced by paraquat in ratsZhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi200725523ndash6
22 ARDS Definition Task Force Ranieri VM RubenfeldGD Thompson BT et al Acute respiratory distress syn-drome the Berlin Definition JAMA 20123072526ndash33
23 Schulz M Hammrlein A Hinkel U Safety and usage pat-tern of an over-the-counter ambroxol cough syrup a com-munity pharmacy based cohort study Int J ClinPharmacol Ther 200644409ndash21
24 Schmalisch G Wauer RR Bohme B Effect of earlyambroxol treatment on lung functions in mechanically ven-tilated preterm newborns who subsequently developed abronchopulmonary dysplasia Respir Med 200094378ndash84
25 Couet W Girault J Reigner BG Steady-state bioavailabil-ity and pharmacokinetics of ambroxol and clenbuterol ad-ministered alone and combined in a new oral formulationInt J Clin Pharmacol Ther Toxicol 198927467ndash72
26 Schulz KF Altman DG Moher D CONSORT GroupCONSORT 2010 Statement updated guidelines for re-porting parallel group randomised trials BMC Med 2010818
27 Leteurtre S Martinot A Duhamel A et al Validation ofthe paediatric logistic organ dysfunction (PeLOD) scoreprospective observational multicentre study Lancet2003362192ndash7
28 Ramsay MAE How to use the Ramsay Score to assess thelevel of ICU Sedation http5jsnaccuminacjpHow20to20use20the20Ramsay20Score20too20assess20the20level20of20ICU20Sedationhtm (1August 2014 date last accessed)
29 Rubenfeld GD Caldwell E Peabody E et al Incidenceand outcomes of acute lung injury N Engl J Med 20053531685ndash93
30 Demling RH Adult respiratory distress syndrome cur-rent concepts New Horiz 19931388ndash401
31 Schoenfeld DA Bernard GR Network ARDS Statisticalevaluation of ventilator-free days as an efficacy measure inclinical trials of treatments for acute respiratory distresssyndrome Crit Care Med 2002301772ndash7
32 Horowitz IN Tai K Hypoalbuminemia in critically ill chil-dren Arch Pediatr Adolesc Med 20071611048ndash1052
33 Wauer RR Schmalisch G Ambroxol for prevention andtreatment of Hyaline membrane disease Eur Resp J 1989257sndash65s
34 Chetan G Rathisharmila R Narayanan P et al Acute re-spiratory distress syndrome in pediatric intensive careunit Indian J Pediatr 2009761013ndash16
35 Dahlem P van Aalderen W Hamaker M et al Incidenceand short-term outcome of acute lung injury in mechanic-ally ventilated children Eur Respir J 200322980ndash5
36 Curley MAQ Hibberd PL Fineman LD et al Effect ofprone positioning on clinical outcomes in children with
High-dose Oral Ambroxol for pulmonary ARDS 349
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
acute lung injury a randomized controlled trial JAMA2005294229ndash37
37 Flori HR Glidden DV Rutherford GW et al Pediatricacute lung injury prospective evaluation of risk factorsassociated with mortality Am J Respir Crit Care Med2005171995ndash1001
38 Erickson S Schibler A Numa A et al Paediatric StudyGroup Australian and New Zealand Intensive Care Society(ANZICS) Acute lung injury in pediatric intensive care in
Australia and New Zealand a prospective multicentre ob-servational study Pediatr Crit Care Med 20078317ndash23
39 Capsoni F Ongari AM Minonzio F Effect of ambroxolon human phagocytic cell function Boll Ist Sieroter Milan198564236ndash9
40 Sample Size Calculator Two Parallel Sample MeansHypothesis One-Sided Non-InferioritySuperiorityhttpwwwcctcuhkeduhkstatmeantsmp_suphtm(24 March 2015 date last accessed)
350 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
- fmv033-TF1
- fmv033-TF2
- fmv033-TF3
- fmv033-TF4
- fmv033-TF6
- fmv033-TF7
- fmv033-TF8
- fmv033-TF9
- fmv033-TF10
- fmv033-TF11
- fmv033-TF12
- fmv033-TF13
- fmv033-TF15
-

(lt3 days) or late (gt3 days) deaths in the twogroups ARDS was considered as primary cause ofdeath in 53 (917) patients three of them wereimmunocompromised Forty-one percent (717)
of deaths were ascribed to HCAIs while onesuccumbed to hyperkalemia-induced arrhythmiaAmong survivors median (interquartile range) venti-lation duration was 7 (6) and 8 (45) days inambroxol and placebo groups respectively Diarrheawas noted in 6 (19) patients receiving ambroxolOne patient developed renal failure on D2 ofambroxol Serial blood pressure and cardiac compo-nent of PeLOD score were comparable in the twogroups during first 14 days contrasting the experi-mental data [33]
Table 1 Baseline patientsrsquo characteristics atenrollment
Characteristics Placebo(nfrac14 34)
Ambroxol(nfrac14 32)
Age (year) median (IQR) 115 (322) 137 (342)Age Number ()lt 1 year 16 (47) 13 (40)1ndash5 years 11 (32) 14 (44)gt5 years 7 (21) 5 (16)
Sex ratio (MF) 2311 2210Nutritional status (reference NCHS median)a
Normal (gt80) 18 (56) 17 (50)PEM grade 1 (71ndash80) 5 (16) 4 (12)PEM grade 2 (61ndash70) 5 (16) 8 (24)PEM grade 3 (51ndash60) 3 (9) 5 (15)PEM grade 4 (50) 1 (3) 0 (0)Serum albumin at
admission median(IQR) gmdl
229 (088) 260 (100)
Number ofpatients withhypoalbuminemia()b
24 (706) 23 (719)
PRISM III scoremedian (IQR)
500 (700) 600 (775)
PeLOD scoremedian (IQR)c
550 (1000) 1000 (1000)
Cause of pARDSPneumonia 29 (85) 27 (84)Bronchiolitis 5 (15) 1 (3)Kerosene poisoning 0 (0) 2 (6)Aspiration pneumonia 0 (0) 1 (3)Pulmonary hemorrhage 0 (0) 1 (3)
Blood culture positive 4 (12) 4 (13)Febrile Neutropenia 2 (6) 1 (3)
IQRfrac14 interquartile range PEMfrac14 protein energy malnutritionpARDSfrac14 Pulmonary Acute Respiratory DistressaMalnutrition was graded based on the criteria defined by IndianAcademy of PediatricsbHypoalbuminemia was defined as an albumin level of lt34 gdl for pa-tients gt7 months and lt25 gdl for patients lt7 months [32]cPeLOD Pediatric Logistic Organ Dysfunction (non-pulmonary) Score
Table 2 Baseline respiratory characteristics atenrollment
Respiratory characteristics Placebo(nfrac14 34)
Ambroxol(nfrac14 32)
PaO2FiO2 ratioa
mean (SD)1771 (707) 1906 (816)
Severity of ARDSnumber ()Mild ARDS
(PF ratio 201ndash300)10 (29) 14 (44)
Moderate ARDS(PF ratio 101ndash200)
20 (59) 14 (44)
Severe ARDS(PF ratio 100)
4 (12) 4 (12)
PEEP mean (SD) 65 (25) 62 (16)Quantitative pulmonary involvement
(as per chest radiograph)1 quadrant 0 (0) 0 (0)2 quadrant 2 (6) 2 (6)3 quadrant 7 (21) 6 (19)4 quadrant 25 (73) 24 (75)MAP mean (SD) 123 (51) 117 (42)OI mean (SD) 95 (108) 76 (46)VT (mlkg) mean (SD) 57 (17) 54 (13)PIP mean (SD) 194 (69) 186 (42)
Murrayrsquos lung injury scoreMild to moderate
(01ndash25)26 (76) 22 (69)
Severe (gt25) 8 (24) 10 (31)
IQRfrac14 interquartile range SDfrac14 standard deviation PaO2frac14 partial pres-sure of arterial oxygen FiO2frac14 fraction of inspired oxygenPEEPfrac14 positive end expiratory pressure PIPfrac14 peak inflating pressureMAPfrac14mean airway pressure OIfrac14 oxygenation Index VTfrac14 tidalvolumeaArterial blood gases in both groups were assessed at 0800 hours daily
High-dose Oral Ambroxol for pulmonary ARDS 343
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
D I S C U S S I O NCurrent study add to scarcely available data on clin-ical characteristics and outcomes of ventilated pediat-ric ARDS patients from developing economies [2 334] Ours being a tertiary care hospital without refer-ral and transport system we usually receive patientsvery late Thus patients are likely to be the severestof lot Pneumonia and bronchiolitis were commonest(90) causes of ARDS making it a syndrome ofrelatively homogeneous etiology in our setting as
against 40ndash65 reported from industrialized econo-mies (Table 4) PRISM-III score calculated fromdata collected during first 24 h of PICU admissionwere comparable with that in other pediatric ARDSstudies [35 37] However as all of our patients wereresuscitated and received post-resuscitation support-ive care (including hand-ventilation) for significantperiod in ERPWs before being shifted to PICUmany vital signs might have improved by the timethey reached PICU Thus actual PRISM-III scoresat beginning of hand-ventilation in ERPWs is likelyto be higher than ones calculated at PICU admissionmaking them sicker than what got reflected inPRISM-III scores All-cause mortality (of 26) is sig-nificantly higher compared with industrializedeconomies (Table 4) after factoring in higher meanPaO2FiO2 (gt175) lower mean OI (lt10) andlesser number of patients with immunocompromisedstatus Poor referral advanced stage of illness at ad-mission and suboptimal post-resuscitation care inERPWs may be one set of possible causative fac-tors While in PICU suboptimal patientsndashnurseratio poorly trained critical care nurses and poor in-fection control practices may be another These arethe issues of concern and indicate potentials of im-provement in critical care in the study settings
Early treatment was planned to have potentialbeneficial effects of ambroxol early during acute phase
Table 3 Primary and secondary outcome variables
Outcome Placebo (nfrac14 34) Ambroxol (nfrac14 32) pa
Primary outcome variableVentilator-free days at D14 (VFD14)b 50 (70) 50 (97) 056Ventilator-free days at D14 (VFD14) (mean 6 SD) 44 (36) 50 (45) ndash
Secondary outcome variablesAlive and ventilator-free at D14c 24 (71) 21 (66) 045Ventilator days among survivorsb 80 (45)(nfrac14 25) 70 (60) (nfrac14 24) 055Number of days to recover from ARDSd among survivorsb 100 (50)(nfrac14 25) 85 (70)(nfrac14 24) 054PICU stay among survivors (day)b 1200 (500) 1150 (775) 042All-cause mortalityc 9 (26) 8 (25) 089Early deaths (3 days)c 3 (38) 4 (44) 077Late deaths (gt3 days)c 5 (62) 5 (56)
ap-values are based on MannndashWhitney U test for number of VFD14 ventilator days among survivors time-to-recovery from ARDS duration of PICUstay v2 test (or Fisher Exact Test) for number of patients alive and ventilator-free at day 14 all-cause mortalitybData expressed as median (interquartile range)cData expressed as number (percentage)dAmong survivors number of days from randomization to meeting extubation readiness criteria for 24 consecutive hours through day 14
Time to recovery (Days)6050403020100
Cum
ulat
ive
a
t giv
en ti
me
10
08
06
04
02
00
placebo-censoreddrug-censoredplacebodrug
Study Groups
Fig 2 KaplanndashMeier curves comparing time-to-recoveryfrom ARDS in the two groups (censored for in-PICUmortality Log-Rank test pfrac14 094)
344 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
(a)
(b)
(c)
0
10
20
30
40
50
60
70
0 2 4 6 8 10 12 14 16
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
OI
0
100
200
300
400
500
600
700
0 5 10 15
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
PF
0
2
4
6
8
10
12
14
16
18
0 5 10 15
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
PEEP
Fig 3 Dot plot showing trend of mean PaO2FiO2 ratio oxygenation Index and PEEP during first 14 days
High-dose Oral Ambroxol for pulmonary ARDS 345
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
of illness We demonstrated safety tolerance and roleof high-dose oral ambroxol (40 mgkgday in fourdivided doses) in ventilated pARDS patients for thefirst time Ambroxol failed to improve oxygenationventilation VFD time-to-recovery mortality and thusto suggest therapeutic potential in pARDS in thestudy setting owing to small sample size Two-thirdsof patients had hypoalbuminemia and thus gut edema
possibly affecting ambroxolrsquos bioavailability Dosagechosen was maximal safe dose based on availableclinical data Therapeutic efficacy and safety of fur-ther higher dose may be subject of future scrutinyHigher doses may also be helpful in eradicating patho-gens adhered to bronchiolaralveolar epithelium [39]Ambroxol selectively gets concentrated in lungswithin 3 min of intravenous administration but it falls
(a)
(a)
0
50
100
150
200
250
0 2 4 6 8 10 12 14 16
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
PaCO
2
0
2
4
6
8
10
12
14
0 2 4 6 8 10 12 14 16
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
TV
FIG 4 Dot plot showing trend of mean tidal volume and PaCO2 during first 14 days
346 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
Tab
le4
Com
pari
son
ofcl
inic
alch
arac
teri
stic
san
dou
tcom
eof
pedi
atri
cA
RD
Sin
vari
ous
stud
ies
Clin
ical
Pro
file
Dah
lem
etal
[35
]C
urle
yet
al[
36]
Flor
iet
al[
37]
Wils
onet
al[
9]A
NZ
ICS
[38]
Hu et
al[
3]Z
hu etal
[2]
Che
tan
etal
[34
]In
dex
stud
y
nfrac14
443
nfrac14
102
nfrac14
328
nfrac14
152
nfrac14
117
nfrac14
306
nfrac14
401
nfrac14
17nfrac14
66
Stud
ype
riod
1998
ndash200
020
01ndash2
004
1996
ndash200
020
00ndash2
003
2004
ndash200
520
06ndash2
007
2009
2003
