hepatitis b
TRANSCRIPT

1

DEPARTMENT OF PUBLIC
HEALTH DENTISTRY
SEMINAR
HEPATITIS B
Presented by:-
Dr. Amrita Rastogi
2

CONTENTS
HISTORY
INTRODUCTION
PREVALENCE OF HEPATITIS B
HEPATITIS B VIRUS
STRUCTURE OF HEPATITIS B VIRUS
REPLICATION OF HEPATITIS B VIRUS
MODES OF TRANSMISSION
HIGH-RISK GROUPS FOR HBV INFECTION
STAGES OF THE DISEASE
3
PATHOLOGY & PATHOGENISIS
SIGNS AND SYMPTOMPS
CLINICAL FEATURES
CLINICAL OUTCOME OF THE DISEASE
DIAGNOSIS
LEVELS OF PREVENTION
CONCLUSION
REFERENCES
4
HISTORY (1)
o Its an ancient disease first described in 5th century B.C.
o Earliest recognized blood-borne outbreak of hepatitis
was in Germany in 1883 after receiving smallpox
vaccine.
o In 1947 MacCalum and Bauer introduce the term
Hepatitis A for infectious and Hepatitis B for serum
hepatitis
o This terminology was adopted by WHO in 1973
5

INTRODUCTION (1)(2)
The term hepatitis describes inflammation of the liver.
Hepatitis may be caused by alcohols, drugs, autoimmune
diseases, metabolic diseases, and viruses. Viral infections
accounts for more than half the cases of acute hepatitis.
Viral hepatitis is a systemic infection affecting the liver
predominately with primary inflammation of the liver by
any one of a heterogeneous group of hepatotropic viruses6

Different types of Hepatitis viruses are:-
Hepatitis A (HAV) (1973)
Hepatitis B (HBV) (1970)
Hepatitis C (HCV) (1988)
Hepatitis D (HDV) (1977)
Hepatitis E (HEV) (1983)
Hepatitis F – Not separate entity – Mutant of B Virus.
Hepatitis G (HGV) (1995)7
All of these are RNA viruses except HBV which is a
DNA viruses.
The viral hepatitis is classified as:
Acute hepatitis (self-limited liver injury of less than 6
months)
Chronic hepatitis ( hepatic inflammation more than 6
months)
8

Hepatitis B is a serious and common infectious diseases
of the liver, affecting millions of people throughout the
world.
The severe pathological consequences of persistent HBV
infections include the development of chronic hepatic
insufficiency, cirrhosis and hepato cellular carcinoma
(HCC). In addition, HBV carriers can transmit the
disease for many years.
9
PREVALENCE OF HEPATITIS B (4)(5)
More than 2,000 million people alive today have been
infected with HBV at some time in their lives. Of these, about
350 million remain infected chronically and become carriers
of virtues. Three quarters of the world’s population live where
there are high levels of infection.
Every year there are over 4 million acute causes of HBV, and
about 25% of carriers, 1 million people a year, die from
chronic active hepatitis, cirrhosis or primary liver cancer. 10

11. Worldwide prevalence of hepatitis B carriers and primary hepatocellular
carcinoma. (Courtesy Centers for Disease Control and Prevention, Atlanta.)
12
The world can be divided into 3 areas where the
prevalence of chronic hepatitis infection is high (>8%),
intermediate(2-8%), and low (<2%).
High endemicity areas include south-east Asia and
Pacific Basin, sub-Saharan Africa, parts of middle east,
some countries in eastern Europe. In these areas about
70-90% of population becomes HBV infected before the
age of 40, and 8 to 20% of people are HBV carriers.

Low endemicity areas include North America, Western
and Northern Europe, Australia. The carrier rate here 2%
and less than 20% of the population infected with HBV
The rest of the world falls into intermediate range of
HBV prevalence, with 2 to 8% of a given population
being HBV carriers.
13

HEPATITIS B VIRUS (5)(6)
Hepatitis B is caused by the hepatitis B virus (HBV), an
enveloped virus containing a partially double stranded,
circular DNA genome, and classified within the family
of hepadnavirus.
14

The virus interferes with the functions of liver while
replicating in hepatocytes. The immune system is then
activated to produce a specific reaction to combat and
possibly eradicate the infectious agents. As a
consequence of pathological damage, the liver becomes
inflamed.
HBV may be the cause of upto 80% of all cases of
hepatocellular carcinoma world wide. 15
STRUCTURE OF HEPATITIS B VIRUS (5)(6)(7)
Hepatitis virus is a DNA virus with a remarkably
compact genomic structure.
It have circular partially double-stranded DNA viruses.
Replication occurs by reverse transcriptase.
It is small, circular, 3200 base- pair size, HBV DNA
codes for four sets of viral products and has a complex,
multi particle structure.16

