heart failure management: 2013 update richard z aramini, pharmd pgy-1 pharmacy resident february 19...
TRANSCRIPT

Heart Failure Management:2013 Update
Richard Z Aramini, PharmD PGY-1 Pharmacy ResidentFebruary 19th, 2014
1

Disclosure Statement
• I, Richard Z Aramini, have nothing to disclose or possess any conflict of interest in this presentation.
2
Objectives
• Be able to identify the basic pathophysiology of Heart Failure
• Describe the efficacy and pharmacological effects of various agents used to manage HF
• Employ a treatment plan for patients with various stages of HF
3
Take Home Messages
• Be familiar with what’s new
• Know when to use specific agents
• Learn something interesting
4

Fundamentals
“The minute you get away from fundamentals – whether its proper technique, work ethic or mental preparation – the bottom can fall out of your game, your schoolwork, your job, whatever you’re doing.”
― Michael Jordan
6
Overview• Epidemiology /Pathophysiology Review
• Etiology of Heart Failure
• Treatment by Stage
• Changes from 2013 Guidelines
• Review of Agents
7

Guidelines2005: ACCF/AHA Guideline Update for the Diagnosis and Management of Chronic Heart
Failure
2006: CCS consensus conference recommendations on heart failure
2008: ESC guidelines for the diagnosis and treatment of acute and chronic heart failure
2009: Update on ACCF/AHA Heart Failure Guidelines
2010: HFSA Comprehensive Heart Failure Practice Guideline
2012: CCS Heart Failure Management Guidelines Update
2012: ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure
2013: ACCF/AHA Guideline for the Management of Heart Failure
ACCF/AHA: The American College of Cardiology/ American Heart AssociationCCS: Canadian Cardiovascular SocietyESC: European Society of CardiologyHFSA: Heart Failure Society of America
8

Epidemiology of Heart Failure• Lifetime risk: 20% for Americans >40 years of age• 20 per 1,000 individuals age 65-69• >80 per 1,000 individuals age 85+
• 5.1 million Americans with clinical heart failure• >650,000 new cases diagnosed annually• Incidence has remained stable over last several decades
• Relative Risk (NHANES I)• Coronary Heart Disease: RR: 8.1• Diabetes: RR: 1.9• Cigarette Smoking: RR: 1.6• Hypertension: RR: 1.4• Obesity: RR: 1.3 9
2013 ACCF/AHA Guideline for the Management of Heart Failure. Circulation. 2013;128:1810-1852

