herbal drugs: a vierew on actices rp 1 file4 1 herbal drugs: a review on practices although animal...
TRANSCRIPT

3D.D. Joshi, Herbal Drugs and Fingerprints: Evidence Based Herbal Drugs, DOI 10.1007/978-81-322-0804-4_1, © Springer India 2012
Introduction
Herbal drugs have been used throughout history similar to the way modern pharmaceuticals are utilized today (i.e., to improve human health). Fossil evidence suggests that plants were used medici-nally in prehistoric times. Although the fi rst use of plant-derived pharmaceuticals may be dif fi cult to pinpoint, but use of herbals for human health is the basis for the modern pharmaceutical industry. History makes a man wise, so we start from the point to the present to have prosperous future on the subject to be discussed. Traditional herbal drugs are very popular in different systems of medicines like Indian system of medicine (ISM), traditional Chinese system (TCM), Unani natur-opathy, oestropathy, and homeopath. All over the world, plants play an important role in healthcare of majority of population. In India alone, nearly two million traditional health practitioners use plants for treatment of various ailments [ 1 ] . In traditional system, only a few markers of phar-macologically active constituents were employed to assess the quality and authenticity of complex herbal medicines; however, the therapeutic effects of herbal drugs are based on the complex interac-tion of numerous ingredients in combination, which are totally different from those of synthetic drugs. Thus, many kinds of chemical fi ngerprint methods to control the quality of herbal drugs have gradually come into practices, such as thin-layer chromatography, gas chromatography, and high-performance liquid chromatography. The
chromatographic fi ngerprint analysis represents a comprehensive qualitative approach for the purpose of species authentication, evaluation of quality, and ensuring the consistency and stability of herbal drugs and their related products. The entire composition of compounds is evaluated to determine not only the presence or absence of desired markers or active constituents but the complete set of ratios of all detectable analytes. The chemical fi ngerprints obtained by chromato-graphic and electrophoretic techniques, espe-cially by hyphenated chromatographies, are strongly recommended for the purpose of quality control of herbal drugs, to decipher ingredients, and therefore be used for authentication and identi fi cation of the herbal products. Current global regulations recommend a drug, which is assessed to toxicity, and other clinical data.
Asian Continent and Traditional Herbal Drugs
The two famous ancient human civilizations of world, the Chinese civilization and the Vedic civilization, were from Asia, had well- fl ourished healthcare system, mainly based on herbals, and still have acceptance as time tasted system.
China and Japan
Traditional Chinese medicines (TCM) have been used by Chinese people from ancient times,
1 Herbal Drugs: A Review on Practices

4 1 Herbal Drugs: A Review on Practices
although animal and mineral materials have been used, but primary source of remedies is botanical. In TCM, about 12,000 herbals are used by tradi-tional healers, of which 500 are common. Herbals are generally used only after processing, for example, stir-frying or soaking in vinegar or wine. In clinical practice, traditional diagnosis may be followed by the prescription of a complex and often individualized remedy. TCM are still common use in China. More than half of the population regularly uses traditional remedies, with the highest prevalence in rural areas. About 5,000 traditional remedies are available in China, accounting for approximately one fi fth of the entire Chinese pharmaceutical market [ 2 ] . Chinese herbalists usually do not prescribe single herb for their patients, but recommend in combi-nations of 8–15 herbs. There are three major rea-sons to support the combination practice. Mutual reinforcement involves combining two or more very similar herbs together to create a stronger effect. Mutual assistance is the way to use one herb to help another work better. Mutual restraint is meant to use one herb to reduce or eliminate side effects of another herb in the combination. Historically, Chinese medicines were practiced largely within a family-based lineage system, from generation to generation. The speci fi c tech-niques and knowledge required to practice were transmitted from teacher to student in the context of an apprenticeship relationship; because of this way of transmitting the art and science of Chinese medicine, there emerged many different styles of practice, each associated with a particular family lineage. At the time of the Chinese Cultural Revolution, a decision was made to standardize and secularize the practice of Chinese medicine. This was carried out by examining the various family lineages, extracting what they seemed to have in common, eliminating anything that the communist government considered to be too overtly spiritual, and naming the resulting collec-tion of knowledge and techniques as traditional Chinese medicine (TCM), of fi cially approved version of Chinese medicine, which subsequently is being taught largely in government-sponsored schools instead of within a family-based appren-ticeship system, and has three main objectives:
(a) to treat acute diseases by killing pathogen; (b) to heal chronic illness (e.g., gastrointestinal disorder, respiratory disorder, allergies, immune system de fi ciency) by strengthening the body, helping to recover it; and (c) maintaining daily life healthy by keeping the balance of human body.
In general, under TCM, herbs can treat a wide variety of diseases and conditions, as compared to synthetic drugs, and have much gentler and safer impact. Most of Chinese herbs do not cause side effects; even a few can be easily counter-acted with other herbs. For these reasons, people turned to TCM. More and more people rely on TCM as alternative after synthetic medicine failed and is a very good alternative for those who are looking for a natural alternative for the con-ventional western medicine. Presently, there are many highly ef fi cient Chinese herbal patented medicines, for pain syndromes, gastrointestinal disorders, neurological disorders, stress-related syndromes, respiratory disorders, heart problems, sexual dysfunction, allergies, and immune system de fi ciencies, as well as replacements for antibiotics and anti-in fl ammatory drugs [ 3 ] . A major disad-vantage of the standardization of TCM is lack of its spiritual roots. Contemporary practitioners wishing to revive this spiritual rooting, and the knowledge/techniques associated with it, often name themselves as practitioners of “Classical Chinese Medicine” (i.e., the form of the medicine prior to the Cultural Revolution) or fi ve-element practitioners. Generally speaking, a TCM practi-tioner will rely primarily upon the “eight-principle” diagnostic framework. A TCM practitioner is likely to pay more attention to physical symp-toms and design treatment to eliminate the symp-toms. The fi ve-element practitioners, on the other hand, tend to be more focused on the emotional and spiritual aspects of the imbalance and aim their treatments at the root cause of the dishar-mony. Great variety exists among the Chinese practitioners, but both the “eight principles” and “ fi ve-element” frameworks are important aspects of theoretical foundation of the medicine. The uniqueness of Chinese medicines is the insight look that physical, emotional, mental, and spiritual aspects of an individual are always

5Asian Continent and Traditional Herbal Drugs
interconnected and exist within a larger web which ultimately includes the entire cosmos. Some herbs are too strong for pregnant women and may cause miscarriage. Certain foods can have adverse effects on the herbal therapy. It is a thumb rule that during use of TCM, one should avoid the raw food (e.g., vegetables should be cooked, but fruits are okay), greasy, strong-tasting or -smelling, dif fi cult to digest (such as beef), or irritating to the digestive system (like spicy foods). So it is recommended to consult to the health expert before using TCM.
In Japanese traditional healing system, many herbal remedies found their way from China into the Japan, through Korea. Herbs native to Japan have been classi fi ed in the fi rst pharmaco-poeia of Japanese traditional medicine in the ninth century [ 4 ] .
Indian Subcontinent
Ayurveda, a medical system primarily practiced in India known for nearly 5,000 years, includes diet and herbal remedies, while emphasizing the body, mind, and spirit in disease prevention and treatment. During Vedic civilization, Ayurvedic scholars were very particular for quality control and site for collection of suitable raw herbs for medicine (e.g., Himalaya is the best place for collection of medicinal plants of hill origin [ 5 ] ). There is description that scholars were not afraid to diseases even to death, as they had expertise to keep it away up to certain period by use of their unique formulations [ 6 ] . In Vedic civilization, Ayurveda was a system of healing cognized by sages of the Vedanta philosophy, which describe the relation of doctor (Vaidhya) and patient as friends. The doctor had prime duty to protect the life of his patient without any discrimination, as the royal doctor of Ravan treated Laxaman, the younger brother of Lord Ram during Ram–Ravan battle. He disclosed the habitat of the unique healing herb and instructed to Hanuman to collect it [ 7 ] . The collection practices were of high moral value as Lord Hanuman had dif fi culty in identi fi cation of the herb, and to avoid adultera-tion, he pulled the whole hill and went to Lanka
from Himalaya; fi nally, Sushen selected proper herb and treated Laxaman [ 8 ] . Ayurveda, generally mistaken with exotic herbs, oils, and therapies, this is not what it is. It is fi nding of harmony with the whole of life and ultimately realizing our true universal nature as pure cosmic consciousness beyond koshas (bodies) or ahamkara (ego). The word Ayur + Veda = Ayurveda [(life) + (knowledge or wisdom)] describes how the ancient sages cognize Ayurveda, where fi rst we have to go beyond our own limited perspective of our current experience of mind and try to see with more clarity what mind really is and how all of our experience is directly affected by it. The eternity of Ayurveda is also described in the Charak Samhita (one of the scriptures in Sanskrit language). Acharya Charak (600 bc ) was the father of Ayurvedic medicine. His renowned work “Charak Samhita” which is considered the encyclopedia of Ayurveda today goes in depth about his principals, diagnoses, and cures that still retain their potency and truth even after a couple of millennia. His research led to the facts of the human anatomy, embryology, pharmacology, blood circulation, and diseases like diabetes, tuberculosis, and heart disease. Charak Samhita describes medicinal qualities and functions of 100,000 medicinal plants on which present scientists are still doing research to fi nd the fact as per their language. Therefore, even Ayurveda, popularly known as the fi fth Veda, is originated in the divine mind and descended from the divine sources to the ancient physicians.
This ancient Indian science of healing seeks to reestablish the harmony between the body and its habitat by creating the optimum health environ-ment. Over centuries, Ayurveda has had a nurturing in fl uence on ancient TCM, Unani, and the humoral medicine practiced by Hippocrates in Greece. The entire science of Ayurveda is based on the “ fi ve great elements” (Panchabhuta) theory. These fi ve elements are earth (prithvi), water (jal), fi re (agni or tej), air (vayu), and ether (space or akash). Ayurveda strongly advocate for ele-mental structure of the body. There are also fi ve mahabhutas (elements) in the human body, and these fi ve mahabhutas are represented in the form of doshas, dhatus, and malas. Outside the body,