ndash200
620
07ndash2
008
Cou
ntry
ofst
udy
Net
herl
ands
USA
USA
USA
Aus
tral
iaan
dN
ewZ
eala
ndC
hina
Chi
naIn
dia
Indi
a
Pne
umon
ia11
4
56
35
34
46
75
63
18
82
Bro
nchi
oliti
s15
9
14
ndash7
12
ndashndash
ndash9
Asp
irat
ion
ndash11
15
8
8ndash
ndash6
5Se
psis
341
15
13
36
17
15
34
30
3
Nea
rdr
owni
ngndash
ndash9
53
ndash2
6ndash
Car
diac
dise
ase
ndashndash
7ndash
ndashndash
9ndash
ndashP
aO2
FiO
2ra
tio21
15a
147
and
153a
b
128
and
126a
b
17
71
and
190
6ab
Oxy
gena
tion
Inde
xN
A15
0an
d18
0a
b
200
and
205
ab
95
and
76a
b
Imm
uno-
com
prom
ised
Stat
us9
1N
A
34
45
Oth
ers
91
421
11
9
ndash1
540
2
Mor
talit
y27
8
22
28
35
45
30
70
26
NAfrac14
Info
rmat
ion
not
avai
labl
efrac14
info
rmat
ion
coul
dno
tbe
retr
ieve
ddu
eto
non-
acce
ssib
ility
offu
llm
anus
crip
ts
a Mea
nbIn
the
two
arm
sof
the
stud
yco
hort
High-dose Oral Ambroxol for pulmonary ARDS 347
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
dramatically at 2 h [33] Thus for sustained clinicaleffect more frequent administration (4 hourly or even2 hourly) may be required As pARDS was mostlycaused by pneumonia and bronchiolitis and majority(92) of survivors required ventilation for 14 daysD14 may be an optimal reference for measure of VFDin the study setting This pilot trial is relied on a con-venience sample results (Table 3) from which indi-cates need of sample size of 388 patients in each armwith one-sided significance level (a error) of 005 and80 power to detect 20 improvement in theobserved median VFD14 of 5 days (ie reduction of1 day in VFD14) [40]
Strengths include randomized design and care-fully planned protocols to define ventilator manage-ment sedation and extubation readiness to minimizevariations in daily management of patients Thereare many limitations as well major one being the un-regulated unmonitored hand-ventilation beforePICU admission which may have caused baro-trauma Lack of specific information on its durationmay be a potential confounder Study cohort was re-stricted to pARDS only These issues are unavoid-able and need to be tolerated to develop clinicallyefficacious interventions in the prevalent settingsHowever these would affect generalizability of re-sults Study was underpowered to demonstrate dif-ference in VFD14 There is lack of data onpharmacokinetics of enterally administered ambroxolin critically ill children It needs to be addressed be-fore conducting similar study in future Further in-flammatory oxidative and anti-protease markersshould also be evaluated to assess its pharmacologicefficacy Stratification according to severity of ARDSmay identify a subgroup of responders
C O N C L U S I O N SStudy provides useful information on prevalent situ-ation in the resource-constraint economies informsabout limitations in conducting trials in these set-tings and questionable generalizability of their re-sults Pediatric pARDS is mostly caused bypneumonia and bronchiolitis After factoring inhigher PaO2FiO2 lower OI and lesser patientswith immunocompromised states mortality is highcompared with industrialized peers High-dose oralambroxol failed to improve VFD14 In the current
cost-conscious health care environment its potentialas adjuvant therapy should be explored after havingaddressed the aforementioned issues Large pro-spective study of appropriate power with higherdoses of oral ambroxol administered more frequentlyis desirable VFD14 as composite outcome measuresis suggested for ventilated pediatric pARDS patientshowever it needs further validation
A C K N O W L E D G E M E N T SThe drug (ambroxol hydrochloride) was provided by MsAristo Pharmaceuticals Pvt Ltd Mumbai (India) The tabletsof drug (ambroxol) and placebo (lactose) was prepared atUniversity Institute of Pharmaceutical Sciences PunjabUniversity Chandigarh (India)
Work done at Emergency and Critical Care DivisionAdvanced Pediatrics Center Postgraduate Institute ofMedical Education and Research Chandigarh-160012 India
Presented at the 20th ESPNIC Medical amp NursingAnnual Congress at Verona Italy June 15ndash17 2009rdquo
R E F E R E N C E S1 Ventre KM Arnold JH Acute lung injury and acute re-
spiratory didtress syndrome In Nichols DG (ed) RogerrsquosTextbook of Pediatric Intensive Care 4th ednPhiladelphia PA Lippincott Williams amp Wilkins 2008731ndash66
2 Zhu YF Xu F Lu XL et al Chinese Collaborative StudyGroup for Pediatric Hypoxemic Respiratory FailureMortality and morbidity of acute hypoxemic respiratoryfailure and acute respiratory distress syndrome in infantsand young children Chin Med J 20121252265ndash71
3 Hu X Qian S Xu F et al Chinese Collaborative StudyGroup for Pediatric Respiratory Failure Incidence man-agement and mortality of acute hypoxemic respiratory fail-ure and acute respiratory distress syndrome from aprospective study of Chinese paediatric intensive care net-work Acta Paediatr 201099715ndash21
4 Hanson JH Flori H Application of the acute respiratorydistress syndrome network low-tidal volume strategy topediatric acute lung injury Respir Care Clin N Am 200612349ndash57
5 De Luca D Piastra M Tosi F et al Pharmacological thera-pies for pediatric and neonatal ALIARDS an evidence-based review Curr Drug Targets 201213906ndash16
6 Brun-Buisson C Richard JC Mercat A et al REVA-SRLFAH1N1v 2009 Registry Group Early corticosteroids insevere influenza AH1N1 pneumonia and acute respiratorydistress syndrome Am J Respir Crit Care Med 20111831200ndash6
348 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
7 Singer P Shapiro H Enteral omega-3 in acute respiratorydistress syndrome Curr Opin Clin Nutr Metab Care200912123ndash8
8 Pacht ER DeMichele SJ Nelson JL et al Enteral nutri-tion with eicosapentaenoic acid gamma-linolenic acidand antioxidants reduces alveolar inflammatory mediatorsand protein influx in patients with acute respiratory dis-tress syndrome Crit Care Med 200331491ndash500
9 Wilson DF Thomas NJ Markowitz BP et al Effect ofexogenous surfactant (calfactant) in pediatric acutelung injury a randomized controlled trial JAMA 2005293470ndash6
10 Matthay MA Abraham E Beta-adrenergic agonist therapyas a potential treatment for acute lung injury Am J RespirCrit Care Med 2006173254ndash5
11 Perkins GD McAuley DF Thickett DR et al The szlig-Agonist Lung Injury Trial (BALTI) a randomizedplacebo-controlled clinical trial Am J Respir Crit CareMed 2006173281ndash7
12 Wunderer H Morgenroth K Weis G The cleaningsystem of the airways physiology pathophysiologyand effects of ambroxol Med Monatsschr Pharm20093242ndash7
13 Malerba M Ragnoli B Ambroxol in the 21st centurypharmacological and clinical update Expert Opin DrugMetab Toxicol 200841119ndash29
14 Li Q Yao G Zhu X High-dose ambroxol reduces pul-monary complications in patients with acute cervical spi-nal cord injury after surgery Neurocrit Care 201216267ndash72
15 Wauer RR Schmalisch G Bohme B et al Randomizeddouble blind trial of Ambroxol for the treatment of respira-tory distress syndrome Eur J Pediatr 1992151357ndash63
16 Refai M Brunelli A Xiume F et al Short-term periopera-tive treatment with ambroxol reduces pulmonarycomplications and hospital costs after pulmonary lobec-tomy a randomized trial Eur J Cardiothorac Surg 200935469ndash73
17 Xia DH Xi L Xv C et al The protective effects ofambroxol on radiation lung injury and influence on pro-duction of transforming growth factor beta(1) and tumornecrosis factor alpha Med Oncol 201027697ndash701
18 Ulas MM Hizarci M Kunt A et al Protective effect ofambroxol on pulmonary function after cardiopulmonarybypass J Cardiovasc Pharmacol 200852518ndash23
19 Wang Y Wang FY Pan Z et al Effects of ambroxolcombined with low-dose heparin on TNF-alpha andIL-1beta in rabbits with acute lung injury [Article inChinese] Zhongguo Ying Yong Sheng Li Xue Za Zhi201127231ndash5
20 Su X Wang L Song Y et al Inhibition of inflammatoryresponses by ambroxol a mucolytic agent in a murinemodel of acute lung injury induced by lipopolysaccharideIntensive Care Med 200430133ndash140
21 Ma YT Tian YP Shi HW et al Effects of high doseambroxol on lung injury induced by paraquat in ratsZhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi200725523ndash6
22 ARDS Definition Task Force Ranieri VM RubenfeldGD Thompson BT et al Acute respiratory distress syn-drome the Berlin Definition JAMA 20123072526ndash33
23 Schulz M Hammrlein A Hinkel U Safety and usage pat-tern of an over-the-counter ambroxol cough syrup a com-munity pharmacy based cohort study Int J ClinPharmacol Ther 200644409ndash21
24 Schmalisch G Wauer RR Bohme B Effect of earlyambroxol treatment on lung functions in mechanically ven-tilated preterm newborns who subsequently developed abronchopulmonary dysplasia Respir Med 200094378ndash84
25 Couet W Girault J Reigner BG Steady-state bioavailabil-ity and pharmacokinetics of ambroxol and clenbuterol ad-ministered alone and combined in a new oral formulationInt J Clin Pharmacol Ther Toxicol 198927467ndash72
26 Schulz KF Altman DG Moher D CONSORT GroupCONSORT 2010 Statement updated guidelines for re-porting parallel group randomised trials BMC Med 2010818
27 Leteurtre S Martinot A Duhamel A et al Validation ofthe paediatric logistic organ dysfunction (PeLOD) scoreprospective observational multicentre study Lancet2003362192ndash7
28 Ramsay MAE How to use the Ramsay Score to assess thelevel of ICU Sedation http5jsnaccuminacjpHow20to20use20the20Ramsay20Score20too20assess20the20level20of20ICU20Sedationhtm (1August 2014 date last accessed)
29 Rubenfeld GD Caldwell E Peabody E et al Incidenceand outcomes of acute lung injury N Engl J Med 20053531685ndash93
30 Demling RH Adult respiratory distress syndrome cur-rent concepts New Horiz 19931388ndash401
31 Schoenfeld DA Bernard GR Network ARDS Statisticalevaluation of ventilator-free days as an efficacy measure inclinical trials of treatments for acute respiratory distresssyndrome Crit Care Med 2002301772ndash7
32 Horowitz IN Tai K Hypoalbuminemia in critically ill chil-dren Arch Pediatr Adolesc Med 20071611048ndash1052
33 Wauer RR Schmalisch G Ambroxol for prevention andtreatment of Hyaline membrane disease Eur Resp J 1989257sndash65s
34 Chetan G Rathisharmila R Narayanan P et al Acute re-spiratory distress syndrome in pediatric intensive careunit Indian J Pediatr 2009761013ndash16
35 Dahlem P van Aalderen W Hamaker M et al Incidenceand short-term outcome of acute lung injury in mechanic-ally ventilated children Eur Respir J 200322980ndash5
36 Curley MAQ Hibberd PL Fineman LD et al Effect ofprone positioning on clinical outcomes in children with
High-dose Oral Ambroxol for pulmonary ARDS 349
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
acute lung injury a randomized controlled trial JAMA2005294229ndash37
37 Flori HR Glidden DV Rutherford GW et al Pediatricacute lung injury prospective evaluation of risk factorsassociated with mortality Am J Respir Crit Care Med2005171995ndash1001
38 Erickson S Schibler A Numa A et al Paediatric StudyGroup Australian and New Zealand Intensive Care Society(ANZICS) Acute lung injury in pediatric intensive care in
Australia and New Zealand a prospective multicentre ob-servational study Pediatr Crit Care Med 20078317ndash23
39 Capsoni F Ongari AM Minonzio F Effect of ambroxolon human phagocytic cell function Boll Ist Sieroter Milan198564236ndash9
40 Sample Size Calculator Two Parallel Sample MeansHypothesis One-Sided Non-InferioritySuperiorityhttpwwwcctcuhkeduhkstatmeantsmp_suphtm(24 March 2015 date last accessed)
350 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
- fmv033-TF1
- fmv033-TF2
- fmv033-TF3
- fmv033-TF4
- fmv033-TF6
- fmv033-TF7
- fmv033-TF8
- fmv033-TF9
- fmv033-TF10
- fmv033-TF11
- fmv033-TF12
- fmv033-TF13
- fmv033-TF15
-
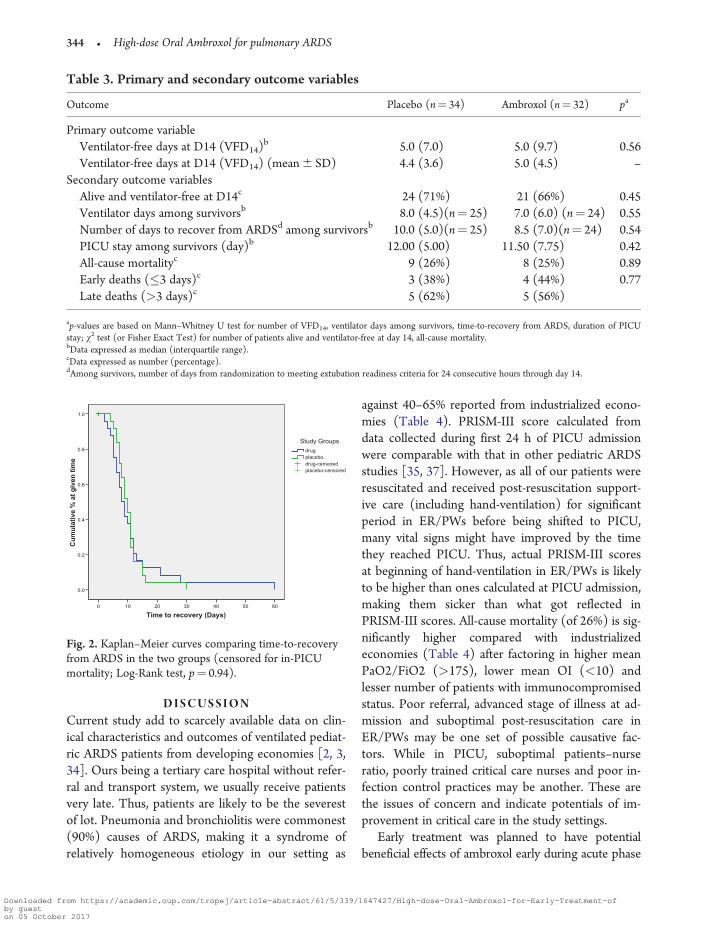
D I S C U S S I O NCurrent study add to scarcely available data on clin-ical characteristics and outcomes of ventilated pediat-ric ARDS patients from developing economies [2 334] Ours being a tertiary care hospital without refer-ral and transport system we usually receive patientsvery late Thus patients are likely to be the severestof lot Pneumonia and bronchiolitis were commonest(90) causes of ARDS making it a syndrome ofrelatively homogeneous etiology in our setting as
