health systems research unit report back from cardiovascular disease working group western cape...
TRANSCRIPT

HEALTH SYSTEMS RESEARCH UNIT
Report Back from Cardiovascular DiseaseWorking Group
Western Cape Burden of DiseaseWestern Cape Burden of Disease
Volume 6 of 7

1. Develop a conceptual framework based upon a literature review to identify the causal factors associated with poor diet and lack of physical activity.
2. Review the epidemiological data of the distribution of these risk factors across the province.
3. Systematicaly review interventions that have sought to address these risk factors.
4. Further planned that the working group will systematically identify the most appropriate and feasible interventions that could be considered in the Province.
5. Finally an analysis of the context of policy-making in regard to these interventions will be undertaken to include a stakeholder analysis.
Operational process of CVD work group:
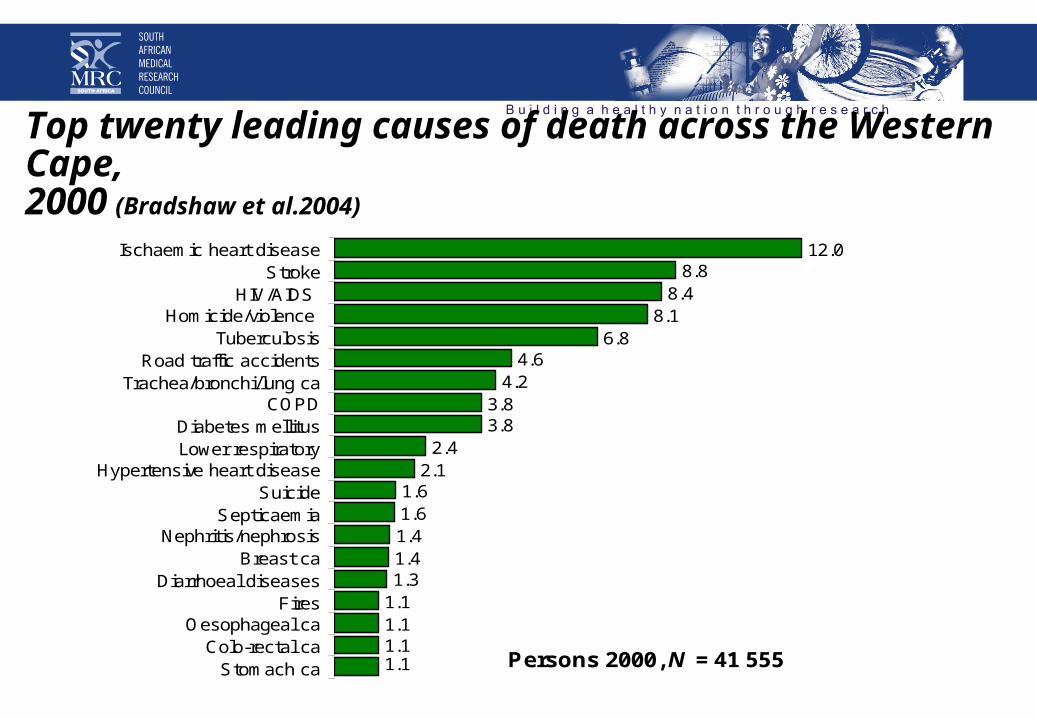
12.08.8
8.48.1
6.84.6
4.23.83.8
2.42.1
1.61.61.41.41.3
1.11.11.11.1
Ischaemic heart diseaseStroke
HIV/AIDS Homicide/violence
TuberculosisRoad traffic accidents
Trachea/bronchi/lung caCOPD
Diabetes mellitusLower respiratory
Hypertensive heart diseaseSuicide
SepticaemiaNephritis/nephrosis
Breast caDiarrhoeal diseases
FiresOesophageal ca
Colo-rectal caStomach ca
Top twenty leading causes of death across the Western Cape,2000 (Bradshaw et al.2004)
Persons 2000, N = 41 555
Ischaemic heart diseaseStroke
HIV/AIDS Homicide/violence
TuberculosisRoad traffic accidents
Trachea/bronchi/lung caCOPD
Diabetes mellitusLower respiratory
Hypertensive heart diseaseSuicide
SepticaemiaNephritis/nephrosis
Breast caDiarrhoeal diseases
FiresOesophageal ca
Colo-rectal caStomach ca

