hepatitis c antibody profile and viraemia prevalence in adults with severe haemophilia
TRANSCRIPT

British Journal o/ Haematofogu. 199 1, 79, 5 1 2- 5 1 5
RAPID PAPER
Hepatitis C antibody profile and viraemia prevalence in adults with severe haemophilia
R. s. TEDDER, M. BRIGGS, c. RING, P. w. TUKE, P. JONES,* G. F. s A V I D G E , t B. RODGERSS A N D I . A. GARSON Division of Virology, Department of Medical Microbiology, University College and Middlesex School of Medicine, London, *Northern Regional Haemophilia Service, The Royal Victoria Infirmary, Newcastle upon Tyne, tHaemophilia Centre, S t Thomas’ Hospital. London, and $ Wellcome Diagnostics, Beckenham, Kent
Received 16 July 1991; acceptedfor publication 9 August 1991
Summary, Sera from 21 patients who had received large amounts of unheated factor VIII concentrate were tested for antibodies to the hepatitis C virus (HCV) by both commercial (Ortho C100) and ‘in house’ ELISAs. ‘In house’ assays utilized recombinant structural (core) or non-structural (replicase) HCV proteins generated by a baculovirus expression system. Antibodies to HCV were detected in 100% of the sera by the core protein based ELISA but in only 62% and 19% by the C100 and replicase based ELISAs, respectively. Hepatitis C
viraemia was demonstrated in 90% of the patients by in vitro amplification of the 5’ non-coding region of the HCV genome. Amplification with primer sets from two other regions of the genome proved less efficient a t detecting viraemia. We conclude that the prevalance of hepatitis C infection in haemophiliacs may have been underestimated previously and that almost all HCV-infected patients have evidence of on-going viral replication.
Chronic liver disease is increasingly recognized as a signifi- cant cause of morbidity and mortality in patients with haemophilia (Eyster et a / . 1985). Before the introduction of heat treatment of clotting factor concentrates in the mid 1980s almost all patients who received factor VIII concen- trate for the first time acquired non-A, non-B hepatitis (NANBH) (Fletcher et a / . 1983). Approximately 70% of these developed chronic liver enzyme abnormalities (Cederbaum et a / , 1982) and at least 20% of patients progressed to cirrhosis, in some cases in as little as 5 years (Triger & Preston, 1990).
The nature of the infectious agent responsible for NANBH remained unknown until the identification of the hepatitis C virus (HCV) genome by Choo et a/ (1989). Serological studies based on the detection of antibodies to C100, a recombinant non-structural HCV protein (Kuo et al. 1989). revealed that many haemophiliacs have been exposed to the virus. Esti- mates of the seroprevalence of an t i41 00 among patients regularly receiving factor VIII concentrates vary consider- ably from study to study, although most estimates fall within the 55-85% range (Esteban et al. 1989: Noel et a / . 1989: Koggendorf et al. 1989: Ludlam et a / . 1989; Makris et a / , 1990). However, the extent to which the anti-Cl00 in haemophilic sera represents active HCV infection, rather than merely indicating previous exposure to the virus, is unknown, as is the accuracy with which various serological assays identify infected patients. Correspondence: llr J. A Carson, Division of Virology, Department of Medical Microbiology, UCMSM, School of Pathology, 67 Ridinghouse Street. London W1 P 7PN.
In the present study we address these questions by investigating, in a group of patients who have received large amounts of unheated factor VIII concentrate. the relation- ship between the presence of antibodies to various HCV proteins and the presence of the virus itself. In the absence of any culture system or antigen assay for HCV we have resorted to viral genome detection using a polymerase chain reaction (PCR) assay which has been shown to be capable of detecting the virus in both serum samples and factor VIII concentrates (Garson et al, 1990a. d).
