heart failure:. case 1 67 year old man presented with anterior wall mi in may. underwent stent...
TRANSCRIPT

Heart Failure:Heart Failure:
Case 1Case 1• 67 year old man• Presented with anterior wall MI in May.
Underwent stent placement in the LAD. The other arteries were patent.
• Echo demonstrated mildly-moderate decreased LV systolic function with anteroapical akinesis
• Unremarkable recovery. Started on aspirin, plavix, simvastatin, atenolol 25mg and discharged home
• 67 year old man• Presented with anterior wall MI in May.
Underwent stent placement in the LAD. The other arteries were patent.
• Echo demonstrated mildly-moderate decreased LV systolic function with anteroapical akinesis
• Unremarkable recovery. Started on aspirin, plavix, simvastatin, atenolol 25mg and discharged home

November 1November 1
• Acute onset of shortness of breath
• Wife called Mada,
• HR 94 BP 114/60 RR 28 sat 91%
• Bibasilar crackles
• Acute onset of shortness of breath
• Wife called Mada,
• HR 94 BP 114/60 RR 28 sat 91%
• Bibasilar crackles

ECGECG
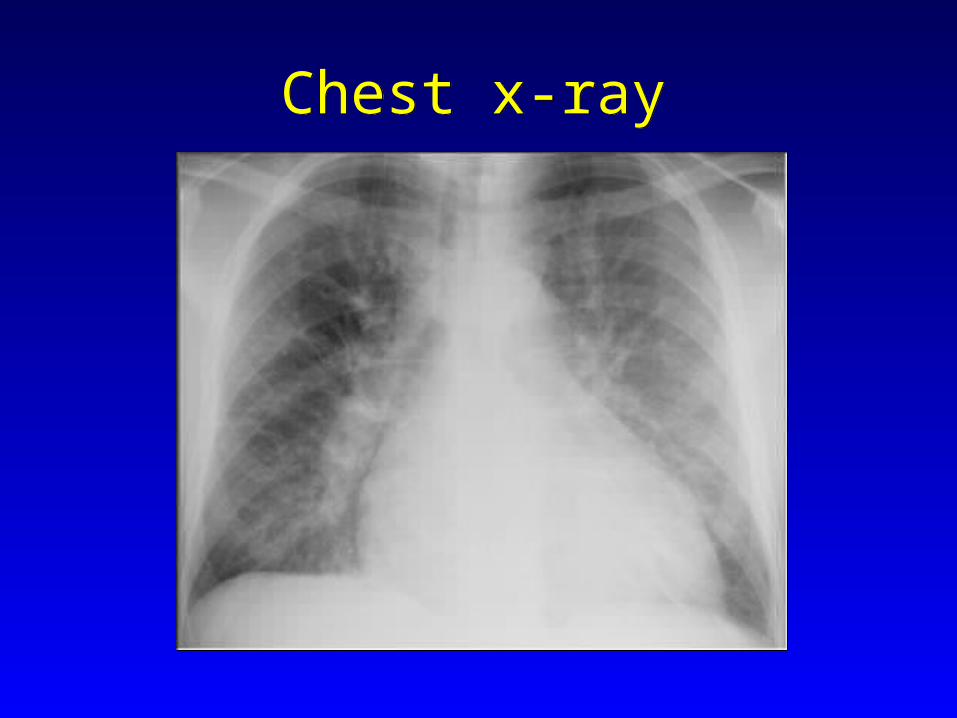
Chest x-rayChest x-ray

EchoEcho
• Dilated LV with moderately-severely decreased function.
• Anteroseptal and apical dyskinesis
• Moderate-severe mitral regurgitation
• Normal RV size and function
• Mild pulmonary hypertension
• Dilated LV with moderately-severely decreased function.
• Anteroseptal and apical dyskinesis
• Moderate-severe mitral regurgitation
• Normal RV size and function
• Mild pulmonary hypertension

What happened?What happened?

Biomechanical Model of Heart FailureBiomechanical Model of Heart Failure
Myocardial Myocardial Dysfunction Dysfunction Myocardial Myocardial
Dysfunction Dysfunction
↑↑AfterloadAfterload↑↑AfterloadAfterload
↑↑ PreloadPreload↑↑ PreloadPreload
↑↑ ContractilityContractility↑↑ ContractilityContractility
Neurohormonal Neurohormonal ActivationActivation
Neurohormonal Neurohormonal ActivationActivation
Renin-Renin-Angiotensin Angiotensin AldosteroneAldosterone
Renin-Renin-Angiotensin Angiotensin AldosteroneAldosterone
Sympathetic Sympathetic StimulationStimulation
Sympathetic Sympathetic StimulationStimulation
VasoconstrictionVasoconstrictionVasoconstrictionVasoconstriction
Sodium & Water Sodium & Water RetentionRetention
Sodium & Water Sodium & Water RetentionRetention
Cardiac Cardiac Remodeling Remodeling
Cardiac Cardiac Remodeling Remodeling
Beta Beta BlockersBlockers
Beta Beta BlockersBlockers×××× ACE-I ACE-I
ARBARBACE-I ACE-I ARBARB××××SpironolactoneSpironolactoneSpironolactoneSpironolactone ××××
××××DiureticsDiureticsDiureticsDiuretics