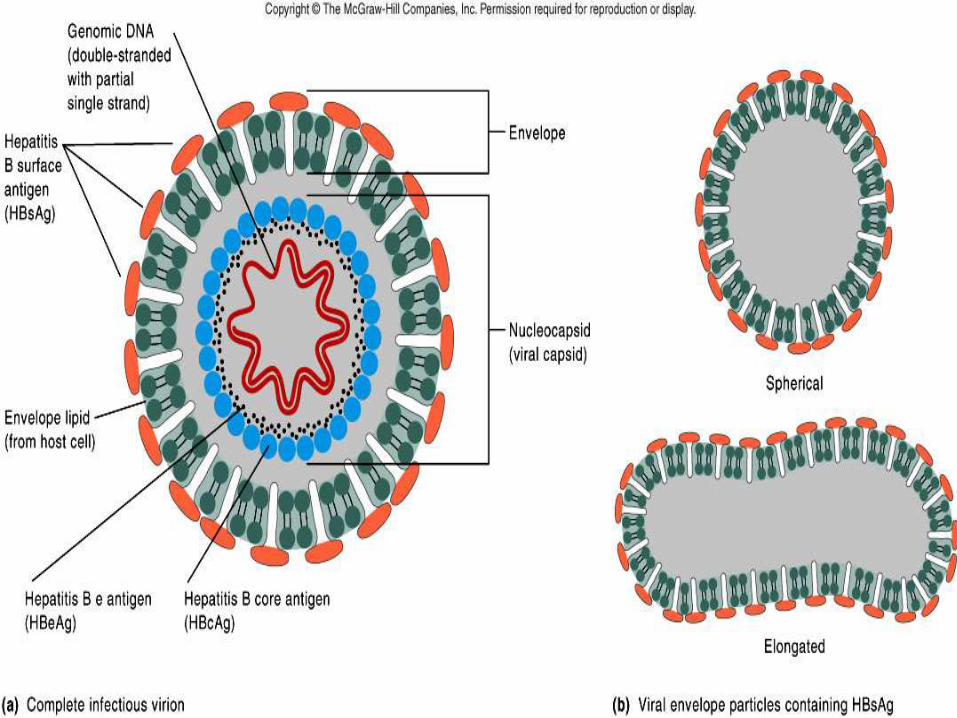
The hepatitis B virus is 42nm in diameter and composed
of 27 nm nucleocapsid core (HBcAG), surrounded by
outer lipo protein coat (also called envelope) containing
the surface antigen (HBsAG)
Virion also referred to as Dane particle (ds-tranded DNA)
Core antigens located in the center (nucleocapsid)
* Core antigen (HBcAg)
* e antigen (HBeAg
17
18

HBsAg = surface (coat) protein
HBcAg = inner core protein
HBeAg = secreted protein19

REPLICATION OF HEPATITIS B VIRUS (7)(8)
20
The HBV virion binds to a receptor at the surface of the
hepatocyte.
Viral nucleocaspids enter the cell and reach the nucleus,
where the viral genome is delivered.

21
Reverse transcription: one of the mRNAs is replicated with a
reverse transcriptase making the DNA that will eventually be
the core of the progeny virion
RNA intermediate: HBV replicates through an RNA
intermediate and produces and release antigenic decoy
particles.
Integration: Some DNA integrates into host genome causing
carrier state

HOW THE VIRUS REPRODUCES ?
1.First the virus attached to a liver cell membrane
22

