heavy metal treatment: using instruments for soft tissue...
TRANSCRIPT

Heavy Metal Treatment: Using Instruments for Soft
Tissue Mobilization Phillip Vardiman, PhD, LAT, ATC
Assistant Professor University of Kansas
Department of Health, Sport and Exercise Sciences Applied Physiology Laboratory
Background • Assistant Professor University of
Kansas • Graston Technique M1 Instructor to
KU Athletic Training Education Program
• Graston Module 1 and 2 • No funding for research has been
provided by GT or other company
IASTM
Overview
What is Instrument Assisted Soft Tissue Mobilization (IASTM)
History
Clinical Indications
Research Overview
Clinical Applications
Discussion
Questions

Instrument Assisted Soft Tissue Mobilization
A therapeutic modality and manual therapy technique that when combined with rehabilitative exercises improves musculoskeletal function.
History of IASTM
Gua Sha-(Gwah Shah) Gau = Scrape, Scratch and Sha= Sand(the reddening, petechiae that occurs) A.K.A. Coining, Spooning, Scraping
Cao Gio(Vietnam)- (ceow yah) Catch the wind
Kerokan(Indonesia)- coining, spooning, scraping
Traditional East-Asian Alternative Medicine
The use of an instrument to cause friction at the skin surface Transitory Petechiae Ecchymosis Thought to bring the static blood,
“wind”, or bad spirit from the body so that it can be carried away

IASTM
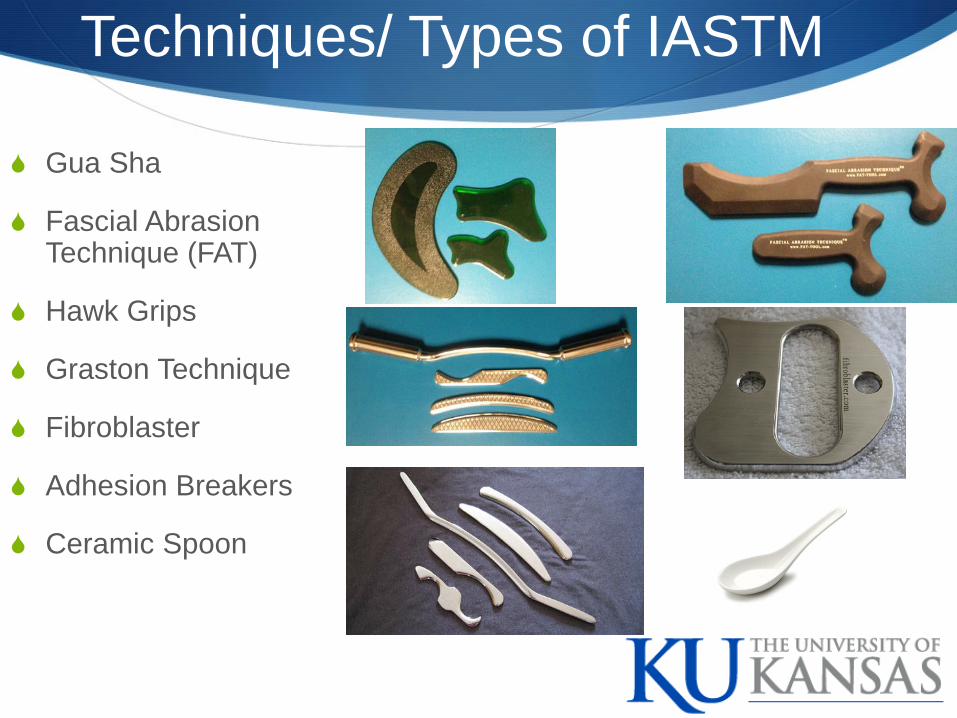
Gua Sha
Fascial Abrasion Technique (FAT)
Hawk Grips
Graston Technique
Fibroblaster
Adhesion Breakers
Ceramic Spoon
Techniques/ Types of IASTM
Clinical Indications
Pain
Soft Tissue Injury
Small and Large Treatment Areas
Decreased Range of Motion
Scar Tissue Restriction of motion Excessive Scarring (Keloid,
Hypertropic)
Fascial Restrictions
Unsuccessful Treatment With Traditional Cross-Fiber Massage or Therapeutic Massage
Tendinopathies Lateral Epicondylosis Medial Epicondylosis Supraspinatus Tendinosis Achilles Tendinosis Dequervains Syndrome Patellar Tendinosis
Fascial Syndromes Plantar fascitis ITB Syndrome Compartment Syndromes Trigger Fingers
Clinical Indications (Cont.)
Relative Contraindications Cancer
Burn Scars (Mature scars 9 months post-healing
Kidney dysfunction
Pregnancy
Medications, Anticoagulants, Steroids, hormone replacements, NSAIDS
Rheumatoid arthritis
Varicose veins

