hematologic disorders powerpoint
DESCRIPTION
This presentation talks about hematologic disorders.TRANSCRIPT
Hematologic DisordersHematologic Disorders
Case StudyCase Study
You have been assigned to care for MA.
He is a 4 year old male who was admitted for pneumonia. He is on 1L O2. He is afebrile. HR 136, RR 26, B/P 100/60. Oxygen saturation is 93%. His mother is at the bedside. During shift report you are given information that he is eating and drinking well. His IV fluids were decreased to TKO rate. He is on day 3 of antibiotics.
You complete the 8 am assessment.
Findings: Skin pale and cool to touch. Cap refill 2 seconds. Lethargic. No appetite. Not interested in playing. Lungs with bilateral course sounds. S1 S2 heart sounds with splitting of S2. Generally thin, well appearing child.
What additional information would you like?

Case StudyCase Study
Eats pasta, cheese, crackers, chicken nuggets Eats pasta, cheese, crackers, chicken nuggets and “McDonalds”.and “McDonalds”.
Drinks primarily soda and “Juicy Juice”Drinks primarily soda and “Juicy Juice” No MVINo MVI Favorite activities: “video games”, watching Favorite activities: “video games”, watching
cartoonscartoons Sleeps 16 hours per day. Falls asleep easily Sleeps 16 hours per day. Falls asleep easily
and “eveywhere”and “eveywhere” Lives in “St.Charles”. 70 year old home.Lives in “St.Charles”. 70 year old home. Lives with parents and 8 year old female sibling.Lives with parents and 8 year old female sibling.

CBCCBC
WBC: 6.5 range: 5.5-15.5WBC: 6.5 range: 5.5-15.5
RBC: 4.1 range: 3.1-4.5RBC: 4.1 range: 3.1-4.5
HGB: 10.9 range: >11.5HGB: 10.9 range: >11.5
HCT: 29.5 range: > 33.5HCT: 29.5 range: > 33.5
MCV: 69 range: > 80MCV: 69 range: > 80
MCHC: 19 range: 24-30MCHC: 19 range: 24-30
Retic: 0.8% range: 0.5% – 2.0%Retic: 0.8% range: 0.5% – 2.0%
Iron Related TestsIron Related Tests
Serum ferritin: 2 range: 7-142 ng/mlSerum ferritin: 2 range: 7-142 ng/ml
Total Iron: 30 range: 50-120 mcg/dlTotal Iron: 30 range: 50-120 mcg/dl
Pb LevelPb Level
Lead level: 6 range: <10mg/dlLead level: 6 range: <10mg/dl

Iron Deficiency AnemiaIron Deficiency Anemia
Most common cause of anemiaMost common cause of anemiaDecreased iron intakeDecreased iron intake Increased iron or blood lossIncreased iron or blood loss Increased growthIncreased growthRare before 4-6 months of ageRare before 4-6 months of ageCan be associated with Pb poisoiningCan be associated with Pb poisoiningFamily education is criticalFamily education is critical
The Plan of CareThe Plan of Care
Administer iron (elemental iron)Administer iron (elemental iron) Iron therapy continued for at least 3 months after Hgb Iron therapy continued for at least 3 months after Hgb
has normalizedhas normalized Hgb should increase within 2 weeksHgb should increase within 2 weeks Increase iron rich foodsIncrease iron rich foods Give iron on empty stomach in an acidic environmentGive iron on empty stomach in an acidic environment Clean teeth after iron administrationClean teeth after iron administration Administer iron with vitamin CAdminister iron with vitamin C Black stoolsBlack stools Consider social service referralConsider social service referral
Sickle Cell DiseaseSickle Cell Disease
African Americans, Mediterranean, Indian, African Americans, Mediterranean, Indian, and Middle Eastern individuals affectedand Middle Eastern individuals affected
Trait found in 8% of AATrait found in 8% of AAAutosomal recessiveAutosomal recessiveSickle cell trait individuals may be Sickle cell trait individuals may be
symptomatic under extreme conditionssymptomatic under extreme conditions
Genetic TransmissionGenetic Transmission
1 parent (+) and 1 parent (-) then,1 parent (+) and 1 parent (-) then,
50% risk trait50% risk trait
2 parents (+) then,2 parents (+) then,
25% unaffected, 25% disease, 50% trait25% unaffected, 25% disease, 50% trait

