hemolytic anemia - cancer medicine and hematology
TRANSCRIPT
Hemolytic Anemia
Jean M. Connors, MD
Brigham and Women’s Hospital
Dana Farber Cancer Institute
Harvard Medical School
Boston, MA

Conflicts of Interest
Pfizer/Bristol Meyer SquibbIndependent Review CommitteeScientific Ad BoardsConsultant
PortolaScientific Ad Boards
Unum TherapeuticsDSMB
• Overview of hemolytic anemia– Non-immune
• HS, HE• G6PD
– Immune• WAIHA• CAD
• Testing• Treatment
Outline
Question 2
• Anemia: How do you know it is hemolytic? – Increased reticulocyte count and absolute
retics– Peripheral smear: abnormal RBC
morphology– Decreased haptoglobin– Increased LDH– Increased indirect bilirubin– DAT: negative or positive?
• If positive what type of antibody
Approach
Question 2
• Classification– Intrinsic vs extrinsic to RBC– Non-immune– Autoimmune – Alloimmune
• Site of destruction– Intravascular vs extravascular
Approach

Question 2
• Inherited, with rare exceptions (PNH, acquired alpha thal)
• Mutations resulting in:– Membrane/cytoskeleton component defect– Hemoglobinopathy– Decreased enzymatic/metabolic function
Intrinsic RBC Etiology
Question 2
• Antibodies• Hypersplenism• Shear stress• Oxidants• Pathogens
– Malaria– Babesiosis– Clostridium perfringens
Extrinsic RBC Etiology
Question 1
• Most common inherited enzyme defect– Multiple mutations, track with ethnicity– can not reduce NADP or subsequently glutathione
• X-linked– males more significantly affected
• Most patients asymptomatic• Hemolytic crises linked to oxidative stress:
– Infection– Drugs– Fava beans: Mediterranean variant only
