high dependency care audit for children & young people in scotland – interim report
DESCRIPTION
High Dependency Care Audit for Children & Young People in Scotland – Interim Report. Background to the High Dependency Care (HDC) Audit. The Kerr Report recommended: “that the age for admitting children & young people to acute care in paediatric facilities is up to their 16 th birthday”. - PowerPoint PPT PresentationTRANSCRIPT

High Dependency Care Audit for Children & Young
People in Scotland – Interim Report
Background to the High Dependency Care (HDC) Audit• The Kerr Report recommended:
“that the age for admitting children & young people to acute care in paediatric facilities is up to their 16th birthday”.
• Delivering for Health:– “continued provision of paediatric intensive care and high
dependency care (HDC) is an immediate issue for NHSScotland in the light of trends in activity and case mix that may not be sustainable within current provision.”
• SEHD commissioned NSD to conduct audit, to assess demand across Scotland and the current capacity to provide HDC:– quantity – high dependency care audit;– quality – assessing paediatric services against national
standards (West Midland Guidelines).

HDC Audit - Methodology
• Aim to identify where children with HDC needs are currently managed, how many, levels of HDC care and the number transferred.
• Development of a set of national high dependency care criteria and classification standards.
• 12-14 month prospective audit – in all hospitals across Scotland.
• Include all children up to their 16th birthday.
• Pilot conducted in wards within DGH, Tertiary Hospitals and Adult Hospitals.