Absolute Contraindications
Open Wounds/ Unhealed suture sites/ sutures
Thrombophlebitis
Uncontrolled Hypertension
Inflammatory conditions due to infection
Contagious or infectious skin conditions
Hematoma/ Myositis Ossificans
Osteomyelitis
Unstable fractures

Research Overview Butterfield (2008) MSSE
Rabbit Model Cyclic Compression improved function, attenuated necrosis and
leukocyte infiltration following EEP
Haas et al. (2013) BJSM Rabbit Model Dose Dependent (N, Hz, Time) MLL aided recovery in active muscle
properties in rabbits
Loghmani and Warden 2009 Rat MCL complete disruption. Found the IASTM accelerated healing
Davidson et al. 1995 Functional assessment of rats after achilles tendon injury Found increased fibroblast proliferation with use of IASTM
1. Haas et al. Br J Sports Med 2013: 47:83-88 2. Cunningham and Butterfield; ASWEB.ORG
Research Overview
Vardiman, Siedlik, Hawkins, Herda, Cooper, and Gallagher (2013) Intramuscular Response to IASTM IASTM to Gastroc/Soleus Complex MTS, EMG, MMG, ROM, PT, PFAQ
Take Home IL-6 and TNF-α(p>0.05) Inflammatory Intramuscular
Myokines Passive and Active Muscle Properties are still being
analyzed (Stay tuned……..)
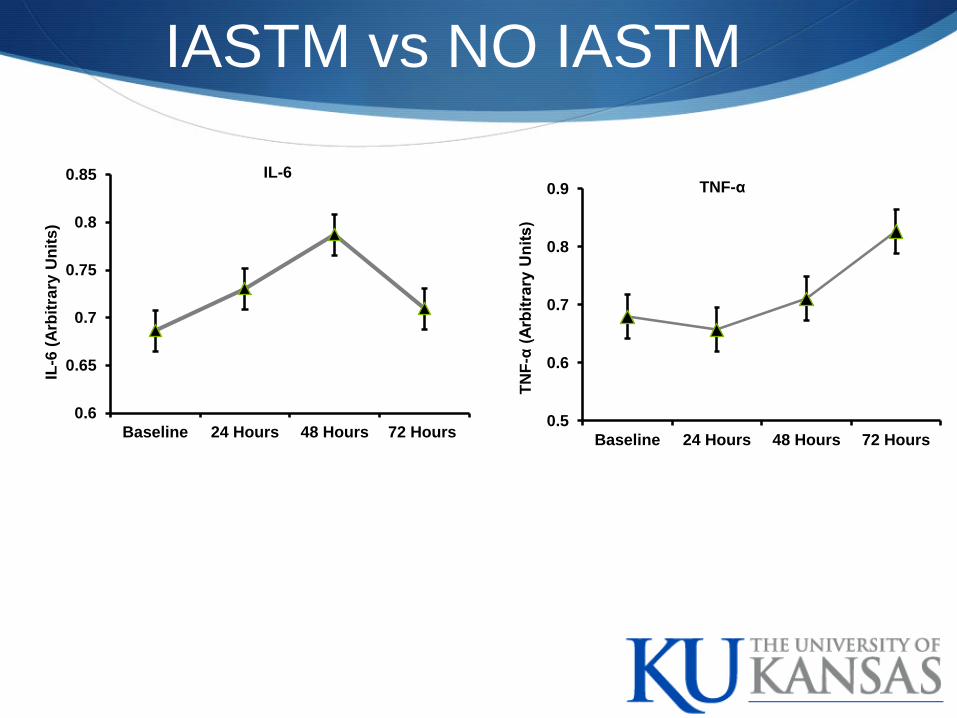
IASTM vs NO IASTM
0.5
0.6
0.7
0.8
0.9
Baseline 24 Hours 48 Hours 72 Hours
TNF-α
TNF-
α (A
rbitr
ary
Uni
ts)
0.6
0.65
0.7
0.75
0.8
0.85
Baseline 24 Hours 48 Hours 72 Hours
IL-6
IL-6
(Arb
itrar
y U
nits
)
Research Overview
Vardiman, Andre, Maresh, Graham, Gallagher, Moodie, and Moodie (2012) Functional Squat Test Pre/Post IASTM to
Functional Squat Test 3-D Motion Capture Assessment (ROM) and
PFAQ
Take Home No change in Functional Squat Performance No change in perception of functional abiltiy