6 1 Herbal Drugs: A Review on Practices
they form the basic ingredients of the drugs and food ingredients. In a normal body of a living being, these substances remain in a particular proportion. However, because of enzymatic action inside the human body, this ratio of fi ve mahabhutas or their equilibrium inside the body gets disturbed. The body has, however, a natural tendency to maintain equilibrium. It eliminates some of the mahabhutas which are in excess and takes some of the mahabhutas which are in short-age. This shortage of mahabhutas is replenished through the ingredients of herbs, food, drinks, etc.
Traditional Herbal Drugs in Europe
The “doctrine of signatures,” adopted and pro-moted by Dioscorides, a Greek, working as a Roman military physician, and wrote his De Materia Medica , whereby plants have been used for medicinal purposes according to their resem-blance to parts of the human anatomy, for exam-ple, shape or color. Theophrastus (372–286 bc ) introduced the word “orchids” for the under-ground tubers, which resemble to testicles (Fig. 1.1 ). The Greeks referred to testicles as “orchis . ” In Enquiry into Plants, Theophrastus has reported that the orchids had medicinal properties. Naturally, this led to orchid tubers
being used to heal diseases of the testicles, and to stimulate lust (Table 1.1 ), and supposed to produce a male progeny if given to men as whole new tubers; and if the shriveled old tubers were given to women, this should produce female children [ 9 ] .
William Turner was the fi rst English herbalist (1568) to describe the four main uses, including the treatment of alcoholic gastritis [ 8 ] , and after 11 years, Williams Langham reported antipyretic, anti-consumption, and anti-diarrheal effects [ 9 ] . John Parkinson in 1640 described the tubers to increase fertility in men, and the Ottomans extracted the Salep of the dried tubers [ 10 ] . In the East, Salep was (and is) mainly made from Orchis morio , but it could be made in the UK from Orchis mascula , the early purple orchid, or from Orchis maculata or Orchis latifolia. Orchids, pre-sumably as Salep, were dispensed in London in Oliver Cromwell’s time, and before the introduc-tion of coffee, hot drinks of Salep were sold at stalls in the streets of London. The tubers were mainly imported from the East but also came from Oxfordshire. In Hamlet, Ophelia’s fantastic garlands included “long purples” that were gen-erally known either by a rude name or by the name “dead man’s fi ngers” in rude scenes, a refer-ence to testicles, then the orchids must have been of the genera Orchis or Ophrys, second from the
Fig. 1.1 Tubers of early purple orchid [ 9 ]

7Traditional Herbal Drugs in America
implies genus Dactylorhiza where the tubers are palmate and resemble fi ngers. Today, Salep is largely collected from Asia. Turkey uses the greatest bulk in making ice cream and beverages, but not allowed to export the tubers any more. Turkey still uses vast quantities, as takes 2,600 tubers to obtain 1 kg of dried tubers [ 9 ] .
Traditional Herbal Drugs in America
Vanilla, an aromatic oil, is exuded from the seed pods of v anilla, a well-known example of tradi-tional herbal healing knowledge of America (Table 1.2 ) [ 9 ] . Apparently the word “vanilla” is derived from the Spanish word “vainilla” which in turn came from the Latin “vagina” or pod or
sheath. The most important vanilla species is Vanilla planifolia , introduced into Europe by the Spanish in 1510 and brought to popularity in the UK when the Marquess of Blandford introduced it here in 1800. Unlike Salep, vanilla can be farmed, but the fl avor and aroma molecule, vanil-lin (4-hydroxy-3-methoxy-benzaldehyde), is now produced synthetically. The Aztecs had several uses for vanilla, but today its medicinal uses are con fi ned to relieving nausea and improving food intake in patients receiving chemotherapy and as a diagnostic aroma for Alzheimer’s disease, with loss of the sense of smell being an early manifes-tation of this condition. It has been described as an antimicrobial agent and acts as preservative to prolong the life of food products. Vanilla pom-pona was also used to fl avor tobacco in Cuba [ 9 ] .
Table 1.1 Summarized detail of orchid products in European healing system [ 9 ]
Author Year Proposed use of orchid
Preparation Indication
Turner W 1568 Tuber with goats milk Aphrodisiac Dry Antiaphrodisiac Topical Antiseptic Tuber Gastrointestinal due to wine
Langham W 1579 Tuber Antipyretic Tuber Anti-consumption Tuber Anti-diarrhea
Parkinson J, Ottomans 1640 Tuber Increase fertility in men Tuber (Salep) Aphrodisiac
Make ice cream (Turkey) Coffee substitute (Albania)
Table 1.2 Medical uses of vanilla [ 9 ]
Author Year Proposed use of vanilla derivatives
Aztec herbal 1552 Flavoring and perfume prevent fatigue in those holding public of fi ce, bestow the bodily strength of a gladiator Drive weariness far away Drive out fear and fortify the human heart
Menashian et al . 1992 Improve food intake and reduce nausea and vomiting in patients given chemotherapy
Fladby et al . 2004 Diagnostic of Alzheimer’s disease (patients cannot smell vanilla)
Fitzgerald et al . 2004 Antimicrobial against Escherichia coli, Lactobacillus plantarum, and Listeria innocua

8 1 Herbal Drugs: A Review on Practices
Traditional Herbal Drugs in Australia
The historical records describe the use of orchids by Australian aborigines and early settlers (Table 1.3 ). In addition, many orchid bulbs were employed as emergency bush food, for example, Gastrodia sesamoides (roasted), Dendrobium speciosum, and Caladenia species. Diuris maculata has sweet-tasting tubers, but Lawler and Slaytor warn that some Australian herbal bulbs have toxic alkaloids, for example, Liparis re fl exa [ 9 ] .
Traditional Herbal Drugs in Africa
The traditional healing systems of Africa are still a matter of study. Brian Morris has described 12 medicinal plants currently used as medicine in Malawi. Nine of these are used for stomach com-plaints and two for fertility problems. Interestingly, two species, Cyrtorchis arcuata and Eulophia cucullata, are employed to promote friendship, the former being dried and pounded into a powder and the latter prepared as an infusion of the roots. Cyrtorchis arcuata is also employed to treat diabetes or skin infections and Eulophia cucul-lata to prevent epilepsy. An infusion of the leaves and pseudobulbs of Bulbophyllum maximum is used to protect against sorcery and Tridactyle tricuspis to treat madness [ 9 ] .
In Zambia, medicinal plants as boiled root tubers of terrestrial orchids are used to make a
food dish, chikanda or kinaka . The orchids involved are from three genera Disa, Habenaria, and Satyrium. The orchids have become scarce in Zambia and are now illegally imported from Tanzania. Four million Tanzanian herbals are currently sent from Tanzania to Zambia each year. In Africa, an amulet of leaves of Ansellia africana impregnated with a paste made from the pseudobulbs is considered as a contraceptive but, most conveniently, only in the short term for unmarried women. In the Molucca islands, the seeds of Grammatophyllum scriptum have been added to a woman’s food to ensnare her for life. Berliocchi also pointed out that Bourbon tea, popular in the nineteenth century, was made from an infusion of orchids from Mauritius and Reunion that included Angraecum fragrans . The tea was thought to be a sedative. A tincture was also made to apply to the fi ngertips and improve the sense of touch. Both vanilla and Salep are widely in use for a delicious fl avoring and won-derful perfume, respectively, and used in making ice cream and beverages, although many are not enthusiastic about the aroma of Salep [ 9 ] .
Industrialization of Herbal Drugs and Legislation
The safety of some herbal ingredients have been recently called into question because of the identi fi cation of adverse events associated with their use and, increasingly, because of the dem-onstration of clinically relevant interactions between herbs and prescribed drugs, for example, the adverse events (stroke, heart attacks, heart-rate irregularities, liver toxicity, seizures, psychoses, and death) associated with use of ephedra in formulations for weight loss. The bodybuilding effects and increased energy due to kava-kava (also known as kawa), widely used in Europe and increasingly in Canada to treat anxiety, nervous-ness, insomnia, pain, and muscle tension, have raised issues to some countries to enforce regula-tions restricting or banning these products. A few herbs in common use have been suspected of causing cancer. These include Aristolochia , Rubia tinctorum , Morinda of fi cinalis, and Senecio riddellii .
Table 1.3 Use of medicinal plants by Australian aborigi-nes and early settlers [ 9 ]
Name of medicinal plants Uses
Cymbidium canaliculatum Cure for dysentery Food
Cymbidium madidum Oral contraceptive Cure for dysentery
Dendrobium teretifolium (bruised leaves)
Rub to relieve pain
Dendrobium discolor Poultice Young canes Mature canes (bruise and extract with spirit)
Cures ringworm