Pathophysiology• Complex clinical syndrome resulting from structural or
functional impairment of ventricular filling and the ejection of blood
• Symptoms include:• Dyspnea• Fatigue• Fluid retention
• No single diagnostic test
10
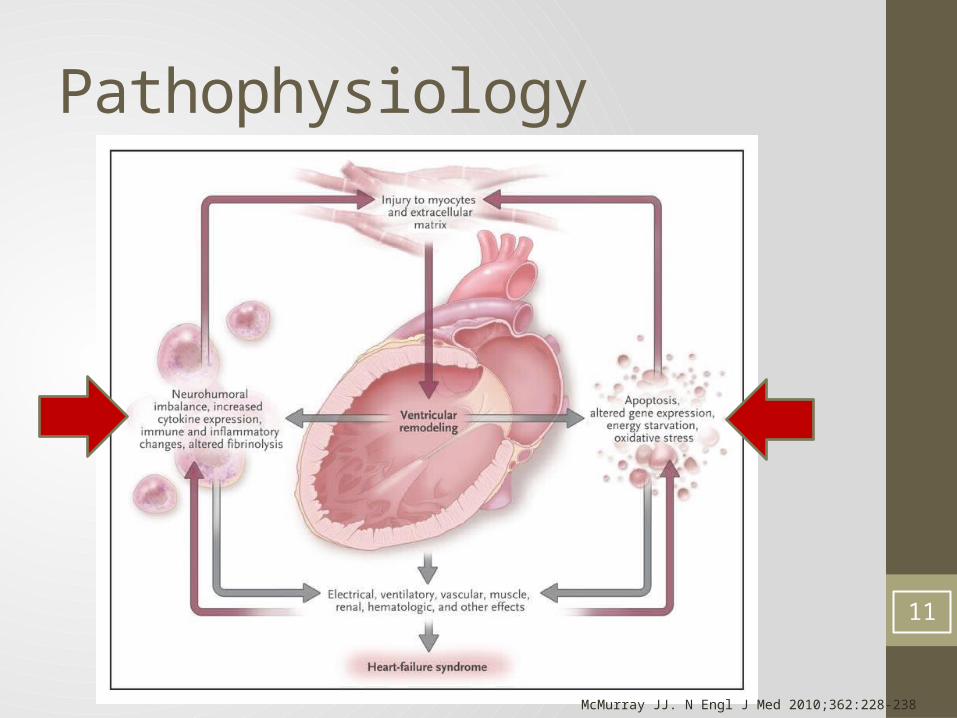
Pathophysiology
McMurray JJ. N Engl J Med 2010;362:228-238
11
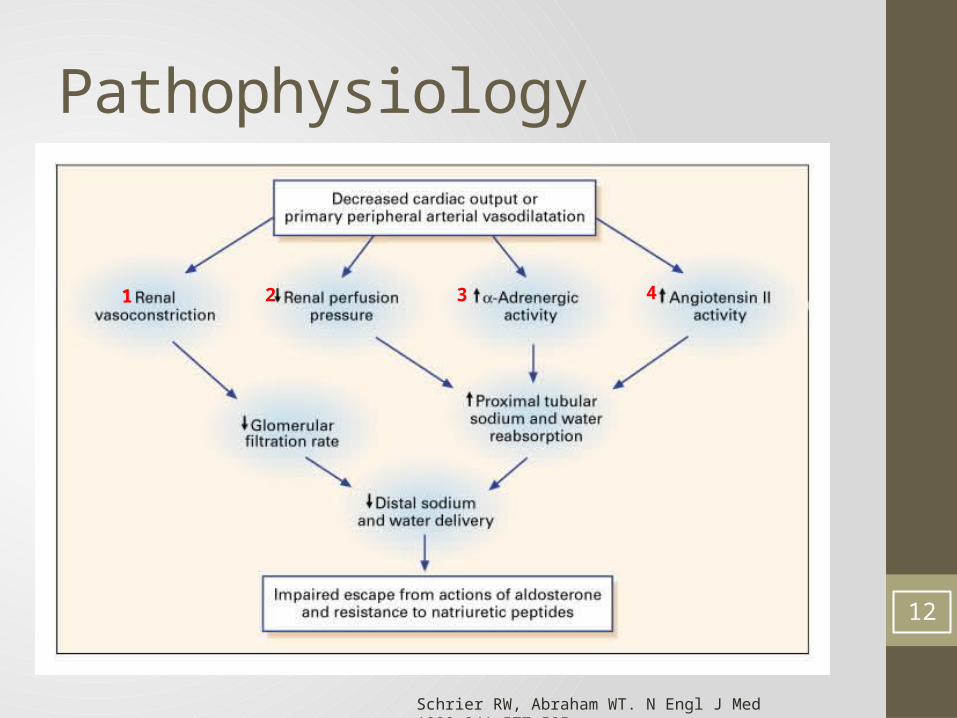
Pathophysiology
Schrier RW, Abraham WT. N Engl J Med 1999;341:577-585
1 2 3 4
12