against 40ndash65 reported from industrialized econo-mies (Table 4) PRISM-III score calculated fromdata collected during first 24 h of PICU admissionwere comparable with that in other pediatric ARDSstudies [35 37] However as all of our patients wereresuscitated and received post-resuscitation support-ive care (including hand-ventilation) for significantperiod in ERPWs before being shifted to PICUmany vital signs might have improved by the timethey reached PICU Thus actual PRISM-III scoresat beginning of hand-ventilation in ERPWs is likelyto be higher than ones calculated at PICU admissionmaking them sicker than what got reflected inPRISM-III scores All-cause mortality (of 26) is sig-nificantly higher compared with industrializedeconomies (Table 4) after factoring in higher meanPaO2FiO2 (gt175) lower mean OI (lt10) andlesser number of patients with immunocompromisedstatus Poor referral advanced stage of illness at ad-mission and suboptimal post-resuscitation care inERPWs may be one set of possible causative fac-tors While in PICU suboptimal patientsndashnurseratio poorly trained critical care nurses and poor in-fection control practices may be another These arethe issues of concern and indicate potentials of im-provement in critical care in the study settings
Early treatment was planned to have potentialbeneficial effects of ambroxol early during acute phase
Table 3 Primary and secondary outcome variables
Outcome Placebo (nfrac14 34) Ambroxol (nfrac14 32) pa
Primary outcome variableVentilator-free days at D14 (VFD14)b 50 (70) 50 (97) 056Ventilator-free days at D14 (VFD14) (mean 6 SD) 44 (36) 50 (45) ndash
Secondary outcome variablesAlive and ventilator-free at D14c 24 (71) 21 (66) 045Ventilator days among survivorsb 80 (45)(nfrac14 25) 70 (60) (nfrac14 24) 055Number of days to recover from ARDSd among survivorsb 100 (50)(nfrac14 25) 85 (70)(nfrac14 24) 054PICU stay among survivors (day)b 1200 (500) 1150 (775) 042All-cause mortalityc 9 (26) 8 (25) 089Early deaths (3 days)c 3 (38) 4 (44) 077Late deaths (gt3 days)c 5 (62) 5 (56)
ap-values are based on MannndashWhitney U test for number of VFD14 ventilator days among survivors time-to-recovery from ARDS duration of PICUstay v2 test (or Fisher Exact Test) for number of patients alive and ventilator-free at day 14 all-cause mortalitybData expressed as median (interquartile range)cData expressed as number (percentage)dAmong survivors number of days from randomization to meeting extubation readiness criteria for 24 consecutive hours through day 14
Time to recovery (Days)6050403020100
Cum
ulat
ive
a
t giv
en ti
me
10
08
06
04
02
00
placebo-censoreddrug-censoredplacebodrug
Study Groups
Fig 2 KaplanndashMeier curves comparing time-to-recoveryfrom ARDS in the two groups (censored for in-PICUmortality Log-Rank test pfrac14 094)
344 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
(a)
(b)
(c)
0
10
20
30
40
50
60
70
0 2 4 6 8 10 12 14 16
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
OI
0
100
200
300
400
500
600
700
0 5 10 15
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
PF
0
2
4
6
8
10
12
14
16
18
0 5 10 15
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
PEEP
Fig 3 Dot plot showing trend of mean PaO2FiO2 ratio oxygenation Index and PEEP during first 14 days
High-dose Oral Ambroxol for pulmonary ARDS 345
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
of illness We demonstrated safety tolerance and roleof high-dose oral ambroxol (40 mgkgday in fourdivided doses) in ventilated pARDS patients for thefirst time Ambroxol failed to improve oxygenationventilation VFD time-to-recovery mortality and thusto suggest therapeutic potential in pARDS in thestudy setting owing to small sample size Two-thirdsof patients had hypoalbuminemia and thus gut edema
possibly affecting ambroxolrsquos bioavailability Dosagechosen was maximal safe dose based on availableclinical data Therapeutic efficacy and safety of fur-ther higher dose may be subject of future scrutinyHigher doses may also be helpful in eradicating patho-gens adhered to bronchiolaralveolar epithelium [39]Ambroxol selectively gets concentrated in lungswithin 3 min of intravenous administration but it falls
(a)
(a)
0
50
100
150
200
250
0 2 4 6 8 10 12 14 16
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
PaCO
2
0
2
4
6
8
10
12
14
0 2 4 6 8 10 12 14 16
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
TV
FIG 4 Dot plot showing trend of mean tidal volume and PaCO2 during first 14 days
346 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
Tab
le4
Com
pari
son
ofcl
inic
alch
arac
teri
stic
san
dou
tcom
eof
pedi
atri
cA
RD
Sin
vari
ous
stud
ies
Clin
ical
Pro
file
Dah
lem
etal
[35
]C
urle
yet
al[
36]
Flor
iet
al[
37]
Wils
onet
al[
9]A
NZ
ICS
[38]
Hu et
al[
3]Z
hu etal
[2]
Che
tan
etal
[34
]In
dex
stud
y
nfrac14
443
nfrac14
102
nfrac14
328
nfrac14
152
nfrac14
117
nfrac14
306
nfrac14
401
nfrac14
17nfrac14
66
Stud
ype
riod
1998
ndash200
020
01ndash2
004
1996
ndash200
020
00ndash2
003
2004
ndash200
520
06ndash2
007
2009
2003
ndash200
620
07ndash2
008
Cou
ntry
ofst
udy
Net
herl
ands
USA
USA
USA
Aus
tral
iaan
dN
ewZ
eala
ndC
hina
Chi
naIn
dia
Indi
a
Pne
umon
ia11
4
56
35
34
46
75
63
18
82
Bro
nchi
oliti
s15
9
14
ndash7
12
ndashndash
ndash9
Asp
irat
ion
ndash11
15
8
8ndash
ndash6
5Se
psis
341
15
13
36
17
15
34
30
3
Nea
rdr
owni
ngndash
ndash9
53
ndash2
6ndash
Car
diac
dise
ase
ndashndash
7ndash
ndashndash
9ndash
ndashP
aO2
FiO
2ra
tio21
15a
147
and
153a
b
128
and
126a
b
17
71
and
190
6ab
Oxy
gena
tion
Inde
xN
A15
0an
d18
0a
b
200
and
205
ab
95
and
76a
b
Imm
uno-
com
prom
ised
Stat
us9
1N
A
34
45
Oth
ers
91
421
11
9
ndash1
540
2
Mor
talit
y27
8
22
28
35
45
30
70
26
NAfrac14
Info
rmat
ion
not
avai
labl
efrac14
info
rmat
ion
coul
dno
tbe
retr
ieve
ddu
eto
non-
acce
ssib
ility
offu
llm
anus
crip
ts
a Mea
nbIn
the
two
arm
sof
the
stud
yco
hort
High-dose Oral Ambroxol for pulmonary ARDS 347
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
dramatically at 2 h [33] Thus for sustained clinicaleffect more frequent administration (4 hourly or even2 hourly) may be required As pARDS was mostlycaused by pneumonia and bronchiolitis and majority(92) of survivors required ventilation for 14 daysD14 may be an optimal reference for measure of VFDin the study setting This pilot trial is relied on a con-venience sample results (Table 3) from which indi-cates need of sample size of 388 patients in each armwith one-sided significance level (a error) of 005 and80 power to detect 20 improvement in theobserved median VFD14 of 5 days (ie reduction of1 day in VFD14) [40]
Strengths include randomized design and care-fully planned protocols to define ventilator manage-ment sedation and extubation readiness to minimizevariations in daily management of patients Thereare many limitations as well major one being the un-regulated unmonitored hand-ventilation beforePICU admission which may have caused baro-trauma Lack of specific information on its durationmay be a potential confounder Study cohort was re-stricted to pARDS only These issues are unavoid-able and need to be tolerated to develop clinicallyefficacious interventions in the prevalent settingsHowever these would affect generalizability of re-sults Study was underpowered to demonstrate dif-ference in VFD14 There is lack of data onpharmacokinetics of enterally administered ambroxolin critically ill children It needs to be addressed be-fore conducting similar study in future Further in-flammatory oxidative and anti-protease markersshould also be evaluated to assess its pharmacologicefficacy Stratification according to severity of ARDSmay identify a subgroup of responders
C O N C L U S I O N SStudy provides useful information on prevalent situ-ation in the resource-constraint economies informsabout limitations in conducting trials in these set-tings and questionable generalizability of their re-sults Pediatric pARDS is mostly caused bypneumonia and bronchiolitis After factoring inhigher PaO2FiO2 lower OI and lesser patientswith immunocompromised states mortality is highcompared with industrialized peers High-dose oralambroxol failed to improve VFD14 In the current
cost-conscious health care environment its potentialas adjuvant therapy should be explored after havingaddressed the aforementioned issues Large pro-spective study of appropriate power with higherdoses of oral ambroxol administered more frequentlyis desirable VFD14 as composite outcome measuresis suggested for ventilated pediatric pARDS patientshowever it needs further validation
A C K N O W L E D G E M E N T SThe drug (ambroxol hydrochloride) was provided by MsAristo Pharmaceuticals Pvt Ltd Mumbai (India) The tabletsof drug (ambroxol) and placebo (lactose) was prepared atUniversity Institute of Pharmaceutical Sciences PunjabUniversity Chandigarh (India)
Work done at Emergency and Critical Care DivisionAdvanced Pediatrics Center Postgraduate Institute ofMedical Education and Research Chandigarh-160012 India
Presented at the 20th ESPNIC Medical amp NursingAnnual Congress at Verona Italy June 15ndash17 2009rdquo
R E F E R E N C E S1 Ventre KM Arnold JH Acute lung injury and acute re-
spiratory didtress syndrome In Nichols DG (ed) RogerrsquosTextbook of Pediatric Intensive Care 4th ednPhiladelphia PA Lippincott Williams amp Wilkins 2008731ndash66
2 Zhu YF Xu F Lu XL et al Chinese Collaborative StudyGroup for Pediatric Hypoxemic Respiratory FailureMortality and morbidity of acute hypoxemic respiratoryfailure and acute respiratory distress syndrome in infantsand young children Chin Med J 20121252265ndash71
3 Hu X Qian S Xu F et al Chinese Collaborative StudyGroup for Pediatric Respiratory Failure Incidence man-agement and mortality of acute hypoxemic respiratory fail-ure and acute respiratory distress syndrome from aprospective study of Chinese paediatric intensive care net-work Acta Paediatr 201099715ndash21
4 Hanson JH Flori H Application of the acute respiratorydistress syndrome network low-tidal volume strategy topediatric acute lung injury Respir Care Clin N Am 200612349ndash57
5 De Luca D Piastra M Tosi F et al Pharmacological thera-pies for pediatric and neonatal ALIARDS an evidence-based review Curr Drug Targets 201213906ndash16
6 Brun-Buisson C Richard JC Mercat A et al REVA-SRLFAH1N1v 2009 Registry Group Early corticosteroids insevere influenza AH1N1 pneumonia and acute respiratorydistress syndrome Am J Respir Crit Care Med 20111831200ndash6
348 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
7 Singer P Shapiro H Enteral omega-3 in acute respiratorydistress syndrome Curr Opin Clin Nutr Metab Care200912123ndash8
8 Pacht ER DeMichele SJ Nelson JL et al Enteral nutri-tion with eicosapentaenoic acid gamma-linolenic acidand antioxidants reduces alveolar inflammatory mediatorsand protein influx in patients with acute respiratory dis-tress syndrome Crit Care Med 200331491ndash500
9 Wilson DF Thomas NJ Markowitz BP et al Effect ofexogenous surfactant (calfactant) in pediatric acutelung injury a randomized controlled trial JAMA 2005293470ndash6
10 Matthay MA Abraham E Beta-adrenergic agonist therapyas a potential treatment for acute lung injury Am J RespirCrit Care Med 2006173254ndash5
11 Perkins GD McAuley DF Thickett DR et al The szlig-Agonist Lung Injury Trial (BALTI) a randomizedplacebo-controlled clinical trial Am J Respir Crit CareMed 2006173281ndash7
12 Wunderer H Morgenroth K Weis G The cleaningsystem of the airways physiology pathophysiologyand effects of ambroxol Med Monatsschr Pharm20093242ndash7
13 Malerba M Ragnoli B Ambroxol in the 21st centurypharmacological and clinical update Expert Opin DrugMetab Toxicol 200841119ndash29
14 Li Q Yao G Zhu X High-dose ambroxol reduces pul-monary complications in patients with acute cervical spi-nal cord injury after surgery Neurocrit Care 201216267ndash72
15 Wauer RR Schmalisch G Bohme B et al Randomizeddouble blind trial of Ambroxol for the treatment of respira-tory distress syndrome Eur J Pediatr 1992151357ndash63
16 Refai M Brunelli A Xiume F et al Short-term periopera-tive treatment with ambroxol reduces pulmonarycomplications and hospital costs after pulmonary lobec-tomy a randomized trial Eur J Cardiothorac Surg 200935469ndash73
17 Xia DH Xi L Xv C et al The protective effects ofambroxol on radiation lung injury and influence on pro-duction of transforming growth factor beta(1) and tumornecrosis factor alpha Med Oncol 201027697ndash701
18 Ulas MM Hizarci M Kunt A et al Protective effect ofambroxol on pulmonary function after cardiopulmonarybypass J Cardiovasc Pharmacol 200852518ndash23
