heart and lungs philippe heart... · 2014-05-22 · heart and lungs philippe meyer, md heart...
TRANSCRIPT

Heart and Lungs
Philippe Meyer, MD
Heart Failure and Cardiovascular rehabilitation Cardiology Service University Hospital of Geneva, Switzerland [email protected]
SGK Herbsttagung – Zürich - 22.11.2012

Anatomical proximity
Common pulmonary circulation

There are many conditions resulting from heart-lungs interactions in heart failure
Left-sided pulmonary hypertension
Sleep-disordered breathing
Acute pulmonary edema
Cor pulmonale
Restrictive lung disease
Right ventricular failure post-PE

There are many conditions resulting from heart-lungs interactions in heart failure
Left-sided pulmonary hypertension
Sleep-disordered breathing
Acute pulmonary edema
Cor pulmonale
Restrictive lung disease
Right ventricular failure post-PE

Plan
Definitions and epidemiology
Pathophysiology
Clinical implications
Therapies

Plan
Definitions and epidemiology
Pathophysiology
Clinical implications
Therapies

Definition of pulmonary hypertension (PH)
Mean pulmonary artery pressure (PAP)
≥25 mmHg
at rest
Galie N et al. Eur Heart J. 2009;30:2493-2537

Galie N et al. Eur Heart J. 2009;30:2493-2537
Most common form of PH

Hemodynamic definitions of PH due to left heart disease
Galie N et al. Eur Heart J. 2009;30:2493-2537
Definitions Characteristics
Post-capillary PH Mean PAP ≥25 mmHg at rest
PCWP >15 mmHg

«Passive» PH in heart failure
3.5 l/min
CO
• Transpulmonary gradient (TPG) = Mean PAP - Pulmonary Capillary
Wedge Pressure (PCWP) = 7 mmHg
TPG
(PCWP)

«Reactive or «out of proportion» PH in heart failure
4.6 l/min
CO
• Transpulmonary gradient (TPG) = Mean PAP - Pulmonary Capillary
Wedge Pressure (PCWP) = 23 mmHg
TPG
(PCWP)

Hemodynamic definitions of PH due to left heart disease
Galie N et al. Eur Heart J. 2009;30:2493-2537
Definitions Characteristics
Post-capillary PH Mean PAP ≥25 mmHg at rest
PCWP >15 mmHg
Passive PH TPG ≤12 mmHg
PVR ≤3 WU
Reactive (out of proportion) PH TPG >12 mmHg
PVR >3 WU

The concept of «reversibility» of PH
• Assessment of PH reversibility by different pharmacological agents during right heart catheterization is useful for stratifying risk before heart transplantation
• PH is considered reversible if PVR can be lowered to ≤2.5 Wood units (WU) without systemic hypotension (SBP >85 mmHg)

Hemodynamic definitions of PH due to left heart disease
Galie N et al. Eur Heart J. 2009;30:2493-2537
Haddad F Prog Cardiovasc Dis. 2011;54:154-167
Definitions Characteristics
Post-capillary PH Mean PAP ≥25 mmHg at rest
PCWP >15 mmHg
Passive PH TG ≤12 mmHg
PVR ≤3 WU
Reactive (out of proportion) PH TG >12 mmHg
PVR >3 WU
Reversible (vasoreactive) PH PVR ≤2.5 WU
Syst BP >85 mmHg
Non-reversible (non vasoreactive) PH PVR >2.5 WU or
Syst BP ≤85 mmHg
PH is highly prevalent in patients with HF
• ~40% in HF with reduced LVEF (NYHA functional class III-IV)
– Passive PH in 2/3 to 3/4 of cases
• 50-80% in HF with preserved LVEF
depending on populations and PH diagnostic criteria used
Galie N et al. Eur Heart J. 2009;30:2493-2537
Haddad F Prog Cardiovasc Dis. 2011;54:154-167

Plan
Definitions and epidemiology
Pathophysiology
Clinical implications
Therapies

Pathophysiology of PH in heart failure
Left-sided HF
LV filling pressures
«Passive» PH
gas exchange
STRUCTURAL CHANGES (AT-II, TNF, ET1, hypoxia)
VASOREACTIVITY ( ET1, NO)
RV failure
«Reactive» PH
Genes
Genes

Plan
Definitions and epidemiology
Pathophysiology
Clinical implications
Therapies