What didn’t happen that should have happened?
What didn’t happen that should have happened?
AABB
CC
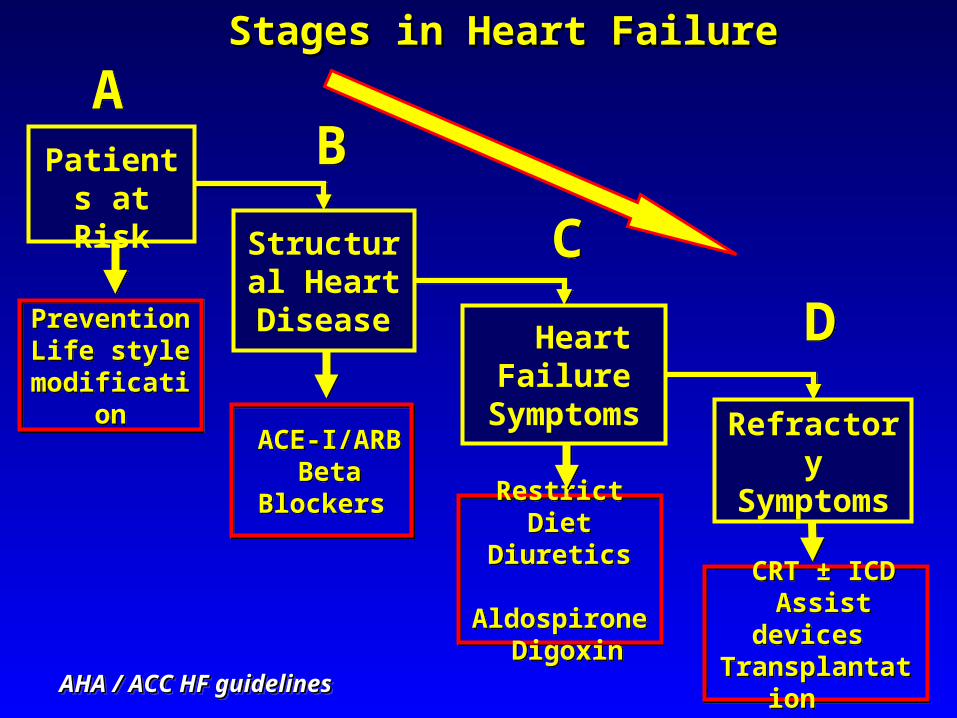
DDPreventionLife style
modification
PreventionLife style
modification
ACE-I/ARB Beta
Blockers
ACE-I/ARB Beta
BlockersRestrict Diet
Diuretics Aldospirone
Digoxin
Restrict DietDiuretics
Aldospirone Digoxin
CRT ± ICD Assist devices Transplantation
CRT ± ICD Assist devices Transplantation
Stages in Heart FailureStages in Heart Failure
Refractory Symptoms
Heart Failure
Symptoms
Structural Heart
Disease
Patients at Risk
AHA / ACC HF guidelinesAHA / ACC HF guidelinesAHA / ACC HF guidelinesAHA / ACC HF guidelines
Hospital CourseHospital Course
• Admitted with a diagnosis of acute decompensated heart failure.
• What is the first thing you do?
• Admitted with a diagnosis of acute decompensated heart failure.
• What is the first thing you do?
Comprehensive inhibition of neurohormonal activation
Comprehensive inhibition of neurohormonal activation
– achieve euvolemia with diuretics and salt restriction
– ACE-inhibitors– Beta-blockers (so far only carvedilol,
bisoprolol and extended release metoprolol)
– Careful spironolactone
– achieve euvolemia with diuretics and salt restriction
– ACE-inhibitors– Beta-blockers (so far only carvedilol,
bisoprolol and extended release metoprolol)
– Careful spironolactone

COPERNICUSCOPERNICUSNEJM 2001NEJM 2001COPERNICUSCOPERNICUSNEJM 2001NEJM 2001
Beta BlockerBeta BlockerBeta BlockerBeta Blocker
242424240000 20202020161616161212121288884444 28282828
PlaceboPlacebo
CarvedilolCarvedilol
MonthsMonthsMonthsMonths
Su
rviv
al %
Su
rviv
al %
35%35%35%35%
100100100100
90909090
80808080
60606060
70707070
50505050
ACE-InhibitorACE-InhibitorACE-InhibitorACE-Inhibitor
CONSENSUSNEJM 1987CONSENSUSNEJM 1987
1001001001009090909080808080
6060606070707070
50505050
MonthsMonths
PlaceboPlacebo
EnalaprilEnalapril
121211111010998877665500
4433221100
4040404030303030
Su
rviv
al %
Su
rviv
al %
PlaceboPlacebo
EnalaprilEnalapril
31%31%31%31%

Spironolactone
RALESRALESNEJM 1999NEJM 1999
If...If...
• If the patient cannot tolerate ACE-inhibitor, ARB may be substituted (valsartan)
• If the patient cannot tolerate beta blocker, ACE-I and ARB may be combined
• Isosorbide and hydralazine can be considered in patients who cannot tolerate ACE-I
• If the patient cannot tolerate ACE-inhibitor, ARB may be substituted (valsartan)
• If the patient cannot tolerate beta blocker, ACE-I and ARB may be combined
• Isosorbide and hydralazine can be considered in patients who cannot tolerate ACE-I

Now what should we do?Now what should we do?• A. Cardiac catheterization to see if the stent
is patent• B. Stress thallium to see if there is residual
ischemia• C. Exercise echo to see if the mitral
regurgitation and pulmonary hypertension worsen with exercise
• D. Transesophageal echo to determine severity of mitral regurgitation
• A. Cardiac catheterization to see if the stent is patent
• B. Stress thallium to see if there is residual ischemia
• C. Exercise echo to see if the mitral regurgitation and pulmonary hypertension worsen with exercise
• D. Transesophageal echo to determine severity of mitral regurgitation

Other considerationsOther considerations
• A. Put in a defibrillator
• B. Put in a pacemaker to allow for target doses of beta blocker
• C. Put in a biventricular pacemaker
• D. Add amiodarone for the prevention of sudden cardiac death
• A. Put in a defibrillator
• B. Put in a pacemaker to allow for target doses of beta blocker
• C. Put in a biventricular pacemaker
• D. Add amiodarone for the prevention of sudden cardiac death

Implantable Cardiac Defibrillator (ICD)
Implantable Cardiac Defibrillator (ICD)
SCD-HeFTSCD-HeFTN Engl J Med 2005N Engl J Med 2005SCD-HeFTSCD-HeFTN Engl J Med 2005N Engl J Med 2005
ICD
ICD implantation:• Patients with LVEF<30% • NYHA II-IV
ICD implantation:• Patients with LVEF<30% • NYHA II-IV
23%
N=2,521 IHD/NIHDNYHA class II-III LVEF < 35%