2. The virus is then transported into the liver cell.
23
3. The core particle then releases it’s contents of DNA and
DNA polymerase into the liver cell nucleus.
24
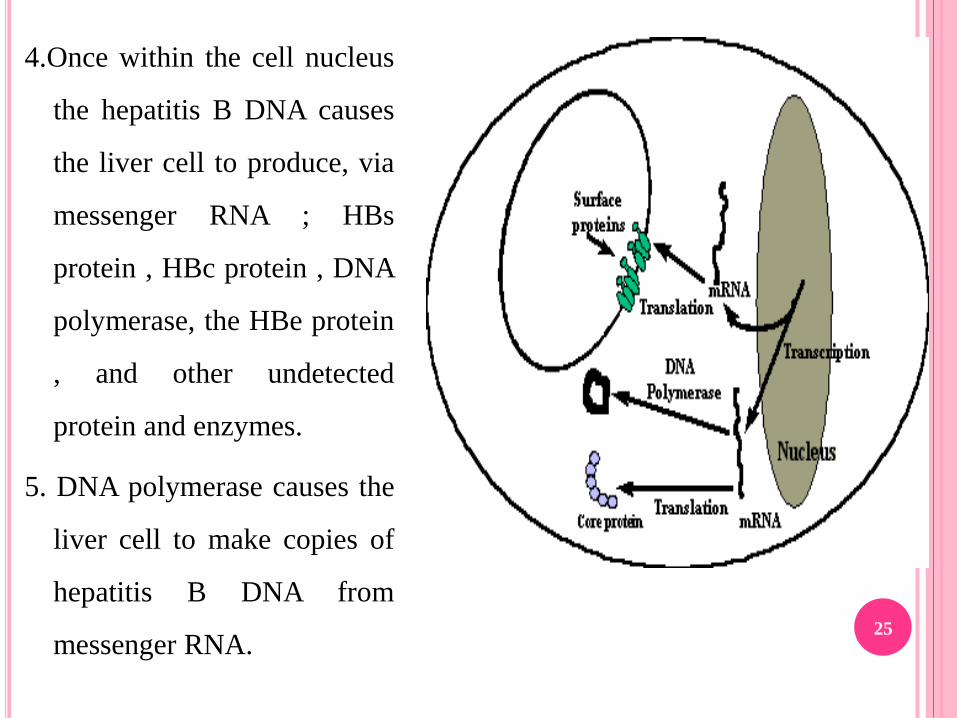
4.Once within the cell nucleus
the hepatitis B DNA causes
the liver cell to produce, via
messenger RNA ; HBs
protein , HBc protein , DNA
polymerase, the HBe protein
, and other undetected
protein and enzymes.
5. DNA polymerase causes the
liver cell to make copies of
hepatitis B DNA from
messenger RNA.25
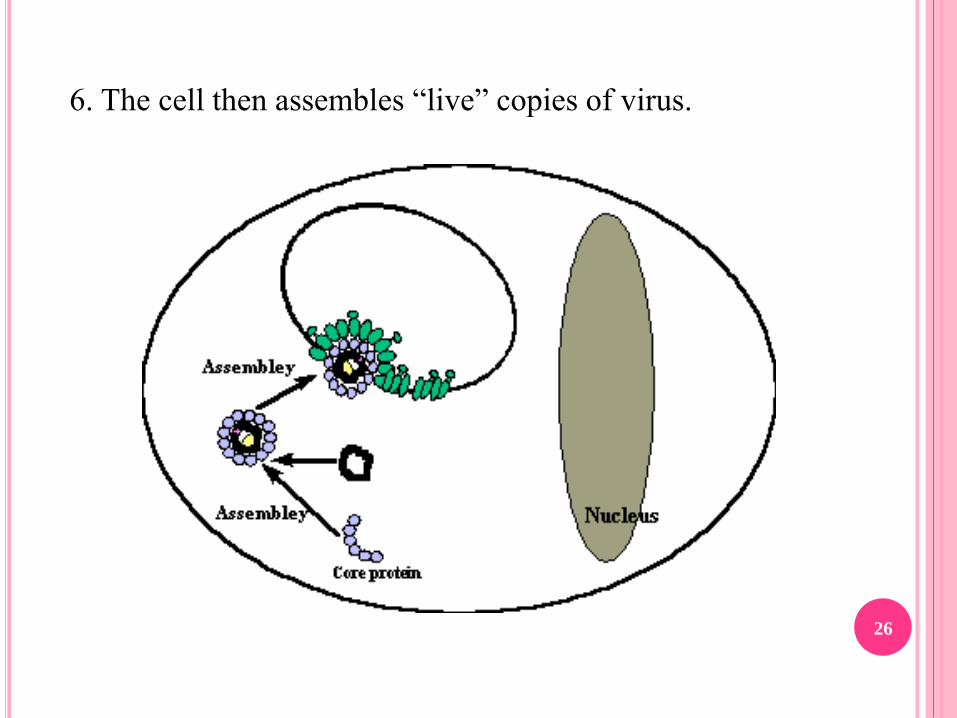
6. The cell then assembles “live” copies of virus.
26

7.However because of the excess numbers of surface
proteins produced many of these stick together to form
small spheres and chains. These can give a characteristic “
ground glass” appearance to blood samples seen under
microscope.
27

8. The copies of the virus and excess surface antigen are
released from the liver cell membrane into blood stream
and from there can infect other liver cells
28

29
MODES OF TRANSMISSION (9)
Sexual - sex workers and homosexuals are particular at
risk.
Parenteral - IVDA, Health Workers are at increased risk.
Perinatal - Mothers who are HBeAg positive are much
more likely to transmit to their offspring than those who
are not. Perinatal transmission is the main means of
transmission in high prevalence populations.30

31
Perinatal transmission Horizontal transmission
Mother
Infant
Host
Perinatal
• 90% of infected infants become chronically infected
• 6% of people infected over the age of 5 become chronically infected
Recipient
Child-to-child
Contaminated needles
Sexual contacts
Healthcare worker
Blood transfusion

32
Heterosexual*
(41%)
Homosexual Activity (9%)
Household Contact (2%)Health Care Employment (1%)
Others (1%)
Unknown (31%)
Injecting
Drug Use
(15%)

HIGH-RISK GROUPS FOR HBV INFECTION (9)
People from endemic regions
Babies of mothers with chronic HBV
Intravenous drug abusers
People with multiple sex partners
Hemo dialysis patients
Health care personnel who have contact with blood
Residents and staff members of institutions for the
mentally retarded 33
STAGES OF THE DISEASES (10)(11)
FIRST STAGE
The duration of this stage for healthy adults is
approximately 2-4 weeks and coincide with the
incubation period. For newborns, the duration of this
period often is decades.
Active viral replication is known to continue despite
little or no elevation in the aminotransferase levels and
no symptoms of illness.
34