Projected percentage increase in CVD deaths 2000-2040
Taken from Leeder et al 2005

Triple burden of disease in the Western Province

NCD rates similar across the various communities
Figure 4: Age standardised NCD death rate per 100 000 in 2001
0
100
200
300
400
500
600
700
800
900
1000
Ath
lon
e
Bla
auw
be
rg
Ce
ntr
al
He
lderb
erg
Khaye
litsh
a
Mitc
hells
Pla
in
Nya
ng
a
Oo
sten
berg
South
Pen
insu
la
Tyg
erb
erg
East
Tyg
erb
erg
We
st
Metr
o/U
nic
ity

Increasing numbers of middle age workers
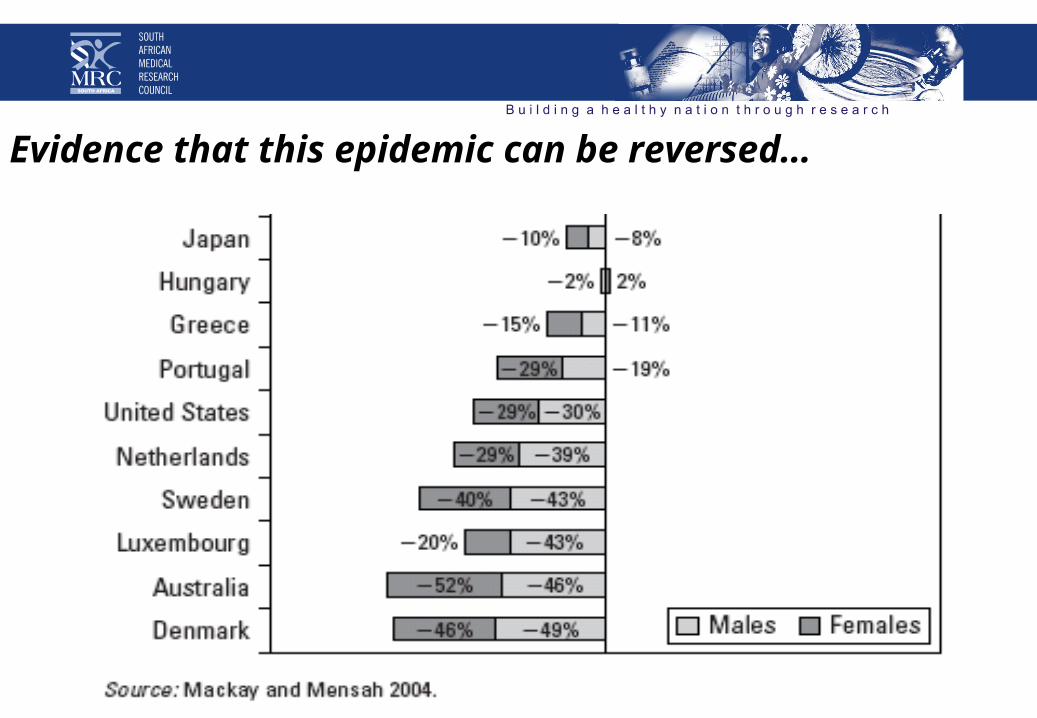
Evidence that this epidemic can be reversed…