Biventricular PacingBiventricular Pacing

Cardiac-Resynchronization Therapy (CRT)
Cardiac-Resynchronization Therapy (CRT)
• Ventricular conduction delays cause dysynchronous contraction
• Biventricular pacing synchronizes ventricle contraction
• Ventricular conduction delays cause dysynchronous contraction
• Biventricular pacing synchronizes ventricle contraction
Cardiac Function:
EF↑ LV size↓ MR ↓
Exercise Capacity
Quality of life
Hospitalizations
Mortality
Cardiac Function:
EF↑ LV size↓ MR ↓
Exercise Capacity
Quality of life
Hospitalizations
Mortality
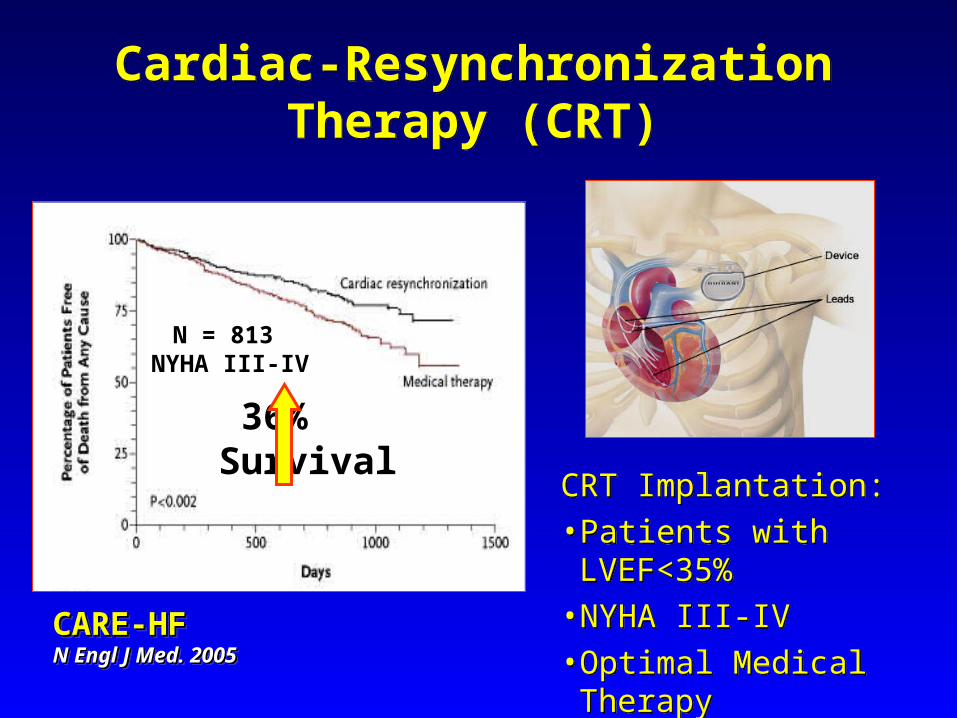
CARE-HFCARE-HFN Engl J Med. 2005N Engl J Med. 2005CARE-HFCARE-HFN Engl J Med. 2005N Engl J Med. 2005
36% Survival
Cardiac-Resynchronization Therapy (CRT)
Cardiac-Resynchronization Therapy (CRT)
CRT Implantation:• Patients with LVEF<35% • NYHA III-IV• Optimal Medical Therapy• QRS >120 ms
CRT Implantation:• Patients with LVEF<35% • NYHA III-IV• Optimal Medical Therapy• QRS >120 ms
N = 813 NYHA III-IV
What other therapies are available
What other therapies are available
• Prevention - Control risk factorsPrevention - Control risk factors
• Life style modificationsLife style modifications
• Treat etiologic cause / aggravating Treat etiologic cause / aggravating factorsfactors
• Optimized Drug therapyOptimized Drug therapy
• Specialized care – eg Shikum Lev or Specialized care – eg Shikum Lev or Heart Failure clinicsHeart Failure clinics
• Prevention - Control risk factorsPrevention - Control risk factors
• Life style modificationsLife style modifications
• Treat etiologic cause / aggravating Treat etiologic cause / aggravating factorsfactors
• Optimized Drug therapyOptimized Drug therapy
• Specialized care – eg Shikum Lev or Specialized care – eg Shikum Lev or Heart Failure clinicsHeart Failure clinics

What is the prognosis?What is the prognosis?
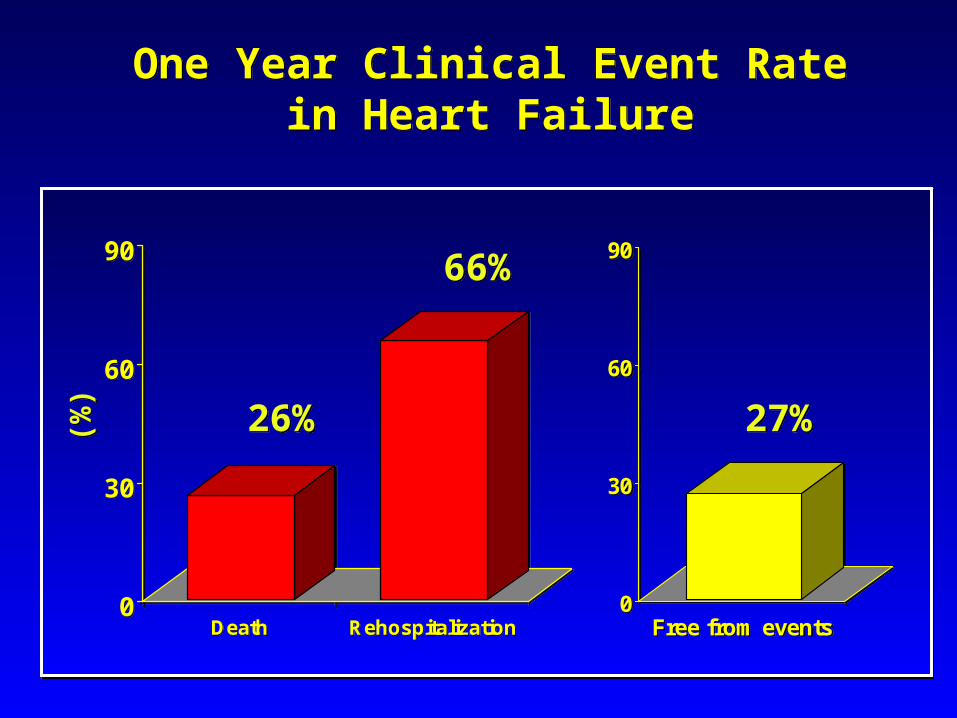
One Year Clinical Event Rate in Heart Failure
One Year Clinical Event Rate in Heart Failure
(%)
(%)
0
30
60
90
Death Rehospitalization0
30
60
90
Death Rehospitalization0
30
60
90
Free from events0
30
60
90
Free from events
26%26%
66%66%
27%27%