SECOND STAGE
In the second stage, an inflammatory reaction with a
cytopathic effect occurs.
HBeAg can be identified in the sera and a decline of the levels
of HBV DNA is seen.
The duration of this stage for patients with acute infection is
approximately 3-4 weeks (symptomatic period).
For patients with chronic infection, 10 years or more may
elapse before cirrhosis develops. 35

THIRD STAGE
In the third stage, the host can target the infected hepatocytes
and the HBV Viral replication no longer occurs.
HBeAb can be detected. The HBV DNA levels are lower or
undetectable, and aminotransferase levels are within the
reference range.
In this stage, an integration of the viral genome into the host's
hepatocyte genome takes place.
HBsAg still is present. 36

FOURTH STAGE
In the fourth stage, the virus cannot be detected and
antibodies to various viral antigens have been produced.
Different factors have been postulated to influence the
evolution of these stages, including age, sex,
immunosuppression, and co-infection with other viruses.
37

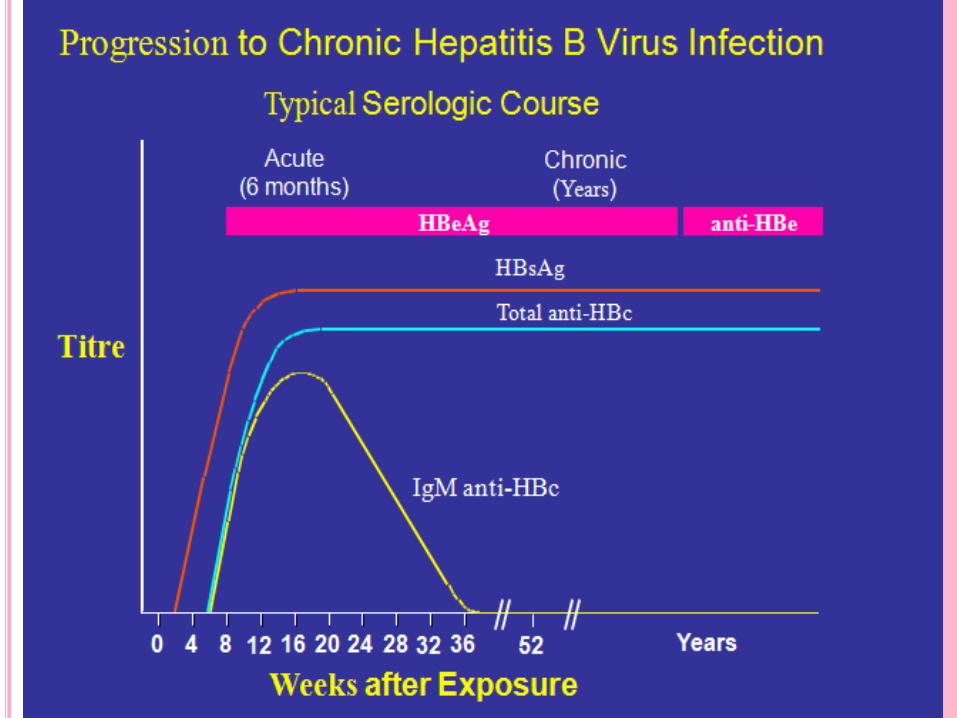
PATHOLOGY (11)(12)
Three antigen-antibody system
1) HBsAg-- anti-HBs system:
HBsAg appears 1-2 weeks (late up to 11-12 weeks) after
exposure, persists for 1-6 weeks( even 5 months) in acute
hepatitis B.
In chronic patients or carrier, HBsAg persist many years
HBsAg is the marker of infectivity
38

HBsAg can be found in blood and secretions: saliva,
urine, semen, tears, sweat and breast milk
Anti-HBs appear after HBsAg disappear several weeks
(or months) anti-HBs is protective antibody, can persist
for many years
39

2) HBcAg—anti-HBc system
HBcAg can be found in the nuclei of liver cells, no free
HBcAg in serum
HBcAg is the marker of replication of HBV
The stage called window phase
Anti-HBc IgM is a marker of acute infection and acute attack
of chronic infection of HBV. Anti-HBc IgG is the marker of
past infection, high titer means low level replication of HBV40

3) HBeAg—anti-HBe system
HBeAg is a soluable antigen
HBeAg is a reliable indicator of active replication of HBV
Anti-HBe is a marker of reduced infectivity. If exist long
may be a marker of integration of HBV into liver cell
41

42
43

PATHOGENISIS (11)
HBV invades into the human body by skin and mucosa, Via
blood flow enters the liver and other organs such as pancreas,
bile ducts, vessels, WBC, bone marrow, glomerular basement
membrane.
HBcAg,HBsAg,HBeAg and HLA-Ⅰappear on the liver cells
infected with are recognized by CTL simultaneously and lead
to the cytolysis of liver cells.44