IASTM, Functional Assessment, Perception of Functional Ability

Vardiman, Graham, Siedlik, Herda, Moodie, & Gallagher (2013) IASTM following SL-EEP Muscle Biopsies at 24 and 48 hours ROM, SL-1RM, Pressure Tolerance Found
SL1RM (P<0.001) PT (P=0.009) ROM (P=0.003) Greater in TL vs. CL and was significantly
greater over time (P<0.001) IL-6 and TNF-α (P>.05)
Take Home IASTM attenuated the decrease in ROM following EEP
Research Overview
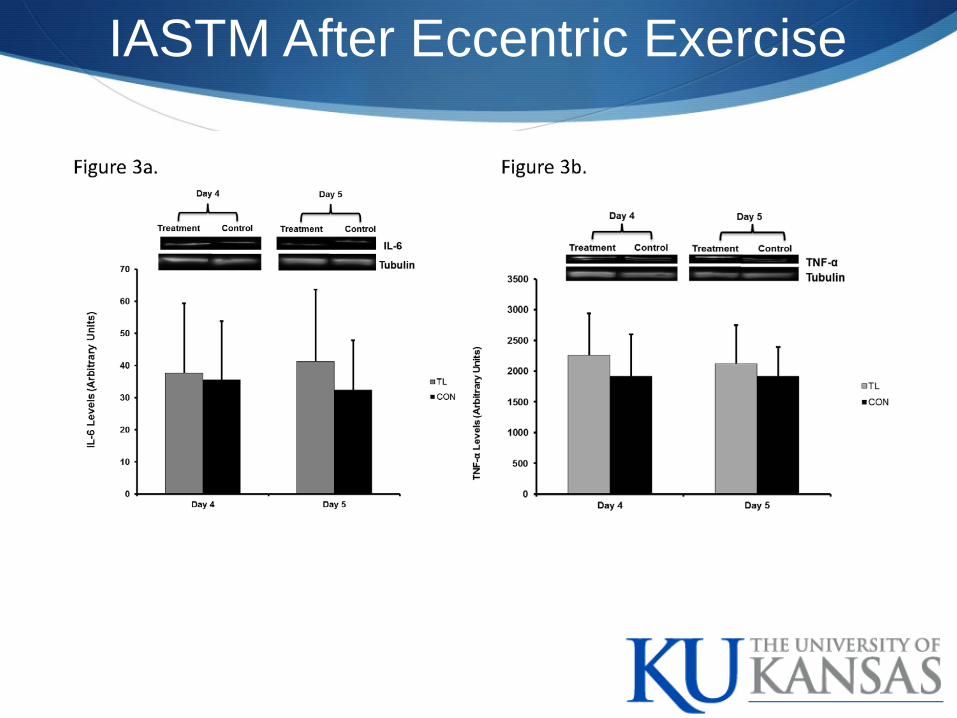
IASTM After Eccentric Exercise
Case studies have shown Graston Technique® to relieve symptoms of….
carpal tunnel syndrome (Baker, 1999; Burke, 2007)
lateral epicondylitis (Haller, 1999)
achilles tendonitis (Hammer, 2008)
plantar fasciitis (Hammer, 2008)
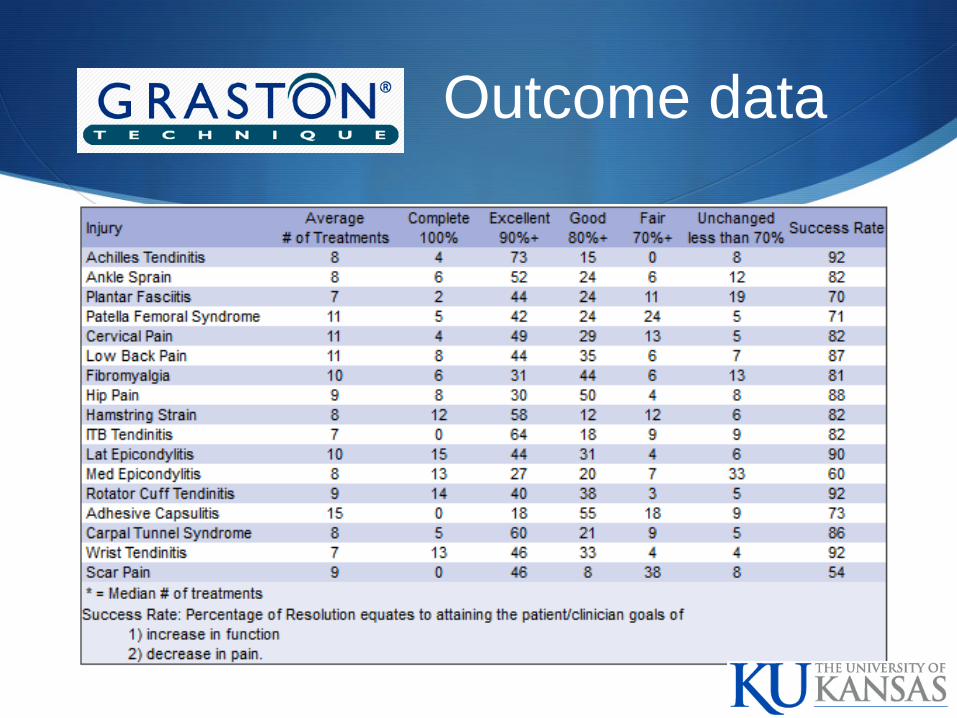
Outcome data
60 subjects (20 in each group)
Hip adduction ROM increased 25% in GISTM group 15% in Gua Sha
Holtz BJ, Davey K, Engleman N, Kaeser C, Wood-Vossmer K, Bayliss AJ, Loghmani MT.
3 patients
Patients achieved a mean decrease in pain of 3/10 per the NPRS
Mean improvement of 11.2% LEFS Score 0 Minimum Score Score 80 Maximum score Lower the score greater the disability Minimal Clinically Important Difference = 9 scale points (11%)
Journal of Manipulative and Physiological Therapeutics (JMPT). 2011 Feb; 138-142.
10 patients
Numeric Pain Rating Scale - baseline to follow-up (p=.002)
Lower Extremity Functional Scale – baseline to follow-up (p=.017)
Global Rating of Change Score – 70% improved outcomes
GISTM used in combination with Dynamic Balance Training had the greatest effect on Foot and Ankle Ability Measure (FAAM), visual analog scale (VAS) ankle ROM in 4 directions Star Excursion Balance
Indicates GISTM may be of benefit in treatment of CAI

5 treatment sessions
20% increase in LEFS
Decreased “at worst” pain rating from 7/10 to 3/10
APTA Combined Sections Meeting [poster presentation]. Chicago (IL). 2012 Feb.