9Phytochemical Standardization
Although prolonged and apparently uneventful use of a substance usually offers testimony of its safety, investigation of the potential toxicity of naturally occurring substances may reveal previously unsuspected problems.
The recent global resurgence of interest in herbal drugs has led to an increase in the demand for them. The need of the hour is to evolve a sys-tematic approach and to develop well-designed methodologies for the standardization of herbal raw materials and herbal formulations. Traditional systems of medicine are in use since centuries all over the world. According to one estimate, 80% of the world population still depends on herbal products for their primary healthcare needs. The toxic side effect of drugs of modern medi-cine and the lack of medicines for many chronic ailments have led to the reemergence of the herbal drugs, with possible treatments for many health problems. They have stood the test of time for their safety, ef fi cacy, cultural acceptability, and lesser side effects. The chemical constituents present in them are a part of the physiological functions of living fl ora, and hence they are believed to have better compatibility with the human body. Most diseases, like diabetes, heart diseases, cancer, and psychiatric disorders, are multifactorial and hence need therapeutic inter-vention at more than one level. Plants with com-plex phytochemical mixtures have advantage over single molecules in treating such diseases, with an added advantage of being devoid of toxic side effects [ 10 ] .
With commercialization of the herbal drugs assurance of safety, quality and ef fi cacy has become an important issue. The herbal raw mate-rial is prone to a lot of variations due to several factors, the important ones being the identity of the plants and seasonal variation (which depend on the time of collection), the ecotypic, genotypic, and chemotypic variations, drying and storage conditions, and the presence of xenobiotics. WHO stresses the importance of the qualitative and quantitative methods for characterizing the samples and quanti fi cation of the biomarkers and chemical markers with fi ngerprint pro fi les. A known ingredient of the herbal leads to logical therapeutic ef fi cacy, whereas the active ingredients
are not yet known; the marker ingredient speci fi c for that particular botanical is chosen for analytical purpose. The advancements in modern methods of analysis and the development of their applica-tion have made it possible to solve many of these problems. Techniques like HPTLC, GC, MS, HPLC, LC–MS, and GC–MS are extremely valuable to establish the markers for unknown herbals. Starting from sourcing of the raw mate-rial, standardization, and preparation of the extracts to formulation of the extracts into suitable dosage form, the problems vary with each plant species and part of the plant that is being used. At each and every step, phytochemical pro fi les have to be generated and a multiple-marker-based standardization strategy needs to be adopted to minimize batch-to-batch variation and to maintain quality and ensure safety and ef fi cacy [ 10 ] .
Phytochemical Standardization
In herbals and herbal drugs, standardization starts with correct identity of the sample, organoleptic evaluation, pharmacognostic evaluation, volatile matter, quantitative evaluation (ash values, extrac-tive values), phytochemical evaluation, test for the presence of xenobiotics, microbial load test-ing, toxicity testing, and biological activity. The phytochemical pro fi le has a special signi fi cance as it is directly linked with the activity of the herbal drugs. The fi ngerprint pro fi les serve as guideline to the phytochemical pro fi le of the drug in ensuring the quality, while quanti fi cation of the marker compound(s) serves as an additional parameter in assessing the quality of the sample. Phytochemical standardization encompasses all possible information generated with regard to the chemical constituents present in an herbal drug. Hence, the phytochemical evaluation for standardization purpose includes (1) preliminary testing for the presence of different chemical groups, (2) quanti fi cation of chemical groups of interest (e.g., total alkaloids, total phenolics, total triterpenic acids, total tannins), (3) establishment of fi ngerprint pro fi les, (4) multiple-marker-based fi ngerprint pro fi les, and (5) quanti fi cation of important chemical constituents.

10 1 Herbal Drugs: A Review on Practices
Extraction of Therapeutics
The phytochemical evaluation is done by scienti fi cally designed work plan and fi nally vali-dated before the chemical characterization of the herb. Based on the physical and chemical proper-ties, the therapeutics may be extracted by:
Supercritical Fluid Extraction This is the most technologically advanced extrac-tion system. Supercritical fl uid extraction (SFE) involves use of gases, usually CO
2 , and com-
pressing them into a dense liquid. This liquid is then pumped through a cylinder containing the material to be extracted. From there, the extract-loaded liquid is pumped into a separation chamber where the extract is separated from the gas and the gas is recovered for reuse. Solvent properties of CO
2 can be manipulated and adjusted by
varying the pressure and temperature. The advan-tages of SFE are the versatility it offers in pin-pointing the desired constituents to extract from a given material and the fact that end product has no solvent residues left in it (CO
2 evaporates
completely). The downside is that this technology is quite expensive. There are many other gases and liquids that are highly ef fi cient as extraction solvents when put under pressure. Coupled SFE-SFC System in which a sample is extracted with a supercritical fl uid which then places the extracted material in the inlet part of a super-critical fl uid chromatographic system. The extract is than chromatographed directly using super-critical fl uid. Coupled SFE–GC and SFE–LC system in which a sample is extracted using a supercritical fl uid which is then depressurized to deposit the extracted material in the inlet part or a column of gas or liquid chromatographic system, respectively. SFE is characterized by robustness of sample preparation, reliability, less time-consuming, high yield, and also has potential for coupling with a number of chromatographic methods [ 10 ] .
Microwave-Assisted Extraction An innovative, microwave-assisted solvent extraction technology known as microwave-assisted processing (MAP) offers many advantages
over conventional methods. Applications include the extraction of high-value compounds from natural sources, including nutraceuticals and functional food ingredients, and pharmaceutical actives from biomass. MAE technology offers a few advantages as (a) improved products, increased purity of crude extracts, and improved stability of marker compounds, possibility to use less toxic solvents and (b) reduced processing costs, increased recovery and purity of marker compounds, very fast extraction rates and reduced energy and solvent usage. With microwaves drive extraction as opposed to diffusion, very fast extraction rates and greater solvent fl exibility are possible. Many variables, including the micro-wave power and energy density, can be tuned to deliver desired product attributes and optimize process economics. The process can be custom-ized to optimize for commercial/cost reasons, and excellent extracts are produced from widely varying substrates. Examples include, but are not limited to, antioxidants from dried herbs, carote-noids from single cells and plant sources, taxanes from taxus biomass, essential fatty acids from microalgae and oilseeds, phytosterols from medicinal plants, polyphenols from green tea, fl avor constituents from vanilla and black pepper, essential oils from various sources, and many more [ 10 ] .
Solid-Phase Extraction This involves sorption of solutes from a liquid medium into a solid adsorbent by the same mech-anisms by which molecules are retained on chro-matographic stationary phases. These adsorbents, like chromatographic media, come in the form of beads or resins that can be used in column or in batch form. They are often used in the commer-cially available form of syringes packed with medium (typically a few hundred milligrams to a few grams) through which the sample can be gently forced with the plunger or by vacuum. Solid-phase extraction media include reverse phase, normal phase, and ion-exchange media. This is method for sample puri fi cation that sepa-rates and concentrates the analyte from solution of crude extracts by adsorption onto a disposable solid-phase cartridge. The analyte is normally

11Phytochemical Standardization
retained on the stationary phase, washed and then evaluated with different mobile phases, for exam-ple, when an aqueous extract is passed down a column containing reverse-phase packing mate-rial, everything that is fairly nonpolar binds, whereas everything polar passes through [ 10 ] .
Analysis for Marker and Chromatographic Fingerprint
A chromatographic fi ngerprint of an herbal drug is a chromatographic pattern of the extract of pharmacologically active ingredients. This chro-matographic pro fi le is featured by the fundamental attributions of integrity and fuzziness or same-ness and differences so as to chemically represent the herbal drug investigated. The chromatographic fi ngerprints are used for authentication and identi fi cation of herbal drugs accurately. Herbal drug and its extract have hundreds of unknown components, and many of them are in low amount, sometimes in various concentrations, so it is very important to obtain reliable chromatographic fi ngerprints that represent pharmacologically active and chemically characteristic components of the herbal drug. In the phytochemical evalua-tion of herbal drugs, TLC is being employed extensively for the following reasons: (i) It enables rapid analysis of herbal extracts with minimum sample cleanup requirement, (ii) it provides qualitative and semiquantitative infor-mation of the resolved compounds, and (iii) it enables the quanti fi cation of chemical constituents. Fingerprinting using HPLC and GLC is also carried out in speci fi c cases. In TLC fi ngerprinting, the data that can be recorded using a high-performance TLC (HPTLC) scanner includes the chromato-gram, R
f values, the color of the separated bands,
their absorption spectra, l max, and shoulder in fl ection(s) of all the resolved bands. All of these, together with the pro fi les on derivatization with different reagents, represent the TLC fi ngerprint pro fi le of the sample. The information so generated has a potential application in the identi fi cation of an authentic drug in excluding the adulterants and in maintaining the quality and consistency of the drug. HPLC fi ngerprinting
includes recording of the chromatograms, retention time of individual peaks, and the absorption spectra (recorded with a photodiode array detector) with different mobile phases. Similarly, GLC is used for generating the fi ngerprint pro fi les of volatile oils and fi xed oils of herbal drugs. Furthermore, the recent approaches of applying hyphenated chromatography and spectrometry such as high-performance liquid chromatography–diode array detection (HPLC–DAD), gas chromatography–mass spectroscopy (GC–MS), capillary electrophoresis–diode array detection (CE–DAD), high-performance liquid chromatog-raphy–mass spectroscopy (HPLC–MS), and high-performance liquid chromatography–nuclear magnetic resonance (HPLC–NMR) spectroscopy are in use to generate additional spectral informa-tion, which is very helpful for the qualitative analysis and even for the online structural eluci-dation [ 10, 11 ] .
Preparative HPLC to Isolate Therapeutic
There are basically two types of preparative HPLC. One is low-pressure (typically under 5 bar) traditional PLC (pressure liquid chroma-tography), based on the use of glass or plastic columns fi lled with low-ef fi ciency packing mate-rials of large particles and large size distribution. A more recent form PLC, preparative high-performance liquid chromatography (Prep HPLC) has been gaining popularity in pharmaceutical industry. In preparative HPLC (pressure >20 bar), larger stainless steel columns and packing materi-als (particle size 10–30 m m) are needed. The examples of normal-phase silica columns are Kromasil 10 m m, Kromasil 16 m m, and Chiralcel AS 20 m m, whereas for reverse phase are Chromasil C18, Chromasil C8, and YMC C18. The aim is to isolate or purify compounds, whereas in analytical work, the goal is to get information about the sample. Preparative HPLC is closer to analytical HPLC than traditional PLC because its higher column ef fi ciencies and faster solvent velocities permit more dif fi cult separa-tion to be conducted more quickly. In analytical HPLC, the important parameters are resolution,