Acute Exacerbations Contribute to the Progression of Heart Failure
Acute Exacerbations Contribute to the Progression of Heart Failure
Am J Cardiology 2005Am J Cardiology 2005
TimeTime
Ven
tric
ula
r fu
nct
ion
Ven
tric
ula
r fu
nct
ion
Acute eventAcute event

Treatment – All PatientsTreatment – All PatientsTreatment – All PatientsTreatment – All Patients
• Prevention - Control risk factorsPrevention - Control risk factors
• Life style modificationsLife style modifications
• Treat etiologic cause / aggravating Treat etiologic cause / aggravating factorsfactors
• Optimized Drug therapyOptimized Drug therapy
• Specialized care – Increase complianceSpecialized care – Increase compliance
• Advanced TreatmentAdvanced Treatment
• Prevention - Control risk factorsPrevention - Control risk factors
• Life style modificationsLife style modifications
• Treat etiologic cause / aggravating Treat etiologic cause / aggravating factorsfactors
• Optimized Drug therapyOptimized Drug therapy
• Specialized care – Increase complianceSpecialized care – Increase compliance
• Advanced TreatmentAdvanced Treatment

Next patientNext patient
• 76 year old man
• CABG and AVR 10 years ago
• Normal LV systolic function on most recent echo
• Presents to the ER with acute decompensated heart failure.
• 76 year old man
• CABG and AVR 10 years ago
• Normal LV systolic function on most recent echo
• Presents to the ER with acute decompensated heart failure.
In the ERIn the ER
• HR 118 and irregular
• Blood pressure 132/64
• RR 22
• O2 Sat 94%
• HR 118 and irregular
• Blood pressure 132/64
• RR 22
• O2 Sat 94%

The ECGThe ECG

What happened?What happened?

Heart Failure with preserved EF
Heart Failure with preserved EF
Inability to fill normally
LA pressure
diastolicdysfunction
AtrialfibrillationCHF

HFPEF- EtiologyHFPEF- Etiology
• Left ventricular hypertrophy– Hypertension– Aortic stenosis
• Coronary artery disease• Diabetes• Elderly• Infiltrative/restrictive• Unexplained
• Left ventricular hypertrophy– Hypertension– Aortic stenosis
• Coronary artery disease• Diabetes• Elderly• Infiltrative/restrictive• Unexplained
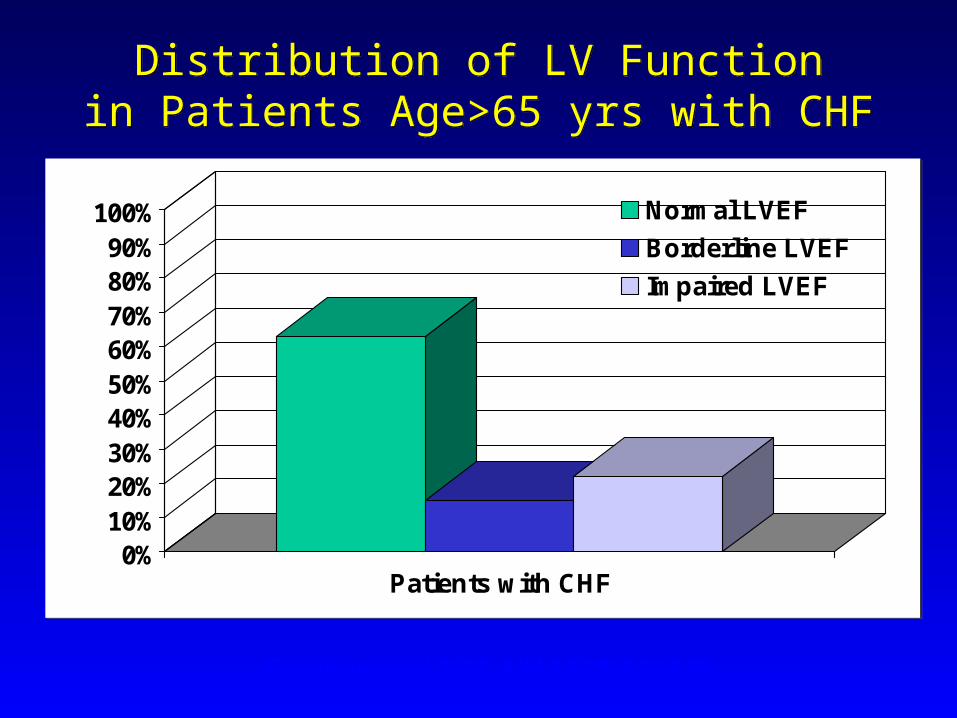
Distribution of LV Functionin Patients Age>65 yrs with CHF
Distribution of LV Functionin Patients Age>65 yrs with CHF
0%10%20%30%40%50%60%70%80%90%
100%
Patients with CHF
Normal LVEF
Borderline LVEF
Impaired LVEF
0%10%20%30%40%50%60%70%80%90%
100%
Patients with CHF
Normal LVEF
Borderline LVEF
Impaired LVEF
Gottdiener et al 2002. AIM 137(8):631-639

Pressure/Volume RelationshipPressure/Volume Relationship
Burkhoff et al 2003. Circ 107(5):656-658.

Diastolic Heart Failure - Diagnosis
Diastolic Heart Failure - Diagnosis
Is there a test thatwill diagnose
diastolic heart failure?