Case Study
Warren, AJ. (2013) Effects of Graston Technique IASTM in the Treatment of Chronic Exertional Compartment Syndrome of the Lower Leg: A Case Study. Found
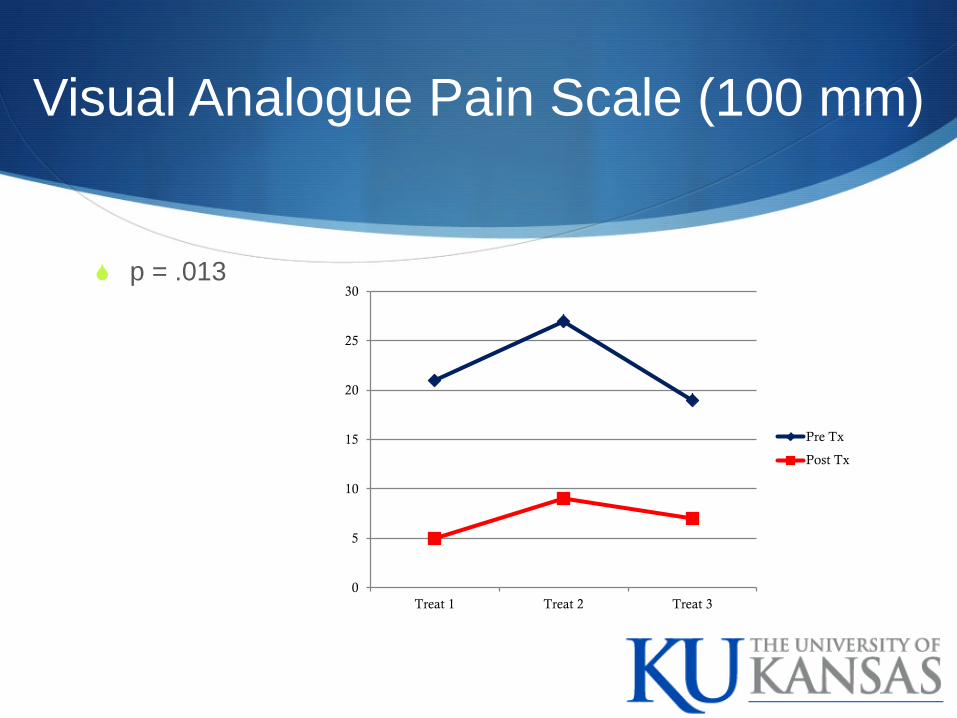
Visual Analogue Pain Scale (100 mm)
p = .013
0
5
10
15
20
25
30
Treat 1 Treat 2 Treat 3
Pre Tx
Post Tx
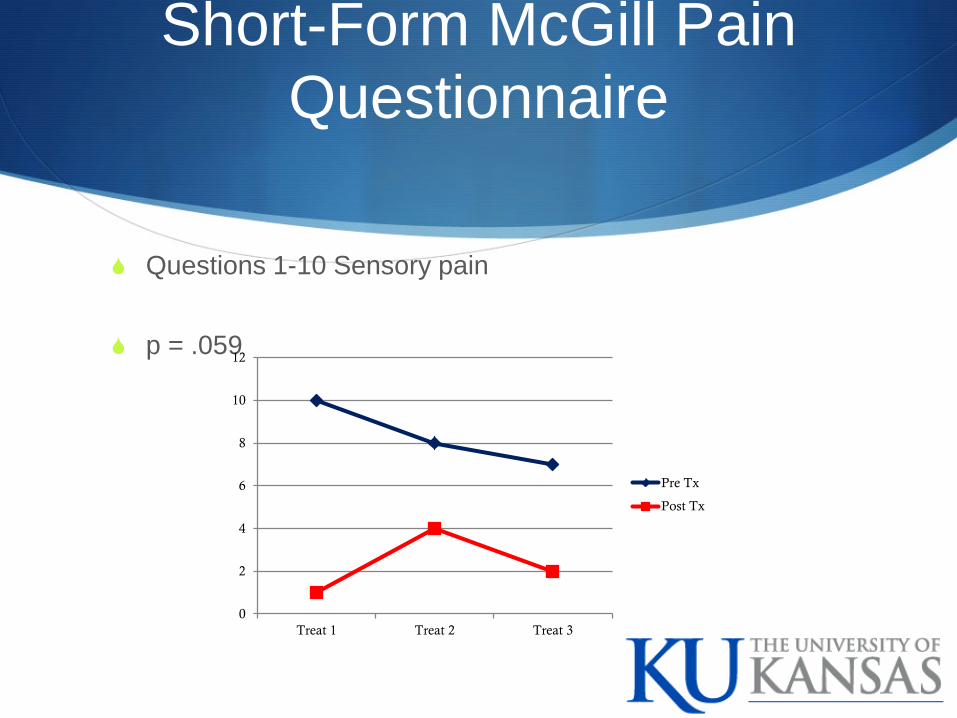
Short-Form McGill Pain Questionnaire
Questions 1-10 Sensory pain
p = .059
0
2
4
6
8
10
12
Treat 1 Treat 2 Treat 3
Pre Tx
Post Tx