– Chemicals– Diabetic ketoacidosis
G6PD Deficiency

G6PD Deficiency
Prevalence of G6PD deficiency similar to malaria.

Glucose-6-Phosphate (G6PD) Deficiency
Figure 10-7 Heinz bodies in a patient withoxidant hemolysis.
Bunn & Lux, Chapter 10
Figure 10-6 Red cell metabolic pathways.
Question 1
• Diagnosis– Heinz bodies (denatured, pptd hgb), bite cells on smear– G6PD enzyme activity level
• Not accurate during acute crisis– Beutler fluorescent spot test– PCR for common variants (Mediterranean, A-)
• Treatment– Avoid offending drugs, foods, chemicals– Transfuse if necessary– Folic acid– Splenectomy often ineffective
G6PD Deficiency
Question 1
• Drugs– Antimalarials
• Primaquin, quinacrine– Sulfonamides– Dapsone– Phenacetin, asa– Nitrofurans– Mothballs– Rasburicasewww.g6pd.org/en/G6PDDeficiency/SafeUnsafe
G6PD Deficiency

Question 1• Mutations in cytoskeletal proteins
– Ankyrin 50-60% HS and 90% HE– Spectrin, band 3 in HS, protein 4.1 in HE
• Clinical severity ranges from mild to severe– Evidence of hemolytic anemia from birth– Exacerbations of hemolysis only when stressed
• infection
• Diagnosis– Evidence of extravascular hemolysis– Peripheral smear– Osmotic fragility test: hypotonic NaCl solutions– EMA: decreased eosin-5-maleimide binding by RBCs
assessed by flow cytometry
HS and HE
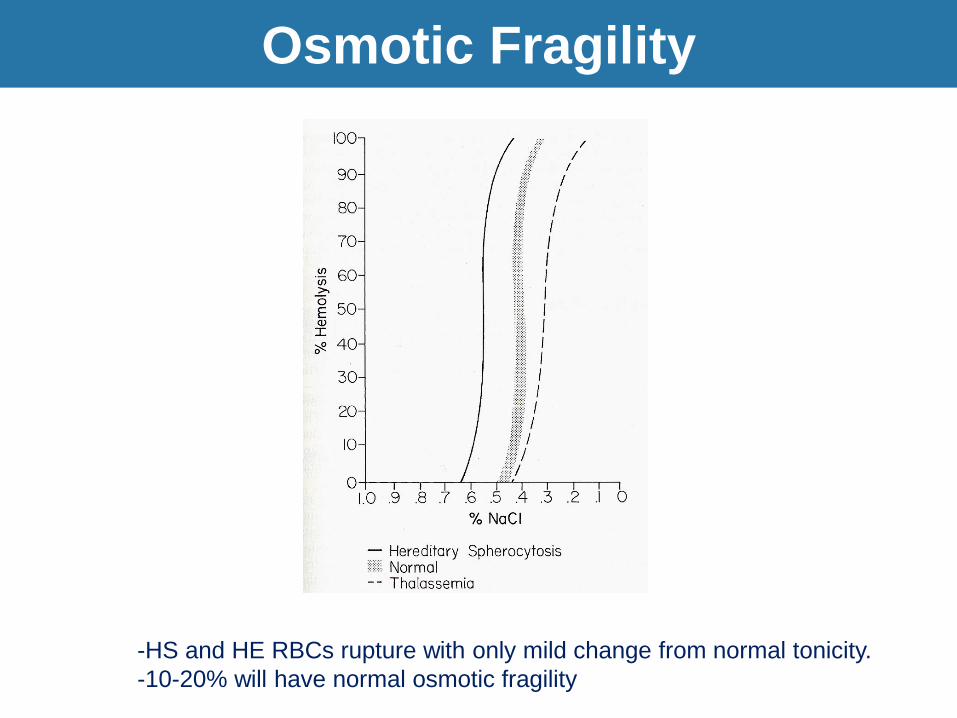
Osmotic Fragility
-HS and HE RBCs rupture with only mild change from normal tonicity.-10-20% will have normal osmotic fragility
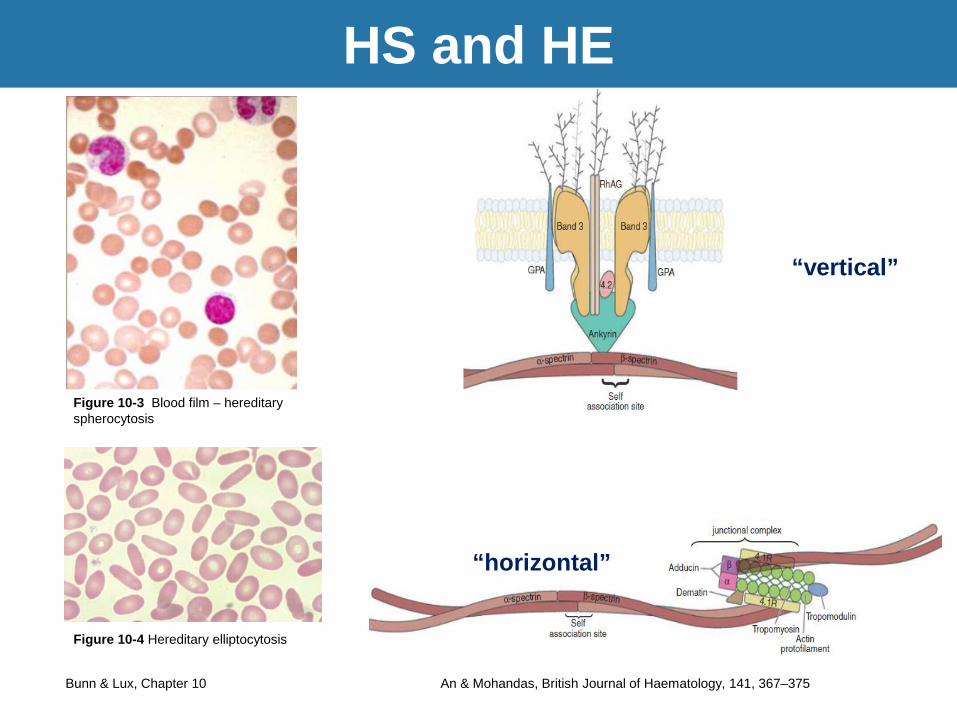
Hereditary Spherocytosis (HS) and Hereditary Elliptocytosis (HE)