Heart Failure One Year Survival
Heart Failure One Year Survival
Preserved Preserved LVFLVF
Preserved Preserved LVFLVF
Adjusted SurvivalP=0.26=0.26
Adjusted SurvivalP=0.26=0.26
Reduced Reduced LVFLVF
Reduced Reduced LVFLVF
Su
rviv
al (
%)
Su
rviv
al (
%)
Su
rviv
al (
%)
Su
rviv
al (
%)
100100100100
90909090
80808080
60606060
70707070
50505050121212120000 101010108888666644442222
MonthsMonthsMonthsMonths
• CONSENSUS I• VeHFT I• SOLVD• SAVE• VeHFT II• CONSENSUS II• ATLAS• PROVED• RADIANCE• DIG
• CONSENSUS I• VeHFT I• SOLVD• SAVE• VeHFT II• CONSENSUS II• ATLAS• PROVED• RADIANCE• DIG
MDC CIBIS I CIBIS II ANZ PRECISE MOCHA MERIT-HF COPERNICUS CAPRICORN CHF-STAT
ELITE ValHFT ELITE II CHARM RESOLVD PRAISE WATCH RALES GESICA COMET
World’s Literature of Large or Randomized Trials of the Treatment of
Systolic Heart Failure
World’s Literature of Large or Randomized Trials of the Treatment of
Systolic Heart Failure

Randomized Trials of Treatment of D-CHF
Randomized Trials of Treatment of D-CHF
Zile et al 2002. Circ 105(12):1503-1508.
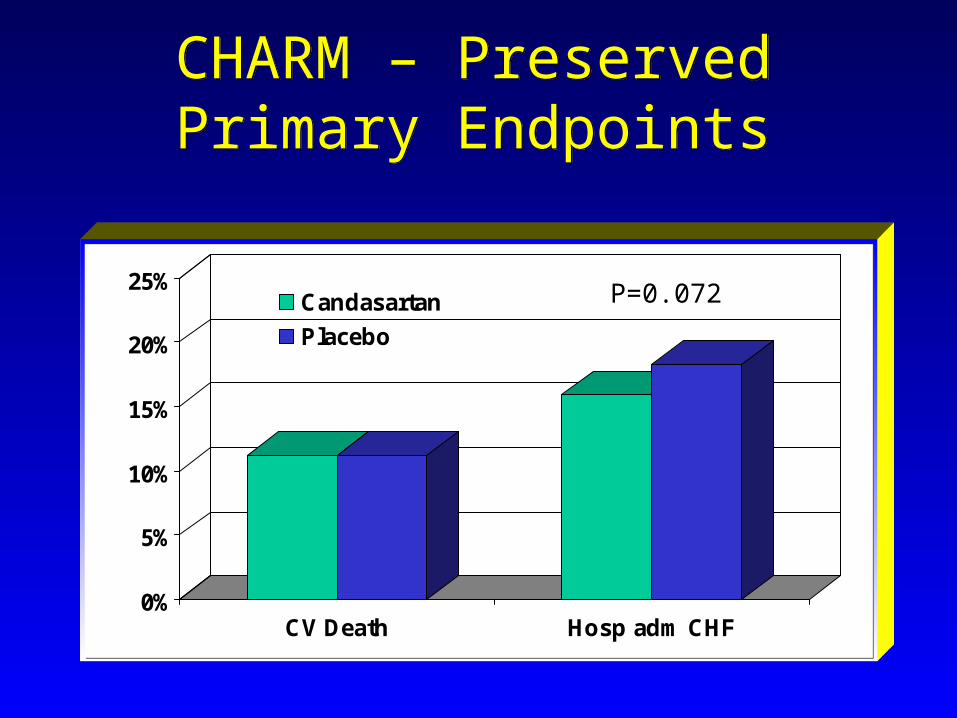
CHARM – PreservedPrimary Endpoints
CHARM – PreservedPrimary Endpoints
0%
5%
10%
15%
20%
25%
CV Death Hosp adm CHF
Candasartan
Placebo
0%
5%
10%
15%
20%
25%
CV Death Hosp adm CHF
Candasartan
Placebo
P=0.072

Diastolic CHF – Goals of Therapy
Diastolic CHF – Goals of Therapy
• Reduce preload• Decrease heart rate• Normalize blood pressure• Maintain atrial contraction• Improve relaxation• Cause regression of LVH• Decrease interstitial fibrosis• Treat ischemia• Decrease neurohumoral activation
• Reduce preload• Decrease heart rate• Normalize blood pressure• Maintain atrial contraction• Improve relaxation• Cause regression of LVH• Decrease interstitial fibrosis• Treat ischemia• Decrease neurohumoral activation

In the ERIn the ER• The patient was given IV beta blocker and
digoxin, with slowing of his heart rate to the 80s.
• Echo demonstrated :– Dilated atria– Normal LV chamber size with mild hypertrophy.
Normal RV size and function– Normally functioning aortic prosthesis– Mild-moderate mitral regurgitation– Mild pulmonary hypertension
• The patient was given IV beta blocker and digoxin, with slowing of his heart rate to the 80s.
• Echo demonstrated :– Dilated atria– Normal LV chamber size with mild hypertrophy.
Normal RV size and function– Normally functioning aortic prosthesis– Mild-moderate mitral regurgitation– Mild pulmonary hypertension

What do you do now?What do you do now?
• A. Begin anticoagulation, and plan to cardiovert the patient in 3 weeks
• B. Begin anticoagulation and plan for TEE cardioversion in the next few days
• C. Begin anticoagulation, and initiate amiodarone therapy in preparation for cardioversion
• D. Give digoxin in order to lead to spontaneous cardioversion
• A. Begin anticoagulation, and plan to cardiovert the patient in 3 weeks
• B. Begin anticoagulation and plan for TEE cardioversion in the next few days
• C. Begin anticoagulation, and initiate amiodarone therapy in preparation for cardioversion
• D. Give digoxin in order to lead to spontaneous cardioversion
Case PresentationCase Presentation
• 66 year old male
• Shortness of breath – few months
• FC NYHA I III• Chest CT: enlarged lymph nodes
• Biopsy: Sarcoidosis
• Treated with Steroids
• 66 year old male
• Shortness of breath – few months
• FC NYHA I III• Chest CT: enlarged lymph nodes
• Biopsy: Sarcoidosis
• Treated with Steroids