12 1 Herbal Drugs: A Review on Practices
sensitivity, and fast analysis time, whereas in preparative HPLC, both the degree of solute purity as well as the amount of compound that can be produced per unit time, that is, throughput or recovery, are important. This is very important in pharmaceutical industry of today because new products (natural, synthetic) have to be intro-duced to the market as quickly as possible; using such a powerful puri fi cation technique makes it possible to spend less time on the synthesis conditions [ 10, 12 ] .
Most traditional drugs are administered as mixtures of many components, and with today’s knowledge of the many possible interactions between drugs, and between food and drugs, ethnopharmacological research deals with this aspect too. Additive, synergistic, or antagonis-tic effects are all possible. Various admixtures have also been shown to affect the bioavailabi-lity of pharmacologically active principles. Pharmacological studies of traditional herbal drugs provides clue to the isolation of active principles [ 10 ] .
Biochemical Approach
The traditional medicines, which are generally prepared by means of aqueous extracts, have hundreds of chemical compounds. Modern clinical trial proved that a complex formulation com-posed of up to 20 herbs had greater ef fi cacy than single herb used. Obviously, there exists certain relation between biological activity and chemical composition of herbal medicine, and it is called as quantitative composition–activity relationship (QCAR). Experimental studies, such as random controlled trials (RCT), often provide the most trustworthy methods for establishing causal rela-tionships from data, in which one or more vari-ables is changed (typically random) to measure its effect on other variables. In recent years, the relation between active ingredients of herbal drugs and biological activity is one type of causal rela-tionship which has been attempted. When the amount of active components in certain formula-tion varied, its therapeutic effect correspondingly changed. Thus, causal analytical methods are
employed to study the relation of chemical composition and bioactivity of herbs, which is helpful to discover active components. There are few methods available for discovering causal relationships, in which the actual process of con-trolled experiment can be stimulated through series of conditional dependence tests. A recent approach called “stepwise causal adjacent rela-tionship discovery” (STEPCARD) method has been developed to overcome the disadvantage of existing causal discovery algorithm, as well as the unreliability of traditional statistical methods, for example, stepwise regression. The main idea of STEPCARD is using conditional dependency test to determine causal adjacent relationships between explanatory variables and predictor. For a given data set containing chemical composition matrix (parameter X) and bioactivity information matrix (parameter Y), STEPCARD algorithm can be applied to choose the components or component combinations most correlative to the biological activity of original formulation (comparison drug). The computational results of STEPCARD algorithm dealing with chemical and biological data represents the minimal signi fi cant level used in conditional independent test to pick out at least one variable. But there is lack of scienti fi c approach to study correlations of their chemical constitution and pharmacological mech-anism. However, this work affords a new strategy to identify active component or component com-binations of ethnic medicine and is helpful to accelerate the speed of new drug discovery [ 13 ] .
Reverse Pharmacology
In normal drug discovery course, “laboratories to clinic” approach is followed; while for herbal medi-cine research, “clinics to laboratories” approach – a true reverse pharmacology – is followed (Table 1.4 ). The ethnomedicine is based on its use for many years, and its clinical existence is presumed. For bringing more objectivity and to con fi rm ethnic claims, systematic clinical trials are necessary. In latter, clinical experiences, observations, or available data becomes a starting point, whereas with conventional drug research, it is at the end.

13New Drug Development
Reverse pharmacology is the science of integrating documented clinical/experiential hits into leads by transdisciplinary exploratory studies and fur-ther developing these into drug candidates by experimental and clinical research. In reverse pharmacology approach process, safety remains the most important starting point, and ef fi cacy becomes a matter of validation. The scope of reverse pharmacology is to understand the mech-anisms of action at multiple levels of biological orga nization and to optimize safety, ef fi cacy, and acceptability of the leads in natural products based on relevant science [ 14 ] .
New Drug Development
Synthetic Drug Development
In synthetic drug discovery, we have to recognize an event at fi rst and the molecule as possible drug is applied, which can provide valuable insights for drug development. Historically, several such clinical hits do not often pursued quickly and rigorously by the drug discovery teams. The potential molecule, if any, as desired has to cross the long journey of about 10–15 years, to be called drug (Fig. 1.2 ) [ 14 ] .
Table 1.4 Search for new pharmacological agents; general pathways [ 14 ]
Forward pharmacology Reverse pharmacology
Compound discovered Isolate a therapeutic target
Assay for biological activity Identify a compound that affects target
Determine mechanism Modify drug to maximize effects
Demonstrate the desired biological function in vivo
Process Process 1. Cell- or physiologically directed 1. Molecular target-directed 2. Unbiased as to the compound’s mechanism of action 2. Compound has demonstrated in vitro activity 3. Must determine the mechanism of action often using
in vitro methods 3. Must demonstrate in vitro activity
4. Must demonstrate the compound acts by the proposed mechanism of action
TARGETIDENTIFICATION
LEADIDENTIFICATION
LEADOPTMIZATION
PRECLINICALSTUDIES
CLINICALTRIALS
Drug to market 10-15 years
Expensive, time consuming, numerous bottlenecks
Fig. 1.2 Synthetic route for drug discovery [ 14, 15 ]

14 1 Herbal Drugs: A Review on Practices
Modern Approach for Drug Development
Reverse pharmacology (RP) is designed to dis-cover new herbal drugs as an academic discipline to reduce three major bottlenecks of costs, time, and toxicity, major challenges associated with synthetic route. RP can be perceived to comprise of three phases: fi rst, the experiential phase that includes robust documentation of clinical obser-vations of the biodynamic effects of standardized herbal drugs by meticulous record keeping. Secondly, it includes exploratory studies for tolerance, drug interactions, dose-range fi nding in ambulant patients of de fi ned subsets of the disease, and para-clinical studies in relevant in vitro and in vivo models to evaluate the target activity. Third phase includes experimental studies, basic and clinical, at several levels of biological organization, to identify and validate the reverse pharmacological correlates of herbal drug safety and ef fi cacy. The scope of reverse pharmacology is to understand the mechanisms of action at multiple levels of biology and to optimize safety, ef fi cacy, and acceptability. In this approach, scientist travels a reverse path from “clinics to laboratory” rather than classical “laboratory to clinics” (Fig. 1.3 ), with journey of 4–5 years, as a new drug [ 14, 15 ] .
Fingerprints of Drugs: Needs and Values
In recent years, interest on plant-based drugs has increased considerably, with annual growth rate between 5 and 15 %, but the quality control and
quality assurance still remains a challenge because of the high variability of chemical com-ponents involved, which has generated a need to developed methods for fi ngerprinting. Herbal drugs, singularly and in combinations, contain a myriad of compounds in complex matrices in which no single active constituent is responsible for the overall ef fi cacy. This creates a challenge in establishing quality control standards for raw materials and standardization of fi nished herbal drugs. The main cause of confusion is language as during translating from Chinese pin-yin termi-nology into western languages or when the same name is used in different regions for different parts of the plant, or even different species or genera, for example, a problem and confusion resulting in the mistaken use of an herb in the beginning of the 1990s in Belgium. Stephania tetrandra , which is used in herbal treatment against obesity, was exchanged with Aristolochia fangchi, a herb resulting in a severe nephropathy because of the presence of aristolochic acid. Confusion probably occurred because of the sim-ilarity in the pin-yin terminology of both plants: feng fang ji vs. guang fang ji , respectively [ 11 ] .
To ease out such problems, the identity and quality can be derived from chromatographic or spectral fi ngerprints. These fi ngerprints can be de fi ned as “a chromatographic pattern of an herbal extract showing some common pharmaco-logically active and/chemical characteristic com-pounds.” The entire fi ngerprints are used as a source of information because by assaying only a number of compounds from the extract, the total intrinsic quality of the herb is not necessarily assessed. The fi ngerprint chromatograms and spectra are also accepted by the WHO as an
Reverse Pharmacology
LARGE SCALE TRIALSRELEVANTSCIENCE
SAFETYSTUDIES
PARACLINICALSTUDIES
CLINICALTRIALS
PHASE II & I
Drug to market 4-5 Years
Economic, time spring, least bottlenecks
Fig. 1.3 Modern approach for herbal drugs development [ 14, 15 ]