Causes of Heart Failure• Cardiac Disorders• Pericardium• Myocardium• Endocardium• Heart Valves
• Impaired left ventricular function• Cardiomyopathy• Dilated ventricle• Hypertrophic ventricle
• Impaired Ejection Fraction• Heart Failure with Preserved Ejection Fraction• Heart Failure with Reduced Ejection Fraction 13
2013 ACCF/AHA Guideline for the Management of Heart Failure. Circulation. 2013;128:1810-1852
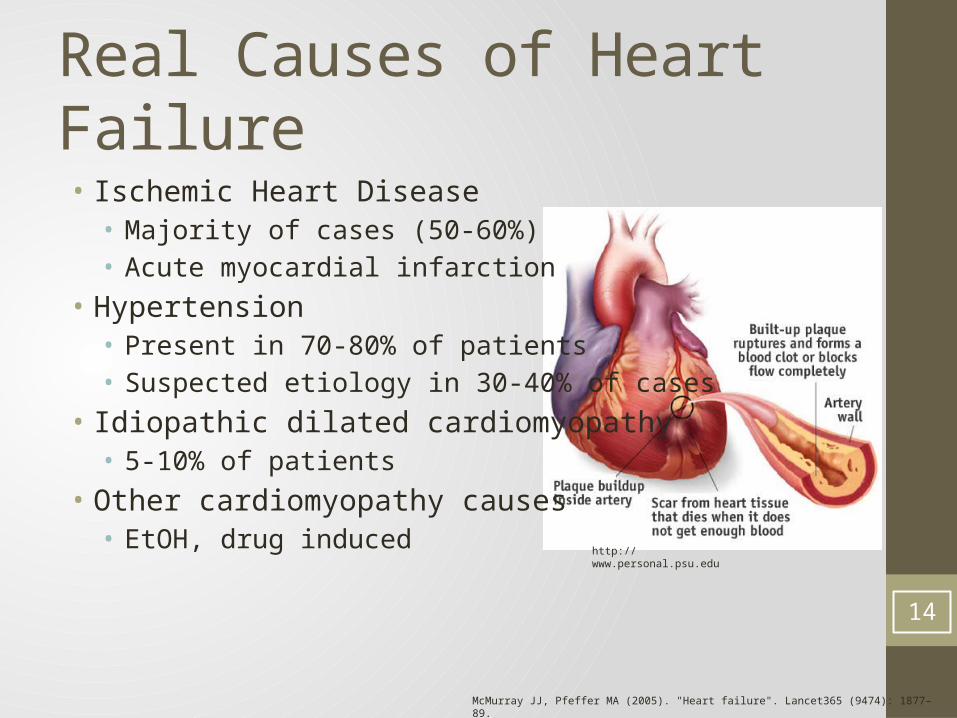
Real Causes of Heart Failure• Ischemic Heart Disease• Majority of cases (50-60%)• Acute myocardial infarction
• Hypertension• Present in 70-80% of patients• Suspected etiology in 30-40% of cases
• Idiopathic dilated cardiomyopathy• 5-10% of patients
• Other cardiomyopathy causes• EtOH, drug induced
McMurray JJ, Pfeffer MA (2005). "Heart failure". Lancet365 (9474): 1877–89.
http://www.personal.psu.edu
14
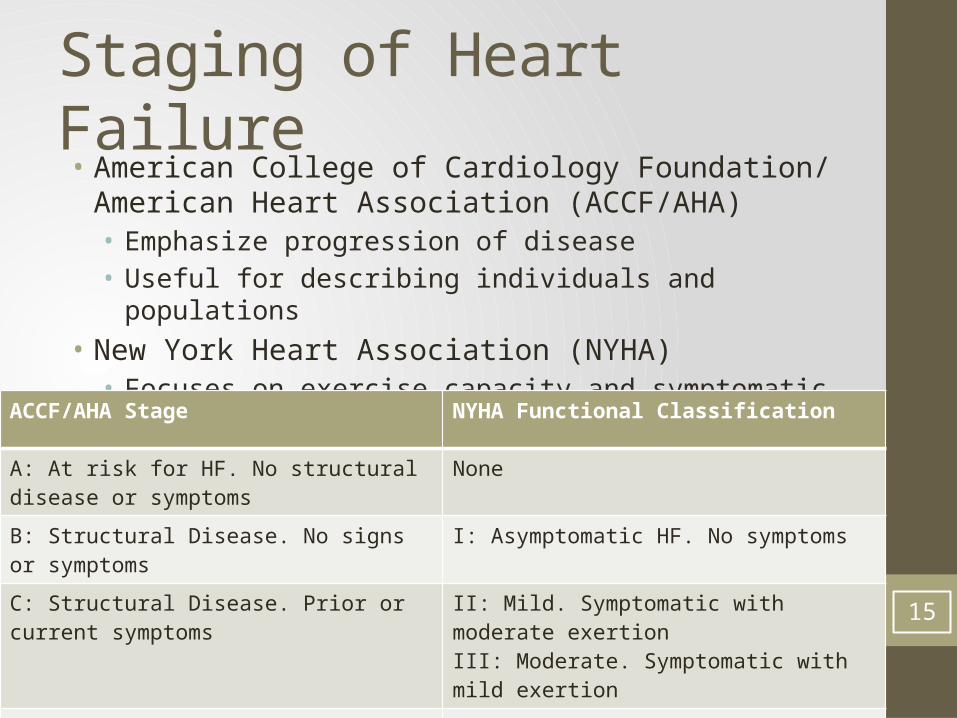
Staging of Heart Failure• American College of Cardiology Foundation/ American Heart
Association (ACCF/AHA)• Emphasize progression of disease• Useful for describing individuals and populations
• New York Heart Association (NYHA)• Focuses on exercise capacity and symptomatic status of disease
ACCF/AHA Stage NYHA Functional Classification
A: At risk for HF. No structural disease or symptoms
None
B: Structural Disease. No signs or symptoms I: Asymptomatic HF. No symptoms
C: Structural Disease. Prior or current symptoms II: Mild. Symptomatic with moderate exertionIII: Moderate. Symptomatic with mild exertion
D: Refractory HF requiring specialized interventions
IV: Severe. Symptomatic at rest15