PH was repeatedly associated with mortality in HF
Study Patients Criteria Follow-up HR for death
Abramson 1992
(n=108)
Outpatient HFrEF
NYHA I–IV
TR velocity
>2.5 m/s 28 months 3.35
Cappola 2002
(n=1134) Outpatient HFrEF
PVR
>3 WU 48 months
Unadjusted
HR 2.3
Lam 2009
(n=244) Outpatient HFpEF PASP 34 months
1.2 per 10 mmHg
PASP
Aronson 2011
(n=242)
Hospitalized HFrEF
NYHA II
mPAP
>25 mmHg 6 months
2.8 (passive PH)
4.8 (reactive PH)
Szwejkowski
2012 (n=1612)
Outpatient HFrEF
Loop diuretics PASP 2.8 years
1.06 per 5 mmHg
PASP
Bursi 2012
(n=1049)
Outpatient HFrEF
+ HFpEF
PASP
>54 mmHg 2.7 years 2.07

PH was repeatedly associated with mortality in HF
Study Patients Criteria Follow-up HR for death
Abramson 1992
(n=108)
Outpatient HFrEF
NYHA I–IV
TR velocity
>2.5 m/s 28 months 3.35
Cappola 2002
(n=1134) Outpatient HFrEF
PVR
>3 WU 48 months
Unadjusted
HR 2.3
Lam 2009
(n=244) Outpatient HFpEF PASP 34 months
1.2 per 10 mmHg
PASP
Aronson 2011
(n=242)
Hospitalized HFrEF
NYHA II
mPAP
>25 mmHg 6 months
2.8 (passive PH)
4.8 (reactive PH)
Szwejkowski
2012 (n=1612)
Outpatient HFrEF
Loop diuretics PASP 2.8 years
1.06 per 5 mmHg
PASP
Bursi 2012
(n=1049)
Outpatient HFrEF
+ HFpEF
PASP
>54 mmHg 2.7 years 2.07

Bursi F et al. J Am Coll Cardiol 2012;59:222-31
• 1049 ambulatory HF patients, irrespective of LVEF
• PASP estimated by Doppler echo
• Follow-up 2.7 ± 1.9 years
Adjusted HR = 2.07

PH reversibility and prognosis pre-transplantation
• 298 patients, NYHA III-IV, LVEF, 3-months follow-up post-tx
• PH reversibility assessed by nitroprusside during RHC
Costard-Jäckle A, et al. J Am Coll Cardiol 1992;19:48e54.
PVR >2.5 WU Deaths: 17.9%
PVR <2.5 WU
Deaths: 6.9%
PVR <2.5 WU
PVR >2.5 WU
Deaths: 40.6%
SBP <85 mmHg
Deaths: 27.5%
SBP >85 mmHg
Deaths: 3.8%
Baseline RHC After Nitroprusside

Listing criteria for cardiac transplantation
• PH and elevated PVR should be considered as a relative contraindication to cardiac transplantation when PASP is >60 mmHg in the presence of PVR >5 WU or TPG >16-20 mmHg
• Patients can be considered eligible if PH is reversible by testing without systemic hypotension
Mehra MR et al. J Heart Lung Transplant 2006;25:1024e42.