MATERIALS AND METHODS
Patients. Serum samples were obtained from 21 adult males attending the haemophilia centres a t St Thomas’ Hospital, London, and The Royal Victoria Infirmary, New- castle. One of the patients had von Willebrand’s disease, the others had haemophilia A. All had received repeated infu- sions of unheated commercial factor VIII concentrate over a period of many years. Details of diagnosis, treatment history, hepatitis B virus (HBV) and human immunodeficiency virus (HIV) serology, and transaminase levels are given in Table I. Thirty control sera were obtained from routine donors attending the North London Blood Transfusion Centre. All sera were stored at - 20°C prior to testing.
Serology. Three immunoassays for antibodies to HCV proteins were employed. ( i ) A commercial ‘first generation’ test (Ortho Diagnostic Systems) using the C100 protein as antigenic substrate. C100 is a yeast-expressed recombinant
512
HCV Antibodies and Viraernia in Haernophilia 5 1 3 Table 1. Clinical, serological and biochemical data summary
Age Patient (yr)
1 37 2' 34 3 2 5 4 26 5 34 6 28 7 3 1 8 61 9 40
10 24 1 1 29 12 40 I 3 42 14 2 0 15 3 1 I 0 3 3 17 40 I X 3 0 19 49 20 24 21 22
F.vw level Treatment (%) duration
< 1 Lifetime 27 12 years
3 . 5 Lifetime < 1 Lifetime < 1 Lifetime
0 Lifetime 0 Lifetime
< 1 Lifetime 0 Lifetime 1.6 Lifetime 0 Lifetime 0 Lifetime
< 1 Lifetime < 1 Lifetime
7 Lifetime < 1 Lifetime < 1 Lifetime < I Lifetime < 1 Lifetime < 1 Lifetime < 1 Lifetime
Quantity HBV past year (K) HIV HBc sAg LFTs
3 64 + - 20
8 -
228 + 3 1 + 64 +
377 + 66 +
121 + 21 + 23 + 36 + 22 + 25 + 52 + 43 + 81 + 1 5 + 64 + 1 5 + 45 +
2 4 . 4 4 157, N A
43 ,51 43.242 33 .46 89, 196
119.85 4 6 , 4 6 94.274
127, 125 49, 38 26. 3 1 10. 17 79 .79 26. 1 5 3 1 . 3 0 14 .23 55.28 81 ,114 3 3 , 3 0
727.448
F.VIII = factor VIII: Quantity past year=quantity of factor VlII received over the previous year: K = 1000 units of factor VIII: HIV = human immunodeficiency virus antibody status: HHV= hepatitis I3 virus serology: HBc=antibody to HUV core: sAg= hepatitis B surface antigen: LFTs = last two liver function test results. for patients 1-1 2 alanine aminotransfer- ase was measured (upper limit of normal 40 l t l / l ) , for patients 1 3-2 1 aspartate transaminase was measured (upper limit of normal 37 IUj l ) , bold figures denote abnormal values; *This patient had von Willehrand's disease: t e antigen negative. anti-e positive.
0 I 2 3 4 5 6 I 8 9 10 K b
NS2 NS3 NS4 NS5
p E q cDNA clones
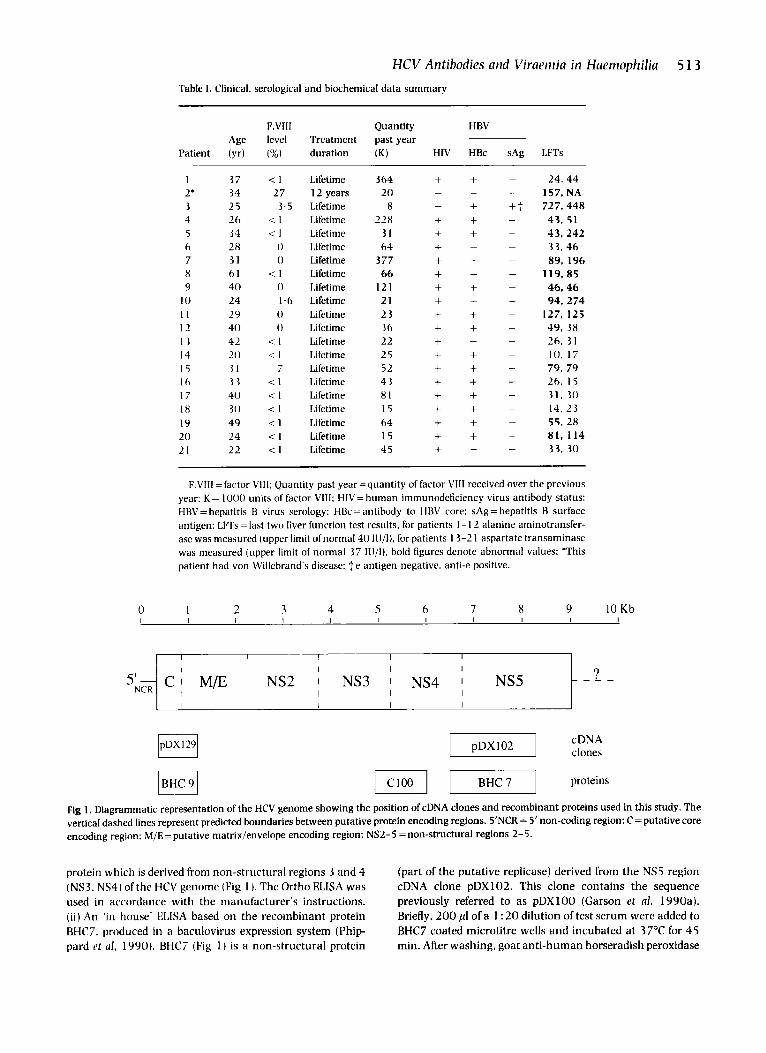