Case PresentationCase Presentation
• Systolic murmur on the apex
• Echo 1 year previously:
• Mod-severe Mitral Regurgitation
• LV size and Function normal
• Moderate PHT (50 mmHg)
• Started on Enalapril, metoprolol & Fusid
• Systolic murmur on the apex
• Echo 1 year previously:
• Mod-severe Mitral Regurgitation
• LV size and Function normal
• Moderate PHT (50 mmHg)
• Started on Enalapril, metoprolol & Fusid
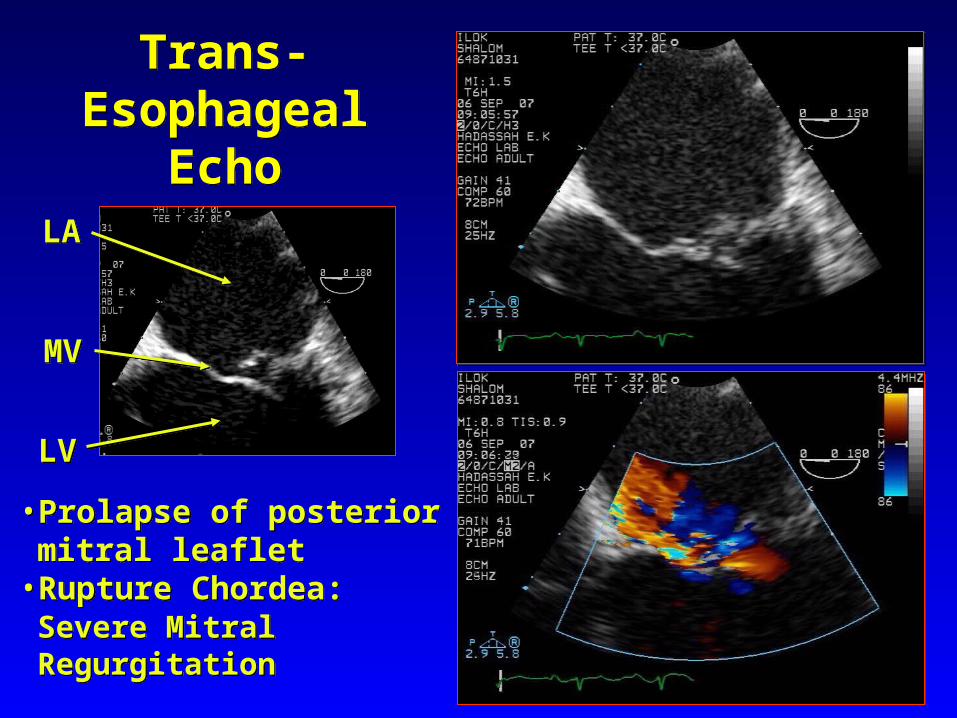
Trans-EsophagealEcho
Trans-EsophagealEcho
• Prolapse of posterior mitral leaflet
• Rupture Chordea:Severe Mitral Regurgitation
• Prolapse of posterior mitral leaflet
• Rupture Chordea:Severe Mitral Regurgitation
LVLV
MVMV
LALA
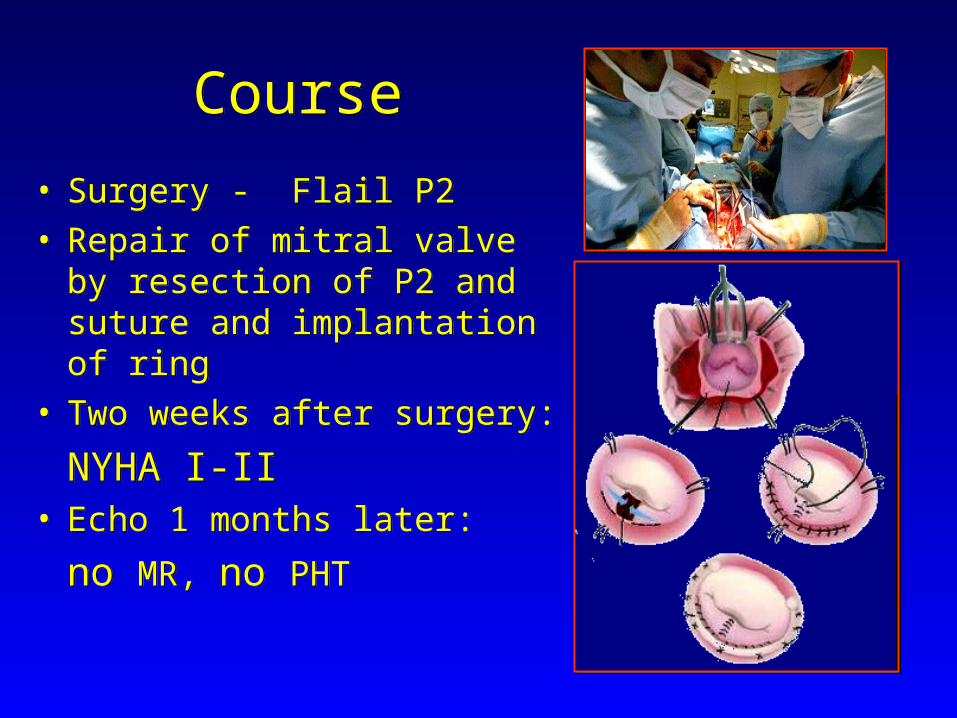
CourseCourse
• Surgery - Flail P2 • Repair of mitral valve by
resection of P2 and suture and implantation of ring
• Two weeks after surgery:
NYHA I-II• Echo 1 months later:
no MR, no PHT
• Surgery - Flail P2 • Repair of mitral valve by
resection of P2 and suture and implantation of ring
• Two weeks after surgery:
NYHA I-II• Echo 1 months later:
no MR, no PHT

Next caseNext case
• 41 year old woman
• Previously healthy
• Presents with acute decompensated heart failure
• 41 year old woman
• Previously healthy
• Presents with acute decompensated heart failure