HDC Audit – roll out began in October 2006, all hospitals were participating by end of
Nov. Health Board Children’s
WardsAdult Wards
Ayrshire & Arran 2 4
Borders 1 7
Dumfries & Galloway 1 5
Fife 3 13
Forth Valley 2 16
Greater Glasgow & Clyde
12 142
Grampian 7 9
Highland 1 19
Lanarkshire 2 13
Lothian 12 36
Orkney 0 3
Shetland 0 3
Tayside 6 10
Western Isles 0 4
Total 49 284
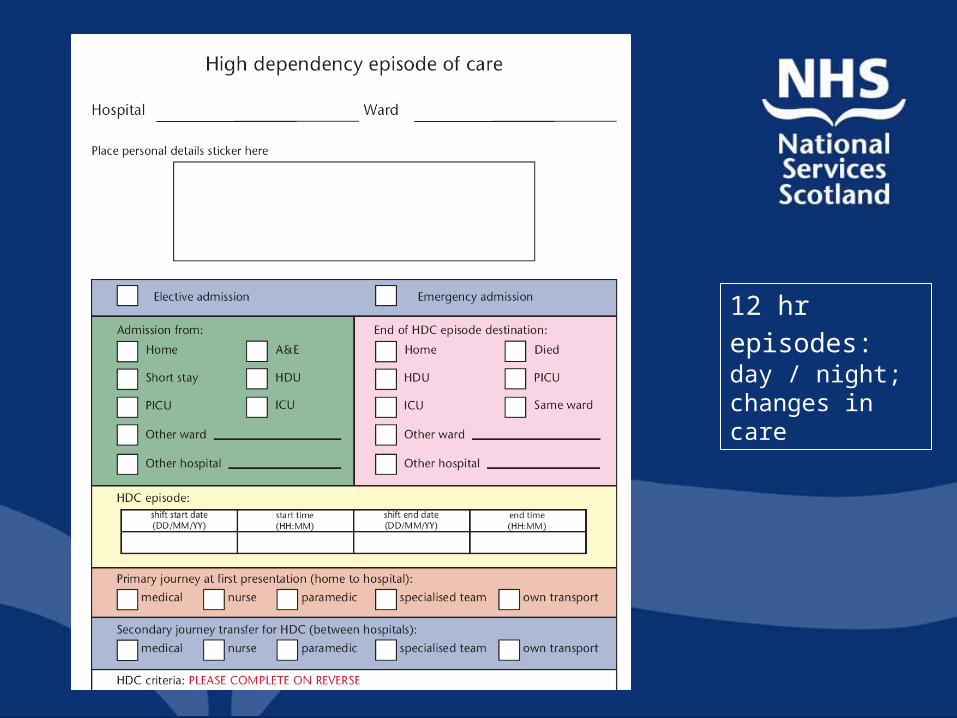
12 hr episodes: day / night; changes in care
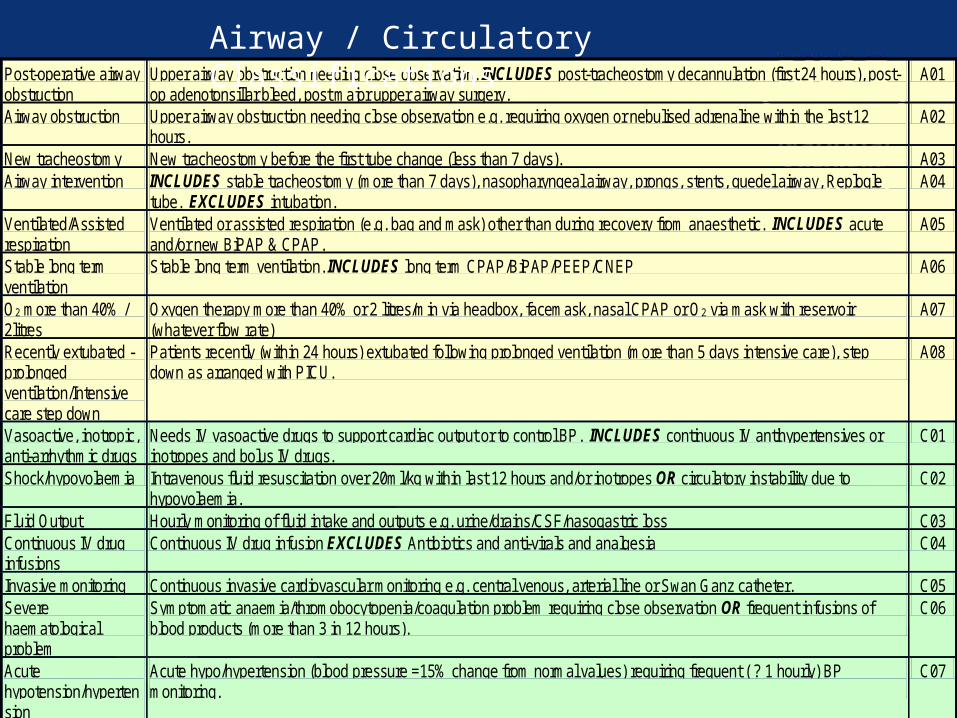
Post-operative airway obstruction
Upper airway obstruction needing close observation. INCLUDES post-tracheostomy decannulation (first 24 hours), post-op adenotonsillar bleed, post major upper airway surgery.
A01
Airway obstruction Upper airway obstruction needing close observation e.g. requiring oxygen or nebulised adrenaline within the last 12 hours.
A02
New tracheostomy New tracheostomy before the first tube change (less than 7 days). A03 Airway intervention INCLUDES stable tracheostomy (more than 7 days), nasopharyngeal airway, prongs, stents, guedel airway, Replogle
tube. EXCLUDES intubation. A04
Ventilated/Assisted respiration
Ventilated or assisted respiration (e.g. bag and mask) other than during recovery from anaesthetic. INCLUDES acute and/or new BiPAP & CPAP.
A05
Stable long term ventilation
Stable long term ventilation. INCLUDES long term CPAP/BiPAP/PEEP/CNEP A06
O2 more than 40% / 2litres
Oxygen therapy more than 40% or 2 litres/min via headbox, facemask, nasal CPAP or O2 via mask with reservoir (whatever flow rate)
A07
Recently extubated - prolonged ventilation/Intensive care step down
Patients recently (within 24 hours) extubated following prolonged ventilation (more than 5 days intensive care), step down as arranged with PICU.
A08
Vasoactive, inotropic, anti-arrhythmic drugs
Needs IV vasoactive drugs to support cardiac output or to control BP. INCLUDES continuous IV antihypertensives or inotropes and bolus IV drugs.
C01
Shock/hypovolaemia Intravenous fluid resuscitation over 20ml/kg within last 12 hours and/or inotropes OR circulatory instability due to hypovolaemia.
C02
Fluid Output Hourly monitoring of fluid intake and outputs e.g. urine/drains/CSF/nasogastric loss C03 Continuous IV drug infusions
Continuous IV drug infusion EXCLUDES Antibiotics and anti-virals and analgesia C04
Invasive monitoring Continuous invasive cardiovascular monitoring e.g. central venous, arterial line or Swan Ganz catheter. C05 Severe haematological problem
Symptomatic anaemia/thromobocytopenia/coagulation problem requiring close observation OR frequent infusions of blood products (more than 3 in 12 hours).