…from…Preventing Chronic Diseases: a vital investment. Geneva, World Health Organization, 2005.
Aetiology of chronic non-communicable diseases
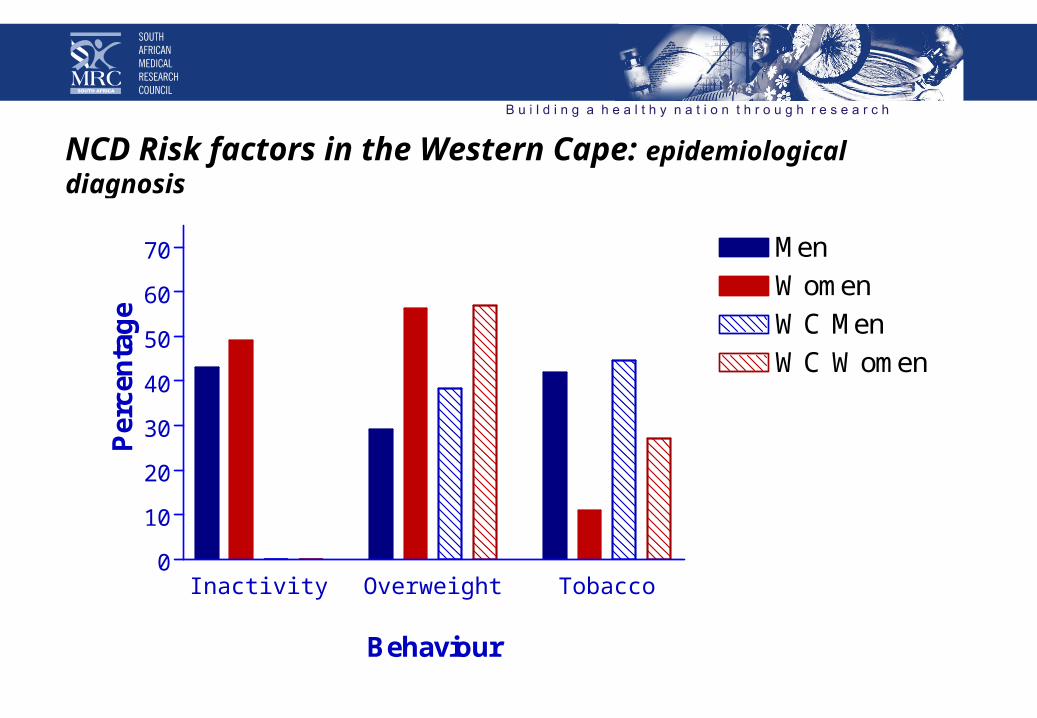
NCD Risk factors in the Western Cape: epidemiological diagnosis
Inactivity Overweight Tobacco0
10
20
30
40
50
60
70 MenWomenWC MenWC Women
Behaviour
Per
cen
tag
e

Smoking Overweight Inactivity0
10
20
30
40
50
National (M)
National (F)
W Cape (M)
W Cape (F)
Pre
va
len
ce
(%
)
Source: Youth Risk Behavior Survey, 2002
Behavioural diagnosis: national risk factor survey in adolescents:
Smoking
• Important interventions have already been put in place• Surveys suggest that there has been a reversal of upward
prevalence of smoking especially amongst African men• Important sub-groups still have high levels• Systematic review of interventions in pregnancy• Interventions with pregnant women being evaluated presently
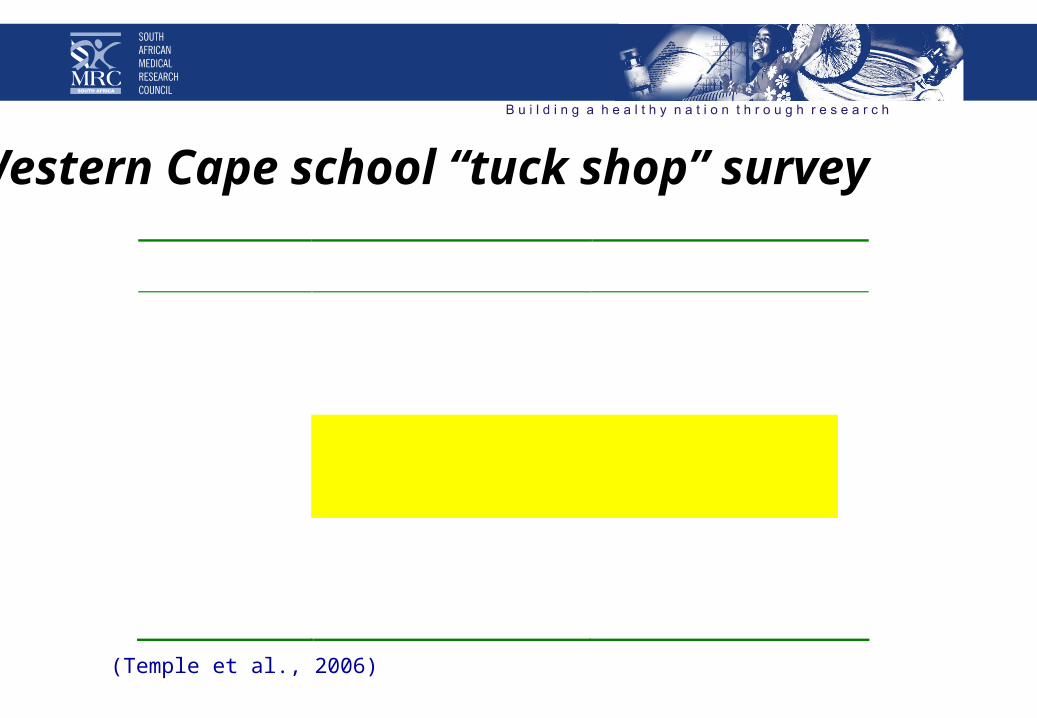
Western Cape school “tuck shop” survey
Category Items % of pupils who purchased
“Healthy” Fruit 11.8% Fruit juice 10.7% Nuts 6.5% Brown bread 4.6% “Unhealthy” Potato chips 46.3% Sweets and chocolates 46.0% Soft drinks 33.2% French fries 25.6% Meat pies, sausage rolls 12.2% Cookies 11.8% “Fat cakes” (fried dough) 9.5% Hot dogs 8.2% White bread 5.5%
(Temple et al., 2006)
The potential future of nutritional risks
Systematic Review• Systematic approaches designed to increase levels of participation in
physical activity,
• Approaches above may have included interventions targeting changes in awareness, knowledge and/or attitudes toward nutrition and physical activity, improving self-efficacy, skill or competency concerning these behaviors;
• Interventions may also have included programs or strategies targeting changes in social norms, policy and physical environment, health services or consumer behavior etc, leading to, for example, increased consumption of fruits and vegetables, reduced dietary fat intake, reduced obesity prevalence and increased levels of health-enhancing physical activity.