Figure 10-4 Hereditary elliptocytosis
Figure 10-3 Blood film – hereditary spherocytosis
An & Mohandas, British Journal of Haematology, 141, 367–375Bunn & Lux, Chapter 10
HS and HE
“vertical”
“horizontal”

The EndHS and HE
Sam Lux

Question 1
• Treatment: varies with severity– “typical” HS and HE: mild to moderate anemia,
increased bili, splenomegaly, erythroid hyperplasia– Severe and atypical forms rare, manifest from birth,
can have life threatening hemolytic crises • Splenectomy
– Normalizes RBC lifespan, anemia and increased biliusually resolve, spherocytes persist
– Treat with folate especially if hemolysis persists• Gallstones
– Pigmented stones common
HS and HE
Question 1
• Autoimmune
• Alloimmune– Transfusion– HSCT– Maternal/fetal: Rh, Kell
• Drug induced
Immune Hemolytic Anemia
Question 1
• Warm autoimmune hemolytic anemia (WAIHA)
• Cold agglutinin syndrome (CAS)
• Paroxsymal cold hemoglobinuria (PCH)– Donath Landsteiner antibodies
• Mixed AIHA
• Atypical AIHA (DAT negative)
• The first RCT of any treatment for any AIHA was published this year—for warm AIHA
Autoimmune Hemolytic Anemia
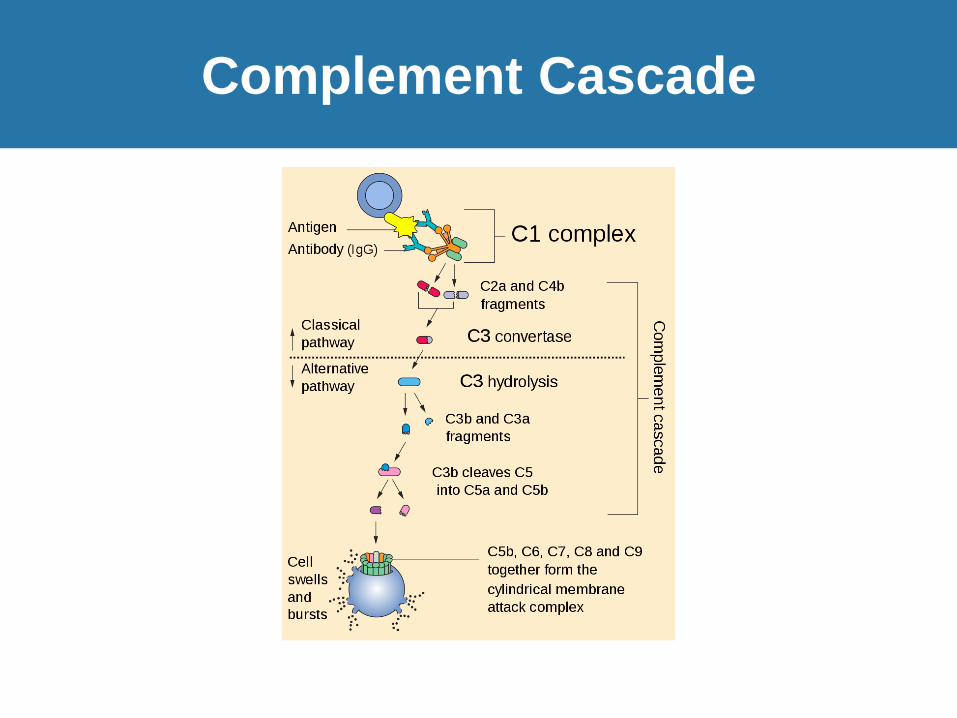
Complement Cascade
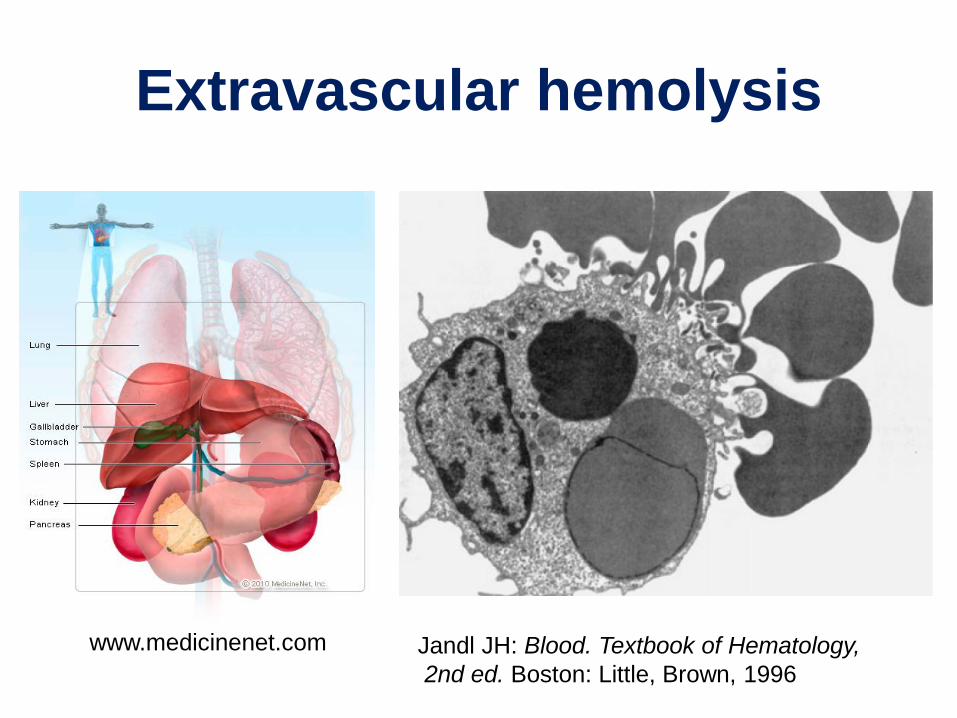
Extravascular hemolysis
Jandl JH: Blood. Textbook of Hematology,2nd ed. Boston: Little, Brown, 1996
www.medicinenet.com
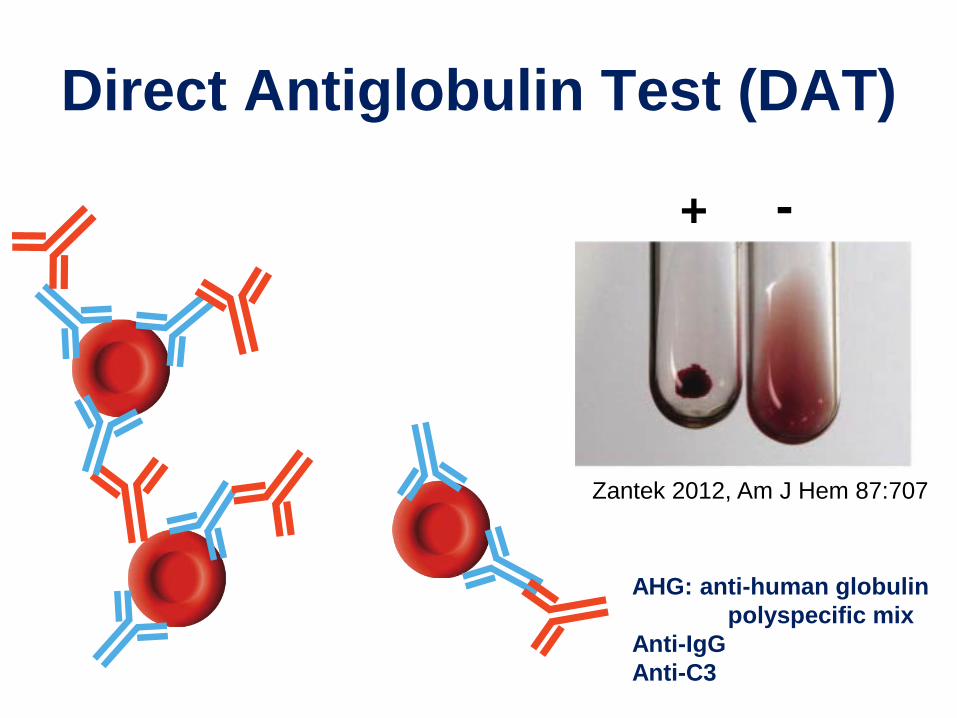
Direct Antiglobulin Test (DAT)
Zantek 2012, Am J Hem 87:707
+ -
AHG: anti-human globulinpolyspecific mix
Anti-IgGAnti-C3
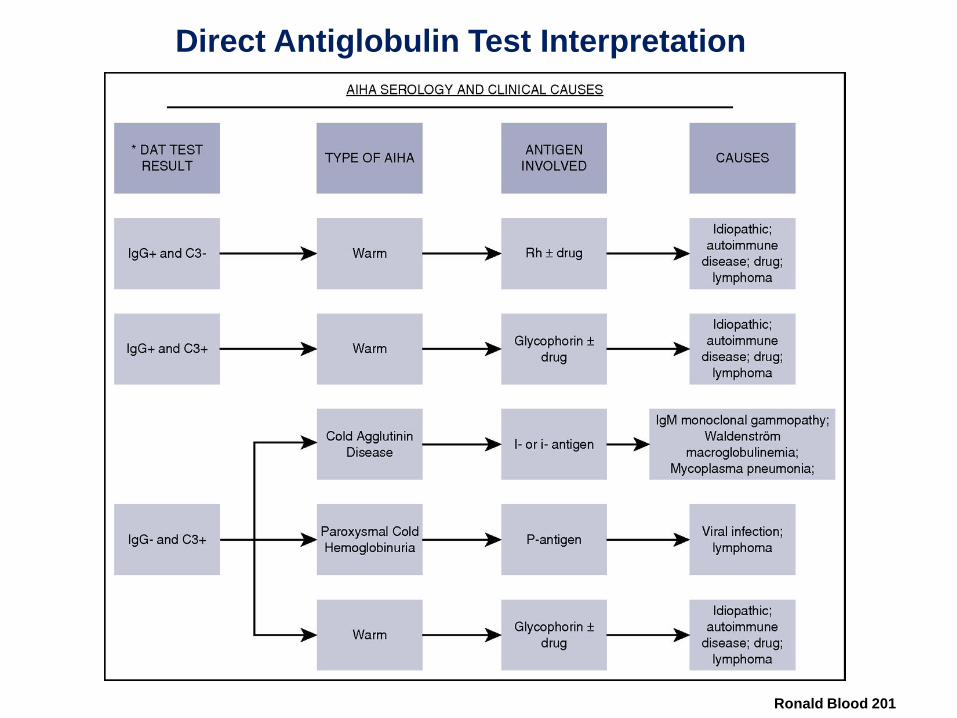
Direct Antiglobulin Test Interpretation