Helper T cell are activated by the receptor of HLA- on
its surface combing with HBsAg, HBcAg and HLA-
antigen on the B cells promote B cell to release anti-
HBs and clear HBV
The representation of HBcAg on the liver cells may
cause cytopathy
45
SIGNS AND SYMPTOMS (12)
Fever
Fatigue
Loss of appetite
Nausea
Vomiting
Abdominal pain
Dark urine
Clay-colored bowel movements
Joint pain
Jaundice
Hepatomegaly
46

Symptoms begin an average of 3 months (range: 2–
5months) after exposure to HBV.
Symptoms typically last for several weeks but can persist
for up to 6 months.
47

CLINICAL FEATURES (12)(13)
48
Incubation period Average 60-90 days
Range 45-180 days
Clinical illness (jaundice) <5 yrs- <10%
>5yrs- 30-50%
Acute case-fatality rate 0.5%-1%
Chronic infection <5 yrs- 30-90%
>5yrs- 2-10%
Premature mortality from
chronic liver disease
15%-25%
CLINICAL FEATURES
ACUTE HEPATITIS B
Incubation period- 45to 120 days average 60 to 90 days.
Phases of disease
1. Preicteric
2. Icteric
3. Convalescent49
Preicteric
a. Tiredness
b. Anorexia
c. Vague abdominal discomfort
d. Nausea & Vomiting
e. Sometime arthralgias & rash
50

• Icteric
a. Within 10days of initial symptoms
b. Dark urine Pale stool Yellowish discoloration of
mucous membranes.
c. Total bilirubin- exceeds 20 to 40 mg/l
d. Hepatosplenomegaly
e. After disappearance of jundice-Anti HBs.
51

• Convalescent
a. Anti HBc IgM to IgG type
b. Transient presence of HBsAg, HBeAg and viral DNA
(<6 months)
c. Seroconversion to anti HBsAg and anti HBeAg
52

Chronic Hepatitis B
After acute infection virus remain in 5 to 10% cases of
adult, even more higher among children upto 70 to 90%.
350 million of person worldwide are chronic carriers.
Among them 100 million in China.
Among the persistent carrier 70% will develop Chronic
persistent hepatitis and remaining 30% will develop
Chronic active hepatitis.53
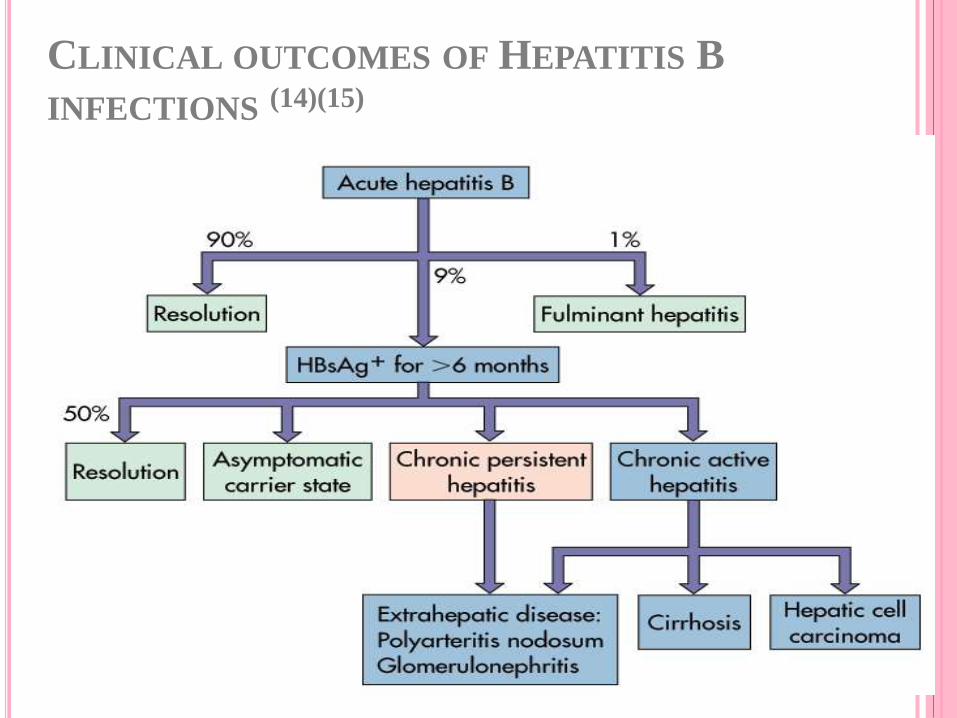
CLINICAL OUTCOMES OF HEPATITIS B
INFECTIONS (14)(15)
54