19 Wang Y Wang FY Pan Z et al Effects of ambroxolcombined with low-dose heparin on TNF-alpha andIL-1beta in rabbits with acute lung injury [Article inChinese] Zhongguo Ying Yong Sheng Li Xue Za Zhi201127231ndash5
20 Su X Wang L Song Y et al Inhibition of inflammatoryresponses by ambroxol a mucolytic agent in a murinemodel of acute lung injury induced by lipopolysaccharideIntensive Care Med 200430133ndash140
21 Ma YT Tian YP Shi HW et al Effects of high doseambroxol on lung injury induced by paraquat in ratsZhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi200725523ndash6
22 ARDS Definition Task Force Ranieri VM RubenfeldGD Thompson BT et al Acute respiratory distress syn-drome the Berlin Definition JAMA 20123072526ndash33
23 Schulz M Hammrlein A Hinkel U Safety and usage pat-tern of an over-the-counter ambroxol cough syrup a com-munity pharmacy based cohort study Int J ClinPharmacol Ther 200644409ndash21
24 Schmalisch G Wauer RR Bohme B Effect of earlyambroxol treatment on lung functions in mechanically ven-tilated preterm newborns who subsequently developed abronchopulmonary dysplasia Respir Med 200094378ndash84
25 Couet W Girault J Reigner BG Steady-state bioavailabil-ity and pharmacokinetics of ambroxol and clenbuterol ad-ministered alone and combined in a new oral formulationInt J Clin Pharmacol Ther Toxicol 198927467ndash72
26 Schulz KF Altman DG Moher D CONSORT GroupCONSORT 2010 Statement updated guidelines for re-porting parallel group randomised trials BMC Med 2010818
27 Leteurtre S Martinot A Duhamel A et al Validation ofthe paediatric logistic organ dysfunction (PeLOD) scoreprospective observational multicentre study Lancet2003362192ndash7
28 Ramsay MAE How to use the Ramsay Score to assess thelevel of ICU Sedation http5jsnaccuminacjpHow20to20use20the20Ramsay20Score20too20assess20the20level20of20ICU20Sedationhtm (1August 2014 date last accessed)
29 Rubenfeld GD Caldwell E Peabody E et al Incidenceand outcomes of acute lung injury N Engl J Med 20053531685ndash93
30 Demling RH Adult respiratory distress syndrome cur-rent concepts New Horiz 19931388ndash401
31 Schoenfeld DA Bernard GR Network ARDS Statisticalevaluation of ventilator-free days as an efficacy measure inclinical trials of treatments for acute respiratory distresssyndrome Crit Care Med 2002301772ndash7
32 Horowitz IN Tai K Hypoalbuminemia in critically ill chil-dren Arch Pediatr Adolesc Med 20071611048ndash1052
33 Wauer RR Schmalisch G Ambroxol for prevention andtreatment of Hyaline membrane disease Eur Resp J 1989257sndash65s
34 Chetan G Rathisharmila R Narayanan P et al Acute re-spiratory distress syndrome in pediatric intensive careunit Indian J Pediatr 2009761013ndash16
35 Dahlem P van Aalderen W Hamaker M et al Incidenceand short-term outcome of acute lung injury in mechanic-ally ventilated children Eur Respir J 200322980ndash5
36 Curley MAQ Hibberd PL Fineman LD et al Effect ofprone positioning on clinical outcomes in children with
High-dose Oral Ambroxol for pulmonary ARDS 349
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
acute lung injury a randomized controlled trial JAMA2005294229ndash37
37 Flori HR Glidden DV Rutherford GW et al Pediatricacute lung injury prospective evaluation of risk factorsassociated with mortality Am J Respir Crit Care Med2005171995ndash1001
38 Erickson S Schibler A Numa A et al Paediatric StudyGroup Australian and New Zealand Intensive Care Society(ANZICS) Acute lung injury in pediatric intensive care in
Australia and New Zealand a prospective multicentre ob-servational study Pediatr Crit Care Med 20078317ndash23
39 Capsoni F Ongari AM Minonzio F Effect of ambroxolon human phagocytic cell function Boll Ist Sieroter Milan198564236ndash9
40 Sample Size Calculator Two Parallel Sample MeansHypothesis One-Sided Non-InferioritySuperiorityhttpwwwcctcuhkeduhkstatmeantsmp_suphtm(24 March 2015 date last accessed)
350 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
- fmv033-TF1
- fmv033-TF2
- fmv033-TF3
- fmv033-TF4
- fmv033-TF6
- fmv033-TF7
- fmv033-TF8
- fmv033-TF9
- fmv033-TF10
- fmv033-TF11
- fmv033-TF12
- fmv033-TF13
- fmv033-TF15
-
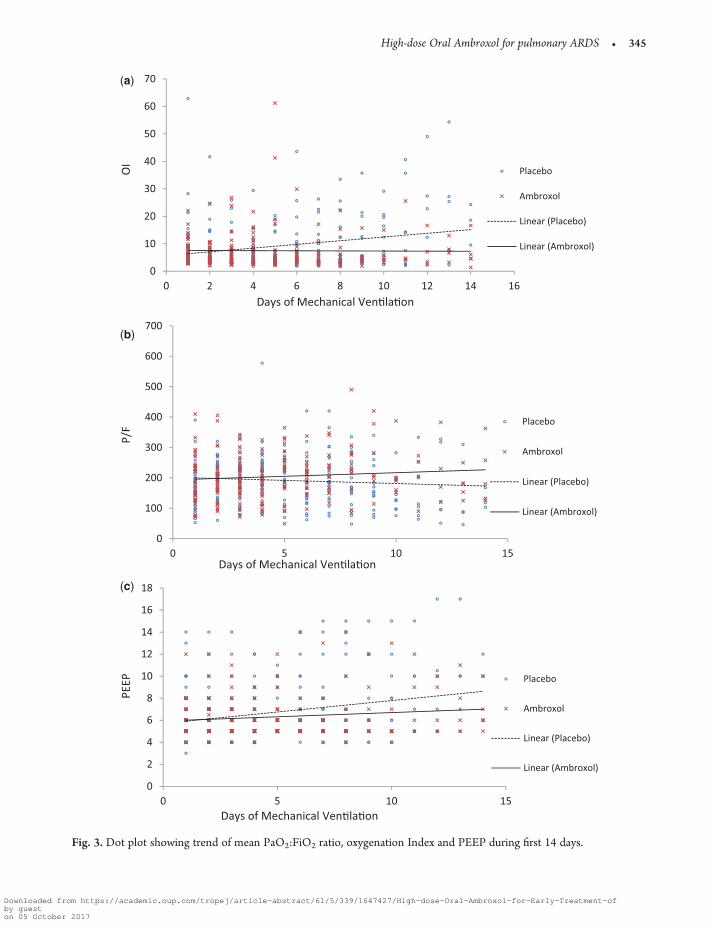
(a)
(b)
(c)
0
10
20
30
40
50
60
70
0 2 4 6 8 10 12 14 16
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
OI
0
100
200
300
400
500
600
700
0 5 10 15
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
PF
0
2
4
6
8
10
12
14
16
18
0 5 10 15
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
PEEP
Fig 3 Dot plot showing trend of mean PaO2FiO2 ratio oxygenation Index and PEEP during first 14 days
High-dose Oral Ambroxol for pulmonary ARDS 345
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
of illness We demonstrated safety tolerance and roleof high-dose oral ambroxol (40 mgkgday in fourdivided doses) in ventilated pARDS patients for thefirst time Ambroxol failed to improve oxygenationventilation VFD time-to-recovery mortality and thusto suggest therapeutic potential in pARDS in thestudy setting owing to small sample size Two-thirdsof patients had hypoalbuminemia and thus gut edema
possibly affecting ambroxolrsquos bioavailability Dosagechosen was maximal safe dose based on availableclinical data Therapeutic efficacy and safety of fur-ther higher dose may be subject of future scrutinyHigher doses may also be helpful in eradicating patho-gens adhered to bronchiolaralveolar epithelium [39]Ambroxol selectively gets concentrated in lungswithin 3 min of intravenous administration but it falls
(a)
(a)
0
50
100
150
200
250
0 2 4 6 8 10 12 14 16
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
PaCO
2
0
2
4
6
8
10
12
14
0 2 4 6 8 10 12 14 16
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
TV
FIG 4 Dot plot showing trend of mean tidal volume and PaCO2 during first 14 days
346 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
Tab
le4
Com
pari
son
ofcl
inic
alch
arac
teri
stic
san
dou
tcom
eof
pedi
atri
cA
RD
Sin
vari
ous
stud
ies
Clin
ical
Pro
file
Dah
lem
etal
[35
]C
urle
yet
al[
36]
Flor
iet
al[
37]
Wils
onet
al[
9]A
NZ
ICS
[38]
Hu et
al[
3]Z
hu etal
[2]
Che
tan
etal
[34
]In
dex
stud
y
nfrac14
443
nfrac14
102
nfrac14
328
nfrac14
152
nfrac14
117
nfrac14
306
nfrac14
401
nfrac14
17nfrac14
66
Stud
ype
riod
1998
ndash200
020
01ndash2
004
1996
ndash200
020
00ndash2
003
2004
ndash200
520
06ndash2
007
2009
2003
ndash200
620
07ndash2
008
Cou
ntry
ofst
udy
Net
herl
ands
USA
USA
USA
Aus
tral
iaan
dN
ewZ
eala
ndC
hina
Chi
naIn
dia
Indi
a
Pne
umon
ia11
4
56
35
34
46
75
63
18
82
Bro
nchi
oliti
s15
9
14
ndash7
12
ndashndash
ndash9
Asp
irat
ion
ndash11
15
8
8ndash
ndash6
5Se
psis
341
15
13
36
17
15
34
30
3
Nea
rdr
owni
ngndash
ndash9
53
ndash2
6ndash
Car
diac
dise
ase
ndashndash
7ndash
ndashndash
9ndash
ndashP
aO2
FiO
2ra
tio21
15a
147
and
153a
b
128
and
126a
b
17
71
and
190
6ab
Oxy
gena
tion
Inde
xN
A15
0an
d18
0a
b
200
and
205
ab
95
and
76a
b
Imm
uno-
com
prom
ised
Stat
us9
1N
A
34
45
Oth
ers
91
421
11
9
ndash1
540
2
Mor
talit
y27
8
22
28
35
45
30
70
26
NAfrac14
Info
rmat
ion
not
avai
labl
efrac14
info
rmat
ion
coul
dno
tbe
retr
ieve
ddu
eto
non-
acce
ssib
ility
offu
llm
anus
crip
ts
a Mea
nbIn
the
two
arm
sof
the
stud
yco
hort
High-dose Oral Ambroxol for pulmonary ARDS 347
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
dramatically at 2 h [33] Thus for sustained clinicaleffect more frequent administration (4 hourly or even2 hourly) may be required As pARDS was mostlycaused by pneumonia and bronchiolitis and majority(92) of survivors required ventilation for 14 daysD14 may be an optimal reference for measure of VFDin the study setting This pilot trial is relied on a con-venience sample results (Table 3) from which indi-cates need of sample size of 388 patients in each armwith one-sided significance level (a error) of 005 and80 power to detect 20 improvement in theobserved median VFD14 of 5 days (ie reduction of1 day in VFD14) [40]
Strengths include randomized design and care-fully planned protocols to define ventilator manage-ment sedation and extubation readiness to minimizevariations in daily management of patients Thereare many limitations as well major one being the un-regulated unmonitored hand-ventilation beforePICU admission which may have caused baro-trauma Lack of specific information on its durationmay be a potential confounder Study cohort was re-stricted to pARDS only These issues are unavoid-able and need to be tolerated to develop clinicallyefficacious interventions in the prevalent settingsHowever these would affect generalizability of re-sults Study was underpowered to demonstrate dif-ference in VFD14 There is lack of data onpharmacokinetics of enterally administered ambroxolin critically ill children It needs to be addressed be-fore conducting similar study in future Further in-flammatory oxidative and anti-protease markersshould also be evaluated to assess its pharmacologicefficacy Stratification according to severity of ARDSmay identify a subgroup of responders
C O N C L U S I O N SStudy provides useful information on prevalent situ-ation in the resource-constraint economies informsabout limitations in conducting trials in these set-tings and questionable generalizability of their re-sults Pediatric pARDS is mostly caused bypneumonia and bronchiolitis After factoring inhigher PaO2FiO2 lower OI and lesser patientswith immunocompromised states mortality is highcompared with industrialized peers High-dose oralambroxol failed to improve VFD14 In the current
cost-conscious health care environment its potentialas adjuvant therapy should be explored after havingaddressed the aforementioned issues Large pro-spective study of appropriate power with higherdoses of oral ambroxol administered more frequentlyis desirable VFD14 as composite outcome measuresis suggested for ventilated pediatric pARDS patientshowever it needs further validation
A C K N O W L E D G E M E N T SThe drug (ambroxol hydrochloride) was provided by MsAristo Pharmaceuticals Pvt Ltd Mumbai (India) The tabletsof drug (ambroxol) and placebo (lactose) was prepared atUniversity Institute of Pharmaceutical Sciences PunjabUniversity Chandigarh (India)
Work done at Emergency and Critical Care DivisionAdvanced Pediatrics Center Postgraduate Institute ofMedical Education and Research Chandigarh-160012 India
Presented at the 20th ESPNIC Medical amp NursingAnnual Congress at Verona Italy June 15ndash17 2009rdquo
R E F E R E N C E S1 Ventre KM Arnold JH Acute lung injury and acute re-
spiratory didtress syndrome In Nichols DG (ed) RogerrsquosTextbook of Pediatric Intensive Care 4th ednPhiladelphia PA Lippincott Williams amp Wilkins 2008731ndash66
2 Zhu YF Xu F Lu XL et al Chinese Collaborative StudyGroup for Pediatric Hypoxemic Respiratory FailureMortality and morbidity of acute hypoxemic respiratoryfailure and acute respiratory distress syndrome in infantsand young children Chin Med J 20121252265ndash71
3 Hu X Qian S Xu F et al Chinese Collaborative StudyGroup for Pediatric Respiratory Failure Incidence man-agement and mortality of acute hypoxemic respiratory fail-ure and acute respiratory distress syndrome from aprospective study of Chinese paediatric intensive care net-work Acta Paediatr 201099715ndash21
4 Hanson JH Flori H Application of the acute respiratorydistress syndrome network low-tidal volume strategy topediatric acute lung injury Respir Care Clin N Am 200612349ndash57
5 De Luca D Piastra M Tosi F et al Pharmacological thera-pies for pediatric and neonatal ALIARDS an evidence-based review Curr Drug Targets 201213906ndash16
6 Brun-Buisson C Richard JC Mercat A et al REVA-SRLFAH1N1v 2009 Registry Group Early corticosteroids insevere influenza AH1N1 pneumonia and acute respiratorydistress syndrome Am J Respir Crit Care Med 20111831200ndash6
348 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
7 Singer P Shapiro H Enteral omega-3 in acute respiratorydistress syndrome Curr Opin Clin Nutr Metab Care200912123ndash8
8 Pacht ER DeMichele SJ Nelson JL et al Enteral nutri-tion with eicosapentaenoic acid gamma-linolenic acidand antioxidants reduces alveolar inflammatory mediatorsand protein influx in patients with acute respiratory dis-tress syndrome Crit Care Med 200331491ndash500
9 Wilson DF Thomas NJ Markowitz BP et al Effect ofexogenous surfactant (calfactant) in pediatric acutelung injury a randomized controlled trial JAMA 2005293470ndash6