Fig 1 , Diagrammatic representation of the HCV genome showing the position of cDNA clones and recombinant proteins used in this study. The vertical dashed lines represent predicted houndaries between putative protein encoding regions. 5'NCR = 5' non-coding region: C = putative core encoding region: M/E= putative matrix/envelope encoding region; NS2-5 = non-structural regions 2-5.
protein which is derived from non-structural regions 3 and 4 (NS3. NS4) of the HCV genome (Fig 1 ). The Ortho ELISA was used in accordance with the manufacturer's instructions. (ii) An 'in house' ELISA based on the recombinant protein BHC7. produced in a baculovirus expression system (Phip- pard rt ul. 1990) . BHC7 (Fig 1 ) is a non-structural protein
(part of the putative replicase) derived from the NS5 region cDNA clone pDX102. This clone contains the sequence previously referred to as pDXl00 (Garson et al. 1990a) . Briefly, 200 pI of a 1 : 20 dilution of test serum were added to BHC7 coated microtitre wells and incubated at 37OC for 45 min. After washing, goat anti-human horseradish peroxidase

5 14 R. S. Tedder et al conjugate was added and incubated at 37°C for 3 0 min; bound conjugate was detected with tetramethyl benzidine. The cut-off value was calculated as the mean absorbance (A) of four negative controls plus 0.2 A units. (iii) An ‘in house’ ELISA based on the baculovirus-expressed recombinant protein BHC9 (Fig 1). BHC9 is a structural protein (putative core) derived from a 0.84 kb cDNA clone designated pDX129 (Phippard et al, 1990). The assay protocol was exactly as described above but using BHC9 coated microtitre wells.
Polymerase chuin reaction. HCV-RNA was detected in serum by nested PCR as previously described (Garson et a/ . 1990b) but using random hexamers in place of antisense primer for cDNA synthesis. Three separate regions of the HCV genome were amplified. (i) The part of the NS5 region represented by clone pDXl00 (Garson et al, 1990a). (ii) The highly con- served 5’ non-coding region (Fig 1: Garson et al, 1 9 9 0 ~ ) . (i i i) The part of the structural protein encoding region represented by clone pDXl29 (Fig 1 : Phippard et al, 1990). using a novel set of primers: outer S’GGTGGAATT- - CACCTGTTGCCGCGCAG (sense) and S’GCTTGAATTCCAG- - CAATCGTTCGTG (antisense), inner SACTAG- GAAGCTTTCCG AGCGGT (sense) and S‘CGfiCGGAATTCATAAGCGGAAGC _ _ (antisense). Under- lined letters denote nucleotides altered in order to introduce artificial restriction sites to facilitate cloning of products. The contamination prevention measures of Kwok & Higuchi (1989) were applied strictly throughout the study.