15Multidisciplinary Strategy to Develop Fingerprints
identi fi cation and quali fi cation technique for medicinal herbs and herbal drugs. Analysis and handling of the fi ngerprint data is an important aspect for stricter quality control to check the conscious adulterations, where another plant is sold, or to the unconscious mistaken use of “look-alikes” [ 11 ] .
The concept of phytoequivalence is in practice in order to ensure consistency of herbal products. According to this concept, a chemical pro fi le, such as chromatographic fi ngerprint, for herbal product should be constructed and compared with the pro fi le of a clinically proven reference prod-uct. Chinese State Food and Drug Administration have framed a regulation for the compositions of liquid injections with herbal ingredients using stringent quality procedures for chemical assay and standardization. Fingerprints of herbal medic-inal liquid injections are compulsorily to follow the above procedure of standardization and fi nger-prints. In addition, among the various experi-mental techniques, chromatographic methods are highly recommended for fi nding out fi ngerprints of herbal products because of the high separation ability.
Multidisciplinary Strategy to Develop Fingerprints
Modern Chemistry and Pharmacology
Herbal drugs are just considered as encapsulated dried plant material, without the quality check and/of the plant material, but it is not at all. Most of the ingredients are extracts produced from a de fi ned part of a plant and represent a large col-lection of compounds, and these compounds are responsible for the overall activity of the drug. Extracts are standardized on the basis of the con-tent of these compounds, for example, the puri fi ed fraction of opium poppy ( Papaver somniferum ), highly effective for pain and insomnia, has addic-tive nature. When it was realized, there was tension ignited between China and England in the mid-nineteenth century. Similar example may be cited that hypericin, the active compound in extracts of St John’s wort ( Hypericum perforatum ),
is used to prevent and treat some forms of depression. Standard operating procedures and raw material speci fi cation were developed to have St John’s wort extracts of de fi ned hypericin content, and consistent yield, from different batches of plant material. Despite the apparent simplicity of this botanical, a study comparing 10 products showed variations from the label claim for hypericin ranging from 22 to 140 %. Another example may be cited using ginseng products, standardized for two types of chemical moieties of active com-pounds, (1) ginsenosides and (2) eleutherosides, and are generally standardized for the total con-tent of each class of compound. Although this form of standardization provides a means of comparing products, it does not ensure that large variations do not exist within each class of com-pound that could affect the effectiveness of a preparation. Similarly, a widely advertised diet supplements from the South African plant Hoodia gordonii were found to contain no putative active ingredients and were likely derived from different plants [ 13 ] .
Standardization of herbals and herbal products refers to the production of a plant preparation that is consistent in terms of composition and ef fi cacy. The standardization processes begin with the source of the raw material and continue till the characterization of fi nished product with the same quality as drugs. The environmental condi-tions signi fi cantly affect phytochemical pro fi les and fi nally the ef fi cacy of the end product. Herbal extracts prepared by the herb of certain location can vary from year to year, as the secondary metabolite production is regulated by tempera-ture, drought, or fl ood, as well as by geographical location. Therefore, biochemical pro fi ling for each batch is used to ensure that a consistent material is being used to produce a quality material and rejection of a particular crop, also. A variety of molecular techniques including restriction fragment length polymorphism, random ampli fi cation of polymorphic DNA, and DNA sequencing are used to authenticate plant mate-rial and detect adulterant plant species. Each technique has advantages and disadvantages in terms of cost, accuracy, reproducibility, time, and taxonomic level of identi fi cation. New technologies

16 1 Herbal Drugs: A Review on Practices
and advances in molecular biochemistry have strong scienti fi c logic to prove that these tech-niques are correct for standard regulatory norms [ 13 ] .
Standardization of Fingerprints
With the awareness of side effects of synthetic drugs and rise of strains resistant to antibiotics, pharmaceutical industries are turning to plant-based drug. There is a common trend to look the chromatographic fi ngerprints for unknown herb, at the fi rst. A consistent general pro fi le is moni-tored without regard for spot/peak identity that may not be related to activity. The American Herbal Pharmacopoeia describes the use of marker compounds for characterizing products with LC and/HPTLC fi ngerprint, which is useful for establishing a baseline for speci fi city and sensitivity. Other chromatographic techniques with advantages and limitations are also in practice [ 13 ] .
Identifying active compounds in herbals is often a challenge even though the process is based on simple principles. Usually, active compounds are isolated from a complex matrix by activity-guided fractionation, which uses chromatographic techniques such as HPLC for separating compounds, followed by activity mea-surements made with an in vitro assay related to in vivo activity (e.g., measuring the inhibitory activity of aldose reductase, associated with dia-betes). The process is complicated when herbals have activity related to complex metabolic disor-ders that involve multiple metabolic pathways. Sensitive in vitro assays are essential to the pro-cess because fractionation can produce hundreds of fractions requiring testing in sub-milligram quantities. The active components may be major components of the botanical or minor compo-nents with high activity.
A major hypothetical advantage of herbals over conventional single-component drugs is the presence of multiple active compounds that together provide a potentiating effect that may not be achievable by any single compound. This advantage presents a unique challenge for the
process of activity-guided fractionation, however, because the relative activity of fractions may decrease with greater purity and may even be lost entirely. The potentiating activity of the individu-ally active components of herbals can be assessed by recombining the fractions after separation followed by con fi rmation of biological activity. The complexity of the process increases when multiple in vitro assays are used for activity-guided fractionation, each yielding a different set of active compounds. Alternatively, the interac-tions of herbal components could be negative, as in the case of the diminished bioavailability of caffeine resulting from the fl avonoids in tea [ 1 ] .
Compounds identi fi ed by activity-guided fractionation are tested in appropriate animal models to con fi rm in vivo activity. The isolation steps may involve chromatographic procedures by solvent partitioning, medium-pressure liquid chromatography, and countercurrent chromatog-raphy. Depending on the compound and informa-tion about its chemistry, it is possible to synthesize the compound also. Synthesis of the compounds may be dif fi cult and expensive yet more economical and ef fi cient than isolating a comparable amount from a plant. Pure active compounds are gener-ally obtained for testing and quality control.
Pharmacokinetics of Standardized Form
The extraction and puri fi cation process, often necessary to concentrate therapeutic ingredients to a suf fi cient level, may alter the properties, mainly as their solubility and bioavailability. The active compounds within herbal preparations are very often hydrophobic and tend to precipi-tate at high concentrations, so attempting to improve ef fi cacy by increasing concentration can be counterproductive. The use of solubilizers and bioenhancers is a logical consideration for many standardized herbals just as for drugs. A wide range of enhancers is available, each with speci fi c solubility properties. One widely used enhancer is Capmul MCM C10, a glyceryl monocaprate produced from edible fats and oils and commonly used in lip products. In a rat study examining the

17Pharmacokinetics of Standardized Form
enteric bioavailability of the antibiotic ceftriax-one, Capmul increased bioavailability by as much as 80 %. In a similar study, coenzyme Q10 was formulated with self-emulsifying drug delivery systems, which are mixtures of an oil, a surfac-tant, a co-surfactant, and the active substance used for improving the bioavailability of lipo-philic compounds. The optimized formulation doubled the bioavailability of coenzyme Q10 in dogs. A similar formulation of a lipid-based self-micro-emulsifying drug delivery system was used to enhance the bioavailability of a silymarin preparation from Silybum marianum (milk thistle) for liver disease in rabbits. Bioenhancers are effectively used for pharmaceuticals, dietary supplements, and botanicals [ 13, 16 ] .
Case Study
In a study for therapeutic herb and value addition on it using standardized extract, the ethanolic extract of Artemisia dracunculus was evaluated. Artemisia dracunculus is a potential herb for pre-venting and treating type 2 diabetes. The extract is active in both chemically induced diabetic mice
and a genetic model that develops severe type 2 diabetes. The plants used for the production of the extract were grown hydroponically. The extract was initially characterized by LC–MS with a photodiode array detector and an electron impact mass detector using spectral database matching. The chromatograms of the extract, measured at 254 nm, and the total ion current electron impact mass spectrometry (EI–MS) were determined. The crude extract was fractionated into ten simple fractions based on HPLC reten-tion. The active window was de fi ned by using activity-guided fractionation and in vitro assays such as glucose uptake into muscle cells. Because the identity of the compounds from spectral matching of chromatographic peaks was only tentative, initial standardization of the extract for scienti fi c quality control was based on the area of the most abundant peaks in the retention time period thought to contain the active compounds. Preparatory HPLC was subsequently used to isolate subfractions from the active fractions and pure compounds from the subfractions. Activity-guided fractionation and compound puri fi cation led to the identi fi cation of active compounds within the peaks (Fig. 1.4b ). Compound
0.010
a
b
20 30 40
1.0
0.0
0.2
AU
AU
Time (min.)
Fig. 1.4 Quality control assessment of Artemisia dra-cunculus plants. Shown are HPLC chromatograms mea-sured by a photodiode array detector at 254 nm from identical ethanolic extractions of plants of Artemisia dra-cunculus that were vegetative at age 6 weeks ( a ) and were
mature fl owering plants at age 17 weeks ( b ). The pro fi le of B is consistent with the pro fi le of the reference extract, whereas the pro fi le of A contains both quantitative and qualitative differences, making it unacceptable as material for production [ 13 ]