EchoEcho

Patient begins to deteriorate, and is in low grade cardiogenic
shock
Patient begins to deteriorate, and is in low grade cardiogenic
shock
• What are possible causes?
• What do you do?
• What are possible causes?
• What do you do?
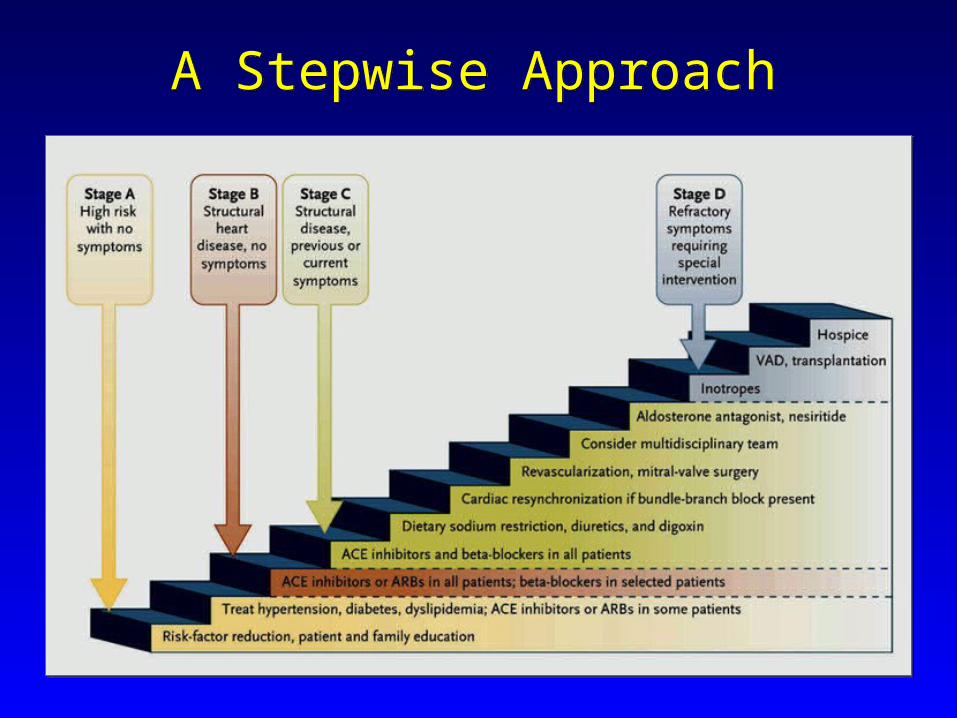
A Stepwise ApproachA Stepwise Approach
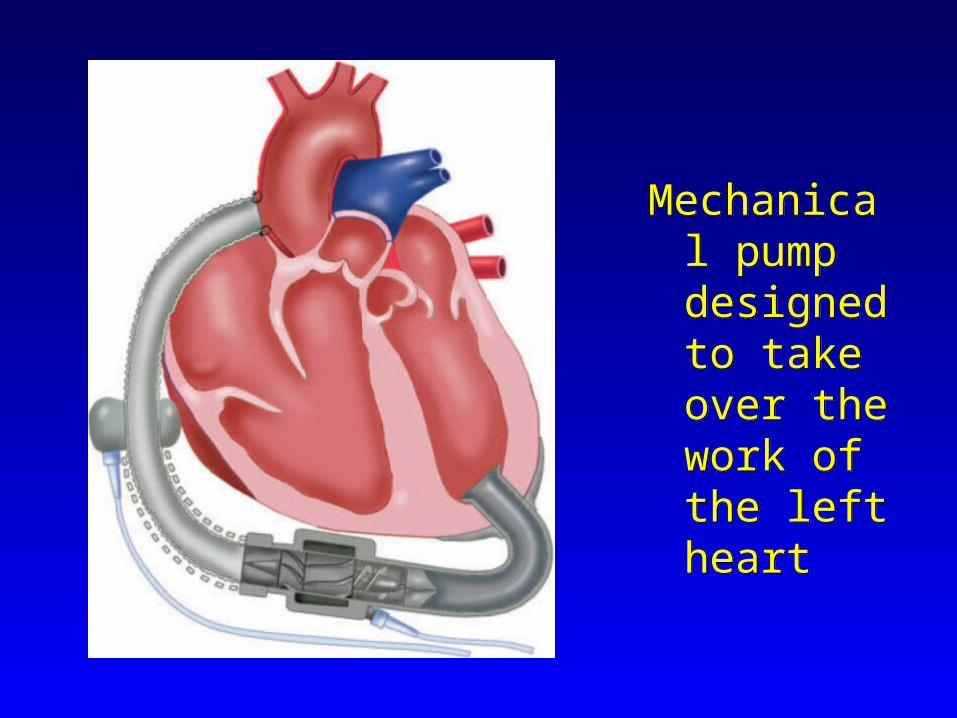
Mechanical pump designed to take over the work of the left heart
Mechanical pump designed to take over the work of the left heart

IndicationsIndications
• Transplant candidate or Destination candidate
• Hemodynamics:– Cardiac index < 2l/min/m2
– PCWP > 20mmHg– SBP < 80mmHg or MAP < 65mmHg– On maximal medical therapy
• Transplant candidate or Destination candidate
• Hemodynamics:– Cardiac index < 2l/min/m2
– PCWP > 20mmHg– SBP < 80mmHg or MAP < 65mmHg– On maximal medical therapy

Cardiac considerationsCardiac considerations
• Right ventricular function
• Valve disease (aortic regurgitation, mitral stenosis)
• Intracardiac shunt
• Ventricular arrhythmias
• Ischemia (consider RCA graft)
• Right ventricular function
• Valve disease (aortic regurgitation, mitral stenosis)
• Intracardiac shunt
• Ventricular arrhythmias
• Ischemia (consider RCA graft)
Non-cardiac considerationsNon-cardiac considerations
• Neurologic status
• Infection
• Risk of bleeding
• Urine output/urea
• Bilirubin
• Pulmonary disease
• Patient preference
• Neurologic status
• Infection
• Risk of bleeding
• Urine output/urea
• Bilirubin
• Pulmonary disease
• Patient preference
Technical considerationsTechnical considerations
• BSA < 1.5m2
• Prosthetic valves
• Reoperation
• LV thrombus
• BSA < 1.5m2
• Prosthetic valves
• Reoperation
• LV thrombus