Stage Management
Stage A
• At Risk for Heart Failure
Stage B
• Structural Heart Disease
Stage C
• Prior or Current Symptoms
Stage D
• Refractory Heart Failure16
“A” as in All Right• Stage A • At risk for HF. No structural disease or symptoms
• Manage patients risk factors• Hypertension
• Thiazide diuretics• ACE Inhibitors
• Hyperlipidemia• Lifestyle changes• Statins
• Control/avoid conditions that may lead to HF• Obesity• Diabetes mellitus• Tobacco use• Use of known cardiotoxic agents
17

“B” as in Better Treat• Stage B• Structural Disease. No signs or symptoms• Often a patient with recent or remote MI or ACS
• Initiate ACE Inhibitor• Prevent progression to symptomatic HF• Reduce mortality• ARB for ACEI intolerant • In ALL patients with reduced ejection fraction
• Initiate Beta Blocker• Approved beta blockers
• Metoprolol• Carvedilol• Bisoprolol
• Reduce mortality• In ALL patients with reduced ejection fraction
18

Stage B Cont.• Start a Statin• In all patients with history of MI or ACS
• Control Hypertension• Prevent LV hypertrophy
• Avoid Nondihydropyridine Calcium Channel Blockers• Diltiazem• Verapamil• Harmful in asymptomatic patients
19

“C” as in Symptomatic• Stage C• Structural Heart Disease. Prior or current symptoms• Recommendations added to Stage B
• Non-Pharmacologic Interventions• Patients should be educated about self care• Exercise training for those able• Sodium restriction• Continuous positive airway pressure
20

Class C Cont.• Diuretic Therapy• Loop diuretics• Patients with reduced ejection fraction• Symptomatic improvement
• Aldosterone Antagonist• NYHA II-IV• Reduced ejection fraction
• ACE Inhibitor + ARB• Persistently symptomatic• Those unable to use aldosterone antagonist
21

Class C Cont.• Hydralazine and Isosorbide Dinitrate• African Americans• NYHA III-IV on optimal therapy
• Digoxin• Beneficial in reduced ejection fraction• Reduce hospitalization
22

“D” as in Dyspnea at Rest• Stage D• Refractory heart failure• Specialized interventions
• Water Restriction• 1.5-2 Liters per day
• Ionotropic Support• Bridge therapy• Maintain end-organ performance• For patients awaiting definitive therapy
23

What’s New?• GDMT (guideline-directed medical therapy)• No longer “optimal medical therapy”• ACEI’s, BBs
• Patient Education• Balanced view of sodium restriction• No strong evidence• May be beneficial in volume overloaded patients
• Expanded use of aldosterone antagonists• Expanded use of MSC (mechanical circulatory support)• Intensified diuretic use in acute exacerbations
24
HFSA 2010 Comprehensive Heart Failure Practice Guideline. J Card Fail 2010;16:e1-e194.2013 ACCF/AHA Guideline for the Management of Heart Failure. Circulation. 2013;128:1810-1852

GDMTHFrEF Stage C
NYHA Class I – IVTreatment:
For NYHA class II-IV patients. Provided estimated creatinine
>30 mL/min and K+ <5.0 mEq/dL
For persistently symptomatic African Americans, NYHA class III-IV
Class I, LOE AACEI or ARB AND
Beta Blocker
Class I, LOE CLoop Diuretics
Class I, LOE AHydral-Nitrates
Class I, LOE AAldosterone Antagonist
AddAdd Add
For all volume overload, NYHA class II-IV patients
25
2013 ACCF/AHA Guideline for the Management of Heart Failure. Circulation. 2013;128:1810-1852
Sodium Restriction• Previous Guidelines:• Dietary instruction regarding sodium intake is recommended in
all patients with HF• Dietary sodium restriction (2-3 g daily) is recommended for
patients with the clinical syndrome of HF• New Guidelines:• Sodium restriction is reasonable for patients with symptomatic
HF to reduce congestive symptoms• Widely Embraced Idea• Not well supported by evidence• Particularly its effect on mortality
26
HFSA 2010 Comprehensive Heart Failure Practice Guideline. J Card Fail 2010;16:e1-e194.2013 ACCF/AHA Guideline for the Management of Heart Failure. Circulation. 2013;128:1810-1852