HEPATOCELLULAR CARCINOMA
Only 5% patient with cirrhosis develop HCC.
HCC is responsible for 90% of primary malignant tumor of
liver.
Worldwide 7th most common cancer in male while 9th in
female.
Causes >500000 deaths annually with male & female ratio
4:1.55
Appears after a mean duration of about 35 years of HBV
infection.
56

FULMINANT HEPATITIS
Rare condition, develop in about 1% cases.
It is due to massive necrosis of liver substance.
Usually fatal
Survival in adult is uncommon.
Genetic heterogeneity, co-infection, host immunological
factors are responsible.57
EXTRA-HEPATIC MANIFESTATIONS (15)
Mediated by circulating immune complexes
Both acute hepatitis & chronic hepatitis
Acute hepatitis –10-20%
Serum sickness like illness,
Fever, rash, artralgia.
Gainotti- Crosti syndrome
Papular acrodermatits (children)
Glomerular disease
58

DIAGNOSIS (16)(17)
HBsAg - used as a general marker of infection.
HBsAb - used to document recovery and/or immunity to HBV
infection.
anti-HBc IgM - marker of acute infection.
anti-HBcIgG - past or chronic infection.
HBeAg - indicates active replication of virus and therefore
infectiveness.59

Anti-Hbe - virus no longer replicating. However, the
patient can still be positive for HBsAg which is made by
integrated HBV.
HBV-DNA - indicates active replication of virus, more
accurate than HBeAg especially in cases of escape
mutants. Used mainly for monitoring response to therapy.
60
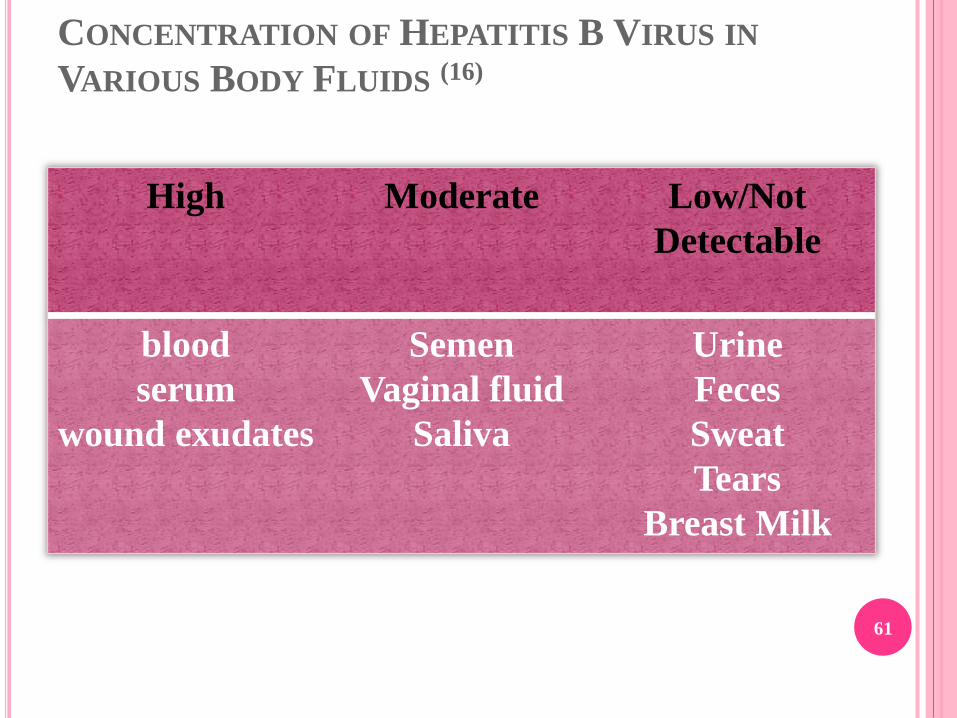
CONCENTRATION OF HEPATITIS B VIRUS IN
VARIOUS BODY FLUIDS (16)
High Moderate Low/Not
Detectable
blood
serum
wound exudates
Semen
Vaginal fluid
Saliva
Urine
Feces
Sweat
Tears
Breast Milk
61
LEVELS OF PREVENTION FOR HEPATITIS B (17)(18)
Primary Prevention
Advocacy and raising awareness of all types of viral
hepatitis infections help to reduce transmission in the
community.
Safe and effective vaccines are widely available for the
prevention of HAV and HBV infections and an HEV
vaccine has recently been licensed in China.
Implementation of blood safety strategies, including
blood supplies based on voluntary non-remunerated
blood donations, effective public education on blood
donation, donor selection, and quality-assured screening
of all donated blood and blood components used for
transfusion can prevent transmission of HBV and HCV.62
Infection control precautions in health care and community
settings can prevent transmission of viral hepatitis as well as
many other diseases.
Safe injection practices can protect against HBV and HCV
transmission.
Safer sex practices.
Harm reduction practices for injecting drug users prevent
HAV, HBV and HCV transmission.
Occupational safety measures prevent transmission of viral
hepatitis to health care workers.
Safe food and water provide protection against HAV and HEV
infection
.63