RESULTS
All but one of the 21 patients had received lifelong therapy with blood products (mean age 33 years: range 20-61) and all had been treated with at least 8000 units of factor VIII concentrate (mean 82 000 units) in the previous year. Nineteen were infected with HIV and 1 6 had serological evidence of previous hepatitis B infection (antibody to hepatitis B core: anti-HBc). One of the anti-HBc positive sera contained detectable hepatitis B surface antigen (HBsAg). Transaminase levels were raised in 15/21 patients (Table I).
The prevalence of antibodies to HCV was found to be significantly affected by the choice of immunoassay. Whereas the BHC9 LISA based on structural protein (core) detected antibodies in all 21 sera, those based on non-structural proteins C l 0 0 and BHC7 (replicase) detected antibodies in only 1 3 (62%) and four (19%) sera respectively (Table 11). Four of the sera were reactive in all three assays, nine were reactive in two assays and the remaining eight reacted in the BHC9 ELISA only. Thirty control sera from routine blood donors did not react in any of the imrnunoassays.
The prevalence of hepatitis C viraemia detected by PCR was also affected by the choice of assay (Table 11). The highest prevalence was found with the 5’ non-coding region primer set (1 9 /2 1, 90%) and the lowest with the primer set derived from the pDX129 region (4/21. 19x1. The pDXlOO region primer set gave an intermediate result (7/2 1, 33%). Two sera (nos. 5 and 20) proved negative with all three sets ofprimers. No PCR signals were generated from any of the 30 control sera.
Table 11. Results of PCR and serological analysis
PCR primer sets ELISA antigens
Patient pDXl00 pDX129 5’NCR ClOO BHC7 BHC9
1 2 3 4 5 6 7 8 9
10 1 1 12 1 3 14 1 5 16 17 18 19 20 21
+ + + + + + + + + + + + + + + + + +
-
-
+
+ + + + + + + + + + + + + + + + + + + + +
+ =HCV RNA detected by PCR/A above the cut-off in ELISA. - =HCV RNA not detected by PCR/A below the cut-off in ELISA. pDX100=asequence (Garsonetal, 1990a)contained with theclone pDX102 (Fig 1). S’NCR= 5’ non-coding region.
DISCUSSION
The patients studied were selected because of prolonged treatment with high doses of unheated factor VIII concen- trate. Therefore it was not unexpected that we found a high prevalence of infection with HIV and HBV, viruses known to be transmitted in pooled blood products.
It is clear from the data presented that the choice of target protein used in an U S A for anti-HCV is of the utmost importance. The prevalence of anti-HCV based on reactivity to C100, was 62% (13/21), a figure consistent with earlier studies using similar assays (Noel et al, 1989: Makris et al, 1990). The proportion of sera which reacted with BHC7 was much lower. In contrast, judging by reactivity to the structural protein BHC9. all 21 patients had been exposed to HCV. This 100% seroprevalence is probably a true reflection of this group’s HCV exposure in view of the very high incidence of post treatment NANBH in recipients of commer- cial unheated factor VIII concentrate (Fletcher ct a / . 1983). Furthermore, it is unlikely that reactivity to BHC9 in the sera from the eight anti-Cl00 negative patients was false, since seven of these also contained HCV-RNA. It is of interest to note that antibodies to HCV were detected in all 2 1 patients (BHC9 U S A ) despite the high rate of coinfection with HIV.
Clearly the use of single HCV proteins. particularly if non- structural, may lead to underestimates of the prevalence of infection. Recently introduced ‘second generation’ commer-

HCV Antibodies and Viraemia in Haemophilia 5 15 cia1 assays which incorporate structural proteins have been shown. like the BHC9 ELISA used in this study, to be capable of detecting antibody in sera that were unreactive in tests based on the non-structural C lOO protein alone (Craxi et a / , 199 1 ). The hypothesis that non-structural proteins may be relatively poor antigens for use in anti-HCV ELISAs is also supported by the infrequency with which antibody to BHC7 (replicase) was detected in these patients.