Patient populationsPatient populations
• Post-cardiotomy failure
• Myocarditis
• Acute MI
• Acute decompensation of chronic heart failure
• Ventricular arrhythmias
• Post-cardiotomy failure
• Myocarditis
• Acute MI
• Acute decompensation of chronic heart failure
• Ventricular arrhythmias

Probability of Survival to TransplantProbability of Survival to Transplant
Frazier et al., J Thorac CV Surg 2001
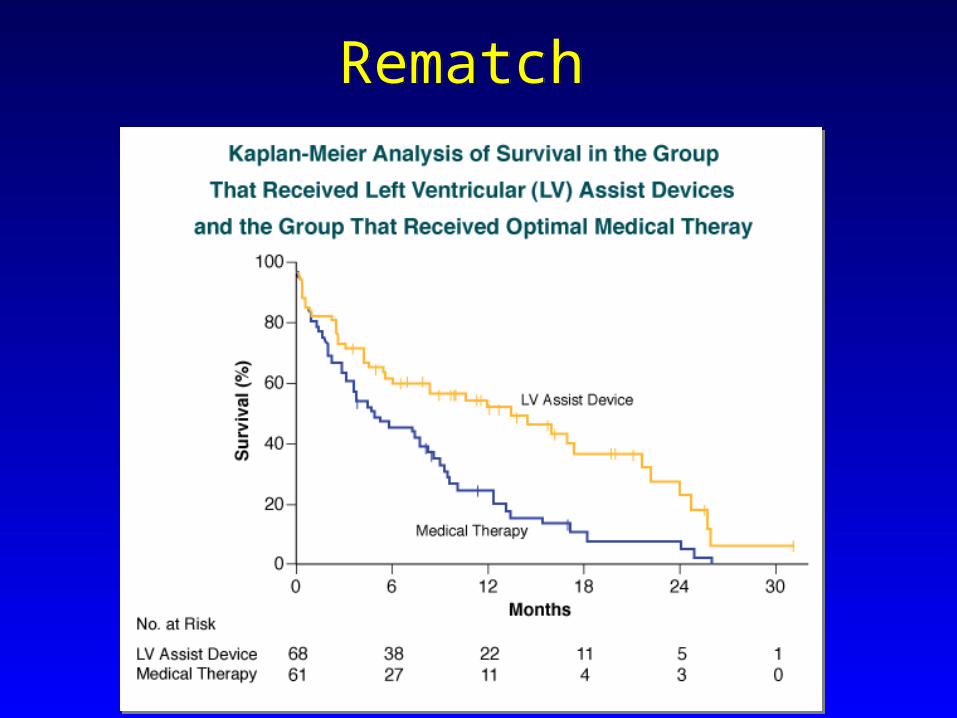
Rematch Rematch

Follow upFollow up
• The patient underwent LVAD placement, and underwent cardiac transplant one year later.
• The patient underwent LVAD placement, and underwent cardiac transplant one year later.
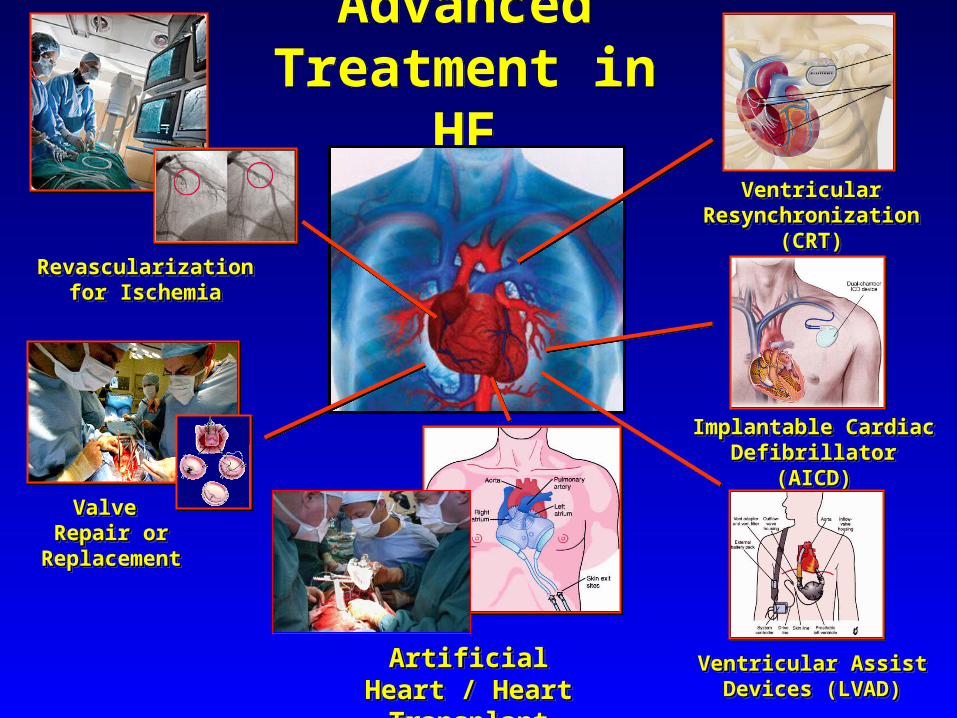
Advanced Treatment in HF
Advanced Treatment in HF
RevascularizationRevascularizationfor Ischemiafor Ischemia
RevascularizationRevascularizationfor Ischemiafor Ischemia
Valve Valve Repair or Repair or
ReplacementReplacement
Valve Valve Repair or Repair or
ReplacementReplacement
Ventricular Ventricular Resynchronization (CRT)Resynchronization (CRT)
Ventricular Ventricular Resynchronization (CRT)Resynchronization (CRT)
Implantable Cardiac Implantable Cardiac Defibrillator (AICD)Defibrillator (AICD)
Implantable Cardiac Implantable Cardiac Defibrillator (AICD)Defibrillator (AICD)
Ventricular Assist Ventricular Assist Devices (LVAD)Devices (LVAD)
Ventricular Assist Ventricular Assist Devices (LVAD)Devices (LVAD)
Artificial Heart / Artificial Heart / Heart TransplantHeart TransplantArtificial Heart / Artificial Heart /
Heart TransplantHeart Transplant

Thank youThank you