Various levels of intervention for prevention & health promotionbased on McKinlay, 1995 (extracted from Rowland, 2006)
Type of intervention Examples of interventions
1. Downstream interventions
Interventions that target the individual, usually those at risk
Individual counseling Group counseling Education Self-help programmes Pharmacological treatments
2. Midstream interventions
Interventions that target populations, usually using organisational structures or the natural environment
Worksite and community-based health promotion programmes School-based activities Community based activities targeting at-risk populations
3. Upstream interventions
Interventions that aim to strengthen social norms that promote healthy behaviour and to redirect counter veiling social forces.
National and state wide media and social marketing campaigns Economic incentives and disincentives Policies restricting access Policies affecting marketing and sales Policies restricting advertising and promotion
Community/ecological interventions target all levels; structural interventions target either or both midstream (2) & upstream levels (3)
Results from review
A review of more than 300 interventions have shown
• that very few studies are from developing countries • and none published were from sub-Saharan Africa.
• Despite this, there have been numerous successful interventions which have been sustainable and cost-effective and have the potential to be used in the South African context.

Summary of best practice review by setting (1):
Settings
Strongly recommended Recommended/Promising Not shown to be effective
Policy (Government) & Environment
Government regulatory policies to support healthier composition of staple foods (e.g. replacing palm oil with soy reduces saturated fatty acid content of the oil)
Environmental interventions
targeting the built environment, and policy to reduce barriers to physical activity for transport and increase space for recreational activity
Point-of-decision prompts to
encourage increased use of the stairs
Pricing strategies (fiscal policies), signage and point-of-purchase prompts in grocery stores, vending machines, cafeterias and restaurants to support healthier choices
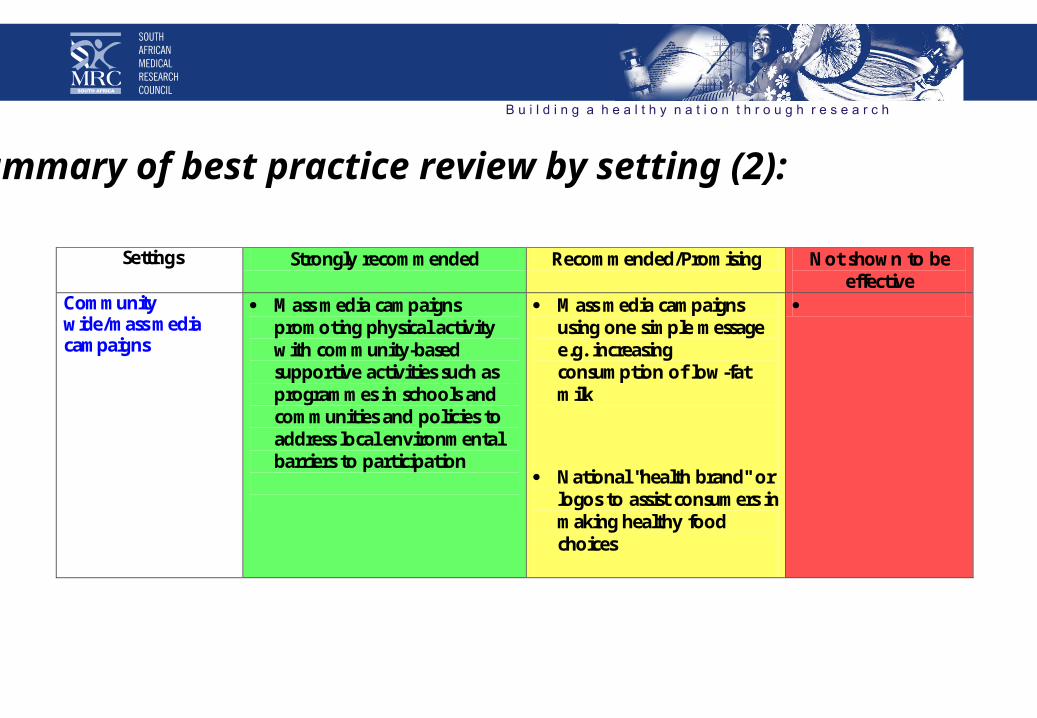
Summary of best practice review by setting (2):
Settings
Strongly recommended Recommended/Promising Not shown to be effective
Community wide/mass media campaigns
Mass media campaigns promoting physical activity with community-based supportive activities such as programmes in schools and communities and policies to address local environmental barriers to participation
Mass media campaigns using one simple message e.g. increasing consumption of low-fat milk
National "health brand" or logos to assist consumers in making healthy food choices