Mechanical Circulatory Support
• First used in 1984 as bridge for transplantation
• Recommended prior to definitive management• Carefully selected patients• Reduced ejection fraction
• May be used as:• “Bridge to recovery”• “Bridge to decision”
27
Kirklin J, Naftel D. Circulation. 2008 bio.felk.cvut.cz

Intensified Diuretics• Previous Guidelines:• When congestion fails to improve in response to diuretic therapy,
the following options should be considered:• Re-evaluating presence/absence of congestion• Sodium and fluid restriction• Increasing doses of loop diuretic• Continuous infusion of a loop diuretic • Addition of a second type of diuretic orally or intravenously
• New Guidelines:• Patients should be promptly treated with intravenous loop diuretics
to reduce morbidity• Dose should equal or exceed their chronic oral daily dose• Be given as either intermittent boluses or continuous infusion• Add a second (thiazide) diuretic• Low-dose dopamine infusion may be considered
28
HFSA 2010 Comprehensive Heart Failure Practice Guideline. J Card Fail 2010;16:e1-e194.2013 ACCF/AHA Guideline for the Management of Heart Failure. Circulation. 2013;128:1810-1852

Pharmacologic Agents• Diuretics• ACE Inhibitors• Angiotensin Receptor Blockers• Beta Blockers• Aldosterone Receptor Antagonists• Hydralazine and Isosorbide Dinatrate• Digoxin• Miscellaneous Agents• Agents to avoid in Heart Failure
29
2013 ACCF/AHA Guideline for the Management of Heart Failure. Circulation. 2013;128:1810-1852
Thiazide Diuretics• Benefit• Not potent enough for most HF patients• First line for hypertension
• Mechanism of action• Blocks reabsorption of sodium and chloride in the distal tubule
• When to use• Stage A• Added to loop diuretic therapy
• Sequential nephron blockade
• Contraindications• Anuria• Hypersensitivity 30

Thiazide(-like) DiureticsDiuretic Initial Dose Max Daily Dose Duration
Chlorothiazide 250-500mg 1000mg 6-12 hours
Chlorthalidone 12.5-25mg 100mg 24-72 hours
HCTZ 25-50mg 200mg 6-12 hours
Indapamide 2.5mg 5mg 36 hours
Metolazone 2.5mg 20mg 12-24 hours 31
2013 ACCF/AHA Guideline for the Management of Heart Failure. Circulation. 2013;128:1810-1852

Loop Diuretics• Benefit• Symptomatic benefit only• Decrease sodium and water retention (preload)
• Mechanism of action• Blocks Na-K-2CL co-transport of the ascending loop of Henle
• When to use• Mainstay of HF diuretic therapy• Not mandatory
• Contraindications• Anuria• Hypersensitivity
32
2013 ACCF/AHA Guideline for the Management of Heart Failure. Circulation. 2013;128:1810-1852

Loop Diuretics• Potent fluid elimination• Less effective in controlling blood pressure
• Patients should monitor weight daily• Report significant weight gain• Peripheral edema often not evident until ~10 lbs
33

Loop Diuretics
Diuretic Daily Dose Max Daily Dose Duration
Bumetanide 0.5-1mg 10mg 4-6 hours
Furosemide 20-40mg 600mg 6-8 hours
Torsemide 10-20mg 200mg 12-16 hours
Ethacrynic Acid 50-100mg 200mg 6-8 hours
34
2013 ACCF/AHA Guideline for the Management of Heart Failure. Circulation. 2013;128:1810-1852

Sequential Nephron Blockade
http://3.bp.blogspot.com
35
ACE Inhibitors- Benefits• Reduce morbidity and mortality
• Decrease preload and afterload
• Decrease sympathetic activation
• Prevent LV remodeling
• Slows heart failure progression
36
2013 ACCF/AHA Guideline for the Management of Heart Failure. Circulation. 2013;128:1810-1852

Mechanism of Action
http://www.google.com
37

ACE Inhibitors• When to use• All patients with recent or remote MI or ACS• All patients with reduced EF • Part of guideline-directed medical therapy (GDMT)
• Side Effects• Cough
• Fluid overload, concomitant pulmonary disease, infection• Hyperkalemia
• Reduced renal excretion• Acute Renal Insufficiency
• Monitor BUN and SCr
38
2013 ACCF/AHA Guideline for the Management of Heart Failure. Circulation. 2013;128:1810-1852