C06
Acute hypotension/hypertension
Acute hypo/hypertension (blood pressure =15% change from normal values) requiring frequent ( ? 1 hourly) BP monitoring.
C07
Cardioversion Has required cardioversion or DC countershock within the last 12 hours. H01 Acute or external pacing
Acute or external cardiac pacing. H02
CPR Cardiopulmonary resuscitation (within the last 12 hours). H03 Post-cardiac surgery (non ICU)
Post Cardiac Surgery (first 24 hours). H04
BMT/severe neutropenia
Any child post bone marrow transplant and/or severe neutropenia (neutrophils below 0.5 or falling). I01
Sepsis Suspected septicaemia. INCLUDE all who require at least hourly observations, including meningococcal I02 Acute renal replacement therapy/Hourly cycle PD/Acute renal failure
Acute renal replacement therapy (haemodialysis, haemofiltration) OR hourly cycle peritoneal dialysis (EXCLUDES CCPD) OR acute renal failure (urine output less than 1ml/kg/hour). EXCLUDES chronic renal failure.
K01
Diabetic ketoacidosis (DKA)
Diabetic ketoacidosis with continued deterioration in conscious level after the start of therapy. K02
Fluid/electrolyte derangement/ severe metabolic derangement
Potential/actual severe metabolic derangement, fluid or electrolyte derangement. INCLUDES frequent U&E monitoring, multiple electrolyte supplements (more than 2 in 12 hours), regular blood gas/glucose monitoring and/or frequent changes to fluid regimes and hourly urine measurement.
K03
GCS less than 12 GCS less than 12. N01
Airway / Circulatory Classifications
Co-ordination of HDC Audit
• Each hospital has a designated co-ordinator and deputy.
• Key to ensuring the quality of the data returned to NSD:– interpretation of HDC criteria – peer review;– link with NSD regarding queries on the audit
forms;– meet regularly to discuss issues.
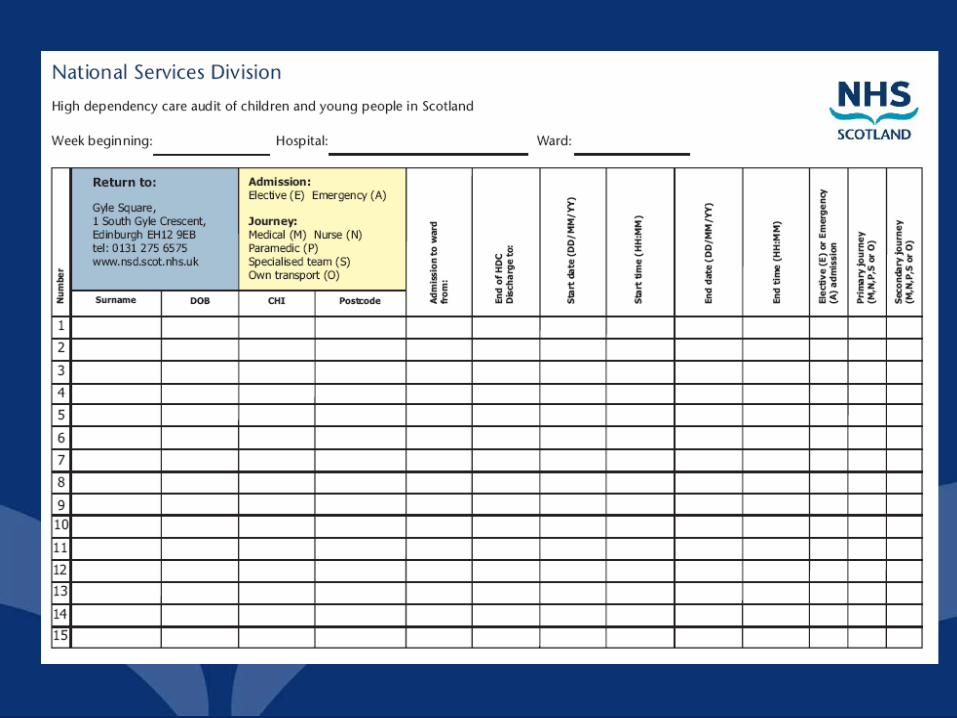
• Completed forms returned on a weekly basis from paediatric wards and monthly basis from adult wards
Audit forms should contain – the patient’s complete journey
Each form should contain the following: • hospital & ward;
• patient details – CHI, DoB, Postcode,
• type of admission – emergency / elective;
• date & time per patient – when HDC commenced & ended, not shifts.
• admission from – where was the patient prior to coming to the hospital;
• primary journey – how did the child get to the hospital;
• secondary journey – if child was transferred from another hospital – how was the child transferred;
• end destination – when HDC ended where did the child go;
• HDC criteria – for complete 12 hr period.