HEPATITIS B VACCINATION (19)
1965 Discovery of Australian antigen
1973 Successful HBV infection of chimpanzees
1981 Licensure of plasma-derived vaccine
1986 Licensure of recombinant vaccine
1991 Universal infant vaccination
1996 Universal adolescent vaccination 64

Vaccines against hepatitis B were introduced in the early,
1980s.
More than 110 countries have adopted a national policy
of immunizing all infants with hepatitis B vaccine.
HB vaccine is the most effective tool in preventing the
transmission of HBV and HVD. Vaccine are composed
of the surface antigen of HBV(HBsAg), and are
produced by two different methods: plasma derived or
recombinant DNA.
65
PLASMA DERIVED VACCINE
These vaccines, derived from the plasma of HBsAg-
positive donors, consist of highly purified, formalin-
inactivated and/or heat-inactivated, alum-absorbed,
hepatitis B sub virion particles (22nm) of HBsAg that are
free to detectable nucleic acid and therefore,
noninfectious.
The first plasma derived vaccines were manufactured in
USA and France in 1981-1982.
66

RECOMMENDATION FOR PRE EXPOSURE
IMMUNIZATION WITH HEPATITIS B
Infants (Universal immunization)
Infants and adolescents not vaccinated previously
(catch-up vaccination)
Person with occupational risk
Haemodialysis patients
Recipients of blood and blood products
Susceptible drug abusers.
Sexually active men or women
Susceptible inmates who have a history of high risk
behavior67
Household contacts and sex partners of HBV carriers
Population with a high incidence of disease
International traveler to area of high HBV endemicity
Transplant candidates.
68

COMBINATION VACCINES
The HBsAg vaccines can be combined with other
vaccines such as Calmetta-Guerin Bacillus(BCG),
measles, mumps, and rubella, Haemophilus influenzae b,
diptheria, tetanus and petussis combined with polio.
Neonates born to mother who are HBsAg positive should
be given a combination of passive and active
immunization to provide immediate protection in the first
6 hours after delivery, followed by long term immunity
with the vaccine.
69

The vaccine is administered by intramuscular injection in
the antrolateral aspect of the thigh of the new born and
infants or deltoid (arm) muscle of children and adults in
order to achieve optimal protection.
It is particular effective within 48 hours of the incident. It
may also be given to neonates who are at increased risk
of contracting hepatitis B i.e. whose mothers are HBsAg
and HBeAg positive.
Hepatitis B Immunoglobulin - HBIG may be used to
protect persons who are exposed to hepatitis B.
70

HEPATITIS B VACCINE
ADOLESCENT AND ADULT SCHEDULE
71
Dose
Primary 1
Primary 2
Primary 3
Minimum
Interval
- - -
4 weeks
8 weeks*
Usual
Interval
---
1 month
5 months
*third dose must be separated from
first dose by at least 16 weeks

RECOMMENDED DOSE OF HEPATITIS B VACCINE
72
Infants and children
<11 years of age
Adolescents 11-19 years
Adults >20 years
Recombivax HB
Dose (mcg)
0.5 mL (5)
0.5 mL (5)
1.0 mL (10)
Engerix-B
Dose (mcg)
0.5 mL (10)
0.5 mL (10)
1.0 mL (20)
Factors for decreased vaccine response:
- Smoking
- Obesity
- HIV infection
- Imunocompromised patients
-Haemodialysis
- Prematurity
- Genetic factors
- Chronic disease.
- Subcutaneous injection
- Freezing of vaccine
- Accelerated schedule
73

DENTAL CONSIDERATION
For dentists : Hepatitis B & Hepatitis C virus are
important as they can be transmitted by various methods
as it is most common blood borne infection.
Its is associated with many clinical features which are
encountered by dentist like:
o Sjorgren’s syndrome
o lichen planus
o glossitis and/or angular cheilosis
o Mucosal Ecchymosis
74

Management for dentists:
Pre – Exposure vaccination : Engerix. Which is available
commonly.
Maintaining proper sterilization and infection control
measures.
More use of disposable products like disposable gloves,
mouth mask, syringes, etc.
Proper disposal of used needles.
75
ROLE OF A PUBLIC HEALTH DENTIST
A public health dentist can play an important role in preventing the
hepatitis B by:
Educating people about ways of mode of transmission of diseases.
By telling the real facts and myths related to disease.
To encourage people for vaccination
Telling about healthy lifestyle and habits to prevent any kind of liver
related diseases.
76
SECONDARY PREVENTION (20)
Early diagnosis provides the best opportunity for effective
medical support and prevention of further spread. It also
allows the infected persons to take steps to prevent
transmission of the disease to others. Early diagnosis of
those with chronic infection also allows people to take
precautions to protect the liver from additional harm,
specifically by abstaining from alcohol and tobacco
consumption and avoiding certain drugs that are known
to be toxic to the liver.
77
Treatment of acute HBV infection is primarily supportive.
Good nutrition and bed rest should be reinforced.
Abstinence from alcohol and the use of hepatotoxic drugs is
also necessary.
Conversely, chronic HBV infection may be progressive and,
therefore, requires management. The goals of therapy include
minimization of hepatocellular damage and viral clearance.
78