Summary of best practice review by setting (3):
Settings
Strongly recommended Recommended/Promising Not shown to be effective
School-based settings
School-based interventions that focus on diet and/or physical activity, are comprehensive and multi-component and include: Curriculum on diet and/or physical activity taught by trained teachers, supportive school environment/policies, a physical activity program, parental/family component ,food service component (healthy food options available through school food services: cafeteria, vending machines, etc)
A more focused approach may also be successful, for example, programs aimed at reducing sedentary behaviour and increasing participation in physical activity, if they are accompanied by supportive activities and curricularised.
After-school physical activity programmes or holiday programmes not linked to existing school or community programmes
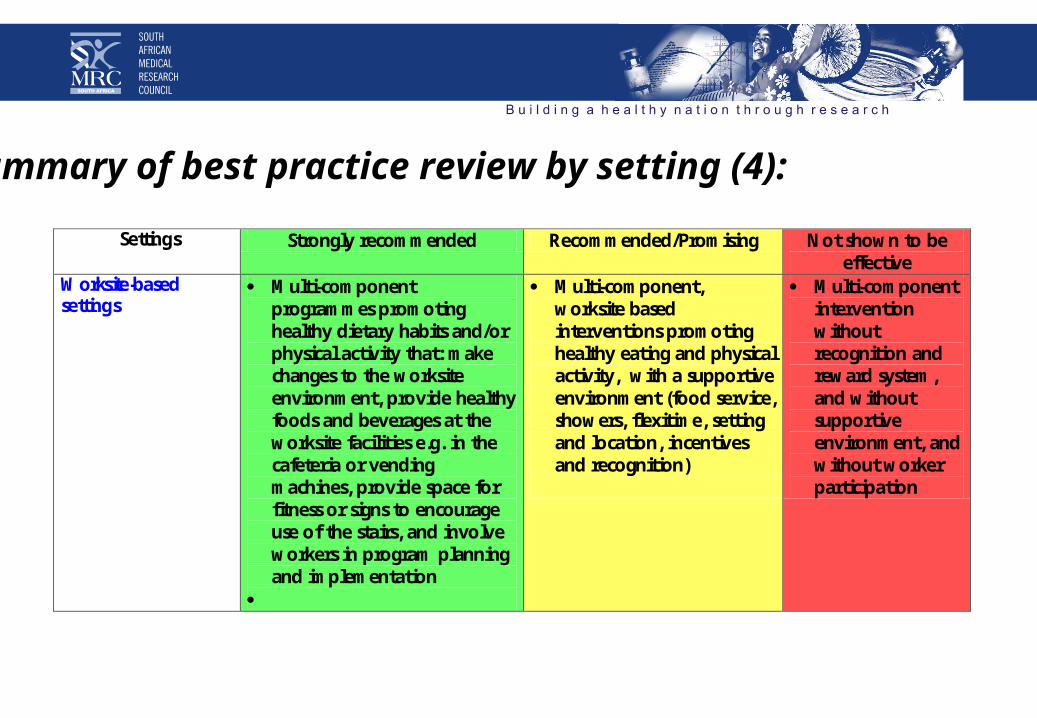
Summary of best practice review by setting (4):
Settings
Strongly recommended Recommended/Promising Not shown to be effective
Worksite-based settings
Multi-component programmes promoting healthy dietary habits and/or physical activity that: make changes to the worksite environment, provide healthy foods and beverages at the worksite facilities e.g. in the cafeteria or vending machines, provide space for fitness or signs to encourage use of the stairs, and involve workers in program planning and implementation
Multi-component, worksite based interventions promoting healthy eating and physical activity, with a supportive environment (food service, showers, flexitime, setting and location, incentives and recognition)
Multi-component intervention without recognition and reward system, and without supportive environment, and without worker participation
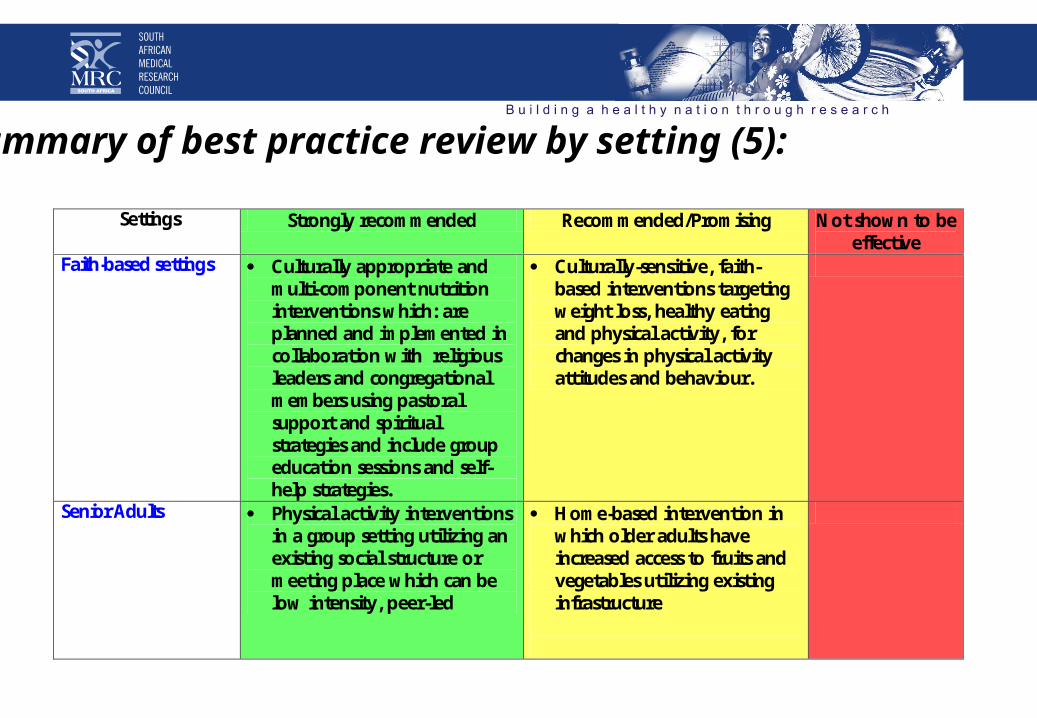
Summary of best practice review by setting (5):
Settings
Strongly recommended Recommended/Promising Not shown to be effective
Faith-based settings
Culturally appropriate and multi-component nutrition interventions which: are planned and implemented in collaboration with religious leaders and congregational members using pastoral support and spiritual strategies and include group education sessions and self-help strategies.
Culturally-sensitive, faith-based interventions targeting weight loss, healthy eating and physical activity, for changes in physical activity attitudes and behaviour.
Senior Adults
Physical activity interventions in a group setting utilizing an existing social structure or meeting place which can be low intensity, peer-led
Home-based intervention in which older adults have increased access to fruits and vegetables utilizing existing infrastructure