Ronald Blood 201

Question 1• Incidence: 1 to 2 cases/100,000 per year• F > M• Adults > children• IgG pan-agglutinins, react with all cells
– Ag target usually protein, often Rh but poorly defined– Extravascular hemolysis
• Primary (idiopathic)• Secondary
– CLL– Lymphomas and lymphoproliferative disorders– SLE
WAIHA
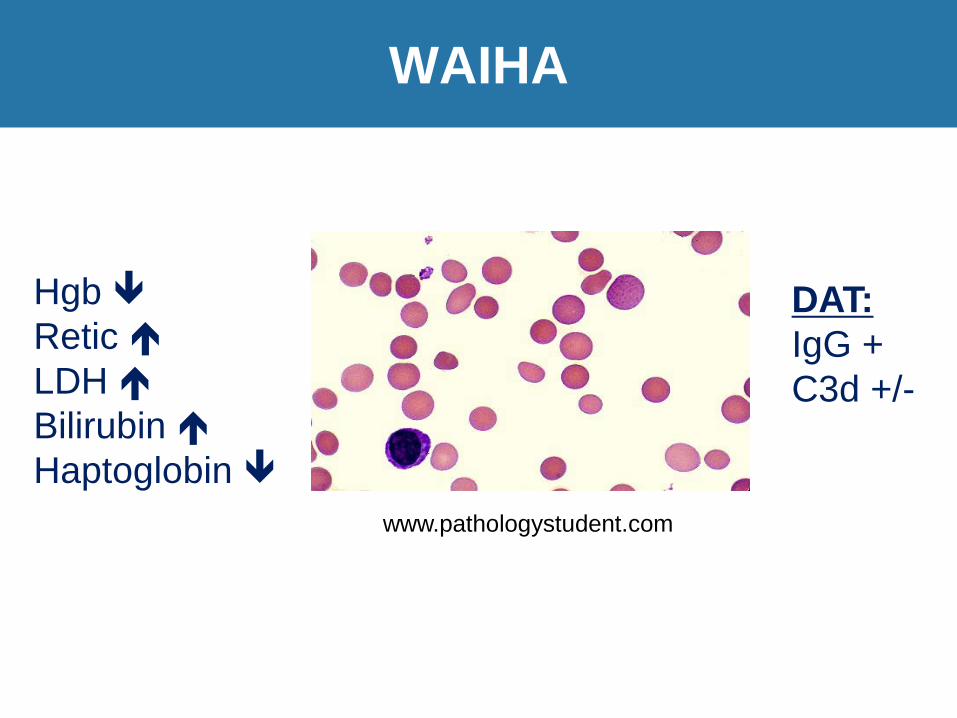
WAIHA: diagnosis
www.pathologystudent.com
DAT:IgG +C3d +/-
Hgb Retic LDH Bilirubin Haptoglobin
WAIHA

WAIHA: therapyOften extremely rapid onset, patients have significant
symptoms: weakness, SOB, tachycardiaTransfuse, despite difficulty with cross match
• 1st line therapy: steroids– Prednisone 1 mg/kg/d– Continue at least 2 weeks until hct clearly improved,
then slow taper– 80% respond within 3 weeks– Less than 20% have sustained response– “Failure” usually defined as requiring more than 15
mg/day of prednisone or equivalent to maintain Hgb>10; Hct >30
Primary WAIHA: Treatment
WAIHA: therapy
• 2nd line therapy: refractory or relapsedSplenectomy:
– 80% early CR, 60-70% CR at 2-3 yrs– May reduce steroid requirement– Complications: sepsis, thrombosis– Laparoscopic vs open splenectomy
Primary WAIHA: Treatment
WAIHA: therapy• 3rd line therapy: rituximab• Standard 4-wk dosing• 80% initial response• Poor data on long term outcome, but likely fewer long
term responses than in ITP• Preferred therapy in those w/ contraindications to
splenectomy
• Refractory: – MMF, csa, cytoxan, vincristine, azathioprine,
alemtuzumab
Primary WAIHA: Treatment
WAIHA: therapy• Use rituximab as 1st line with steroids?