RV dysfunction is also an established predictor of mortality in HF
Guazzi M et al. Nat. Rev. Cardiol. 2010;7:648–659
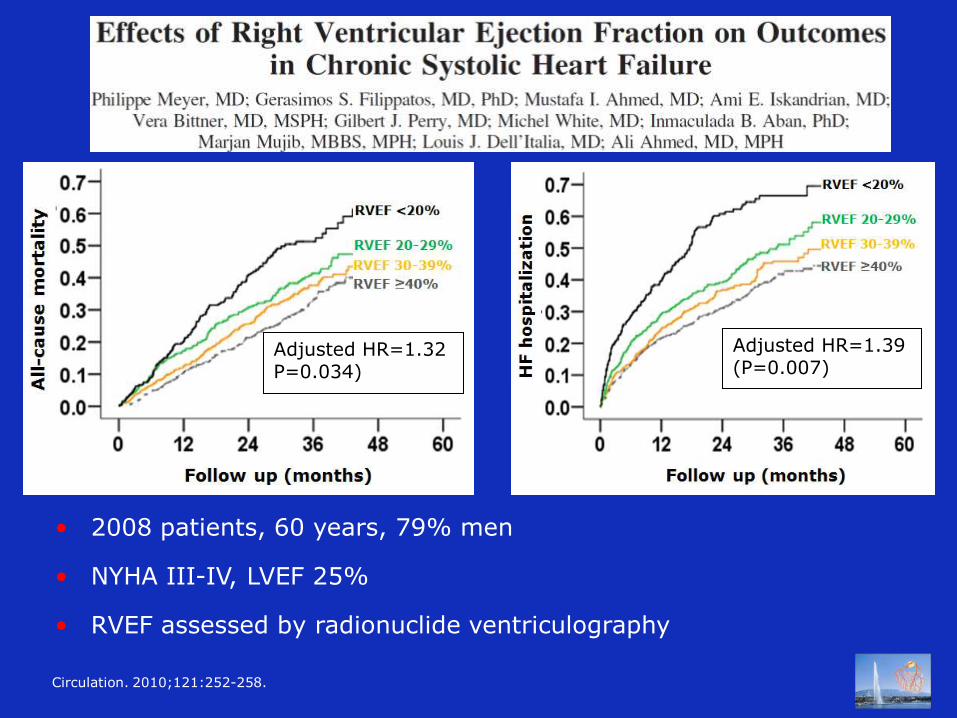
• 2008 patients, 60 years, 79% men
• NYHA III-IV, LVEF 25%
• RVEF assessed by radionuclide ventriculography
Circulation. 2010;121:252-258.
Adjusted HR=1.32 P=0.034)
Adjusted HR=1.39 (P=0.007)

Plan
Definitions and epidemiology
Pathophysiology
Clinical implications
Therapies

«General» HF therapy
• Several studies have shown that PH may regress after optimization of traditional evidence-based HF therapies (drugs, devices)
• The most spectacular effect on PAP reduction has been reported after LVAD implantation in several studies

• 50 patients, 54 years, 68% men
• HeartMate II «bridge to transplant», mean 281 days
• RHC at 3 months post-LVAD and 1 months post-tx
J Thorac Cardiovasc Surg 2010;140:447-452.
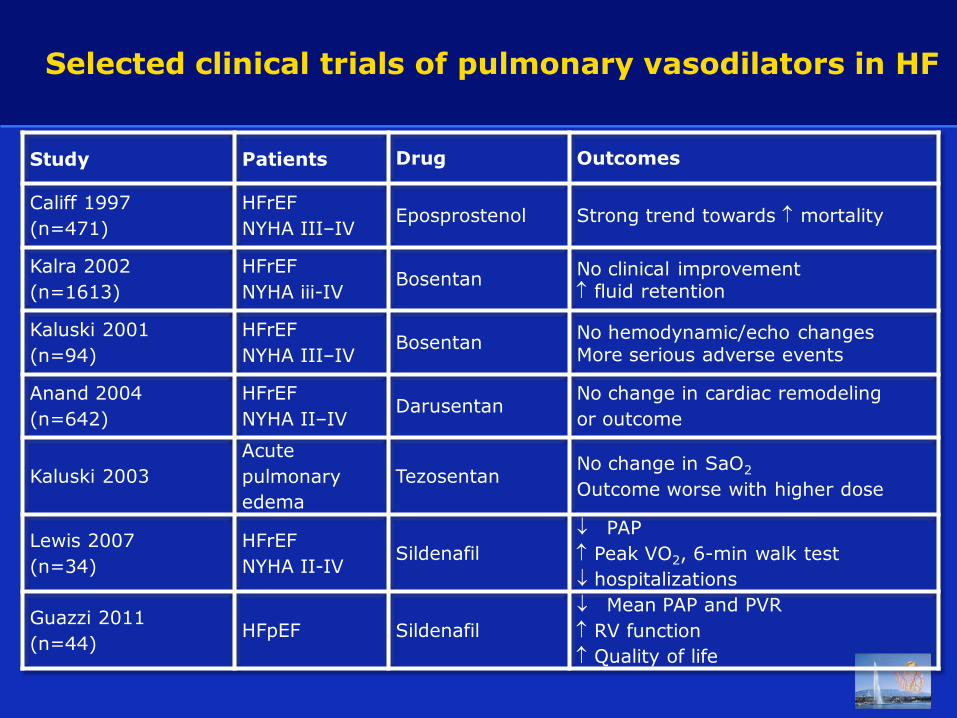
Selected clinical trials of pulmonary vasodilators in HF
Study Patients Drug Outcomes
Califf 1997
(n=471)
HFrEF
NYHA III–IV Eposprostenol Strong trend towards mortality
Kalra 2002
(n=1613)
HFrEF
NYHA iii-IV Bosentan
No clinical improvement fluid retention
Kaluski 2001
(n=94)
HFrEF
NYHA III–IV Bosentan
No hemodynamic/echo changes More serious adverse events
Anand 2004
(n=642)
HFrEF
NYHA II–IV Darusentan
No change in cardiac remodeling
or outcome
Kaluski 2003
Acute
pulmonary
edema
Tezosentan No change in SaO2
Outcome worse with higher dose
Lewis 2007
(n=34)
HFrEF
NYHA II-IV Sildenafil
PAP
Peak VO2, 6-min walk test
hospitalizations
Guazzi 2011
(n=44) HFpEF Sildenafil
Mean PAP and PVR
RV function
Quality of life