ACE Inhibitor on Nephron
http://www.google.com
39

ACE InhibitorsAgent Initial Dose Target Dose Max Daily Dose
Captopril 6.25mg TID 122.7mg/day 50mg TID
Enalapril 2.5mg BID 16.6mg/day 10-20mg BID
Fosinopril 5-10mg Daily N/A 40mg Daily
Lisinopril 2.5-5mg Daily 32.5-35mg/day 20-40mg Daily
Perindopril 2mg Daily N/A 8-16mg Daily
Quinapril 5mg BID N/A 20mg BID
Ramipril 1.25mg-2.5mg Daily N/A 10mg Daily
Trandolapril 1mg Daily N/A 4mg Daily 40
2013 ACCF/AHA Guideline for the Management of Heart Failure. Circulation. 2013;128:1810-1852

Angiotensin Receptor Blockers• Benefit• Similar to that of ACE inhibitor
• Mechanism of action• Angiotensin II receptor antagonist
• When to use• In ACE inhibitor-intolerant individuals• May be used in place of ACE inhibitors• In addition to ACE Inhibitor
• Also on beta blocker• Aldosterone antagonist not indicated or tolerated
• NOT TO BE USED with ACE inhibitor AND aldosterone antagonist
41

ARB AgentsAgent Initial Dose Target Dose Max Daily
DoseCandesartan 4-8mg Daily 24mg/day 32mg Daily
Losartan* 25-50mg Daily 129mg/day 50-150mg Daily
Valsartan 20-40mg BID 254mg/day 160mg BID
*Not indicated FDA indicated for heart failure
42
2013 ACCF/AHA Guideline for the Management of Heart Failure. Circulation. 2013;128:1810-1852

Beta Blockers• Benefit• Reduces morbidity and mortality• Improves cardiac function
• Increases EF• Improved exercise tolerance
• Slows disease progression• Mechanism of action• Beta-adrenergic blockers selective for beta-1 receptors
• When to use• GDMT• ALL patients with reduced EF• May be initiated in hospital after acute event 43
2013 ACCF/AHA Guideline for the Management of Heart Failure. Circulation. 2013;128:1810-1852

Beta Blocker AgentsAgent Initial Dose Target Dose Max Daily Dose
Bisoprolol 1.25mg Daily 8.6mg/day 10mg Daily
Carvedilol 3.125mg BID 37mg/day 50mg BID
Carvedilol CR 10mg Daily N/A 80mg Daily
Metoprolol Succinate
12.5-25mg Daily 159mg/day 200mg Daily
• Likely worsening of symptoms initially• Increase SOB, weight gain
• Slow titration upward• Over 6-8 weeks to target dose
44
2013 ACCF/AHA Guideline for the Management of Heart Failure. Circulation. 2013;128:1810-1852

Aldosterone Antagonists• Benefit• Reduction in morbidity and mortality
• Mechanism of action• Blocks distal renal tubules increasing Na and H20 excretion• Blocks effect on arterial smooth muscle
• When to Use• NYHA II-IV• LVEF <35%• Creatinine <2.5 in men; <2.0 in women
• eGFR > 30 ml/min• Potassium < 5.0 mEq/L• OR Following an acute MI with LVEF < 40%
• Who develop symptoms• Have a history of diabetes
45
2013 ACCF/AHA Guideline for the Management of Heart Failure. Circulation. 2013;128:1810-1852