18 1 Herbal Drugs: A Review on Practices
identi fi cation was con fi rmed with the use of com-mercial standards, mass fragmentation pattern libraries, or a combination of LC–MS, LC–MS/MS, and NMR. The abundance of these com-pounds is used for direct standardization of the extract in addition to ultraviolet spectra, thereby decreasing the likelihood that unknown compounds can interfere with the analysis. Electrospray ionization, a sensitive detection method, was used to enhance the level of standardization by con fi rming the molecular weights of the active compounds and providing additional chemical information about active compounds. Assays were then used to validate the activity component of the standardization process. Hence, this is an example of a standardization technique that has evolved together with the development of the herbal drug [ 13 ] .
Development of standardized method to prepare Artemisia dracunculus extract. (A) Photodiode array detection at 254 nm from HPLC separation provides a sensitive pro fi le of the extract that was used for general fi ngerprinting. (B) LC-electron-impact (EI)–MS analysis of the extract provides both qualitative and quantitative data for the com-ponents and provides partial or complete com-pound identi fi cation, especially when con fi rmed by comparison with chemical standards and other spectroscopy techniques such as NMR. Compounds identi fi ed in B are 1-6-demethoxy-capillarisin, 2-davidigenin, 3-sakuranetin, 4-2, 4-dihydroxy-4-methoxydihydrochalcone, and 5-2, 4-dihydroxy-4-methoxy-di-hydrochalcone. Further, the LC–MS-electrospray ionization (ESI) analysis of the extract provides sensitive and quantitative selected ion chromatograms speci fi c for the molecular weights of the com-pounds of interest (M-H for negative ESI), validating the other chromatographic techniques as well as the ability to detect compounds that may not be detectable by other means (e.g., compound with m / z 515)
Multi-herbal preparations are a rich resource with a potential as future ingredients in herbal dietary supplements. Scienti fi c validation of herbal therapeutics is necessary to ensure consistent results between research studies and herbal prod-ucts. Although many challenges exist at every
level of development, the identity of the active compounds and the validation of their ef fi cacy will be a requisite for the quality control and standardization of herbal drugs. Patenting of drugs derived from indigenous systems of medicine has started to take epidemic proportions. The current value of the world market for medic-inal plants from leads given by indigenous and local communities is estimated to be $43 billion. Using traditional knowledge increased the ef fi ciency of screening plants for medical proper-ties by more than 400%. The failures and non-sustainability of the chemical route to agriculture and health care provide an opportunity to reeval-uate traditional knowledge systems and move from the false hierarchy of these systems to a plurality. Such a pluralistic view of knowledge systems will imply respect for the different sys-tems in their own logic and in their own episte-mological foundations. It will also mean that one system does not have to serve as the measure of scienti fi c adequacy for all systems and diverse systems do not need to be reduced to the language and logic of dominating knowledge systems. Evidence-based herbal drugs have a universal acceptability [ 13 ] .
Commercial Manufacturing and Quality Control
The term “standardized herbal extract” deciphers the extract for free from any potentially hazard-ous chemical manufactured by raw plant materi-als obtained from plants that are cultivated speci fi cally for producing the extract or are obtained as a by-product from the production of another product, or are collected from the wild, for example, ginseng is grown speci fi cally for the production of related extract, whereas grape seed extract is a by-product of the commercial wine-making industry. Herbals have been collected as they grow in their native environments, but this practice raises concerns about the consistency of end products and is considered an irresponsible collection technique that can lead to environmental destruction and the endangerment of species when not restricted to research purposes.

19Regulatory Norms for Herbal Drugs
Plants grown speci fi cally for the production of speci fi c extract for basic research are ideally sourced from a characterized and uniform genetic material with a taxonomic record of the genus, species, and cultivar or other additional identi fi ers. Records are maintained for the source of the seed, locations and conditions of cultivation, and exposure to possible chemical treatments such as pesticides. Ideally, herbals are cultivated under controlled conditions such as hydroponics within climate-controlled green-houses yielding consistent plant material. Only with tight control over the entire process of herbals production can seed-to-pill standardiza-tion be achieved. When source plants are pro-cured in various regions of the world, records of plant identi fi cation, maintenance of voucher specimens, and biochemical pro fi ling may suf fi ce. Raw materials from international sources also be carefully monitored for contamination from a variety of sources including co-harvested weed plants, toxic phytochemicals, and heavy metals. Plants that were not directly treated with pesticides can become contaminated by chemi-cal drift. Depending on the formulation, humid-ity, and temperature, pesticides can drift from the site of intended application by as much as 4.8 km (3 miles) [ 12, 17– 19 ] .
Regulatory Norms for Herbal Drugs
The increasing acceptance of herbals as drug has alarmed the regulating authorities globally. The speculators and opportunist are under scan using the different norms by each country; a few are as below:
The Therapeutic Goods Act
In Australia, the “Therapeutic Goods Act 1989,” sets out the legal requirements for the import, export, manufacture, and supply. It has details of the requirements for listing or registering all ther-apeutic goods in the Australian Register of Therapeutic Goods (ARTG), as well as many other aspects of the law including advertising,
labeling, and product appearance. Australian manufacturers of therapeutic goods must be licensed, and their manufacturing processes must comply with the principles of GMP. All medicines manufactured for supply in Australia must be listed or registered in the ARTG, unless they are speci fi cally exempt or excluded. Listed medicines are considered to be of lower risk than registered medicines. Most complementary medicines (e.g., herbal, vitamin, and mineral products) are exam-ples of listed products. Medicines assessed as having a higher level of risk must be registered (not listed). Registered medicines include non-prescription (low-risk, OTC) medicines and pre-scription (high-risk) medicines. Complementary medicines (also known as “traditional” or “alter-native” medicines) include vitamin, mineral, herbal, aromatherapy, and homeopathic products. Complementary medicines may be either listed or registered, depending on their ingredients and the claims made. Most complementary medicines are listed in the ARTG, and some are registered (Therapeutics Good Administration, 1999). In New Zealand, supplements in the market are largely manufactured in the USA, follow the TGA, but regulations are not restric-tive, and there are no limits on ingredients or potencies, and structure/function claims are allowed [ 20 ] .
Drug Administration Law
In China, many herbal drugs have been used for hundreds of years, and it is assumed in many cases that they must work, for example, about 7,000 species of plants are used in China as herbal drugs, but only 230 are most common, with in-depth pharmacological, analytical, and clinical studies. The 2000 edition of the Chinese Pharmacopoeia included 784 items on TCM and 509 on Chinese patent medicines. Herbal medi-cines in China are normally considered as medic-inal products with special requirements for marketing. New drugs have to be investigated and approved according to the drug administra-tion law. New traditional Chinese medicines are classi fi ed under fi ve categories based on the