PathophysiologyPathophysiology
PathophysiologyPathophysiology
HbSHbS Increased RBC destructionIncreased RBC destructionDecreased RBC lifespanDecreased RBC lifespanMicrocirculation obstructionsMicrocirculation obstructionsHigh reticulocyte countHigh reticulocyte countBrain, Heart, Kidney, Eye, SpleenBrain, Heart, Kidney, Eye, Spleen

ManifestationsManifestations Stressful event causes sickling crisis (deoxygenation, acidosis, Stressful event causes sickling crisis (deoxygenation, acidosis,
dehydration)dehydration) Vaso-occlusive, acute sequestration, or aplastic crisisVaso-occlusive, acute sequestration, or aplastic crisis InfectionInfection Delayed growth/pubertyDelayed growth/puberty Pallor, jaundice, fatiguePallor, jaundice, fatigue Avascular necrosis of hips and shouldersAvascular necrosis of hips and shoulders Renal dysfunctionRenal dysfunction RetinopathyRetinopathy PriapismPriapism Cerebral InfarctCerebral Infarct Acute chest syndromeAcute chest syndrome CardiomyopathyCardiomyopathy

PAIN!!!!
Nursing ManagementNursing Management
Fever (>101.3)Fever (>101.3)IV Abx, cultures, hydrationIV Abx, cultures, hydration
Prophylactic penicillin therapyProphylactic penicillin therapy Influenza and pneumovax vaccineInfluenza and pneumovax vaccine Oxygen therapyOxygen therapy HydrationHydration Strict I and OStrict I and O TransfusionTransfusion Pain ManagementPain Management

General Patient Education General Patient Education GuidelinesGuidelines
Fluid IntakeFluid IntakeFrequent urinationFrequent urinationDiscuss risk for infectionDiscuss risk for infection Importance of primary careImportance of primary careCaution against extremes in temperatureCaution against extremes in temperaturePain ManagementPain ManagementAdequate RestAdequate Rest
Beta-ThalassemiaBeta-Thalassemia
Thalassemia majorThalassemia major or or Cooley’s anemiaCooley’s anemiaBeta-polypeptide chain abnormalityBeta-polypeptide chain abnormalityAbnormality of Hgb synthesis resulting in Abnormality of Hgb synthesis resulting in
hemolysis of erythrocyteshemolysis of erythrocytesExagerrated RBC production Exagerrated RBC production
(erythropoiesis)/destruction(hemolysis)(erythropoiesis)/destruction(hemolysis) Increased intestinal absorption of iron Increased intestinal absorption of iron
resulting in hemosiderosisresulting in hemosiderosis
Etiology and IncidenceEtiology and Incidence
Autosomal recessiveAutosomal recessiveCan have mild expression of geneCan have mild expression of gene
thalassemia minorthalassemia minorMediterranean descent primarily affectedMediterranean descent primarily affected


Clinical ManifestationsClinical Manifestations
Frontal bossingFrontal bossing Maxillary prominenceMaxillary prominence Wide-set eyesWide-set eyes Flat noseFlat nose HepatosplenomegalyHepatosplenomegaly Jaundice, pallorJaundice, pallor Growth retardationGrowth retardation Severe anemiaSevere anemia

Therapeutic ManagementTherapeutic Management
RBC transfusionRBC transfusion
Chelation therapy (deferoxamine)Chelation therapy (deferoxamine)
SplenectomySplenectomy
Bone Marrow TransplantBone Marrow Transplant