Aldosterone Antagonists
http://3.bp.blogspot.com/-
46

Aldosterone Antagonists• High mortality reduction when used appropriately • RR Reduction of Mortality: 30%• RR Reduction of Hospitalization: 35%• NNT: 6 Patients
• DO NOT USE• SCr >2.5 in men; 2.0 in women• eGFR < 30 ml/min• Serum K > 5.0 mEq/L• In combination with ACEI and ARB
Agent Initial Dose Max Daily DoseSpironolactone 12.5-25mg Daily 25mg BIDEplerenone 25mg Daily 50mg Daily
47
2013 ACCF/AHA Guideline for the Management of Heart Failure. Circulation. 2013;128:1810-1852
Hydralazine & Isosorbide Dinitrate• Benefit• Reduced morbidity and mortality • Reduces preload and afterload
• Mechanism of action• Vasodilates arteries• Relaxes smooth muscle of vasculature
• When to use• African Americans receiving optimal GDMT
• NYHA Class III-IV• Patients who cannot tolerate ACE or ARB
48
2013 ACCF/AHA Guideline for the Management of Heart Failure. Circulation. 2013;128:1810-1852
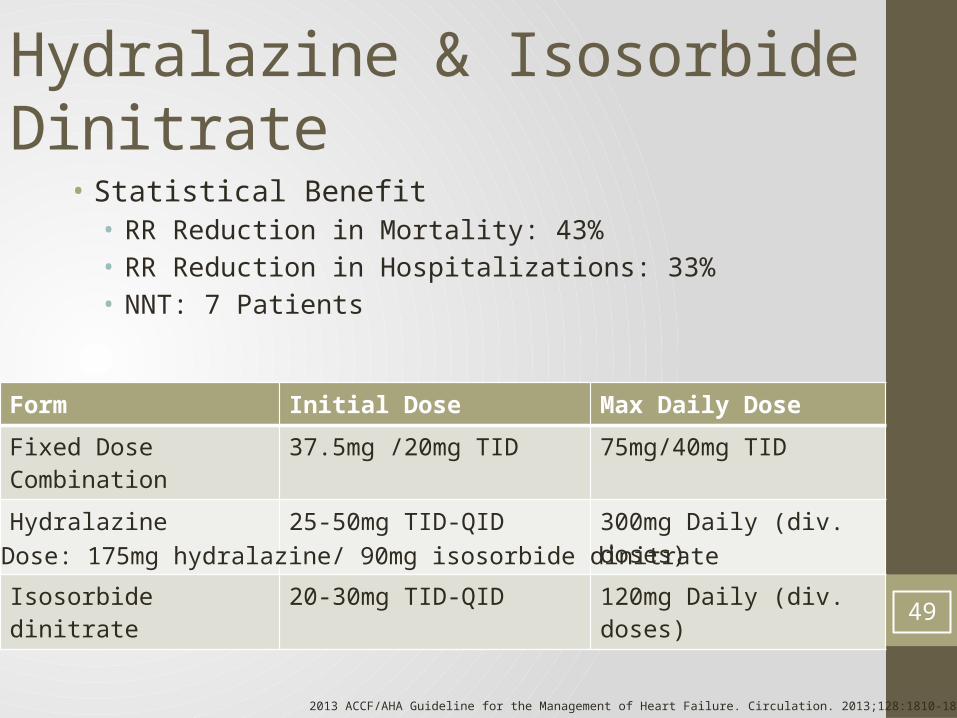
• Statistical Benefit• RR Reduction in Mortality: 43%• RR Reduction in Hospitalizations: 33%• NNT: 7 Patients
Hydralazine & Isosorbide Dinitrate
Form Initial Dose Max Daily Dose
Fixed Dose Combination 37.5mg /20mg TID 75mg/40mg TID
Hydralazine 25-50mg TID-QID 300mg Daily (div. doses)
Isosorbide dinitrate 20-30mg TID-QID 120mg Daily (div. doses)
49
*Target Dose: 175mg hydralazine/ 90mg isosorbide dinitrate
2013 ACCF/AHA Guideline for the Management of Heart Failure. Circulation. 2013;128:1810-1852
Digoxin• Benefit• Improvement in symptoms• Improved exercise tolerance• Decreased number of hospitalizations
• Mechanism of action• Positive ionotropic effect• Decreased sympathetic outflow• Improved baroreceptor function and vagal tone
• When to use• Reduced ejection fraction• Symptomatic on optimal therapy• Target Concentration: 0.5-1.0 ng/ml 50
2013 ACCF/AHA Guideline for the Management of Heart Failure. Circulation. 2013;128:1810-1852

Digoxin
https://lh4.googleusercontent.com
51

Miscellaneous Agents• Anticoagulation• Patients requiring anticoagulation
• Atrial fibrillation• Risk of stroke
• Statins• Not useful in absence of other indications
• Omega-3 Fatty Acids• Reasonable in NYHA class II-IV• Reduce morbidity, mortality, and hospitalizations
• Nutritional Supplements• Not recommended as treatment
• Hormonal therapies• Not recommended as treatment
52
2013 ACCF/AHA Guideline for the Management of Heart Failure. Circulation. 2013;128:1810-1852

What NOT to Use• Most antiarrhythmic drugs• Amiodarone and dofetilide (neutral mortality)• Flecainide- RR: 3.6 (CI: 1.7 to 8.5)
• Calcium channel blockers• Except amlodipine
• NSAIDs• Thiazolidinediones• Ionotropic support outside of indication• Dopamine• Dobutamine• Milrinone
N Engl J Med 1989;321:406–12
Lancet. 350 1997:1417-1424
53

Non-pharmacologic Interventions• Fluid restriction• Stage D• 1.5-2L per day
• Salt restriction• Reasonable in Stage C Symptomatic patients• Not supported by strong evidence
http://www.scienceguardian.com http://www.rightthisminute.com
54

Sodium Studies
55
Lennie TA et al. J Card Fail. 2011;17:325–30.