Summary of best practice review by setting (6): Settings
Strongly recommended Recommended/Promising Not shown to be
effective Community-support Settings
Nutrition education programs and healthy lifestyle programes that target high risk groups (e.g. menopausal, pre-diabetic women), that are multi-component and incorporate education and information, along with behavioural interventions
Utilising an existing phone-in service to provide dietary advice \
Programmes that target low-income/low literacy populations and provided focused nutrition education in addition to the standard program
Supermarket tours and on-
site educational programs to support purchasing of healthier foods
Community-participation
campaign with inter-sectoral cooperation (e.g. Walking school bus)
Community-based programmes developed without community participation.
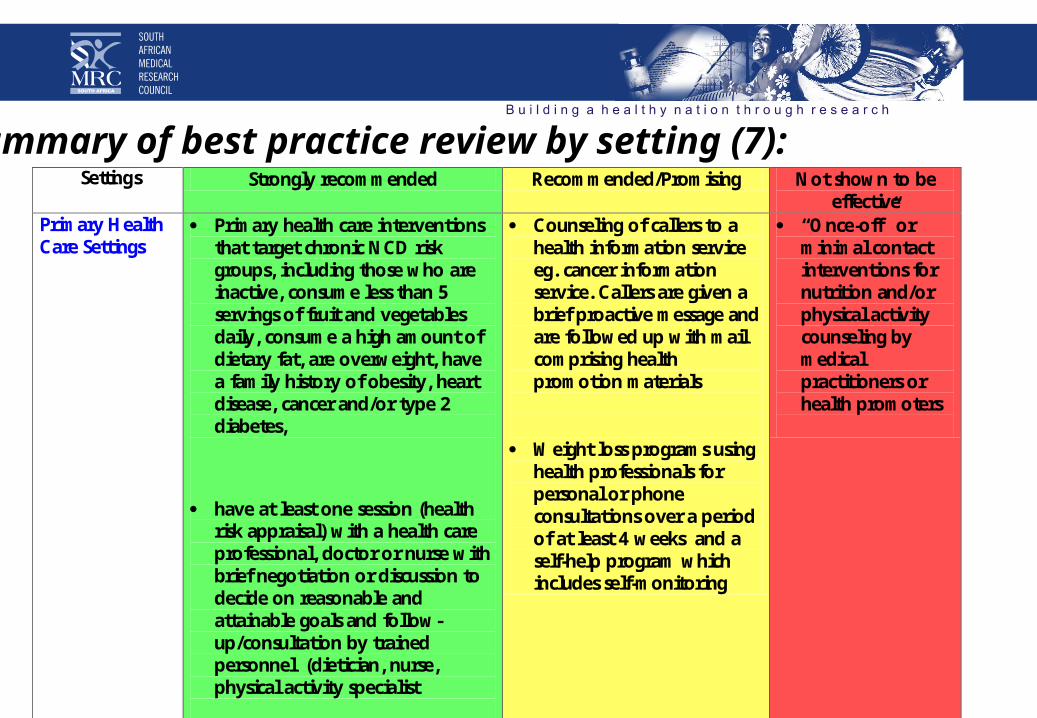
Summary of best practice review by setting (7): Settings
Strongly recommended Recommended/Promising Not shown to be
effective Primary Health Care Settings
Primary health care interventions that target chronic NCD risk groups, including those who are inactive, consume less than 5 servings of fruit and vegetables daily, consume a high amount of dietary fat, are overweight, have a family history of obesity, heart disease, cancer and/or type 2 diabetes,
have at least one session (health risk appraisal) with a health care professional, doctor or nurse with brief negotiation or discussion to decide on reasonable and attainable goals and follow-up/consultation by trained personnel (dietician, nurse, physical activity specialist
Counseling of callers to a health information service eg. cancer information service. Callers are given a brief proactive message and are followed up with mail comprising health promotion materials
Weight loss programs using
health professionals for personal or phone consultations over a period of at least 4 weeks and a self-help program which includes self-monitoring
“Once-off” or minimal contact interventions for nutrition and/or physical activity counseling by medical practitioners or health promoters