Possible adverse effects to interferon include fever and
chills, headache, depression, malaise, tachycardia, bone
marrow suppression, alopecia and, on rare occasion
,cardiac or renal failure.
79

In acute hepatitis B the treatment is basically
symptomatic
Rest
Ant emetics to control vomiting
Plenty of fluids and carbohydrates
Hepatotropic agents
80

Chronic Hepatitis B (20)(21)
Interferon - for HBeAg +ve carriers with chronic active hepatitis.
Response rate is 30 to 40%.
Lamivudine - a nucleoside analogue reverse transcriptase
inhibitor. Well tolerated, most patients will respond favorably.
However, tendency to relapse on cessation of treatment. Another
problem is the rapid emergence of drug resistance.
Successful response to treatment will result in the disappearance
of HBsAg, HBV-DNA, and seroconversion to HBeAg. 81

82

TERTIARY PREVENTION
There is no surgical treatment for hepatitis B.
In case of advanced liver damage because of hepatitis and
condition becomes life-threatening, their is need a liver
transplant.
In rare cases, acute hepatitis B progresses rapidly to liver
failure, a deadly condition called fulminant hepatitis. For
people who develop this condition, a liver transplant is the
only treatment choice.
83

CONCLUSION
Hepatitis B is the most common serious liver infection in
the world. It is caused by the hepatitis B virus (HBV)
that attacks liver cells and can lead to liver failure,
cirrhosis scarring) or cancer of the liver. The virus is
transmitted through contact with blood and bodily fluids
that contain blood.
84
The hepatitis B virus is 100 times more infectious than the
AIDS virus. Yet, hepatitis B can be prevented with a safe
and effective vaccine. For the 400 million people
worldwide who are chronically infected with hepatitis B
the vaccine is of no use. However, there are promising
new treatments for those who live with chronic
hepatitisB.
85

REFERENCES1. Hepatitis B Epidemiology and Prevention of Vaccine-
Preventable Diseases The Pink Book: Course Textbook - 12thEdition Second Printing (May 2012) Center Of DiseasesControl
2. Fauci ,Braunwald, Isselbacher Harrison’s Principle of internalmediciene vol-2 14th edition.
3. Haslett, Chivers, Boon Davidson’s Principles and Practice ofMediciene. 2004 19th edition.
4. Churchill’s Illustrated Medical Dictionary, New York ,Churchill Livingstone, 1989.
5. Harmanjit Singh Hira Text book of General Medicine forDental Students.
6. Manual of Clinical Microbiology, Patrick R Murray 9th
edition.
7. Topely and Wilson’s, Virology volume-1 ,9th edition. 86

8. Mandell’s, Principle and Practice of Infectious Diseases,
5th edition
9. Documents on Hepatitis A-E published by WHO,
Department of Communicable Diseases Surveillance
and Response
10. Textbook of Microbiology, Ananthanarayan and
Paniker,7th edition
11. European Association for the Study of the Liver. EASL
clinical practice guidelines: management of chronic
hepatitis B. J Hepatol 2009;50:227–242.
87
12. Ganem D, Schneider RJ. Hepadnaviridae: The Viruses andTheir Replication. In : Knipe DM et al., eds. Fields Virology,4th edition, Philadelphia, Lippincott Willams& Wikins,2001:2923-2969.
13. Ganem D, Prince AM. Hepatitis B virus infection – naturalhistory and clinical consequences. N Engl J Med2004;350:1118–1129.
14. Hepatitis B ; World Health Organization, Department ofCommunicable Diseases Surveillance and Response;WHO/CDC/LYO/2002.2: Hepatitis B.
15. Center for Disease Control and prevention. Hepatitis Bvaccine. 1998(http://www.cdc.gov/ncidod/diseases/b/hebqafn.htm)
16. Gitlin N. Hepatitis B: diagnosis, prevention, and treatment.Clinical Chemistry, 1997, 43:1500-1506.
17. Prevention and Control of Viral Hepatitis; Frame Work forglobal action;WHO/HSP/PED/HIP/GHP/2012.1
88
18. Jacobsen KH, Wiersma ST. Hepatitis A virus
seroprevalence by age and world region, 1990 and 2005
Vaccine, 2010, 28: 6653–6657.
19. Perz JF et al. The contributions of hepatitis B virus and
hepatitis C virus infections to cirrhosis and primary
liver cancer worldwide. Journal of Hepatology,
2006,45: 529–538.
20. World Health Organization. Hepatitis B vaccines.
Weekly Epidemiological Record, 2004.79:255-263.
21.Hepatitis B Department of Health and Human Services
Center Of disease conrol and prevention ; Division of
viral hepatitis.June 2010 (WWW.CDC.gov/hepatitis)
89

90