10 Matthay MA Abraham E Beta-adrenergic agonist therapyas a potential treatment for acute lung injury Am J RespirCrit Care Med 2006173254ndash5
11 Perkins GD McAuley DF Thickett DR et al The szlig-Agonist Lung Injury Trial (BALTI) a randomizedplacebo-controlled clinical trial Am J Respir Crit CareMed 2006173281ndash7
12 Wunderer H Morgenroth K Weis G The cleaningsystem of the airways physiology pathophysiologyand effects of ambroxol Med Monatsschr Pharm20093242ndash7
13 Malerba M Ragnoli B Ambroxol in the 21st centurypharmacological and clinical update Expert Opin DrugMetab Toxicol 200841119ndash29
14 Li Q Yao G Zhu X High-dose ambroxol reduces pul-monary complications in patients with acute cervical spi-nal cord injury after surgery Neurocrit Care 201216267ndash72
15 Wauer RR Schmalisch G Bohme B et al Randomizeddouble blind trial of Ambroxol for the treatment of respira-tory distress syndrome Eur J Pediatr 1992151357ndash63
16 Refai M Brunelli A Xiume F et al Short-term periopera-tive treatment with ambroxol reduces pulmonarycomplications and hospital costs after pulmonary lobec-tomy a randomized trial Eur J Cardiothorac Surg 200935469ndash73
17 Xia DH Xi L Xv C et al The protective effects ofambroxol on radiation lung injury and influence on pro-duction of transforming growth factor beta(1) and tumornecrosis factor alpha Med Oncol 201027697ndash701
18 Ulas MM Hizarci M Kunt A et al Protective effect ofambroxol on pulmonary function after cardiopulmonarybypass J Cardiovasc Pharmacol 200852518ndash23
19 Wang Y Wang FY Pan Z et al Effects of ambroxolcombined with low-dose heparin on TNF-alpha andIL-1beta in rabbits with acute lung injury [Article inChinese] Zhongguo Ying Yong Sheng Li Xue Za Zhi201127231ndash5
20 Su X Wang L Song Y et al Inhibition of inflammatoryresponses by ambroxol a mucolytic agent in a murinemodel of acute lung injury induced by lipopolysaccharideIntensive Care Med 200430133ndash140
21 Ma YT Tian YP Shi HW et al Effects of high doseambroxol on lung injury induced by paraquat in ratsZhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi200725523ndash6
22 ARDS Definition Task Force Ranieri VM RubenfeldGD Thompson BT et al Acute respiratory distress syn-drome the Berlin Definition JAMA 20123072526ndash33
23 Schulz M Hammrlein A Hinkel U Safety and usage pat-tern of an over-the-counter ambroxol cough syrup a com-munity pharmacy based cohort study Int J ClinPharmacol Ther 200644409ndash21
24 Schmalisch G Wauer RR Bohme B Effect of earlyambroxol treatment on lung functions in mechanically ven-tilated preterm newborns who subsequently developed abronchopulmonary dysplasia Respir Med 200094378ndash84
25 Couet W Girault J Reigner BG Steady-state bioavailabil-ity and pharmacokinetics of ambroxol and clenbuterol ad-ministered alone and combined in a new oral formulationInt J Clin Pharmacol Ther Toxicol 198927467ndash72
26 Schulz KF Altman DG Moher D CONSORT GroupCONSORT 2010 Statement updated guidelines for re-porting parallel group randomised trials BMC Med 2010818
27 Leteurtre S Martinot A Duhamel A et al Validation ofthe paediatric logistic organ dysfunction (PeLOD) scoreprospective observational multicentre study Lancet2003362192ndash7
28 Ramsay MAE How to use the Ramsay Score to assess thelevel of ICU Sedation http5jsnaccuminacjpHow20to20use20the20Ramsay20Score20too20assess20the20level20of20ICU20Sedationhtm (1August 2014 date last accessed)
29 Rubenfeld GD Caldwell E Peabody E et al Incidenceand outcomes of acute lung injury N Engl J Med 20053531685ndash93
30 Demling RH Adult respiratory distress syndrome cur-rent concepts New Horiz 19931388ndash401
31 Schoenfeld DA Bernard GR Network ARDS Statisticalevaluation of ventilator-free days as an efficacy measure inclinical trials of treatments for acute respiratory distresssyndrome Crit Care Med 2002301772ndash7
32 Horowitz IN Tai K Hypoalbuminemia in critically ill chil-dren Arch Pediatr Adolesc Med 20071611048ndash1052
33 Wauer RR Schmalisch G Ambroxol for prevention andtreatment of Hyaline membrane disease Eur Resp J 1989257sndash65s
34 Chetan G Rathisharmila R Narayanan P et al Acute re-spiratory distress syndrome in pediatric intensive careunit Indian J Pediatr 2009761013ndash16
35 Dahlem P van Aalderen W Hamaker M et al Incidenceand short-term outcome of acute lung injury in mechanic-ally ventilated children Eur Respir J 200322980ndash5
36 Curley MAQ Hibberd PL Fineman LD et al Effect ofprone positioning on clinical outcomes in children with
High-dose Oral Ambroxol for pulmonary ARDS 349
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
acute lung injury a randomized controlled trial JAMA2005294229ndash37
37 Flori HR Glidden DV Rutherford GW et al Pediatricacute lung injury prospective evaluation of risk factorsassociated with mortality Am J Respir Crit Care Med2005171995ndash1001
38 Erickson S Schibler A Numa A et al Paediatric StudyGroup Australian and New Zealand Intensive Care Society(ANZICS) Acute lung injury in pediatric intensive care in
Australia and New Zealand a prospective multicentre ob-servational study Pediatr Crit Care Med 20078317ndash23
39 Capsoni F Ongari AM Minonzio F Effect of ambroxolon human phagocytic cell function Boll Ist Sieroter Milan198564236ndash9
40 Sample Size Calculator Two Parallel Sample MeansHypothesis One-Sided Non-InferioritySuperiorityhttpwwwcctcuhkeduhkstatmeantsmp_suphtm(24 March 2015 date last accessed)
350 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
- fmv033-TF1
- fmv033-TF2
- fmv033-TF3
- fmv033-TF4
- fmv033-TF6
- fmv033-TF7
- fmv033-TF8
- fmv033-TF9
- fmv033-TF10
- fmv033-TF11
- fmv033-TF12
- fmv033-TF13
- fmv033-TF15
-
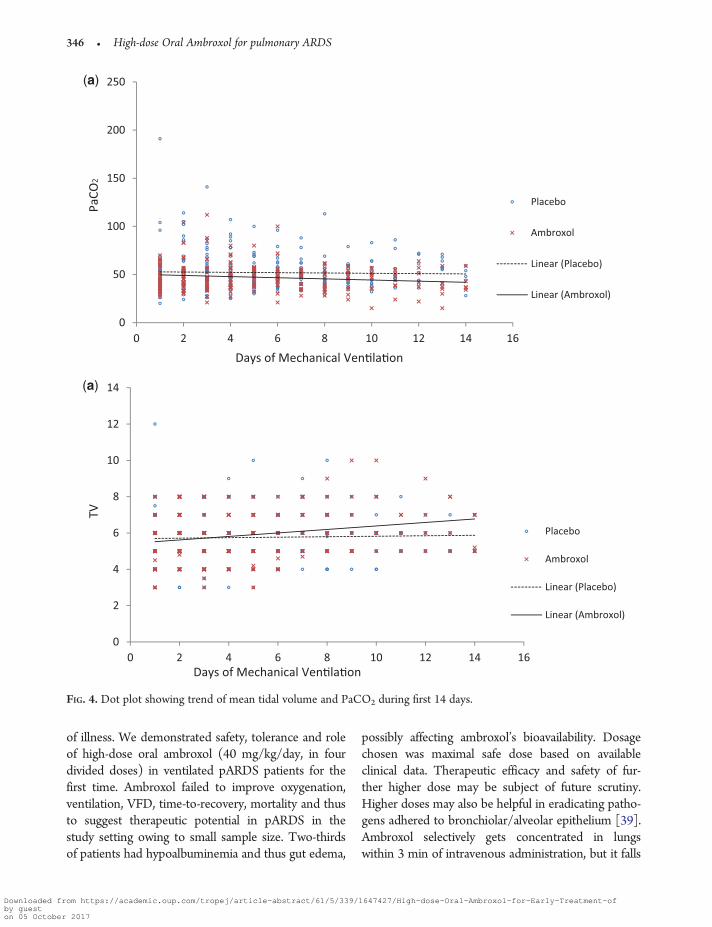
of illness We demonstrated safety tolerance and roleof high-dose oral ambroxol (40 mgkgday in fourdivided doses) in ventilated pARDS patients for thefirst time Ambroxol failed to improve oxygenationventilation VFD time-to-recovery mortality and thusto suggest therapeutic potential in pARDS in thestudy setting owing to small sample size Two-thirdsof patients had hypoalbuminemia and thus gut edema
possibly affecting ambroxolrsquos bioavailability Dosagechosen was maximal safe dose based on availableclinical data Therapeutic efficacy and safety of fur-ther higher dose may be subject of future scrutinyHigher doses may also be helpful in eradicating patho-gens adhered to bronchiolaralveolar epithelium [39]Ambroxol selectively gets concentrated in lungswithin 3 min of intravenous administration but it falls
(a)
(a)
0
50
100
150
200
250
0 2 4 6 8 10 12 14 16
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
PaCO
2
0
2
4
6
8
10
12
14
0 2 4 6 8 10 12 14 16
Placebo
Ambroxol
Linear (Placebo)
Linear (Ambroxol)
Days of Mechanical Venlaon
TV
FIG 4 Dot plot showing trend of mean tidal volume and PaCO2 during first 14 days
346 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
Tab
le4
Com
pari
son
ofcl
inic
alch
arac
teri
stic
san
dou
tcom
eof
pedi
atri
cA
RD
Sin
vari
ous
stud
ies
Clin
ical
Pro
file
Dah
lem
etal
[35
]C
urle
yet
al[
36]
Flor
iet
al[
37]
Wils
onet
al[
9]A
NZ
ICS
[38]
Hu et
al[
3]Z
hu etal
[2]
Che
tan
etal
[34
]In
dex
stud
y
nfrac14
443
nfrac14
102
nfrac14
328
nfrac14
152
nfrac14
117
nfrac14
306
nfrac14
401
nfrac14
17nfrac14
66
Stud
ype
riod
1998
ndash200
020
01ndash2
004
1996
ndash200
020
00ndash2
003
2004
ndash200
520
06ndash2
007
2009
2003
ndash200
620
07ndash2
008
Cou
ntry
ofst
udy
Net
herl
ands
USA
USA
USA
Aus
tral
iaan
dN
ewZ
eala
ndC
hina
Chi
naIn
dia
Indi
a
Pne
umon
ia11
4
56
35
34
46
75
63
18
82
Bro
nchi
oliti
s15
9
14
ndash7
12
ndashndash
ndash9
Asp
irat
ion
ndash11
15
8
8ndash
ndash6
5Se
psis
341
15
13
36
17
15
34
30
3
Nea
rdr
owni
ngndash
ndash9
53
ndash2
6ndash
Car
diac
dise
ase
ndashndash
7ndash
ndashndash
9ndash
ndashP
aO2
FiO
2ra
tio21
15a
147
and
153a
b
128
and
126a
b
17
71
and
190
6ab
Oxy
gena
tion
Inde
xN
A15
0an
d18
0a
b
200
and
205
ab
95
and
76a
b
Imm
uno-
com
prom
ised
Stat
us9
1N
A
34
45
Oth
ers
91
421
11
9
ndash1
540
2
Mor
talit
y27
8
22
28
35
45
30
70
26
NAfrac14
Info
rmat
ion
not
avai
labl
efrac14
info
rmat
ion
coul
dno
tbe
retr
ieve
ddu
eto
non-
acce
ssib
ility
offu
llm
anus
crip
ts
a Mea
nbIn
the
two
arm
sof
the
stud
yco
hort
High-dose Oral Ambroxol for pulmonary ARDS 347
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
dramatically at 2 h [33] Thus for sustained clinicaleffect more frequent administration (4 hourly or even2 hourly) may be required As pARDS was mostlycaused by pneumonia and bronchiolitis and majority(92) of survivors required ventilation for 14 daysD14 may be an optimal reference for measure of VFDin the study setting This pilot trial is relied on a con-venience sample results (Table 3) from which indi-cates need of sample size of 388 patients in each armwith one-sided significance level (a error) of 005 and80 power to detect 20 improvement in theobserved median VFD14 of 5 days (ie reduction of1 day in VFD14) [40]
Strengths include randomized design and care-fully planned protocols to define ventilator manage-ment sedation and extubation readiness to minimizevariations in daily management of patients Thereare many limitations as well major one being the un-regulated unmonitored hand-ventilation beforePICU admission which may have caused baro-trauma Lack of specific information on its durationmay be a potential confounder Study cohort was re-stricted to pARDS only These issues are unavoid-able and need to be tolerated to develop clinicallyefficacious interventions in the prevalent settingsHowever these would affect generalizability of re-sults Study was underpowered to demonstrate dif-ference in VFD14 There is lack of data onpharmacokinetics of enterally administered ambroxolin critically ill children It needs to be addressed be-fore conducting similar study in future Further in-flammatory oxidative and anti-protease markersshould also be evaluated to assess its pharmacologicefficacy Stratification according to severity of ARDSmay identify a subgroup of responders
C O N C L U S I O N SStudy provides useful information on prevalent situ-ation in the resource-constraint economies informsabout limitations in conducting trials in these set-tings and questionable generalizability of their re-sults Pediatric pARDS is mostly caused bypneumonia and bronchiolitis After factoring inhigher PaO2FiO2 lower OI and lesser patientswith immunocompromised states mortality is highcompared with industrialized peers High-dose oralambroxol failed to improve VFD14 In the current
cost-conscious health care environment its potentialas adjuvant therapy should be explored after havingaddressed the aforementioned issues Large pro-spective study of appropriate power with higherdoses of oral ambroxol administered more frequentlyis desirable VFD14 as composite outcome measuresis suggested for ventilated pediatric pARDS patientshowever it needs further validation
A C K N O W L E D G E M E N T SThe drug (ambroxol hydrochloride) was provided by MsAristo Pharmaceuticals Pvt Ltd Mumbai (India) The tabletsof drug (ambroxol) and placebo (lactose) was prepared atUniversity Institute of Pharmaceutical Sciences PunjabUniversity Chandigarh (India)
Work done at Emergency and Critical Care DivisionAdvanced Pediatrics Center Postgraduate Institute ofMedical Education and Research Chandigarh-160012 India
Presented at the 20th ESPNIC Medical amp NursingAnnual Congress at Verona Italy June 15ndash17 2009rdquo
R E F E R E N C E S1 Ventre KM Arnold JH Acute lung injury and acute re-
spiratory didtress syndrome In Nichols DG (ed) RogerrsquosTextbook of Pediatric Intensive Care 4th ednPhiladelphia PA Lippincott Williams amp Wilkins 2008731ndash66
2 Zhu YF Xu F Lu XL et al Chinese Collaborative StudyGroup for Pediatric Hypoxemic Respiratory FailureMortality and morbidity of acute hypoxemic respiratoryfailure and acute respiratory distress syndrome in infantsand young children Chin Med J 20121252265ndash71
3 Hu X Qian S Xu F et al Chinese Collaborative StudyGroup for Pediatric Respiratory Failure Incidence man-agement and mortality of acute hypoxemic respiratory fail-ure and acute respiratory distress syndrome from aprospective study of Chinese paediatric intensive care net-work Acta Paediatr 201099715ndash21
4 Hanson JH Flori H Application of the acute respiratorydistress syndrome network low-tidal volume strategy topediatric acute lung injury Respir Care Clin N Am 200612349ndash57