• Meta-analysis of rituximab in AIHA – Overall response rate 70% for warm AIH– Complete response rate 42% for warm AIHA
• RCT of rituximab* vs placebo in newly diagnosed warm AIHA, in conjunction with prednisone.– 1 yr ORR 75% rituximab vs 31% placebo (p=0.032)
– 2 yrs 10/16 still with CR vs 3/16 placebo– More infections in placebo group
Primary WAIHA: TreatmentRituximab—2nd Line?
Autoimmun Rev 2015
* Two doses of 1000 mg 2 weeks apart Am. J. Hematol. 2017

• Treat WAHIA alone or underlying disorder or both?
• SLE– Steroids alone usually successful– Splenectomy not as effective, rituximab :PML risk?
• CLL– Fludarabine associated WAIHA
• NHL– Poor response to steroids, splenectomy– Treatment aimed at lymphoma
Secondary WAIHA: Treatment
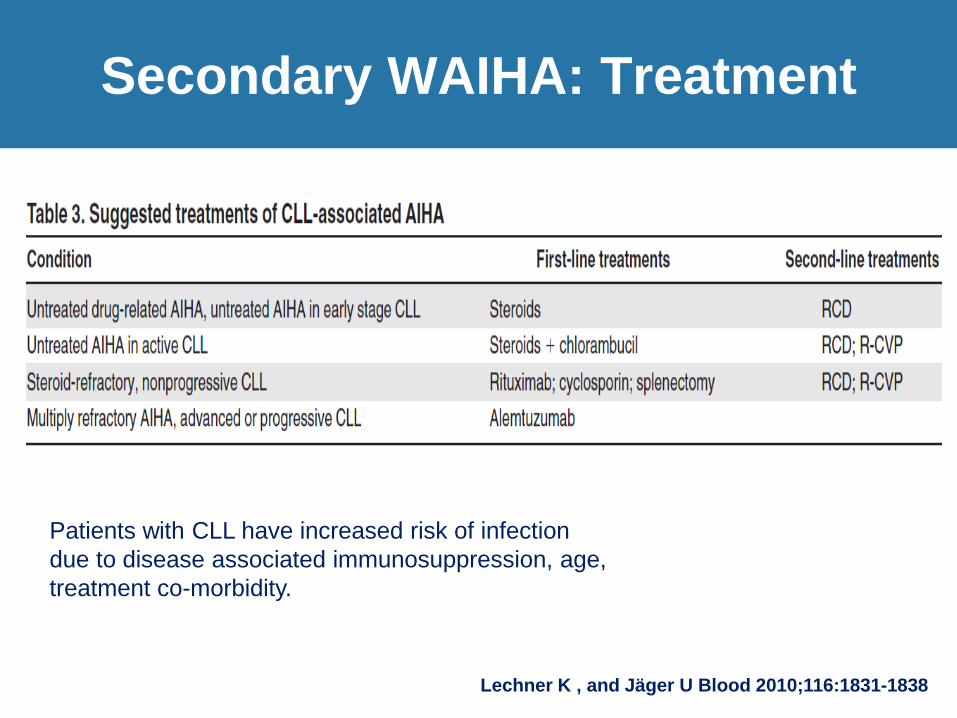
Secondary WAIHA: Treatment
Lechner K , and Jäger U Blood 2010;116:1831-1838
Patients with CLL have increased risk of infection due to disease associated immunosuppression, age, treatment co-morbidity.