Present Pain Index (PPI)
p = .038
5 = Excruciating 4 = Horrible 3 = Distressing 2 = Discomforting 1 = mild pain 0 = no pain
0
0.5
1
1.5
2
2.5
Treat 1 Treat 2 Treat 3
Pre Tx Post Tx
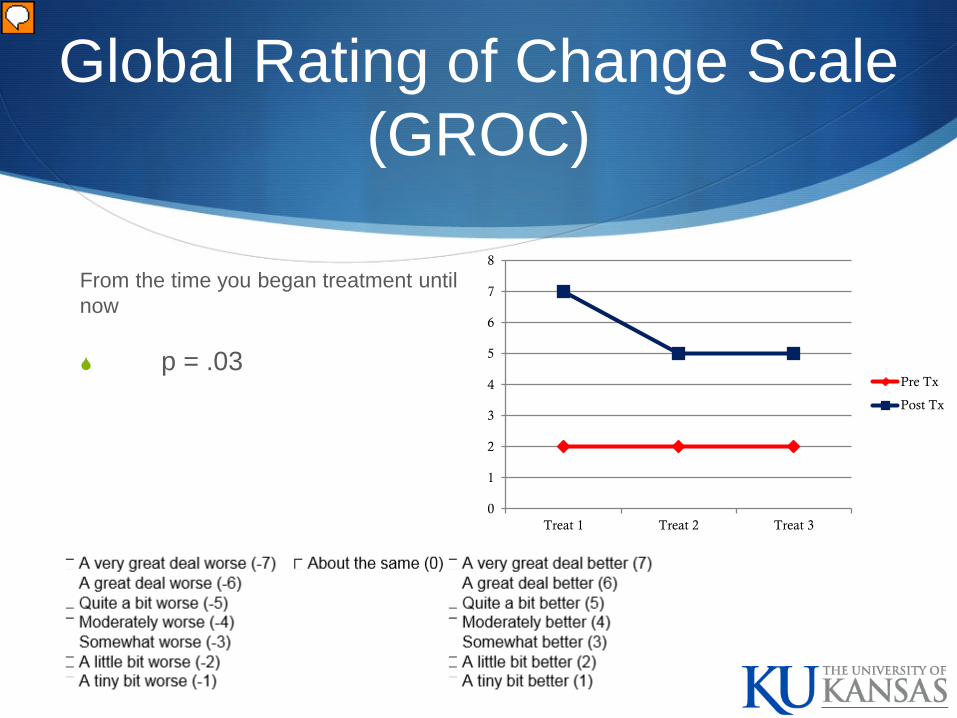
Global Rating of Change Scale (GROC)
From the time you began treatment until now
p = .03
0
1
2
3
4
5
6
7
8
Treat 1 Treat 2 Treat 3
Pre Tx
Post Tx