BRANNIGAN
BRANNIGAN


HDC Audit progress• Database Issues:
– delays developing database;– backlog of data entry;– quality of initial audit forms received – still
working on clearing the outstanding queries;– delay in feedback to wards/hospitals.
• Data presented is not complete due to backlog/queries.
• Staffing issues within NSD.
• To end of December information on 1369 children has been received. (Still adding to database for Jan/Feb - to date 1687)

Number of Children included in the HDC Audit
Hospital October November December Total
Aberdeen Royal Infirmary 1 2 0 3
Balfour Hospital 0 0 1 1
Belford Hospital 7 5 3 15
Borders General Hospital 8 8 2 18
Caithness General Hospital 3 6 2 11
Crosshouse Hospital 21 25 0 46
Dr Gray's Hospital 14 6 3 23
Dumfries & Galloway Royal Infirmary 1 19 8 28
Gilbert Bain Hospital 2 1 2 5
Ninewells Hospital 24 42 49 115
Perth Royal Infirmary 0 3 2 5
Queen Margaret Hospital 0 3 2 5
Raigmore Hospital 15 18 11 44
Royal Aberdeen Children's Hospital 46 88 39 173
Royal Alexandra Hospital 0 9 3 12
Royal Hospital for Sick Children (Edinburgh) * 58 68 49 175
Southern General Hospital 0 4 2 6
Stirling Royal Infirmary 38 29 14 81
St John's Hospital at Howden 4 4 4 12
Victoria Hospital 14 30 4 48
Wishaw General Hospital 53 36 13 102
Yorkhill NHS Trust * 0 237 204 441
Total Number of Children Included in Audit 309 643 417 1369
* Significant amount of outstanding data entry

HDC Audit – planning tool / issues impacting on children’s services
• Capacity:– no of HDC episodes; no. of children; episodes per
child;
• Location:– where do children receive HDC; type of hospital,
regional location.
• Demand:– proportion emergency / elective admissions.
• Staffing:– proportion day / night HDC
• Patient Pathway:– how many children are transferred to another
hospital;– how do children arrive at hospital;– where do they go after HDC.

Breakdown of HDC for children in audit to date.
HDC care provided in Short Stay, Paediatric Ward, HDU.
Treatment CodeNo. of Patients Categories
Post-operative airway obstruction 12
Airway obstruction 12
Airway intervention 13
AirwayVentilated/Assisted respiration 13
Stable long-term ventilation 3
O2 more than 40% 63
Recently extubated - prolonged ventilation/Intensive care step down
1
Vasoactive, inotropic, anti-arrhythmic drugs 1
Fluid balance 42
Shock/hypovalaemia 4
CirculatoryMultiple IV drugs or continuous infusion 33
Invasive monitoring 9
Severe haematological problem 5
Acute hypotension/hypertension 1
Cardioversion 1 Cardiac
CPR 1
BMT/severe neutropenia 6 Infection
Septicaemia 10
Acute renal replacement therapy/Hourly cycle PD/Acute renal failure
1
Diabetic ketoacidosis (DKA) 7 Renal
Severe metabolic/fluid/electrolyte derangement 10

Treatment CodeNo. of Patients Categories
GCS 8-12 14
Prolonged/recurrent seizures 9
Complex anti-convulsants 6 Neurology
Post - craniotomy 1
Hourly neuro observations 50
Apnoeas/cyanotic episodes 8
Deterioration to ventilation 7
Severe asthma/bronchodilators 34 Respiratory
ECG and Sa02 monitoring 30
2+ chest drains & hourly replacement 1
Arrhythmias 2
Sedation or GA for ward procedure 49
Complex pain control 28
Frequent sampling/dressings 10
End of life care 3 Other
Major trauma 3
Previous rapid deterioration resulting in PICU admission 3
Central lines 1
Minor surgery, same day 1 Neonates
Morphine 2
Breakdown of HDC for children in audit to date.
HDC care provided in Short Stay, Paediatric Ward, HDU.

Where children who require HDC were admitted from:
Oct Nov Dec Jan Feb
% % % % %
A & E 29 25 30 22 54
Same Ward 0 1 5 0 0
HDU (transferred from HDU to Wd still requiring
HDC) 6 1 6 0 0
Home 29 48 43 31 8
ICU 0 0 0 0 0
Other Ward 19 19 19 46 38
Other Hospital 12 5 3 0 0
PICU 0 0 0 0 0
Short Stay 5 1 5 1 0
Patient Journey
HDC Audit – implications for children’s nurses
• Aim is to produce report Spring 2008; supporting the planning of local, regional and national planning of critical care services.
• Assessment of paediatric facilities, will be included in final report.
• Provide evidence to support local needs analysis:– training – differing between hospital
environments;– staffing levels;– facilities;– equipment– epidemiological data of patient base
(Data Warehouse linkage).

HDC Audit – implications for children’s services
• Ethos of Delivering for Health is to provide services as locally as possible.
• Current paediatric service provision – centralisation of paediatric intensive care (2) and high dependency units (4).
• This audit will identify the number of children with high dependency care needs across all hospitals and wards – linking to the development of a managed critical care network.

Acknowledgements to -Julie AdamsProject Manager National Services Division