5 De Luca D Piastra M Tosi F et al Pharmacological thera-pies for pediatric and neonatal ALIARDS an evidence-based review Curr Drug Targets 201213906ndash16
6 Brun-Buisson C Richard JC Mercat A et al REVA-SRLFAH1N1v 2009 Registry Group Early corticosteroids insevere influenza AH1N1 pneumonia and acute respiratorydistress syndrome Am J Respir Crit Care Med 20111831200ndash6
348 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
7 Singer P Shapiro H Enteral omega-3 in acute respiratorydistress syndrome Curr Opin Clin Nutr Metab Care200912123ndash8
8 Pacht ER DeMichele SJ Nelson JL et al Enteral nutri-tion with eicosapentaenoic acid gamma-linolenic acidand antioxidants reduces alveolar inflammatory mediatorsand protein influx in patients with acute respiratory dis-tress syndrome Crit Care Med 200331491ndash500
9 Wilson DF Thomas NJ Markowitz BP et al Effect ofexogenous surfactant (calfactant) in pediatric acutelung injury a randomized controlled trial JAMA 2005293470ndash6
10 Matthay MA Abraham E Beta-adrenergic agonist therapyas a potential treatment for acute lung injury Am J RespirCrit Care Med 2006173254ndash5
11 Perkins GD McAuley DF Thickett DR et al The szlig-Agonist Lung Injury Trial (BALTI) a randomizedplacebo-controlled clinical trial Am J Respir Crit CareMed 2006173281ndash7
12 Wunderer H Morgenroth K Weis G The cleaningsystem of the airways physiology pathophysiologyand effects of ambroxol Med Monatsschr Pharm20093242ndash7
13 Malerba M Ragnoli B Ambroxol in the 21st centurypharmacological and clinical update Expert Opin DrugMetab Toxicol 200841119ndash29
14 Li Q Yao G Zhu X High-dose ambroxol reduces pul-monary complications in patients with acute cervical spi-nal cord injury after surgery Neurocrit Care 201216267ndash72
15 Wauer RR Schmalisch G Bohme B et al Randomizeddouble blind trial of Ambroxol for the treatment of respira-tory distress syndrome Eur J Pediatr 1992151357ndash63
16 Refai M Brunelli A Xiume F et al Short-term periopera-tive treatment with ambroxol reduces pulmonarycomplications and hospital costs after pulmonary lobec-tomy a randomized trial Eur J Cardiothorac Surg 200935469ndash73
17 Xia DH Xi L Xv C et al The protective effects ofambroxol on radiation lung injury and influence on pro-duction of transforming growth factor beta(1) and tumornecrosis factor alpha Med Oncol 201027697ndash701
18 Ulas MM Hizarci M Kunt A et al Protective effect ofambroxol on pulmonary function after cardiopulmonarybypass J Cardiovasc Pharmacol 200852518ndash23
19 Wang Y Wang FY Pan Z et al Effects of ambroxolcombined with low-dose heparin on TNF-alpha andIL-1beta in rabbits with acute lung injury [Article inChinese] Zhongguo Ying Yong Sheng Li Xue Za Zhi201127231ndash5
20 Su X Wang L Song Y et al Inhibition of inflammatoryresponses by ambroxol a mucolytic agent in a murinemodel of acute lung injury induced by lipopolysaccharideIntensive Care Med 200430133ndash140
21 Ma YT Tian YP Shi HW et al Effects of high doseambroxol on lung injury induced by paraquat in ratsZhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi200725523ndash6
22 ARDS Definition Task Force Ranieri VM RubenfeldGD Thompson BT et al Acute respiratory distress syn-drome the Berlin Definition JAMA 20123072526ndash33
23 Schulz M Hammrlein A Hinkel U Safety and usage pat-tern of an over-the-counter ambroxol cough syrup a com-munity pharmacy based cohort study Int J ClinPharmacol Ther 200644409ndash21
24 Schmalisch G Wauer RR Bohme B Effect of earlyambroxol treatment on lung functions in mechanically ven-tilated preterm newborns who subsequently developed abronchopulmonary dysplasia Respir Med 200094378ndash84
25 Couet W Girault J Reigner BG Steady-state bioavailabil-ity and pharmacokinetics of ambroxol and clenbuterol ad-ministered alone and combined in a new oral formulationInt J Clin Pharmacol Ther Toxicol 198927467ndash72
26 Schulz KF Altman DG Moher D CONSORT GroupCONSORT 2010 Statement updated guidelines for re-porting parallel group randomised trials BMC Med 2010818
27 Leteurtre S Martinot A Duhamel A et al Validation ofthe paediatric logistic organ dysfunction (PeLOD) scoreprospective observational multicentre study Lancet2003362192ndash7
28 Ramsay MAE How to use the Ramsay Score to assess thelevel of ICU Sedation http5jsnaccuminacjpHow20to20use20the20Ramsay20Score20too20assess20the20level20of20ICU20Sedationhtm (1August 2014 date last accessed)
29 Rubenfeld GD Caldwell E Peabody E et al Incidenceand outcomes of acute lung injury N Engl J Med 20053531685ndash93
30 Demling RH Adult respiratory distress syndrome cur-rent concepts New Horiz 19931388ndash401
31 Schoenfeld DA Bernard GR Network ARDS Statisticalevaluation of ventilator-free days as an efficacy measure inclinical trials of treatments for acute respiratory distresssyndrome Crit Care Med 2002301772ndash7
32 Horowitz IN Tai K Hypoalbuminemia in critically ill chil-dren Arch Pediatr Adolesc Med 20071611048ndash1052
33 Wauer RR Schmalisch G Ambroxol for prevention andtreatment of Hyaline membrane disease Eur Resp J 1989257sndash65s
34 Chetan G Rathisharmila R Narayanan P et al Acute re-spiratory distress syndrome in pediatric intensive careunit Indian J Pediatr 2009761013ndash16
35 Dahlem P van Aalderen W Hamaker M et al Incidenceand short-term outcome of acute lung injury in mechanic-ally ventilated children Eur Respir J 200322980ndash5
36 Curley MAQ Hibberd PL Fineman LD et al Effect ofprone positioning on clinical outcomes in children with
High-dose Oral Ambroxol for pulmonary ARDS 349
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
acute lung injury a randomized controlled trial JAMA2005294229ndash37
37 Flori HR Glidden DV Rutherford GW et al Pediatricacute lung injury prospective evaluation of risk factorsassociated with mortality Am J Respir Crit Care Med2005171995ndash1001
38 Erickson S Schibler A Numa A et al Paediatric StudyGroup Australian and New Zealand Intensive Care Society(ANZICS) Acute lung injury in pediatric intensive care in
Australia and New Zealand a prospective multicentre ob-servational study Pediatr Crit Care Med 20078317ndash23
39 Capsoni F Ongari AM Minonzio F Effect of ambroxolon human phagocytic cell function Boll Ist Sieroter Milan198564236ndash9
40 Sample Size Calculator Two Parallel Sample MeansHypothesis One-Sided Non-InferioritySuperiorityhttpwwwcctcuhkeduhkstatmeantsmp_suphtm(24 March 2015 date last accessed)
350 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
- fmv033-TF1
- fmv033-TF2
- fmv033-TF3
- fmv033-TF4
- fmv033-TF6
- fmv033-TF7
- fmv033-TF8
- fmv033-TF9
- fmv033-TF10
- fmv033-TF11
- fmv033-TF12
- fmv033-TF13
- fmv033-TF15
-
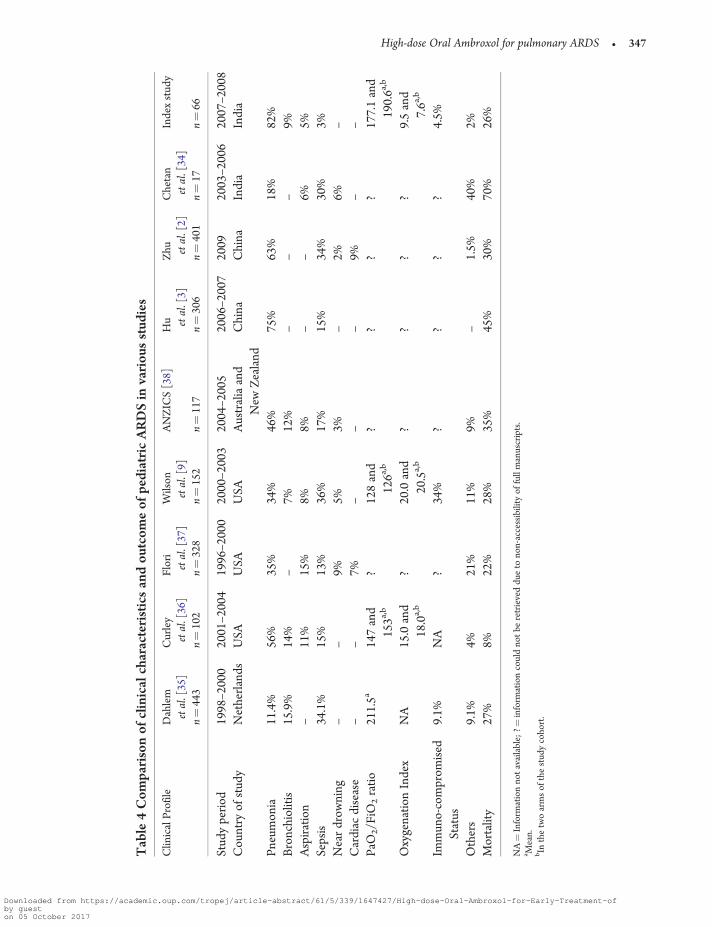
Tab
le4
Com
pari
son
ofcl
inic
alch
arac
teri
stic
san
dou
tcom
eof
pedi
atri
cA
RD
Sin
vari
ous
stud
ies
Clin
ical
Pro
file
Dah
lem
etal
[35
]C
urle
yet
al[
36]
Flor
iet
al[
37]
Wils
onet
al[
9]A
NZ
ICS
[38]
Hu et
al[
3]Z
hu etal
[2]
Che
tan
etal
[34
]In
dex
stud
y
nfrac14
443
nfrac14
102
nfrac14
328
nfrac14
152
nfrac14
117
nfrac14
306
nfrac14
401
nfrac14
17nfrac14
66
Stud
ype
riod
1998
ndash200
020
01ndash2
004
1996
ndash200
020
00ndash2
003
2004
ndash200
520
06ndash2
007
2009
2003
ndash200
620
07ndash2
008
Cou
ntry
ofst
udy
Net
herl
ands
USA
USA
USA
Aus
tral
iaan
dN
ewZ
eala
ndC
hina
Chi
naIn
dia
Indi
a
Pne
umon
ia11
4
56
35
34
46
75
63
18
82
Bro
nchi
oliti
s15
9
14
ndash7
12
ndashndash
ndash9
Asp
irat
ion
ndash11
15
8
8ndash
ndash6
5Se
psis
341
15
13
36
17
15
34
30
3
Nea
rdr
owni
ngndash
ndash9
53
ndash2
6ndash
Car
diac
dise
ase
ndashndash
7ndash
ndashndash
9ndash
ndashP
aO2
FiO
2ra
tio21
15a
147
and
153a
b
128
and
126a
b
17
71
and
190
6ab
Oxy
gena
tion
Inde
xN
A15
0an
d18
0a
b
200
and
205
ab
95
and
76a
b
Imm
uno-
com
prom
ised
Stat
us9
1N
A
34
45
Oth
ers
91
421
11
9
ndash1
540
2
Mor
talit
y27
8
22
28
35
45
30
70
26
NAfrac14
Info
rmat
ion
not
avai
labl
efrac14
info
rmat
ion
coul
dno
tbe
retr
ieve
ddu
eto
non-
acce
ssib
ility
offu
llm
anus
crip
ts
a Mea
nbIn
the
two
arm
sof
the
stud
yco
hort
High-dose Oral Ambroxol for pulmonary ARDS 347
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
dramatically at 2 h [33] Thus for sustained clinicaleffect more frequent administration (4 hourly or even2 hourly) may be required As pARDS was mostlycaused by pneumonia and bronchiolitis and majority(92) of survivors required ventilation for 14 daysD14 may be an optimal reference for measure of VFDin the study setting This pilot trial is relied on a con-venience sample results (Table 3) from which indi-cates need of sample size of 388 patients in each armwith one-sided significance level (a error) of 005 and80 power to detect 20 improvement in theobserved median VFD14 of 5 days (ie reduction of1 day in VFD14) [40]
Strengths include randomized design and care-fully planned protocols to define ventilator manage-ment sedation and extubation readiness to minimizevariations in daily management of patients Thereare many limitations as well major one being the un-regulated unmonitored hand-ventilation beforePICU admission which may have caused baro-trauma Lack of specific information on its durationmay be a potential confounder Study cohort was re-stricted to pARDS only These issues are unavoid-able and need to be tolerated to develop clinicallyefficacious interventions in the prevalent settingsHowever these would affect generalizability of re-sults Study was underpowered to demonstrate dif-ference in VFD14 There is lack of data onpharmacokinetics of enterally administered ambroxolin critically ill children It needs to be addressed be-fore conducting similar study in future Further in-flammatory oxidative and anti-protease markersshould also be evaluated to assess its pharmacologicefficacy Stratification according to severity of ARDSmay identify a subgroup of responders
C O N C L U S I O N SStudy provides useful information on prevalent situ-ation in the resource-constraint economies informsabout limitations in conducting trials in these set-tings and questionable generalizability of their re-sults Pediatric pARDS is mostly caused bypneumonia and bronchiolitis After factoring inhigher PaO2FiO2 lower OI and lesser patientswith immunocompromised states mortality is highcompared with industrialized peers High-dose oralambroxol failed to improve VFD14 In the current
cost-conscious health care environment its potentialas adjuvant therapy should be explored after havingaddressed the aforementioned issues Large pro-spective study of appropriate power with higherdoses of oral ambroxol administered more frequentlyis desirable VFD14 as composite outcome measuresis suggested for ventilated pediatric pARDS patientshowever it needs further validation
A C K N O W L E D G E M E N T SThe drug (ambroxol hydrochloride) was provided by MsAristo Pharmaceuticals Pvt Ltd Mumbai (India) The tabletsof drug (ambroxol) and placebo (lactose) was prepared atUniversity Institute of Pharmaceutical Sciences PunjabUniversity Chandigarh (India)
Work done at Emergency and Critical Care DivisionAdvanced Pediatrics Center Postgraduate Institute ofMedical Education and Research Chandigarh-160012 India
Presented at the 20th ESPNIC Medical amp NursingAnnual Congress at Verona Italy June 15ndash17 2009rdquo
R E F E R E N C E S1 Ventre KM Arnold JH Acute lung injury and acute re-
spiratory didtress syndrome In Nichols DG (ed) RogerrsquosTextbook of Pediatric Intensive Care 4th ednPhiladelphia PA Lippincott Williams amp Wilkins 2008731ndash66
2 Zhu YF Xu F Lu XL et al Chinese Collaborative StudyGroup for Pediatric Hypoxemic Respiratory FailureMortality and morbidity of acute hypoxemic respiratoryfailure and acute respiratory distress syndrome in infantsand young children Chin Med J 20121252265ndash71
3 Hu X Qian S Xu F et al Chinese Collaborative StudyGroup for Pediatric Respiratory Failure Incidence man-agement and mortality of acute hypoxemic respiratory fail-ure and acute respiratory distress syndrome from aprospective study of Chinese paediatric intensive care net-work Acta Paediatr 201099715ndash21
4 Hanson JH Flori H Application of the acute respiratorydistress syndrome network low-tidal volume strategy topediatric acute lung injury Respir Care Clin N Am 200612349ndash57