Flexibility rating out of 10 max
p = .42
Treat 1 Treat 2 Treat 3
Pre Tx 5 6 5
Post Tx 6 6 5
4.44.64.8
55.25.45.65.8
66.2
Fle
xibi
lity
Chart Title
Perceived Functional Ability Questionnaire (PFAQ)
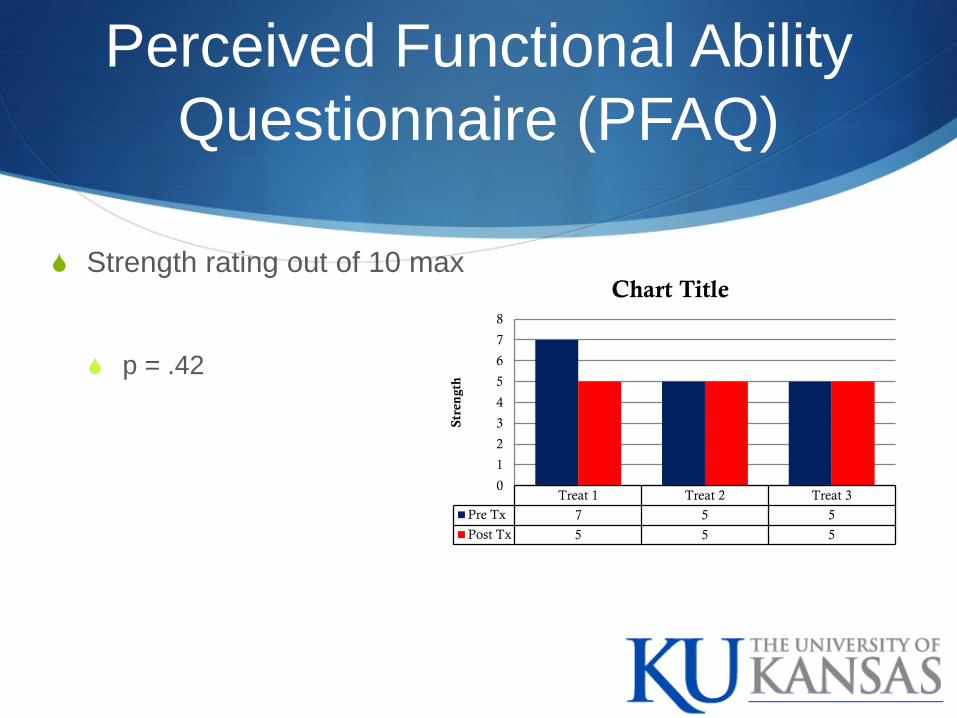
Perceived Functional Ability Questionnaire (PFAQ)
Strength rating out of 10 max
p = .42
Treat 1 Treat 2 Treat 3
Pre Tx 7 5 5
Post Tx 5 5 5
0
1
2
3
4
5
6
7
8
Stre
ngt
h
Chart Title

IASTM
Musculotindinous Stiffness
EMG / MMG
Electromechanical Delay
Rate of Force Development Slope of the torque-time curve (∆ torque / ∆ time)
Rate of Velocity Development Slope of the velocity-time curve (∆ velocity / ∆ velocity)

Questions?