The antibodies against HCV detected here do not simply reflect past infection because evidence of hepatitis C viraemia, and thus of on-going viral replication, is present in 90% of cases. This high prevalence of viraemia is unlikely to be due to immunosuppression resulting from concurrent HIV infection since similar findings have been reported in HIV negative individuals (Brillanti et al. 1991).
The primers selected for the detection of HCV-KNA greatly influenced the efficiency with which viraemia was detected. Primer sets based upon the 5' non-coding region sequence were clearly superior to those based on either replicase or core region sequences. This finding extends our previous observations (Garson et a / . 199Oc) and confirms the data of Okamoto et a/ ( 1 990) regarding the high level of sequence conservation of the 5' non-coding region in comparison with other parts of the HCV genome. Although we failed to detect HCV-KNA in two patients it is possible that they were viraemic at a level below the threshold ofdetectability by PCR (approximately 10' HCV genomes/ml). It is noteworthy that six of the viraemic patients had serum transaminase levels which fell within the normal range on the two occasions sampled, demonstrating that enzyme elevation is not a secure surrogate marker for viraemia in HCV infection.
We conclude that the prevalence of HCV infection in haemophiliacs may have been underestimated in earlier studies based upon the C l O O ELISA. Futhermore. our data suggest that antibody to HCV is more likely to indicate persisting viraemia than immunity, even in the face of normal serum transaminases. Further studies are needed to establish the role of antiviral therapy in these patients.
ACKNOWLEDGMENTS
We thank Clinical Nurse Specialist Maureen Fearns for her valuable assistance, also Dr P. Highfield and colleagues at Wellcome Diagnostics for kindly providing the recombinant HCV proteins. We are grateful to Drs M. Contreras and J. Barbara of the North London Blood Transfusion Service for making control sera available for this study.
REFERENCES
Brillanti. S . . Garson. j.A.. Tuke, P.W.. Ring, C.. Briggs, M., Masci. C.. Miglioli M.. Barbara, L. & Tedder. R.S. (1991) Etrect of interferon therapy on hepatitis C viraemia in community acquired non-A, non-B hepatitis. journal of Medical Virology. 34, 136-141.
Cederbaum. A.I.. Blatt, P.M. & Levine. P.H. (1982) Abnormal serum transaminase levels in patients with haemophilia A. Archives of Iiitemcil Medicine. 142. 481-484.
Choo. Q.1 ... Kuo, C.. Weiner. A.J.. Overby. L.R.. Bradley, D.W. & Houghton. M. (1989) Isolation of a cDNA clone derived from a blood borne non-A. non-B viral hepatitis genome. Science. 244. 35Y-362.
Craxi A.. Fiorentino. G.. Di Marco. V.. Marino. L.. Magrin. S.. Fabriano. C. & Pagliaro. L. (1991) Second generation tests in diagnosis of chronic hepatitis C. Lancet. 337, 1 354.
Esteban J.I.. Esteban. R.. Viladomiu. C.. Lopez-Talavera. J.C.. Gonza- lez. A.. Hernandez. j.M.. Roget. M.. Vergas. V.. Cenesca. J.. Buti. J., Cuardia. J., Houghton. M., Choo. Q.L. & Kuo. G. ( I 990) Hepatitis C virus antibodies among risk groups in Spain. I m c e t . ii, 294-297.
Eyster. M.E.. Whitehurst. D.A., Catalano. P.M.. McMillan. C.W., Goodnight. S.H.. Kasper. C.K.. Gill. J.C.. Aledort. L.M.. Hilgartner. M.W.. Levine. P.H., Edson. J.R.. Hathaway. W.E.. Lusher, J.M.. Gill, G.M.. Poole. W.K. & Shapiro, S.S. (19x5) Long-term follow-up of haemophiliacs with lymphocytopenia or thrombocytopenia. Blood. 66. 1 3 17-1 320.