Nursing InterventionsNursing Interventions
OxygenationOxygenation Monitor Hgb level, iron levelMonitor Hgb level, iron level HydrationHydration Management of sequelae of hemosiderosisManagement of sequelae of hemosiderosis Chelation therapy educationChelation therapy education Psychosocial supportPsychosocial support Vigilant primary care (immunizations, prompt Vigilant primary care (immunizations, prompt
treatment of infection, etc.)treatment of infection, etc.) Genetic counselingGenetic counseling
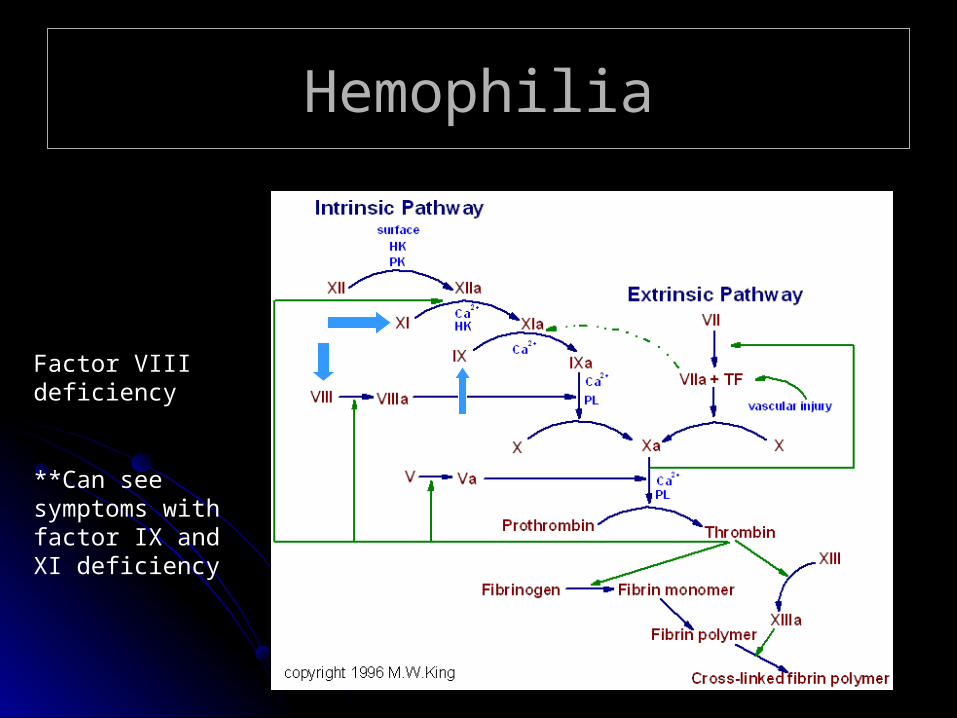
HemophiliaHemophilia
Factor VIII deficiency
**Can see symptoms with factor IX and XI deficiency

EtiologyEtiology
X-linkedX-linked
Autosomal recessiveAutosomal recessive

ManifestationsManifestations
EpistaxisEpistaxisBleeding gumsBleeding gumsHematuriaHematuriaPetechiaPetechiaFrequent bruisingFrequent bruisingMuscle/joint bleedingMuscle/joint bleedingCircumcision bleeding excessiveCircumcision bleeding excessive


Diagnostic EvaluationDiagnostic Evaluation
Quantitative immunoelectrophorectic Quantitative immunoelectrophorectic assayassay
Factors VIII and IX assaysFactors VIII and IX assaysPlatelet countPlatelet countFibrinogen levelFibrinogen levelBleeding timeBleeding timePTPTPTTPTT

ManagementManagement
Avoid rectal temperature measurementAvoid rectal temperature measurement Measure the affected joint/extremityMeasure the affected joint/extremity Assess LOCAssess LOC Apply gentle pressure to superficial woundsApply gentle pressure to superficial wounds Administer factor (prophylactically)Administer factor (prophylactically) Administer clot stabilizing medicationAdminister clot stabilizing medication RICERICE Consider co-morbidity (Consider co-morbidity (??)) Extensive family education (safe environment, prompt Extensive family education (safe environment, prompt
treatment, acceptable activities, medication education)treatment, acceptable activities, medication education)