Selected clinical trials of pulmonary vasodilators in HF
Study Patients Drug Outcomes
Califf 1997
(n=471)
HFrEF
NYHA III–IV Eposprostenol Strong trend towards mortality
Kalra 2002
(n=1613)
HFrEF
NYHA iii-IV Bosentan
No clinical improvement fluid retention
Kaluski 2001
(n=94)
HFrEF
NYHA III–IV Bosentan
No hemodynamic/echo changes More serious adverse events
Anand 2004
(n=642)
HFrEF
NYHA II–IV Darusentan
No change in cardiac remodeling
or outcome
Kaluski 2003
Acute
pulmonary
edema
Tezosentan No change in SaO2
Outcome worse with higher dose
Lewis 2007
(n=34)
HFrEF
NYHA II-IV Sildenafil
PAP
Peak VO2, 6-min walk test
hospitalizations
Guazzi 2011
(n=44) HFpEF Sildenafil
Mean PAP and PVR
RV function
Quality of life

Selected clinical trials of pulmonary vasodilators in HF
Study Patients Drug Outcomes
Califf 1997
(n=471)
HFrEF
NYHA III–IV Eposprostenol Strong trend towards mortality
Kalra 2002
(n=1613)
HFrEF
NYHA iii-IV Bosentan
No clinical improvement fluid retention
Kaluski 2001
(n=94)
HFrEF
NYHA III–IV Bosentan
No hemodynamic/echo changes More serious adverse events
Anand 2004
(n=642)
HFrEF
NYHA II–IV Darusentan
No change in cardiac remodeling
or outcome
Kaluski 2003
Acute
pulmonary
edema
Tezosentan No change in SaO2
Outcome worse with higher dose
Lewis 2007
(n=34)
HFrEF
NYHA II-IV Sildenafil
PAP
Peak VO2, 6-min walk test
hospitalizations
Guazzi 2011
(n=44) HFpEF Sildenafil
Mean PAP and PVR
RV function
Quality of life

• 44 patients, 72 years, 80% men
• Clinical HF, diastolic dysfunction, LVEF >50%, and PASP >40 mmHg
• Sildenafil 3 x 50 mg vs placebo
Circulation. 2011;124:164-174.
PVR (WU)

But…
Phosphodiesterase-5 inhibitors should still be
considered as experimental since their
benefits have not been proved in a large RCT
with clinical endpoints

Galie N et al. Eur Heart J. 2009;30:2493-2537

Promising novel agents
• Direct stimulator of soluble guanylate cyclase (sGC)
• Phase 2 clinical trial in patients with HFrEF and mPAP ≥25 mmHg
• Presented at AHA congress on November 5th
• No effect on mean PAP but increase in cardiac output
• Good safety profile

Conclusions
• PH due to left-sided heart failure is the most common cause of PH
• Left-sided PH and RV dysfunction are independent predictors of poor outcomes in patients with chronic HF
• Most of selective pulmonary vasodilators were disappointing in HF but patients selection may have been inadequate
• Promising results have been observed with the use of PDE-5 inhibitors but larger clinical trials are needed
• Further research is needed on the pathophysiology of left-sided PH in order to improve its management

Thank you for your attention
Philippe Meyer, MD
Heart Failure and Cardiovascular rehabilitation Cardiology Service University Hospital of Geneva, Switzerland [email protected]
SGK Herbsttagung – Zürich - 22.11.2012