School Setting
• * Multi-component school programs which include;– a nutrition-based curriculum offered by trained teachers, a physical activity
component; – a healthy school environment and parental involvement.
• The curriculum should preferably run over 3 years in grade 4-6 children. • Two excellent examples in this regard are the PATHWAYS study which was
developed for American Indians and the Know Your Body Program offered to primary school children in Crete.
• Both of these studies were adapted to local culture, values and norms and showed positive outcomes in behavior, clinically and in psycho-social aspects.
Worksite Setting
The successful studies were characterized by the following:
• nutrition and physical activity advice/group sessions;
• a physical activity program;
• changes in the food service canteens;
• use of printed materials and use of multi-media to promote health messages.
• One of the most important factors in promoting successful outcomes was the use of an employee committee who participated in planning and managing a worksite program.
• A good example of this is the Treatwell -5-a Day program.

Primary Health Care Setting
• Interventions in primary health care and in the community with successful outcomes at the lowest level of cost.
• These include using physicians to endorse healthy programs, dietitians or nurses to do group counseling.
• The use of self-help materials for patients to use on their own.
• Brief cholesterol screening programs with a minimum time spent on counseling were also effective in some studies.
• The use of the media as a means of conveying healthy lifestyle messages was also shown to be effective in many studies.
Modification to improve diet
• * Ban advertising of foods during children’s programs on radio & TV or reduce the market pressure on children by regulating advertising and obtaining cooperation from the mass media and Internet providers
• * Introduce advertising and educational campaigns (multi-media) to promote increased consumption of fruit and vegetables and decreased consumption of fat, saturated fats, sugar and salt. Includes developing and building-on to the food-based dietary guidelines of the DOH.
• * Ensure that communities have access to healthy and safe foods (food security) – such as food gardens, food outlets
• * Develop and implement a policy for schools on foods which are allowed to be sold/provided at the schools-including feeding schemes and tuckshops

Further Recommendations
• Introduce a nutrition & healthy lifestyle curriculum aimed at schoolchildren for the prevention of CVD
• Ensure that all state facilities provide healthy foods (high in fruit and vegetables, low in salt, sugar and fats to inmates and patients
• Develop a system of incentives for companies who introduce healthy canteens and physical activity facilities for their staff
• trans fat: getting rid of partially hydrogenated oils is one of the simplest ways to prevent CVD.
• Cut the sodium content of packaged and restaurant foods could make a huge dent in CVD.
• "1% Or Less": switch people in several communities from high-fat to low-fat or fat-free milk.
Modification methods to improve physical activity
• * Ensure that urban development includes access to areas for physical activity
• * Introduce advertising campaigns (multi-media) to promote physical activity
• * Introduce a physical activity curriculum aimed at schoolchildren for the prevention of CVD
• * Ensure that all schools have adequate space and facilities for physical activity
• * Ensure that all communities have access to safe areas where they can be physically active

Modification methods to reduce tobacco use and alcohol
• * Increase the price of alcohol and cigarettes• * Ban advertising of alcohol• * Introduce a school policy of a smoke free environment
Members of the Working Group
Authors • Prof Mickey Chopra (HSRU, MRC) • Dr Nelia Steyn (CDL, MRC)• Prof Vicky Lambert (UCT)Expert Committee• Prof. Thandi Puoane (SOPH, UWC)• Prof. Krisela Steyn (University of Cape Town)• Prof Dinky Levitt (University of Cape Town)• Dr Yusuf Saloojee (National Council Against Smoking)• Dr Emmanual Deviaud (Health Economist, MRC)• Dr Sue Parnell (University of Cape Town)• Prof Vanessa Watson (Planning, UCT)• Dr Lesley Bourne (Health and Development, MRC)