Von Willebrand’s DiseaseVon Willebrand’s Disease
Most common inherited bleeding disorderMost common inherited bleeding disorder Autosomal dominant inheritedAutosomal dominant inherited Dysfunction of Von Willebrand’s proteinDysfunction of Von Willebrand’s protein
(carrier protein for VIII and co-factor for platelet (carrier protein for VIII and co-factor for platelet binding to endothelial tissue)binding to endothelial tissue)
Variable severityVariable severity Prolonged bleedingProlonged bleeding Treat with DDAVPTreat with DDAVP FFP and cryoprecipitate prophylacticallyFFP and cryoprecipitate prophylactically Family educationFamily education
Immune Thrombocytopenic Immune Thrombocytopenic PurpuraPurpura
Acquired bleeding disorderAcquired bleeding disorder? Autoimmune? AutoimmunePlatelet < 150,000, purpuric rash, normal Platelet < 150,000, purpuric rash, normal
bone marrowbone marrowTreatment: watchful waiting, IVIG, Treatment: watchful waiting, IVIG,
steroids, platelet transfusionsteroids, platelet transfusion

Nursing InterventionsNursing Interventions
Soft tooth brushSoft tooth brush Gentle pressure to superficial woundsGentle pressure to superficial wounds Monitor labs (?)Monitor labs (?) Discuss home environment/safe environmentDiscuss home environment/safe environment Appropriate play activities for diagnosis and Appropriate play activities for diagnosis and
developmental agedevelopmental age Steroid use education (risk for infection, tapering Steroid use education (risk for infection, tapering
medication)medication) Caregiver supportCaregiver support Reinforce need for vigilant follow-up Reinforce need for vigilant follow-up IVIG – delay MMR for at least 10 monthsIVIG – delay MMR for at least 10 months Avoid medications that affect platelet functionAvoid medications that affect platelet function

Pediatric HIV InfectionPediatric HIV Infection
9000 children < age 13 diagnosed (2001)9000 children < age 13 diagnosed (2001)Transmission: perinatal = 90%Transmission: perinatal = 90%Other causes: blood products, abuseOther causes: blood products, abuseAfrican American and Latinos affectedAfrican American and Latinos affectedHalf of new diagnosis in the US occur in Half of new diagnosis in the US occur in
adolescents age 15-24 yearsadolescents age 15-24 yearsChronic conditionChronic condition

Vertical TransmissionVertical Transmission
General risk is multifactoral (viral load, PROM, General risk is multifactoral (viral load, PROM, prematurity, low birth weight, treatment regimen)prematurity, low birth weight, treatment regimen)
Combination therapy with Protease Inhibitors = Combination therapy with Protease Inhibitors = risk of transmission 1%risk of transmission 1%
General risk without treatment = 20-25%General risk without treatment = 20-25% No breastfeedingNo breastfeeding Prenatal diagnosis of HIV criticalPrenatal diagnosis of HIV critical Consider mandatory screening of all newbornsConsider mandatory screening of all newborns