5 De Luca D Piastra M Tosi F et al Pharmacological thera-pies for pediatric and neonatal ALIARDS an evidence-based review Curr Drug Targets 201213906ndash16
6 Brun-Buisson C Richard JC Mercat A et al REVA-SRLFAH1N1v 2009 Registry Group Early corticosteroids insevere influenza AH1N1 pneumonia and acute respiratorydistress syndrome Am J Respir Crit Care Med 20111831200ndash6
348 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
7 Singer P Shapiro H Enteral omega-3 in acute respiratorydistress syndrome Curr Opin Clin Nutr Metab Care200912123ndash8
8 Pacht ER DeMichele SJ Nelson JL et al Enteral nutri-tion with eicosapentaenoic acid gamma-linolenic acidand antioxidants reduces alveolar inflammatory mediatorsand protein influx in patients with acute respiratory dis-tress syndrome Crit Care Med 200331491ndash500
9 Wilson DF Thomas NJ Markowitz BP et al Effect ofexogenous surfactant (calfactant) in pediatric acutelung injury a randomized controlled trial JAMA 2005293470ndash6
10 Matthay MA Abraham E Beta-adrenergic agonist therapyas a potential treatment for acute lung injury Am J RespirCrit Care Med 2006173254ndash5
11 Perkins GD McAuley DF Thickett DR et al The szlig-Agonist Lung Injury Trial (BALTI) a randomizedplacebo-controlled clinical trial Am J Respir Crit CareMed 2006173281ndash7
12 Wunderer H Morgenroth K Weis G The cleaningsystem of the airways physiology pathophysiologyand effects of ambroxol Med Monatsschr Pharm20093242ndash7
13 Malerba M Ragnoli B Ambroxol in the 21st centurypharmacological and clinical update Expert Opin DrugMetab Toxicol 200841119ndash29
14 Li Q Yao G Zhu X High-dose ambroxol reduces pul-monary complications in patients with acute cervical spi-nal cord injury after surgery Neurocrit Care 201216267ndash72
15 Wauer RR Schmalisch G Bohme B et al Randomizeddouble blind trial of Ambroxol for the treatment of respira-tory distress syndrome Eur J Pediatr 1992151357ndash63
16 Refai M Brunelli A Xiume F et al Short-term periopera-tive treatment with ambroxol reduces pulmonarycomplications and hospital costs after pulmonary lobec-tomy a randomized trial Eur J Cardiothorac Surg 200935469ndash73
17 Xia DH Xi L Xv C et al The protective effects ofambroxol on radiation lung injury and influence on pro-duction of transforming growth factor beta(1) and tumornecrosis factor alpha Med Oncol 201027697ndash701
18 Ulas MM Hizarci M Kunt A et al Protective effect ofambroxol on pulmonary function after cardiopulmonarybypass J Cardiovasc Pharmacol 200852518ndash23
19 Wang Y Wang FY Pan Z et al Effects of ambroxolcombined with low-dose heparin on TNF-alpha andIL-1beta in rabbits with acute lung injury [Article inChinese] Zhongguo Ying Yong Sheng Li Xue Za Zhi201127231ndash5
20 Su X Wang L Song Y et al Inhibition of inflammatoryresponses by ambroxol a mucolytic agent in a murinemodel of acute lung injury induced by lipopolysaccharideIntensive Care Med 200430133ndash140
21 Ma YT Tian YP Shi HW et al Effects of high doseambroxol on lung injury induced by paraquat in ratsZhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi200725523ndash6
22 ARDS Definition Task Force Ranieri VM RubenfeldGD Thompson BT et al Acute respiratory distress syn-drome the Berlin Definition JAMA 20123072526ndash33
23 Schulz M Hammrlein A Hinkel U Safety and usage pat-tern of an over-the-counter ambroxol cough syrup a com-munity pharmacy based cohort study Int J ClinPharmacol Ther 200644409ndash21
24 Schmalisch G Wauer RR Bohme B Effect of earlyambroxol treatment on lung functions in mechanically ven-tilated preterm newborns who subsequently developed abronchopulmonary dysplasia Respir Med 200094378ndash84
25 Couet W Girault J Reigner BG Steady-state bioavailabil-ity and pharmacokinetics of ambroxol and clenbuterol ad-ministered alone and combined in a new oral formulationInt J Clin Pharmacol Ther Toxicol 198927467ndash72
26 Schulz KF Altman DG Moher D CONSORT GroupCONSORT 2010 Statement updated guidelines for re-porting parallel group randomised trials BMC Med 2010818
27 Leteurtre S Martinot A Duhamel A et al Validation ofthe paediatric logistic organ dysfunction (PeLOD) scoreprospective observational multicentre study Lancet2003362192ndash7
28 Ramsay MAE How to use the Ramsay Score to assess thelevel of ICU Sedation http5jsnaccuminacjpHow20to20use20the20Ramsay20Score20too20assess20the20level20of20ICU20Sedationhtm (1August 2014 date last accessed)
29 Rubenfeld GD Caldwell E Peabody E et al Incidenceand outcomes of acute lung injury N Engl J Med 20053531685ndash93
30 Demling RH Adult respiratory distress syndrome cur-rent concepts New Horiz 19931388ndash401
31 Schoenfeld DA Bernard GR Network ARDS Statisticalevaluation of ventilator-free days as an efficacy measure inclinical trials of treatments for acute respiratory distresssyndrome Crit Care Med 2002301772ndash7
32 Horowitz IN Tai K Hypoalbuminemia in critically ill chil-dren Arch Pediatr Adolesc Med 20071611048ndash1052
33 Wauer RR Schmalisch G Ambroxol for prevention andtreatment of Hyaline membrane disease Eur Resp J 1989257sndash65s
34 Chetan G Rathisharmila R Narayanan P et al Acute re-spiratory distress syndrome in pediatric intensive careunit Indian J Pediatr 2009761013ndash16
35 Dahlem P van Aalderen W Hamaker M et al Incidenceand short-term outcome of acute lung injury in mechanic-ally ventilated children Eur Respir J 200322980ndash5
36 Curley MAQ Hibberd PL Fineman LD et al Effect ofprone positioning on clinical outcomes in children with
High-dose Oral Ambroxol for pulmonary ARDS 349
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
acute lung injury a randomized controlled trial JAMA2005294229ndash37
37 Flori HR Glidden DV Rutherford GW et al Pediatricacute lung injury prospective evaluation of risk factorsassociated with mortality Am J Respir Crit Care Med2005171995ndash1001
38 Erickson S Schibler A Numa A et al Paediatric StudyGroup Australian and New Zealand Intensive Care Society(ANZICS) Acute lung injury in pediatric intensive care in
Australia and New Zealand a prospective multicentre ob-servational study Pediatr Crit Care Med 20078317ndash23
39 Capsoni F Ongari AM Minonzio F Effect of ambroxolon human phagocytic cell function Boll Ist Sieroter Milan198564236ndash9
40 Sample Size Calculator Two Parallel Sample MeansHypothesis One-Sided Non-InferioritySuperiorityhttpwwwcctcuhkeduhkstatmeantsmp_suphtm(24 March 2015 date last accessed)
350 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
- fmv033-TF1
- fmv033-TF2
- fmv033-TF3
- fmv033-TF4
- fmv033-TF6
- fmv033-TF7
- fmv033-TF8
- fmv033-TF9
- fmv033-TF10
- fmv033-TF11
- fmv033-TF12
- fmv033-TF13
- fmv033-TF15
-

dramatically at 2 h [33] Thus for sustained clinicaleffect more frequent administration (4 hourly or even2 hourly) may be required As pARDS was mostlycaused by pneumonia and bronchiolitis and majority(92) of survivors required ventilation for 14 daysD14 may be an optimal reference for measure of VFDin the study setting This pilot trial is relied on a con-venience sample results (Table 3) from which indi-cates need of sample size of 388 patients in each armwith one-sided significance level (a error) of 005 and80 power to detect 20 improvement in theobserved median VFD14 of 5 days (ie reduction of1 day in VFD14) [40]
Strengths include randomized design and care-fully planned protocols to define ventilator manage-ment sedation and extubation readiness to minimizevariations in daily management of patients Thereare many limitations as well major one being the un-regulated unmonitored hand-ventilation beforePICU admission which may have caused baro-trauma Lack of specific information on its durationmay be a potential confounder Study cohort was re-stricted to pARDS only These issues are unavoid-able and need to be tolerated to develop clinicallyefficacious interventions in the prevalent settingsHowever these would affect generalizability of re-sults Study was underpowered to demonstrate dif-ference in VFD14 There is lack of data onpharmacokinetics of enterally administered ambroxolin critically ill children It needs to be addressed be-fore conducting similar study in future Further in-flammatory oxidative and anti-protease markersshould also be evaluated to assess its pharmacologicefficacy Stratification according to severity of ARDSmay identify a subgroup of responders
C O N C L U S I O N SStudy provides useful information on prevalent situ-ation in the resource-constraint economies informsabout limitations in conducting trials in these set-tings and questionable generalizability of their re-sults Pediatric pARDS is mostly caused bypneumonia and bronchiolitis After factoring inhigher PaO2FiO2 lower OI and lesser patientswith immunocompromised states mortality is highcompared with industrialized peers High-dose oralambroxol failed to improve VFD14 In the current
cost-conscious health care environment its potentialas adjuvant therapy should be explored after havingaddressed the aforementioned issues Large pro-spective study of appropriate power with higherdoses of oral ambroxol administered more frequentlyis desirable VFD14 as composite outcome measuresis suggested for ventilated pediatric pARDS patientshowever it needs further validation
A C K N O W L E D G E M E N T SThe drug (ambroxol hydrochloride) was provided by MsAristo Pharmaceuticals Pvt Ltd Mumbai (India) The tabletsof drug (ambroxol) and placebo (lactose) was prepared atUniversity Institute of Pharmaceutical Sciences PunjabUniversity Chandigarh (India)
Work done at Emergency and Critical Care DivisionAdvanced Pediatrics Center Postgraduate Institute ofMedical Education and Research Chandigarh-160012 India
Presented at the 20th ESPNIC Medical amp NursingAnnual Congress at Verona Italy June 15ndash17 2009rdquo
R E F E R E N C E S1 Ventre KM Arnold JH Acute lung injury and acute re-
spiratory didtress syndrome In Nichols DG (ed) RogerrsquosTextbook of Pediatric Intensive Care 4th ednPhiladelphia PA Lippincott Williams amp Wilkins 2008731ndash66
2 Zhu YF Xu F Lu XL et al Chinese Collaborative StudyGroup for Pediatric Hypoxemic Respiratory FailureMortality and morbidity of acute hypoxemic respiratoryfailure and acute respiratory distress syndrome in infantsand young children Chin Med J 20121252265ndash71
3 Hu X Qian S Xu F et al Chinese Collaborative StudyGroup for Pediatric Respiratory Failure Incidence man-agement and mortality of acute hypoxemic respiratory fail-ure and acute respiratory distress syndrome from aprospective study of Chinese paediatric intensive care net-work Acta Paediatr 201099715ndash21
4 Hanson JH Flori H Application of the acute respiratorydistress syndrome network low-tidal volume strategy topediatric acute lung injury Respir Care Clin N Am 200612349ndash57
5 De Luca D Piastra M Tosi F et al Pharmacological thera-pies for pediatric and neonatal ALIARDS an evidence-based review Curr Drug Targets 201213906ndash16
6 Brun-Buisson C Richard JC Mercat A et al REVA-SRLFAH1N1v 2009 Registry Group Early corticosteroids insevere influenza AH1N1 pneumonia and acute respiratorydistress syndrome Am J Respir Crit Care Med 20111831200ndash6
348 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
7 Singer P Shapiro H Enteral omega-3 in acute respiratorydistress syndrome Curr Opin Clin Nutr Metab Care200912123ndash8
8 Pacht ER DeMichele SJ Nelson JL et al Enteral nutri-tion with eicosapentaenoic acid gamma-linolenic acidand antioxidants reduces alveolar inflammatory mediatorsand protein influx in patients with acute respiratory dis-tress syndrome Crit Care Med 200331491ndash500
9 Wilson DF Thomas NJ Markowitz BP et al Effect ofexogenous surfactant (calfactant) in pediatric acutelung injury a randomized controlled trial JAMA 2005293470ndash6
10 Matthay MA Abraham E Beta-adrenergic agonist therapyas a potential treatment for acute lung injury Am J RespirCrit Care Med 2006173254ndash5
11 Perkins GD McAuley DF Thickett DR et al The szlig-Agonist Lung Injury Trial (BALTI) a randomizedplacebo-controlled clinical trial Am J Respir Crit CareMed 2006173281ndash7
12 Wunderer H Morgenroth K Weis G The cleaningsystem of the airways physiology pathophysiologyand effects of ambroxol Med Monatsschr Pharm20093242ndash7
13 Malerba M Ragnoli B Ambroxol in the 21st centurypharmacological and clinical update Expert Opin DrugMetab Toxicol 200841119ndash29