Primary CAD: clinical features
• Symptoms and findings
– Chronic anemia
– Intravascular hemolysis
– Hemoglobinuria, urine hemosiderin
– Plasma hemoglobin
– Acrocyanosis
Cold Agglutinin Syndromes
• IgM antibodies against carbohydrate antigens– I vs I
• Primary cold agglutinin disease (CAD)– Incidence: 1/1,000,000 F=M– Monoclonal B cell lymphoproliferative disorder usually
with IgMk against I antigen
• Secondary cold antibody-mediated AIHA– Mycoplasma pneumoniae: anti-I IgM– Infectious mononucleosis: anti-i IgM– Lymphoid neoplasms: anti-I or anti-i IgM– SLE
Cold Agglutinin Syndromes
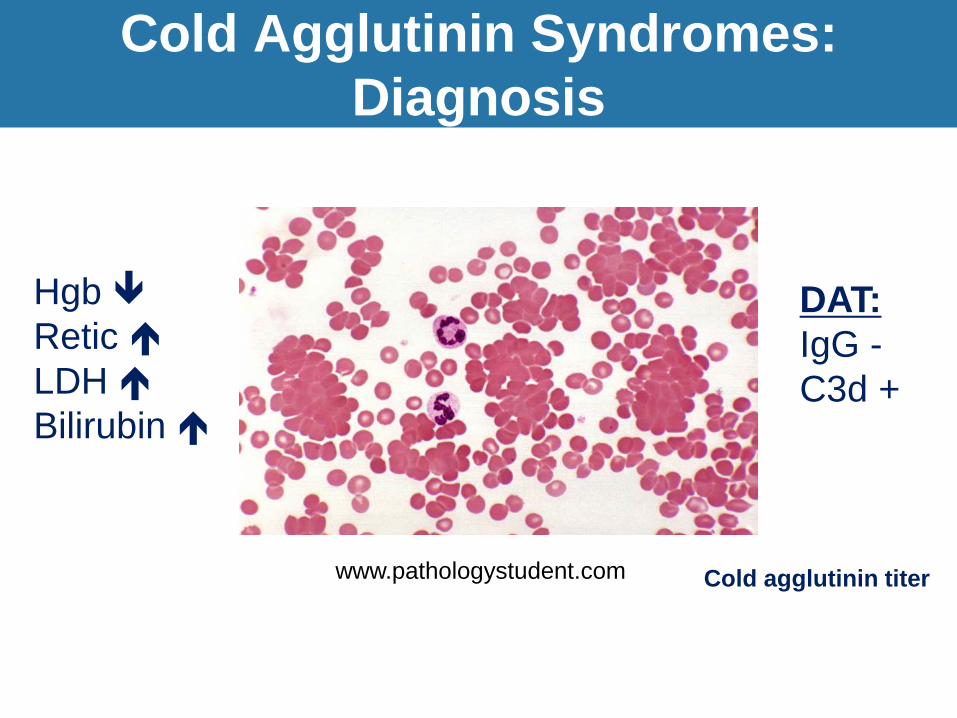
CAS: diagnosis
DAT:IgG -C3d +
Hgb Retic LDH Bilirubin
www.pathologystudent.com Cold agglutinin titer
Cold Agglutinin Syndromes: Diagnosis
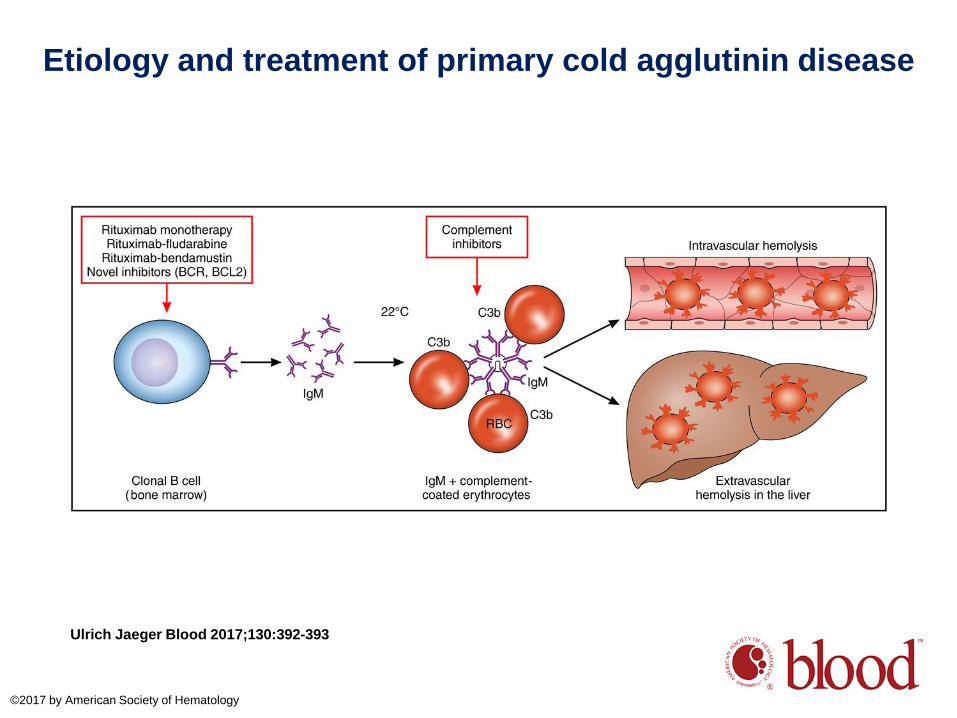
Etiology and treatment of primary cold agglutinin disease
Ulrich Jaeger Blood 2017;130:392-393
©2017 by American Society of Hematology
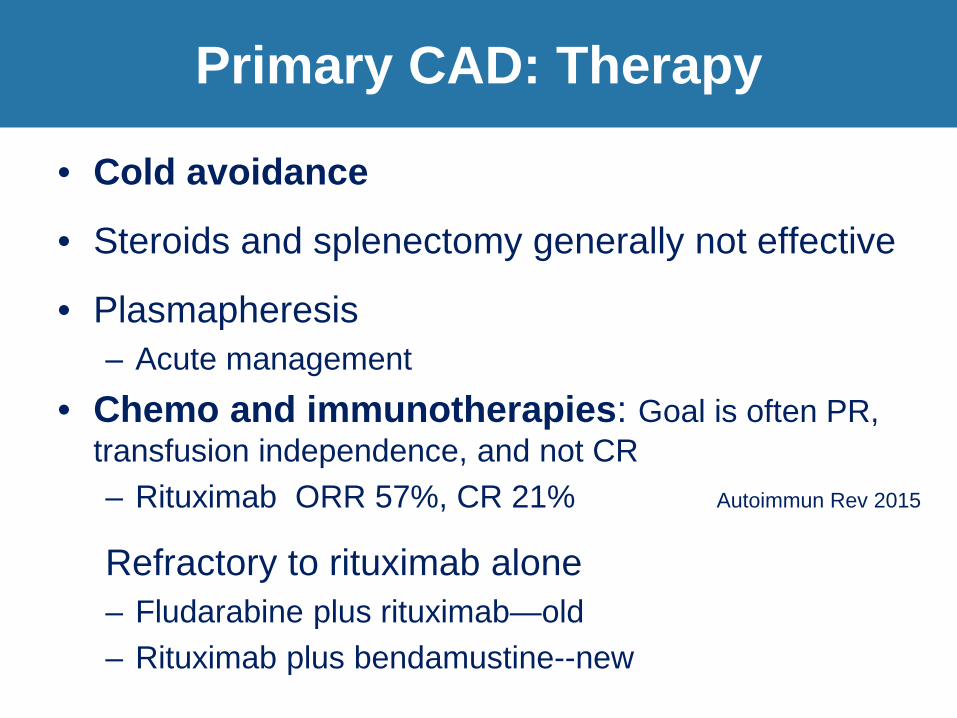
Primary CAD: therapy• Cold avoidance
• Steroids and splenectomy generally not effective
• Plasmapheresis– Acute management
• Chemo and immunotherapies: Goal is often PR, transfusion independence, and not CR– Rituximab ORR 57%, CR 21% Autoimmun Rev 2015