Pediatric Specific ManifestationsPediatric Specific Manifestations
Typically faster progressionTypically faster progression Higher viral load Higher viral load FTT and developmental delay is a common FTT and developmental delay is a common
findingfinding High risk for PCP (start prophylaxis empirically)High risk for PCP (start prophylaxis empirically) Lymphocytic interstitial pneumonitisLymphocytic interstitial pneumonitis Higher CD4 counts indicate severe immune Higher CD4 counts indicate severe immune
suppression (<750 in children under 1 year of suppression (<750 in children under 1 year of age) Review table 41-1 p. 1053age) Review table 41-1 p. 1053
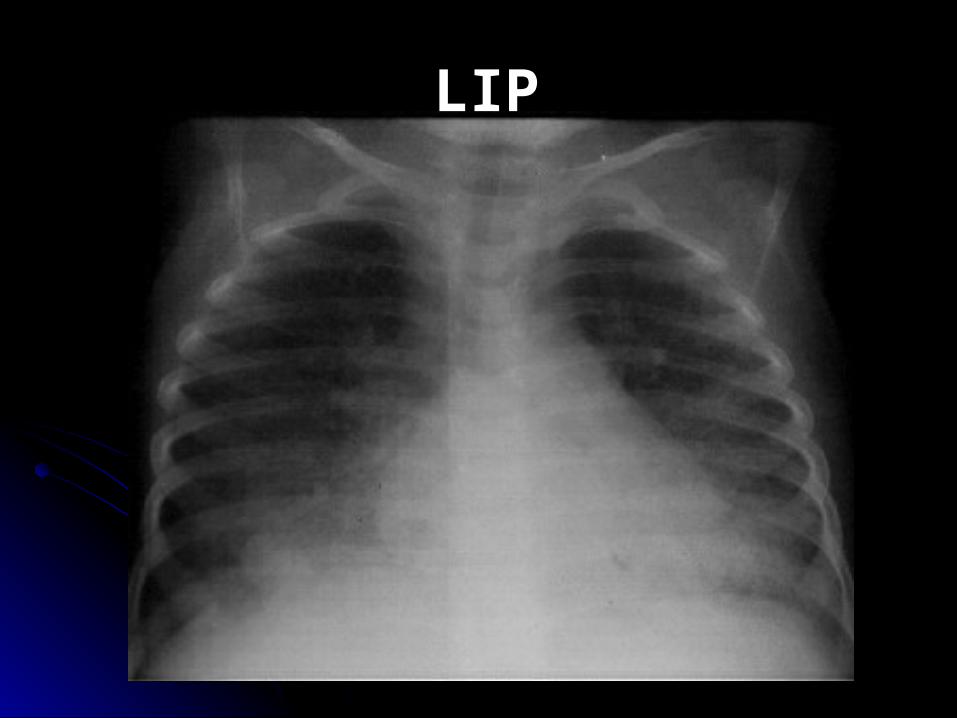
LIP

Other ManifestationsOther Manifestations
LymphadenopathyLymphadenopathy HepatosplenomegalyHepatosplenomegaly Recurrent URI, otitis media, sinusitisRecurrent URI, otitis media, sinusitis ParotitisParotitis CardiomyopathyCardiomyopathy Chronic diarrhea/malabsorptionChronic diarrhea/malabsorption Peripheral neuropathyPeripheral neuropathy Persistent candidiasisPersistent candidiasis Skin InfectionsSkin Infections
Pediatric DiagnosisPediatric Diagnosis
Elisa and Western Blot (after 18 mos.)Elisa and Western Blot (after 18 mos.)PCR: qualitative and quantitativePCR: qualitative and quantitativeKnown exposed: test within 48 hoursKnown exposed: test within 48 hoursPositive result confirmed with a repeat Positive result confirmed with a repeat
assayassayNegative at birth: test at 1-2 months, 6 Negative at birth: test at 1-2 months, 6
months, and 18 monthsmonths, and 18 months If positive: use CD4 and viral load to If positive: use CD4 and viral load to
assess response to therapyassess response to therapy

PCP ProphylaxisPCP Prophylaxis
Initiate on exposed infant at 4-6 weeksInitiate on exposed infant at 4-6 weeksTrimethoprim-sulfamethoxazoleTrimethoprim-sulfamethoxazoleContinue until definitive negative diagnosisContinue until definitive negative diagnosisCan administer M-W-F, or 1 dose dailyCan administer M-W-F, or 1 dose dailySpecific caregiver educationSpecific caregiver education

ImmunizationsImmunizations
Consider immune status when immunizingConsider immune status when immunizingPneumococcal and Influenza requiredPneumococcal and Influenza requiredFollow usual immunization scheduleFollow usual immunization scheduleConsider Varicella although often Consider Varicella although often
contraindicatedcontraindicatedMMR allowed if health immune systemMMR allowed if health immune system If exposed to varicella, give immune- If exposed to varicella, give immune-
globulin (V-zig) within 24-48 hoursglobulin (V-zig) within 24-48 hours