20 1 Herbal Drugs: A Review on Practices
amendment and supplement regulation of approval of new traditional medicines [ 20 ] :
Class 1 1. Arti fi cial alternatives of Chinese crude drugs 2. Newly discovered Chinese crude drugs and
their preparations 3. Active constituents extracted from Chinese
crude drugs and their preparations 4. Active constituents extracted from a composite
formulation of traditional Chinese medicines
Class 2 1. Injection of traditional Chinese medicines 2. Use of new medicinal parts of Chinese crude
drugs and their preparations 3. Effective fractions extracted from Chinese
crude drugs or natural drugs and their preparations
4. Chinese crude drugs arti fi cially developed in an animal body and their preparations
5. Effective fractions extracted from a composite formulation
Class 3 1. New composite formulations of traditional
Chinese medicines. 2. Composite preparations of traditional Chinese
medicines and chemical drugs with the main ef fi cacy due to the traditional Chinese medicine.
3. Domestically cultivated or bred crude drugs originally imported and commonly used in China, and their preparations.
Class 4 1. Preparation with a change of dosage form or
route of administration. 2. Botanical crude drugs acclimatized from their
origin or crude drugs from a domesticated wild animal in China.
Class 5 In 1995, the preparatory committee on Chinese
medicines was formed to manage the imple-mentation of these recommendations; as a result, 31 potent Chinese medicines that may potentially cause adverse effects have been
identi fi ed. Proprietary preparations containing a combination of herbal ingredients and conventional drugs are regulated in the same manner as other conventional drugs. The majority of suppliers are state-owned or state-connected. The pharmacopoeial TCM allows the parallel manufacturing and sale of both pharmaceutical drugs and traditional herbal at a point also.
Ayush
For traditional medicines in India, an authorized body Ayush has adopted strict guidelines for all herbal drugs (related to Ayurveda, Yoga, Unani, Siddha, and Homeopathy) to be exported from India [ 14 ] . With respect to this, Department of AYUSH Govt. of India gave some parameters for Drug Development, Standardization & Quality of Ayurveda, Siddha, and Unani drugs, which include fi ve protocols as [ 21 ] : Protocol-I: Standardization of single plant
material Protocol-II: SOP of preparation of extracts Protocol-III: Standardization of plant extract Protocol-IV: SOP of fi nished product Protocol-V: Standardization of formulations
These protocols based on most common parameters such as morphological evaluation, microscopic evaluation, physicochemical evalua-tion, particle size, bulk density and tap density (in case of powder crude drugs or powder formu-lations), and assay for constituents (marker %, major compounds like alkaloids, glycosides, fl avonoids/saponin). With respect to above parameters are test for heavy/toxic metals (lead, cadmium, mercury, and arsenic), microbial con-tamination (total viable aerobic count, total Enterobacteriaceae, and total fungal count), test for speci fi c pathogen ( E. coli , Salmonella spp., S. Aureus, Pseudomonas aeruginosa ), pesticide residue (DDT, HCH, endosulfan, aldrin, mala-thion, and parathion), test for a fl atoxine (B
1 , B
2 ,
G 1 , G
2 ), and chelating agent (for Bhasma, Lepa,
Aswarista, etc.). Further stability assessment and self life, safety assessment, documentation of safety based on experience or toxicological studies,
21Regulatory Norms for Herbal Drugs
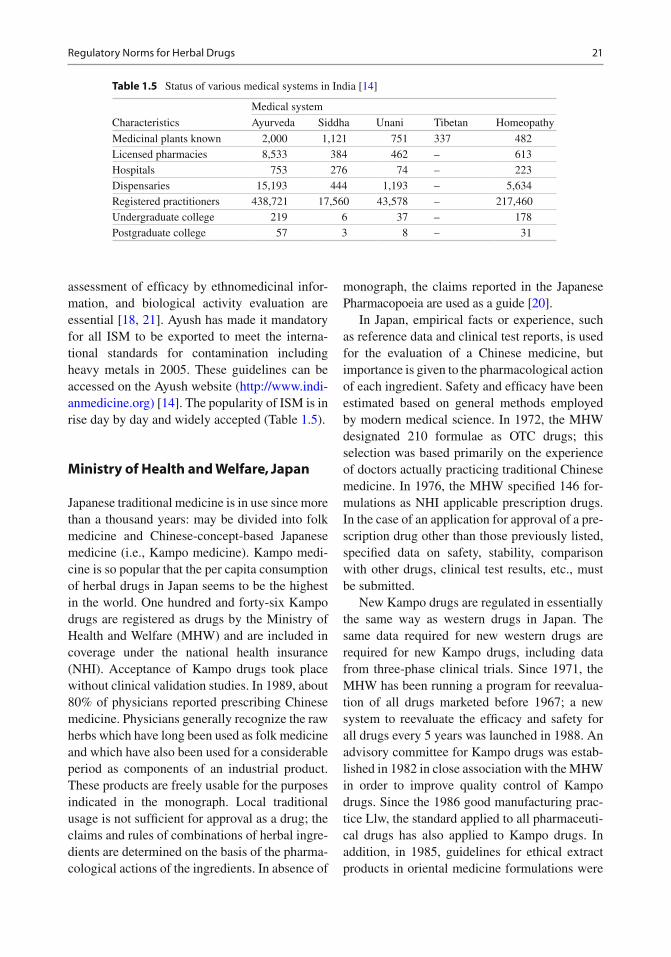
assessment of ef fi cacy by ethnomedicinal infor-mation, and biological activity evaluation are essential [ 18, 21 ] . Ayush has made it mandatory for all ISM to be exported to meet the interna-tional standards for contamination including heavy metals in 2005. These guidelines can be accessed on the Ayush website ( http://www.indi-anmedicine.org) [ 14 ] . The popularity of ISM is in rise day by day and widely accepted (Table 1.5 ).
Ministry of Health and Welfare, Japan
Japanese traditional medicine is in use since more than a thousand years: may be divided into folk medicine and Chinese-concept-based Japanese medicine (i.e., Kampo medicine). Kampo medi-cine is so popular that the per capita consumption of herbal drugs in Japan seems to be the highest in the world. One hundred and forty-six Kampo drugs are registered as drugs by the Ministry of Health and Welfare (MHW) and are included in coverage under the national health insurance (NHI). Acceptance of Kampo drugs took place without clinical validation studies. In 1989, about 80% of physicians reported prescribing Chinese medicine. Physicians generally recognize the raw herbs which have long been used as folk medicine and which have also been used for a considerable period as components of an industrial product. These products are freely usable for the purposes indicated in the monograph. Local traditional usage is not suf fi cient for approval as a drug; the claims and rules of combinations of herbal ingre-dients are determined on the basis of the pharma-cological actions of the ingredients. In absence of
monograph, the claims reported in the Japanese Pharmacopoeia are used as a guide [ 20 ] .
In Japan, empirical facts or experience, such as reference data and clinical test reports, is used for the evaluation of a Chinese medicine, but importance is given to the pharmacological action of each ingredient. Safety and ef fi cacy have been estimated based on general methods employed by modern medical science. In 1972, the MHW designated 210 formulae as OTC drugs; this selection was based primarily on the experience of doctors actually practicing traditional Chinese medicine. In 1976, the MHW speci fi ed 146 for-mulations as NHI applicable prescription drugs. In the case of an application for approval of a pre-scription drug other than those previously listed, speci fi ed data on safety, stability, comparison with other drugs, clinical test results, etc., must be submitted.
New Kampo drugs are regulated in essentially the same way as western drugs in Japan. The same data required for new western drugs are required for new Kampo drugs, including data from three-phase clinical trials. Since 1971, the MHW has been running a program for reevalua-tion of all drugs marketed before 1967; a new system to reevaluate the ef fi cacy and safety for all drugs every 5 years was launched in 1988. An advisory committee for Kampo drugs was estab-lished in 1982 in close association with the MHW in order to improve quality control of Kampo drugs. Since the 1986 good manufacturing prac-tice Llw, the standard applied to all pharmaceuti-cal drugs has also applied to Kampo drugs. In addition, in 1985, guidelines for ethical extract products in oriental medicine formulations were
Table 1.5 Status of various medical systems in India [ 14 ]
Medical system
Characteristics Ayurveda Siddha Unani Tibetan Homeopathy
Medicinal plants known 2,000 1,121 751 337 482 Licensed pharmacies 8,533 384 462 – 613 Hospitals 753 276 74 – 223 Dispensaries 15,193 444 1,193 – 5,634 Registered practitioners 438,721 17,560 43,578 – 217,460 Undergraduate college 219 6 37 – 178 Postgraduate college 57 3 8 – 31

22 1 Herbal Drugs: A Review on Practices
developed. The MHW has three major systems for collection of adverse reaction data. The fi rst is a voluntary system involving 2,915 monitoring hospitals. The second system, the pharmacy monitoring system, which includes 2,733 phar-macies, collects data on cases [ 20 ] .
Ministry of Health, Saudi Arabia
In Saudi Arabia, registration of medicinal prod-ucts by the ministry of health is obligatory for any ingredient having medicinal effects such as herbal preparations, health and supplementary food, medicated cosmetics, antiseptics, or medical devices [ 20 ] .
A few important organizations known for strict regulations related to herbal drugs are as per Table 1.6 [ 19 ] have guidelines for safe use of herbal drugs.
WHO Guidelines for Assessment of Herbal Drugs
The WHO has recently de fi ned traditional medi-cine as comprising therapeutic practices that have been in existence, often for hundreds of years,
before the development and spread of modern medicine and are still in use today. As per WHO, every herbal formulation must be standardized. WHO collaborates and assists health ministries in establishing mechanisms for the introduction of traditional plant drugs into primary healthcare programs, in assessing safety and ef fi cacy, and in ensuring adequate supplies and the quality control of raw and processed materials. According to WHO guidelines, less stringent selection proce-dures could be applied for the screening, chemical analyses, clinical trials, and regulatory measures, but the procedure for pure phytochemicals for quality control should be identical to that for syn-thetic drugs according to WHO guidelines. The traditional preparations comprise medicinal plants, minerals, organic matter, etc. Some of the important parameters are stability testing, safety assessment, speci fi c therapeutic activity analysis, and estimation of the active constituents in plant raw material and fi nished products. The objective of WHO guidelines is to de fi ne basic criteria for the evaluation of quality, safety, and ef fi cacy of herbal drugs and therefore to assist national regu-latory authorities, scienti fi c organizations, and manufacturers to undertake an assessment of the documentation/submission/dossiers in respect of such products. The manufacturing procedure and
Table 1.6 Different national regulatory authorities and guidelines [ 19 ]
S. no. Country Regulatory authority Guidelines
1 Australia Australian Department of Health Guidelines for preparation and presentation of applications for investigational drug and drug products
2 Canada Health Protection Board Preclinical toxicology guidelines 3 European Union Committee for Proprietary
Medicinal Products Recommendation for the development of nonclinical testing strategies
4 France Ministry of Public Health and Social Security
Guidelines for analytical, pharmacological, and toxicological testing of pharmaceuticals
5 India Directorate General of Health Services
Drug and cosmetic rules
6 Japan Ministry of Health and Welfare Guidelines for toxicity studies of drugs 7 Nordic countries Nordic Council on Medicines Guidelines for registration of new drugs 8 UK Department of Health and Social
Security Guidance notes on application for product licenses
9 USA Food and Drug Administration Guidelines for assessment of drugs and medical device, safety in animals (issued by PMA, prepare in conjugation with FDA)

23Regulatory Norms for Herbal Drugs
formula including the amount of excipients should be described in detail. A method of identi fi cation, and quanti fi cation, if applicable, of the plant material in the fi nished product should be de fi ned. If the identi fi cation of an active prin-ciple is not possible, it should be suf fi cient to identify a characteristic substance or mixture of substances (e.g., chromatographic fi ngerprint) to ensure consistent quality of the product. According to WHO, “herbal drugs” should be regarded as fi nished, labeled medicinal products that contain as active ingredients aerial or under-ground parts of plants or other plant material, or combinations thereof, whether in the crude state or as plant preparations. Plant material includes juices, gums, fatty oils, essential oils, and any other substance of this nature. Herbal medicines may contain excipients in addition to the active ingredients. Drugs containing plant material combined with chemically de fi ned active sub-stances, including chemically de fi ned, isolated constituents of plants, are not considered to be herbal medicines. Exceptionally, in some coun-tries, herbal drugs may also contain, by tradition, natural organic or inorganic active ingredients which are not of plant origin. Multicomponent herbal formulations can be standardized with newer techniques such as DNA fi ngerprinting, HPTLC, liquid chromatography, and mass spec-troscopy. The value of animal testing to establish safety and toxicity is not so critical if the herbs are used in traditional forms. Nevertheless, all the critical pharmacopoeial tests such as dissolution time, microbial, pesticide, and heavy metals con-tamination must be in accordance with global standards, and all the Ayurvedic medicine manu-facture must be in accordance with current good manufacturing procedures for herbs [ 20 ] .
Analysis of Raw Herb Raw material can be de fi ned as starting material or any intermediate which will be utilized for further processing. Before fi nished pharmaceutical dosage forms are produced, the identity, purity, and quality of raw materials as per speci fi cations for impurities and other related substances present must be established with use of suitable test methods. Pharmacopoeias and formularies of
various countries provide standardized test methods for the most common and widely used materials in their monographs. Stored drug samples are prone to attack by harmful mycotoxin-producing fungi. Detection of mycotoxins (a fl atoxin B, acliratoxin, citrinin, and zearalenone) is certainly a matter of great concern in stored drugs of important medicinal plants, for example, fruits of Emblica of fi cinalis (1.51 m g/g); Terminalia chebula (1.19 m g/g) have developed an HPTLC method for the detection of a fl atoxins B
1 , B
2 , G
1 ,
and G 2 from herbal raw materials and estimated
the production of a fl atoxins in caffeinated and decaffeinated tea samples. Studies revealed that caffeine acts as a good inhibitor for the growth of a fl atoxins in stored drugs [ 20 ] .
Quality Control Techniques as per WHO A lot of analytical techniques have been devel-oped for renewed for quality control of drugs from plant origin. The quality control step is for selecting targets to assess authenticity and inherent quality, but many traditional drugs are claimed to exert their effects because each type of chemical compound present many have a different activity and then seem of all of these may modify the action of the major active component. Chromatographic fi ngerprinting emphasizes an integral formulation of pharmaco-logically active and phytopharmaceutically char-acteristic components of samples with similar or different attributions. This technique can be used for the assessment of quality consistency and sta-bility of herbal extracts or products by visible observation and comparison of the standardized fi ngerprint pattern. Fingerprinting of the herbals is done by HPLC, HPTLC, MS, LC–MS [ 1 ] , H–NMR, etc. Apart from this, there are some methods to evaluate the fi ngerprint quality of herbal materials or pharmaceutical products, such as correlative chromatography, comparative analysis, wavelet analysis, and arti fi cial neural networks (ANN) [ 20 ] .
Evaluation of plant materials and their derived products has always been an important part of the professional expertise of a pharmacognosist. However, over the years the nature and degree of this evaluation have changed. Initially, it was