Refractory to rituximab alone– Fludarabine plus rituximab—old– Rituximab plus bendamustine--new
Primary CAD: Therapy
Question 1
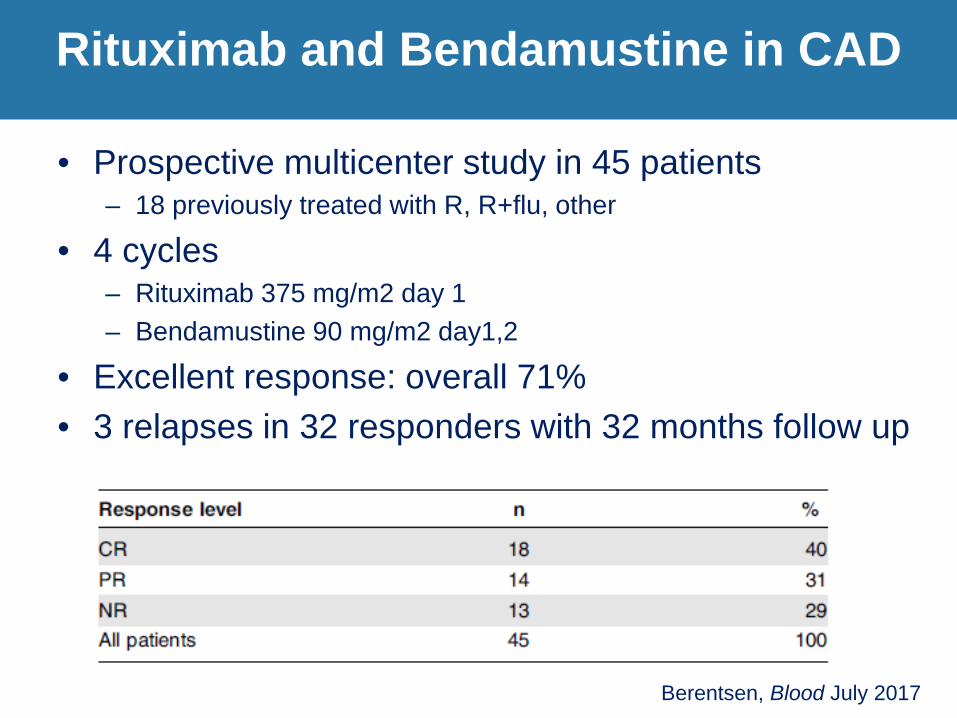
• Prospective multicenter study in 45 patients – 18 previously treated with R, R+flu, other
• 4 cycles– Rituximab 375 mg/m2 day 1– Bendamustine 90 mg/m2 day1,2
• Excellent response: overall 71% • 3 relapses in 32 responders with 32 months follow up
—Q 2Rituximab and Bendamustine in CAD
Berentsen, Blood July 2017
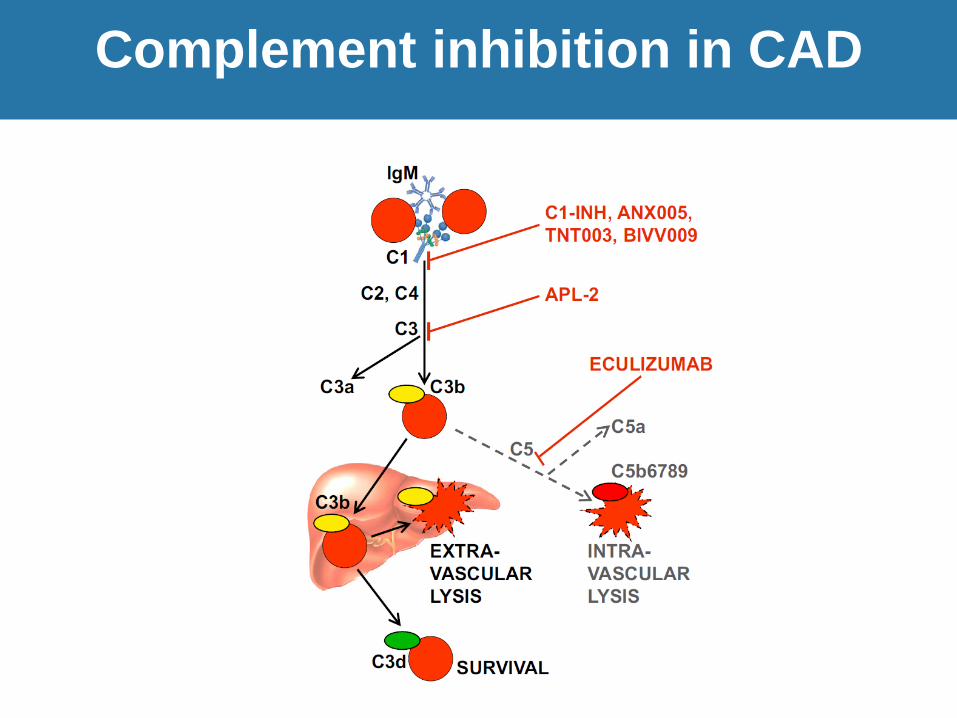
Question 1—Q 2Complement inhibition in CAD

Question 1
• Eculizumab– Case reports – Phase II study in 13 patients: decreased hemolysis
and transfusion requirements ASH 2015
• TNT009– Inhibits C1s in the classical complement pathway– In vitro, mouse, and healthy volunteer studies
demonstrate inhibition of activation of classical complement pathway and formation of C3b
• Both require indefinite treatment or use as bridge until response from other treatments achieved
—Q 2Complement inhibition in CAD
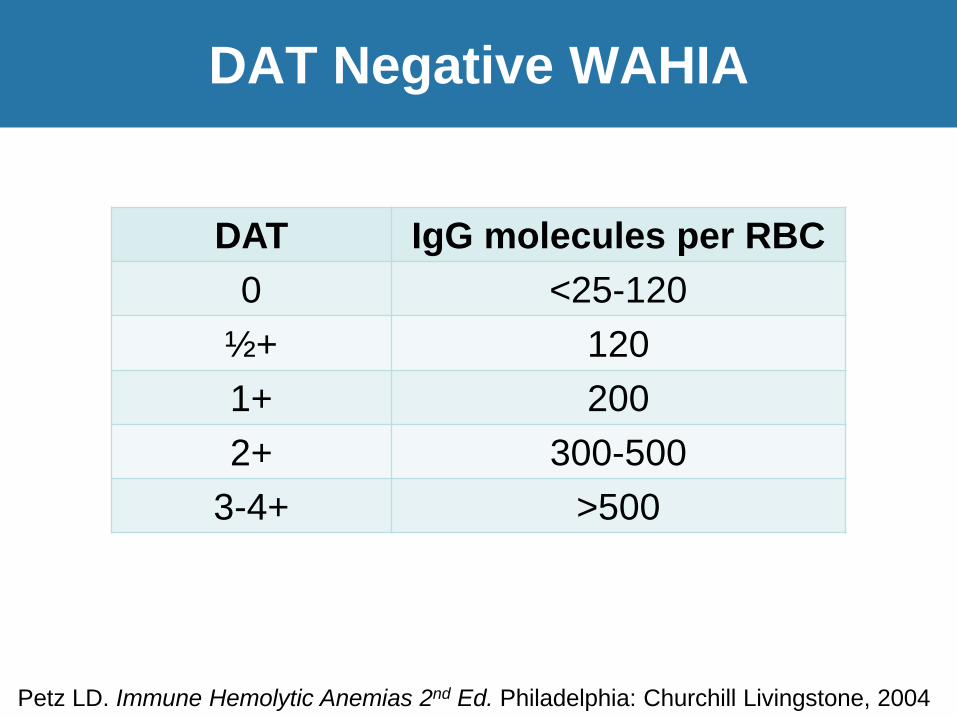
DAT-negative WAIHA
DAT IgG molecules per RBC0 <25-120
½+ 1201+ 2002+ 300-500
3-4+ >500
Petz LD. Immune Hemolytic Anemias 2nd Ed. Philadelphia: Churchill Livingstone, 2004