Sodium Studies
56
Arcand J et al. Am J Clin Nutr. 2011;93:332–7.

What did we learn today?
57

Thank you• Dr. Miller • Dr. Rodney • Dr. Steele
• All of you for listening!
58http://www.cats-on-tshirts.com

References• 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology
Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;128:1810-1852• Lindenfeld, J, Albert NM, Boehmer JP, Collins SP, Ezekowitz JA, Givertz MM, Klapholz M, Moser DK, Rogers JG, Starling RC, Stevenson
WG, Tang WHW, Teerlink JR, Walsh MN. HFSA 2010 Comprehensive Heart Failure Practice Guideline. J Card Fail 2010;16:e1-e194.• Roger VL, Weston SA, Redfield MM, et al. Trends in heart failure incidence and survival in a community-based population. JAMA
2004;292:344–50.• Owan TE, Redfield MM. Epidemiology of diastolic heart failure. Prog. Cardiovasc Dis 2005;47:320–32.• The Booming Dynamics of Aging: From Awareness to Action. The White House Conference on Aging. Washington, DC: US
Department of Health and Human Services; 2011.• Pitt B, Zannad F, Remme WJ, et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure.
Randomized Aldactone Evaluation Study Investigators. N Engl J Med 1999; 341:709.• McMurray JJ, Pfeffer MA (2005). "Heart failure". Lancet365 (9474): 1877–89. doi:10.1016/S0140-6736(05)66621-4. PMID 15924986.• Boren SA, Wakefield BJ, Gunlock TL, et al. Heart failure self-management education: a systematic review of the evidence. Int J Evid
Based Healthc. 2009;7:159-68.• Cruz F, Issa VS, Ayub-Ferreira SM, et al. Effect of a sequential education and monitoring programme on quality-of-life components in
heart failure. Eur J Heart Fail. 2010• The Cardiac Arrhythmia Suppression Trial (CAST) Investigators. Preliminary report: effect of encainide and flecainide on mortality in
a randomized trial of arrhythmia suppression after myocardial infarction. N Engl J Med 1989;321:406–12• Amiodarone Trials Meta-Analysis Investigators. Effect of prophylactic amiodarone on mortality after acute myocardial infarction and
in congestive heart failure: meta-analysis of individual data from 6500 patients in randomised trials. Lancet. 350 1997:1417-1424.• Kirklin J, Naftel D. Advances in Heart Failure. Mechanical Circulatory Support: Registering a Therapy in Evolution. Circulation: Heart
Failure. 2008; 1: 200-205• Arcand J, Ivanov J, Sasson A, et al. A high-sodium diet is associated with acute decompensated heart failure in ambulatory heart
failure patients: a prospective follow-up study. Am J Clin Nutr. 2011;93:332–7.• Lennie TA, Song EK, Wu JR, et al. Three gram sodium intake is associated with longer event-free survival only in patients with
advanced heart failure. J Card Fail. 2011;17:325–3059


Test Your Knowledge• True or false:• Heart failure is synonymous with left ventricular hypertrophy.
• Answer:• False
61

Test Your Knowledge• Which of these has shown to reduce morbidity and mortality
in patients with heart failure?A. Coenzyme Q10B. Milk ThistleC. L-arginineD. Omeg-3 fatty acids
• Answer:• D. Omega-3 fatty acids
62

Test Your Knowledge• True or False:• Digoxin has shown to have improved mortality in patients with
heart failure.
• Answer:• False
63

Test Your Knowledge• All patients with Stage B heart failure should be initiated on
which classes of medication for mortality benefit (select all that apply):A. Beta BlockerB. ACE InhibitorC. Loop DiureticD. Cardiac Glycoside
• Answer: • A and B. Beta Blocker and ACE Inhibitor
64

Test Your Knowledge• Which calcium channel blocker has been shown to be safe in
patients with heart failure:A. DiltiazemB. VerapamilC. FelodipineD. Amlodipine
• Answer: • D. Amlodipine
65