Fletcher. M.L.. Trowell. J.M.. Craske. I.. Pavier. K. & Riza, C.R. ( 1 98 3 ) Non-A non-B hepatitis after transfusion of factor VIII in infrequently treated patients. British Medial journal. 287, 1754- 1757.
Garson. j.A.. Preston, F.E.. Makris. M.. Tuke. P.. Ring. C., Machin. S,j. & Tedder. R.S. ( 1990d) Detection by PCR of hepatitis C virus in factor Vll l concentrates, Lancet, 335, 1473.
Carson. J.A., Ring. C.. Tuke. P.W. & Tedder. R.S. ( 1 990c) Enhanced detection by PCR of hepatitis C virus RNA. Lancet. 336.237-238.
Carson. j.A.. Tedder. R.S.. Briggs. M.. Tuke. P.. Glazebrook. J.A.. Trute. A., Parker, D.. Barbara, J.A.J.. Contreras. M. 81 Aloysius. S. ( 1 990a) Detection of hepatitis C viral sequences in blood donations by "nested" polymerase chain reaction and prediction of infecti- vity. Lancet. 335, 1419-1422.
Carson, J.A.. Tuke. P.W.. Makris. M.. Briggs. M.. Machin. S.J.. Preston. F.E. & Tedder. R.S. ( 1990b) Demonstration of viraemia patterns in haemophiliacs treated with hepatitis C virus-contami- nated factor VIlI concentrates. Lancet. 336, 1022-1025.
Kuo. G.. Choo. Q.L.. Alter, H.j.. Gitnick. AX.. Redeker. A.G.. Purcell. R.H.. Miyamura. T.. Dienstag. J.L.. Alter. M.J.. Stevens. C.E.. Tegtrneier. C.E.. Bonino. F.. Colombo, M.. Lee. 1Y.S.. Kuo. C.. Berger. K.. Shuster. j.R.. Overby. L.R.. Bradley. D.W. & Houghton. M. (1 989) An assay for circulating antibodies to a major etiologic virus of human non-A. non-B hepatitis. Science. 244, 362-364.
Kwok. S. & Higuchi. R. (1989) Avoiding false positives with PCR. Nature. 339, 237-238.
Ludlam, C.A.. Chapman, D.. Cohen. B. & Litton. P.A. (1989) Antibodies to hepatitis C virus in haemophilia. Lancet. ii, 560-561.
Makris. M.. Preston, F.E.. Triger. D.R.. Underwood, J.C.E.. Choo. Q.L.. Kuo. G. & Houghton. M. ( 1 990) Hepatitis C antibody and chronic liver disease in haemophilia. Lancet. 335, 11 17-1 119.
Noel, L.. Guerois. C.. Maisonneuve. P.. Verroust. F. & Laurian. Y. ( I 989) Antibodies to hepatitis C virus in haemophilia. Lancet. ii, 560.
Okamoto. H., Okada. S.. Sugiyama. Y.. Tanaka. T.. Sugai. Y.. Akahane. Y.. Machida. A,. Mishiro. S.. Yoshinawa, H., Miyakawa. Y. & Mayumi. M. (1 990) Detection of hepatitis C virus RNA by a two-stage polymerase chain reaction with two pairs of primers deduced from the 5' noncoding region. japanese journal of Experi- niental Medicine. 60. (4). 21 5-222.
Phippard. D.. Glazebrook. 1.. Rodgers. B.. Garson. J . , Briggs. M. & Parker D. (1990) Recombinant ELISA and PCR analysis of PTNANBH serum samples. Proceedings of the VlIltli Internritionnl Congress of Virologu. Berlin. p. 196.
Roggendorf, M.. Deinhardt. F.. Rasshofer. R.. Eberle. 1.. Hopf, U.. Moller. B., Zachoual. R.. Pape. G.. Schramm. W. 6; Rornmel. F. (1989) Antibodies to hepatitis C virus. Lancet, ii. 325.
Triger, D.R. & Preston, F.E. (1 990) Chronic liver disease in haemo- philiacs. (Annotation). British journal of Haernatology. 74, 241 -245.