DAT Negative WAHIA
Hemolytic Anemia: Unanswered questions
1-10% WAIHA cases will have negative Coombs.Reasons for a negative Coombs Test:
• Low titer antibody that is insufficient to agglutinate the cells in a Coombs Test
• Low affinity antibody that is removed with washing during the test
• Alternative isotype antibody that doesn’t react with Coombs sera –IgA: 1-2%
• Patient doesn’t have AIHA
DAT Negative WAHIA

• Enhanced DAT– Many enhanced antibody detection techniques:
• Flow cytometry, low ionic strength wash, polybrene– Detect low concentration of antibody– Detect alternative isotypes – Positive in 90% Coombs negative WAIHA– Negative test does not absolutely rule out WAIHA
– Must also consider alternative diagnosis
DAT Negative WAIHA
Autoimmune Hemolytic Anemia
• Vaccinate prior to splenectomy• Pneumococcus• Haemophilus influenza• Meningococcus• Influenza• Provide prophylactic antibiotics
• Open vs laproscopic?• Portal vein thrombosis rate estimated at 8-50%• No definitive answer for open vs laproscopic• VTE prophylaxis post-op?
• Increased risk over lifetime of thrombosis?• Increased PE, ischemic heart disease
Splenectomy
Jean M. Connors [email protected]