24 1 Herbal Drugs: A Review on Practices
considered suf fi cient to authenticate the plant material by comparison with a standard botanical description or monograph. Later, it was realized that, for detection of adulterants, this practice must be supplemented with other important pro-cedures like microscopy, chemical tests, and advanced analytical techniques. The main goal of pharmacognosy is to assess the value of raw materials and to ensure that the fi nal product is of the required standard. Strict standardization procedures and pharmacognostical studies of medicinal plants reduce drastically much of the accidents in wrong prescriptions of traditional herbal drugs, where a plant can be differentiated. The use of herbal drugs is growing steadily, particularly for the treatment of asthma and aller-gic diseases, as health supplements and tonics. Numerous reports on the presence of heavy metals in herbal drugs are being presented regularly. Federal agencies have put in a lot of efforts to regulate the use of herbal drugs; nevertheless, the situation is worse in developing and underdevel-oped countries. Some of the crucial discoveries in the safe use of herbal drugs were brought out through intensive pharmacognostical research, so need of hi-tech fi ngerprints is stressed by regula-tory authorities.
References
1. Venkatesh V. Medicinal plant scenario in India. Bangalore: Foundation for Revitalization of Local Health Traditions; 2002.
2. Li L. Opportunity and challenge of traditional Chinese medicine in face of the entrance to WTO (World Trade Organization). Chin Inform Tradit Chin Med. 2000;7:7–8 (in Chinese).
3. Reninger E. TCM (Traditional Chinese Medicine) and fi ve element styles of practice. 2011. http://taoism.about.com/od/qigongchinesemedicine/a/TCM.htm . Accessed 7 Sept 2011.
4. Saito H. Regulation of herbal medicines in Japan. Pharmacol Regul. 2000;41:515–9.
5. Shastri P K. Charak Samhita. 2nd ed., (Chaukhamba Sanskrit Sansthan, Varanasi, Edited by Ganga Sahay Pande). 1983;Sloka number 39, p. 7.
6. Shastri P K. Charak Samhita. 2nd ed., (Chaukhamba Sanskrit Sansthan, Varanasi, Edited by Ganga Sahay Pande). 1983;Sloka number 39, p. 14.
7. Tulshidas. Ramcharitmanas, Lanka Kand. (Published by Gita Press Gorakhpur, India) p. 809.
8. Tulshidas. Ramcharitmanas, Lanka Kand. (Published by Gita Press Gorakhpur, India) p. 811.
9. Bulpitt CJ. The uses and misuses of orchids in medi-cine. Q J Med. 2005;98:625–31.
10. Patil PS, Shettigar R. An advancement of analytical techniques in herbal research. J Adv Sci Res. 2010;1(1):08–14.
11. Heyden YV. Extracting information from chromato-graphic herbal fi ngerprints. LCGC Europe. 2008;21(9): also available at http://chromatographyonline. fi ndanalytichem.com/lcgc/Column%3A+Practical+Data+Handling/Extracting-Information-from-Chromatographic-Herbal/ArticleStandard/Article/detail/565826?contextCategoryId=47195 . Accessed 8 Aug 2011.
12. Mukherjee PK, Ponnusankar S, Venkatesh M. Ethno medicine in complementary therapeutics. In: Ethnomedicine: a source of complementary therapeu-tics. Trivandrum: Research Signpost; 2010. p. 29–52.
13. Ribnicky DM, Poulev A, Schmidt B, Cefalu WT, Raskin I. Evaluation of botanicals for improving human health. Am J Clin Nutr. 2008;87(2):472S–5S.
14. Joshi DD, Sharma RK. Herbal drugs in patent regime. Saarbrü cken: VDM Publisher; 2011. p. 23–40. p. 69–70. ISBN ISBN-13: 978-3639321821.
15. Patwardhan B, Vaidya ADB, Chorghade M, Joshi SP. Reverse pharmacology and systems: approaches for drug discovery and development. Curr Bioact Compd. 2008;4:201–12.
16. Lazo JS. Rear-view mirror and crystal balls: a brief re fl ection on drug discovery. Mol Interv. 2008;8(2):60–3. Speaking of Pharmacology. Editorial.
17. Giri L, Andola HC, Purohit VK, Rawat MSM, Rawal RS, Bhatt ID. Chromatographic and spectral fi ngerprinting standardization of traditional medicines: an overview as modern tools. Res J Phytochem. 2010;4:234–41.
18. Morgan K. Medicine of the gods: basic principles of Ayurvedic medicine. 2002. [ http://www.compulink.co.uk/~mandrake/ayurveda.htm ].
19. Rath SK, Sharma S, Srivastava S. Regulatory toxicology for pharmaceuticals. CRIPS. 2001;2(2):2–9.
20. IARC Monograph. Some traditional herbal medicines. Vol. 82. p. 43–67.
21. Patra KC, Parta SK, Harwansh RK, Kumar KJ. Traditional approaches towards standardization of herbal medicines: a review. J Pharm Sci Technol. 2010;2(11):372–9.
Bibliography
Andola HC, Gaira KS, Rawal RS, Rawat MSM, Bhatt ID. Habitat dependent variations in berberine content of Berberis asiatica Roxb. Ex DC in Kumaun, West Himalaya. Chem Biodivers. 2010;7:415–20.
Andola HC, Rawal RS, Rawat MSM, Bhatt ID, Purohit VK. Analysis of berberine content using HPTLC fi ngerprinting of root and bark of three Himalayan Berberis species. Asian J Biotechnol. 2010;2:239–45.

25Bibliography
Gong F, Wang BT, Chau FT, Liang YZ. Data preprocessing for chromatographic fi ngerprint of herbal medicine with chemometric approaches. Anal Lett. 2005;38:2475–92.
Guo FQ, Liang YZ, Xu CJ, Li XN, Huang LF. Analyzing of the volatile chemical constituents in Artemisia capillaris herba by GC-MS and correlative chemometric resolu-tion methods. J Pharm Biomed Anal. 2004;35:469–78.
Joshi DD, Uniyal RC. Different chemo-types of Gokhru (Tribulus terrestris) : a herb used for improving phy-sique and physical performance. Int J Green Pharm. 2008;2(3):138–41.
Joshi DD, Kharkwal H. Commercial manufacturing of herbal medicines: recent trends to select suitable chemo-types as raw herb. Indo Italian workshop on bacteria and fungi for environmental sustainability. 2010. p. 79–81.
Kala CP. Health traditions of Buddhist community and role of Amchis in trans-Himalayan region of India. Curr Sci. 2005;89(8):1331–8.
Li L. Opportunity and challenge of traditional Chinese medicine in face of the entrance to WTO (World Trade Organization). Chin Inform Tradit Chin Med. 2000;7:7–8 (in Chinese).
Meester FD, Waston RR. Wild type food in health promo-tion and disease prevention. Totowa: Humana Press Inc; 2009.
Ran XR, Yang HH, Liang QL, Chen J, Wang YM, Luo GA, Li P, Li KM, Chen YW. Difference analysis of mass spectra and its application to research of Chinese multiherb remedy. Gaodeng Xuexiao Huaxue Yanjiu. 2007;2:250–3.
Sagar Bhanu PS, Zafar R, Panwar R. Herbal drug stan-dardization. Indian Pharm. 2005;4(35):19–22.
Wohlmuth H, Penman KG, Pearson T, Lehmann RP. Pharmacognosy and chemo-types of passion fl ower ( Passi fl ora incarnata ). Biol Pharma Bull. 2010;33(6):1015–8.
Xie PS. Discussion of the present situations, development and problems of fi ngerprint of Chinese medicines. Zhongyaocai. 2007;3:257–9.
Ye M, Han J, Chen HB, Zheng JH, Guo DA. Analysis of phenolic compounds in rhubarbs using liquid chroma-tography coupled with electrospray ionization mass spectrometry. J Am Soc Mass Spectrom. 2007;18:82–91.