14 Li Q Yao G Zhu X High-dose ambroxol reduces pul-monary complications in patients with acute cervical spi-nal cord injury after surgery Neurocrit Care 201216267ndash72
15 Wauer RR Schmalisch G Bohme B et al Randomizeddouble blind trial of Ambroxol for the treatment of respira-tory distress syndrome Eur J Pediatr 1992151357ndash63
16 Refai M Brunelli A Xiume F et al Short-term periopera-tive treatment with ambroxol reduces pulmonarycomplications and hospital costs after pulmonary lobec-tomy a randomized trial Eur J Cardiothorac Surg 200935469ndash73
17 Xia DH Xi L Xv C et al The protective effects ofambroxol on radiation lung injury and influence on pro-duction of transforming growth factor beta(1) and tumornecrosis factor alpha Med Oncol 201027697ndash701
18 Ulas MM Hizarci M Kunt A et al Protective effect ofambroxol on pulmonary function after cardiopulmonarybypass J Cardiovasc Pharmacol 200852518ndash23
19 Wang Y Wang FY Pan Z et al Effects of ambroxolcombined with low-dose heparin on TNF-alpha andIL-1beta in rabbits with acute lung injury [Article inChinese] Zhongguo Ying Yong Sheng Li Xue Za Zhi201127231ndash5
20 Su X Wang L Song Y et al Inhibition of inflammatoryresponses by ambroxol a mucolytic agent in a murinemodel of acute lung injury induced by lipopolysaccharideIntensive Care Med 200430133ndash140
21 Ma YT Tian YP Shi HW et al Effects of high doseambroxol on lung injury induced by paraquat in ratsZhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi200725523ndash6
22 ARDS Definition Task Force Ranieri VM RubenfeldGD Thompson BT et al Acute respiratory distress syn-drome the Berlin Definition JAMA 20123072526ndash33
23 Schulz M Hammrlein A Hinkel U Safety and usage pat-tern of an over-the-counter ambroxol cough syrup a com-munity pharmacy based cohort study Int J ClinPharmacol Ther 200644409ndash21
24 Schmalisch G Wauer RR Bohme B Effect of earlyambroxol treatment on lung functions in mechanically ven-tilated preterm newborns who subsequently developed abronchopulmonary dysplasia Respir Med 200094378ndash84
25 Couet W Girault J Reigner BG Steady-state bioavailabil-ity and pharmacokinetics of ambroxol and clenbuterol ad-ministered alone and combined in a new oral formulationInt J Clin Pharmacol Ther Toxicol 198927467ndash72
26 Schulz KF Altman DG Moher D CONSORT GroupCONSORT 2010 Statement updated guidelines for re-porting parallel group randomised trials BMC Med 2010818
27 Leteurtre S Martinot A Duhamel A et al Validation ofthe paediatric logistic organ dysfunction (PeLOD) scoreprospective observational multicentre study Lancet2003362192ndash7
28 Ramsay MAE How to use the Ramsay Score to assess thelevel of ICU Sedation http5jsnaccuminacjpHow20to20use20the20Ramsay20Score20too20assess20the20level20of20ICU20Sedationhtm (1August 2014 date last accessed)
29 Rubenfeld GD Caldwell E Peabody E et al Incidenceand outcomes of acute lung injury N Engl J Med 20053531685ndash93
30 Demling RH Adult respiratory distress syndrome cur-rent concepts New Horiz 19931388ndash401
31 Schoenfeld DA Bernard GR Network ARDS Statisticalevaluation of ventilator-free days as an efficacy measure inclinical trials of treatments for acute respiratory distresssyndrome Crit Care Med 2002301772ndash7
32 Horowitz IN Tai K Hypoalbuminemia in critically ill chil-dren Arch Pediatr Adolesc Med 20071611048ndash1052
33 Wauer RR Schmalisch G Ambroxol for prevention andtreatment of Hyaline membrane disease Eur Resp J 1989257sndash65s
34 Chetan G Rathisharmila R Narayanan P et al Acute re-spiratory distress syndrome in pediatric intensive careunit Indian J Pediatr 2009761013ndash16
35 Dahlem P van Aalderen W Hamaker M et al Incidenceand short-term outcome of acute lung injury in mechanic-ally ventilated children Eur Respir J 200322980ndash5
36 Curley MAQ Hibberd PL Fineman LD et al Effect ofprone positioning on clinical outcomes in children with
High-dose Oral Ambroxol for pulmonary ARDS 349
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
acute lung injury a randomized controlled trial JAMA2005294229ndash37
37 Flori HR Glidden DV Rutherford GW et al Pediatricacute lung injury prospective evaluation of risk factorsassociated with mortality Am J Respir Crit Care Med2005171995ndash1001
38 Erickson S Schibler A Numa A et al Paediatric StudyGroup Australian and New Zealand Intensive Care Society(ANZICS) Acute lung injury in pediatric intensive care in
Australia and New Zealand a prospective multicentre ob-servational study Pediatr Crit Care Med 20078317ndash23
39 Capsoni F Ongari AM Minonzio F Effect of ambroxolon human phagocytic cell function Boll Ist Sieroter Milan198564236ndash9
40 Sample Size Calculator Two Parallel Sample MeansHypothesis One-Sided Non-InferioritySuperiorityhttpwwwcctcuhkeduhkstatmeantsmp_suphtm(24 March 2015 date last accessed)
350 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
- fmv033-TF1
- fmv033-TF2
- fmv033-TF3
- fmv033-TF4
- fmv033-TF6
- fmv033-TF7
- fmv033-TF8
- fmv033-TF9
- fmv033-TF10
- fmv033-TF11
- fmv033-TF12
- fmv033-TF13
- fmv033-TF15
-

7 Singer P Shapiro H Enteral omega-3 in acute respiratorydistress syndrome Curr Opin Clin Nutr Metab Care200912123ndash8
8 Pacht ER DeMichele SJ Nelson JL et al Enteral nutri-tion with eicosapentaenoic acid gamma-linolenic acidand antioxidants reduces alveolar inflammatory mediatorsand protein influx in patients with acute respiratory dis-tress syndrome Crit Care Med 200331491ndash500
9 Wilson DF Thomas NJ Markowitz BP et al Effect ofexogenous surfactant (calfactant) in pediatric acutelung injury a randomized controlled trial JAMA 2005293470ndash6
10 Matthay MA Abraham E Beta-adrenergic agonist therapyas a potential treatment for acute lung injury Am J RespirCrit Care Med 2006173254ndash5
11 Perkins GD McAuley DF Thickett DR et al The szlig-Agonist Lung Injury Trial (BALTI) a randomizedplacebo-controlled clinical trial Am J Respir Crit CareMed 2006173281ndash7
12 Wunderer H Morgenroth K Weis G The cleaningsystem of the airways physiology pathophysiologyand effects of ambroxol Med Monatsschr Pharm20093242ndash7
13 Malerba M Ragnoli B Ambroxol in the 21st centurypharmacological and clinical update Expert Opin DrugMetab Toxicol 200841119ndash29
14 Li Q Yao G Zhu X High-dose ambroxol reduces pul-monary complications in patients with acute cervical spi-nal cord injury after surgery Neurocrit Care 201216267ndash72
15 Wauer RR Schmalisch G Bohme B et al Randomizeddouble blind trial of Ambroxol for the treatment of respira-tory distress syndrome Eur J Pediatr 1992151357ndash63
16 Refai M Brunelli A Xiume F et al Short-term periopera-tive treatment with ambroxol reduces pulmonarycomplications and hospital costs after pulmonary lobec-tomy a randomized trial Eur J Cardiothorac Surg 200935469ndash73
17 Xia DH Xi L Xv C et al The protective effects ofambroxol on radiation lung injury and influence on pro-duction of transforming growth factor beta(1) and tumornecrosis factor alpha Med Oncol 201027697ndash701
18 Ulas MM Hizarci M Kunt A et al Protective effect ofambroxol on pulmonary function after cardiopulmonarybypass J Cardiovasc Pharmacol 200852518ndash23
19 Wang Y Wang FY Pan Z et al Effects of ambroxolcombined with low-dose heparin on TNF-alpha andIL-1beta in rabbits with acute lung injury [Article inChinese] Zhongguo Ying Yong Sheng Li Xue Za Zhi201127231ndash5
20 Su X Wang L Song Y et al Inhibition of inflammatoryresponses by ambroxol a mucolytic agent in a murinemodel of acute lung injury induced by lipopolysaccharideIntensive Care Med 200430133ndash140
21 Ma YT Tian YP Shi HW et al Effects of high doseambroxol on lung injury induced by paraquat in ratsZhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi200725523ndash6
22 ARDS Definition Task Force Ranieri VM RubenfeldGD Thompson BT et al Acute respiratory distress syn-drome the Berlin Definition JAMA 20123072526ndash33
23 Schulz M Hammrlein A Hinkel U Safety and usage pat-tern of an over-the-counter ambroxol cough syrup a com-munity pharmacy based cohort study Int J ClinPharmacol Ther 200644409ndash21
24 Schmalisch G Wauer RR Bohme B Effect of earlyambroxol treatment on lung functions in mechanically ven-tilated preterm newborns who subsequently developed abronchopulmonary dysplasia Respir Med 200094378ndash84
25 Couet W Girault J Reigner BG Steady-state bioavailabil-ity and pharmacokinetics of ambroxol and clenbuterol ad-ministered alone and combined in a new oral formulationInt J Clin Pharmacol Ther Toxicol 198927467ndash72
26 Schulz KF Altman DG Moher D CONSORT GroupCONSORT 2010 Statement updated guidelines for re-porting parallel group randomised trials BMC Med 2010818
27 Leteurtre S Martinot A Duhamel A et al Validation ofthe paediatric logistic organ dysfunction (PeLOD) scoreprospective observational multicentre study Lancet2003362192ndash7
28 Ramsay MAE How to use the Ramsay Score to assess thelevel of ICU Sedation http5jsnaccuminacjpHow20to20use20the20Ramsay20Score20too20assess20the20level20of20ICU20Sedationhtm (1August 2014 date last accessed)
29 Rubenfeld GD Caldwell E Peabody E et al Incidenceand outcomes of acute lung injury N Engl J Med 20053531685ndash93
30 Demling RH Adult respiratory distress syndrome cur-rent concepts New Horiz 19931388ndash401
31 Schoenfeld DA Bernard GR Network ARDS Statisticalevaluation of ventilator-free days as an efficacy measure inclinical trials of treatments for acute respiratory distresssyndrome Crit Care Med 2002301772ndash7
32 Horowitz IN Tai K Hypoalbuminemia in critically ill chil-dren Arch Pediatr Adolesc Med 20071611048ndash1052
33 Wauer RR Schmalisch G Ambroxol for prevention andtreatment of Hyaline membrane disease Eur Resp J 1989257sndash65s
34 Chetan G Rathisharmila R Narayanan P et al Acute re-spiratory distress syndrome in pediatric intensive careunit Indian J Pediatr 2009761013ndash16
35 Dahlem P van Aalderen W Hamaker M et al Incidenceand short-term outcome of acute lung injury in mechanic-ally ventilated children Eur Respir J 200322980ndash5
36 Curley MAQ Hibberd PL Fineman LD et al Effect ofprone positioning on clinical outcomes in children with
High-dose Oral Ambroxol for pulmonary ARDS 349
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
acute lung injury a randomized controlled trial JAMA2005294229ndash37
37 Flori HR Glidden DV Rutherford GW et al Pediatricacute lung injury prospective evaluation of risk factorsassociated with mortality Am J Respir Crit Care Med2005171995ndash1001
38 Erickson S Schibler A Numa A et al Paediatric StudyGroup Australian and New Zealand Intensive Care Society(ANZICS) Acute lung injury in pediatric intensive care in
Australia and New Zealand a prospective multicentre ob-servational study Pediatr Crit Care Med 20078317ndash23
39 Capsoni F Ongari AM Minonzio F Effect of ambroxolon human phagocytic cell function Boll Ist Sieroter Milan198564236ndash9
40 Sample Size Calculator Two Parallel Sample MeansHypothesis One-Sided Non-InferioritySuperiorityhttpwwwcctcuhkeduhkstatmeantsmp_suphtm(24 March 2015 date last accessed)
350 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
- fmv033-TF1
- fmv033-TF2
- fmv033-TF3
- fmv033-TF4
- fmv033-TF6
- fmv033-TF7
- fmv033-TF8
- fmv033-TF9
- fmv033-TF10
- fmv033-TF11
- fmv033-TF12
- fmv033-TF13
- fmv033-TF15
-

acute lung injury a randomized controlled trial JAMA2005294229ndash37
37 Flori HR Glidden DV Rutherford GW et al Pediatricacute lung injury prospective evaluation of risk factorsassociated with mortality Am J Respir Crit Care Med2005171995ndash1001
38 Erickson S Schibler A Numa A et al Paediatric StudyGroup Australian and New Zealand Intensive Care Society(ANZICS) Acute lung injury in pediatric intensive care in
Australia and New Zealand a prospective multicentre ob-servational study Pediatr Crit Care Med 20078317ndash23
39 Capsoni F Ongari AM Minonzio F Effect of ambroxolon human phagocytic cell function Boll Ist Sieroter Milan198564236ndash9
40 Sample Size Calculator Two Parallel Sample MeansHypothesis One-Sided Non-InferioritySuperiorityhttpwwwcctcuhkeduhkstatmeantsmp_suphtm(24 March 2015 date last accessed)
350 High-dose Oral Ambroxol for pulmonary ARDS
Downloaded from httpsacademicoupcomtropejarticle-abstract6153391647427High-dose-Oral-Ambroxol-for-Early-Treatment-ofby gueston 05 October 2017
- fmv033-TF1
- fmv033-TF2
- fmv033-TF3
- fmv033-TF4
- fmv033-TF6
- fmv033-TF7
- fmv033-TF8
- fmv033-TF9
- fmv033-TF10
- fmv033-TF11
- fmv033-TF12
- fmv033-TF13
- fmv033-TF15
-