Nursing ManagementNursing Management
Continual and repeated educationContinual and repeated education Assistance with adherence to medication regimen (HAART)Assistance with adherence to medication regimen (HAART) Psychosocial assessment and attention to the individual patient and Psychosocial assessment and attention to the individual patient and
family needsfamily needs Disclosure (when to, when not to)Disclosure (when to, when not to) Dispelling mythsDispelling myths Integrating cultural practices, family beliefs, and resources into the Integrating cultural practices, family beliefs, and resources into the
plan of careplan of care Education regarding transmission precautionsEducation regarding transmission precautions Nutrition (high calorie, high protein)Nutrition (high calorie, high protein) Support respiratory statusSupport respiratory status Skin careSkin care Develop a plan that allows the child to maximize function for as long Develop a plan that allows the child to maximize function for as long
as possibleas possible

Specific Adolescent IssuesSpecific Adolescent Issues
Isolating nature of the diseaseIsolating nature of the diseaseLoss of other affected family membersLoss of other affected family membersDisclosure (dating, intimacy, life planning)Disclosure (dating, intimacy, life planning) Incorporate the adolescent into decision Incorporate the adolescent into decision
making processmaking processMedication educationMedication educationPromoting integration with peersPromoting integration with peers
Systemic Lupus ErythematousSystemic Lupus Erythematous
Frequent onset at puberty (9-15 years)Frequent onset at puberty (9-15 years) Uncommon in children <10 yearsUncommon in children <10 years More common in females: approx. 8:1More common in females: approx. 8:1 More common in African American, Asian, and More common in African American, Asian, and
Latino descentLatino descent Characterized by exacerbation:remissionCharacterized by exacerbation:remission More severe in childrenMore severe in children 5-year survival: 90% with renal disease5-year survival: 90% with renal disease
100% without renal disease100% without renal disease
EtiologyEtiology
Genetic predispositionGenetic predisposition Immune system dysregulationImmune system dysregulationEnvironmental stimuli (triggers)Environmental stimuli (triggers)Hormonal influencesHormonal influencesMultisystem, autoimmune diseaseMultisystem, autoimmune diseaseVariability in disease severityVariability in disease severity

ManifestationsManifestations
1997 American College of Rheumatology1997 American College of Rheumatology
Specific ManifestationsSpecific Manifestations
Malar rashMalar rashNephritis: proteinuria >0.5 g/d, cellular castsNephritis: proteinuria >0.5 g/d, cellular castsSeizures Seizures PsychosisPsychosisPleuritisPleuritisPericarditisPericarditis

ManagementManagement Immunosuppression (steroids, Cytoxan)Immunosuppression (steroids, Cytoxan) Support symptomsSupport symptoms Monitor vital sign trendsMonitor vital sign trends Caution with live vaccine administration particularly with Caution with live vaccine administration particularly with
immunecompromoised statusimmunecompromoised status Hep B, influenza, pneumococcalHep B, influenza, pneumococcal Nephritis = low NA diet (2gm/day), may have HTN as a result of Nephritis = low NA diet (2gm/day), may have HTN as a result of
renal involvementrenal involvement Avoid alfalfa (trigger)Avoid alfalfa (trigger) Sun ProtectionSun Protection Physical therapyPhysical therapy Individualized psychosocial plan based on type and severity of Individualized psychosocial plan based on type and severity of
symptomssymptoms Family education (medication, triggers, natural history of disease, Family education (medication, triggers, natural history of disease,
integrating illness into life goals)integrating illness into life goals)
Pediatric ConsiderationsPediatric Considerations
Most frequent cause of death with SLE = Most frequent cause of death with SLE = overwhelming infectionoverwhelming infection
Team approach to care (social work is a critical Team approach to care (social work is a critical component)component)
Reinforce early intervention of any symptomsReinforce early intervention of any symptoms Always assess mouth for ulcers (early sign of Always assess mouth for ulcers (early sign of
exacerbation)exacerbation) Caution against pregnancy, OCP use and Caution against pregnancy, OCP use and
possible exacerbations related to hormonal possible exacerbations related to hormonal shifts (adolescent)shifts (adolescent)
